Back to Journals » International Journal of Nanomedicine » Volume 21
Cell Membrane-Coated Nanoparticles: Advanced Drug Delivery Systems for Chronic Wound Healing Therapy
Authors Zhao X, Liu Q, Xu Z, Yang F, Li Z, Bai X, Zhu H, Liu Y, Wang Y ![]()
Received 27 August 2025
Accepted for publication 29 January 2026
Published 26 February 2026 Volume 2026:21 563555
DOI https://doi.org/10.2147/IJN.S563555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Eng San Thian
Xuan Zhao,1– 4,* Qinxin Liu,1– 4,* Zhikai Xu,1– 4 Fan Yang,1– 4 Zhanfei Li,1– 4 Xiangjun Bai,1– 4 Hao Zhu,5 Yukun Liu,6 Yuchang Wang1– 4
1Division of Trauma Surgery, Emergency Surgery & Surgical Critical, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 2Trauma Center, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 3Department of Emergency and Critical Care Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 4Sino-German Research Institute of Disaster Medicine, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 5Department of Orthopedic Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 6Department of Plastic and Aesthetic Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yukun Liu, Email [email protected] Yuchang Wang, Email [email protected]
Abstract: Cell membrane-coated nanoparticles (CMNPs) have emerged as a promising platform for targeted drug delivery and therapeutic applications due to their unique properties, such as improved biocompatibility, prolonged circulation time, and ability to mimic natural cell functions. The preparation of CMNPs involves three critical stages: extraction of the cell membrane, preparation of the nanoparticle core, and membrane coating. The cell membrane is isolated through various methods, including hypotonic lysis, freeze-thaw cycles, and centrifugation, with careful attention paid to preserving its integrity and functionality. Nanoparticle cores, which can be organic (eg, PLGA, liposomes) or inorganic (eg, metal-based cores), offer distinct advantages in terms of drug loading capacity, stability, and therapeutic potential. The fusion of the core and the membrane is typically achieved through techniques such as membrane extrusion, sonication, and electroporation. These methods enable the efficient formation of core-shell nanostructures, which can be utilized for a range of biomedical applications, particularly in drug delivery, cancer therapy, and tissue regeneration. This review discusses the key aspects of CMNP preparation, including membrane extraction and purification techniques, core selection, and fusion methods, as well as the current trends and future directions in the development of CMNPs for therapeutic purposes.
Keywords: cell membrane-coated nanoparticles, drug delivery, wound healing, nanoparticles, chronic wound healing
Introduction
Chronic non-healing wounds (CRWs) are defined as wounds that fail to achieve complete structural and functional repair within the expected timeframe, despite receiving standard systemic treatments. Due to their complex pathogenesis, prolonged course, and poor prognosis, CRWs present one of the most challenging clinical problems.1,2 Based on their complicated mechanisms of pathogenesis, chronic wounds are often categorized into seven subtypes: diabetic foot ulcers, pressure ulcers, burns, surgical incisions, neuropathic ulcers, arterial ulcers, and venous ulcers. Among these, non-healing pressure ulcers (NHPUs), venous ulcers (VUs), and diabetic foot ulcers (DFUs) are the most common.3,4 In recent years, the prevalence of chronic wound patients has surged, primarily due to the increasing numbers of individuals with conditions such as diabetes and obesity, in addition to external physical injuries.5,6 In the United States, chronic wounds affect approximately 10.5 million Medicare beneficiaries (an increase of 2.3 million compared to 2014), with annual treatment costs exceeding $25 billion.7,8 Despite this, there are still numerous challenges in rapidly and efficiently promoting the healing of skin wounds.
At present, the clinical treatment of chronic wounds mainly relies on traditional methods such as debridement, dressing coverage, negative pressure drainage, and hyperbaric oxygen therapy, as well as emerging biological therapies such as growth factor and stem cell therapy. However, all these strategies have obvious limitations:9–15traditional debridement and dressing replacement can only provide a basic physical barrier and passive healing environment, and are unable to actively regulate the microenvironment of the wound surface. Systemic antibiotic administration is difficult to achieve an effective concentration at the infection site and is prone to drug resistance. Exogenous growth factors and stem cells, however, are confronted with bottlenecks such as poor stability in vivo, low survival rates, and insufficient targeting.
In response to these challenges, researchers have proposed many new therapeutic methods in wound healing studies, aiming to develop effective treatments for various stages of wound healing, or even for the entire process. Since wounds exhibit differences in molecular and cellular mechanisms, the treatment strategies for these injuries are diverse.16 The emergence of nanoparticle (NPs) technology has provided a new approach to overcoming the aforementioned limitations. In recent years, localized drug delivery strategies using nanoparticles (NPs), stem cells, bioprinting, extracellular matrix (ECM), platelet-rich plasma, cold atmospheric plasma, and microRNAs have been increasingly applied in the treatment of CRWs. These strategies can be used to initiate and maintain cellular functions, activate collagen synthesis, promote angiogenesis, regulate cytokines, activate growth factors (GFs), and provide antimicrobial effects, among other functions.17 Among these, various types of nanoparticles have been widely used in wound healing therapy due to their unique properties.18 NPs, with its nanoscale size effect, can effectively penetrate the biofilm barrier, protect the active ingredients of drugs from degradation, and accumulate locally in the wound through the enhanced penetration and retention effect (EPR).19,20 These nanoparticles can also load various drugs, enhancing the stability and solubility of the encapsulated agents, facilitating transmembrane transport, prolonging circulation time, and improving safety and efficacy.21,22 For example, mesoporous silica nanoparticles (MSNs), with their unique mesoporous structure, large surface area, high loading capacity, stable pore volume, controllable particle size, ease of surface functionalization, and excellent biocompatibility and biodegradability, make them excellent substrates for constructing various nanocomposite drug delivery systems.23 Through special design, MSNs have significantly accelerated the healing process of diabetic wounds (DWs) and infectious wounds.24–26 Common engineered precision nanoparticles for drug delivery include polymeric nanoparticles, inorganic nanoparticles, and lipid nanoparticles, each of which has multiple subtypes with distinct advantages and disadvantages in drug loading, delivery efficiency, and patient response.27
However, most nanoparticle platforms are synthetically engineered, and their foreign nature may lead to recognition by the immune system once they enter the body, resulting in their rapid clearance, which limits their biostability and targeting ability.28,29 This limitation reveals a key scientific question: How can we retain the excellent drug loading capacity of synthetic nanoparticles while endowing them with the biological intelligence for seamless interaction with biological systems? Cell membrane-coated nanoparticles (CNPs) technology is precisely a revolutionary strategy to address this challenge, ingeniously integrating the high loading capacity of synthetic nanomaterials with the biocompatibility of natural cell membranes.28–31 To enable nanoparticles to achieve immune escape, cell membrane-coated nanoparticles (CNNPs) emerged. In recent years, CNNPs have shown promising prospects for disease diagnosis, treatment and prevention.30,31 Compared with traditional nanoparticles, CNPs demonstrate unique advantages in the treatment of chronic wounds: their natural membrane structure can precisely identify and target the lesion site, effectively evade immune clearance, and prolong the duration of drug action;32,33 At the same time, it can actively interact with the wound microenvironment through the receptor proteins retained on the membrane surface, achieving multiple functions such as inflammation regulation, targeted bacterial clearance, and promotion of angiogenesis.34 By coating the core of synthetic nanoparticles with natural cell membranes, the resulting CNNPs exhibit a range of surface markers that enable them to replicate natural cellular interactions and be used in various biomedical applications.35 This bionic strategy endows CNNPs with numerous universal advantages, including excellent biocompatibility, long-cycle characteristics, immune escape ability, and active targeted delivery capability, enabling them to perform exceptionally well in complex physiological environments.28–31 The core breakthrough of this bionic strategy lies in successfully bridging the gap between the physicochemical advantages of synthetic nanoparticles and the functional complexity of biological systems, providing an innovative approach to addressing the aforementioned scientific gaps. CNNPs have certain advantages. For instance, the cell membrane endows nanoparticles with natural physicochemical properties and biological characteristics, which prevent them from being cleared by the immune system and extend their half-life, and also enhance the safety of nanoparticles in animals. In addition, through cell membrane modification, the functions of nanoparticles can be made more effective, specific and targeted.32,33 Various cell types have been used as sources for the membranes to coat nanoparticles, and each type can utilize its unique properties to provide functions for the nanoparticle core, with the materials being adaptable according to the required applications.30
In this review, we mainly discuss the construction and properties of different types of cell membrane-coated nanoparticles, with a focus on explaining how CNNPs improve wound healing by bridging the functional gap between synthetic materials and biological systems, analyzing their potential mechanisms of action in treatment, and exploring the opportunities and challenges that will be faced in the future.
Pathophysiology of Chronic Wound Healing
Skin is an important organ that covers the surface of the human body and directly interacts with the external environment, serving functions such as immunity, sensation, and protection.36,37 When factors such as trauma, burns, and physiological/medical conditions cause damage or disruption to the skin’s structure and function, the anatomical integrity of the skin is compromised, leading to the loss of its physiological functions.38,39 After injury, the damaged skin initiates a complex repair process involving interactions between various cell types, cytokines, and biological mediators. Typically, this repair process progresses through several stages: clot formation, inflammation, new tissue formation (including re-epithelialization and granulation tissue formation), and finally, tissue remodeling and contraction40 (Figure 1). Following tissue injury, both endogenous and exogenous coagulation pathways are rapidly activated within the body to form a clot that temporarily seals the wound gap. At the same time, local vascular smooth muscle contraction limits blood flow to reduce blood loss.41,42 The hemostatic fibrin clot, composed of platelets and coagulation cascade factors, not only prevents hemorrhage but also forms a temporary scaffold for cell adhesion and migration.43–45 Subsequently, platelets are activated by thrombin and release various growth factors. These growth factors act as biological signals, recruiting neutrophils, monocytes, leukocytes, and macrophages to the wound site, mediating the inflammatory response, protecting the skin from infection, and secreting more growth factors to accelerate wound healing.46–48 The wound then enters the proliferative phase, characterized by cellular proliferation and migration.48 In the wound area, pro-angiogenic factors released by platelets and inflammatory cells promote the gradual formation of new blood vessels and capillaries.49 Among them, hypoxia-inducible factor-1 α (HIF-1α), as a key regulatory factor for cells to respond to hypoxic environments, promotes the transcription of pro-angiogenic factors such as vascular endothelial growth factor (VEGF) during normal healing and is crucial for the formation of new blood vessels.50,51 Meanwhile, fibroblasts continue to migrate and form granulation tissue.52,53 The transforming growth factor -β (TGF-β) signaling pathway plays a core role in this process, regulating the differentiation of fibroblasts into myofibroblasts and extracellular matrix synthesis.54,55 As fibroblasts accumulate and proliferate, extracellular matrix (ECM) components such as collagen, proteoglycans, and elastin are continuously produced. Additionally, some fibroblasts differentiate into myofibroblasts, which help close the wound through their contractile function.54 Subsequently, activated keratinocytes at the wound margins migrate into the injured area, completing the re-epithelialization process.56 Finally, in the remodeling phase, type III collagen in granulation tissue gradually transitions to type I collagen, while collagen fibers rearrange, cross-link, and align, thereby strengthening and contracting the ECM, ultimately forming a mature scar. This process is characterized by structural remodeling and cellular attrition.57,58
 |
Figure 1 Phases of wound healing (a) Schematic of a skin wound as it closes to illustrate the various phases and contributing cell players. (b) Immediately upon tissue damage, a clot forms to temporarily plug the wound gap. (c) Soon after this, the wound inflammatory response kicks in, with innate immune cells, neutrophils and macrophages drawn from local resident populations and through recruitment by extravasation from nearby vessels before migrating into the wound. (d) These inflammatory cells, particularly macrophages, orchestrate the formation of granulation tissue to replace the missing connective tissue, which entails wound angiogenesis, fibroblast migration and deposition of a new collagen matrix. (e) As the granulation tissue is being laid down, resurfacing is driven by re-epithelialization, which involves both epidermal migration and cell division to restore barrier integrity. (f) Finally, these episodes cease as the wound edges confront one another and the wound has healed; however, the various cells and tissues have not resolved and remodelled, which they now do to varying degrees, generally leaving a wound scar. Abbreviations: DAMPs, damage-associated molecular patterns; ECM, extracellular matrix; PAMPs, pathogen-associated molecular patterns; VEGF, vascular endothelial growth factor.40 |
Wound repair is a highly organized and complex pathological process. However, when the wound fails to progress through this organized process, healing is delayed, ultimately leading to chronic wounds.59,60 Despite differences in etiology, chronic wounds share certain common features, including prolonged inflammatory exudation, persistent infection, bacterial biofilm formation, and elevated levels of proteases and reactive oxygen species (ROS)4,61 (Figure 2). These factors contribute to tissue necrosis, epithelial regeneration defects, and reduced angiogenesis, ultimately resulting in delayed or non-healing wounds62,63 The inflammatory response is crucial for wound healing. In chronic wounds, the nuclear factor -κB (NF-κB) signaling pathway is continuously activated, leading to the overexpression of pro-inflammatory cytokines (such as TNF-α, IL-1β and IL-6), which further recruit and activate neutrophils and macrophages, forming a vicious cycle and hindering the transition of the wound from the inflammatory stage to the proliferating stage.64–66 However, when systemic defects (such as hyperglycemia in diabetes) and local insults (such as infection and hypoxia) are present, the inflammatory phase is prolonged, leading to delayed wound healing.67,68 In such cases, there is extensive infiltration of neutrophils and macrophages, and the wound microenvironment is characterized by an increase in pro-inflammatory cytokines and unchecked protease activity.64,65 For example, studies have shown that diabetic wounds are closely associated with heightened pro-inflammatory features caused by the overexpression of inflammatory cytokines (such as TNF-α).66 Additionally, large amounts of ROS are released into the wound environment, placing chronic wounds in a highly pro-oxidative state, which damages cell membranes and the extracellular matrix.69 Due to the imbalance in the inflammatory response, the proliferation and function of endothelial cells and fibroblasts are severely inhibited.70 Moreover, the imbalance between pro-angiogenic and anti-angiogenic mediators leads to impaired angiogenesis in chronic wounds. For instance, hypoxia-inducible factor 1-alpha (HIF-1α) is considered a key angiogenic mediator, and its expression is reduced due to metabolic disturbances (such as hyperglycemia).50 The decreased expression of HIF-1α significantly inhibits the transcription of pro-angiogenic factors such as VEGF and impairs neovascularization.51 Furthermore, due to limited HIF-1α levels and fibroblast dysfunction, the expression levels and activities of pro-angiogenic growth factors, such as platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF), are significantly suppressed. The result is poor angiogenesis, leading to insufficient nutrient supply, further delaying tissue remodeling and wound healing.51
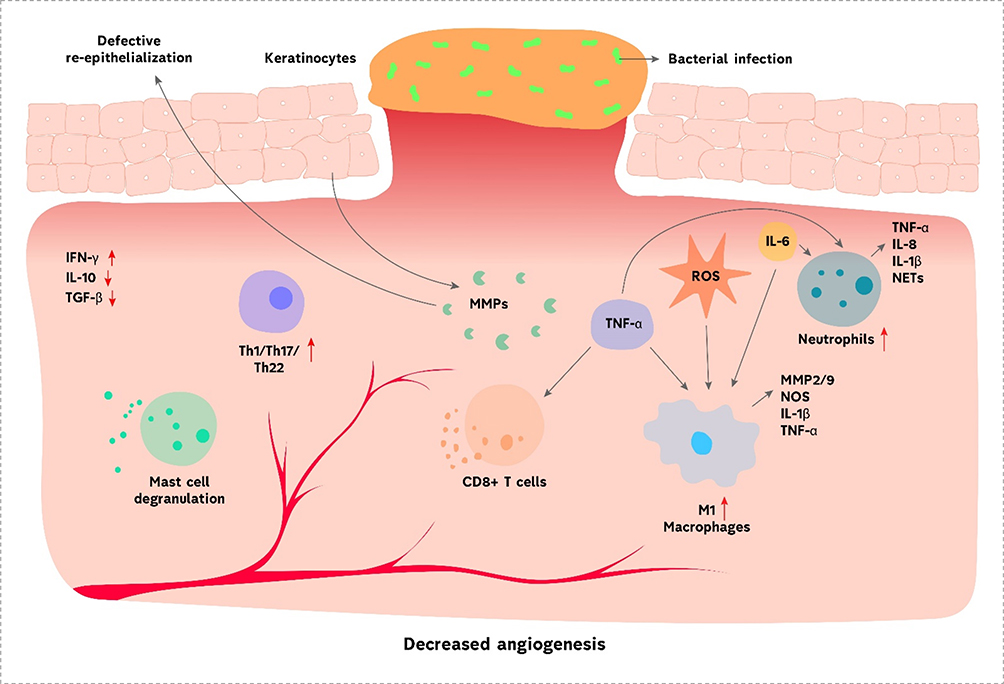 |
Figure 2 Immune system in chronic wound healing. Common features of chronic wounds are recurrent bacterial infections, decreased angiogenesis, impaired tissue epithelialization and overabundance of ROS. The prolonged presence of neutrophils and M1 macrophages leads to a highly inflammatory profile in the wound. The process is enhanced by mast cells and CD8+ T cells’ activity. The level of other inflammatory T cell subtypes, such as Th1, Th17 and Th22, is also increased. Various MMPs, secreted by keratinocytes, contribute to defective re-epithelialization. Together, all those pathological processes promote inflammation, tissue fibrosis and poor vascularization.61 Upward arrows indicate upregulation, while downward arrows indicate downregulation. |
In the wound microenvironment, infection, tissue hypoxia, local ischemia, and excessive protease activity collectively contribute to keratinocyte dysfunction. Dysfunctional keratinocytes exhibit excessive proliferation at the edges of chronic wounds but fail to migrate and close the wound, resulting in incomplete or excessive keratinization.71 Additionally, dermal and/or epidermal cells in chronic wounds fail to respond to repair stimuli. These cells exhibit abnormal phenotypes, such as lower expression of growth factor (GF) receptors and reduced mitotic potential, preventing them from responding to external environmental signals.72 Moreover, various pro-epithelialization factors, such as vitronectin and tenascin-C, are inactivated and degraded by proteolytic cleavage.38 ECM remodeling is the final stage of wound healing. During ECM remodeling, collagen undergoes repeated synthesis and degradation to replace the matrix rich in fibronectin with a stronger collagenous matrix. During this process, various cytokines and enzymes play key roles, such as transforming growth factor-β1, transglutaminase, and lysyl oxidase. However, in chronic wounds, these cytokines and enzymes are inhibited and degraded by overactive proteases.55 In particular, impaired function of the TGF-β signaling pathway will directly affect the differentiation of myofibroblasts and collagen deposition, leading to tissue remodeling disorders.54,55 Additionally, enzymes from the matrix metalloproteinase (MMP) family control the conversion of type III collagen to type I collagen. Dysfunction of these enzymes also leads to ECM remodeling failure and delayed wound healing.73
Preparation and Classification of Cell Membrane-Coated Nanoparticles
Preparation of Cell Membrane-Coated Nanoparticles (CMNPs)
The preparation of Cell Membrane-Coated Nanoparticles (CMNPs) involves three major steps: extraction of the cell membrane, preparation of the nanoparticle core, and coating the core with the cell membrane. Each step is crucial in the design of CMNPs and plays an important role in ensuring the efficacy and functionality of the final product74 (Figure 3).
 |
Figure 3 The fabrication of CMCNNPs. (A) Acquisition of cell membrane vesicles from cell culture. (B) Manufacture techniques of NPs. (C) Fusion techniques of vesicles and NPs. 74 The original figure contained a spelling error “drived”, corrected here as “derived”. Abbreviations: AFM, atomic force microscopy; DLS, dynamic light scattering; LC-MS, liquid chromatography–mass spectrometry; TEM, transmission electron microscopy; XRD, x-ray diffraction. |
Cell Membrane Extraction
The extraction of the cell membrane involves isolating and purifying the membrane, which consists of phospholipids embedded with specific surface proteins.75 These membranes play a central role in various biological functions, such as material transport and signal recognition.28 The extraction process needs to be carried out under mild conditions to preserve the purity and integrity of the membrane. This ensures that the cell membrane can replicate its functional properties on the surface of the nanoparticle core and minimize adverse effects.76,77 Common membrane separation methods include hypotonic lysis, freeze-thaw cycles, sonication, and homogenization,78–81 while purification methods include differential centrifugation, density gradient centrifugation, and ultrafiltration.82–84 In practice, the extraction method is selected based on the type of cells used. For nucleated cells, such as leukocytes, cancer cells, and stem cells, the process is more complex. First, the target cells need to be isolated from tissue or blood, followed by cell culture.85–88 Afterward, the cell membranes are extracted using methods like hypotonic lysis, mechanical disruption, and discontinuous sucrose gradient centrifugation to remove the cell nucleus and cytoplasm. The membranes are then cleaned with plasma buffer and further purified by ultrasonication and extrusion through a porous polycarbonate membrane.89 For non-nucleated cells, such as mature red blood cells and platelets, the extraction process is relatively simple. Cells are separated from whole blood, then subjected to hypotonic lysis or repeated freeze-thaw cycles to mechanically disrupt the membrane. Differential centrifugation removes soluble proteins, and the membrane is then extruded into nanoparticles.79,90
Nanoparticle Core
The nanoparticle core serves as an effective carrier for delivering cargo to the target tissue. Different types of cores confer different properties and functions to the CMNPs. The core can be either organic or inorganic, each offering distinct advantages. Organic cores are generally safer, with better loading capacity and biocompatibility, while inorganic cores have unique functionalities in areas like photodynamic therapy, fluorescence imaging, and magnetic resonance imaging (MRI).76,77,91 Organic cores have better biocompatibility and biodegradability.92,93 For example, the FDA has approved materials like gelatin, liposomes, and poly(lactic-co-glycolic acid) (PLGA) for clinical applications. Among these, PLGA is the most commonly used material for fabricating membrane-biomimetic carriers and has significant clinical application potential. Membranes can be modified on PLGA particles to prevent aggregation and achieve better delivery efficiency.76,77,94 A widely used inorganic core is the liposome, which is similar to the cell membrane.95,96 Liposomes are biodegradable colloids capable of carrying both hydrophobic and hydrophilic drugs.97,98 Moreover, they are flexible, which allows them to penetrate in vivo barriers.97 Cell membrane coating enhances the stability of the phospholipid membrane, providing longer circulation times without compromising the drug-loading capacity.99 Compared to organic cores, inorganic cores have superior stability and resistance to enzymatic degradation. They are also cost-effective, easy to synthesize, and can be coated with appropriate membrane vesicles. Furthermore, by manipulating the form, size, composition, and surface properties of inorganic nanoparticles, their inherent electrical, optical, and magnetic properties can be enhanced to fully utilize their therapeutic potential.76,77,100 Therefore, the selection of the core material should be based on the specific delivery needs of the cargo.
Fusion of Core and Cell Membrane
Once the nanoparticle core and cell membrane are prepared, the next crucial step is the fusion of the two components. This process is typically achieved using methods like membrane extrusion, sonication, or microfluidic electroporation.101–103
Membrane Extrusion
This is the most commonly used method, also known as the “top-down” approach. It involves subjecting the cells to hypertonic treatment or repeated freeze-thaw cycles to obtain empty membranes devoid of cellular contents. The extracted membranes are then extruded through a porous filter together with other nanostructures to form core-shell structures of cell membrane-derived nanoparticles.104 Although this method is fast and simple, large-scale production can be challenging.
Sonication
This method uses ultrasound treatment to mix the purified cell membranes with the nanoparticle core, resulting in the cell membrane coating the surface of the nanoparticle core. The application of ultrasonic energy disrupts both components, promoting the spontaneous formation of the core-shell nanostructures. This method not only yields results similar to membrane extrusion but also reduces material loss.105,106
Electroporation
This method utilizes microfluidic devices to apply electrical pulses, facilitating the entry of the nanoparticle core into the cell membrane. This allows the fusion of the core and the cell membrane to form the desired CMNPs.30,106
Classification of Cell Membrane-Coated Nanoparticles (CNNPs)
The plasma membrane is embedded with various biomolecules, playing a vital role in processes such as recognition and signal transduction. Therefore, theoretically, directly transferring the intact cell membrane onto nanoparticles (NPs) can impart the physiological functions of the membrane, including its significant ability to interface with and interact with the surrounding environment.28,76,77 Currently, numerous types of cell membranes or hybrid membranes have been explored for constructing biomimetic CNNPs, with each type of membrane coating imparting specific characteristics31 (Figure 4A).
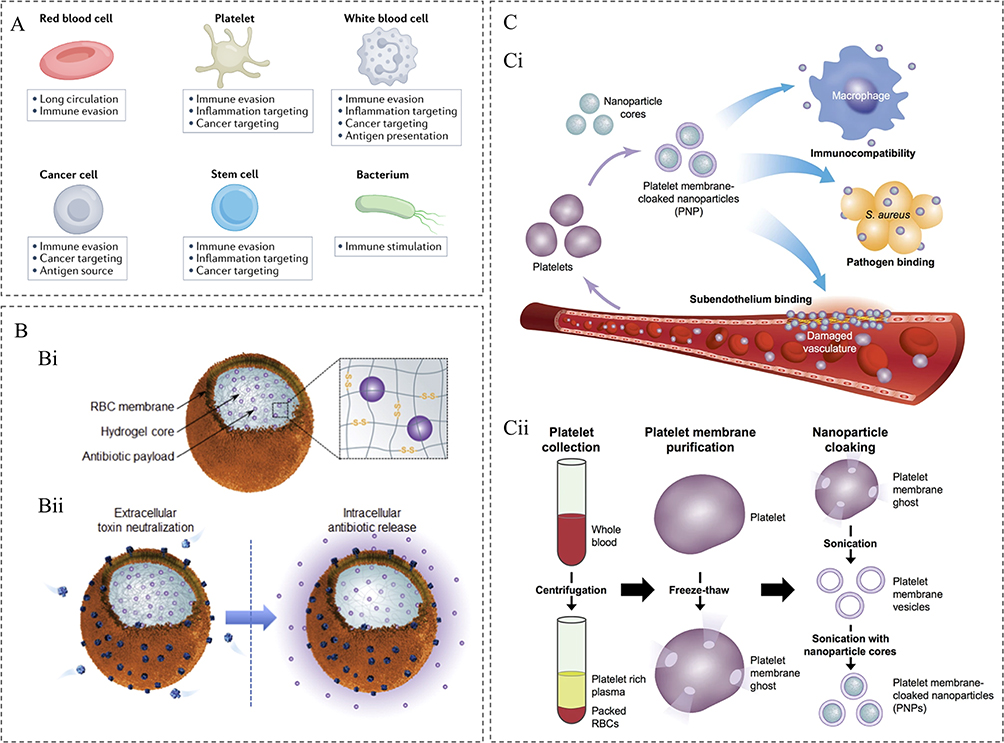 |
Figure 4 (A) Common membrane sources for the fabrication of cell membrane-coated nanoparticles. Cell membrane-coated nanoparticles can be fabricated using cell membrane materials sourced from red blood cells, platelets, immune cells, cancer cells, stem cells or bacteria. Each type of membrane coating confers specific properties that can be leveraged for anticancer applications.31 (B) Schematic illustrations of a red blood cell (RBC) membrane-coated nanogel (RBC-nanogel) system for combinatorial extracellular toxin neutralization and intracellular redox-responsive antibiotic release. (Bi) The RBC-nanogel is constructed with a natural RBC membrane shell and a hydrogel core containing antibiotic payload. The hydrogel core is cross-linked with disulfide bonds, cleavable in reducing environment. (Bii) In extracellular environment, the RBC-nanogel absorbs and neutralizes pore-forming toxins (PFTs) secreted by bacteria. Such toxin sequestration facilitates the intracellular uptake of the toxin-secreting bacteria and the RBC-nanogel. Once inside the cell, the RBC-nanogel rapidly releases its encapsulated antibiotic payload triggered by a redox reaction.107 (Ci) Poly(lactic-co-glycolic acid) (PLGA) nanoparticles are enclosed entirely in plasma membrane derived from human platelets. The resulting particles possess platelet-mimicking properties for immunocompatibility, subendothelium binding, and pathogen adhesion. (Cii) Schematic depicting the process of preparing PNPs.108 |
Red blood cells (RBCs) are responsible for transporting oxygen and nutrients and have a lifespan of about 120 days in circulation. When RBC membranes are used to coat NPs, the resulting particles exhibit surface antigens consistent with the “self” identity, allowing these particles to circulate for longer periods without being recognized and eliminated by macrophages in the body.109,110 RBCs possess good biocompatibility and low immunogenicity, making them an ideal material for preparing long-circulating NPs. For instance, Zhang et al constructed an RBC-nanogel system for combined virulence inhibition and reactive antibiotic delivery to treat methicillin-resistant Staphylococcus aureus (MRSA) infections107 (Figure 4B). Platelets, which are non-nucleated cell fragments, are involved in many pathophysiological processes, including atherosclerosis, tumor progression, and inflammation. Similar to RBC membranes, platelet membranes also contain various “self” markers. CD47 helps platelets evade phagocytosis by macrophages, while CD55 and CD59 prevent complement system activation; therefore, platelet membranes are also suitable for CNNPs.111 Zhang et al first demonstrated the preparation of platelet membrane-coated nanoparticles (PNPs). Compared with uncoated NPs, PNPs reduced macrophage-like cell uptake, did not trigger complement activation in human plasma, and exhibited platelet-mimicking characteristics108 (Figure 4C).
Inflammatory cells can adhere to and traverse endothelial cells, specifically migrating to sites of inflammation. Leveraging this property, researchers have designed carrier systems derived from inflammatory cells for precise delivery of anti-inflammatory drugs.112 These NPs, coated with inflammatory cell membranes, effectively retain various biomarkers such as CD45, CD3Z, lymphocyte function-associated antigen-1 (LFA-1), and various adhesion molecules. These “leukocyte-like” markers not only help avoid rapid clearance by the mononuclear phagocyte system but also promote NP traversal through endothelial cells, allowing accumulation at inflammation sites.112 Among these, neutrophil membrane-coated nanoparticles are particularly unique as they not only precisely target inflammation sites but also target circulating tumor cells (CTCs), effectively preventing early tumor metastasis and potentially inhibiting the further development of established metastatic lesions.85 In recent years, tumor cell membrane-coated functionalized nanoparticles have been increasingly developed.88,92 Compared to other cell types, tumor cell-derived NPs can not only passively leak from capillaries due to the enhanced permeability and retention effect but also actively bind to tumor cells through homotypic recognition.113 Studies have shown that the targeting efficiency of tumor cell membrane-coated NPs is 20 times and 40 times greater than that of RBC membrane-coated NPs and bare NPs, respectively.113 Additionally, mesenchymal stem cells (MSCs) have been used in the construction of CNNPs. Stem cells possess self-renewal and multi-directional differentiation potential, along with low immunogenicity and ease of acquisition. These cells exhibit specific tumor-homing ability through interactions between chemokine receptors and endothelial adhesion molecules, making MSC membrane-coated NPs specifically target tumor lesions, thus reducing the systemic toxicity and side effects of chemotherapy drugs.114 In addition to these, many other types of cell membranes have been applied to CNP construction, such as bacterial cell membranes,115 fibroblast membranes,116 and pancreatic β-cell membranes.117
In addition to single cell membranes, recent years have seen researchers combine multiple cell membranes to develop hybrid membranes with enhanced functionality, expanding their application potential.76,118 For example, hybrid NPs coated with both RBC and platelet membranes can circulate for extended periods, making them an ideal choice for in vivo studies.94 Mixed RBC/platelet membrane-coated polypyrrole NPs (PPyNP) can effectively kill tumor cells upon near-infrared laser irradiation and possess self-targeting and prolonged in vivo circulation, showing broad application prospects.119 Recently, Liu et al used a hybrid membrane of platelet membranes and CCR2-high-expressing cell membranes to coat nanoparticles and loaded them with rapamycin and TPPU, two small molecule drugs, to target pathological regions associated with Alzheimer’s disease (AD). These nanoparticles can cross the blood-brain barrier and release drugs at the inflammation sites to enhance autophagy and alleviate neuroinflammation, thereby achieving AD treatment.20 In summary, by integrating the characteristics of different cell types, hybrid membranes can be created, resulting in NPs with longer in vivo circulation half-lives and stronger targeting capabilities, providing new ideas for drug delivery.
Whether single-cell membranes or hybrid cell membrane-coated nanoparticles, the functionality of CNNPs primarily depends on their surface functional proteins. With advancements in material science and medicine, the targeting and monitoring capabilities of cell membrane-based nanoplatforms are continuously improving. To enhance the properties of membrane-coated CNNPs and achieve more precise targeting for research and treatment, cell membrane modification has become a highly promising new research direction.120,121 Cell membrane modification can primarily be divided into physical, chemical, and bioengineering types. Physical methods anchor targeting groups on the cell membrane through lipid structure and membrane fluidity. Chemical methods utilize activated chemical bonding sites for covalent attachment. Bioengineering methods involve transfecting or transducing the required proteins or peptides into the cell membrane. These three methods provide diverse possibilities for cell membrane modification.120 These designs demonstrate the diverse characteristics of cell membrane-coated nanoparticles, as well as the flexible and controllable loading capacities of the nanoparticle core. This makes cell membrane-coated nanoparticles a promising platform for chronic wound healing treatment and highlights their vast potential in targeted drug delivery and immune modulation.
Various Strategies of Cell Membrane-Coated Nanoparticles in Chronic Wound Treatment
The application of cell membrane-coated nanoparticles (CNNPs) in chronic wound treatment represents a cutting-edge therapeutic strategy, combining the advantages of nanotechnology and biomaterials to offer a novel and effective treatment approach. Chronic wounds are typically difficult to heal due to factors such as infection, inflammation, and poor blood circulation. Cell membrane-coated nanoparticles can accelerate the healing process of chronic wounds and enhance treatment efficacy through several strategies (Table 1).
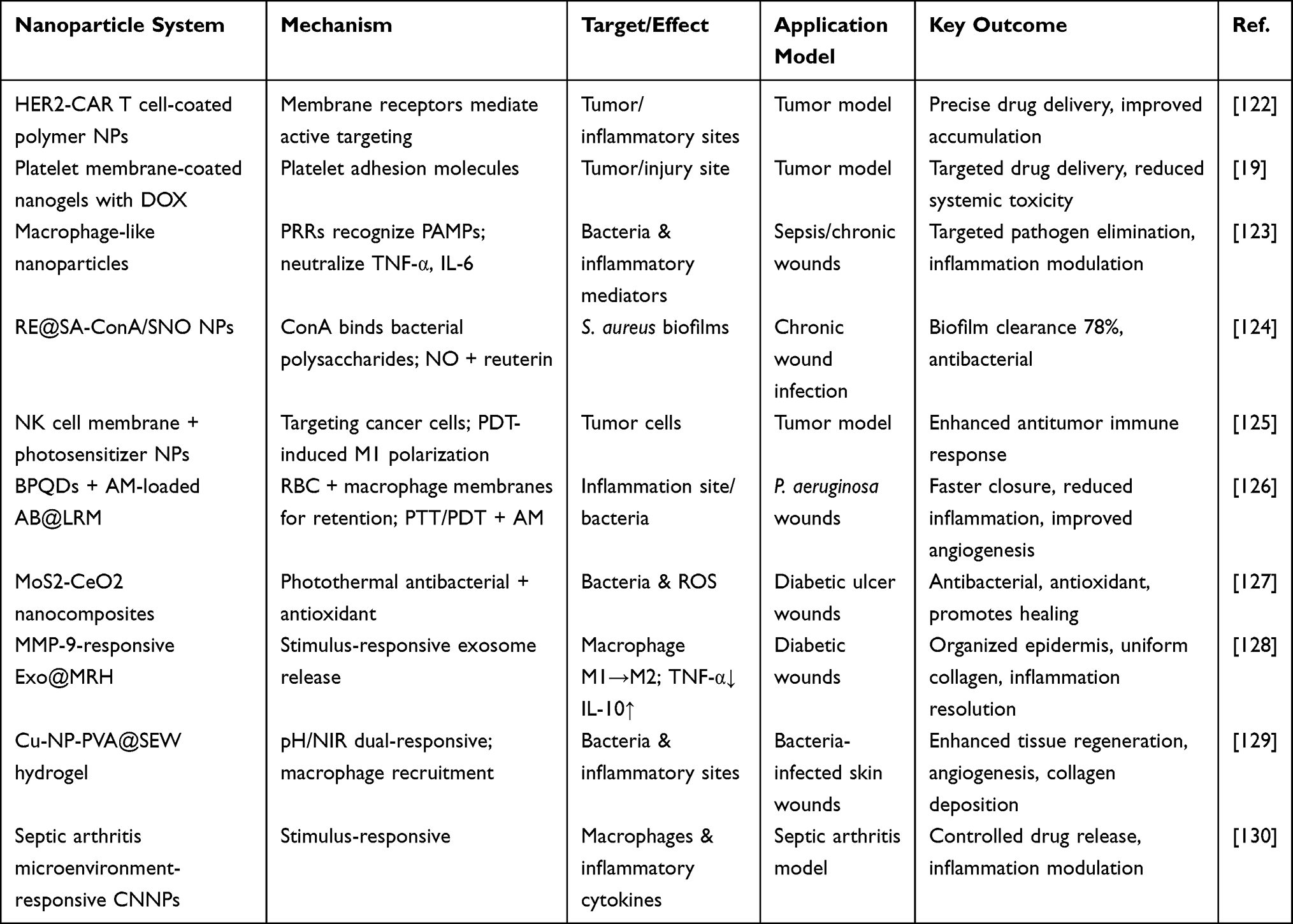 |
Table 1 Strategies and Representative Cases of Cell Membrane-Coated Nanoparticles (CNNPs) in Chronic Wound Treatment |
Targeted Drug Delivery for Therapeutic Treatment
CNNPs leverage the characteristics of cell membranes to enhance biocompatibility, extend circulation time, and potentially confer targeting capabilities. In drug delivery, nanoparticles can protect drugs from degradation, increase accumulation at the site of injury, and reduce systemic side effects. For example, HER2-based chimeric antigen receptor (CAR) engineered T cell-coated polymer nanoparticles,122 and platelet membrane-coated nanogels loaded with doxorubicin,19 utilize specific receptors or adhesion molecules on the cell membrane, enabling active targeting and tumor accumulation, thus achieving precise drug delivery. The microenvironment of chronic wounds is characterized by persistent inflammation, and cell membrane-coated nanoparticles can target inflammatory or infected areas to enhance local drug accumulation. For instance, macrophage-like nanoparticles possess the same antigenic exterior as macrophages, thereby inheriting their ability to bind to endotoxins and pro-inflammatory cytokines. Specifically, pattern recognition receptors (PRRs) on the macrophage cell membrane, such as Toll-like receptors (TLRs), can recognize pathogen-associated molecular patterns (PAMPs). Thereby mediating the targeting and elimination of pathogens such as bacteria; Meanwhile, these membrane structures can bind to and neutralize inflammatory mediators, such as tumor necrosis factor -α (TNF-α) and interleukin-6 (IL-6). It provides a brand-new perspective for the treatment of sepsis.123
In rheumatoid arthritis (RA), the fibroblast-like synoviocytes (FLS) “regulatory” phenotype (FLSreg) is defective, while FLS in RA instead act as a “pro-inflammatory” phenotype, mediating prolonged inflammation. Liu et al encapsulated IFN-γ and rapamycin-induced FLSreg cell membranes on nanoparticles, demonstrating significant therapeutic effects, stability, and inflammation-targeting capabilities in an RA model].131 In chronic wound treatment, nanoparticles loaded with drugs for targeted delivery have shown positive effects. For example, Jin et al developed a microneedle patch with nanoparticles (RE@SA-Con A/SNO NP) (Figure 5A), where the nanoparticles are composed of sodium alginate (SA) encapsulating an antibacterial agent (reuterin) and immobilized Concanavalin A (Con A) along with NO molecules. These nanoparticles specifically recognize bacterial polysaccharides on the surface to achieve targeted antibacterial effects (Figure 5B).124 The results showed that RE@SA-Con A/SNO NPs effectively targeted and bound to the surface of Staphylococcus aureus. In contrast, when Con A protein was replaced with bovine serum albumin (BSA), the nanoparticles lost their ability to target harmful bacteria (Figure 5C). These findings confirm the targeted ability of RE@SA-Con A/SNO NPs, as Con A interacts with mannose and glucose residues on the bacterial surface. In vitro experiments indicated that RE@SA-Con A/SNO NPs exhibited excellent bacterial clearance, consistent with the antibacterial results, and showed the best biofilm clearance effect against Staphylococcus aureus (Figure 5D and E). Due to the synergistic antibacterial effect of reuterin and NO molecules, the biofilm clearance rate reached 78.13±1.48%. Therefore, combining the natural targeting ability of cell membranes with the efficient drug delivery capability of nanoparticles may enhance the delivery efficiency and targeting of nanoparticles, paving the way for the development of targeted drug delivery nanoplatforms for chronic wound microenvironments.
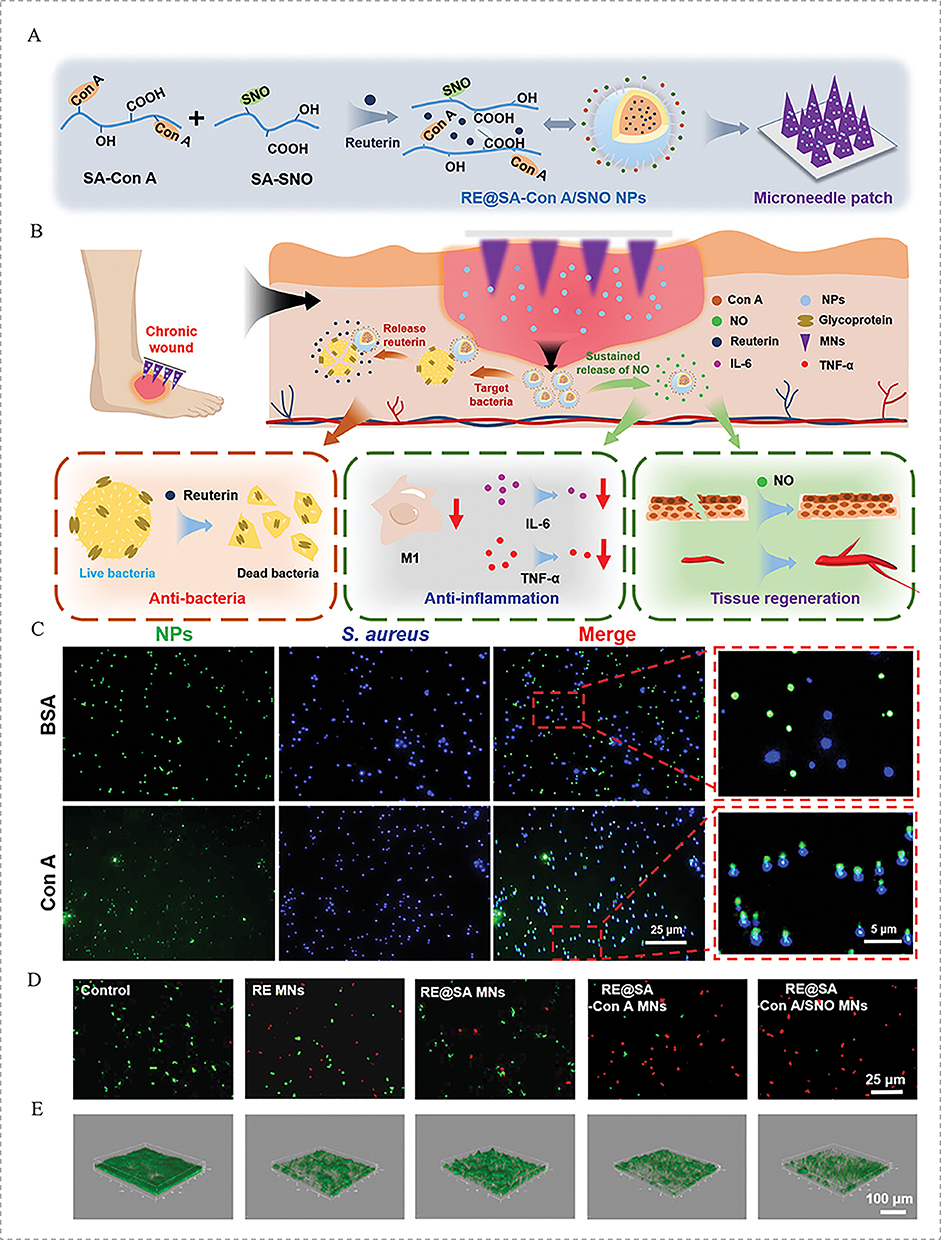 |
Figure 5 (A) Schematic illustration of the synthesis of RE@SA-Con A/SNO NPs and subsequent encapsulation in a MN patch. (B) Schematic illustration of the application of a MN patch loaded with RE@SA-Con A/SNO NPs for targeted and synergistic therapy of chronic wounds. (C) Representative fluorescence-field microscopy images of RE@SA-Con A/SNO-FITC NPs targeting bacteria. (D) Live/dead assay of S. aureus after incubation with different MNs for 24 h. (E) Confocal laser scanning microscopy of S. aureus with different treatments. Green: live bacteria.124 Red downward arrows indicate downregulated expression. |
Phototherapy Combined Treatment
Phototherapy combined treatment is a strategy that integrates phototherapy with other therapeutic approaches to enhance treatment efficacy. In the field of tumor treatment, immunotherapy combined with phototherapy is often used to strengthen the effects of tumor immunotherapy. Currently, the combination of cell membrane-coated nanoparticles (CNNPs) with phototherapy has synergistically enhanced tumor immunotherapy. For instance, using natural killer (NK) cell membranes combined with photosensitizer-loaded nanoparticles has endowed the nanoparticles with the ability to specifically target cancer cells. While undergoing photodynamic therapy (PDT), this combination induces M1 macrophage polarization, producing an antitumor immune response, thus enhancing the antitumor immune efficacy of NK cell membrane-coated nanoparticles.125 A key question arises: can CNNPs and phototherapy be applied together for the treatment of refractory wounds? This issue is worth attention, as numerous preclinical studies have combined phototherapy with nanotechnology to develop photothermal-sensitive nanoparticle platforms, which could help improve bacterial clearance in refractory wounds.
Photothermal therapy (PTT) primarily relies on photosensitizers generating heat under near-infrared (NIR) light irradiation to damage bacterial membrane structures and cause irreversible damage to bacterial proteins, thereby killing the bacteria. However, while PTT provides heat to tissues, the local high temperatures can lead to excessive reactive oxygen species (ROS) production in the body, causing oxidative stress damage to the skin tissue and severely hindering normal wound healing. To address this, researchers have developed bio-nanomaterials with excellent photothermal conversion properties, which help promote wound healing and resist oxidative stress, thereby protecting healing tissues from damage caused by oxidation.132 For example, molybdenum disulfide-cerium oxide (MoS2-CeO2) nanocomposites not only possess photothermal antibacterial properties through polyethylene glycol (PEG)-modified MoS2 nanosheets but also have antioxidant activity through cerium oxide nanoparticles (CeO2 NPs). These materials can eliminate excessive ROS around diabetic ulcer wounds and, through the inherent antibacterial activity of CeO2 nanoparticles, MoS2-CeO2 nanocomposites exhibit excellent PTT antibacterial properties under 808 nm laser irradiation, demonstrating reduced wound infection risks for both Gram-positive and Gram-negative bacteria.127
Recently, Xiong et al introduced a macrophage membrane-coated cascade-targeting photothermal nanosystem that can accurately target and eradicate intracellular bacterial infections in a cascade manner.133 Liu et al used the fusion of red blood cell membranes and macrophage cell membranes to form a composite cell membrane shell, which further encapsulated drug-loaded liposomes to create a biomimetic liposome (AB@LRM). Specifically, photosensitizer black phosphorus quantum dots (BPQDs) and the classic antibiotic amikacin (AM) were loaded into AB@LRM (Figure 6A). Through the guidance of the macrophage membrane and the long-term retention ability of the red blood cell membrane, the system can accurately target inflammation sites, ultimately exhibiting effective antibacterial activity (Figure 6B). This biomimetic liposome is applied for precise antibacterial treatment, effectively treating Pseudomonas aeruginosa infections in both pneumonia (Figure 6C) and wounds (Figure 6D).126 Furthermore, due to the excellent photothermal and photodynamic properties of BPQDs, when exposed to NIR laser irradiation, BPQDs act as effective antibacterial agents, significantly increasing bacterial sensitivity to antibiotics. In infection wound models, wounds treated with AB@LRM (+) for 11 days showed significantly faster healing effects (Figure 6E and F). H&E staining images revealed that the infection areas treated with AB@LRM (+) exhibited a marked reduction in inflammatory cells and complete epithelial regeneration in the wound areas, showing typical skin morphological features with hair follicles and blood vessels (Figure 6G). Additionally, immunofluorescence at the wound site in the AB@LRM (+) group showed the best vascular formation and density (Figure 6H).
 |
Figure 6 (A) The preparation process of AB@LRM NPs. (B) The synergistic therapeutic mechanisms against bacterial infections. Applications of AB@LRM (+) in the treatment of (C) bacterial pneumonia and (D) bacteria-infected wound healing caused by P. aeruginosa. (E) Representative photographs of infected wounds on days 0, 2, 5, 8, and 11. (F) Monitoring of wound closure during 11 d treatments in each group (G). H&E staining of the infected wound tissues (scale bar = 100 µm). (H) Representative immunofluorescence images of angiogenesis (CD31) (scale bar = 50 µm) and the quantifications of vessel density (n = 5).126 |
Therefore, the strategy of combining cell membrane-coated nanoparticles with phototherapy to exert antibacterial effects offers a highly feasible approach for treating refractory wounds. The synergistic effects of photothermal therapy (PTT), photodynamic therapy (PDT), and biomimetic targeting provide an innovative solution for the management of complex wounds.
Intelligent Response to the Wound Microenvironment
Recently, stimulus-responsive drug delivery nanoparticle systems (DDS) based on multifunctional nanoparticles have garnered significant attention due to their ability to release drugs on demand at specific sites in response to external or internal signals. These intelligent nanocarriers can be customized to respond to various stimuli, such as redox potential, pH changes, light, or enzyme activation, and even to multiple or dual stimuli simultaneously.23,134 Therefore, drug delivery carriers used to promote wound healing also need to respond to the specific characteristics of the wound microenvironment, such as pH changes or the presence of enzymes, by designing stimulus-responsive nanocarriers for controlled drug release.
As previously mentioned, during the inflammatory process, the inflammatory microenvironment rich in cytokines and proteases (such as matrix metalloproteinases, MMPs) plays a crucial role, as these components typically increase after wound formation and during the inflammatory response. This suggests that MMPs may serve as biomarkers of the wound inflammatory microenvironment. Based on this, Meng et al developed an MMP-9-responsive exosome delivery system (Exo@MRH).128 This system is formed by the cross-coupling of oxidized dextran, matrix metalloproteinase (MMP)-9 sensitive peptide and carboxymethyl chitosan containing M2 macrophage-derived exosomes (M2-exOS). The on-demand release of M2-exOS promotes the polarization of macrophages from the M1 phenotype to the M2 phenotype at the molecular level. M2-Exos may regulate polarization signaling pathways (such as STAT6, PPARγ, etc.) within macrophages by delivering specific mirnas or proteins, thereby affecting the expression of downstream inflammatory factors (such as TNF-α, IL-6, IL-10, etc), and thus promoting the transition from the inflammatory phase to the proliferative phase. And it accelerated the healing of diabetic wounds (Figure 7A). Histological analysis using H&E and Masson staining on day 14 showed (Figure 7B) that the Exo@MRH group had well-organized epidermis and more uniform dermal collagen deposition. Immunofluorescence staining (Figure 7C) shows that Exo@MRH effectively promotes the transformation of Mφ from M1 to M2, reduces chronic inflammation and promotes the healing of diabetic wounds.
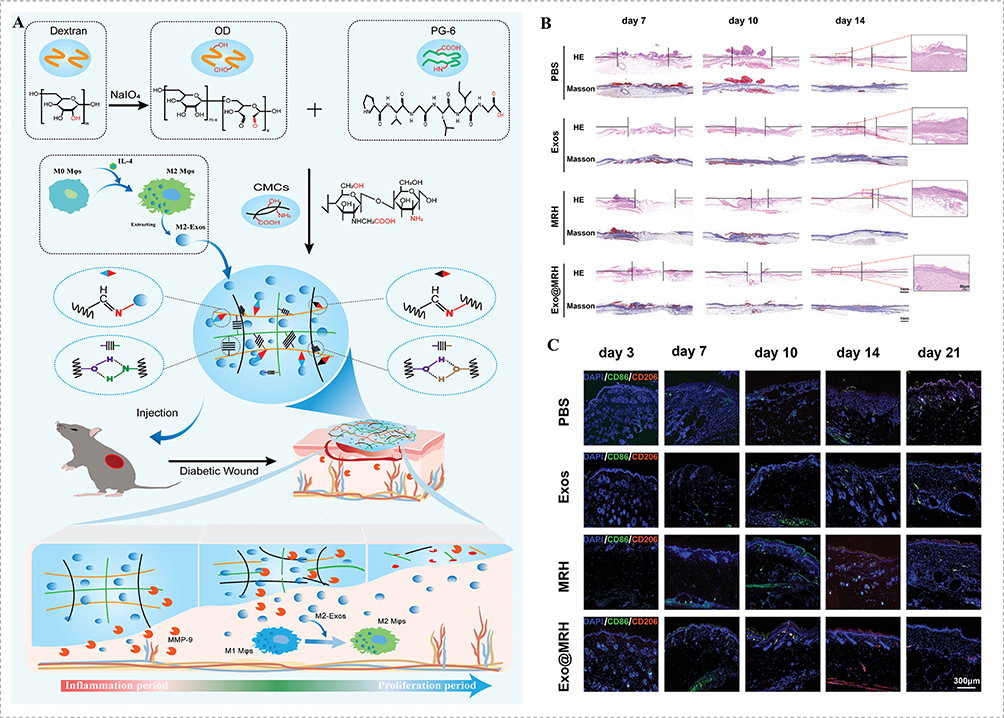 |
Figure 7 (A) Schematic diagram of Exo@MRH facilitating diabetic wound healing by guiding timely switch of M1-M2 Mφs. (B) Representative images of scar widths stained by H&E and collagen fibers stained by Masson. (C) Immunofluorescence costaining.128 |
In addition, researchers have further enhanced the efficacy of nanoparticles in chronic wound treatment by combining photothermal therapy with nanotechnology. For example, Zha et al prepared a near-infrared (NIR)/pH dual-responsive copper nanoparticle (Cu-NP)-polyvinyl alcohol (PVA) hydrogel film loaded with macrophage recruitment agent SEW2871 (SEW) for the treatment of bacterial-infected skin wounds. The results showed that humic acid (Has) promoted M2 macrophage polarization in a dose-dependent manner. Through NIR-induced local thermal therapy, Cu-HAs nanoparticles successfully eradicated bacterial infection. This PVA@Cu-HAs NPs@SEW hydrogel film improved tissue regeneration by promoting M2 macrophage polarization, alleviating oxidative stress, enhancing angiogenesis, and promoting collagen deposition.129 Currently, inflammation microenvironment-responsive CNNPs have shown progress in the treatment of septic arthritis.130 Thus, future development of cell membrane-coated nanoparticles with intelligent responsiveness to the wound microenvironment could enable the timely, on-demand, and controlled release of drugs, offering promising prospects for chronic wound management.
Cell Membrane-Coated Nanoparticles Promote Chronic Refractory Wound Healing Through Multiple Mechanisms
Chronic refractory wounds, despite having different etiologies, share common characteristics in their wound microenvironment, including persistent inflammation, bacterial infection, bacterial biofilm formation, and elevated levels of proteases and ROS. These factors are intertwined, leading to tissue necrosis, defects in epithelial regeneration, and reduced angiogenesis. As an emerging drug delivery platform, cell membrane-coated nanoparticles (CNNPs) can exert therapeutic effects through various mechanisms. Their potential therapeutic mechanisms include inhibiting infection, promoting angiogenesis, improving the local inflammatory environment, and promoting tissue regeneration. These mechanisms together make CNNPs a promising platform for tissue engineering and drug delivery (Table 2).
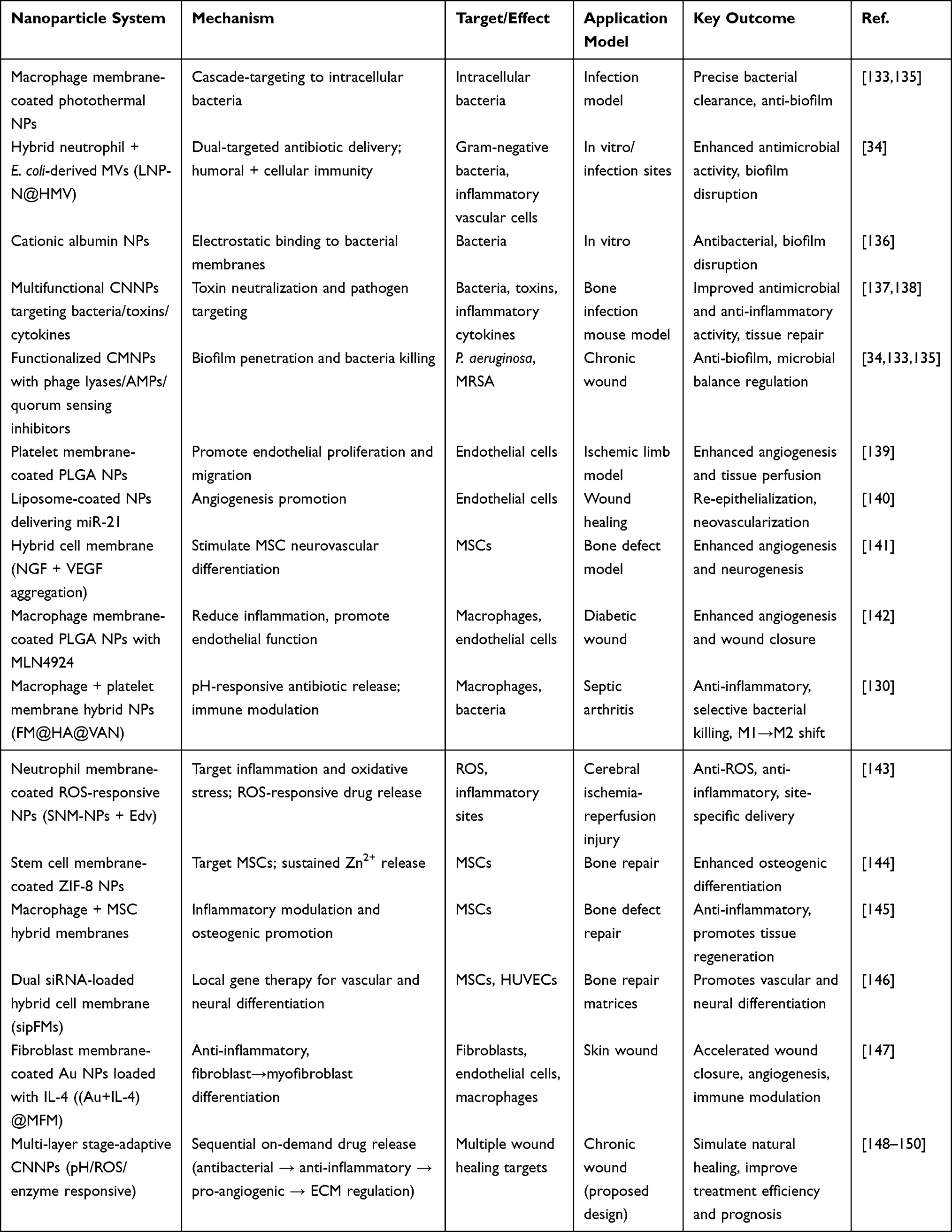 |
Table 2 Mechanisms and Representative Cases of Cell Membrane-Coated Nanoparticles (CNNPs) in Chronic Refractory Wound Healing |
Inhibition of Bacterial Infection
CNNPs have been reported to cleverly evade immune system recognition, precisely target pathogenic bacteria, neutralize harmful toxins, and deliver antibiotics to combat bacterial infections.151,152 Due to the close interaction between pathogens and cell membranes, various cell membrane-mimicking nanostructures have been used as decoys to alleviate pathogen infection, such as liposomes and cell membrane-derived nanostructures.30,100,151 Given the diversity of these cell membrane components, their functions also vary. For example, leukocyte membrane-coated biomimetic nanoparticles possess immune evasion and inflammatory chemotaxis properties. Xiong et al utilized this feature by coating photothermal nanoparticles with macrophage cell membranes to successfully create an intelligent cascading-targeting nanomaterial system. This system can precisely target and completely eliminate intracellular bacterial infections through a cascading mechanism.133,135
Additionally, bacterial membrane vesicles (MVs) have also been widely studied as potential therapeutic delivery systems for bacterial infections. The pathogen-associated molecular patterns (PAMPs) on the surface of MVs can activate the human immune system, and through a “bacteria-suppressing-bacteria” strategy, MVs can effectively inhibit the progression of bacterial infection.153 To overcome the non-specificity issue of MVs as drug carriers, Peng et al combined neutrophils with E. coli-derived MVs to prepare hybrid cell membrane vesicles targeting the inflammatory microenvironment. Antibiotic norfloxacin (Nor) was loaded into these hybrid vesicles (LNP@HMV), forming a therapeutic nanoparticle system (LNP-N@HMV) (Figure 8A). This dual-targeted system can deliver antibiotics and activate both humoral and cellular immunity, precisely targeting inflammatory vascular cells and Gram-negative bacteria, significantly enhancing accumulation at infection sites, and showing remarkable potential in preventing Gram-negative bacterial infections (Figure 8B).34 In vitro experiments showed that LNP-N@HMV exhibited good antimicrobial and biofilm-disrupting activity, with bactericidal assays demonstrating superior antimicrobial efficacy (Figure 8C). Furthermore, live/dead cell staining showed that LNP-N@HMV at a Nor concentration equivalent to 0.5 μg/mL almost completely eliminated all bacteria from the biofilm (Figure 8D). Moreover, CNNPs can achieve selective targeting through electrostatic interactions with bacterial membranes. Cationic albumin nanoparticles, for example, can bind to bacterial cell wall components, demonstrating significant antibacterial activity and biofilm disruption.136
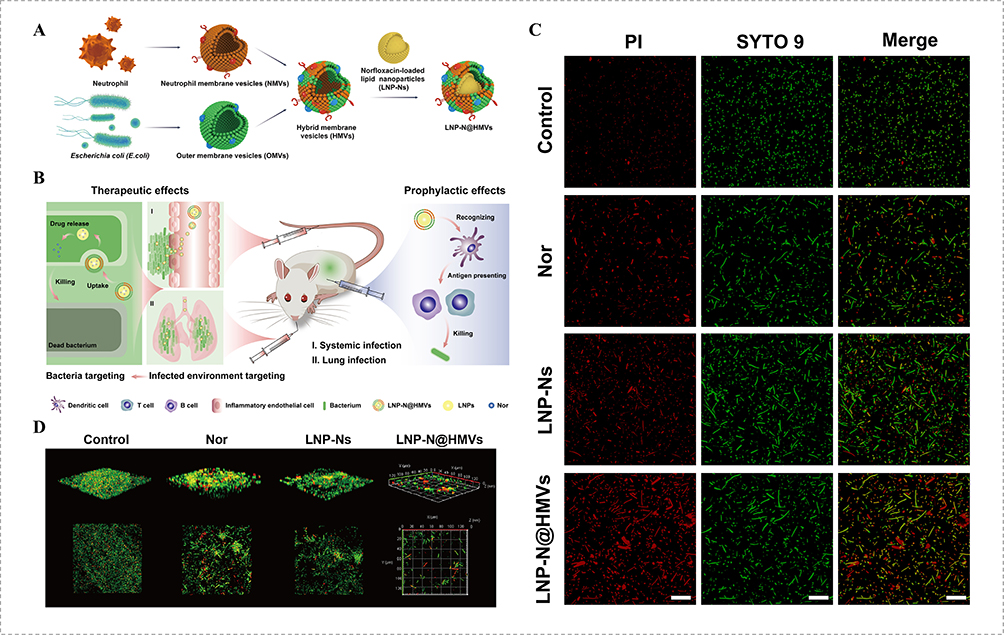 |
Figure 8 (A) Construction of hybrid cell membrane–coated antibiotic delivery system LNP-N@HMVs. (B) Application of LNP-N@HMVs in dual-targeted treatment and prophylaxis of bacterial infections. (C) Confocal microscopic images of E. coli (~108 CFU mL−1) with different treatments at the equivalent Nor concentration of 0.24 μg mL−1 and stained with Live/Dead BacLight bacterial viability kit (green, all the bacteria; red, dead bacteria). Scale bar, 20 μm. (D) Confocal microscopic images of E. coli biofilm with different treatments at the equivalent Nor concentration of 0.5 μg mL−1 for 24 hours and stained with Live/Dead BacLight bacterial viability kit.34 |
The protein toxins secreted by pathogens break through the cell membrane barrier through various complex mechanisms to exert their virulence.154 Given the destructive nature of toxins and their key role in various pathophysiological processes, targeting toxins is undoubtedly a rational strategy for treating diseases. By neutralizing toxins, the pathogenic mechanisms that directly cause many severe symptoms can be effectively alleviated.155,156 In the treatment of sepsis, multifunctional CNNPs have demonstrated strong therapeutic effects by precisely targeting pathogens, toxins, and inflammatory cytokines.137 This strategy has shown improved therapeutic outcomes in bacterial infection mouse models. In a mouse model of bone infection, CNNPs synthesized through electroporation preserved the integrity of the membrane structure and the correct functioning of protein, thus exhibiting excellent recognition and adsorption capabilities for bacteria, toxins, and inflammatory cytokines. This approach significantly enhanced antimicrobial and anti-inflammatory activity, promoting bone tissue repair.138
It is worth noting that the difficulty in healing chronic wounds is closely related to specific bacterial communities and the biofilms they form, especially the complex biofilm barriers composed of key pathogenic bacteria such as Pseudomonas aeruginosa and methicillin-resistant Staphylococcus aureus (MRSA),157,158 It is an important reason for the failure of traditional antibiotic treatment。In recent years, CMNPs have demonstrated cutting-edge advantages in anti-biofilm and regulating the ecological balance of wound microbiota. Through functionalized membrane surface modifications (such as integrating phage lyases, antimicrobial peptides or quorum sensing inhibitors), CMNPs can precisely identify and bind to the above-mentioned specific pathogenic bacteria, thereby penetrating the biofilm matrix and releasing the carried drugs to directly kill the residual bacteria inside34,133,135。In addition, some CMNPs designs interfere with the bacterial quorum sensing system, inhibit the expression of genes related to biofilm formation, and promote the disintegration of mature biofilms rather than merely killing bacteria, which helps to reduce the development of drug resistance. At the level of microbiota regulation, the precise targeting of CMNPs enables them to eliminate dominant pathogenic bacteria while minimizing disturbance to the symbiotic beneficial flora of the wound, or by delivering prebiotics, postbiotics and other components, actively reshape the microecology conducive to host healing,159 and promote the repair of chronic wounds in a coordinated manner from the perspective of restoring microbial balance.
Promotion of Angiogenesis
Angiogenesis is a crucial process in wound healing, especially in chronic wounds where insufficient angiogenesis leads to hypoxia and restricted nutrient supply, delaying tissue repair.50,51 Therefore, stimulating angiogenesis at the wound site is an important strategy for treating chronic wounds. Firstly, CNNPs can promote the proliferation and migration of endothelial cells by providing a stable microenvironment, thereby accelerating angiogenesis. For example, recent studies have found that platelet membrane-coated poly(lactic-co-glycolic acid) (PLGA) nanoparticles effectively promote endothelial cell proliferation and migration, significantly improving tissue perfusion and promoting angiogenesis in ischemic limb models.139 These innovative approaches provide new ideas and directions for the treatment of ischemic changes in refractory wounds.
Significant progress has also been made in the use of CNNPs to promote angiogenesis in wound healing. CNNPs can serve as drug delivery systems, directly delivering angiogenesis-promoting factors to the wound site. For example, liposome-coated nanoparticles can effectively deliver angiogenesis-related microRNAs (such as miR-21), promoting reepithelialization, dermal reconstruction, and neovascularization at the wound site.140 In addition to drug delivery, local enrichment of growth factors is also an innovative approach. For instance, Qiao et al designed a hybrid cell membrane with specific surface receptors that could aggregate neurotrophic growth factor (NGF) and vascular endothelial growth factor (VEGF). This approach enhanced the neurovascular differentiation of mesenchymal stem cells (MSCs), stimulated the osteogenic differentiation of MSCs via paracrine signaling related to nerves and blood vessels, and further promoted angiogenesis and neurogenesis around bone defects.141
Finally, CNNPs can promote angiogenesis by modulating the inflammatory response. Certain nanoparticles can regulate the expression of inflammatory cytokines, drive macrophage polarization towards the M2 phenotype, enhance angiogenesis, and promote tissue repair. For example, the neddylation inhibitor MLN4924 can suppress the production of pro-inflammatory cytokines, enhance endothelial cell formation, and promote angiogenesis in diabetic wound healing. Based on this, Zeng et al developed a macrophage membrane-coated PLGA nanoparticle drug delivery system (M-NPs/MLN4924) loaded with MLN4924, which protects the drug from clearance, reduces local inflammation, and promotes wound healing in diabetic mice.142 Further evaluation of the effects of M-NPs/MLN4924 on human umbilical vein endothelial cell (HUVEC) proliferation and angiogenesis revealed that it enhanced cell proliferation, migration, and angiogenesis.
Modulation of the Inflammatory Microenvironment
Inflammation is a critical stage in wound healing; however, excessive or prolonged inflammation can lead to the formation of chronic wounds. Therefore, regulating the inflammatory response to maintain immune balance is one of the key strategies for promoting wound healing.160,161 Additionally, macrophages play a central role in wound healing, as their polarization state determines the progression of inflammation and the efficiency of tissue repair.162 By mimicking the biological functions of natural cell membranes, CNNPs can effectively interact with the immune system, demonstrating great potential in the treatment of inflammation-related diseases.123,163 CNNPs can efficiently bind with various types of cytokines through the respective cytokine receptors on the cell membrane. Cytokine neutralization can inhibit the activation of downstream macrophages and prevent the propagation of immune cascades, thus alleviating inflammation.130
In the treatment of septic arthritis, Yu et al designed a multifunctional nanoparticle drug delivery system based on macrophage membrane and platelet membrane hybrid membranes (FM@HA@VAN) (Figure 9A). The nanoparticles utilize macrophage-mediated inflammatory homing and platelet-guided bacterial targeting, exhibiting long-lasting retention and selective targeting of the infection site. Upon responding to pH changes at the infection site, the encapsulated vancomycin and hyaluronic acid are rapidly released, generating strong bactericidal and anti-inflammatory effects, and protecting articular cartilage (Figure 9B).130 Immunofluorescence analysis showed that FM@HA@VAN co-cultures reduced iNOS expression while increasing the CD206 level in macrophages. Furthermore, Western blot (WB) analysis also confirmed the potential of FM@HA@VAN in inducing the M1 to M2 macrophage phenotype shift.
 |
Figure 9 (A) Schematic of the two main steps in the preparation of FM@HA@VAN nanoparticles: 1) The HAMA is prepared by functionalizing HA through methacrylation and is subsequently copolymerized with DEGDA to fabricate HANG, which is then loaded with vancomycin to prepare HA@VAN. 2) FM is prepared by fusing MM and PM using the co-extrusion technique, and subsequently co-extruded with HA@VAN. (B) The mechanisms of action of the FM@HA@VAN nanoparticles for dual-targeted therapy of septic arthritis in vitro and in vivo (The rat image was created in BioRender. Zeping, (Y) (2024) https://BioRender.com/y23n096). 130 The original figure contained a spelling error “bactria. Green upward arrows indicate upregulated expression, while red downward arrows indicate downregulated expression. Abbreviations: MA, methacrylic anhydride; HAMA, methacrylated hyaluronic acid; HA, hyaluronic acid; DEGDA, di(ethylene glycol) diacrylate; HANG, hyaluronic acid nanogel; VAN, vancomycin; FM, fused membrane; MM, macrophage membrane; PM, platelet membrane; IFM, inflammation. |
Duan et al recently developed an innovative oral formulation, where macrophage membrane-coated nanoparticles are encapsulated in enteric polymer-coated gelatin capsules. This design cleverly protects the nanoparticles from degradation in the stomach, ensuring they are accurately delivered to the colon. At the site of colonic inflammation, these nanoparticles act as “decoys” that attract and bind to macrophages while neutralizing pro-inflammatory cytokines, thus playing a pivotal role in the treatment of inflammatory bowel disease.164 Overall, through design, CNNPs exhibit excellent anti-inflammatory modulation capabilities, demonstrating great potential in the treatment of inflammation-related diseases, such as chronic refractory wounds.
Oxidative stress is another key feature of chronic wounds, and inhibiting oxidative stress can promote tissue repair and regeneration, making antioxidant properties equally important in wound healing. Fortunately, CNNPs not only show potential in inhibiting excessive inflammatory responses and immune modulation but can also enhance the antioxidant capacity at the site of inflammation. For instance, in cerebral ischemia-reperfusion injury (CIRI), the accumulation of ROS leads to various oxidative damages, causing glial cell activation, infiltration of inflammatory cells, production of pro-inflammatory cytokines, and ultimately neuronal cell death. Edaravone (Edv) is a primary drug used in clinical stroke treatment to clear ROS; however, it has limitations such as low efficiency in crossing the blood-brain barrier, a short half-life, and strong toxic side effects at high concentrations. Therefore, increasing the drug concentration at the lesion site while reducing systemic toxicity is crucial. To address this, Dong et al developed a biomimetic nanoparticle system (SNM-NPs) wrapped in neutrophil membranes, which enables precise targeting of active oxygen and the inflammatory microenvironment.143 By modifying with stroke-homing peptide (SHp), SNM-NPs can target damaged neurons more rapidly. Furthermore, SNM-NPs are ROS-responsive, leading to the release of edaravone (Edv), which clears ROS and inhibits neuroinflammation. This demonstrates that CNNPs not only modulate inflammation but also precisely target inflammatory sites, exhibiting excellent ROS scavenging abilities.
Promoting Tissue Regeneration
CNNPs hold significant potential in the fields of wound repair and tissue regeneration. By simulating the unique properties of cell membranes, this technology greatly enhances the compatibility, targeting ability, and intercellular interactions of nanoparticles in the body, showcasing great potential in promoting tissue regeneration and repair at the wound site.28,76,77 First, CNNPs can be integrated with stem cell therapy by delivering specific signaling molecules to promote the directional differentiation and functional activity of stem cells. In the field of bone tissue repair, Ren et al developed an innovative nanoplatform that uses stem cell membranes (SCMs) to encapsulate zeolitic imidazolate framework-8 (ZIF-8) nanoparticles. This design not only improves biocompatibility but also enhances targeting capability toward mesenchymal stem cells (MSCs). The biomimetic nanoparticles regulate the sustained release of Zn2+, promoting specific internalization into MSCs, thereby significantly enhancing the osteogenic potential of the stem cells.144 Studies have shown that hybrid cell membranes derived from macrophages and MSCs retain the anti-inflammatory phenotype of macrophages and promote osteogenic differentiation. By regulating the inflammatory microenvironment, they promote the repair of bone defects.145 Building on this, Qiao et al prepared a dual siRNA formulation targeting soluble vascular endothelial growth factor receptor 1 (sFlt-1) and p75 neurotrophin receptor (p75NTR) for local delivery, extracted hybrid membranes as a dual siRNA gene delivery vector. These cell membrane-loaded dual siRNAs (sipFMs) enabled local gene therapy to promote the vascular and neural differentiation of bone repair matrices (Figure 10A).146 SipFMs effectively promoted the differentiation and migration of human umbilical vein endothelial cells (HUVECs), and in vitro experiments demonstrated that the platform promoted vascular differentiation (Figure 10B and C) and neural differentiation (Figure 10D) of MSCs.
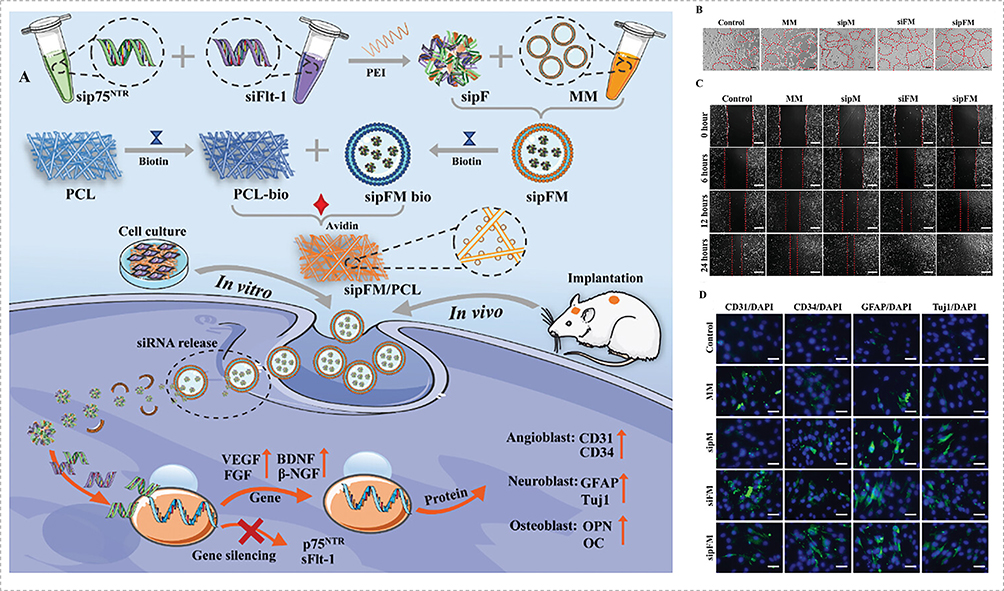 |
Figure 10 (A) Schematic illustrations of the dual siRNA-loaded cell membrane functionalized matrix facilitate bone regeneration with angiogenesis and neurogenesis The GFMs can regulate the expression of vascular-related genes and nerve-related genes, and promote the paracrine function of vascular and nerve factors in vitro. The bone repair matrix based on angiogenesis and neurogenesis improves the bone defects microenvironment and achieves bone defect repair and bone integration. (B) The images of the tube formation of HUVECs. Red dotted lines indicate the tube structures identified and quantified by ImageJ during tube formation analysis. The scale bar = 200 µm. (C) The images of wound healing assay. Red dotted lines indicate the initial wound edges used as reference for migration distance measurement at different time points. The scale bar = 50 µm. (D) The expression of CD31, CD34, GFAP, and Tuj1 markers of MSCs cultured with siRNA@MMs for 7 days. The scale bar = 50 µm.146 Red upward arrows indicate upregulated expression. |
Fibroblasts play a crucial role during the proliferative phase, where they migrate along the fibrin network and initiate epithelial regeneration at the wound edges. These cells secrete large amounts of extracellular matrix (ECM) proteins at the damaged area.54,56 Additionally, fibroblasts are temporarily activated into myofibroblasts, a highly contractile subtype of fibroblasts whose stress fibers consist of cytoplasmic actin and myosin, enabling them to express ECM proteins like collagen I (Col I) and alpha-smooth muscle actin (α-SMA).165 Myofibroblasts provide adhesion structures to the matrix and close the wound through cell contraction.166 Therefore, modulating the biological activity of myofibroblasts during the proliferative phase is a promising strategy to improve the outcome of dysregulated skin wound healing. In recent years, researchers in the field of wound repair have focused on using cell membrane-coated nanoparticle platforms to activate the transformation of fibroblasts into myofibroblasts, thus promoting skin wound healing. Additionally, by leveraging the drug delivery capabilities of CNNPs, cytokines are delivered to stimulate the proliferation and migration of key cells, such as fibroblasts and endothelial cells, to promote granulation tissue formation and epidermal regeneration. For example, Jia et al used cell membranes extracted from fibroblasts to coat gold nanoparticles and loaded them with IL-4 cytokine to promote skin wound healing (Figure 11A). This nanoparticle platform, (Au+IL-4)@MFM NPs, effectively cleared bacterial infections, modulated the inflammatory response, and promoted the transformation of fibroblasts into myofibroblasts, thereby accelerating the wound healing process (Figure 11B).147 Experimental results showed that (Au+IL-4)@MFM NPs promoted the differentiation of fibroblasts into myofibroblasts and enhanced fibroblast proliferation and migration, while promoting angiogenesis in skin wounds and inducing the conversion of endogenous macrophages into an anti-inflammatory phenotype (Figure 11C–F).
 |
Figure 11 (A) Preparation of gold nanoparticles, derivation of myofibroblast membrane, and synthesis of (Au+IL-4)@MFM NPs. (B) Regulatory mechanism of (Au+IL-4)@MFM NPs in wound healing process. The NPs release gold nanoparticles to clear bacteria, deliver IL-4 to repolarize macrophages for accelerating inflammation, and induce myofibroblast membrane to activate fibroblast-myofibroblast transition for improving outcomes of dysregulated skin wound healing. (C) The immunohistochemical images of CD31 expression (CD31 is an endothelial cell marker) at 6 d and 12 d. Scale bar = 100 μm. (D) The immunofluorescent images of CD31/α-SMA expression (CD31 is an endothelial cell marker, α-SMA is a myofibroblast marker) at 6 d and 12 d. Cell nucleus is stained with DAPI in blue, CD31 is stained in red, and α-SMA is stained in green. Scale bar = 50 μm. (E), (F) The immunofluorescent images of ARG1 (marker of M2 macrophage) and iNOS (marker of M1 macrophage) after different treatments for 6 and 12 d. Cell nucleus is stained with DAPI in blue, ARG1 is stained in red, and iNOS is stained in green. Scale bar = 100 μm.147 CD31 expression is shown, serving as an endothelial cell marker for angiogenesis. α-SMA expression is shown, serving as a myofibroblast marker for myofibroblast differentiation.147 Arrows indicate representative staining markers. Red upward arrows represent upregulated expression. |
As mentioned earlier, wound healing is a highly dynamic and orderly multi-stage process, involving the close connection of the inflammatory phase, proliferative phase and remodeling phase. Although existing studies have listed the independent functions of CNNPs in terms of antibacterial, anti-inflammatory, angiogenic promotion and tissue regeneration, their intelligent response and sequential treatment ability in intervening at different healing stages still need to be further clarified. The design of future CNNPs can focus on simulating the temporal nature of the natural healing process. By constructing environment-responsive nanoplatforms, on-demand release of different therapeutic drugs can be achieved148–150。For instance, multi-layer coated CNNPs with pH, ROS or enzyme responsiveness can be designed to preferentially release antibacterial drugs and anti-inflammatory factors during the inflammatory period to control infection and excessive inflammation. Subsequently, during the proliferative phase, in response to microenvironmental changes (such as elevated pH or expression of specific matrix metalloproteinases), the release of pro-angiogenic drugs (such as VEGF) or growth factors is triggered to promote granulation tissue formation and re-epithelialization; Ultimately, during the remodeling period, factors regulating the synthesis and degradation of ECM are continuously released to optimize the quality of tissue repair. Such stage adaptive CNNPs can not only precisely match the dynamic demands of the healing process, but also significantly improve the treatment efficiency and prognosis of chronic refractory wounds by reducing off-target effects and optimizing drug utilization.
Current Challenges
In recent years, Cell Membrane-Coated Nanoparticles (CMNPs) have demonstrated significant potential in chronic wound treatment due to their superior biocompatibility, prolonged circulation, and active targeting properties. However, despite advances in basic research, this technology still faces numerous challenges, including issues related to the source and large-scale production of cell membranes, nanoparticle stability and drug release control, biocompatibility and safety evaluation, immunogenicity, personalized treatment strategies, and technical barriers to clinical translation.29,167,168 Among them, quality control is the core challenge in achieving clinical transformation, especially how to ensure that each batch of products is uniformly controllable in terms of size, coating efficiency and biological activity to meet the strict standards of drug research and development.167,169 Addressing these key issues will be crucial for advancing the clinical application of CMNPs.
Firstly, the large-scale production of CMNPs is constrained by the source of cell membranes. Currently, cell membranes derived from red blood cells, macrophages, platelets, stem cells, and other sources are used to coat nanoparticles, imparting different biological functions. However, large-scale extraction and purification of cell membranes still face challenges, such as high cell culture costs, membrane protein denaturation during the extraction process, and batch-to-batch variations.170 Therefore, developing efficient membrane extraction and purification technologies, as well as establishing standardized quality control systems, are key steps for the industrialization of CMNPs. In terms of quality control, it is necessary to establish a series of quantifiable and repeatable evaluation criteria, ranging from the management of the cell bank at the cell source, to the monitoring of the composition and activity of membrane proteins during the membrane extraction process, and finally to the physical and chemical properties (such as size, Zeta potential, and coating integrity) and biological functions (such as targeting and immune escape ability) of the final CMNPs products.169
Secondly, the stability of CMNPs and the regulation of drug release still require further optimization.171,172 Due to the fluidity and degradable nature of cell membranes, CMNPs may undergo membrane fusion or membrane protein shedding in vivo, affecting their functional stability. Additionally, the cell membrane may influence the drug release rate, limiting the therapeutic effect. Some studies have attempted to enhance the stability and controllable release capability of CMNPs through cross-linking modifications, freeze-drying storage, or the construction of stimulus-responsive CMNPs (eg, pH, enzyme, or redox-responsive). These optimization strategies are crucial for improving the effectiveness of CMNPs in chronic wound treatment. During this process, it is necessary to establish corresponding stability indication methods, such as monitoring particle size changes, membrane protein retention rates and drug leakage rates in accelerated stability tests, and set clear shelf life standards to ensure the consistency of product quality during storage and transportation.
Furthermore, the biocompatibility and safety evaluation of CMNPs still need in-depth research.173 Although CMNPs are derived from natural cell membranes, the long-term degradation and metabolic pathways of CMNPs in vivo are not yet clear. Different types of cell membranes may induce distinct immune responses.171,172 For example, allogeneic cell membranes may contain MHC molecules, increasing immunogenicity and affecting their clinical application. Therefore, establishing a comprehensive biocompatibility assessment system, including in vivo pharmacokinetic analysis, immunogenicity evaluation, and long-term toxicity studies, will aid in advancing CMNPs to clinical trials. It is particularly crucial to establish quality control indicators for safety attributes such as immunogenicity, for instance, to monitor the immune response potential of products between batches through methods like in vitro cytokine release tests.
Regarding personalized treatment, CMNPs hold vast potential for application. For instance, by genetically engineering surface proteins on cell membranes or using the patient’s own cell membranes for nanoparticle coating, personalized drug delivery strategies can be achieved. Additionally, combining artificial intelligence and big data analysis to optimize pathological subtyping and immune status evaluation will help improve the precision and effectiveness of CMNPs in chronic wound treatment. This places higher demands on quality control, that is, it is necessary to develop a fast and efficient quality control platform that can adapt to small-batch and multi-batch production modes, ensuring that even personalized CMNPs products from self-sourced sources can meet the predetermined safety and effectiveness benchmarks.169
Despite the enormous potential shown by CMNPs in basic research, their clinical translation still faces obstacles such as production standardization, regulatory policy gaps, and safety validation issues. In the future, efforts should focus on optimizing cell membrane extraction and nanoparticle synthesis processes, developing low-immunogenicity, high-targeting CMNPs, and establishing stringent preclinical safety evaluation systems.29,167,168 Among them, establishing a full-chain quality control system covering raw materials, intermediates and final products, and promoting regulatory authorities to recognize innovative quality control methods applicable to CMNPs (such as determination based on biological potency), is the inevitable way to break through the bottleneck of clinical transformation.169 Additionally, exploring the combination of CMNPs with other advanced therapies, such as gene editing and stem cell therapy, may further enhance their clinical application value in chronic wound treatment. With the continuous development of nanomedicine and biotechnology, CMNPs are expected to become a key breakthrough strategy in the field of chronic wound repair.
Future Development Directions
With the rapid development of biomedical engineering, nanotechnology, and precision medicine, the application prospects of Cell Membrane-Coated Nanoparticles (CMNPs) in chronic wound repair are becoming increasingly broad. Future research will focus on areas such as cell membrane engineering, intelligent drug delivery, 3D bioprinting, and artificial intelligence-assisted treatment decision-making, aiming to overcome current technological bottlenecks and realize more precise, efficient, and safe wound repair strategies.120,121
In terms of cell membrane engineering, enhancing the targeting ability of CMNPs through genetic or chemical modifications is a key research direction.174,175 For example, modifying integrins or chemokine receptors to increase their specificity for damaged tissues, while employing multi-cell membrane coating strategies, could use red blood cell membranes to extend circulation time and macrophage membranes to enhance targeting capabilities at inflammation sites.85,109,110,112 This would allow for multi-functional synergistic effects. Additionally, the construction of artificial biomimetic membranes can further improve the stability and controllability of CMNPs, enhancing their therapeutic potential.76,118
In the field of intelligent nanoparticle delivery, combining CRISPR-Cas9 and other gene-editing tools with CMNPs can enable targeted regulation of inflammatory factors in wounds (such as TNF-α, IL-1β) or genes that promote tissue repair (such as VEGF, TGF-β).176 A pathological microenvironment-responsive system (such as pH, oxidative stress) can be used to achieve precise drug release, while combining photosensitive or magnetosensitive materials will allow drug release to be controlled by external stimuli, improving the controllability and efficiency of treatment.23,134
The application of 3D bioprinting technology enables the integration of CMNPs with hydrogels, collagen, and other biomaterials to construct bioactive, personalized biomimetic scaffolds.177 These scaffolds can be adapted to the wound morphology of different patients, providing mechanical support while continuously releasing healing-promoting factors. Furthermore, combining patient-specific cell membrane-coated nanomaterials with customized bio-inks can be achieved. High-throughput imaging analysis and computer-aided design (CAD) can precisely match the needs of wound repair.178 The rapid development of Artificial Intelligence (AI) technology also presents new opportunities for the precise application of CMNPs. AI can be used for deep learning analysis of wound images (such as OCT, ultrasound, or infrared thermography) to assess the wound healing status, predict the efficacy of different treatment options, and dynamically optimize CMNP delivery strategies. AI can also be employed for large-scale screening of bioactive molecules, optimizing CMNP membrane protein modification strategies to enhance their potential in personalized treatments.179,180 Despite the challenges of biocompatibility, batch production, and standardization in the clinical translation of CMNPs, interdisciplinary integration is expected to lead to breakthrough progress in chronic wound repair, providing more precise and efficient treatment options for patients.29,167,168
Conclusion
The treatment of chronic wounds remains a major challenge in clinical medicine and biomedical engineering. Traditional therapies are limited by poor biocompatibility, low drug delivery efficiency, and the complexity of the wound microenvironment, which hinder effective healing. In recent years, cell membrane-coated nanoparticles (CMNPs) have emerged as a promising therapeutic strategy. By combining the high loading capacity of synthetic nanoparticles with the biomimetic properties of natural cell membranes, CMNPs can evade immune clearance, achieve targeted delivery, and release therapeutic agents in a controlled and stage-specific manner.
Importantly, CMNPs exhibit multiple synergistic mechanisms, including antibacterial activity, anti-inflammatory effects, promotion of angiogenesis, and facilitation of tissue regeneration, which collectively enhance wound repair. Experimental studies and animal models have demonstrated their efficacy and versatility. Despite these advances, several challenges remain for clinical translation, including large-scale production, quality control, and long-term safety.
With ongoing progress in nanotechnology, biotechnology, and precision medicine, CMNPs are expected to become a core platform for chronic wound management, providing an integrated approach that addresses the multifaceted biological processes of wound healing.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author Yuchang Wang upon reasonable request.
Consent Statement
No individual personal data is included in the study.
Funding
This study was supported by grants from National Natural Science Foundation of China (No. 82002101, 82002096), Natural Science Foundation of Hubei Province (No. 2023AFB825) and Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (No. 2023A15).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hao R, Luo M, Xiao Y, et al. The efficacy and safety of negative-pressure wound therapy combined with platelet-rich plasma in chronic refractory wounds: a systematic review and meta-analysis of randomized controlled trials. Health Sci Rep. 2024;7(11):e70205. doi:10.1002/hsr2.70205
2. Xue X, Bian Y, Yang M, et al. Evaluation of injectable platelet-rich fibrin produced by a simple twice-centrifugation method combined with vacuum sealing drainage technology in the treatment of chronic refractory wounds. Front Bioeng Biotechnol. 2022;10:979834. doi:10.3389/fbioe.2022.979834
3. Mishra A, Kushare A, Gupta MN, et al. Advanced dressings for chronic wound management. ACS Appl Bio Mater. 2024;7(5):2660–31. doi:10.1021/acsabm.4c00138
4. Blanco-Fernandez B, Castaño O, Mateos-Timoneda MÁ, et al. Nanotechnology approaches in chronic wound healing. Adv Wound Care. 2021;10(5):234–256. doi:10.1089/wound.2019.1094
5. Kuehn BM. Chronic wound care guidelines issued. JAMA. 2007;297(9):938–939.
6. Spampinato SF, Caruso GI, De Pasquale R, et al. The treatment of impaired wound healing in diabetes: looking among old drugs. Pharmaceuticals. 2020;13(4):60. doi:10.3390/ph13040060
7. Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17(6):763–771. doi:10.1111/j.1524-475X.2009.00543.x
8. Sen CK. Human wound and its burden: updated 2022 compendium of estimates. Adv Wound Care. 2023;12(12):657–670. doi:10.1089/wound.2023.0150
9. Boateng JS, Matthews KH, Stevens HNE, et al. Wound healing dressings and drug delivery systems: a review. J Pharm Sci. 2008;97(8):2892–2923. doi:10.1002/jps.21210
10. Farahani M, Shafiee A. Wound healing: from passive to smart dressings. Adv Healthc Mater. 2021;10(16):e2100477. doi:10.1002/adhm.202100477
11. Aljghami ME, Saboor S, Amini-Nik S. Emerging innovative wound dressings. Ann Biomed Eng. 2019;47(3):659–675. doi:10.1007/s10439-018-02186-w
12. Catanzano O, Quaglia F, Boateng JS. Wound dressings as growth factor delivery platforms for chronic wound healing. Expert Opin Drug Deliv. 2021;18(6):737–759. doi:10.1080/17425247.2021.1867096
13. Nur MG, Rahman M, Dip TM, et al. Recent advances in bioactive wound dressings. Wound Repair Regen. 2025;33(1):e13233. doi:10.1111/wrr.13233
14. Qiu L, Wang F, Xu Q, et al. Negative pressure wound therapy promotes healing and reduced pain in patients with acute suppurative mastitis. BMC Womens Health. 2022;22(1):243. doi:10.1186/s12905-022-01785-z
15. Huang T, Liu T, Shang M, et al. Clinical application of improved VSD and VSD in the treatment of SSI after abdominal surgery: a retrospective randomized clinical study. Medicine. 2023;102(6):e32785. doi:10.1097/MD.0000000000032785
16. Dam P, Celik M, Ustun M, et al. Wound healing strategies based on nanoparticles incorporated in hydrogel wound patches. RSC Adv. 2023;13(31):21345–21364.
17. Tiwari R, Pathak K. Local drug delivery strategies towards wound healing. Pharmaceutics. 2023;15(2):634. doi:10.3390/pharmaceutics15020634
18. Qin W, Wu Y, Liu J, et al. A comprehensive review of the application of nanoparticles in diabetic wound healing: therapeutic potential and future perspectives. Int J Nanomed. 2022;17:6007–6029. doi:10.2147/IJN.S386585
19. Hu Q, Sun W, Qian C, et al. Anticancer platelet-mimicking nanovehicles. Adv Mater. 2015;27(44):7043–7050. doi:10.1002/adma.201503323
20. Lin RR, Jin -L-L, Xue -Y-Y, et al. Hybrid membrane-coated nanoparticles for precise targeting and synergistic therapy in Alzheimer’s disease. Adv Sci. 2024;11(24):e2306675. doi:10.1002/advs.202306675
21. Kou L, Bhutia YD, Yao Q, et al. Transporter-guided delivery of nanoparticles to improve drug permeation across cellular barriers and drug exposure to selective cell types. Front Pharmacol. 2018;9:27. doi:10.3389/fphar.2018.00027
22. Blanco E, Shen H, Ferrari M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat Biotechnol. 2015;33(9):941–951. doi:10.1038/nbt.3330
23. Zhu J, Niu Y, Li Y, et al. Stimuli-responsive delivery vehicles based on mesoporous silica nanoparticles: recent advances and challenges. J Mater Chem B. 2017;5(7):1339–1352. doi:10.1039/C6TB03066A
24. Verma M, Nisha A, Bathla M, et al. Resveratrol-encapsulated glutathione-modified robust mesoporous silica nanoparticles as an antibacterial and antibiofilm coating agent for medical devices. ACS Appl Mater Interfaces. 2023;15(50):58212–58229. doi:10.1021/acsami.3c13733
25. Liu M, Guinart A, Granados A, et al. Coated cotton fabrics with antibacterial and anti-inflammatory silica nanoparticles for improving wound healing. ACS Appl Mater Interfaces. 2024;16(12):14595–14604. doi:10.1021/acsami.4c00383
26. Yu D, Chen L, Yan T, et al. Enhancing infected diabetic wound healing through multifunctional nanocomposite-loaded microneedle patch: inducing multiple regenerative sites. Adv Healthc Mater. 2024;13(20):e2301985. doi:10.1002/adhm.202301985
27. Mitchell MJ, Billingsley MM, Haley RM, et al. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov. 2021;20(2):101–124. doi:10.1038/s41573-020-0090-8
28. Fang RH, Jiang Y, Fang JC, et al. Cell membrane-derived nanomaterials for biomedical applications. Biomaterials. 2017;128:69–83. doi:10.1016/j.biomaterials.2017.02.041
29. Oroojalian F, Beygi M, Baradaran B, et al. Immune cell membrane-coated biomimetic nanoparticles for targeted cancer therapy. Small. 2021;17(12):e2006484. doi:10.1002/smll.202006484
30. Fang RH, Kroll AV, Gao W, et al. Cell membrane coating nanotechnology. Adv Mater. 2018;30(23):e1706759. doi:10.1002/adma.201706759
31. Fang RH, Gao W, Zhang L. Targeting drugs to tumours using cell membrane-coated nanoparticles. Nat Rev Clin Oncol. 2023;20(1):33–48. doi:10.1038/s41571-022-00699-x
32. Li M, Guo Q, Zhong C, et al. Multifunctional cell membranes-based nano-carriers for targeted therapies: a review of recent trends and future perspective. Drug Deliv. 2023;30(1):2288797. doi:10.1080/10717544.2023.2288797
33. Krishnan N, Peng F-X, Mohapatra A, et al. Genetically engineered cellular nanoparticles for biomedical applications. Biomaterials. 2023;296:122065. doi:10.1016/j.biomaterials.2023.122065
34. Peng XR, Chen J, Gan Y, et al. Biofunctional lipid nanoparticles for precision treatment and prophylaxis of bacterial infections. Sci Adv. 2024;10(14). doi:10.1126/sciadv.adk9754.
35. Narain A, Asawa S, Chhabria V, et al. Cell membrane coated nanoparticles: next-generation therapeutics. Nanomedicine. 2017;12(21):2677–2692. doi:10.2217/nnm-2017-0225
36. Dabrowska AK, Spano F, Derler S, et al. The relationship between skin function, barrier properties, and body-dependent factors. Skin Res Technol. 2018;24(2):165–174. doi:10.1111/srt.12424
37. Nethi SK, Das S, Patra CR, et al. Recent advances in inorganic nanomaterials for wound-healing applications. Biomater Sci. 2019;7(7):2652–2674. doi:10.1039/C9BM00423H
38. Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med. 2014;6(265):265sr6. doi:10.1126/scitranslmed.3009337
39. Gurtner GC, Werner S, Barrandon Y, et al. Wound repair and regeneration. Nature. 2008;453(7193):314–321. doi:10.1038/nature07039
40. Pena OA, Martin P. Cellular and molecular mechanisms of skin wound healing. Nat Rev Mol Cell Biol. 2024;25(8):599–616. doi:10.1038/s41580-024-00715-1
41. Berk BC, Alexander RW, Brock TA, et al. Vasoconstriction: a new activity for platelet-derived growth factor. Science. 1986;232(4746):87–90. doi:10.1126/science.3485309
42. Pool JG. Normal hemostatic mechanisms: a review. Am J Med Technol. 1977;43(8):776–780.
43. Pierce GF, Mustoe TA, Altrock BW, et al. Role of platelet-derived growth factor in wound healing. J Cell Biochem. 1991;45(4):319–326. doi:10.1002/jcb.240450403
44. Furie B, Furie BC. Mechanisms of thrombus formation. N Engl J Med. 2008;359(9):938–949. doi:10.1056/NEJMra0801082
45. Clark RA. Fibrin and wound healing. Ann N Y Acad Sci. 2001;936:355–367. doi:10.1111/j.1749-6632.2001.tb03522.x
46. Kiritsy CP, Lynch AB, Lynch SE. Role of growth factors in cutaneous wound healing: a review. Crit Rev Oral Biol Med. 1993;4(5):729–760. doi:10.1177/10454411930040050401
47. Eming SA, Krieg T, Davidson JM. Inflammation in wound repair: molecular and cellular mechanisms. J Invest Dermatol. 2007;127(3):514–525. doi:10.1038/sj.jid.5700701
48. Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med. 1999;341(10):738–746. doi:10.1056/NEJM199909023411006
49. Velnar T, Bailey T, Smrkolj V. The wound healing process: an overview of the cellular and molecular mechanisms. J Int Med Res. 2009;37(5):1528–1542. doi:10.1177/147323000903700531
50. Xu J, Liu X, Zhao F, et al. HIF1alpha overexpression enhances diabetic wound closure in high glucose and low oxygen conditions by promoting adipose-derived stem cell paracrine function and survival. Stem Cell Res Ther. 2020;11(1):148. doi:10.1186/s13287-020-01654-2
51. Bronckaers A, Hilkens P, Martens W, et al. Mesenchymal stem/stromal cells as a pharmacological and therapeutic approach to accelerate angiogenesis. Pharmacol Ther. 2014;143(2):181–196. doi:10.1016/j.pharmthera.2014.02.013
52. Malinda KM, Sidhu GS, Banaudha KK, et al. Thymosin alpha 1 stimulates endothelial cell migration, angiogenesis, and wound healing. J Immunol. 1998;160(2):1001–1006. doi:10.4049/jimmunol.160.2.1001
53. Tettamanti G, Grimaldi A, Rinaldi L, et al. The multifunctional role of fibroblasts during wound healing in Hirudo medicinalis (Annelida, Hirudinea). Biol Cell. 2004;96(6):443–455. doi:10.1016/j.biolcel.2004.04.008
54. Li B, Wang JH. Fibroblasts and myofibroblasts in wound healing: force generation and measurement. J Tissue Viabil. 2011;20(4):108–120. doi:10.1016/j.jtv.2009.11.004
55. Diller RB, Tabor AJ. The role of the extracellular matrix (ECM) in wound healing: a review. Biomimetics. 2022;7(3):87.
56. Montesinos MC, Gadangi P, Longaker M, et al. Wound healing is accelerated by agonists of adenosine A2 (G alpha s-linked) receptors. J Exp Med. 1997;186(9):1615–1620. doi:10.1084/jem.186.9.1615
57. Gill SE, Parks WC. Metalloproteinases and their inhibitors: regulators of wound healing. Int J Biochem Cell Biol. 2008;40(6–7):1334–1347. doi:10.1016/j.biocel.2007.10.024
58. Ehrlich HP, Hunt TK. Collagen organization critical role in wound contraction. Adv Wound Care. 2012;1(1):3–9. doi:10.1089/wound.2011.0311
59. Mascharak S, Talbott HE, Januszyk M, et al. Multi-omic analysis reveals divergent molecular events in scarring and regenerative wound healing. Cell Stem Cell. 2022;29(2):315–327e6. doi:10.1016/j.stem.2021.12.011
60. Broughton G 2nd, Janis JE, Attinger CE. Wound healing: an overview. Plast Reconstr Surg. 2006;117(7 Suppl):1e–S–32e–S. doi:10.1097/01.prs.0000222562.60260.f9
61. Raziyeva K, Kim Y, Zharkinbekov Z, et al. Immunology of acute and chronic wound healing. Biomolecules. 2021;11(5):700. doi:10.3390/biom11050700
62. Larouche J, Sheoran S, Maruyama K, et al. Immune regulation of skin wound healing: mechanisms and novel therapeutic targets. Adv Wound Care. 2018;7(7):209–231. doi:10.1089/wound.2017.0761
63. Huang YZ, Gou M, Da L-C, et al. Mesenchymal stem cells for chronic wound healing: current status of preclinical and clinical studies. Tissue Eng Part B Rev. 2020;26(6):555–570. doi:10.1089/ten.teb.2019.0351
64. Zhu S, Yu Y, Ren Y, et al. The emerging roles of neutrophil extracellular traps in wound healing. Cell Death Dis. 2021;12(11):984. doi:10.1038/s41419-021-04294-3
65. Wong SL, Demers M, Martinod K, et al. Diabetes primes neutrophils to undergo NETosis, which impairs wound healing. Nature Med. 2015;21(7):815–+. doi:10.1038/nm.3887
66. Seraphim PM, Leal EC, Moura J, et al. Lack of lymphocytes impairs macrophage polarization and angiogenesis in diabetic wound healing. Life Sci. 2020;254:117813. doi:10.1016/j.lfs.2020.117813
67. Wilkinson HN, Hardman MJ. Wound healing: cellular mechanisms and pathological outcomes. Open Biol. 2020;10(9):200223. doi:10.1098/rsob.200223
68. Venosi S, Ceccarelli G, de Angelis M, et al. Infected chronic ischemic wound topically treated with a multi-strain probiotic formulation: a novel tailored treatment strategy. J Transl Med. 2019;17(1):364. doi:10.1186/s12967-019-2111-0
69. Bhutani S, Vishwanath G. Hyperbaric oxygen and wound healing. Ind J Plast Surg. 2012;45(2):316–324. doi:10.4103/0970-0358.101309
70. Pastar I, Stojadinovic O, Yin NC, et al. Epithelialization in wound healing: a comprehensive review. Adv Wound Care. 2014;3(7):445–464. doi:10.1089/wound.2013.0473
71. Rousselle P, Braye F, Dayan G. Re-epithelialization of adult skin wounds: cellular mechanisms and therapeutic strategies. Adv Drug Deliv Rev. 2019;146:344–365.
72. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care. 2015;4(9):560–582. doi:10.1089/wound.2015.0635
73. He S, Walimbe T, Chen H, et al. Bioactive extracellular matrix scaffolds engineered with proangiogenic proteoglycan mimetics and loaded with endothelial progenitor cells promote neovascularization and diabetic wound healing. Bioact Mater. 2022;10:460–473. doi:10.1016/j.bioactmat.2021.08.017
74. Wang KN, Li -Z-Z, Zhou K, et al. Cell membrane-coated nanoparticles for dental, oral, and craniofacial diseases. Research. 2024;7:0478. doi:10.34133/research.0478
75. Simons K, Vaz WL. Model systems, lipid rafts, and cell membranes. Annu Rev Biophys Biomol Struct. 2004;33:269–295. doi:10.1146/annurev.biophys.32.110601.141803
76. Liu Y, Luo J, Chen X, et al. Cell membrane coating technology: a promising strategy for biomedical applications. Nanomicro Lett. 2019;11(1):100. doi:10.1007/s40820-019-0330-9
77. Liu H, Su -Y-Y, Jiang X-C, et al. Cell membrane-coated nanoparticles: a novel multifunctional biomimetic drug delivery system. Drug Deliv Transl Res. 2023;13(3):716–737. doi:10.1007/s13346-022-01252-0
78. Hu CMJ, Zhang L, Aryal S, et al. Erythrocyte membrane-camouflaged polymeric nanoparticles as a biomimetic delivery platform. Proc Natl Acad Sci USA. 2011;108(27):10980–10985. doi:10.1073/pnas.1106634108
79. Wei XL, Gao J, Fang RH, et al. Nanoparticles camouflaged in platelet membrane coating as an antibody decoy for the treatment of immune thrombocytopenia. Biomaterials. 2016;111:116–123. doi:10.1016/j.biomaterials.2016.10.003
80. McMillan JR, Watson IA, Ali M, et al. Evaluation and comparison of algal cell disruption methods: microwave, waterbath, blender, ultrasonic and laser treatment. Appl Energy. 2013;103:128–134. doi:10.1016/j.apenergy.2012.09.020
81. Kuznetsov VI, Haws SA, Fox CA, et al. General method for rapid purification of native chromatin fragments. J Biol Chem. 2018;293(31):12271–12282. doi:10.1074/jbc.RA118.002984
82. Chugh V, Krishna KV, Pandit A. Cell membrane-coated mimics: a methodological approach for fabrication, characterization for therapeutic applications, and challenges for clinical translation. ACS Nano. 2021;15(11):17080–17123. doi:10.1021/acsnano.1c03800
83. Franke WW, Lüder MR, Kartenbeck J, et al. Involvement of vesicle coat material in casein secretion and surface regeneration. J Cell Biol. 1976;69(1):173–195. doi:10.1083/jcb.69.1.173
84. Javed S, Alshehri S, Shoaib A, et al. Chronicles of nanoerythrosomes: an erythrocyte-based biomimetic smart drug delivery system as a therapeutic and diagnostic tool in cancer therapy. Pharmaceutics. 2021;13(3):368. doi:10.3390/pharmaceutics13030368
85. Kang T, Zhu Q, Wei D, et al. Nanoparticles coated with neutrophil membranes can effectively treat cancer metastasis. Acs Nano. 2017;11(2):1397–1411. doi:10.1021/acsnano.6b06477
86. Gao CY, Lin Z, Wu Z, et al. Stem-Cell-membrane camouflaging on near-infrared photoactivated upconversion nanoarchitectures for in vivo remote-controlled photodynamic therapy. ACS Appl Mater Interfaces. 2016;8(50):34252–34260. doi:10.1021/acsami.6b12865
87. Cao HQ, Dan Z, He X, et al. Liposomes coated with isolated macrophage membrane can target lung metastasis of breast cancer. Acs Nano. 2016;10(8):7738–7748. doi:10.1021/acsnano.6b03148
88. Yang R, Xu J, Xu L, et al. Cancer cell membrane-coated adjuvant nanoparticles with mannose modification for effective anticancer vaccination. Acs Nano. 2018;12(6):5121–5129. doi:10.1021/acsnano.7b09041
89. Rao L, He Z, Meng Q-F, et al. Effective cancer targeting and imaging using macrophage membrane-camouflaged upconversion nanoparticles. J Biomed Mater Res Part A. 2017;105(2):521–530. doi:10.1002/jbm.a.35927
90. Rao L, Bu -L-L, Xu J-H, et al. Red blood cell membrane as a biomimetic nanocoating for prolonged circulation time and reduced accelerated blood clearance. Small. 2015;11(46):6225–6236. doi:10.1002/smll.201502388
91. Vijayan V, Uthaman S, Park IK. Cell membrane coated nanoparticles: an emerging biomimetic nanoplatform for targeted bioimaging and therapy. Adv Exp Med Biol. 2018;1064:45–59.
92. Rao L, Bu -L-L, Cai B, et al. Cancer cell membrane-coated upconversion nanoprobes for highly specific tumor imaging. Adv Mater. 2016;28(18):3460–3466. doi:10.1002/adma.201506086
93. Bangham AD, Standish MM, Watkins JC. Diffusion of univalent ions across the lamellae of swollen phospholipids. J Mol Biol. 1965;13(1):238–252. doi:10.1016/S0022-2836(65)80093-6
94. Dehaini D, Wei X, Fang RH, et al. Erythrocyte-platelet hybrid membrane coating for enhanced nanoparticle functionalization. Adv Mater. 2017;29(16). doi:10.1002/adma.201606209.
95. Pitchaimani A, Nguyen TDT, Aryal S. Natural killer cell membrane infused biomimetic liposomes for targeted tumor therapy. Biomaterials. 2018;160:124–137. doi:10.1016/j.biomaterials.2018.01.018
96. Jiang LX, Zhu Y, Luan P, et al. Bacteria - anchoring hybrid liposome capable of absorbing multiple toxins for antivirulence therapy of Escherichia coli infection. Acs Nano. 2021;15(3):4173–4185. doi:10.1021/acsnano.0c04800
97. Niu XQ, Chen JJ, Gao JQ. Nanocarriers as a powerful vehicle to overcome blood-brain barrier in treating neurodegenerative diseases: focus on recent advances. Asian J Pharm Sci. 2019;14(5):480–496. doi:10.1016/j.ajps.2018.09.005
98. Johnston MJW, Semple SC, Klimuk SK, et al. Characterization of the drug retention and pharmacokinetic properties of liposomal nanoparticles containing dihydrosphingomyelin. Biochim Biophys Acta Biomembr. 2007;1768(5):1121–1127. doi:10.1016/j.bbamem.2007.01.019
99. Chen ZJ, Yang S-C, Liu X-L, et al. Nanobowl-supported liposomes improve drug loading and delivery. Nano Lett. 2020;20(6):4177–4187. doi:10.1021/acs.nanolett.0c00495
100. Chen G, Roy I, Yang C, et al. Nanochemistry and nanomedicine for nanoparticle-based diagnostics and therapy. Chem Rev. 2016;116(5):2826–2885. doi:10.1021/acs.chemrev.5b00148
101. Liu T, Shi C, Duan L, et al. A highly hemocompatible erythrocyte membrane-coated ultrasmall selenium nanosystem for simultaneous cancer radiosensitization and precise antiangiogenesis. J Mater Chem B. 2018;6(29):4756–4764. doi:10.1039/C8TB01398E
102. He W, Frueh J, Wu Z, He Q. Leucocyte membrane-coated janus microcapsules for enhanced photothermal cancer treatment. Langmuir. 2016;32(15):3637–3644. doi:10.1021/acs.langmuir.5b04762
103. Rao L, Cai B, Bu -L-L, et al. Microfluidic electroporation-facilitated synthesis of erythrocyte membrane-coated magnetic nanoparticles for enhanced imaging-guided cancer therapy. ACS Nano. 2017;11(4):3496–3505. doi:10.1021/acsnano.7b00133
104. Wang J, Zhu M, Nie G. Biomembrane-based nanostructures for cancer targeting and therapy: from synthetic liposomes to natural biomembranes and membrane-vesicles. Adv Drug Deliv Rev. 2021;178:113974. doi:10.1016/j.addr.2021.113974
105. Copp JA, Fang RH, Luk BT, et al. Clearance of pathological antibodies using biomimetic nanoparticles. Proc Natl Acad Sci USA. 2014;111(37):13481–13486. doi:10.1073/pnas.1412420111
106. Silva AKA, Di Corato R, Pellegrino T, et al. Cell-derived vesicles as a bioplatform for the encapsulation of theranostic nanomaterials. Nanoscale. 2013;5(23):11374–11384. doi:10.1039/c3nr01541f
107. Zhang Y, Zhang J, Chen W, et al. Erythrocyte membrane-coated nanogel for combinatorial antivirulence and responsive antimicrobial delivery against Staphylococcus aureus infection. J Control Release. 2017;263:185–191. doi:10.1016/j.jconrel.2017.01.016
108. Hu CM, Fang RH, Wang K-C, et al. Nanoparticle biointerfacing by platelet membrane cloaking. Nature. 2015;526(7571):118–121.
109. Han X, Wang C, Liu Z. Red blood cells as smart delivery systems. Bioconjugate Chem. 2018;29(4):852–860. doi:10.1021/acs.bioconjchem.7b00758
110. Zhang H. Erythrocytes in nanomedicine: an optimal blend of natural and synthetic materials. Biomater Sci. 2016;4(7):1024–1031. doi:10.1039/C6BM00072J
111. Hu CMJ, Fang RH, Wang K-C, et al. Nanoparticle biointerfacing by platelet membrane cloaking. Nature. 2015;526(7571):118–+. doi:10.1038/nature15373
112. Parodi A, Quattrocchi N, van de Ven AL, et al. Synthetic nanoparticles functionalized with biomimetic leukocyte membranes possess cell-like functions. Nat Nanotechnol. 2013;8(1):61–68. doi:10.1038/nnano.2012.212
113. Fang RH, Hu C-MJ, Luk BT, et al. Cancer cell membrane-coated nanoparticles for anticancer vaccination and drug delivery. Nano Lett. 2014;14(4):2181–2188. doi:10.1021/nl500618u
114. Gao CY, Lin Z, Jurado‐Sánchez B, et al. Stem cell membrane-coated nanogels for highly efficient in vivo tumor targeted drug delivery. Small. 2016;12(30):4056–4062. doi:10.1002/smll.201600624
115. Gao WW, Fang RH, Thamphiwatana S, et al. Modulating antibacterial immunity via bacterial membrane-coated nanoparticles. Nano Lett. 2015;15(2):1403–1409. doi:10.1021/nl504798g
116. Erez N, Truitt M, Olson P, et al. Cancer-associated fibroblasts are activated in incipient neoplasia to orchestrate tumor-promoting inflammation in an NF-kappaB-dependent manner. Cancer Cell. 2010;17(2):135–147. doi:10.1016/j.ccr.2009.12.041
117. Lin CC, Anseth KS. Cell-cell communication mimicry with poly(ethylene glycol) hydrogels for enhancing beta-cell function. Proc Natl Acad Sci U S A. 2011;108(16):6380–6385. doi:10.1073/pnas.1014026108
118. Jiang XH, Wu L, Zhang M, et al. Biomembrane nanostructures: multifunctional platform to enhance tumor chemoimmunotherapy effective drug delivery. J Control Release. 2023;361:510–533. doi:10.1016/j.jconrel.2023.08.002
119. Liu Y, Wang X, Ouyang B, et al. Erythrocyte-platelet hybrid membranes coating polypyrrol nanoparticles for enhanced delivery and photothermal therapy. J Mater Chem B. 2018;6(43):7033–7041. doi:10.1039/C8TB02143K
120. Yan HZ, Shao D, Lao YH, Li M, Hu H, Leong KW. Engineering cell membrane-based nanotherapeutics to target inflammation. Adv Sci. 2019;6(15):1900605.
121. Zhang JA, Feng K, Shen W-T, et al. Research advances of cellular nanoparticles as multiplex countermeasures. Acs Nano. 2024;18(44):30211–30223. doi:10.1021/acsnano.4c09830
122. Yaman S, Ramachandramoorthy H, Iyer P, et al. Targeted chemotherapy via HER2-based chimeric antigen receptor (CAR) engineered T-cell membrane coated polymeric nanoparticles. Bioact Mater. 2024;34:422–435. doi:10.1016/j.bioactmat.2023.12.027
123. Thamphiwatana S, Angsantikul P, Escajadillo T, et al. Macrophage-like nanoparticles concurrently absorbing endotoxins and proinflammatory cytokines for sepsis management. Proc Natl Acad Sci USA. 2017;114(43):11488–11493. doi:10.1073/pnas.1714267114
124. Jin Y, Liu S, Wang X, et al. Multifunctional microneedle patches loaded with engineered nitric oxide-releasing nanocarriers for targeted and synergistic chronic wound therapy. Adv Mater. 2025;37(5):e2413108. doi:10.1002/adma.202413108
125. Deng GJ, Sun Z, Li S, et al. Cell-membrane immunotherapy based on natural killer cell membrane coated nanoparticles for the effective inhibition of primary and abscopal tumor growth. Acs Nano. 2018;12(12):12096–12108. doi:10.1021/acsnano.8b05292
126. Liu H, Tang L, Yin Y, et al. Photoresponsive multirole nanoweapon camouflaged by hybrid cell membrane vesicles for efficient antibacterial therapy of Pseudomonas aeruginosa -infected pneumonia and wound. Adv Sci. 2024;11(35):e2403101. doi:10.1002/advs.202403101
127. Ma T, Zhai X, Huang Y, et al. A smart nanoplatform with photothermal antibacterial capability and antioxidant activity for chronic wound healing. Adv Healthc Mater. 2021;10(13):e2100033. doi:10.1002/adhm.202100033
128. Meng H, Su J, Shen Q, et al. A smart MMP-9-responsive hydrogel releasing M2 macrophage-derived exosomes for diabetic wound healing. Adv Healthc Mater. 2025;14(10):e2404966. doi:10.1002/adhm.202404966
129. Zha K, Xiong Y, Zhang W, et al. Waste to wealth: near-infrared/ph dual-responsive copper-humic acid hydrogel films for bacteria-infected cutaneous wound healing. ACS Nano. 2023;17(17):17199–17216. doi:10.1021/acsnano.3c05075
130. Yu ZP, Wang M, Li J, et al. A fused membrane-camouflaged biomimetic nanosystem for dual-targeted therapy of septic arthritis. Small. 2025;21(9):2410710.
131. Liu Y, Rao P, Qian H, et al. Regulatory fibroblast-like synoviocytes cell membrane coated nanoparticles: a novel targeted therapy for rheumatoid arthritis. Adv Sci. 2023;10(4):2204998.
132. Chen ZS, Zhang L, Yang Y, et al. Photothermal nanozyme-encapsulating microneedles for synergistic treatment of infected wounds. Adv Funct Mater. 2025;35(12):2417415.
133. Xiong JD, Tang H, Sun L, et al. A macrophage cell membrane-coated cascade-targeting photothermal nanosystem for combating intracellular bacterial infections. Acta Biomater. 2024;175:293–306. doi:10.1016/j.actbio.2023.12.045
134. Qin X, Li Y. Strategies to design and synthesize polymer-based stimuli-responsive drug-delivery nanosystems. Chembiochem. 2020;21(9):1236–1253. doi:10.1002/cbic.201900550
135. Wang D, Wang S, Zhou Z, et al. White blood cell membrane-coated nanoparticles: recent development and medical applications. Adv Healthc Mater. 2022;11(7):e2101349. doi:10.1002/adhm.202101349
136. Obuobi S, Wang Y, Khara JS, et al. Antimicrobial and anti-biofilm activities of surface engineered polycationic albumin nanoparticles with reduced hemolytic activity. Macromol Biosci. 2018;18(10):e1800196. doi:10.1002/mabi.201800196
137. Wang XY, Xia Z, Wang H, et al. Cell-membrane-coated nanoparticles for the fight against pathogenic bacteria, toxins, and inflammatory cytokines associated with sepsis. Theranostics. 2023;13(10):3224–3244. doi:10.7150/thno.81520
138. Shi M, Shen K, Yang B, et al. An electroporation strategy to synthesize the membrane-coated nanoparticles for enhanced anti-inflammation therapy in bone infection. Theranostics. 2021;11(5):2349–2363. doi:10.7150/thno.48407
139. Wang P, Di X, Li F, et al. Platelet membrane-coated HGF-PLGA nanoparticles promote therapeutic angiogenesis and tissue perfusion recovery in ischemic hindlimbs. ACS Appl Bio Mater. 2025;8(1):399–409. doi:10.1021/acsabm.4c01373
140. Peng H, Du F, Wang J, et al. Adipose-derived stem-cell-membrane-coated PLGA-PEI nanoparticles promote wound healing via efficient delivery of miR-21. Pharmaceutics. 2024;16(9):1113. doi:10.3390/pharmaceutics16091113
141. Qiao FY, Zou Y, Lv YG. Growth factor collected cell membrane-functionalized matrix for vascular-innervated bone regeneration. Compos B Eng. 2025;291:112019.
142. Zeng RY, Lv B, Lin Z, et al. Neddylation suppression by a macrophage membrane-coated nanoparticle promotes dual immunomodulatory repair of diabetic wounds. Bioact Mater. 2024;34:366–380. doi:10.1016/j.bioactmat.2023.12.025
143. Dong ZF, Tang L, Zhang Y, et al. A homing peptide modified neutrophil membrane biomimetic nanoparticles in response to ROS/inflammatory microenvironment for precise targeting treatment of ischemic stroke. Adv Funct Mater. 2024;34(4):2309167.
144. Ren N, Liang N, Dong M, et al. Stem cell membrane-encapsulated zeolitic imidazolate framework-8: a targeted nano-platform for osteogenic differentiation. Small. 2022;18(26):e2202485. doi:10.1002/smll.202202485
145. Qiao F, Lv Y. Hybrid cell membrane-functionalized matrixes for modulating inflammatory microenvironment and improving bone defect repair. Adv Healthc Mater. 2023;12(19):e2203047.
146. Qiao F, Zou Y, Bie B, et al. Dual siRNA-loaded cell membrane functionalized matrix facilitates bone regeneration with angiogenesis and neurogenesis. Small. 2024;20(8):e2307062. doi:10.1002/smll.202307062
147. Jia Q, Ding Y, Su Z, et al. Cell membrane-camouflaged nanoparticles activate fibroblast-myofibroblast transition to promote skin wound healing. Biofabrication. 2025;17(1):015036. doi:10.1088/1758-5090/ad9cc4
148. Qin J, Jiang K, Yuan Z, et al. A multifunctional MOF heterojunction for combating antibiotic resistance and promoting regenerative immunity. ACS Nano. 2025;19(46):39768–39782. doi:10.1021/acsnano.5c12462
149. Kong X, Hu R, Zhang P, et al. Modulating macrophage–nucleus pulposus cell crosstalk via sequential d rug delivery attenuates disc degeneration. Adv Sci. 2025;12(36):e07178.
150. Correa S, Grosskopf AK, Klich JH, et al. Injectable liposome-based supramolecular hydrogels for the programmable release of multiple protein drugs. Matter. 2022;5(6):1816–1838. doi:10.1016/j.matt.2022.03.001
151. Rao L, Tian R, Chen X. Cell-membrane-mimicking nanodecoys against infectious diseases. ACS Nano. 2020;14(3):2569–2574. doi:10.1021/acsnano.0c01665
152. Wang S, Duan Y, Zhang Q, et al. Drug targeting via platelet membrane-coated nanoparticles. Small Struct. 2020;1(1). doi:10.1002/sstr.202000018.
153. Gan YY, Li C, Peng X, et al. Fight bacteria with bacteria: Bacterial membrane vesicles as vaccines an delivery nanocarriers against bacterial infections. Nanomed Nanotechnol Biol Med. 2021;35:102398.
154. Fang RH, Luk BT, Hu CM, Zhang L. Engineered nanoparticles mimicking cell membranes for toxin neutralization. Adv Drug Delivery Rev. 2015;90:69–80.
155. Rasko DA, Sperandio V. Anti-virulence strategies to combat bacteria-mediated disease. Nat Rev Drug Discov. 2010;9(2):117–128. doi:10.1038/nrd3013
156. Cegelski L, Marshall GR, Eldridge GR, et al. The biology and future prospects of antivirulence therapies. Nat Rev Microbiol. 2008;6(1):17–27. doi:10.1038/nrmicro1818
157. Sankar S, Muthukaliannan GK. Deciphering the crosstalk between inflammation and biofilm in chronic wound healing: phytocompounds loaded bionanomaterials as therapeutics. Saudi J Biol Sci. 2024;31(4):103963. doi:10.1016/j.sjbs.2024.103963
158. Goswami AG, Basu S, Banerjee T, et al. Biofilm and wound healing: from bench to bedside. Eur J Med Res. 2023;28(1). doi:10.1186/s40001-023-01121-7.
159. Ma N, Cai K, Zhao J, et al. Mannosylated MOF encapsulated in Lactobacillus biofilm for dual-targeting intervention against mammalian Escherichia coli infections. Adv Mater. 2025;37(32). doi:10.1002/adma.202503056.
160. McCarty SM, Percival SL. Proteases and Delayed Wound Healing. Adv Wound Care. 2013;2(8):438–447. doi:10.1089/wound.2012.0370
161. James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen. 2008;16(1):37–44. doi:10.1111/j.1524-475X.2007.00321.x
162. Zhao XD, Pei D, Yang Y, et al. Green tea derivative driven smart hydrogels with desired functions for chronic diabetic wound treatment. Adv Funct Mater. 2021;31(18):2009442.
163. Hou MY, Wei Y, Zhao Z, et al. Immuno-engineered nanodecoys for the multi-target anti-inflammatory treatment of autoimmune diseases. Adv Mater. 2022;34(12). doi:10.1002/adma.202108817.
164. Duan Y, Zhang E, Fang RH, et al. Capsulated cellular nanosponges for the treatment of experimental inflammatory bowel disease. Acs Nano. 2023;17(16):15893–15904. doi:10.1021/acsnano.3c03959
165. Fu Y, Zhou Y, Wang K, et al. Extracellular matrix interactome in modulating vascular homeostasis and remodeling. Circ Res. 2024;134(7):931–949. doi:10.1161/CIRCRESAHA.123.324055
166. Younesi FS, Miller AE, Barker TH, Rossi FM, Hinz B. Fibroblast and myofibroblast activation in normal tissue repair and fibrosis. Nat Rev Mol Cell Biol. 2024;25(8):617–638.
167. Ma J, Jiang L, Liu G. Cell membrane-coated nanoparticles for the treatment of bacterial infection. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2022;14(5):e1825. doi:10.1002/wnan.1825
168. Lopes J, Lopes D, Pereira‐Silva M, et al. Macrophage cell membrane-cloaked nanoplatforms for biomedical applications. Small Meth. 2022;6(8):e2200289. doi:10.1002/smtd.202200289
169. Xu CH, Ye P-J, Zhou Y-C, et al. Cell membrane-camouflaged nanoparticles as drug carriers for cancer therapy. Acta Biomater. 2020;105:1–14. doi:10.1016/j.actbio.2020.01.036
170. Chen Y, Zhu M, Huang B, et al. Advances in cell membrane-coated nanoparticles and their applications for bone therapy. Biomater Adv. 2023;144:213232. doi:10.1016/j.bioadv.2022.213232
171. Zeng S, Tang Q, Xiao M, et al. Cell membrane-coated nanomaterials for cancer therapy. Mater Today Bio. 2023;20:100633. doi:10.1016/j.mtbio.2023.100633
172. Bhattacharya S, Beninger P. The emerging role of cell membrane-coated nanomaterials in cancer therapy. Curr Pharm Des. 2024;30:727–741. doi:10.2174/0113816128295414240221063434
173. Zhen X, Cheng P, Pu K. Recent advances in cell membrane-camouflaged nanoparticles for cancer phototherapy. Small. 2019;15(1):e1804105. doi:10.1002/smll.201804105
174. He Y, Zhang S, She Y, et al. Innovative utilization of cell membrane-coated nanoparticles in precision cancer therapy. Exploration. 2024;4(6):20230164. doi:10.1002/EXP.20230164
175. Su T, Huang K, Ma H, et al. Platelet-inspired nanocells for targeted heart repair after ischemia/reperfusion injury. Adv Funct Mater. 2019;29(4). doi:10.1002/adfm.201803567.
176. Fu X, Li J, Wu Y, et al. PAR2 deficiency tunes inflammatory microenvironment to magnify STING signalling for mitigating cancer metastasis via anionic CRISPR/Cas9 nanoparticles. J Control Release. 2023;363:733–746. doi:10.1016/j.jconrel.2023.10.017
177. Chen MS, Zhang Y, Zhang L. Fabrication and characterization of a 3D bioprinted nanoparticle-hydrogel hybrid device for biomimetic detoxification. Nanoscale. 2017;9(38):14506–14511. doi:10.1039/C7NR05322C
178. Vrana NE, Gupta S, Mitra K, et al. From 3D printing to 3D bioprinting: the material properties of polymeric material and its derived bioink for achieving tissue specific architectures. Cell Tissue Bank. 2022;23(3):417–440. doi:10.1007/s10561-021-09975-z
179. Tang S, Tang D, Zhou H, et al. Bacterial outer membrane vesicle nanorobot. Proc Natl Acad Sci U S A. 2024;121(30):e2403460121. doi:10.1073/pnas.2403460121
180. Mozafari N, Mozafari N, Dehshahri A, et al. Knowledge gaps in generating cell-based drug delivery systems and a possible meeting with artificial intelligence. Mol Pharm. 2023;20(8):3757–3778. doi:10.1021/acs.molpharmaceut.3c00162
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
pH/Redox Dual-Responsive Drug Delivery System with on-Demand RGD Exposure for Photochemotherapy of Tumors

Li Y, Nie J, Dai J, Yin J, Huang B, Liu J, Chen G, Ren L
International Journal of Nanomedicine 2022, 17:5621-5639
Published Date: 23 November 2022
Multifunctional Nanoparticles Codelivering Doxorubicin and Amorphous Calcium Carbonate Preloaded with Indocyanine Green for Enhanced Chemo-Photothermal Cancer Therapy

Yu J, Wang L, Xie X, Zhu W, Lei Z, Lv L, Yu H, Xu J, Ren J
International Journal of Nanomedicine 2023, 18:323-337
Published Date: 18 January 2023
Mucoadhesive-to-Mucopenetrating Nanoparticles for Mucosal Drug Delivery: A Mini Review
Zheng B, Liu D, Qin X, Zhang D, Zhang P
International Journal of Nanomedicine 2025, 20:2241-2252
Published Date: 20 February 2025
Progress in the Application of Novel Nanomaterials in Targeted Therapy for Liver Cancer

Wei X, Cao W, Wang S, Zhang Y, Gao Z, Wang S, Yao L, Zhang Z, Li X, Deng W, Xie Y, Li M
International Journal of Nanomedicine 2025, 20:2623-2643
Published Date: 3 March 2025
Nanocarrier-Mediated Delivery Systems of Phytochemicals to Enhance and Accelerate Diabetic Wound Healing Processes
Wahyuningsih ES, Muhaimin M, Chaerunisaa AY, Khairinisa MA
Drug Design, Development and Therapy 2026, 20:607020
Published Date: 18 June 2026