Back to Journals » International Journal of Women's Health » Volume 17
Causal Relationship Between Socioeconomic Inequality and Hormone-Related Gynecologic Diseases: A Two-Sample, Two-Step Mendelian Randomization Study
Authors Yu Y, Mao Z, Feng L, Li N, Jiao X, Zhang T, Cui B ![]()
Received 7 May 2025
Accepted for publication 7 October 2025
Published 23 October 2025 Volume 2025:17 Pages 3829—3839
DOI https://doi.org/10.2147/IJWH.S538836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Yi Yu,* Zhonghao Mao,* Lianlian Feng, Nannan Li, Xinlin Jiao, Teng Zhang, Baoxia Cui
Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baoxia Cui, Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, No. 107 Wenhua West Road, Jinan, Shandong, 250012, People’s Republic of China, Tel +86 185 6008 1862, Email [email protected]
Purpose: Although observational studies suggest a link between socioeconomic status (SES) and hormone-related gynecologic diseases, the causal direction and mediating mechanisms remain unclear. This study aims to explore the causal relationships and potential mediators using genetic data.
Patients and Methods: We conducted univariable and multivariable Mendelian randomization (UVMR and MVMR) analyses using genome-wide association study (GWAS) summary statistics from European populations to assess the causal effects of education, income, and occupation on five hormone-related gynecologic diseases. A two-step MR was applied to explore potential mediators.
Results: Genetically predicted higher educational attainment, but not income or occupation, showed the protective causal effect on the risk of endometriosis. In UVMR and MVMR analyses, a genetic predisposition for higher education was found to be causally associated with reduced rates of endometriosis (UVMR: OR = 0.94, 95% CI: 0.91– 0.98, P = 0.001; MVMR: OR = 0.92, 95% CI: 0.87– 0.98, P = 0.018) and uterine endometriosis (UVMR: OR = 0.91, 95% CI: 0.86– 0.98, P = 0.007; MVMR: OR = 0.88, 95% CI: 0.80– 0.96, P = 0.006). Mediation analysis indicated that major depression (MDD) might play a potential, causal mediating role between education and uterine endometriosis, with a mediation proportion of 12.22%.
Conclusion: These findings provide genetic evidence that educational attainment reduces the risk of uterine endometriosis, partly through MDD. Targeted public health strategies addressing education and mental health may help reduce disease burden.
Keywords: socioeconomic status, educational attainment, endometriosis, Mendelian randomization, major depression, female reproductive health
Introduction
Benign and malignant conditions affecting the female reproductive system exhibit a high global prevalence, significantly impacting women’s health and quality of life.1 Endocrine and metabolic factors play a crucial role in the pathogenesis and progression of numerous gynecological disorders.2 Research indicates that lifestyle habits, psychological factors, and pathological conditions can alter hormone metabolism in women, thereby serving as risk factors for these diseases.2,3 Of particular note is the high comorbidity between certain gynecological conditions and mood disorders, particularly chronic pain conditions like endometriosis, has garnered significant research interest in recent years.4–6 Notably, many of these hormonal and lifestyle-related risk factors are socially patterned, with strong ties to socioeconomic status (SES).
SES is a sociological construct that represents an individual’s relative position within society, typically assessed through education, income, occupational social class, or wealth.7 SES exerts a substantial influence on human behavior, lifestyle, well-being, and longevity.8,9 Recent studies employing both conventional and genetic epidemiological methods have demonstrated that SES disparities affect physical, psychological, and cognitive health outcomes.10–12 Furthermore, existing evidence suggests a correlation between lower SES and unfavorable hormone profiles across various endocrine axes.13 A cross-sectional study conducted in Denmark identified an association between lower SES and increased prevalence of endometriosis.14 Additionally, existing observational studies have suggested a correlation between SES and other hormone-related gynecological conditions, including endometrial cancer, ovarian cancer, uterine fibroids, and polycystic ovary syndrome (PCOS).15–18 Consequently, it is plausible to hypothesize that SES may have a causal relationship with hormone-related gynecological disorders. Among these SES indicators, educational attainment may exert a stronger causal effect on health outcomes. This is because education is typically completed early in life and remains stable thereafter, making it less susceptible to reverse causation. Furthermore, education influences health not only through economic pathways but also by enhancing health literacy and problem-solving skills, offering broader protective mechanisms.19,20 However, the current body of research lacks sufficient evidence to substantiate this potential link.
Mendelian randomization (MR) offers a methodological approach for inferring causality. In traditional observational studies, factors identified as influencing disease risk may later be revealed as non-causal through randomized controlled trials (RCTs), due to biases, confounding variables, and reverse causation. MR studies utilize genetic information as instrumental variables (IVs), effectively simulating natural RCTs.21 Moreover, two-step MR can help identify intermediate traits or mechanisms that lie on the causal pathway, providing insight into modifiable mediators.22
With the maturation of MR techniques and the availability of extensive datasets, research on genetic associations has become feasible. In this two-sample, two-step MR study, we investigated the independent causal effects of SES, encompassing education, income, and occupation, on five hormone-related gynecologic diseases. Additionally, we explored the mediating roles of lifestyle, psychological, and biological factors.
Materials and Methods
Study Design
Figure 1 illustrates the comprehensive study design, which comprises four steps. In Step 1, we employed univariable Mendelian randomization (UVMR) to examine the causal associations between education, income, and occupation and five hormone-related gynecologic diseases. In Step 2, we adjusted for potential confounders using multivariable Mendelian randomization (MVMR). Step 3 involved a further exploration of the causal relationship between SES and various sub-phenotypes of endometriosis. In Step 4, we identified potential mediators in the association between education and uterine endometriosis and quantified the mediating effects using two-step MR.
 |
Figure 1 Overview of the study design. |
Our study was reported according to The STROBE-MR Statement. Ethical approvals were not required for this study, as they had been obtained in the original studies.
Data Sources
Data pertaining to exposures, outcomes, potential mediators, and other variables were derived from summary-level statistics of genome-wide association studies (GWASs) involving individuals of European descent, as detailed in Table 1.
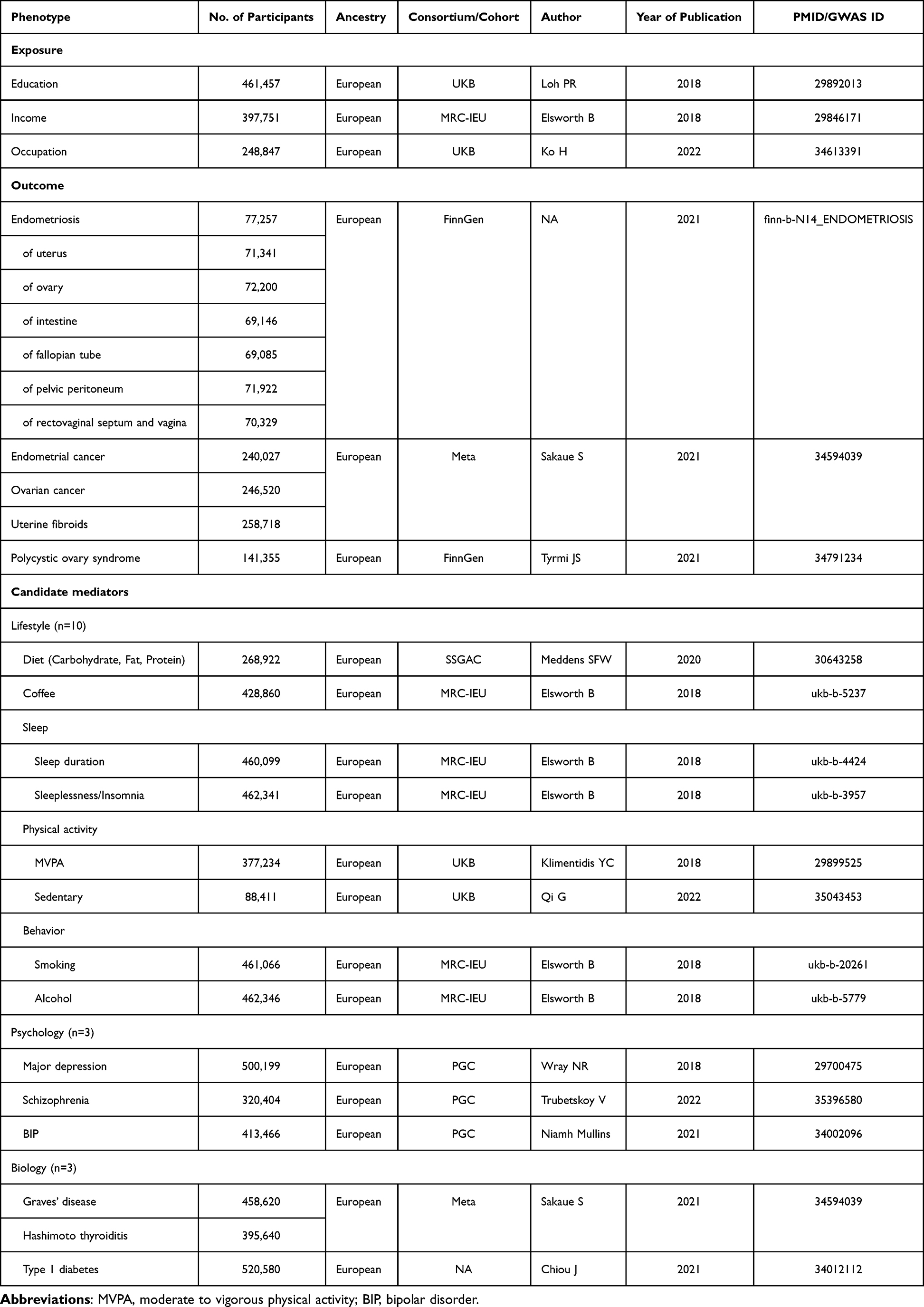 |
Table 1 Summary of the GWAS Data Used in the MR Analyses |
Exposures
The UK Biobank, a substantial prospective cohort, enrolled over 500,000 individuals aged 40 to 69 years from the general UK population and tracked their health outcomes over an extended period. SES was assessed using three indicators, educational attainment, household income, and occupational status. The GWAS data for educational attainment (n = 461,457), household income (n = 397,751), and occupational status (n = 248,847) were sourced from the UK Biobank.9,23–25
Educational attainment was measured by the number of years spent in full-time education.23 Household income was measured as average self-reported, pre-tax household income in 2006–10, on a continuous basis.24 Occupational status was determined using job levels classified by the UK Standard Occupational Classification system, ranging from “one” to “nine”.25 The genetic IVs for education, income, and occupation were identified at a genome-wide significance level (P < 5×10−8) and were independent of each other (linkage disequilibrium r² < 0.001 within 10,000 kb). We excluded single nucleotide polymorphisms (SNPs) associated with confounding factors using PhenoScanner v2. Palindromic SNPs with intermediate allele frequencies were excluded from the analysis. Furthermore, F statistics were calculated to assess the validity of the IVs.
Mediators and Other Traits
Drawing on previous findings (Supplementary Table 1), we identified 16 potential mediators (Table 1) that may play a role in the pathways linking SES to hormone-related gynecologic diseases, with available IVs derived from GWASs. The following criteria were employed in two-step MR to identify causal mediators: (1) the exposure was causally associated with the mediator, but not vice versa; (2) the mediator was causally and independently associated with the outcome; and (3) the exposure-mediator association and the mediator-outcome association were in opposite directions.
Based on a literature review, body size factors and menstrual factors may be associated with education and are also risk factors for endometriosis.26,27 We obtained genetic IVs for waist-to-hip ratio and age at menopause from GWASs and conducted MVMR analyses to adjust for these potential confounders and investigate the direct effect of exposures on outcomes.28,29
Outcomes
FinnGen intends to study the genome and national health register data of 500,000 Finnish individuals.30 Genetic IVs for outcomes were primarily from studies derived from FinnGen, which had little overlap with the GWASs of exposures to decrease the type 1 error rate. Summary-level GWAS data of the endometriosis (8288 cases / 68,969 controls) was accessible with the GWAS ID “finn-b-N14_ENDOMETRIOSIS” in the IEU OpenGWAS database. For further study, due to considerations of data availability, we pooled GWAS data for six sub-phenotypes of endometriosis from the FinnGen cohort.
Statistical Analysis
UVMR and MVMR
MR rests on three key assumptions: (1) the genetic IV is significantly associated with the exposure in UVMR and at least one of the multiple exposures in MVMR; (2) the genetic IV is not associated with confounders; and (3) the genetic IV influences the outcome solely through the exposure (no horizontal pleiotropic effect).31 We used the inverse variance weighted (IVW) method as the main method for UVMR and Weighted median (WM), MR Egger as the auxiliary. In MVMR, MV-IVW was utilized as the main analysis method.
Mediation MR Analysis
In two-step MR, two MR estimates were calculated: (1) the causal effect β1 of the exposure on the mediator and (2) the causal effect β2 of the mediator on the outcome. These two estimates could then be multiplied together to estimate the indirect effect (mediating effect, β1×β2).22 Mediation proportion could be calculated as the indirect effect/total effect of exposure on outcome (β1×β2/β).
MR Sensitivity Analysis
To assess the robustness of the IVW results in UVMR, we employed the WM and MR-Egger methods. MR-Egger regression was utilized to detect horizontal pleiotropy through the intercept term, with a P-value less than 0.05 for the Egger intercept term indicating the presence of horizontal pleiotropic bias. Cochran’s Q test was applied to evaluate the heterogeneity of genetic IVs, and an F statistic greater than 10 was indicative of a strong instrumental variable.
All processes were run using R 4.2.2. and the R package TwoSampleMR, MendelianRandomization, and MVMR.24 P values less than 0.05 were considered statistically significant. Effect sizes were displayed as β coefficient, odds ratio (OR), or proportion, accompanied by 95% confidence interval (95% CI).
Results
Total Effects of SES on Hormone-Related Gynecologic Diseases
In UVMR, genetically predicted extended years of education were causally associated with a reduced risk of endometriosis (OR = 0.94; 95% CI: 0.91–0.98; P = 0.001; Figure 2). Additionally, a modest causal relationship was observed between educational attainment and an increased risk of ovarian cancer (IVW: OR = 1.08, 95% CI: 1.01–1.15, P = 0.027; WM: OR = 1.06, 95% CI: 0.96–1.16, P = 0.244; MR Egger: OR = 0.99, 95% CI: 0.74–1.32, P = 0.927), but not endometrial cancer, uterine fibroids and PCOS (Supplementary Table 2). Furthermore, higher household income and occupational status were not causally linked to the risk of any of the five hormone-related gynecologic diseases examined (Supplementary Table 2). The robustness of the causal effect of education on endometriosis was confirmed by two sensitivity analyses.
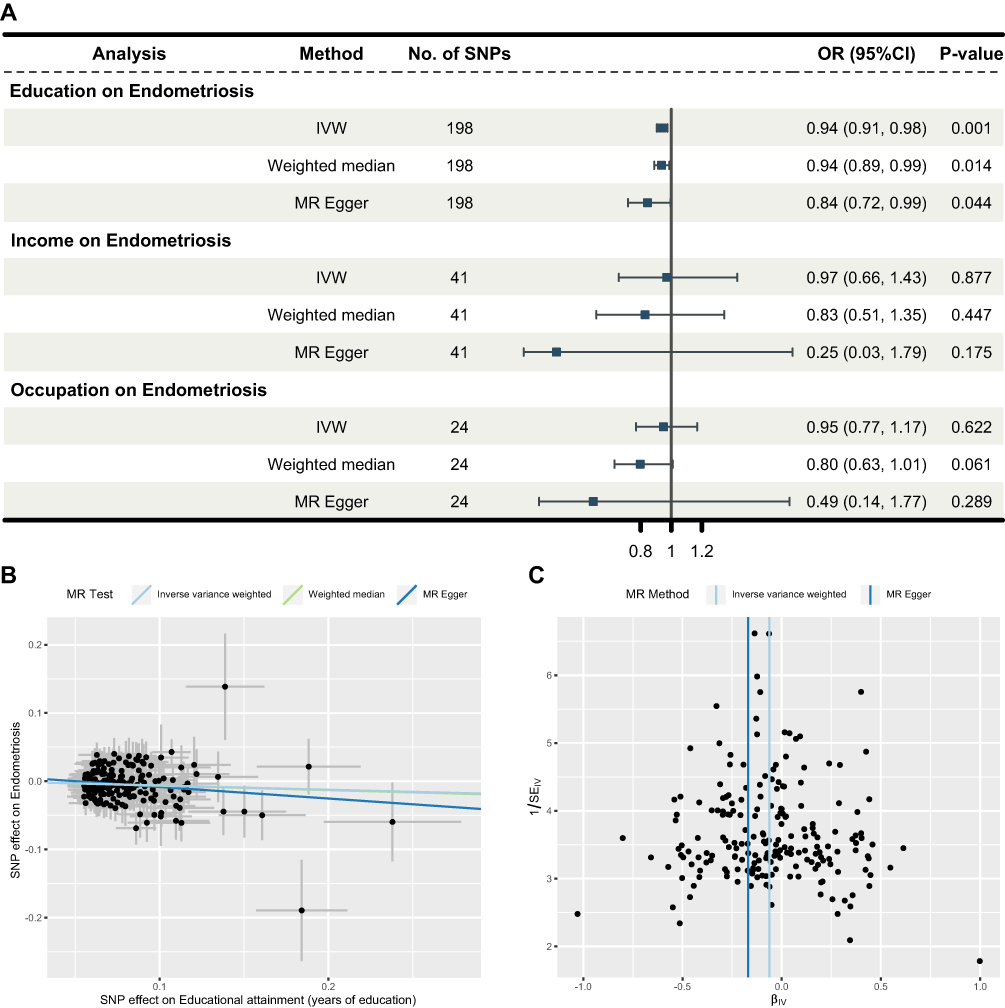 |
Figure 2 UVMR estimates the causal associations of education, income, and occupation with endometriosis. (A) Plots represent OR (95% CI) of IVW for the risk of endometriosis associated with each 1-SD increase in years of schooling, each one-s.d. increase in household income, or each one-point-higher occupational attainment. P < 0.05 is considered significant. (B and C) MR scatter plot and funnel plot for the causal associations of education with endometriosis. |
The genetic IVs for SES and hormone-related gynecologic diseases exhibited no heterogeneity, and there was no evidence of directional pleiotropy. All F statistics for IVs used in the UVMR were >10, suggesting strong instrument variables.
MVMR Analyses Adjusting Potential Confounders
To modulate potential confounders, MVMR analyses of the causal relationship between education and endometriosis and ovarian cancer were performed. After adjusting for waist-hip ratio and age at menopause, it was found that genetically predicted longer years of education remained causally associated with a reduced risk of endometriosis (OR = 0.92; 95% CI: 0.87–0.98; P = 0.018; Supplementary Figure 1), but the association with an increased risk of ovarian cancer was no longer statistically significant (Supplementary Table 3).
Causal Effects of Education on Various Sub-Phenotypes of Endometriosis
Sub-phenotypes of endometriosis can be distinguished based on the location and growth of the ectopic endometrial lesion. To further investigate the causal effects of genetically predicted educational attainment on the risk of six sub-phenotypes of endometriosis, we employed UVMR and MVMR. Among six sub-phenotypes of endometriosis, education showed the strongest protective effect against uterine endometriosis (UVMR: OR = 0.91, 95% CI: 0.86–0.98, P = 0.007; MVMR: OR = 0.88, 95% CI: 0.80–0.96, P = 0.006; Figure 3), while effects on other subtypes were weaker or not statistically significant (Supplementary Figure 2 and Supplementary Table 4). MR leave-one-out sensitivity analysis for educational attainment on endometriosis of the uterus revealed no potentially outlying IVs (Supplementary Figure 3).
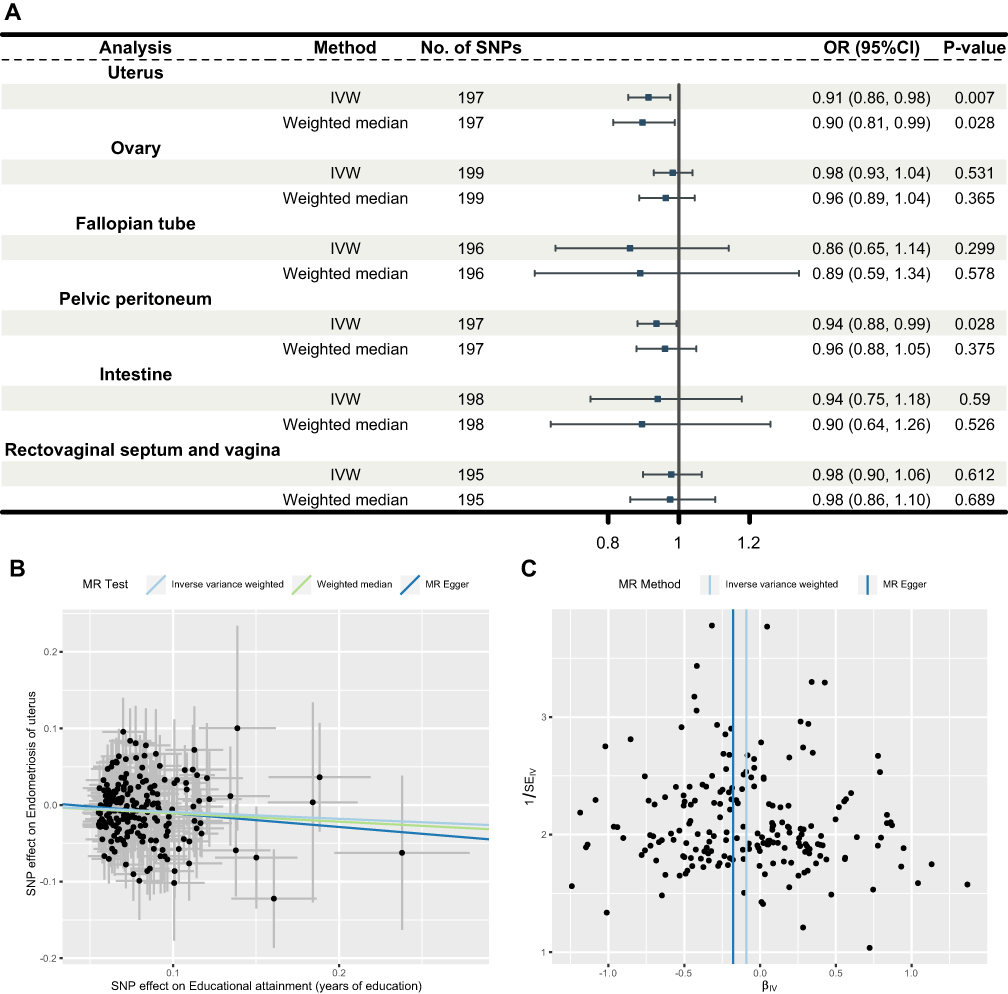 |
Figure 3 Causal effects of education on six sub-phenotypes of endometriosis. (A) In UVMR, IVW prompted the association of genetically predicted higher education with low risks of endometriosis of the uterus and the pelvic peritoneum. (B and C) MR scatter plot and funnel plot for the causal associations of education with endometriosis of the uterus. |
Two-Step MR to Screen for Mediating Pathways
In the subsequent two-step MR analysis aimed at identifying mediating pathways, 16 candidate mediators were evaluated, including 10 lifestyle factors, 3 psychological factors, and 3 biological factors, in the causal relationship between education and endometriosis of the uterus. The analysis indicated that major depressive disorder (MDD) may serve as a potential causal mediator (Supplementary Table 5). In UVMR, a higher genetically determined level of educational attainment was associated with a reduced risk of MDD (β1 = −0.032, 95% CI: −0.046 ~ −0.017; OR = 0.97, 95% CI: 0.95–0.98; P = 3.21E-05). Furthermore, genetically determined higher risks of MDD were causally linked to endometriosis of the uterus (β2 = 0.36, 95% CI: 0.012–0.70; OR = 1.43, 95% CI: 1.01–2.02; P = 0.043; Supplementary Figure 4). The proportion of the causal effect of educational attainment on endometriosis of the uterus mediated by MDD was estimated to be 12.22% (95% CI: 2.11–25.56%). However, the WM and MR Egger methods did not support a causal relationship between depression and uterine endometriosis.
Genetic IVs showed no heterogeneity, and no evidence of directional pleiotropy was observed.
Discussion
In this two-sample MR study, we found that genetically predicted higher educational attainment was causally associated with a reduced risk of endometriosis, particularly uterine endometriosis. This relationship may be partially mediated by MDD. These findings suggest that education may play a protective role in female reproductive health through both direct and indirect pathways. Prior epidemiological research has identified an inverse relationship between educational attainment and mental health disorders, including depression, anxiety, and attention deficit hyperactivity disorder.11 MR studies have corroborated the causal associations among these variables.32,33 Genetic correlation analyses have substantiated that the genetic factors contributing to endometriosis are shared with multiple comorbidities, such as depression.4,6 This two-step MR establishes a novel connection between these factors, potentially facilitating the identification of new targets for intervention.
Previous traditional observational studies and genetic correlation analyses have investigated the association between higher SES, particularly higher educational attainment, and various physical and mental disorders, healthy lifestyles, and multimorbidity,8,10,11 thereby highlighting the extensive benefits of education. Notably, our study identified a significant causal relationship between educational attainment, rather than income or occupation, and the incidence of endometriosis. Previous MVMR study examining the relationship between SES and health outcomes have shown that the protective effects of income and occupation may diminish after adjusting for educational attainment. In contrast, education consistently exhibits an independent causal effect.9 This suggests that education may be a more fundamental driver of health inequalities. The associations identified in observational research between lower income or occupational attainment and an elevated risk of endometriosis may be attributable to confounding by educational factors, rather than direct genetic causation. This finding is credible, as education is associated with enhanced employment opportunities and increased income in later life. Furthermore, higher educational attainment typically facilitates greater access to social resources, improved health literacy, and reduced experiences of debt and financial hardship.19,32 These factors serve as protective mechanisms for both physical and mental health. Nonetheless, while education generally exerts a positive influence on physical and mental well-being, it also perpetuates health inequalities.19 Additionally, the education–health association depends on the historical sociopolitical context, their presence and magnitude differ markedly over time, according to place, and public health events (for example, the COVID-19 pandemic).7 The causality between exposure as complex as SES and gynecologic disease is also multidimensional. There remains a pressing need for rigorous study designs and diverse forms of evidence, such as large-scale cohort studies, to further substantiate these findings.7 Such efforts can aid policymakers in developing evidence-based intervention strategies, enhancing educational attainment, and reducing health disparities among populations with varying SES.32
Endometriosis has emerged as a prevalent global issue, affecting 5–10% of women of reproductive age worldwide.1 It is linked to severe pelvic pain and infertility, significantly impairing quality of life, with current treatment options—surgery, hormonal therapy, and analgesics—seldom offering long-term relief. Research indicates that the financial burden of endometriosis on society is comparable to that of chronic diseases such as type 2 diabetes.34 Recent evidence suggests that endometriosis should be considered a multifactorial, complex systemic disease rather than solely a gynecological condition.35 Concurrently, there has been an emerging interest in investigating the psychiatric comorbidities associated with endometriosis.4,6 The above outlines the biological plausibility of MDD as a potential mediator. The relationship between depressive symptoms and endometriosis has been previously attributed to chronic pain.36 Although chronic pain is undoubtedly a significant contributing factor to this association, it is not the sole factor involved. An epidemiological and genetic association study has demonstrated that endometriosis is connected to women’s mental health through pleiotropic mechanisms.6 Our study builds upon existing evidence regarding the influence of SES on gynecological disorders, suggesting that increasing educational attainment and early intervention in psychological disorders may reduce the risk of endometriosis, which has important public health implications.
There are several highlights of this study. It is the first to identify the causal impact of SES on hormone-related gynecological diseases and to explore causal mediating effects in the impact pathways. We utilized GWAS data from the FinnGen study, with minimal sample overlap, to reduce the type I error rate.30 Additionally, we conducted several sensitivity analyses, employing multiple MR methods. The absence of horizontal pleiotropy suggests that the observed causal effects were not confounded by extraneous factors. We set selection criteria for mediators to ensure the reliability of our overall mediation MR analysis.
However, certain limitations persist. While our focus encompassed lifestyle, psychological, and biological factors, the mediating effects of educational attainment and endometriosis of the uterus were not fully elucidated. Additionally, potential mediators such as environmental endocrine-disrupting compounds and health literacy were excluded from this MR analysis due to constraints.19,37 The analysis was conducted using datasets from European individuals, thereby limiting the generalizability of our findings across different ancestries. Further research is required to explore the causal relationship between SES and hormone-related gynecological diseases in lower-middle-income countries and among diverse racial groups. Due to factors such as the inconsistent results of sensitivity analyses (when compared with the IVW method) regarding the mediating role of MDD, as well as potential weak instrument bias arising from measurement heterogeneity in income and occupation, the interpretation of the results necessitates caution. Therefore, the findings should be regarded as suggestive rather than definitive.
Our findings indicate that policies focused on promoting educational equity, such as enhancing access to quality education and encouraging prolonged schooling for girls, could serve as foundational strategies for reducing the future burden of gynecologic diseases. Furthermore, the potential mediation through MDD underscores the necessity of integrating mental health support into women’s healthcare systems, particularly for those with chronic pain conditions. Addressing these socioeconomic and mental health factors may not only mitigate disease risk but also contribute to narrow the pervasive health disparities observed in women’s reproductive health.
Conclusion
Our MR study showed the causal protective effect of educational attainment on endometriosis of the uterus that is potentially partly mediated by MDD. These findings extend beyond biological insight to offer a powerful mandate for public health action.
Data Sharing Statement
GWAS data sources can be found in Table 1, including the IEU OpenGWAS database (https://gwas.mrcieu.ac.uk/), the UK Biobank (http://www.nealelab.is/uk-biobank/), the FinnGen consortium (https://www.finngen.fi/en), and corresponding original research. Other data are available from the corresponding author.
Ethics Approval and Consent to Participate
Since the GWAS data used in this study are derived entirely from publicly available summary-level statistics, ethical approval is not required. According to Article 32 of China’s Measures for the Ethical Review of Biomedical Research Involving Humans, which took effect on February 18, 2023, biomedical research involving human participants may be exempt from ethical review under the following conditions: Item 1: Research based on public databases that does not involve the identification or use of personal information. Item 2: Analysis of collected data that does not involve the collection of new data or direct intervention in participants. Based on these provisions, this study qualifies for an exemption from ethical review, as it exclusively utilizes publicly accessible data and involves no direct interaction with human subjects or collection of new personal information.
Acknowledgments
We sincerely thank all the participants in the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Viganò P. Endometriosis. Nat Rev Dis Primer. 2018;4(1):9. doi:10.1038/s41572-018-0008-5
2. Patel S, Homaei A, Raju AB, Meher BR. Estrogen: the necessary evil for human health, and ways to tame it. Biomed Pharmacother. 2018;102:403–411. doi:10.1016/j.biopha.2018.03.078
3. Mintziori G, Nigdelis MP, Mathew H, Mousiolis A, Goulis DG, Mantzoros CS. The effect of excess body fat on female and male reproduction. Metabolism. 2020;107:154193. doi:10.1016/j.metabol.2020.154193
4. McGrath IM, Montgomery GW, Mortlock S. Insights from Mendelian randomization and genetic correlation analyses into the relationship between endometriosis and its comorbidities. Hum Reprod Update. 2023;29(5):655–674. doi:10.1093/humupd/dmad009
5. Adewuyi EO, Mehta D, Sapkota Y, et al. Genetic analysis of endometriosis and depression identifies shared loci and implicates causal links with gastric mucosa abnormality. Hum Genet. 2021;140(3):529–552. doi:10.1007/s00439-020-02223-6
6. Koller D, Pathak GA, Wendt FR, et al. Epidemiologic and genetic associations of endometriosis with depression, anxiety, and eating disorders. JAMA Network Open. 2023;6(1):e2251214. doi:10.1001/jamanetworkopen.2022.51214
7. Bann D, Wright L, Hughes A, Chaturvedi N. Socioeconomic inequalities in cardiovascular disease: a causal perspective. Nat Rev Cardiol. 2023;21(4):238–249. doi:10.1038/s41569-023-00941-8
8. Lawrence EM. Why do college graduates behave more healthfully than those who are less educated? J Health Soc Behav. 2017;58(3):291–306. doi:10.1177/0022146517715671
9. Ye CJ, Kong LJ, Wang YY, et al. Mendelian randomization evidence for the causal effects of socio-economic inequality on human longevity among Europeans. Nat Hum Behav. 2023;7(8):1357–1370. doi:10.1038/s41562-023-01646-1
10. Ni Y, Zhou Y, Kivimäki M, et al. Socioeconomic inequalities in physical, psychological, and cognitive multimorbidity in middle-aged and older adults in 33 countries: a cross-sectional study. Lancet Healthy Longev. 2023;4(11):e618–e628. doi:10.1016/S2666-7568(23)00195-2
11. Chlapecka A, Kagstrom A, Cermakova P. Educational attainment inequalities in depressive symptoms in more than 100,000 individuals in Europe. Eur Psychiatry. 2020;63(1):e97. doi:10.1192/j.eurpsy.2020.100
12. Cai J, Wei Z, Chen M, et al. Socioeconomic status, individual behaviors and risk for mental disorders: a Mendelian randomization study. Eur Psychiatry. 2022;65(1):e28. doi:10.1192/j.eurpsy.2022.18
13. Bann D, Hardy R, Cooper R, et al. Socioeconomic conditions across life related to multiple measures of the endocrine system in older adults: longitudinal findings from a British birth cohort study. Soc Sci Med. 2015;147:190–199. doi:10.1016/j.socscimed.2015.11.001
14. Josiasen M, Røssell EL, Zhu T, et al. Prevalence and sociodemographic distribution of endometriosis symptoms and indicators in Denmark. Eur J Obstet Gynecol Reprod Biol. 2025;307:109–120. doi:10.1016/j.ejogrb.2025.01.051
15. Alberg AJ, Moorman PG, Crankshaw S, et al. Socioeconomic status in relation to the risk of ovarian cancer in African-American women: a population-based case-control study. Am J Epidemiol. 2016;184(4):274–283. doi:10.1093/aje/kwv450
16. Massouh N, Jaffa AA, Jaffa MA. Diabetes and the social, biologic, and behavioral determinants of endometrial cancer in the United States. BMC Cancer. 2024;24(1):540. doi:10.1186/s12885-024-12192-y
17. Merkin SS, Phy JL, Sites CK, Yang D. Environmental determinants of polycystic ovary syndrome. Fertil Steril. 2016;106(1):16–24. doi:10.1016/j.fertnstert.2016.05.011
18. Parazzini F, La Vecchia C, Negri E, Cecchetti G, Fedele L. Epidemiologic characteristics of women with uterine fibroids: a case-control study. Obstet Gynecol. 1988;72(6):853–857. doi:10.1097/00006250-198812000-00008
19. Zajacova A, Lawrence EM. The relationship between education and health: reducing disparities through a contextual approach. Annu Rev Public Health. 2018;39:273–289. doi:10.1146/annurev-publhealth-031816-044628
20. Wang N, Jia X, Fan Z, et al. Educational inequalities in cardiovascular diseases and their mediating factors across different generations: a prospective cohort study. Eur Heart J Qual Care Clin Outcomes. 2025;11(5):622–630. doi:10.1093/ehjqcco/qcaf010
21. Lawlor DA, Harbord RM, Sterne JAC, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
22. Carter AR, Sanderson E, Hammerton G, et al. Mendelian randomisation for mediation analysis: current methods and challenges for implementation. Eur J Epidemiol. 2021;36(5):465–478. doi:10.1007/s10654-021-00757-1
23. Loh PR, Kichaev G, Gazal S, Schoech AP, Price AL. Mixed-model association for biobank-scale datasets. Nat Genet. 2018;50(7):906–908. doi:10.1038/s41588-018-0144-6
24. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife. 2018;7:e34408. doi:10.7554/eLife.34408
25. Ko H, Kim S, Kim K, et al. Genome-wide association study of occupational attainment as a proxy for cognitive reserve. Brain J Neurol. 2022;145(4):1436–1448. doi:10.1093/brain/awab351
26. Lin C, Wu Q, Luo Z, Du J, Hong ST, Chae HS. Association between triglyceride-glucose related index and endometriosis varies according to educational level. Nutrients. 2025;17(4):670. doi:10.3390/nu17040670
27. Parazzini F, Esposito G, Tozzi L, Noli S, Bianchi S. Epidemiology of endometriosis and its comorbidities. Eur J Obstet Gynecol Reprod Biol. 2017;209:3–7. doi:10.1016/j.ejogrb.2016.04.021
28. de Ridder CM, Bruning PF, Zonderland ML, et al. Body fat mass, body fat distribution, and plasma hormones in early puberty in females. J Clin Endocrinol Metab. 1990;70(4):888–893. doi:10.1210/jcem-70-4-888
29. Canavez FS, Werneck GL, Parente RCM, Celeste RK, Faerstein E. The association between educational level and age at the menopause: a systematic review. Arch Gynecol Obstet. 2011;283(1):83–90. doi:10.1007/s00404-009-1323-6
30. Kurki MI, Karjalainen J, Palta P, et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature. 2023;613(7944):508–518. doi:10.1038/s41586-022-05473-8
31. Emdin CA, Khera AV, Kathiresan S. Mendelian Randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
32. Jones DP, Wootton RE, Gill D, et al. Mental health as a mediator of the association between educational inequality and cardiovascular disease: a Mendelian randomization study. J Am Heart Assoc. 2021;10(17):e019340. doi:10.1161/JAHA.120.019340
33. Michaëlsson M, Yuan S, Melhus H, et al. The impact and causal directions for the associations between diagnosis of ADHD, socioeconomic status, and intelligence by use of a bi-directional two-sample Mendelian randomization design. BMC Med. 2022;20(1):106. doi:10.1186/s12916-022-02314-3
34. Simoens S, Dunselman G, Dirksen C, et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod Oxf Eng. 2012;27(5):1292–1299. doi:10.1093/humrep/des073
35. Farland LV, Degnan WJ, Bell ML, et al. Laparoscopically confirmed endometriosis and risk of incident stroke: a prospective cohort study. Stroke. 2022;53(10):3116–3122. doi:10.1161/STROKEAHA.122.039250
36. Gambadauro P, Carli V, Hadlaczky G. Depressive symptoms among women with endometriosis: a systematic review and meta-analysis. Am J Obstet Gynecol. 2019;220(3):230–241. doi:10.1016/j.ajog.2018.11.123
37. Interdonato L, Siracusa R, Fusco R, Cuzzocrea S, Di Paola R. Endocrine disruptor compounds in environment: focus on women’s reproductive health and endometriosis. Int J Mol Sci. 2023;24(6):5682. doi:10.3390/ijms24065682
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.