Back to Journals » International Journal of Women's Health » Volume 17
Causal Relationship Between Sex Hormone Binding Globulin and Obstetrical Disorders: A Two-Sample Bidirectional Mendelian Randomization Study
Authors Gan Y, Tan X, Tang Y, Shi Q, Qi H
Received 18 February 2025
Accepted for publication 18 June 2025
Published 11 July 2025 Volume 2025:17 Pages 1985—1999
DOI https://doi.org/10.2147/IJWH.S522635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Everett Magann
Yanqiong Gan,1,2,* Xinlin Tan,2,* Yu Tang,2 Qi Shi,2 Hongbo Qi1
1Department of Obstetrics, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Obstetrics, The Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongbo Qi, Department of Obstetrics, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China, Email [email protected]
Introduction: Obstetrical disorders critically impact maternal and fetal health. Sex hormone-binding globulin (SHBG) regulates pregnancy maintenance and maternal-infant outcomes through hormonal, metabolic, and inflammatory pathways, yet causal relationships with obstetrical disorders remain unclear. This Mendelian randomization (MR) study examined SHBG’s causal effects on 12 obstetrical conditions.
Methods: Using cis-protein quantitative trait loci (cis-pQTLs) of SHBG as instrumental variables, we conducted MR analyses in FinnGen and UK Biobank (UKBB), followed by meta-analyses. Inverse variance weighting (IVW) was primary method, with sensitivity analyses ensuring robustness.
Results: IVW-MR demonstrated reduced risks with elevated SHBG: gestational diabetes (OR[95%]=0.835[0.785– 0.889], PFDR=2.03× 10− 7), hyperemesis gravidarum (OR[95%]=0.823[0.728– 0.931], PFDR=5.94× 10− 3), gestational hypertension (OR[95%]=0.917[0.852– 0.987], PFDR=0.041), and early-pregnancy hemorrhage (OR[95%]=0.853[0.794– 0.916], PFDR=6.90× 10− 5). Meta-analysis confirmed SHBG’s causal role in gestational diabetes (P_combined< 0.05). COLOC revealed shared loci between SHBG and five disorders: gestational diabetes, hyperemesis, early hemorrhage, preterm delivery, and postpartum hemorrhage.
Conclusion: SHBG causally lowers risks of gestational diabetes, hypertension, hyperemesis, miscarriage, and preterm delivery, highlighting its clinical relevance in obstetrical pathophysiology.
Keywords: sex hormone binding globulin, obstetrical disorders, Mendelian randomization
Graphical Abstract:

Introduction
Pregnancy involves a complex array of physiological changes as the body adapts to support the developing fetus. While the adaptations listed above are normal, they can cause pathological conditions, obstetrical disorders, and negative pregnancy outcomes, such as gestational hypertension, gestational diabetes, miscarriage, early delivery, premature delivery, low birth weight, and so on.1–5 They are often connected through mechanisms such as abnormal placental function, metabolic disorders, and inflammatory responses. For example, controlling blood glucose during pregnancy reduces the risk of preeclampsia and preterm delivery, while controlling hypertension reduces the incidence of placental abruption and fetal growth restriction.6 Research has shown that the prevalence and progression of obstetric disorders are closely associated with various factors, including maternal age, overall nutritional status, imbalances in sex hormones, immune function, and genetic predispositions.7 However, there is currently no consensus among various studies regarding these findings. The precise causes of obstetrical disorders remain unclear and necessitate further investigation for validation.
The liver synthesizes and secretes a glycoprotein called sexual hormone binding globulin (SHBG). Through its specific binding to sex hormones, it regulates their biological effects by facilitating their transport and movement through the circulation.8 According to current studies, there may be an association between SHBG levels and insulin resistance, which is a major risk factor for the emergence of metabolic diseases like type 2 diabetes, hypertension, and obesity.9 However, their exact mechanism underlying this relationship remains unknown. There is significant evidence connecting SHBG levels to the occurrence of obstetrical and gynecological conditions, including gestational diabetes, gestational hypertension, and polycystic ovary syndrome.10 However, the majority of research on the subject are observational in nature, and there are not many looking into the relationship between SHBG and obstetric problems. This presents challenges in determining the true nature of this causal relationship, as the existing studies are conflicting. According to observational studies, a decrease in SHBG synthesis can increase the risk of gestational diabetes, which has been linked to a decrease in SHBG levels.11,12 Furthermore, individuals with gestational diabetes generally exhibit lower levels of SHBG. In contrast, a cross-sectional investigation did not discover any association between SHBG levels and the outcomes of an oral glucose tolerance test (OGTT).13
Although cross-sectional studies indicate a statistical connection between SHBG levels and obstetrical disorders like preeclampsia and gestational diabetes,14 the confounding bias and reverse causality interference inherent in traditional observational studies make it difficult to determine the causal temporality between them with the evidence available. Mendelian randomization (MR) is a method of studying genetic variation using Mendelian genetics, which reduces the interference of confounding variables and reverse causation, and is an effective method of exploring causal connection.15 Because naturally occurring genetic variation is randomly distributed among individuals and remains stable from birth, it is unaffected by environmental or social factors.16
Therefore, we conducted a MR study to assess the potential causal connection between genetically determined SHBG levels and the chance of developing gestational diabetes, single spontaneous delivery, excessive vomiting in pregnancy, early pregnancy hemorrhage, postpartum depression, preterm delivery, gestational hypertension, preeclampsia, intrahepatic cholestasis in pregnancy, placenta previa, postpartum hemorrhage, and ectopic pregnancy. The use of genetic variation through MR studies mitigates biases that often limit observational studies, such as reverse causality, and provides more reliable evidence support for exploring connection between exposures of interest (eg, SHBG) and obstetrical disorders, thus exploring whether SHBG can be a potential biomarker for risk stratification in pregnancy and guiding the development of precise clinical strategies for prevention and control.
Materials and Methods
Study Design
Based on public data from studies on humans, this genetic association study looked at how genetic differences affect people. The original articles contain detailed information about participants’ consent and ethical approval for every study that was included in the GWAS. This study followed the guidelines in Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR) (Supplementary Material S1).17 The overview of this study can be seen in Figure 1. Firstly, we selected the instrumental variables (IVs) for SHBG and then investigated the causal relationship between SHBG gene activation and 12 obstetrical disorders in FinnGen consortium and 11 obstetrical disorders in UK Biobank by performing a drug target MR and meta-analysis. Subsequently, we further performed bayesian colocalization analysis to eliminate linkage disequilibrium. After that, reverse MR analysis was performed to confirm the drug target MR findings. The study utilized GWAS summary statistics from various sources, which are detailed in Table 1. The MR investigation relies on three fundamental assumptions: (1) the instrumental variables (IVs) exhibit a robust correlation with the target proteins, (2) the IVs are not affected by any confounding factors, and (3) the IVs exclusively influence the likelihood of obstetrical diseases through the drug targets.
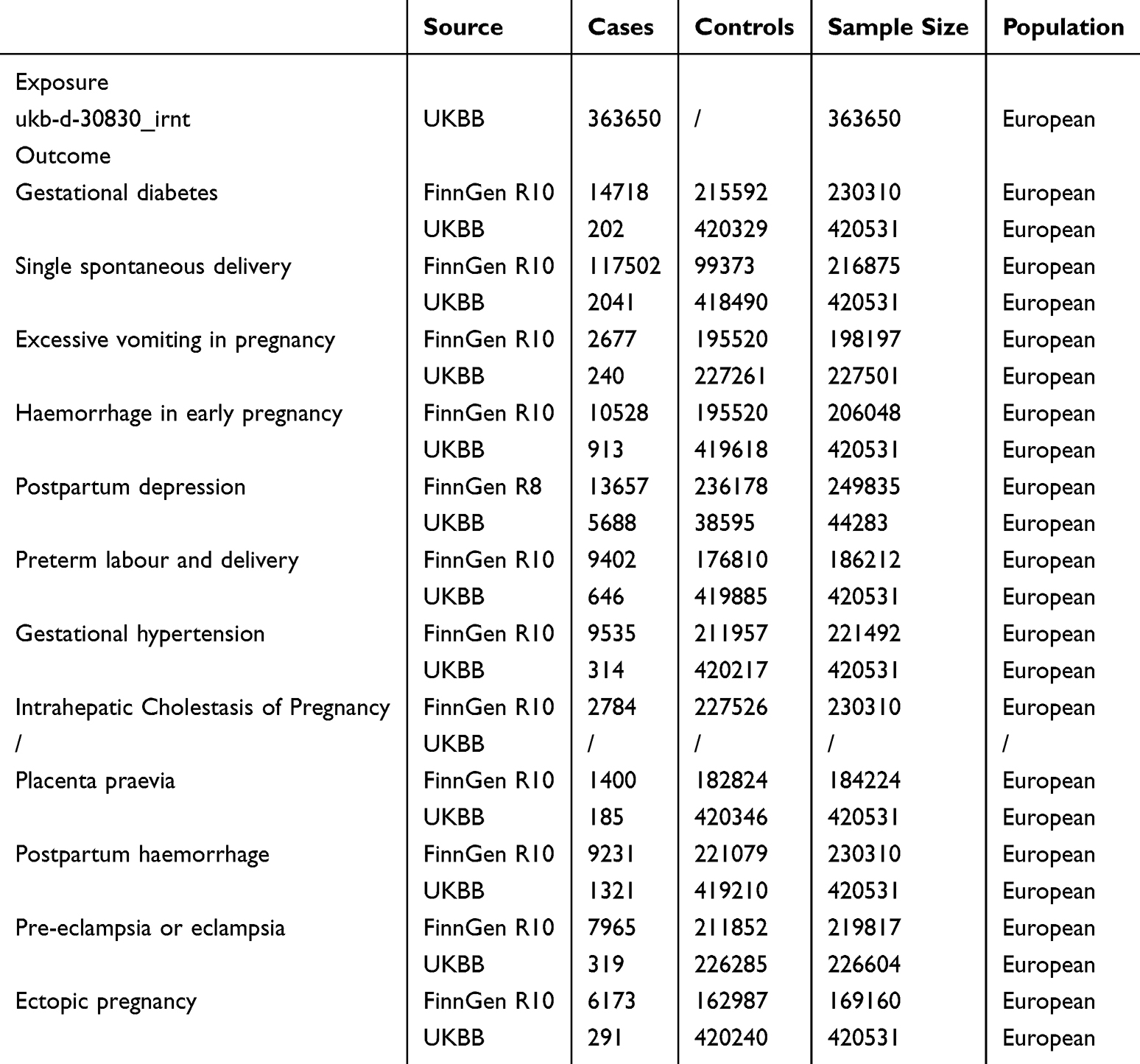 |
Table 1 Positive Results SNPs Characteristics |
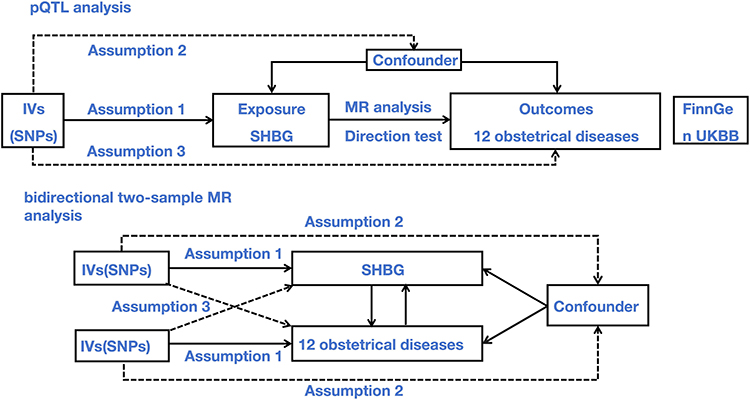 |
Figure 1 The flowchart of present study. The Mendelian randomization method is based on three hypotheses: assumption 1. instrumental variables are closely related to exposure; assumption 2. instrumental variables are independent of any confounding factor; assumption 3. instrumental variables affect the results only through exposure but not through other ways. Abbreviations: MR, Mendelian randomization; IV, Instrumental variable; SNP, single nucleotide polymorphism; SHBG, sex hormone binding globulin. |
Selection of Genetic Instruments
To decrease pleiotropy in the discovery analysis, we used existing cis-pQTLs (cis-protein abundance quantitative trait loci) as the representation for exposure, as they are more likely to directly control gene expression. Based on the deCODE study results, we obtained GWAS summary data for SHBG.18 We chose the most common cis-pQTLs SNPs with a minor allele frequency greater than 1% that showed a statistically significant link to SHBG expression in blood as instrumental factors. The SNPs were detected inside the 1 Mb region of the genetic transcription start location, which encodes the protein under investigation. To mitigate the effects of significant linkage disequilibrium (LD) on the obtained results, the study incorporated SNPs with low-weak LD (r²<0.1). Furthermore, the F-statistics need to be greater than 10 so that exposure traits are linked to instrumental strength. For the MR study, the correct information about cis-pQTLs was gathered, which included 23 single nucleotide polymorphisms (SNPs). Supplement Table 1 provides details on the 23 SNPs. Lastly, the pleiotropic SNPs that were related to other possible factors that could have changed the results were taken out of the data set considering their pleiotropic effects could have changed the results. This was done using the ldlink (https://ldlink.nih.gov/).
Outcome Sources
In our study, we limited the genetic origins of individuals to Europeans in order to prevent any potential bias resulting from varied populations. The data was downloaded from UK Biobank (UKBiobank HRC-imputed, http://www.nealelab.is/uk-biobank/) and FinnGen consortium https://www.finngen.fi/en). A total of 12 obstetrical disorders were investigated using the GWAS system, including gestational diabetes, single spontaneous delivery, excessive vomiting in pregnancy, hemorrhage in early pregnancy, postpartum depression, preterm labor, gestational hypertension, pre-eclampsia, intrahepatic cholestasis of pregnancy, placenta previa, postpartum hemorrhage and ectopic pregnancy, while there is on corresponding data for intrahepatic cholestasis of pregnancy in UK Biobank. And their selection was based on clinical burden, genetic data availability, and the necessity for mechanistic exploration.
MR Analysis
It was used the R software version 4.3.1 along with the “TwoSampleMR” package (version 0.5.7) and “MR PRESSO” package (version 1.0) to conduct all the statistical analyses.19 We used two different approaches to figure out the connections between the cis-pQTLs and the outcomes: the random-effects inverse variance weighted (IVW) method for a group of SNPs and the Wald ratio method for a single SNP. The study data were shown as odds ratios (ORs) and 95% confidence intervals (95% CIs), respectively.20 To cut down on the number of false positive results in our main study, we used the Benjamini-Hochberg method to figure out adjusted P-values and false discovery rate (FDR) corrections. In the MR analysis, a FDR of less than 5% was used as a significance level to check if the effect estimates were statistically significant. If the results did not pass the FDR test and had a theoretical P value of less than 0.05, we considered results to be suggestive of probable causality.21
Bayesian Colocalization Analysis
To determine whether the causal proteins discovered had comparable causal variations of SHBG and obstetrical disorders throughout the chromosomal region, a Bayesian colocalization analysis was conducted using the coloc package in the R software. This method aids in the elimination of any disruption caused by linkage disequilibrium.22 The following theories served as the foundation for the colocalization analysis: (i) H0: There is not a causative variation in the genomic area for exposure or result; (ii) H1: one causal variation that is significantly correlated with exposure alone; (iii) H2: one causal variant that is strongly correlated with outcome alone; (iv) H3: the presence of causative variations within the genomic region that are substantially correlated with exposure or outcome but are influenced by distinct causal variants; (v) H4: The same causal variation drives both exposure and result; (vi) H4/(H3+H4): the colocalization probability in the event that a causal variation for the result is present.22,23 Using default values, colocalization analysis of the indicated causative proteins was carried out (p1=1×10−4; p2=1×10−4; p12=1×10−5). The prior probabilities that were already mentioned were first recommended for pQTL analysis and should be used with care in hypothesis-driven research.24 If there is no evidence to support the colocalization, the posterior probabilities will be similar to the prior probabilities.
Robust Analysis
The Cochran’s Q test was used in the IVW technique to assess heterogeneity and validate the strength of the analytic findings.25 To determine horizontal pleiotropy,26 the MR-PRESSO and MR-Egger intercept techniques were applied. We utilized funnel plots to visually represent potential bias, with a symmetrical funnel indicating minimal bias. The MR-Egger regression was employed to detect the presence of horizontal pleiotropy, while the MR-PRESSO test27 (MR-pleiotropy residual sum and outlier approach) was utilized as an additional verification. Upon identifying outliers, the MR-PRESSO test evaluated whether there was a significant distortion in the data after removing these outliers. In order to evaluate how reliable the results were, a leave-one-out analysis was also performed. Through a methodical process of removing one SNP at a time, it was possible to see if the results were affected or guided by a specific SNP.28 In addition, we utilized the MR Steiger orientation analysis to validate the causal relationship between SHBG and obstetrical disorders.29
Results
Instrumental Characteristics
After conducting a screening process to define cis-pQTLs, a total of 23 instrumental variables were identified. These variables showed r2<0.1 with a 1 Mb and a statistically significant level of P<5×10−8. The MR analysis incorporated these variables and they are available in Supplement Table 1. The instruments of complements studied in this work have F-statistics>10, which suggests a low sensitivity to weak instrument bias.
Discovery Drug Target MR Analysis on SHBG with 12 Obstetrical Disorders
The drug target MR analysis identified a positive connection between specific obstetrical disorders and elevated expression of the SHBG gene in the bloodstream. The random effects IVW approach was mostly used to determine the causative association. In FinnGen consortium, SHBG gene represented obvious protective effect on gestational diabetes (OR[95%]=0.86[0.80–0.91], PFDR=1.75×10−5), single spontaneous delivery (OR[95%]=0.96[0.94–0.99], PFDR=8.53×10−3), excessive vomiting in pregnancy (OR[95%]=0.830[0.750–0.919], PFDR=1.36×10−3), hemorrhage in early pregnancy (OR[95%]=0.908[0.833–0.990], P=0.029), postpartum depression (OR[95%]=0.887[0.829–0.950], PFDR=1.72×10−3) and preterm labor (OR[95%]=0.800[0.740–0.865], PFDR=2.08×10−7), in the contrary with an increased risk of placenta previa (OR[95%]=1.304[1.083–1.570], PFDR=0.010) (Supplement Tables 2, 3 and Figure 2A). Within the UK Biobank consortium, the SHBG gene was linked to a lower probability of early pregnancy hemorrhage (OR[95%]=0.748[0.584–0.959], P=0.022), postpartum hemorrhage (OR[95%]=0.880[0.782–0.992], P=0.036), and ectopic pregnancy (OR[95%]=0.658[0.444–0.976], P=0.038). Conversely, there was a higher probability of a single spontaneous delivery (OR[95%]=1.315[1.138–1.520], PFDR=2.33×10−3), while the SHBG gene was associated with a decreased risk of these events (Supplement Tables 4, 5 and Figure 2B). The Cochrane Q statistics, MR-Egger intercept test (Supplement Table 6), and MR PRESSO test (Supplement Table 7) provided evidence that there was no significant variation in the data and no presence of horizontal pleiotropy in the IVW-MR analysis. In addition, the steiger directionality test did not provide any evidence of a reverse causal connection for the MR estimate (Supplement Table 8). We verified that SHBG and gestational diabetes are causally related (P_combined<0.05) using a meta-analysis (Supplement Table 9 and Figure 3).
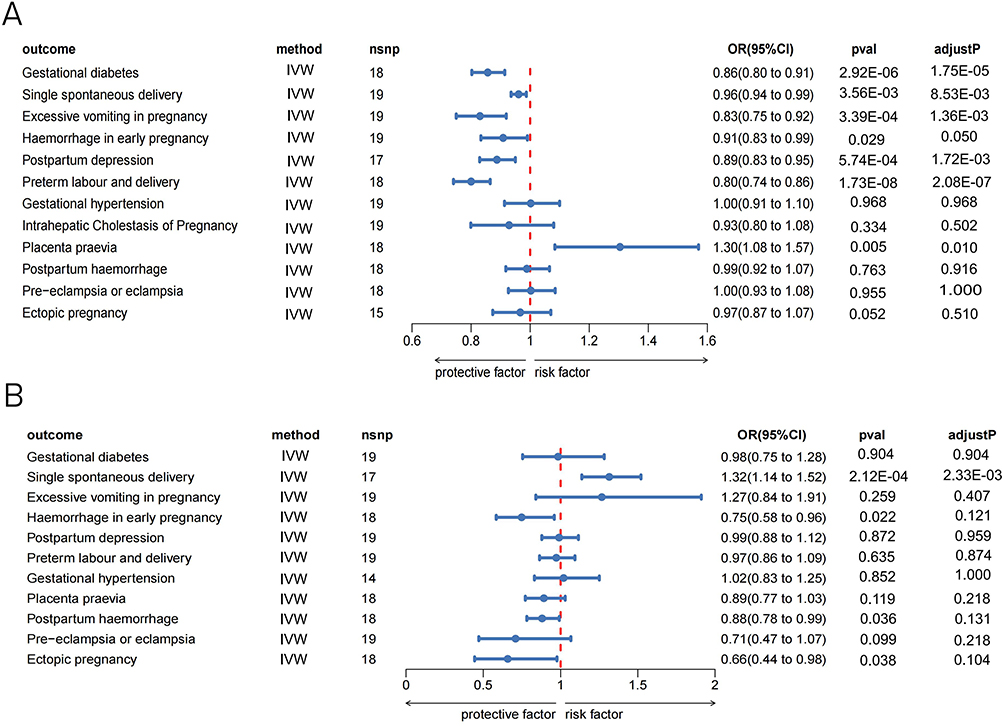 |
Figure 2 Forest plot of associations of SHBG and obstetrical disorders across FinnGen (A) and UK Biobank consortium (B). Abbreviations: SHBG, sex hormone binding globulin; IVW, inverse-variance weighted; OR, odds ratio; CI, confidence interval; SNP, single nucleotide polymorphism. |
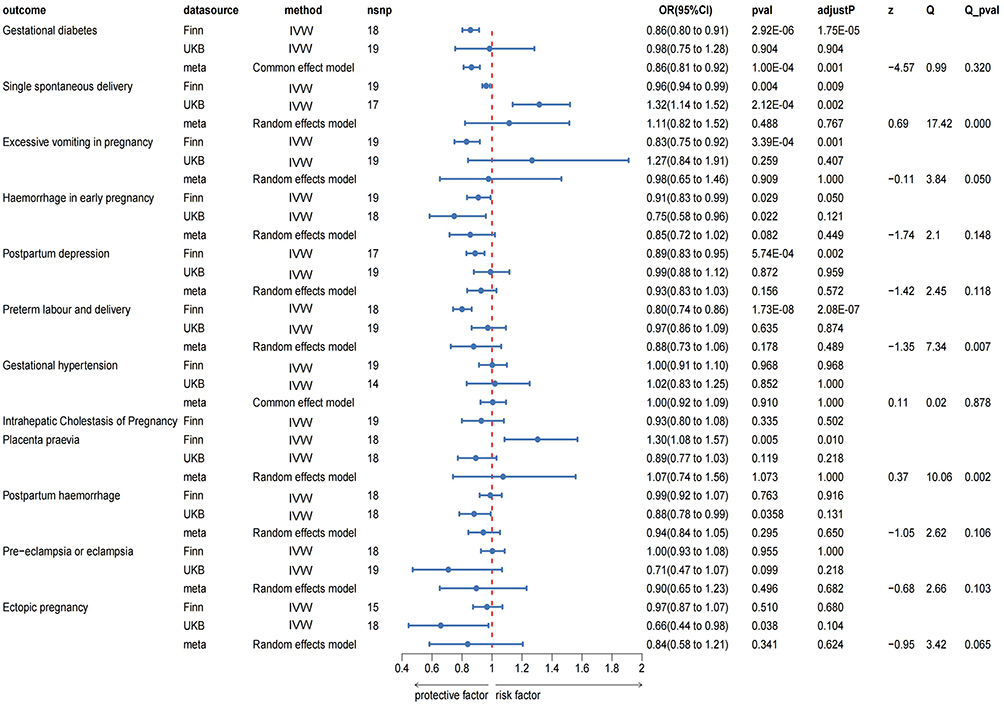 |
Figure 3 Forest plot of pQTL MR estimates in Discovery analysis. Abbreviations: MR, Mendelian randomization; SHBG, sex hormone binding globulin; IVW, inverse-variance weighted; OR, odds ratio; CI, confidence interval; SNP, single nucleotide polymorphism. |
Reverse MR Analysis in FinnGen Study
The reverse MR analysis was performed for SHBG with 12 obstetrical disorders. The threshold value was P<5×10−8, r2<0.001 with kb=10000. The random effects IVW-MR analysis was also found to suggest the increased expression of the SHBG gene associated with a decreased risk of gestational diabetes (OR[95%]=0.835[0.785–0.889], PFDR=2.03×10−7), excessive vomiting in pregnancy (OR[95%]=0.823[0.728–0.931], PFDR=5.94×10−3), gestational hypertension (OR[95%]=0.917[0.852–0.987], PFDR=0.041), hemorrhage in early pregnancy (OR[95%]=0.853[0.794–0.916], PFDR=6.90×10−5), ectopic pregnancy (OR[95%]=0.898[0.820–0.984], PFDR=0.036) and preterm delivery (OR[95%]=0.870[0.810–0.934], PFDR=4.47×10−4), while an increased risk of postpartum hemorrhage (OR[95%]=1.108[1.026–1.197], PFDR=0.022) (Supplement Table 10 and Figure 4A). The majority of them were in line with the findings of the analysis. The absence of statistical heterogeneity and horizontal pleiotropy in IVW-MR was demonstrated by the Cochrane Q statistics, the MR-Egger intercept test (Supplement Table 11), and the MR PRESSO test (Supplement Table 12). The reverse-direction MR analysis provided strong evidence indicating that individuals with an increased genetic predisposition to preterm delivery (Wald ratio: OR[95%]=0.881[0.839–0.926], PFDR=1.54×10−6) and single spontaneous delivery (random effects IVW: OR[95%]=0.937[0.901–0.974], PFDR=5.78×10−3) are more likely to the development of SHBG (Supplement Table 13 and Figure 4B).
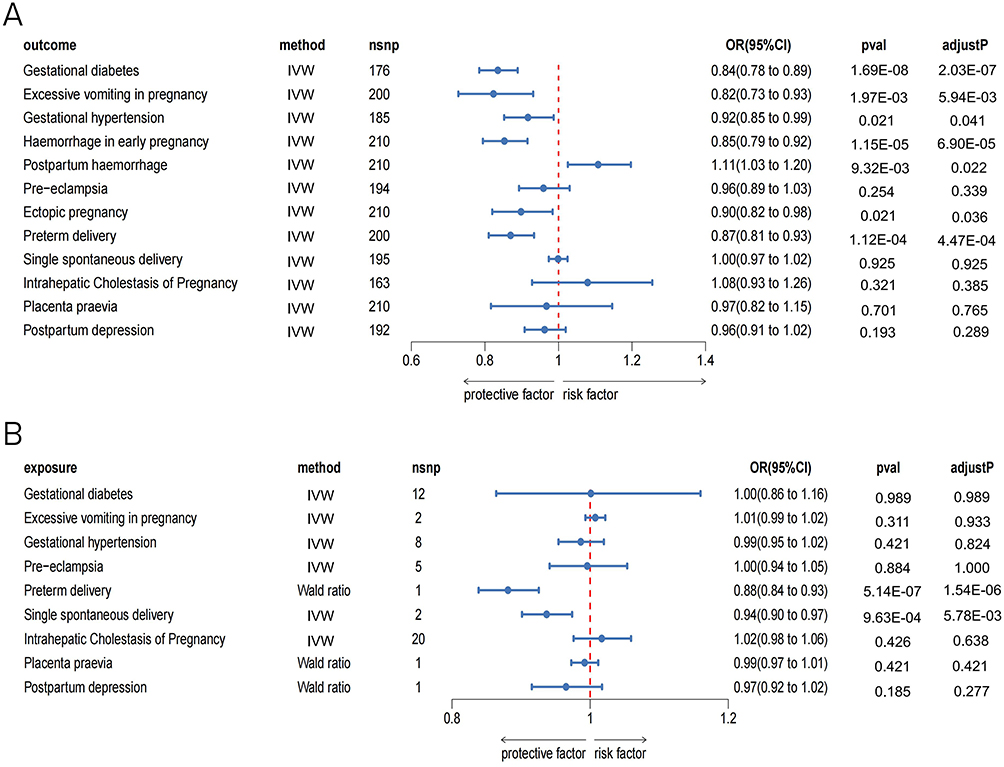 |
Figure 4 Forest plot of two-sample MR estimates in Replication analysis. (A) Positive-direction MR analysis (B) Reverse-direction MR analysis. Abbreviations: MR, Mendelian randomization; SHBG, sex hormone binding globulin; IVW, inverse-variance weighted; OR, odds ratio; CI, confidence interval; SNP, single nucleotide polymorphism. |
Bayesian Colocalization Analysis
In order to ensure the dependability of the two-sample MR findings, we conducted colocalization investigations. The objective of these investigations aimed to analyze the correlation between obstetrical disorders and potential targets indicated by SHBG. Our findings provide compelling evidence of shared genetic variations between the production of SHBG and the development of particular obstetrical disorders. Bayesian colocalization analysis demonstrated strong colocalization between SHBG and gestational diabetes, hemorrhage in early pregnancy, preterm labor and excessive vomiting in pregnancy in FinnGen database [H4/(H3+H4) = 99.2%, 86.9%, 95.8% and 86.1%, respectively] (Figure 5). In UK Biobank database, a strong colocalization between SHBG and postpartum hemorrhage was detected (Figure 6). The results indicated that causal genetic drivers were shared for SHBG and gestational diabetes, hemorrhage in early pregnancy, preterm delivery, excessive vomiting in pregnancy and postpartum hemorrhage. The whole results of colocalization were shown in Table 2.
 |
Table 2 Colocalization Results |
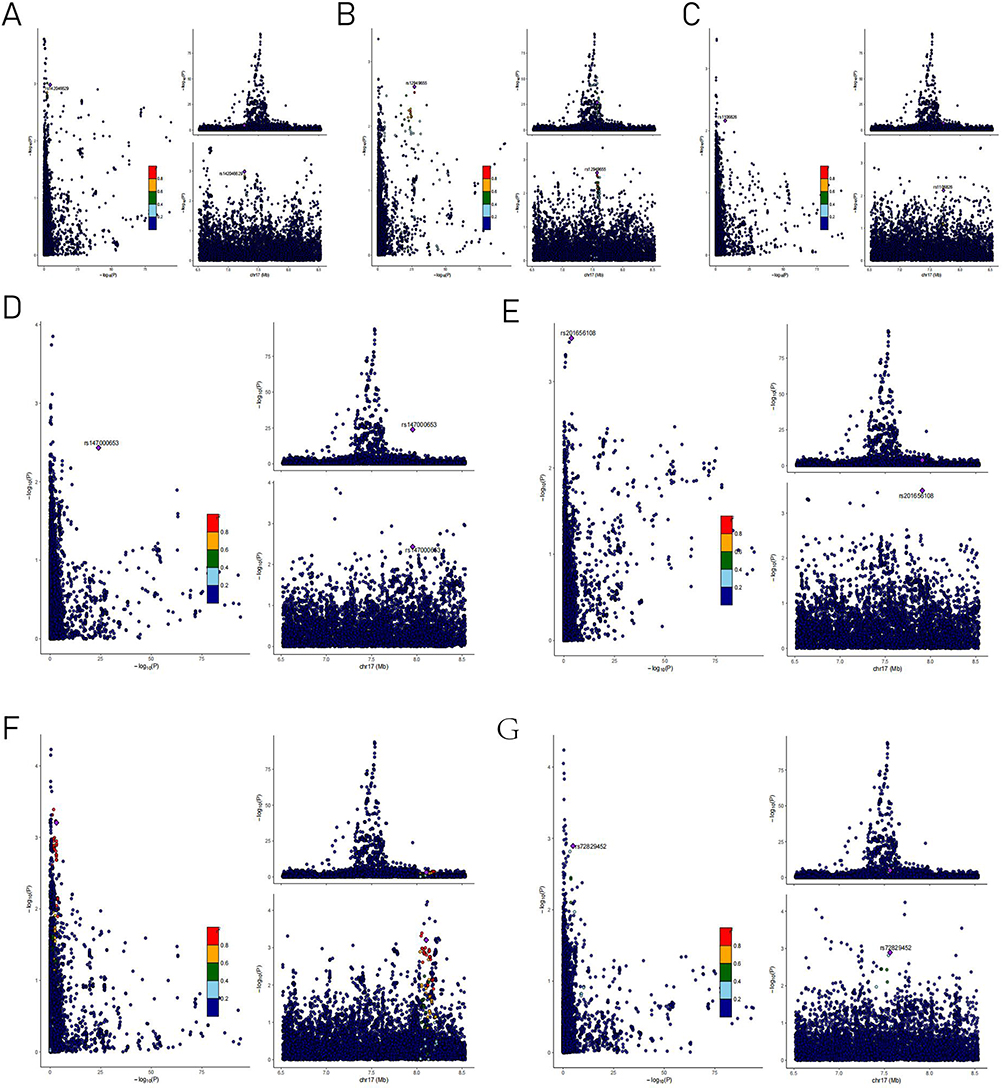 |
Figure 5 The results of the colocalization analysis in FinnGen consortium. LocusCompare plots of gestational diabetes (A), haemorrhage in early pregnancy (B), placenta praevia (C), postpartum depression (D), preterm labour (E), single spontaneous delivery (F), excessive vomiting in pregnancy (G). The purple diamond represents the target SNP (IV) in the colocalization analysis. All other SNPs are color coded according to the strength of linkage disequilibrium (as measured by r2) with this index SNP. Trait 1 represents the obstetrical disorders, and trait 2 represents the SHBG. Abbreviations: SNP, single nucleotide polymorphism; IV, instrumental variable; SHBG, sex hormone binding globulin. |
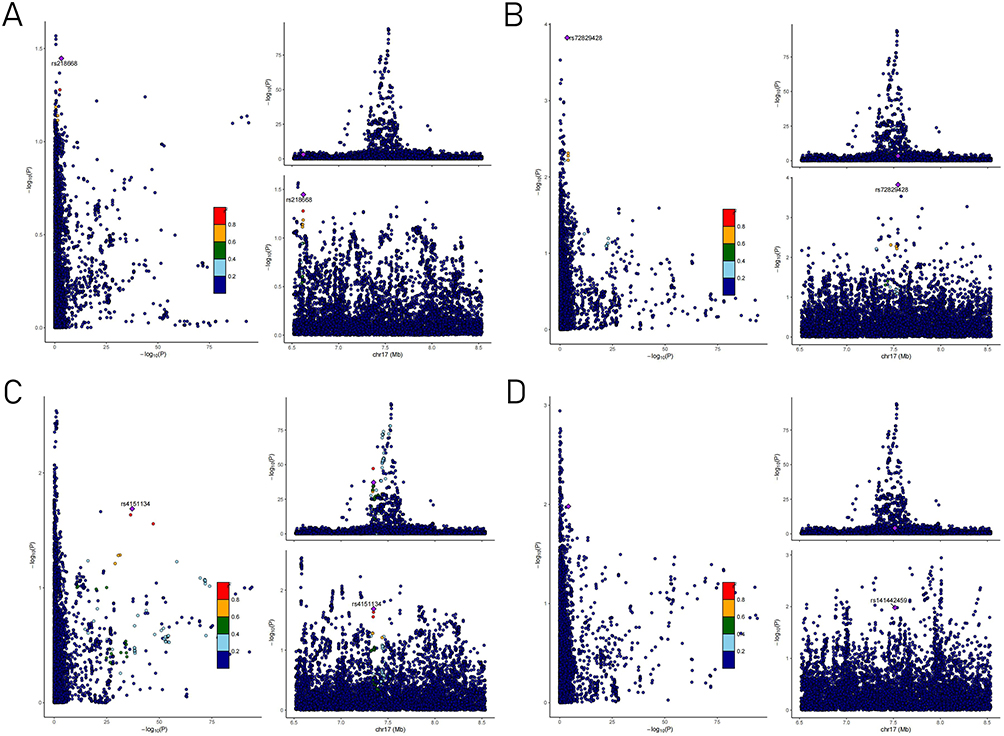 |
Figure 6 The results of the colocalization analysis in UK Biobank consortium. LocusCompare plots of single spontaneous delivery (A), postpartum haemorrhage (B), haemorrhage in early pregnancy (C), ectopic pregnancy (D). The purple diamond represents the target SNP (IV) in the colocalization analysis. All other SNPs are color coded according to the strength of linkage disequilibrium (as measured by r2) with this index SNP. Trait 1 represents the obstetrical disorders, and trait 2 represents the SHBG. Abbreviations: SNP, single nucleotide polymorphism; IV, instrumental variable; SHBG, sex hormone binding globulin. |
Discussion
This research employed a two-sample bidirectional Mendelian randomization study to comprehensively examine the potential causal connection between SHBG and the risk of 12 obstetrical disorders. Our findings demonstrated significant negative causal connection between SHBG and gestational diabetes, gestational hypertension, hyperemesis gravidarum, early hemorrhage pregnancy, and preterm delivery. Additionally, the COLOC analysis suggested that there may be a co-localized link between SHBG and the chances of getting gestational diabetes, hyperemesis gravidarum, early pregnancy hemorrhage, and preterm delivery.
Several observational studies have demonstrated an association between decreased levels of SHBG and an elevated risk of gestational diabetes.12,30 These findings support our research, indicating that low levels of SHBG may play a role in the development of gestational diabetes. This discovery further increases the study’s credibility in terms of genetic analysis. Recent research has revealed that SHBG is not only engaged in glucose metabolism via regulating sex hormone bioactivity, but it may also directly affect insulin signaling pathways and inflammatory responses via sex hormone-independent mechanisms. The fluctuations in endocrine hormone levels and placental factors during pregnancy render pregnant women particularly susceptible to insulin resistance, which ultimately results in elevated blood insulin levels and the onset of gestational diabetes.31 Nevertheless, there are several different routes involved in the intricate interaction between insulin resistance and SHBG. An investigation conducted by Feng et al32 demonstrated the correlation between placental SHBG and the signaling pathway known as phosphatidylinositol 3-kinase/protein kinase B (PI3K/AKT). The study proposed that SHBG may have an inhibitory impact on the PI3K/AKT signaling pathway, which is known to be linked to the emergence of insulin resistance and is also involved in the metabolic disturbances observed in gestational diabetes and reproductive dysfunction. While these concepts are biologically plausible, additional fundamental research is necessary to elucidate the exact mechanisms through which SHBG contributes to the onset of obstetric disorders. Additionally, Zhang et al33 conducted a study indicating that SHBG can impact insulin signaling pathways and glucose transporter proteins (GLUTs) in the placenta. This can result in a reduction in the absorption and utilization of glucose in the cells of the placenta, which in turn increases the likelihood of developing insulin resistance and gestational diabetes. Although these concepts are biologically sound, more research is needed to clarify the mechanism of SHBG’s role in the metabolic process of pregnancy, as well as early warning biomarkers of metabolic disorders in pregnancy, and to promote the development of individualized prevention and treatment protocols.
Expanding on the results of the previously mentioned investigation, Tang et al34 proceeded to examine the levels of SHBG in gestational diabetic patients with varying gestational outcomes. Their research uncovered a robust association between low levels of SHBG and the occurrence of preterm delivery in these patients, suggesting that SHBG could be a valuable predictor of preterm delivery. Further evidence, especially at the genetic level, is provided by the current study to support the hypothesis that SHBG levels and the risk of preterm delivery are directly correlated. Specifically, our research found that a decrease in SHBG production may increase the risk of preterm delivery in expectant mothers. However, given the current lack of understanding regarding the mechanisms underlying preterm delivery and the limited research on the association between SHBG and preterm delivery, it is essential for future studies to explore this issue to establish conclusive evidence. Preliminary analyses suggest several contributing factors. First, SHBG influences uterine stability during pregnancy by binding to free sex hormones (eg, testosterone, estradiol) and altering their bioactivity. When SHBG production is decreased, the bioavailability of free estradiol (E2) varies abnormally. High levels of E2 can increase uterine sensitivity and risk of preterm delivery by upregulating prostaglandin production (eg, PGF2α) in utero. Low levels of SHBG are linked to increased pro-inflammatory molecules including TNF-α and IL-6, which activate the NF-κB pathway. This promotes cervical ripening and premature membrane rupture, leading to preterm delivery. Thus, it is hypothesized that combining SHBG testing with other metabolic indicators in the clinic might offer an essential foundation for predicting and intervening in preterm delivery. The following studies should focus on the direct molecular mechanism of SHBG in preterm delivery, as well as targeted regulation techniques.
Furthermore, our investigation revealed that decreased levels of SHBG were associated with an elevated likelihood of developing gestational hypertension, which supports the conclusions of other prior observational studies.35,36 Zhang et al37 performed an investigation to investigate the correlation between genetic variants associated with the metabolism of sex hormones and angiogenic pathways, and the development of preeclampsia. Their research substantiated the notion that sex hormones do have an impact on the genetic progression of gestational hypertension. Gestational hypertension is caused by a number of causes, such as inadequate remodeling of spiral arteries, the presence of soluble fms-like tyrosine kinase 1 (sFlt1) and vascular endothelial growth factor (VEGF), oxidative stress in the placenta, and immunological dysregulation.38 Nevertheless, the exact mechanism linking SHBG to gestational hypertension remains unclear, necessitating further investigation. Hertig A et al39 demonstrated that sex hormones can suppress the placental inflammatory response associated with preeclampsia. Albrecht et al40 discovered that imbalances in estrogen and progesterone levels could lead to damage to placental endothelial cells and impaired placental function, ultimately leading to the onset of preeclampsia. It is clear that higher SHBG levels during pregnancy decrease free androgens and their damage to the vascular endothelium (eg, oxidative stress and inflammation), while retaining estrogen’s vasoprotective effects (eg, nitric oxide generation). If SHBG levels are inadequate, increasing free androgens may worsen endothelial dysfunction and encourage the development of preeclampsia. In contrast, the study conducted by Lin et al41 did not find any potential cause-and-effect relationship between SHBG levels and preeclampsia, nor with primary hypertension that complicates preeclampsia, through MR analysis. In early pregnancy, a significant increase in estrogen levels stimulates SHBG synthesis, which in turn decreases free androgen levels. If SHBG levels are insufficient, it may lead to an increase in free testosterone, which in turn induces gastrointestinal smooth muscle spasms and delayed gastric emptying, aggravating the symptoms of nausea and vomiting. In addition, low levels of SHBG exacerbate physiologic insulin resistance during pregnancy, leading to disturbances in glucose metabolism and accelerated lipolysis, increased production of ketone bodies, and triggering metabolic acidosis, which can also aggravate vomiting and dehydration. However, there is still a lack of evidence at the genetic level regarding the relationship between SHBG and excessive vomiting during pregnancy. Therefore, in the future, it is necessary to focus on the molecular interaction mechanism between SHBG and key hormones, and construct a precise intervention program based on SHBG gene polymorphisms and targeted therapy. Thus, the connection between SHBG and gestational hypertension remains uncertain, and more studies into SHBG’s interaction with important pathways (eg, sFlt-1/VEGF imbalance) and clinical translational potential is needed.
Our study identified a direct association between reduced SHBG production and the risk of experiencing hyperemesis gravidarum, as determined by MR analysis. Recent studies have mainly concentrated on the hormonal changes occurring during pregnancy and their connection to excessive vomiting, resulting in a scarcity of genetic-level evidence. Sex hormones are essential in controlling SHBG levels, it is necessary to be aware of that.42 The impact that sex hormones have on gastrointestinal function has been validated by a few research studies. In particular, it has been demonstrated that progesterone and estrogen, in particular, block the gastrointestinal tract’s smooth muscle from contracting, which lowers gastrointestinal motility.43 This decrease in motility can contribute to the onset of nausea and vomiting.44 Furthermore, a favorable link has been demonstrated between elevated testosterone levels and the incidence of excessive vomiting during pregnancy.45,46 In early pregnancy, a significant increase in estrogen levels boosts SHBG production, which reduces free androgens. If SHBG levels are inadequate, it may result in an increase in free testosterone, which causes gastrointestinal smooth muscle spasms and delayed stomach emptying, exacerbating nausea and vomiting. Furthermore, low levels of SHBG enhance physiologic insulin resistance during pregnancy, causing disruptions in glucose metabolism and accelerated lipolysis, increased generation of ketone bodies, and metabolic acidosis, which may exacerbate vomiting and dehydration. However, there is currently a lack of genetic evidence supporting the connection between SHBG and hyperemesis gravidarum. Thus, further research should concentrate on the molecular interaction mechanism between SHBG and crucial hormones, as well as the development of a precise intervention program based on SHBG gene polymorphisms and targeted treatment.
Hemorrhage in early pregnancy is a common cause of miscarriage caused by premature abortion.47 The situation not only intensifies the emotional burden and monetary pressure that pregnant women endure, but it also elevates the chances of encountering pregnancy-related complications, undesirable pregnancy outcomes, and a less promising prognosis for the fetus. It is a multifaceted challenge that demands attention and support in order to mitigate its potentially devastating consequences.48 Existing research underscores a profound linkage between aberrant sex hormone levels encountered during pregnancy and the emergence of premature abortion. Furthermore, these hormone concentrations possess the potential to act as a prognostic indicator, to a certain extent, for predicting the outcomes of pregnancies. This suggests that monitoring sex hormone levels in pregnant women can offer crucial insights into their risk of premature abortion and, thereby, assist in the development of preventive strategies.49 Our comprehensive probe has definitively established that a genetic-level decrement in the production of SHBG can substantially augment the chances of encountering hemorrhage during the initial stages of pregnancy. The underlying mechanisms leading to early pregnancy hemorrhage are indeed complex, encompassing a wide array of potential causes, which frequently encompass chromosomal variations in the couple and embryo, anatomical intricacies within the reproductive system, endocrine imbalances in the mother, infectious factors, and immune-mediated factors.50 A comprehensive study delving into the intricate correlation between sex hormone metabolism and premature abortion has unveiled a compelling finding: a considerable reduction in serum progesterone levels contributes significantly to an intensified rejection of placental trophoblast cell by the mother’s immune system. Subsequently, this immune response results in a robust and pronounced rejection of fetal antigens by the maternal immune system, thereby substantially elevating the chances of a future abortion.51
Finally, the current study found that genetically predicted high levels of SHBG were significantly associated with placenta praevia and an increased risk of postpartum hemorrhage, contradicting SHBG’s protective role in other obstetric conditions (eg, gestational diabetes, preterm delivery). There is a lack of research in this area, and this paradox may be due to the body’s pathological state-driven elevation of SHBG, where placenta praevia or underlying placental dysfunction may trigger a localized ischemic-hypoxic or inflammatory response (eg, elevation of IL-6, TNF-α), which stimulates compensatory hepatic increases in SHBG synthesis to bind excess free estrogen and attenuate vascular endothelial damage. The SHBG directly affects angiogenesis and coagulation, and it may disrupt placental spiral artery remodeling by binding to and blocking the action of pro-angiogenic molecules (eg, VEGF, FGF2), resulting in incorrect placental implantation (placenta previa). Also, SHBG may directly regulate angiogenesis and coagulation by competing with estrogen and reducing free estrogen’s ability to promote the synthesis of coagulation factors (eg, fibrinogen, plasminogen), resulting in a relative inhibition of coagulation and an increased risk of postpartum hemorrhage. Based on the above conjecture, more experiments and clinical data are needed for future studies to explore the causal relationship and interaction between the two.
Limitation of This Study
This comprehensive investigation, which was conducted among a European population, establishes a basis for understanding a particular incident. Nevertheless, it is imperative to conduct further research to ascertain the generality of these findings and determine whether they hold true for diverse populations spanning the globe, especially in other countries. Currently, the GWAS statistics accessible in diverse databases tend to be broadly defined and lack fundamental demographic details like age brackets and gender breakdowns. Consequently, this poses challenges in conducting further subgroup evaluations, necessitating the compilation of GWAS data on a significantly larger scale for subsequent investigative endeavors.
Conclusions
Our study revealed negative causal connections between SHBG levels and several obstetrical disorders, including gestational diabetes, gestational hypertension, hyperemesis gravidarum, hemorrhage in early pregnancy, and preterm delivery, providing genetic evidence for a causal connection. Furthermore, we have identified obstetrical disorders that include gestational diabetes, hemorrhage in early pregnancy, preterm delivery, and hyperemesis gravidarum that may share SHBG-associated genetic driving mechanisms, providing evidence for the use of SHBG as a genetic risk marker for obstetric disorders. Thus, further studies should concentrate on the molecular mechanism and clinical translation, combining basic research and clinical data analysis to create an integrated framework of “mechanism - prediction - intervention” to promote accurate prediction and individualized treatment of SHBG in obstetric disorders, ultimately improving maternal and infant health outcomes.
Data Sharing Statement
The data generated in the present research can be accessed in the main text or supplementary materials.
Ethics Approval and Consent to Participate
This study exclusively utilized publicly available summary-level GWAS data and did not require access to any individual-level data, thus no ethical approval or informed permission was required. This study was excluded from approval according to the Chinese Measures for Ethical Review of Life Science and Medical Research Involving Human Beings, Article 32, Item 1 and 2, which went into effect on February 18, 2023.
Acknowledgment
We would like to thank the database for making GWAS data available to the public.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Project approved by the Ministry of Industry and Information Technology of the People’s Republic of China and the National Healthcare Commission for the 5G + Medical and Healthcare Application Pilot Project (Project Name: 5G + Maternal and Child Health Service and Management, JKZX2022-5G03).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384(17):1635–1645. doi:10.1056/NEJMra1513247
2. Jiang L, Tang K, Magee LA, et al. A global view of hypertensive disorders and diabetes mellitus during pregnancy. Nat Rev Endocrinol. 2022;18(12):760–775. doi:10.1038/s41574-022-00734-y
3. Daru J, Zamora J, Fernández-Félix BM, et al. Risk of maternal mortality in women with severe anaemia during pregnancy and post partum: a multilevel analysis. Lancet Glob Health. 2018;6(5):e548–e554. doi:10.1016/S2214-109X(18)30078-0
4. Rana S, Lemoine E, Granger JP, Karumanchi SA. Preeclampsia: pathophysiology, challenges, and perspectives. Circ Res. 2019;124(7):1094–1112. doi:10.1161/CIRCRESAHA.118.313276
5. Turbeville HR, Sasser JM. Preeclampsia beyond pregnancy: long-term consequences for mother and child. Am J Physiol Renal Physiol. 2020;318(6):F1315–f1326. doi:10.1152/ajprenal.00071.2020
6. Xu X, Ding Y. Impact of obstetric disorders on maternal and fetal health: current Perspectives. J Matern Fetal Neonatal Med. 2023;36(1):129–140.
7. Yc X, Li J, Zhang Y. Incidence of maternal pregnancy complications and their influencing factors in China. Int J Obstet Gynaecol. 2023;50(3).
8. Hammond GL, Wu TS, Simard M. Evolving utility of sex hormone-binding globulin measurements in clinical medicine. Curr Opin Endocrinol Diabetes Obes. 2012;19(3):183–189. doi:10.1097/MED.0b013e328353732f
9. Liu W, Huang Z, Tang S, Zhang Z, Yu Q, He J. Changes of serum sex hormone-binding globulin, homocysteine, and hypersensitive CRP levels during pregnancy and their relationship with gestational diabetes mellitus. Gynecol Obstet Invest. 2021;86(1–2):193–199. doi:10.1159/000515085
10. Li MY, Rawal S, Hinkle SN, et al. Sex hormone-binding globulin, cardiometabolic biomarkers, and gestational diabetes: a longitudinal study and meta-analysis. Matern Fetal Med. 2020;2(1):2–9. doi:10.1097/FM9.0000000000000037
11. Yin MQ, Wang YX, Zhu XQ, Qian J, Hu XL. Relationship and predictive value of serum endolipin and sex hormone-binding globulin expression in gestational diabetes mellitus patients with disease and pregnancy outcome. Chin J Fam Plann. 2022;30(5):1128–1132.
12. Choudhury AA, Devi Rajeswari V. Gestational diabetes mellitus - A metabolic and reproductive disorder. Biomed Pharmacother. 2021;143:112183. doi:10.1016/j.biopha.2021.112183
13. McElduff A, Hitchman R, McElduff P. Is sex hormone-binding globulin associated with glucose tolerance? Diabet Med. 2006;23(3):306–312. doi:10.1111/j.1464-5491.2005.01780.x
14. Ligthelm RJ, Borzì V, Gumprecht J, Kawamori R, Wenying Y, Valensi P. Importance of observational studies in clinical practice. Clin Ther. 2007;29(6 Pt 1):1284–1292. doi:10.1016/j.clinthera.2007.07.004
15. Sanderson E, Glymour MM, Holmes MV. Mendelian randomization. Nat Rev Method Primers. 2022;2(1):6. doi:10.1038/s43586-021-00092-5
16. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
17. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
18. Ferkingstad E, Sulem P, Atlason BA, et al. Large-scale integration of the plasma proteome with genetics and disease. Nat Genet. 2021;53(12):1712–1721. doi:10.1038/s41588-021-00978-w
19. Hemani G, Zheng J, Elsworth B, et al. The MR-base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408.
20. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
21. Shi X, Wei T, Hu Y, Wang M, Tang Y. The associations between plasma soluble trem1 and neurological diseases: a Mendelian randomization study. J Neuroinflammation. 2022;19(1):218. doi:10.1186/s12974-022-02582-z
22. Giambartolomei C, Vukcevic D, Schadt EE, et al. Bayesian test for colocalisation between pairs of genetic association studies using summary statistics. PLoS Genet. 2014;10(5):e1004383. doi:10.1371/journal.pgen.1004383
23. Zhao SS, Yiu ZZN, Barton A, Bowes J. Association of lipid-lowering drugs with risk of psoriasis: a Mendelian randomization study. JAMA Dermatol. 2023;159(3):275–280. doi:10.1001/jamadermatol.2022.6051
24. Wallace C. Eliciting priors and relaxing the single causal variant assumption in colocalisation analyses. PLoS Genet. 2020;16(4):e1008720. doi:10.1371/journal.pgen.1008720
25. Tan JS, Liu NN, Guo TT, Hu S, Hua L. Genetically predicted obesity and risk of deep vein thrombosis. Thromb Res. 2021;207:16–24. doi:10.1016/j.thromres.2021.08.026
26. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
27. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
28. Emdin CA, Khera AV, Kathiresan S. Mendelian randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
29. Hemani G, Tilling K, Davey Smith G. Orienting the causal relationship between imprecisely measured traits using GWAS summary data. PLoS Genet. 2017;13(11):e1007081. doi:10.1371/journal.pgen.1007081
30. Bruno B, Blessing MK, Izuchukwu MN, Terry GT, Faeren D. Sex hormone-binding globulin is a valuable diagnostic indicator of gestational diabetes mellitus. Ghana Med J. 2024;58(1):53–59. doi:10.4314/gmj.v58i1.8
31. Corcoran SM, Achamallah N, Loughlin JO, et al. First trimester serum biomarkers to predict gestational diabetes in a high-risk cohort: striving for clinically useful thresholds. Eur J Obstet Gynecol Reprod Biol. 2018;222:7–12. doi:10.1016/j.ejogrb.2017.12.051
32. Feng C, Jin Z, Chi X, et al. SHBG expression is correlated with PI3K/AKT pathway activity in a cellular model of human insulin resistance. Gynecol Endocrinol. 2018;34(7):567–573. doi:10.1080/09513590.2017.1411474
33. Zhang B, Jin Z, Sun L, et al. Expression and correlation of sex hormone-binding globulin and insulin signal transduction and glucose transporter proteins in gestational diabetes mellitus placental tissue. Diabet Res Clin Pract. 2016;119:106–117. doi:10.1016/j.diabres.2016.07.003
34. Tang Y, Deng X, Chen YL. Construction of a risk model for preterm delivery in gestational diabetes mellitus based on Irisin, Kisspeptin and SHBG and its validation. J Southeast Univer. 2023;42(06):813–819.
35. Fan L. Study on the Relationship Between Serum Sex Hormone Binding Globulin and Insulin Resistance in Patients with Preeclampsia. Dalian: Dalian Medical University; 2007.
36. Gao LN, Chen MX, Zhan YQ. Value of serum T, SHBG, CRP, and BTP tests in predicting hypertensive disorders of pregnancy in middle and late pregnancy. Chin J Fam Plann. 2018;26(12):1231–1234.
37. Zhang P. Study on the relationship between polymorphisms of genes related to sex hormone metabolism and angiogenic pathway and the development of preeclampsia. Shanxi Med Univer. 2018.
38. Park MN, Park KH, Lee JE, et al. The expression and activation of sex steroid receptors in the preeclamptic placenta. Int J Mol Med. 2018;41(5):2943–2951. doi:10.3892/ijmm.2018.3474
39. Hertig A, Liere P, Chabbert-Buffet N, et al. Steroid profiling in preeclamptic women: evidence for aromatase deficiency. Am J Obstet Gynecol. 2010;203(5):
40. Albrecht ED, Pepe GJ. Estrogen regulation of placental angiogenesis and fetal ovarian development during primate pregnancy. Int J Dev Biol. 2010;54(2–3):397–408. doi:10.1387/ijdb.082758ea
41. Lin CY, Chen JB, Zhao XM. Genetic causality of hyperandrogenaemia detection index and preeclampsia. J Sichuan Univer. 2024;55(3):566–573.
42. Caglar GS, Ozdemir ED, Cengiz SD, Demirtaş S. Sex-hormone-binding globulin early in pregnancy for the prediction of severe gestational diabetes mellitus and related complications. J Obstet Gynaecol Res. 2012;38(11):1286–1293. doi:10.1111/j.1447-0756.2012.01870.x
43. Al-Shboul OA, Nazzal MS, Mustafa AG, et al. Estrogen relaxes gastric muscle cells via a nitric oxide- and cyclic guanosine monophosphate-dependent mechanism: a sex-associated differential effect. Exp Ther Med. 2018;16(3):1685–1692. doi:10.3892/etm.2018.6406
44. Al-Shboul OA, Mustafa AG, Omar AA, et al. Effect of progesterone on nitric oxide/cyclic guanosine monophosphate signaling and contraction in gastric smooth muscle cells. Biomed Rep. 2018;9(6):511–516. doi:10.3892/br.2018.1161
45. Carlsen SM, Vanky E, Jacobsen G. Nausea and vomiting associate with increasing maternal androgen levels in otherwise uncomplicated pregnancies. Acta Obstet Gynecol Scand. 2003;82(3):225–228. doi:10.1034/j.1600-0412.2003.00008.x
46. Helseth R, Ravlo M, Carlsen SM, Vanky EE. Androgens and hyperemesis gravidarum: a case-control study. Eur J Obstet Gynecol Reprod Biol. 2014;175:167–171. doi:10.1016/j.ejogrb.2014.01.007
47. Harville EW, Wilcox AJ, Baird DD, Weinberg CR. Vaginal bleeding in very early pregnancy. Hum Reprod. 2003;18(9):1944–1947. doi:10.1093/humrep/deg379
48. Parker AL, Crnfa C. Assessment and management of vaginal bleeding in early pregnancy. Women’s Healthc. 2022;10(4):9–28.
49. Gong ZY, Xu YY. Interleukin-17 and pregnancy-related hormone levels in early pregnancy and adverse pregnancy. Chin J Fam Plann. 2021;29(12):2675–2678.
50. Trostian B, McCloughen A, Fethney J, Curtis K. Presentation trends, characteristics and outcomes for women with early pregnancy bleeding in the emergency department: a 10-year data linkage study. Aust N Z J Obstet Gynaecol. 2023;63(6):803–810. doi:10.1111/ajo.13733
51. Wang Y, Liu HL, Qing BL. Predictive value of serum estrone and estriol levels on pregnancy outcome in patients with preeclamptic abortion. Chin Fam Med. 2024;22(05):813–816.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.