Back to Journals » Clinical Ophthalmology » Volume 15
Cataract Surgery in Short Eyes, Including Nanophthalmos: Visual Outcomes, Complications and Refractive Results
Authors Yosar JC ![]() , Zagora SL, Grigg JR
, Zagora SL, Grigg JR ![]()
Received 22 October 2021
Accepted for publication 19 November 2021
Published 27 November 2021 Volume 2021:15 Pages 4543—4551
DOI https://doi.org/10.2147/OPTH.S344465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jason C Yosar,1,2 Sophia L Zagora,1,2 John R Grigg1,2
1Save Sight Institute, University of Sydney, Sydney, NSW, Australia; 2Sydney Eye Hospital, Sydney, NSW, Australia
Correspondence: Jason C Yosar
Sydney Eye Hospital, 8 Macquarie St, Sydney, NSW, 2000, Australia
Tel +61 413378661
Email [email protected]
Background: To report the visual outcomes, complications and refractive results of phacoemulsification surgery and intraocular lens implantation in a large series of adult patients with short and nanophthalmic eyes.
Methods: The records of all patients with axial length < 21.0 mm undergoing phacoemulsification with intraocular lens implantation at an adult teaching hospital were retrospectively reviewed. The main outcome measures were corrected distance visual acuity and refraction at 90 days after surgery and intra- and postoperative complications occurring during the follow-up period.
Results: A total of 71 eyes of 51 patients (median age 71 years, interquartile range 62– 75.5) were included. Surgery resulted in an improvement in corrected distance visual acuity in 53 eyes (74.6%) (95% confidence interval, logMAR 0.11– 0.29) and was logMAR 0.30 or better in 47 eyes (66.2%). Worsening of corrected distance visual acuity occurred in 9 eyes (12.7%). Median postoperative refractive error was − 0.75 dioptres. SRK/T and Kane formula were more accurate in predicting postoperative refraction than Barrett Universal II and Hoffer Q when based on mean absolute error (P < 0.005). Complications occurred in 18 eyes (25.4%). The most frequent complications were iris prolapse, Descemet’s membrane and/or endothelial trauma, transient severe corneal edema and cystoid macular edema. There was no statistically significant difference in complication rates between senior surgeons and senior trainees (P = 0.66).
Conclusion: Cataract surgery in short and nanophthalmic eyes is challenging with a higher complication rate than routine cataract surgery, but frequently results in good visual outcomes. Postoperative refractive outcomes are more difficult to predict in this cohort.
Keywords: cataract, phacoemulsification, nanophthalmos, refractive error
Introduction
Cataract surgery is challenging in short eyes, with increased complication rates and poorer postoperative refractive predictability. Short eyes include simple microphthalmos, complex microphthalmos, nanophthalmos and relative anterior microphthalmos.1–3 Simple or isolated microphthalmos is an eye shorter than the mean by two standard deviations (typically <21.0 mm) with a normal anterior chamber depth and scleral thickness and no anatomical malformations.2–4 Eyes with complex microphthalmos also have a short axial length and normal anterior chamber depth but have anatomical malformations such as anterior segment dysgenesis, chorioretinal colobomas, retinal dysplasia and persistent fetal vasculature.2 Eyes with relative anterior microphthalmos have a normal axial length but a shallow anterior chamber (<2.2 mm) and a small cornea (diameter <11.0 mm) with no other anatomical malformations.3,5 Nanophthalmos features a short axial length, possible smaller cornea (<11.0 mm), shallow anterior chamber and thickened choroid and sclera with no other anatomical malformations.6,7 A historical definition by Duke-Elder described nanophthalmic eyes containing two-thirds the normal volume with an axial length between 16.0 mm to 18.5 mm, moderate to high hypermetropia, shallow anterior chamber, iris convexity and occasional macular hypoplasia.1
Nanophthalmos and microphthalmos is diagnosed primarily by axial length, with cut-offs in the literature including <18.0 mm,8,9 <20.5 mm,10–12 and <21.0 mm.7,13,14 A globe measuring <21.0 mm represents an axial length shorter than average by two standard deviation values.4,14 In addition, scleral thickening or combined retinal-choroidal-scleral thickening is used as an additional diagnostic criterion in some studies.7,14,15
Nanophthalmos is a rare condition with a prevalence of 0.0009–0.017%.16,17 Genes associated with nanophthalmos include NNO1 on chromosome 11 and MFRP on 11q23.3 and autosomal dominant and recessive inheritance patterns may occur.18 Abnormal collagen arrangement in affected eyes leads to poor growth of the eye as well as a thickened but weak sclera, especially posteriorly,7,19 which impairs venous drainage through the vortex veins and may lead to uveal effusion.20,21 The lens has a normal morphology causing a crowding effect that shallows the anterior chamber and predisposes to angle-closure glaucoma.2 Furthermore, the lens increases in size and width with age, further narrowing the angle. Angle-closure glaucoma in nanophthalmic eyes is difficult to manage as laser peripheral iridotomy, medical and surgical treatment are all more challenging, associated with poorer outcomes and may not adequately control intraocular pressure (IOP).7,14,22
Cataract surgery in short eyes is surgically challenging with a higher risk of intra- and postoperative complications. In addition to the increased risk of uveal effusions, an increased risk of aqueous misdirection, cystoid macular edema, choroidal haemorrhage, vitreous haemorrhage, retinal detachment and corneal decompensation has been described.2,7,23 The eye is situated deeper in the orbit and often has poorer pupil dilation and the closer proximity of the iris to the cornea increases the risk of Descemet’s flaps, iris prolapse into the surgical wound and intraoperative corneal endothelial damage.2
Postoperative refraction is more difficult to predict in short eyes using current popular intraocular lens (IOL) formulae.10,24 Older generation formulae such as Hoffer Q, Holladay 1 and SRK/T use two variables (keratometry and axial length) while newer generation formulae such as Haigis, Holladay 2 and Barrett Universal II incorporate up to seven variables to produce greater predictive accuracy.25 Previous studies have suggested superiority of Hoffer Q, Holladay 2 and Haigis over SRK II and SRK/T in short axial lengths.23,26–28 Recently, the novel Kane formula has been demonstrated to be a very accurate IOL formula for short eyes.29–31
This study evaluates the visual outcomes and complications of phacoemulsification surgery in adult short eyes and nanophthalmic eyes at a single tertiary hospital. The secondary purpose is to compare the predicted postoperative refraction in these patients using Barrett Universal II, Hoffer Q, SRK/T and Kane formula.31,39
Materials and Methods
Ethics Committee approval from the South Eastern Sydney Local Health District Human Research Ethics Committee was obtained prior to commencing this retrospective study. The committee approved this study and classified it as a low-risk, retrospective study (HREC: 19/124). Permission was obtained from the dataset owner to use this information for the purposes of this research and all data were anonymised. This study was conducted in accordance with the Declaration of Helsinki.
Biometric measurements performed on 133 morphologically normal eyes with an axial length of two standard deviations shorter than the mean (ie, <21.0 mm) at an adult publicly funded tertiary eye hospital from 2010 to 2019 were included. Patients who did not undergo cataract surgery were excluded (42 eyes). Patients with incomplete medical records (eg, illegible records) or insufficient follow-up (minimum three months) were excluded (17 eyes). Patients who underwent concurrent planned procedures such as vitrectomy or corneal grafting with phacoemulsification surgery were excluded (3 eyes). A total of 71 eyes of 51 patients were included. In 13 of these eyes the postoperative refraction was inadequately recorded. These remaining 58 eyes were included for analysis of postoperative refractive outcomes.
Preoperative data collected from each patient included age, gender, axial length, anterior chamber depth, corneal power, previous or current ocular comorbidities, previous ocular surgical procedures, preoperative refraction (spherical equivalent), preoperative corrected distance visual acuity (CDVA) and preoperative intraocular pressure (IOP). The anaesthetic type, surgical technique, surgeon seniority, intraocular lens power and type, use of additional procedures, use of additional medications and intraoperative and immediate postoperative complications were recorded. “Transient severe corneal edema” was defined as corneal edema fully resolving spontaneously or with medical therapy. “Severe iritis” was defined as anterior chamber cells and/or flare grade >3+ as graded by the Standardization of Uveitis Nomenclature Working Group criteria.32 Postoperative data included CDVA, IOP and refraction (spherical equivalent) at three months after surgery as well as postoperative complications or need for further procedures during the follow-up period.
Visual acuity was measured in Snellen notation and converted to logMAR units for statistical analysis. Visual acuity of counting fingers, hand movements, light perception and no light perception were assigned values of 2.0, 2.3, 2.6 and 2.9, respectively, in line with previous studies.33,34 Biometric measurements were obtained from all patients using IOLMaster 500 or 700 (Carl Zeiss Meditec AG). IOP measurements were collected from all patients using an ICare rebound tonometer (Revenio Group Corporation). A 2.75 mm clear corneal incision was used in conjunction with phacoemulsification using an Infinity phacoemulsification system (Alcon Laboratories, Inc.). DuoVisc viscoelastic system was used in all cases (Alcon Laboratories, Inc.).
The implanted IOL power was used to calculate the predicted postoperative refractive error by four IOL formulae: Barrett Universal II, Hoffer Q, SRK/T and Kane formula. Hoffer Q and SRK/T calculations were performed on the IOLMaster, while Kane39 and Barrett Universal II40 calculations were performed on online calculators. The mean numerical error (defined as the actual postoperative spherical equivalent refraction minus the predicted postoperative spherical equivalent) was calculated. The mean absolute error (defined as the absolute value of the numerical error of the postoperative prediction error) was also calculated.
Data were managed using Excel (Microsoft Corp.) and statistical analysis was performed using Stata version 16 (StataCorp LLC). Preoperative CDVA and IOP were compared with postoperative CDVA and IOP at three months using a non-parametric procedure based on a similar principle to the Wilcoxon signed-rank test. As each patient can contribute either one or two measurements (ie one eye or both eyes), a clustering effect (repeated measures) was accounted. To correct for this effect, the analysis was based on the “minimum distance estimation” principle using a 95% confidence interval for the Von Mises percentile differences between values of a variable for the same patient before and after the intervention using a clustering option within the algorithm. 25% to 75% interquartile ranges (IQR) were reported in addition to medians. The difference in the mean numerical error and mean absolute error between different IOL formulae was analysed using the Friedman test. Post hoc multiple comparisons for significant Friedman tests were done by conducting a series of two sample Friedman tests, using a Bonferroni correction to adjust the overall significant level. To compare complication rates according to surgeon seniority, two-sample proportion tests adjusted for clustering were conducted. As multiple comparisons were conducted, a Bonferroni-adjusted p-value was used. A p-value <0.05 (or the relevant Bonferroni-adjusted p-value) was considered statistically significant. A Medline (PubMed) literature review combining the terms “nanophthalmos”, “microphthalmos” and “cataract” was performed.
Results
Patient Characteristics
Cataract surgery was performed on 71 eyes of 51 patients. The median age at surgery was 71 years (IQR: 62–75.5). The median axial length was 20.48 mm (IQR: 20.06–20.79 mm). The median preoperative CDVA was logMAR 0.48 (IQR: logMAR 0.30–0.88). Further preoperative data are summarised in Table 1. A total of 33 eyes (46.5%) had a history of glaucoma. This included 11 eyes (15.5%) with previous acute angle-closure crisis, 18 eyes (25.4%) with chronic angle-closure glaucoma, two eyes (2.8%) with pseudoexfoliation glaucoma and two eyes (2.8%) with open-angle glaucoma. Neodymium yttrium aluminium garnet (Nd: YAG) laser peripheral iridotomy (PI) was previously performed in 28 eyes (39.4%) and argon laser peripheral iridoplasty was previously performed in two eyes (2.8%). One eye (1.4%) had previously undergone trabeculectomy. No eyes had previously undergone laser refractive surgery. Concurrent ocular comorbidities affecting visual acuity other than glaucoma were present in 29 eyes (40.8%), with multiple non-glaucoma comorbidities occurring in three of these eyes. These comorbidities comprised amblyopia in 10 eyes (14.1%), age-related macular degeneration in six eyes (8.5%), retinal dystrophy in four eyes (5.6%), non-arteritic anterior ischaemic optic neuropathy in three eyes (4.2%), macular telangiectasia in three eyes (4.2%), diabetic macular edema in two eyes (2.8%) and Posner-Schlossman syndrome in one eye (1.4%).
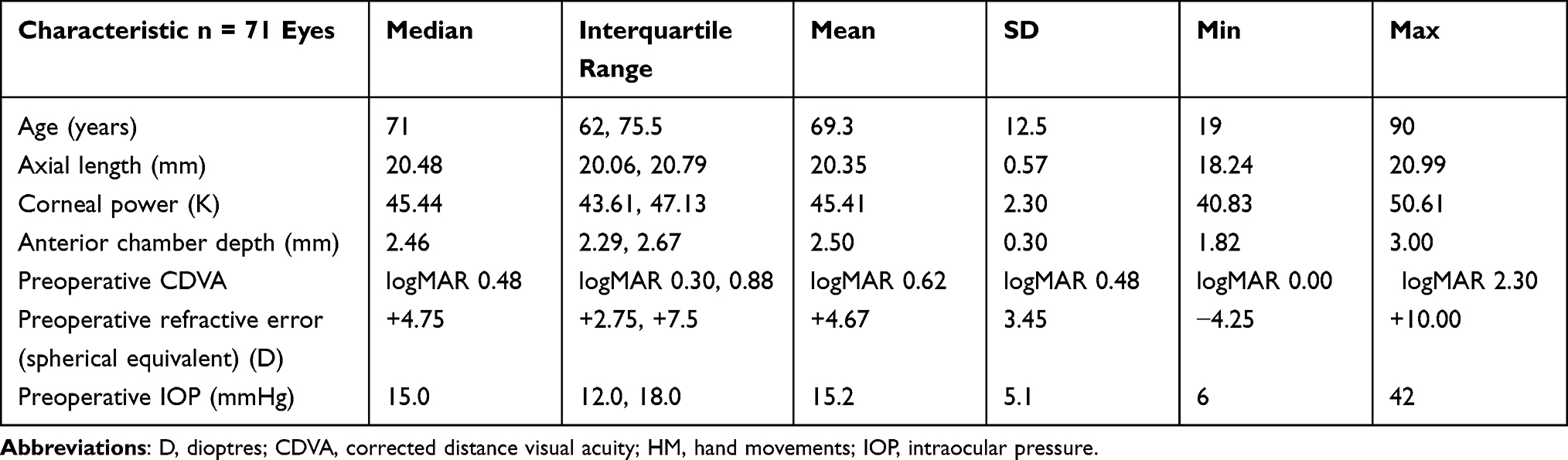 |
Table 1 Preoperative Patient Characteristics |
Surgery
All cases were performed under regional anaesthesia, which was administered by peribulbar injection in 58 eyes (81.7%) and subtenon injection in nine eyes (12.7%); anaesthetic type was not specified in four eyes (5.6%). Surgery was performed by a consultant (senior surgeon) in 20 cases (28.2%) and a senior trainee in 51 cases (71.8%). Phacoemulsification was performed in all cases. Additional surgical procedures included the use of hooks or rings for pupil expansion in eight eyes (11.3%), sclerostomy in three eyes (4.2%), synechiolysis in three eyes (4.2%), lateral canthotomy in two eyes (2.8%), unplanned pars plana vitrectomy and cryotherapy for a retinal tear in one eye (1.4%), unplanned anterior vitrectomy following zonular dehiscence in one eye (1.4%), injection of an anterior chamber air bubble following a Descemet membrane tear in one eye (1.4%), use of a capsular tension ring in one eye (1.4%), surgical iridectomy in one eye (1.4%) and use of an anterior chamber maintainer in one eye (1.4%).
An IOL was implanted into the capsular bag in 69 eyes (97.2%). The IOL was implanted into the ciliary sulcus in one eye (1.4%) due to an intraoperative posterior capsule defect. An IOL was not implanted in one eye (1.4%) due to intraoperative zonular dehiscence. A one-piece IOL was implanted in all eyes. The median IOL power was 31.0 D (IQR: 29.0–34.0 D).
Standard postoperative medication regimen for all patients consisted of topical antibiotics (chloramphenicol drops four times daily) and topical steroids (dexamethasone or prednisolone drops four times daily at the surgeon’s discretion) for four weeks beginning one day postoperatively. Additional intra- or postoperative medications included topical non-steroidal anti-inflammatory drugs (NSAIDs) (eg ketorolac) in 14 eyes (19.7%), oral acetazolamide in 13 eyes (18.3%), topical atropine in eight eyes (11.3%), intracameral phenylephrine in two eyes (2.8%), topical glycerol in one eye (1.4%), subconjunctival 5-fluorouracil injection in one eye (1.4%), orbital floor dexamethasone in one eye (1.4%) and topical hypertonic saline drops (NaCl 5%) in one eye (1.4%).
Visual Outcome
The median postoperative CDVA at three months was logMAR 0.30 (IQR: logMAR 0.18–0.48). This was a significant improvement on the preoperative CDVA (95% confidence interval [CI] for the median minimum distance estimation, logMAR 0.11–0.29). Table 2 shows the change in CDVA in Snellen lines at three months after surgery compared with the preoperative CDVA. Fifty-three eyes (74.6%) experienced improved vision postoperatively, while nine eyes (12.7%) experienced worse vision. Three eyes lost ≥3 Snellen lines. The cause of this was not identified in two eyes, and one eye was left aphakic due to intraoperative zonular dehiscence. Twenty-four eyes (33.8%) did not achieve a CDVA of logMAR 0.30 or better at three months after surgery. The cause of this was pre-existing ocular pathology limiting CDVA in 17 eyes (23.9%) and surgical complications in five eyes (7.0%). The surgical complications in these cases were corneal decompensation in two eyes, cystoid macular edema in two eyes and zonular dehiscence leading to aphakia in one eye. No cause for visual acuity worse than logMAR 0.30 was identified in two eyes (2.8%). Of these 24 eyes that did not achieve logMAR 0.30 or better postoperatively, 14 eyes (50%) still achieved improved vision compared to preoperatively, eight eyes (33.3%) experienced worse vision and two eyes (8.3%) had the same vision before and after surgery.
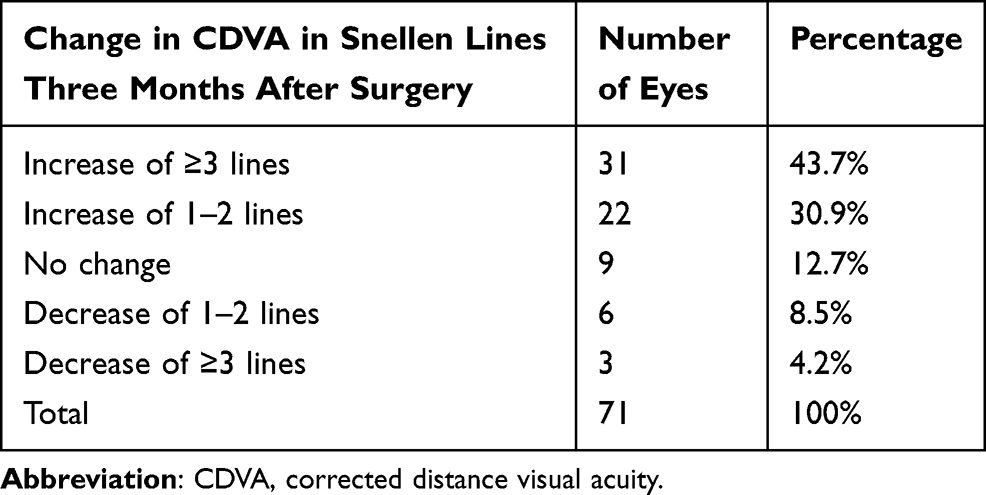 |
Table 2 Change in Corrected Distance Visual Acuity at Three Months After Surgery |
Table 3 summarises the CDVA pre- and post-operatively; two-thirds (66.2%) of eyes achieved logMAR 0.30 or better. The median postoperative IOP at three months was 12 mmHg (IQR: 10–14.75 mmHg, range 7–22 mmHg). This was a significant reduction on the preoperative IOP (95% CI for the median minimum distance estimation, 2–4).
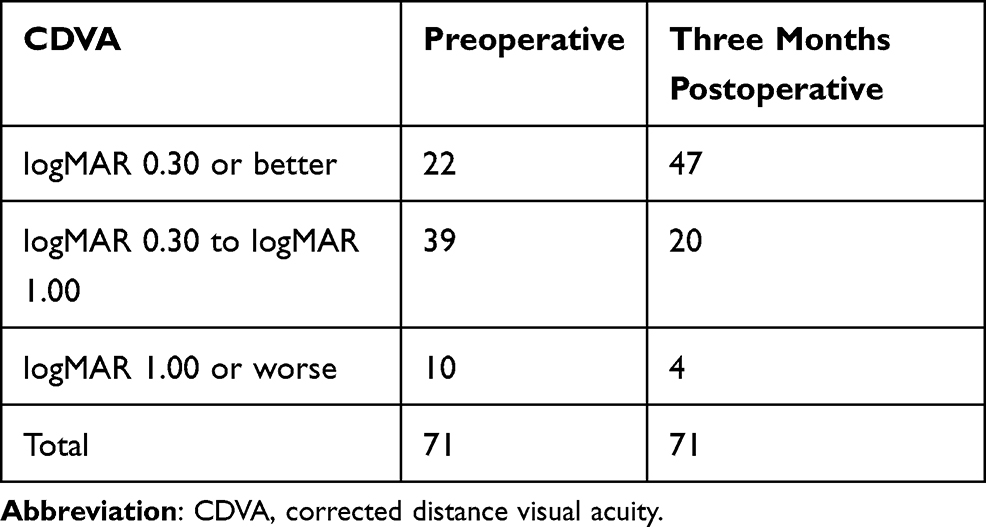 |
Table 3 Corrected Distance Visual Acuity Before and Three Months After Surgery |
Refractive Outcomes
Postoperative refraction was performed on 58 of 71 eyes. The median postoperative refraction of these eyes at three months was −0.75 D (IQR: −1.50 to 0.00 D). There was a tendency towards myopic shift in all four IOL formulae when based on mean numerical error (Table 4). After post hoc analysis, Kane produced the best refractive results followed by SRK/T based on mean numerical error; this was statistically significant (P < 0.005). There was no significant difference between Hoffer Q and Barrett Universal II based on mean numerical error (P = 0.22). The mean absolute error between the four IOL formulae as well as the proportion of eyes achieving within 0.5 dioptres and 1.0 dioptres of predicted postoperative refraction are also summarised in Table 4. Based on mean absolute error, Kane and SRK/T were significantly more accurate than Hoffer Q and Barrett Universal II (P < 0.005) but there was no significant difference between them (P = 0.95). There was also no statistically significant difference between Barrett Universal II and Hoffer Q when based on mean absolute error (P = 0.80). 43.1–62.1% of eyes achieved within 1.0 dioptre of predicted postoperative refraction (Figure 1), with SRK/T the most accurate of the four IOL formulae and Hoffer Q the least accurate. 39.7% of eyes achieved within 0.5 dioptres of predicted postoperative refraction using the Kane formula, the most accurate of the four tested.
 |
Table 4 Prediction Errors for Each Intraocular Lens Formula |
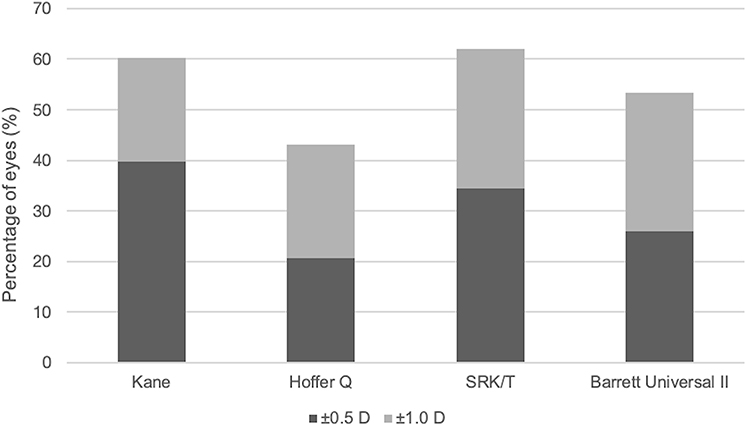 |
Figure 1 Percentage of eyes within 0.5 D and 1.0 D of predicted postoperative refraction using each of the four intraocular lens formulae. |
Complications
No complications occurred in 53 eyes (74.6%). Intra- and/or postoperative complications occurred in 18 eyes (25.4%), with more than one complication occurring in four of those 18 eyes. Iris prolapse, corneal endothelial and/or Descemet membrane trauma, transient severe corneal edema and cystoid macular edema (CME) occurred in 15 eyes (21.1%). Additional surgical interventions due to complications were required in three eyes (4.2%). The median CDVA at three months post-surgery in eyes with complications was logMAR 0.42 (IQR: logMAR 0.21–0.74). Nine (50%) of the 18 eyes with complications achieved a CDVA of logMAR 0.30 or better. No cases of uveal effusion, aqueous misdirection, acute angle-closure glaucoma, retinal detachment, suprachoroidal haemorrhage or endophthalmitis occurred. The difference in complication rates between trainees and consultants was not statistically significant (two-sample test of proportions, P = 0.66).
Discussion
This study evaluates the outcomes and complications of cataract surgery in adult short and nanophthalmic eyes using modern surgical techniques. It confirms that cataract surgery in this population is associated with a higher complication rate than in normal-length eyes but is safer than first reported. The median axial length in our cohort was 20.48 mm; Day et al associated an axial length of <20.5 mm with a four times higher odds of any complication.14 Complications occurred in 18 eyes (25.4%) in our cohort. In comparison, the two highest-powered previous studies evaluated 103 eyes and 43 eyes and demonstrated complication rates of 15.5%14 and 27.9%,12 respectively. No significant differences comparing complication rates by surgeon seniority were found in our study. The surgeon seniority in other published studies on this topic is either not identified, or confined to senior/experienced surgeons only.9,10,13–15
The most common complications in our cohort were iris prolapse, corneal endothelial and/or Descemet membrane trauma, transient severe corneal edema and cystoid macular edema (CME). No cases of CME occurred in conjunction with a posterior capsule defect. No cases of uveal effusion, angle-closure glaucoma, retinal detachment or aqueous misdirection occurred in our cohort; these severe complications have been frequently reported in cataract surgery in nanophthalmic eyes.8–10,12–15 Aqueous misdirection has been reported in 0.4% to 6.0% of cataract surgery in short eyes, occurring most commonly with primary angle closure, which often coexists in nanophthalmic eyes.35 Its risk of development is also higher in eyes shorter than 20.0 mm.14 Severe postoperative uveitis and posterior capsule rupture, two of the most common complications in the literature, only occurred once each in our cohort.
Improvement in CDVA occurred in 74.6% of our cohort. Pre-existing ocular comorbidities limited optimal postoperative CDVA in 17 eyes (23.9%).36,37 Severe visual loss (loss of ≥3 Snellen lines) occurred in three eyes (4.2%) in our cohort, with no explanation identified in two eyes, and a third due to aphakia following zonular dehiscence that was later corrected with a sutured IOL. There was a statistically significant improvement in IOP following surgery, supporting the role of cataract surgery in relieving anterior chamber narrowing in short eyes.
The median postoperative refraction in our cohort was −0.75 D, which is unusual in that most other studies have demonstrated hypermetropia after cataract surgery in nanophthalmic eyes.8,9,11,12 Only one other study in the literature demonstrates a mean myopic postoperative refraction in their cohort.13 Additionally, all four of the chosen IOL formulae in this study predicted a myopic shift based on mean numerical error. In our cohort, SRK/T was significantly more accurate than Hoffer Q and Barrett Universal II in predicting postoperative refraction when based on both mean numerical error and mean absolute error. This contrasts the results of Kane et al that demonstrated no statistically significant difference between seven IOL formulae for eyes shorter than 22.0 mm,25 as well as Narváez et al who demonstrated no differences between four IOL formulae in eyes <22.0 mm.38
Melles et al recently demonstrated the superiority of the Kane formula for short axial lengths.29 This conclusion is supported by our results when using mean numerical error only. When considering mean absolute error, the Kane formula outperformed Hoffer Q and Barrett Universal II but there was no statistically significant difference over SRK/T.
Previous studies have suggested superiority of Hoffer Q, Holladay 2 and Haigis over SRK II and SRK/T in short axial lengths when comparing lens formulae.23,26–28 We noted that the proportion of eyes achieving within 1.0 dioptre of predicted postoperative refraction in our cohort varied from 43.1% to 62.1%, with SRK/T the most accurate and Hoffer Q the least accurate. The number of nanophthalmic eyes achieving within 1.0 dioptre of predicted postoperative refraction in the literature ranges from 42.9% to 66.6%, a comparable figure to our cohort.10–13,28
The limitations of this study are the relatively short follow-up period of three months as well as the retrospective design. A longer follow-up period would be useful in assessing whether the reduction in IOP following surgery results in a reduced need for glaucoma medication in nanophthalmic glaucomatous eyes. Future studies may also evaluate the efficacy of pre-phacoemulsification procedures to deepen the anterior chamber (such as anterior vitrectomy) to prevent common complications such as iris prolapse and Descemet’s membrane trauma.
Conclusions
The majority of cases resulted in improved vision and were uncomplicated. Our results support recent studies that cataract surgery in short eyes including nanophthalmic eyes is safer than first reported.12–14 Challenges in short eye and nanophthalmic cataract surgery remain: complication rates are higher than in non-nanophthalmic eyes, and postoperative refraction is much more difficult to predict, even with the availability of multiple and new IOL formulae.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Ethics Committee approval from the South Eastern Sydney Local Health District Human Research Ethics Committee was obtained prior to commencing this retrospective study. The committee approved this study and classified it as a low-risk, retrospective study (HREC: 19/124). Permission was obtained from the dataset owner to use this information for the purposes of this research and all data were anonymised. This study was conducted in accordance with the Declaration of Helsinki.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Duke-Elder S. Anomalies in the size of the eye. Normal and abnormal development; congenital deformities. In: Duke-Elder S, editor. System of Ophthalmology. Vol. 3. London: Henry Kimpton; 1964:2.
2. Hoffman RS, Vasavada AR, Allen QB, et al. Cataract surgery in the small eye. J Cataract Refract Surg. 2015;41(11):2565–2575. doi:10.1016/j.jcrs.2015.10.008
3. Auffarth GU, Blum M, Faller U, Tetz MR, Volcker HE. Relative anterior microphthalmos: morphometric analysis and its implications for cataract surgery. Ophthalmology. 2000;107(8):1555–1560. doi:10.1016/S0161-6420(00)00240-2
4. Foster PJ, Broadway DC, Hayat S, et al. Refractive error, axial length and anterior chamber depth of the eye in British adults: the EPIC-Norfolk Eye Study. Br J Ophthalmol. 2010;94(7):827–830. doi:10.1136/bjo.2009.163899
5. Nihalani BR, Jani UD, Vasavada AR, Auffarth GU. Cataract surgery in relative anterior microphthalmos. Ophthalmology. 2005;112(8):1360–1367. doi:10.1016/j.ophtha.2005.02.027
6. Faucher A, Hasanee K, Rootman DS. Phacoemulsification and intraocular lens implantation in nanophthalmic eyes: report of a medium-size series. J Cataract Refract Surg. 2002;28(5):837–842. doi:10.1016/S0886-3350(01)01161-0
7. Wu W, Dawson DG, Sugar A, et al. Cataract surgery in patients with nanophthalmos: results and complications. J Cataract Refract Surg. 2004;30(3):584–590. doi:10.1016/j.jcrs.2003.07.009
8. Singh H, Wang JC, Desjardins DC, Baig K, Gagne S, Ahmed II. Refractive outcomes in nanophthalmic eyes after phacoemulsification and implantation of a high-refractive-power foldable intraocular lens. J Cataract Refract Surg. 2015;41(11):2394–2402. doi:10.1016/j.jcrs.2015.05.033
9. Zheng T, Chen Z, Xu J, Tang Y, Fan Q, Lu Y. Outcomes and prognostic factors of cataract surgery in adult extreme microphthalmos with axial length <18 mm or corneal diameter <8 mm. Am J Ophthalmol. 2017;184:84–96. doi:10.1016/j.ajo.2017.09.028
10. Jung KI, Yang JW, Lee YC, Kim SY. Cataract surgery in eyes with nanophthalmos and relative anterior microphthalmos. Am J Ophthalmol. 2012;153(6):1161–8 e1. doi:10.1016/j.ajo.2011.12.006
11. Lemos JA, Rodrigues P, Resende RA, Menezes C, Goncalves RS, Coelho P. Cataract surgery in patients with nanophthalmos: results and complications. Eur J Ophthalmol. 2016;26(2):103–106. doi:10.5301/ejo.5000656
12. Steijns D, Bijlsma WR, Van der Lelij A. Cataract surgery in patients with nanophthalmos. Ophthalmology. 2013;120(2):266–270. doi:10.1016/j.ophtha.2012.07.082
13. Carifi G, Safa F, Aiello F, Baumann C, Maurino V. Cataract surgery in small adult eyes. Br J Ophthalmol. 2014;98(9):1261–1265. doi:10.1136/bjophthalmol-2013-304579
14. Day AC, MacLaren RE, Bunce C, Stevens JD, Foster PJ. Outcomes of phacoemulsification and intraocular lens implantation in microphthalmos and nanophthalmos. J Cataract Refract Surg. 2013;39(1):87–96. doi:10.1016/j.jcrs.2012.08.057
15. Rajendrababu S, Babu N, Sinha S, et al. A randomized controlled trial comparing outcomes of cataract surgery in nanophthalmos with and without prophylactic sclerostomy. Am J Ophthalmol. 2017;183:125–133. doi:10.1016/j.ajo.2017.09.008
16. Shah SP, Taylor AE, Sowden JC, et al. Anophthalmos, microphthalmos, and typical coloboma in the United Kingdom: a prospective study of incidence and risk. Invest Ophthalmol Vis Sci. 2011;52(1):558–564. doi:10.1167/iovs.10-5263
17. Hu Z, Yu C, Li J, et al. A novel locus for congenital simple microphthalmia family mapping to 17p12-q12. Invest Ophthalmol Vis Sci. 2011;52(6):3425–3429. doi:10.1167/iovs.10-6747
18. Sundin OH, Dharmaraj S, Bhutto IA, et al. Developmental basis of nanophthalmos: MFRP Is required for both prenatal ocular growth and postnatal emmetropization. Ophthalmic Genet. 2008;29(1):1–9. doi:10.1080/13816810701651241
19. Stewart DH
20. Jackson TL, Hussain A, Salisbury J, Sherwood R, Sullivan PM, Marshall J. Transscleral albumin diffusion and suprachoroidal albumin concentration in uveal effusion syndrome. Retina. 2012;32(1):177–182. doi:10.1097/IAE.0b013e318218a95a
21. Brockhurst RJ. Nanophthalmos with uveal effusion. A new clinical entity. Arch Ophthalmol. 1975;93(12):1989–1999.
22. Yalvac IS, Satana B, Ozkan G, Eksioglu U, Duman S. Management of glaucoma in patients with nanophthalmos. Eye. 2008;22(6):838–843. doi:10.1038/sj.eye.6702742
23. Wladis EJ, Gewirtz MB, Guo S. Cataract surgery in the small adult eye. Surv Ophthalmol. 2006;51(2):153–161. doi:10.1016/j.survophthal.2005.12.005
24. Day AC, Foster PJ, Stevens JD. Accuracy of intraocular lens power calculations in eyes with axial length <22.00 mm. Clin Exp Ophthalmol. 2012;40(9):855–862. doi:10.1111/j.1442-9071.2012.02810.x
25. Kane JX, Van Heerden A, Atik A, Petsoglou C. Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refract Surg. 2016;42(10):1490–1500. doi:10.1016/j.jcrs.2016.07.021
26. Hoffer KJ. Clinical results using the Holladay 2 intraocular lens power formula. J Cataract Refract Surg. 2000;26(8):1233–1237. doi:10.1016/S0886-3350(00)00376-X
27. Gavin EA, Hammond CJ. Intraocular lens power calculation in short eyes. Eye. 2008;22(7):935–938. doi:10.1038/sj.eye.6702774
28. Carifi G, Aiello F, Zygoura V, Kopsachilis N, Maurino V. Accuracy of the refractive prediction determined by multiple currently available intraocular lens power calculation formulas in small eyes. Am J Ophthalmol. 2015;159(3):577–583. doi:10.1016/j.ajo.2014.11.036
29. Melles RB, Kane JX, Olsen T, Chang WJ. Update on Intraocular Lens Calculation Formulas. Ophthalmology. 2019;126(9):1334–1335. doi:10.1016/j.ophtha.2019.04.011
30. Connell BJ, Kane JX. Comparison of the Kane formula with existing formulas for intraocular lens power selection. BMJ Open Ophthalmol. 2019;4(1):e000251. doi:10.1136/bmjophth-2018-000251
31. Darcy K, Gunn D, Tavassoli S, Sparrow J, Kane JX. Assessment of the accuracy of new and updated intraocular lens power calculation formulas in 10 930 eyes from the UK National Health Service. J Cataract Refract Surg. 2020;46(1):2–7. doi:10.1016/j.jcrs.2019.08.014
32. Abs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516.
33. Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. Resolving the clinical acuity categories “hand motion” and “counting fingers” using the Freiburg Visual Acuity Test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):137–142. doi:10.1007/s00417-008-0926-0
34. Tomkins-Netzer O, Talat L, Bar A, et al. Long-term clinical outcome and causes of vision loss in patients with uveitis. Ophthalmology. 2014;121(12):2387–2392. doi:10.1016/j.ophtha.2014.07.007
35. Shahid H, Salmon JF. Malignant glaucoma: a review of the modern literature. J Ophthalmol. 2012;2012:852659.
36. Walsh MK, Goldberg MF. Abnormal foveal avascular zone in nanophthalmos. Am J Ophthalmol. 2007;143(6):1067–1068. doi:10.1016/j.ajo.2007.01.051
37. Bijlsma WR, van Schooneveld MJ, Van der Lelij A. Optical coherence tomography findings for nanophthalmic eyes. Retina. 2008;28(7):1002–1007. doi:10.1097/IAE.0b013e31816d400c
38. Narvaez J, Zimmerman G, Stulting RD, Chang DH. Accuracy of intraocular lens power prediction using the Hoffer Q, Holladay 1, Holladay 2, and SRK/T formulas. J Cataract Refract Surg. 2006;32(12):2050–2053. doi:10.1016/j.jcrs.2006.09.009
39. Kane J. Kane formula. Available from: https://www.iolformula.com/.
40. Barrett GD. Barrett Universal II Formula. Singapore, Asia-Pacific Association of Cataract and Refractive Surgeons. Available from: http://calc.apacrs.org/barrett_universal2105/.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.