Back to Journals » International Medical Case Reports Journal » Volume 9
Chronic biliary colic associated with ketamine abuse
Authors Al-Nowfal A, Al-Abed Y
Received 16 November 2015
Accepted for publication 22 January 2016
Published 2 June 2016 Volume 2016:9 Pages 135—137
DOI https://doi.org/10.2147/IMCRJ.S100648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Ahmed Al-Nowfal, Yahya A Al-Abed
Department of Surgery, Southend University Hospital, Prittlewell Chase, Westcliff-on-Sea, Essex, UK
Introduction: Biliary colic is a common clinical presentation, with the majority of cases being related to gallstone disease. However, rarely, patients may present with biliary symptoms without evidence of gallbladder stones – referred to as acalculous gallstone disease. This case report details a rare case of chronic biliary colic associated with ketamine abuse.
Case presentation: A 24-year-old Caucasian female presented to the emergency department with a history of intermittent right upper quadrant pain associated with nausea and malaise. She had experienced bouts of similar symptoms three times a year for the past 4 years. Various investigations had been conducted during her multiple admissions, which showed possible dilatation of the common bile duct, with no evidence of gallstones.
Conclusion: Patients can present with a dilated common bile duct and an acalculous cholecystitis. This requires considerable investigation, with an emphasis on drug history, especially with the current rise of recreational hallucinogenic drug abuse.
Keywords: gastroenterology, hepatology, substance abuse, ketamine, acalculous gallstones, biliary disease
Introduction
Biliary colic is a common presentation in clinical practice. The majority of cases are related to gallstone disease. However, rarely, patients may present with biliary symptoms without evidence of gallbladder stones; commonly referred to as acalculous gallstone disease. Patients may present with acalculous biliary colic or cholecystitis. This has been described in association with a wide variety of clinical conditions,1 the majority being related to infections and hematological disorders (Table 1).
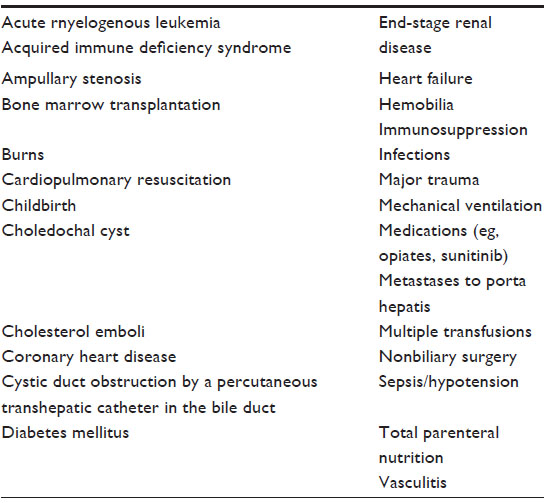 | Table 1 Risk factors for acute acalculous cholecystitis |
There have been recent reports of increasing use of ketamine for recreational purposes (street ketamine).2 Ketamine was originally developed for use in anesthesia, especially within pediatrics. Street ketamine is impure containing 30%–90% ketamine, the reminder being composed of cutting agents such as paracetamol, caffeine, and flour. It is sold as a liquid or white powder. It is injected, snorted, or swallowed. Ketamine has a fast-acting nature and prolonged high with a limited hangover effect, which makes it a popular nightclub drug. Ketamine abuse at moderate-to-high doses can cause sedation, immobility, and amnesia; it increases the risk of serious central nervous system and cardiovascular effects, including respiratory distress or arrest, resulting in death.3
The physical side effects of ketamine when used for ecstasy is well researched and case reports show that ketamine may be associated with chronic epigastric pain, nonobstructive biliary dilatation, abnormal liver function tests, and urinary bladder dysfunction.4
Here, we present a case of a young Caucasian female who had a 4-year history of ketamine abuse and presented with multiple episodes of right upper quadrant (RUQ) pains and symptoms suggestive of biliary colic. Investigations showed a dilated common bile duct (CBD) with no evidence of gallstone disease.
This study was deemed exempt from full review according to the Southend University Hospital Ethical Committee, UK as this was a retrospective, non-comparative study. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Case report
A 24-year-old Caucasian female presented to the emergency department with a history of intermittent RUQ pain associated with nausea and malaise. She reported similar episodes of her symptoms three times a year for the past 4 years. The pain was not associated with meals or posture. She did not have any significant past medical history and did not take any regular medicines. On examination, she was hemodynamically stable; there was no fever or tachycardia and her blood pressure was within normal limits. Abdominal examination showed no evidence of peritonitis but revealed tenderness in the RUQ and epigastric regions. Urine dipstick for blood and pregnancy was negative. Full blood count and serum biochemistry showed a normal white cell count of 5.8×109/L with normal renal and liver function tests. The initial differential diagnoses by the admitting causality officer included biliary colic and peptic ulcer disease. She was admitted and started on opiate analgesics and antispasmodics and her symptoms gradually improved. Ultrasound scan of the abdomen demonstrated a normal liver and gallbladder with no evidence of gallstones but with a dilated CBD of 8.5 mm. Two days following admission, she underwent magnetic resonance cholangio-pancreaticography, which again showed no gallstones, but also conversely no evidence of intra- or extrahepatic biliary dilatation with a CBD of normal diameter.
On review of our patient’s previous hospital admissions, we noted that 60 days prior, she had presented with similar episodes of RUQ pain; ultrasound scan of the abdomen and an esophagogastroduodenoscopy were normal. Two years prior to that, she had presented to a different unit with similar symptoms and at the time radiological investigations revealed a dilated CBD of 11 mm with no other abnormality.
On further enquiry into her social history, the patient admitted recreational use of oral ketamine over the past 4 years, all episodes of which coincided with her intermittent abdominal symptoms. She denied the use of any other illicit drugs and only moderately consumes alcohol.
Discussion
Ketamine is an N-methyl-d-aspartate receptor antagonist developed in 1962 for use in anesthesia.5 However, “street ketamine,” which is a close analog of ketamine, has become a commonly used drug for ecstasy. Unlike the other well-known dissociative illicit drugs, ketamine is very short-acting. It takes effect within about 10 minutes, while its hallucinogenic effects last up to 2 hours when ingested orally, making it a popular “club drug” often used by teens and young adults at dance “rave” parties.6
Ketamine is metabolized by hepatic microsomal enzymes and has a half-life of 2.5 hours. It is excreted mainly through urine (90%), with the remainder through bile.7
Wide variety of symptoms is associated with ketamine abuse. A large number of abusers present with impaired level of consciousness, dizziness, abdominal pain, and lower urinary tract symptoms. The most common physical signs in patients with ketamine abuse are hypertension, tachycardia, and abdominal tenderness.8
Severe urinary bladder dysfunction and recurrent episodes of epigastric pain associated with dilated CBD in the absence of gallstones in ketamine abusers has also been reported.7
A study by Ng et al8 investigated the clinical presentations of ketamine abusers in 233 cases. Abdominal pain was the presenting complaint in 21% of cases while abdominal tenderness was noted in 18% of patients. Two out of 35 patients who had radiological investigations had confirmed dilated bile ducts in the absence of gallstone disease.9 A case series published by Wong et al10 also presented similar findings.
In our case radiological investigations failed to identify a cause for a dilated CBD. Based on previous studies and case series, we believe that the ketamine abuse is the most likely cause for this. Although the exact pathophysiology of ketamine-induced dilated biliary system is unknown, it is postulated that ketamine increases the flow of resistance across the sphincter of Oddi.11
In conclusion, this case report highlights the importance of drug history taking in patients presenting with abdominal pain and specifically biliary colic.
Acknowledgment
We would like to thank all the NHS staff who tirelessly look after their patients in these difficult times. No funding was provided to write this case report.
Disclosure
The authors report no conflicts of interest in this work.
References
Afdhal NH. Acalculous cholecystitis. In: Post TW, editor. UpToDate. Waltham, MA: Wolters Kluwer. Accessed October 18, 2015. | |
Adam R Winstock. The Global Drug Survey 2014 findings. Available from: http://www.globaldrugsurvey.com/facts-figures/the-global-drug-survey-2014-findings. Accessed October 18, 2015. | |
National Institute on Drug Abuse. Hallucinogens and dissociative drugs. Available from: http://www.drugabuse.gov/publications/research-reports/hallucinogens-dissociative-drugs/what-are-effects-common-dissociative-drugs-brain-body. Accessed October 18, 2015. | |
Wood D, Cottrell A, Baker SC, et al. Recreational ketamine: from pleasure to pain. BJU Int. 2011;107(12):1881–1884. | |
Jansen, KL. A review of the nonmedical use of ketamine: use, users and consequences. J Psychoactive Drugs. 2000;32:419–433. | |
Anderson L. Ketamine. Available from: http://www.drugs.com/illicit/ketamine.html. Accessed October 18, 2015. | |
Adamowicz P, Kala M. Urinary excretion rates of ketamine and norketamine following therapeutic ketamine administration: method and detection window considerations. J Anal Toxicol. 2005;29(5):376–382. | |
Ng SH, Tse ML, Ng HW, Lau FL. Emergency department presentation of ketamine abusers in Hong Kong: a review of 233 cases. Hong Kong Med J. 2010;16(1):6–11. | |
Lo RS, Krishnamoorthy R, Freeman JG, Austin AS. Cholestasis and biliary dilatation associated with chronic ketamine abuse: a case series. Singapore Med J. 2011;52(3):e52–e55. | |
Wong SW, Lee KF, Wong J, Ng WW, Cheung YS, Lai PB. Dilated common bile ducts mimicking choledochal cysts in ketamine abusers. Hong Kong Med J. 2009;15(1):53–56. | |
Thune A, Jivegård L, Polland H, Moreau J, Schwartz JC, Svanvik J. Location of enkephalinase and functional effects of [Leu 5]enkephalin and inhibition of enkephalinase in the feline main pancreatic and bile duct sphincters. Clin Sci (Lond). 1992;82:169–173. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.