Back to Journals » Journal of Asthma and Allergy » Volume 15
Caregiver Perceptions of Change in Pediatric Asthma Control During the COVID-19 Pandemic
Authors Pogge G ![]() , Waters EA, Webster GD
, Waters EA, Webster GD ![]() , Prabhakaran S, Hunleth JM, Fedele DA, Shepperd JA
, Prabhakaran S, Hunleth JM, Fedele DA, Shepperd JA ![]()
Received 16 August 2022
Accepted for publication 15 October 2022
Published 20 December 2022 Volume 2022:15 Pages 1795—1804
DOI https://doi.org/10.2147/JAA.S385891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Gabrielle Pogge,1 Erika A Waters,2 Gregory D Webster,1 Sreekala Prabhakaran,3 Jean M Hunleth,2 David A Fedele,4 James A Shepperd1
1University of Florida, Department of Psychology, Gainesville, FL, 32603, USA; 2Washington University School of Medicine, Department of Surgery – Public Health Sciences, Saint Louis, MO, USA; 3University of Florida, Department of Pediatrics, Gainesville, FL, 32603, USA; 4University of Florida, Department of Clinical and Health Psychology, Gainesville, FL, 32603, USA
Correspondence: Gabrielle Pogge, Department of Psychology, University of Florida, PO Box 112250, Gainesville, FL, 32611-2250, USA, Tel +1757-642-0396, Email [email protected]
Purpose: Although several indicators suggest that pediatric asthma control in the United States improved early in the pandemic, other indicators suggest not. Missing are reports from caregivers of the experiences of their children with asthma early in the pandemic.
Methods: Using the PP-ACT and other measures that we specifically constructed for our research, we conducted a cross-sectional national survey of US caregivers of children with asthma (N=595) to examine perceived change in their child’s asthma control and changes in reports of ED visits and use of emergency relief medicine and controller medicine pre-pandemic (January to March 2020) versus early-pandemic (June to September 2020).
Results: Caregivers fell into three groups: most caregivers perceived that their child’s asthma control was improved (50.3%) or unchanged (41.2%), and few reported worse control (8.5%). Surprisingly, all three groups of caregivers reported similar frequencies of early-pandemic and pre-pandemic ED visits and use of emergency relief medicine. Also surprising, caregivers who perceived their child’s asthma as more controlled (compared with the other two groups) reported more frequent ED visits and use of emergency relief medicine, yet also more use of controller medicine at both early-pandemic and pre-pandemic.
Conclusion: The mismatch between caregivers’ perceptions of their child’s early-pandemic asthma control and their reports of ED visits and use of emergency relief medicine suggests that caregivers may rely on a gist (a global evaluation that can include nonbiomedical evidence) when estimating their child’s asthma control. Caregivers and their families could benefit from help from clinicians in understanding the discrepancy between subjective asthma control and asthma control indicators and in understanding what well-controlled asthma looks and feels like.
Keywords: PP-ACT, childhood asthma, ED admissions, coronavirus 19 pandemic, asthma caregivers, United States, perceptions
Introduction
Although the SARS-CoV-2/COVID-19 pandemic represented a worldwide health challenge, it may have provided unanticipated benefits to caregivers of children with asthma. First, a large (27-country) online survey of pediatric asthma providers revealed that 20% reported improved asthma control in their patients after the onset of the pandemic and only 10% reported reduced control in children during the pandemic.1,2 Second, early in the pandemic, hospitals in the United States documented dramatic decreases in emergency department (ED) visits3–9 and hospitalizations2,5,8,10 for pediatric asthma. Third, data from 77 Pediatric Intensive Care Units across the United States revealed a 32% decrease in admissions from April to June of 2020 compared with the same period during the previous three years.11
However, not all evidence suggests that asthma symptoms decreased during the early days of the pandemic. For example, although some studies using hospital records reported a decline in asthma-relevant prescriptions for controller and emergency relief medicines (eg, inhaled corticosteroids [ICS] and albuterol, respectively) during versus before the pandemic,9 others did not.1,5,12
Missing from these investigations of pediatric asthma control during the early months of the pandemic are reports from caregivers of children with asthma. The caregiver perspective is a crucial gap in understanding the hospital data and important because of the key role caregivers play in their children’s asthma care. Caregivers ultimately decide when and how to respond to their child’s symptoms. These decisions are driven in part by their perceptions of the severity of their child’s asthma and—during the pandemic—in part by their perceptions of the risks associated with seeking clinical help. Moreover, perceptions are not independent evaluations, but rather reflect a comparison process. In the case of asthma, caregiver judgements of asthma control are less a reflection of clinical control and more a reflection of how the child’s asthma control today compares with the child’s asthma control in the past.13 For instance, caregivers may perceive their child’s asthma as controlled when it is not simply because the symptoms are less severe now than in the past. The caregiver perspective could provide unique insights into the inconsistency observed in the reports of hospital data. To our knowledge the only study to examine caregiver perceptions was a qualitative study that found that caregivers, who were largely at home with their children during the pandemic, felt an increased sense of personal control over their child’s asthma because they could monitor and respond more quickly to displays of asthma symptoms.12 Needed is more evidence on the reports of caregivers.
In a national survey of caregivers of children with asthma in the United States, we examined caregiver’s perceptions of their child’s asthma control early in the pandemic versus before the onset of pandemic restrictions. We tested two hypotheses:
Perceived Change Hypothesis
We predicted that caregivers would report that compared with the three months before the pandemic restrictions (hereafter, pre-pandemic) their child’s asthma was more controlled (versus less controlled) in the three months early in the COVID-19 pandemic (hereafter, early-pandemic).
Correspondence Hypotheses
We predicted that reports of ED visits and use of emergency relief medicine would (a) decrease from pre-pandemic to early pandemic among caregivers who perceived their child’s asthma as more controlled, (b) increase among caregivers who perceived their child’s asthma as less controlled, and (c) not differ among caregivers who perceived no change in their child’s asthma control. Finally, focusing just on early-pandemic reports, we predicted that caregivers would report fewer early-pandemic ED visits and less use of emergency relief medicine if they perceived their child’s asthma as more controlled than if they perceived their child’s asthma as less controlled.
We also collected data for use of controller medicine and tested for within- and between-groups differences in caregiver’s pre-pandemic and early-pandemic reports. However, we made no directional predictions because prolonged asthma control can eventuate in stepping down, or in some cases, stopping controller medicine.14 Thus, a decrease in use of controller medicine may correspond with both less-controlled and more-controlled asthma.
Materials and Methods
Participants
We report data from a national, cross-sectional survey of 1219 caregivers of children with asthma recruited from September to December 2020 using Qualtrics panels (Qualtrics, Provo, UT). Caregivers were eligible to participate if they reported having a child who: (a) was diagnosed with asthma by a healthcare provider, (b) still had asthma, (c) was younger than age 18, and (d) resided with the caregiver who was completing the survey for at least 90 days a year. In addition, we set a target of one-third of participants with low income. Data collection were part of a larger study. Because of random assignment we instituted for the goals of the larger survey (unrelated to the current investigation), roughly half of caregivers (n=595) responded to the items assessing frequency of asthma management behavior (ie, ED visits, medication use). The final sample size gave us ample statistical power (>.80) to detect small-to-moderate effect sizes (ie, |r|s ≥ 0.10, assuming α=0.05, two-tailed). See the online Supplemental Materials (OSM) for a full discussion of our recruitment decisions. Demographic information appears in Table 1. To ensure anonymity, we did not collect geographic location information about participants. Participants were compensated for their time based on Qualtrics’ recruitment process, which includes sub-contracting to other recruitment firms. Qualtrics handled all participant payments.
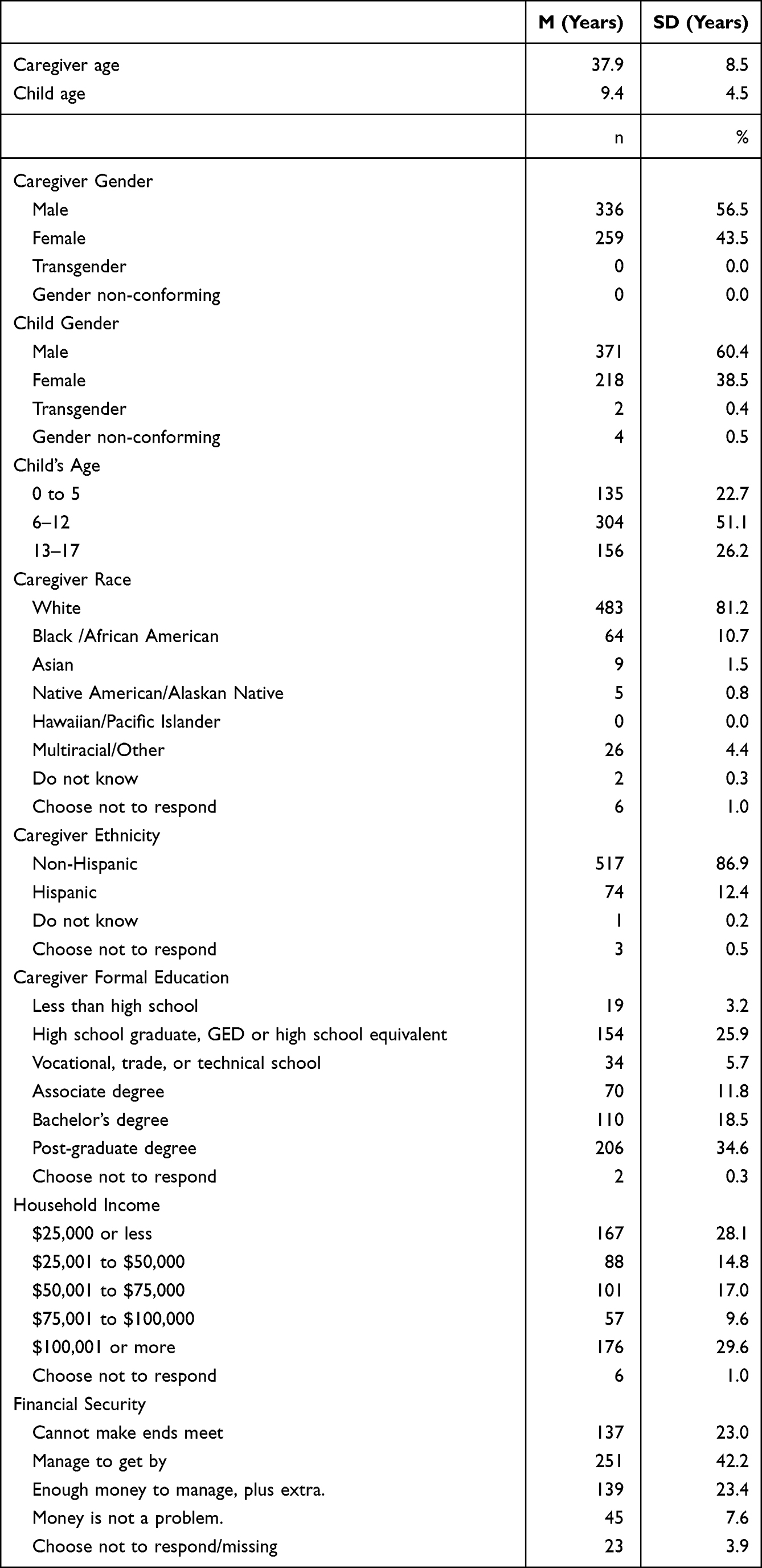 |
Table 1 Demographic Information (N = 595) |
Design and Procedure
In compliance with the Declaration of Helsinki, the Institutional Review Board at the University of Florida approved all procedures and measures (IRB#201802313). Caregivers who consented to participate completed the measures in the order listed in the materials section. With the exception of the PP-ACT15 we constructed all measures specifically for our research. All caregivers responded to the item assessing perceived change in asthma control. Participants could choose not to respond to any item. We excluded such responses from analysis of the item. The pre-registration document, protocol, informed consent, all survey items, data, codebook, analysis script, and Supplementary Methods and results are available at the OSF project page: https://osf.io/awqf8/.
Materials
Frequency of Asthma Management Behavior
Caregivers reported the frequency of engaging in three asthma management behaviors in the past three months (roughly June to September 2020; early-pandemic frequency): ED (ie, urgent care or emergency room) visits when the child was having trouble breathing (n=588; 7 chose not to respond), use of “quick-relief medicine like albuterol” (n=536 prescribed at pre-pandemic; 53 were not prescribed at this time and 6 chose not to respond), and use of “long-term asthma controller medicine [that] helps prevent breathing problems over time and is NOT a ‘quick relief’ medicine like albuterol” (n=492 prescribed at pre-pandemic; 96 were not prescribed at this time and 7 chose not to respond). We then asked caregivers to report the frequency of engaging in the same three asthma management behavior in the three months before the coronavirus pandemic started in the United States, which we defined in the survey item as December 2019 to March 2020 (pre-pandemic frequency). All items used a 1 (never) to 5 response-format (for medication use, 5=more than once per day on average; for ED visits, 5=four or more times).
Perceived Change in Asthma Control
Participants reported whether they thought their child’s asthma in the past four weeks (during the recruitment period, this would fall between roughly June and September 2020) was less controlled, about as controlled, or more controlled than in the four weeks before the pandemic restrictions started in the US, which we defined in the survey item as February 2020. We called these groups the perceived change groups.
Asthma Control
Participants responded to a revised version of the five-item Parent Proxy Asthma Control Test (the PP-ACT),15 which is based on the Asthma Control Test (ACT)16 but yields two scores representing caregivers’ evaluation of their child’s asthma control in the past four weeks: a measure of control of symptoms based on the sum of four items (impairment from asthma, shortness of breath, sleep disruption, and albuterol use), and a one-item measure of subjective control that represents the caregivers’ global, subjective judgment of their child’s asthma control.17 Higher scores indicate greater control. We report results for these two forms of asthma control for descriptive purposes only.
Analysis
We examined the Perceived Change Hypothesis using a chi-square test of equal proportions to test whether similar proportions of caregivers chose each of the three responses to the item assessing perceived change in their child’s asthma control since the start of the pandemic (ie, 33% for each of the three responses: less controlled, similar control, more controlled). To examine the Correspondence Hypotheses, we first conducted three 3 (group: less controlled, similarly controlled, more controlled) × 2 (time: pre-pandemic, early-pandemic) mixed-model ANOVAs to test for the main effects of group and time for each of the three asthma management behaviors (ED visits, use of emergency relief medicine, use of controller medicine). We followed significant main effects with pairwise t-tests (with Bonferroni correction for multiple comparisons) comparing early-pandemic and, separately, pre-pandemic reports across the three groups.
Results
Did Caregivers Report an Increase in Their Child’s Asthma Control?
Consistent with the Perceived Change Hypothesis, a chi-square test of equal proportions revealed that most caregivers perceived their child’s early-pandemic (compared with pre-pandemic) asthma as more controlled (n=296, 50.3%) or unchanged (n=242, 41.1%). Few caregivers reported that their child’s asthma was less controlled (n=50, 8.5%) than before the pandemic restrictions, χ2 (2) = 171.48, p<0.001.
Did Caregivers’ Perceptions Correspond with Their Reports of ED Visits and Use of Emergency Relief Medicine?
The three mixed-effects ANOVAs revealed no main effects of time for any of the three asthma management behaviors: for ED visits, F(1, 575) = 1.81, p=0.18; for emergency relief medicine, F(1, 498) = 0.0003, p=0.98; for controller medicine, F(1, 457) = 1.18, p=0.28. We observed main effects of perceived change group for ED visits, F(2, 575) = 30.72, p<0.001), use of emergency relief medicine, F(2, 498) = 16.29, p<0.001), and use of controller medicine, F(2, 457) = 18.80, p<0.001). Below we describe the effects as they pertain to the Correspondence Hypotheses.
We first compared the reports for the pre-pandemic period vs early-pandemic period separately for caregivers in the three perceived change groups (the more controlled group, the less controlled group, and the unchanged group). Consistent with the correspondence hypothesis, the unchanged group reported no difference in the frequency of ED visits and use of emergency relief medicine in the two time periods (see Table 2). However, inconsistent with the correspondence hypothesis, the other two groups also showed no difference in reports of ED visits and use of emergency relief medicine across the two time periods.
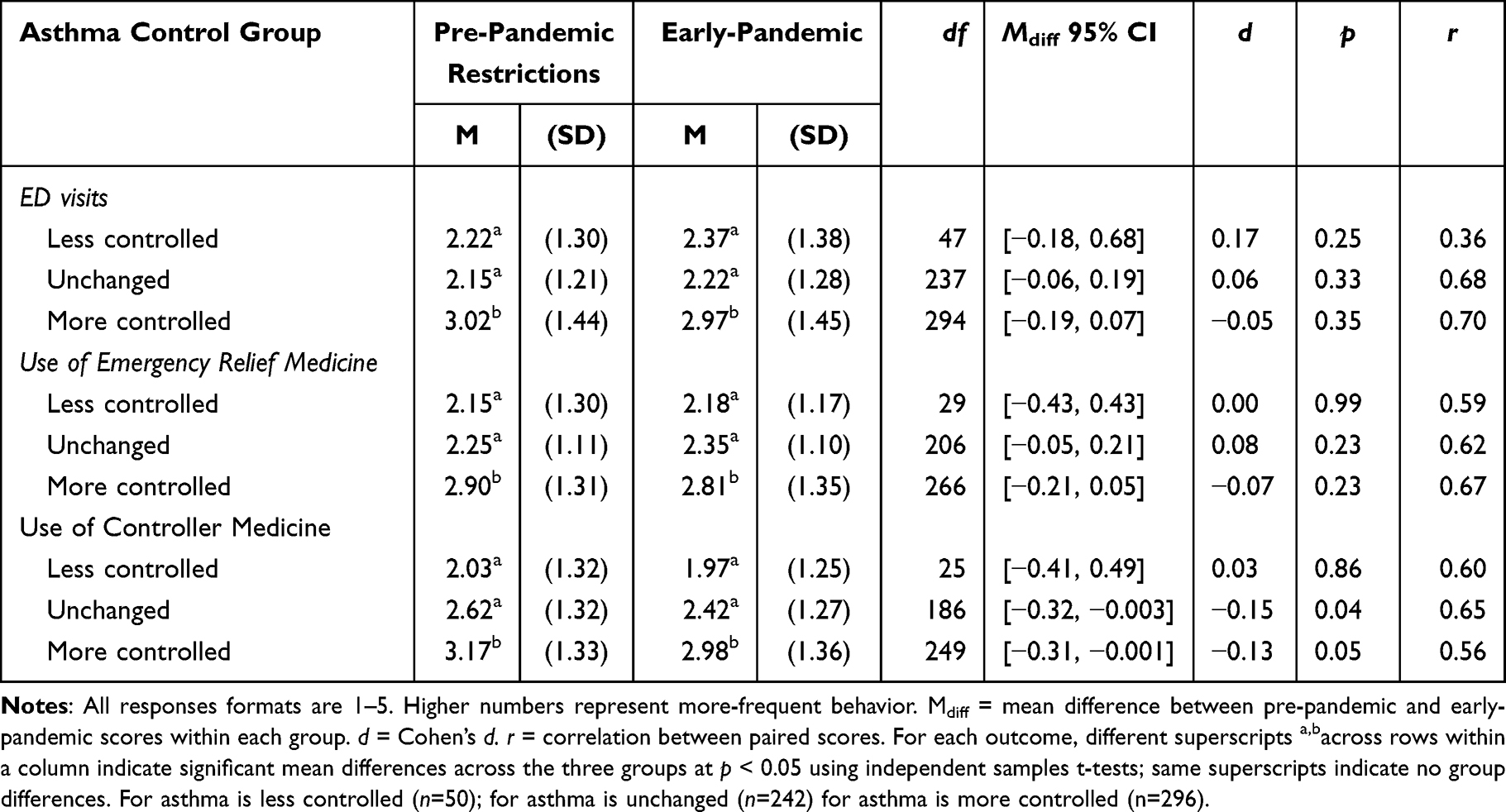 |
Table 2 Mean Reports of Asthma Management Behavior Among Three Groups of Caregivers |
We next compared the three perceived change groups with each other. Contrary to the correspondence hypothesis, the more controlled group (compared with the unchanged group and the less controlled groups) reported more early-pandemic ED visits and use of emergency relief medicine. Although not part of our hypotheses, these differences also appeared pre-pandemic. Both early-pandemic and pre-pandemic, the less controlled and the unchanged group did not differ in ED visits or use of emergency relief medicine.
As a reminder, we made no directional predictions for use of controller medicine. Interestingly, the more controlled group and the unchanged group reported a decrease in use of controller medicine pre-pandemic to early-pandemic (see Table 2). The less controlled group reported a similar frequency in early-pandemic and pre-pandemic use of controller medicine. Finally, in both the early-pandemic and pre-pandemic periods, the more controlled group reported more frequent use of controller medicine than did the other two groups (all ps<0.001). The less controlled and no change group did not differ in use of controller medicine at early-pandemic or at pre-pandemic (ps>0.07).
Ancillary Analyses
To understand the seemingly conflicting findings regarding the correspondence hypotheses, we explored whether the three groups differed in their responses to a standard measure of asthma control that we assessed early in the pandemic: the PP-ACT. Recall that recent studies suggest that the PP-ACT has two components: control of symptoms and impairment and subjective control.17,18 Consistent with prior evidence that the two measures represent different constructs,17,18 we observed a small, negative correlation between these two measures in our sample, r(565) = −0.28, p<0.001. Greater subjective asthma control corresponded with reports of less control over symptoms and impairment. One-way Welch ANOVAs revealed group differences in control of symptoms and impairment, F(2, 141.0) = 27.10, p<0.001, and in subjective control, F(2, 125.0) = 35.90, p<0.001. Table 3 compares responses to these two indicators of asthma control among the three groups of caregivers. The more controlled group reported higher subjective asthma control—yet lower control of symptoms and impairment—than did the other two groups of caregivers (ps <0.001). We return to this intriguing finding in the discussion.
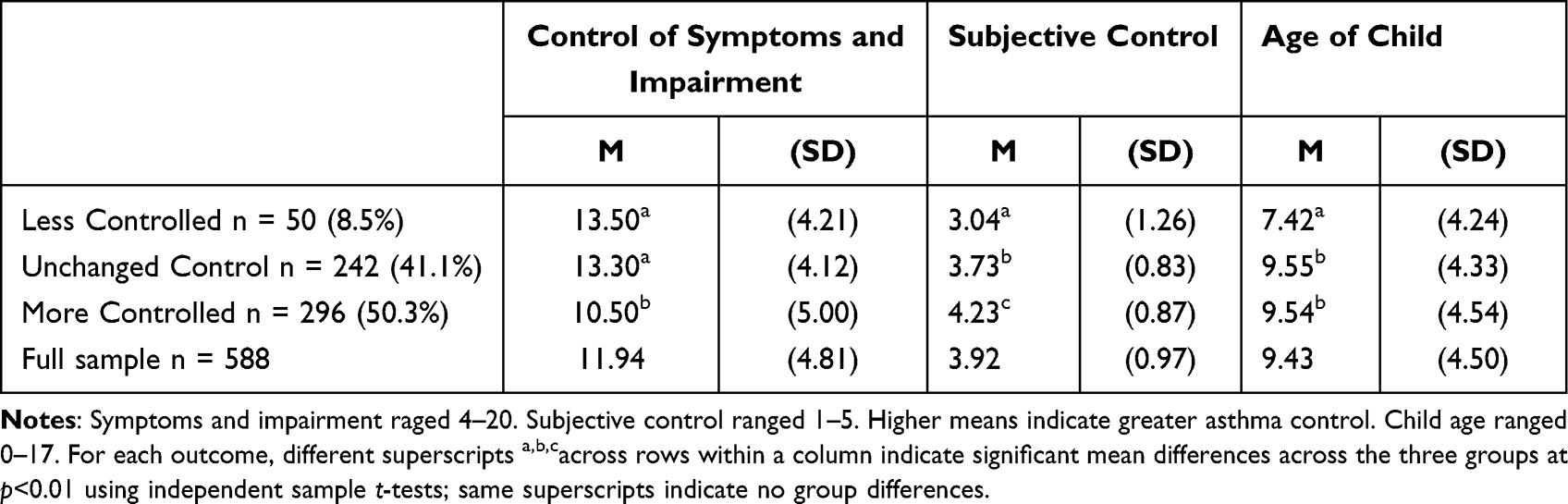 |
Table 3 Asthma Control (PP-ACT) Scores and Age Across Levels of Perceived Change in Asthma Control |
A quarter of caregivers (26.2%) had children who were older (ie, age 13 to 17). Older children often assume greater responsibility for their asthma management than do younger children.19 It is possible that older children were overrepresented among the groups of caregivers who reported improved or no change in asthma control. Older children are less dependent on their caregivers and tend to spend more time away from home compared with younger children.19 Caregivers may thus be less aware of their symptoms and interpreted no news as good news. We examined whether the three groups differed in the average age of the child. Consistent with this possibility, a one-way ANOVA revealed group differences in the mean age of our three groups, F(2,595) = 5.68, p = 0.004). Pairwise comparisons revealed that the children were younger in the less controlled group than in the unchanged group and in the more controlled group (see Table 3). Put another way, 8% of caregivers in the less controlled group reported their child was age 13–17 compared with 29% of caregivers in the more controlled group and 26% of caregivers in the unchanged group.
Discussion
The Perceived Change Hypothesis received strong support. Most caregivers perceived their child’s asthma as more controlled or unchanged in the early-pandemic (June to September 2020) phase compared with before the pandemic restrictions (December 2019 to March 2020). Few perceived their child’s asthma as less controlled. This finding is consistent with a large (27-country) online survey where 20% of pediatric asthma providers reported improved asthma control and only 10% reported reduced control in children during the pandemic.1
The Correspondence Hypothesis received limited support. No group showed differences in the frequency of pre-pandemic and early-pandemic ED visits and use of emergency relief medicine. We predicted no changes for the unchanged group but not for the other two groups of caregivers. We did observe group differences in early-pandemic ED visits and use of emergency relief medicine. However, the effects were opposite of prediction. The more controlled group reported more frequent early-pandemic ED visits and use of emergency relief medicine than did the less controlled group.
Our ancillary analyses revealed two important findings. First, reports of subjective asthma control in the early-pandemic corresponded closely with perceptions of changes in asthma control from pre-pandemic to early-pandemic. Caregivers in the more controlled group reported the highest subjective control, whereas caregivers in the less controlled group reported the lowest subjective control. Surprisingly, their reports for control of symptoms and impairment, if anything, indicated the opposite, with caregivers in the more controlled group also reporting the lowest control of symptoms and impairment compared with the other two groups. These findings replicate prior evidence that the PP-ACT measures two distinct aspects of asthma that may largely be unrelated.18 Second, the three groups differed in the average age of the child with asthma. The age of the caregiver’s child was on average two years younger in the less controlled group than in the more controlled and unchanged control groups.
Stepping back, examination of the data reveals three patterns in the data that seem more important than the confirmation or disconfirmation of our hypotheses. First, we saw no change from pre- to early pandemic in ED visits or albuterol use regardless of group. In short, the pandemic lockdown did not seem to affect caregivers’ reports of asthma experiences that would necessitate immediate intervention such as taking emergency relief medicine or going to the ED. The only place we observed change across time (pre-pandemic to early pandemic) was that caregivers in the no change and more controlled groups, who accounted for 91.5% of all participants, showed a decrease in controller medicine use. This general decrease may have occurred for reasons linked to virtual schooling (eg, reduced exposure to triggers and thus a reduced perceived need for controller medicine) or pandemic-related barriers to adherence (including financial constraints and changes in care routines).
The second larger pattern is that the caregivers who reported their child’s asthma was more controlled consistently differed from the other two groups in responses to all measures. They reported more ED visits both pre- and early pandemic, and more use of emergency relief and controller medicine both pre- and early pandemic. Finally, they reported lower control of asthma symptoms and impairment in their child than did the other two groups yet greater subjective asthma control. The finding that caregivers in the more controlled group differed in their responses from caregivers in the other two groups is, by itself, unremarkable. And given that the differences also occurred in caregivers’ pre-pandemic ratings suggests that the differences reflect something preexisting. What makes the findings remarkable, however, is the third larger pattern: the responses of caregivers in the more controlled group were internally inconsistent. Compared with the other two groups, they reported greater early-pandemic subjective control, yet lower control of asthma symptoms and impairment and more frequent ED visits and use of emergency relief medicine. How do we explain the inconsistency?
The inconsistency is unlikely to be the result of poor memory regarding ED visits because such events are likely stressful, expensive, time-consuming, and rare, which makes them memorable. Moreover, poor memory would presumably apply equally to the three groups of caregivers, yet we found group differences. The difference also does not appear due to differences in the age of the child. Age differences could explain why responses of caregivers in the less controlled group differed from the responses of other caregivers. But the responses of these caregivers did not differ from caregivers in the no change group, whereas the responses of caregivers in the more controlled group differed from both other groups.
Although speculative, one possible explanation is that caregivers’ perceptions of change in their child’s early-pandemic asthma control and their ratings of their child’s subjective asthma control reflect their gist20 interpretation of their child’s asthma control. A gist is an abstract global evaluation that may or may not be tied to any specific piece of evidence. Regarding asthma, caregivers’ gist may or may not arise from specific symptoms their child experiences and can be disconnected from biomedical evidence. Recent research finds that caregivers’ global ratings of their child’s asthma control correlate weakly at best with their reports of symptoms and impairment linked to their child asthma,17,18 suggesting that caregivers’ subjective evaluations or gist regarding their child’s asthma may align poorly with biomedical indicators. Instead, the gist can arise from a variety of contextual factors. For example, in the pandemic context, the gist could reflect an increased sense of personal control over their child’s asthma. During the early pandemic, children moved to virtual schooling, which likely reduced exposure to triggers but also increased the ability of caregivers to monitor and respond more quickly to displays of asthma symptoms, an explanation supported in other research.12 Caregivers who reported an increase in their child’s early-pandemic asthma control may have experienced an increased sense of agency that contributed to their gist of their child’s asthma control. But social, economic, and environmental injustices can challenge asthma management,21 and the increased sense of agency during the early pandemic may not be true of all caregivers.
Clinical Implications
Symptom detection and interpretation shape caregivers’ understandings of asthma in ways that differ from the biomedical model.22 Cognitive interviews we conducted in advance of our survey revealed that some caregivers’ definitions of asthma control diverge from the biomedical definition. Some caregivers interpreted “completely controlled” to mean their child was not experiencing exacerbations. Others believed it meant that their child no longer had asthma. In addition, caregivers’ judgments of their child’s asthma can differ dramatically from their child’s perceptions23 and the judgments of providers.24 Some caregivers report difficulty determining when their child’s symptoms necessitate attention from a provider or ED.25 Collectively, these findings highlight the need for clinicians to help caregivers recognize asthma symptoms and understand how to achieve well-controlled asthma. It might be particularly helpful to prompt caregivers to compare their ratings of their child’s asthma control using the PP-ACT with the results from a spirometer test. Clinicians could use discrepancies in which caregivers overestimate their child’s asthma control as a teaching moment for recognizing poor asthma control.
Limitations and Future Research
We conducted the survey after the pandemic began and thus needed to rely on caregivers’ long-term memories of pre-pandemic asthma control. Therefore, we do not know whether children’s asthma control differed early in the pandemic compared with before the pandemic restrictions. Also, our study was cross-sectional. Thus, we did not assess change over time in asthma control, medication use, or ED visits. Seasonal variations in asthma symptoms (the pre-pandemic estimates were for winter 2020; the early-pandemic estimates were for fall 2020) may have clouded our ability to find differences in ED visits reported in hospital records and other research. It would have been more ideal to assess ED visits during the same time period before and during the pandemic.
We also do not know whether caregivers’ perceptions of improved asthma control during the pandemic were limited to those with children whose asthma is primarily influenced by viral triggers—the children who would presumably benefit most from the decreased exposure to other people during the pandemic. Additionally, caregivers’ reports of their child’s asthma control may or may not align with physiological indicators of asthma control such as spirometry results (a limitation of scale measures of asthma control), which we could not measure in an online survey. Further, because these results are from a single US national sample of caregivers who were primarily non-Hispanic and White the results may not generalize to other caregivers of children with asthma. However, our sample was well-powered to detect small-to-moderate effect sizes, which increases confidence in the observed effects.
Conclusion
We found that caregiver reports of improved asthma control early in the COVID-19 pandemic appeared to conflict with behavioral indicators (ED visits and emergency relief medicine) and a scale measure of early-pandemic asthma control. Although researchers may be inclined to attach less weight to caregiver perceptions than to healthcare utilization, caregiver reports are essential. Caregivers are often the final arbiters on how to treat their children’s asthma and their decisions are grounded in their perceptions of their child’s asthma and their ability to access the medical system. Our findings appear to provide additional evidence that caregivers’ and providers’ understandings of asthma control differ, and suggest the need for clinicians to help families understand what asthma control looks and feels like, and to encourage continued use of controller medicines to achieve well-controlled asthma.
Data Sharing Statement
The data that support the findings of this study are openly available at the OSF project page at https://osf.io/87kpr.
Acknowledgments
This research was supported by the US National Institutes of Health (R01HL137680, MPI Erika Waters, James Shepperd) and the Washington University Institute of Clinical and Translational Sciences grant UL1TR002345 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH. The funder had no role in the collection, analysis, or interpretation of the data, the writing of the report, or the decision to submit the manuscript.
Disclosure
The authors report no conflicts of interest.
References
1. Papadopoulos NG, Custovic A, Deschildre A, et al. Impact of COVID-19 on pediatric asthma: practice adjustments and disease burden. J Allergy Clin Immunol Pract. 2020;8(8):2592–2599. doi:10.1016/j.jaip.2020.06.001
2. Sheehan WJ, Patel SJ, Margolis RHF, et al. Pediatric asthma exacerbations during the COVID-19 pandemic: absence of the typical fall seasonal spike in Washington, DC. J Allergy Clin Immunol Pract. 2021;9(5):2073–2076. doi:10.1016/j.jaip.2021.02.008
3. DeLaroche AM, Rodean J, Aronson PL, et al. Pediatric emergency department visits at US children’s hospitals during the COVID-19 pandemic. Pediatrivcs. 2021;147(4):e202–e39628.
4. Arsenault S, Hoofman J, Poowuttikul P, Secord E. Sustained decrease in pediatric asthma emergency visits during the first year of the COVID-19 pandemic. Allergy Asthma Proc. 2021;42(5):400–402. doi:10.2500/aap.2021.42.210059
5. Kenyon CC, Hill DA, Hendrickson SE, Bryant-Stephens TC, Zorc JJ. Initial effects of the COVID-19 pandemic on pediatric asthma emergency department utilization. J Allergy Clin Immunol Pract. 2020;8(8):2774–2776. doi:10.1016/j.jaip.2020.05.045
6. Levene R, Fein DM, Silver EJ, Joels JR, Khine H. The ongoing impact of COVID-19 on asthma and pediatric emergency health-seeking behavior in the Bronx, an epicenter. Am J Emerg Med. 2021;43:109–114. doi:10.1016/j.ajem.2021.01.072
7. Simoneau T, Greco KF, Hammond A, Nelson K, Gaffin JM. Impact of the COVID-19 pandemic on pediatric emergency department use for asthma. Ann Am Thorac Soc. 2021;18(4):717–719. doi:10.1513/AnnalsATS.202007-765RL
8. Taquechel K, Diwadkar AR, Sayed S, et al. Pediatric asthma health care utilization, viral testing, and air pollution changes during the COVID-19 pandemic. J Allergy Clin Immunol Pract. 2020;8(10):3378–3387. doi:10.1016/j.jaip.2020.07.057
9. Ulrich L, Marcias C, George A, Bai S, Allen E. Unexpected decline in pediatric asthma morbidity during the coronavirus pandemic. Pediatr Pulmonol. 2021;56(7):1951–1956. doi:10.1002/ppul.25406
10. Markham JL, Richardson T, DePorre A, et al. Inpatient use and outcomes at children’s hospitals during the early COVID-19 pandemic. Pediatrics. 2021;147(6):e2020044735. doi:10.1542/peds.2020-044735
11. Zee-Cheng JE, McCluskey CK, Klein MJ, et al. Changes in pediatric ICU utilization and clinical trends during the coronavirus pandemic. Chest. 2021;160(2):529–537. doi:10.1016/j.chest.2021.03.004
12. Jia Y, Bao JQ, Yi M, et al. Impact of the COVID-19 pandemic on asthma control among children: a qualitative study from caregivers’ perspectives and experiences. BMJ. 2021;11(5):e046525.
13. Shepperd JA, Hunleth JM, Maki J, Prabhakaran, S, Pogge, G, Webster, GD, Ruiz, S, Waters, EA, et al. Interpersonal comparison among caregivers of children with asthma. Psychology and Health. 2022. doi:10.1080/08870446.2022.2125514
14. Hamada K, Yasuba H, Tanimura K, Hiramatu M, Kobayashi Y, Kita H. How can we stop ICS? - Risk control therapy by as-needed inhaled fluticasone after stepping down. J Allergy Clin Immun. 2008;121(2):S219. doi:10.1016/j.jaci.2007.12.867
15. DuRivage N, Ross M, Mayne SL, et al. Asthma control test: comparing parent proxy with parent and child report for children 6 to 12 years. Clin Pediatr. 2017;56(4):341–347. doi:10.1177/0009922816675013
16. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immun. 2004;113:59–65. doi:10.1016/j.jaci.2003.09.008
17. Shepperd JA, Webster GD, Pogge G, et al. Psychometric properties and predictive validity of the PP-ACT. J Asthma. 2022:1–11. doi:10.1080/02770903.2022.2036755
18. Przybyszowski M, Stachura T, Szafraniec K, Sladek K, Bochenek G. The influence of self-assessment of asthma control on the asthma control test outcome. J Asthma. 2021;58(4):537–546. doi:10.1080/02770903.2019.1708098
19. Bruzzese J, Bonner S, Vincent EJ, et al. Asthma education: the adolescent experience. Patient Educ Couns. 2004;55(3):392–406. doi:10.1016/j.pec.2003.04.009
20. Brainerd CJ, Reyna VF. Explaining “memory free” reasoning. Psychol Sci. 1992;3(6):332–339. doi:10.1111/j.1467-9280.1992.tb00042.x
21. Hunleth J, Spray J, Ruiz S, et al. Situating household management of children’s asthma in the context of social, economic, and environmental injustice. J Asthma. 2022;59(1):70–78. doi:10.1080/02770903.2020.1837159
22. Spray J, Hunleth J, Ruiz S, et al. How do bodily processes of children’s asthma influence caregiver conceptual models? Soc Sci Med. 2021;294(114706):S260.
23. Davies KJ, DiSantostefano R, Peden DB. Is Johnny wheezing? Parent–child agreement in the childhood asthma in America survey. Pediatr Allergy Immunol. 2011;22(1):31–35. doi:10.1111/j.1399-3038.2010.01016.x
24. Korsten K, Naaktgeboren CA, Bont LJ, van der Ent CK, de Hoog MLA. Defining asthma in children: how well do parents, doctors and spirometry agree? ERJ Open Res. 2020;6(4):348. doi:10.1183/23120541.00348-2019
25. Kelada L, Molloy CJ, Hibbert P, et al. Child and caregiver experiences and perceptions of asthma self-management. NPJ Prim Care Respir Med. 2021;31(1):42. doi:10.1038/s41533-021-00253-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.