Back to Journals » Clinical Interventions in Aging » Volume 20
Care Partner Engagement in Fall Risk Management Programs for Community-Dwelling Older People with Cognitive Impairment: A Systematic Review
Authors Zeng X ![]() , Card A, Choi NG, Zhou Y
, Card A, Choi NG, Zhou Y ![]()
Received 20 July 2025
Accepted for publication 14 November 2025
Published 26 November 2025 Volume 2025:20 Pages 2195—2217
DOI https://doi.org/10.2147/CIA.S553910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Xiaoyi Zeng,1 Amelia Card,1,2 Namkee G Choi,1 Yuanjin Zhou1
1School of Social Work, The University of Texas at Austin, Austin, TX, USA; 2Senior Services of Austin, Austin, TX, USA
Correspondence: Xiaoyi Zeng, School of Social Work, The University of Texas at Austin, 405 W. 25th Street, Stop D3500, Austin, TX, 78705, USA, Email [email protected]
Background/Purpose: Older people with cognitive impairment (CI) are at significantly higher fall risk compared to those without CI. Their care partners’ engagement is critical to facilitate their participation and adherence in fall risk management (FRM) programs. This systematic review aims to synthesize terms and measures of care partner engagement (CPE) in FRM programs for community-dwelling older people with CI, facilitators and barriers to CPE, and promising CPE enhancement strategies.
Methods: We conducted a systematic search of eight databases and included relevant literature published between 1985 and 2024 through a manual search. Guided by a conceptual framework of CPE informed by existing literature, we conducted content analysis and thematic synthesis to address our research aims. We assessed the quality of included studies using the Mixed Methods Appraisal Tool.
Results: Thirty-two studies were included in the synthesis. There was substantial heterogeneity of CPE terms and measures. CPE facilitators and barriers were summarized under three categories: older people with CI (eg, interest, health, and functional statuses), care partners (eg, motivation, perceived burden, caring relationships), and service providers or programs (eg, supportive instructors, service disruptions). CPE enhancement strategies (eg, tailored intervention content, provision of professional and social support) were summarized, with some (eg, using a discussion tool, providing flexible schedules) showing promising effects on CPE.
Conclusion: Our review synthesized the common practice of CPE in FRM programs for community-dwelling older people with CI and introduced a novel conceptual framework to clarify the multidimensional nature of CPE. Our findings emphasized the urgent need to develop consistent language and validated measures for describing and assessing CPE. This review has also identified important considerations, including facilitators, barriers, and promising strategies to enhance CPE in these programs, informing the development of effective care-partner-engaged FRM programs for older people with CI.
Keywords: falls, cognitive impairment, informal caregiving, intervention, behavioral engagement participation
Introduction
Falls are the leading cause of unintentional injury and mortality among older people in the United States.1–3 Cognitive impairment (CI), including both mild cognitive impairment and dementia, is associated with a higher fall risk and fall incidence among older people.4,5 Compared to older people without CI, those with CI have twice the risk of falling and three times the risk of sustaining serious fall-related injuries, such as fractures and head trauma.6–8 Fall risk management (FRM) programs, such as home hazard reduction, physical exercise, education, use of assistive technology, and multifactorial programs, have been designed to reduce the risk of falls and fall-related injuries in older people with CI.5,9 While these programs demonstrated efficacy for cognitively intact older adults, their effectiveness among older people with CI remains inconclusive. This reflects a broader gap in evidence for identifying effective FRM strategies for this high-risk population.9,10
One potential barrier to developing effective FRM programs for older people with CI may be their declining cognitive and functional statuses (eg, severe gait and balance impairment), which can hinder their consistent adherence to program protocols.5,11 In light of these challenges, the involvement of care partners (eg, family members or friends) is critical to support older people with CI in participating in fall risk management programs.11,12 A previous systematic review has shown that care partners often engage in FRM programs through receiving training, collaborating with the healthcare team to implement FRM strategies, and enabling older people with CI to access needed FRM professional services.13 A recent rapid review found that involving care partners in FRM programs can enhance program adherence among older people with CI, as care partners actively assist in identifying fall risk factors and support behavior and lifestyle modifications to reduce fall risk.11
In dementia and caregiving research, care partner engagement (CPE) is a less-explored concept, often framed broadly as a multidimensional and relational process. CPE involves care partners meaningfully engaging in caregiving activities for older people with CI and actively collaborating with them and healthcare providers at various levels across the healthcare system.14–16 While existing reviews on FRM programs for older people with CI emphasize the common practice of involving care partners,5,11,13 they have not examined how CPE has been defined, described, or measured. This lack of clear conceptualization and operationalization of CPE limited further examination of factors that may facilitate or hinder CPE in FRM programs, as well as whether there are promising strategies to enhance CPE. Obtaining these understandings is essential to inform a congruent research effort towards developing effective approaches that meaningfully integrate care partners into the delivery of FRM programs for this at-risk population.
The concept of CPE has been better established for behavioral interventions in other populations, such as child mental health prevention programs and care programs for patients with chronic diseases (eg, cancer, heart failure, and chronic obstructive pulmonary disease).17–20 In these fields, CPE often includes care partners’ efforts to seek or initiate help by enrolling, attending, and actively participating in a program or service, as well as interactions with service providers and follow-up with recommendations.17,19 Drawing on these CPE concepts,14–17,19 this study defines CPE in FRM programs for older people with CI as “a dynamic process involving actions that care partners undertake to maximize the benefits from the program”. We also propose a novel framework comprising five key aspects of CPE in FRM programs: care partners’ enrollment, attendance, active participation, completion, and maintenance of FRM practice.
Each of the five CPE components reflects a distinct aspect of CPE in our definition. Specifically, (1) enrollment indicates care partners’ initiation of seeking or receiving help from service providers for older people with CI by enrolling in FRM programs; (2) attendance refers to care partners’ presence at a single or multiple program sessions or services; (3) active participation captures the quality and extent of their behavioral involvement during program activities for older people with CI, such as meaningfully and actively recording fall incidents, identifying possible environmental fall risk factors, interacting with service providers, and modifying unsafe behaviors; (4) completion denotes whether care partners fulfill the program requirements from the program start to its conclusion, with or without full attendance or constant active participation; and (5) maintenance of FRM practice refers to the extent to which care partners sustain the application of knowledge, skills, and behaviors acquired through FRM programs in their caregiving routines following the conclusion of the intervention.
Built on the proposed conceptual framework of CPE in FRM, we aimed to conduct a systematic review to describe terms used to operationalize CPE and the measurement of CPE (Aim 1), identify facilitators and barriers associated with the five components of CPE (Aim 2), and explore the strategies employed in FRM programs to enhance different components of CPE and their effects (Aim 3).
Methods
Protocol and Registration
Three authors (Y.Z., N.C., and X.Z.) collectively developed the systematic review protocol following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was registered on the International Prospective Register of Systematic Reviews – PROSPERO (registration ID: CRD42023422200).
Search Strategy
We employed a two-step literature search: Step 1, one author (Y.Z.) with extensive experience in dementia caregiving and FRM research identified 17 systematic review articles (see Appendix 1) for citations and references tracking, followed by a literature search using Google Scholar. Step 2, we performed a comprehensive database search across PubMed, PsycINFO, CINAHL, SocINDEX, EMBASE, Web of Science, Cochrane Library, and Health Research Premium Collection in consultation with an experienced librarian. Search terms included (dement* OR Alzheimer OR “Lewy body” OR “Pick’s disease” OR “cognitive impairment” OR “Frontotemporal degeneration” OR “Parkinson’s AND Dementia”) AND (Fall* OR Fell) AND (communit* OR home OR “aging in place” OR “aging-in-place”) AND (caregiv* OR famil* OR friend* OR neighbor* OR relative* OR carer* OR “care partner*” OR spous* OR child* OR “unpaid AND care”) AND (intervention* OR program* OR effect* OR treatment OR therap* OR rehabilitat* OR tool* OR project* OR prevent*) AND (engage* OR involve* OR participat* OR “homework” OR adhere* OR complet* OR assist* OR help* OR initiat* OR coach). The search covered publications from January 1985 to July 31, 2023, when the research team finalized the search protocol. This broad period was chosen to ensure a comprehensive review of the literature. To ensure the inclusion of recent literature, we conducted an updated search in 2024 and identified one additional relevant article to include. Only peer-reviewed human subject studies with full-text available in English were included.
Study Selection Procedures
Two authors (Y.Z. and X.Z.) independently applied the inclusion/exclusion criteria (see Appendix 2) to determine study eligibility for selection. All references for initial screening were imported into Rayyan, an AI-powered online platform for collaborative systematic reviews.21 After removing duplicates, the two authors independently screened articles and were blinded to each other’s decisions following predefined inclusion/exclusion criteria. Both authors screened full texts, and discussions resolved discrepancies, with reasons and decisions documented in Rayyan. Details on the article identification, screening process, and reasons for inclusion and exclusion are provided in Figure 1.
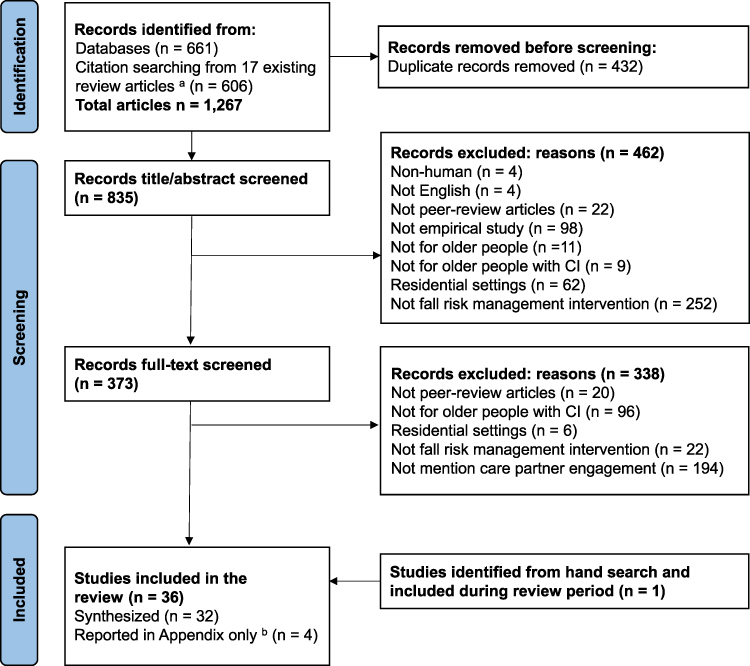 |
Figure 1 PRISMA Chart. Notes: aThe reference list of the 17 relevant review articles identified is provided in Appendix 1. bFour articles had minimum descriptions of care partner engagement (eg, mentioned care partner engagement fewer than five sentences in the entire text). Therefore, the summary of the intervention characteristics of these four studies was presented separately (in Appendix 4) from the included studies. |
Data Extraction
Two authors (X.Z. and A.C.) independently reviewed all full-text articles and extracted data into an Excel spreadsheet, following the PRISMA 2020 systematic review protocol.22 We first retrieved general study information (eg, year, study design), characteristics of study participants (ie, older people with CI, care partners), and key features of the FRM programs (eg, settings, content, and delivery format). Subsequently, guided by our three study aims, we extracted verbatim descriptions, numerical data, key concepts, and summaries, based on our predefined five CPE components. Data that both authors found difficult to interpret (eg, ambiguity about whether an engagement involved older people with CI or care partners) were excluded to avoid potential misinterpretation.
For Aim 1, we extracted terms used to describe CPE, along with any measures used to quantify or assess the CPE. In cases where CPE was reported only at the dyadic level (ie, both older people with CI and care partner), we used the reported dyadic measure as a proxy for CPE, provided the study explicitly stated that care partners’ involvement was required.
For Aim 2, we identified reported facilitators and barriers to CPE. Facilitators were defined as factors that help, enable, or foster CPE, while barriers were those that hinder, limit, or prevent it.23
For Aim 3, we extracted strategies, such as approaches, tools, or technologies, that were designed to enhance CPE and their reported effects. Regarding the effects of the strategies on CPE, we categorized the directions of effects as positive, negative, mixed (ie, both positive and negative), or no evidence of positive effect. These determinations were drawn from either qualitative descriptions or quantitative measures of CPE. Quantitative evidence of effect was reported only if one of the following conditions was met: (1) a rate-based CPE measure (eg, completion rate, attendance rate) was reported; (2) CPE measures were compared across two time points using statistical tests to assess change over time; or (3) a control or comparison group was used to evaluate the effects of the strategies. We did not evaluate the downstream impact of CPE strategies on FRM outcomes, as this was beyond the scope of the current review.
The first author led the review and comparison of all study-level data extractions, flagging discrepancies and verifying them against the original studies in an Excel spreadsheet. Y.Z. and X.Z. further addressed any unresolved issues through iterative discussions.
Data Analysis
We began data analysis by retrieving and calculating descriptive statistics (eg, frequency, proportion, and range) from extracted data to summarize study-level information, participant demographics, and intervention characteristics. For Aim 1, we conducted content analysis, a commonly used analytical approach suitable for objectively describing the common threads derived from the data in a conceptual form.24,25 It allowed us to systematically categorize CPE terms and measures, both quantitatively and qualitatively, reported in the studies according to the five predefined CPE components. For Aims 2 and 3, we adopted a convergent integrated approach to synthesizing and integrating qualitative and quantitative data through data transformation (eg, qualitizing quantitative data into narrative interpretation) following recommended methodological guidance for conducting mixed methods systematic reviews.26 Then, we followed the thematic synthesis approach by organizing the data and coding the findings to develop descriptive themes and subthemes.27 These descriptive themes were then aggregated into higher-level analytical themes to synthesize the main findings within the data.27 For the analysis of Aim 3, when a rate-based measure of CPE was reported without a clearly stated direction of effect, we applied a threshold of 80% (ie, 80% or higher as indicative of a positive effect) as it has been used as a threshold for treatment adherence in previous studies.28,29
All authors reviewed preliminary results and refined the final themes according to our conceptual framework to ensure the accuracy of our analysis. We included 32 studies in the descriptive analysis and thematic synthesis, as four out of the 36 studies were excluded because they contained minimal references to CPE (ie, having fewer than five mentions of CPE throughout the entire text). Therefore, a summary of the intervention characteristics of these four studies was presented separately from the included studies (in Appendix 4).
Quality Appraisal
We employed and adapted the Mixed Methods Appraisal Tool (MMAT), version 2018,30 to assess the methodological quality of the included studies. The MMAT was selected for its appropriateness in evaluating a range of empirical study designs, including qualitative, RCTs, non-RCTs, quantitative descriptive, and mixed-method research. Except for two studies that explicitly aimed to examine facilitators and barriers of the FRM programs that engaged care partners,31,32 none of the other studies included in the final synthesis particularly studied CPE as their primary focus. Therefore, to align the quality appraisal with the specific aims of our review, we adapted the MMAT’s initial screening questions to assess the extent to which each study’s data collection and analytic methods addressed our three review objectives. Ratings were assigned as “yes”, “no”, or “can’t tell”. Two authors (Y.Z. and X.Z.) independently rated the methodological quality of the studies, with particular attention to the appropriateness and adequacy of data collection methods and analysis procedures for CPE within the context of our review aims. Both authors compared the ratings and collectively resolved discrepancies through discussions. A full summary of the appraisal of CPE-specific data quality is provided in Appendix 5.
Results
Our review included 32 studies that provided adequate descriptions of CPE within FRM programs targeting community-dwelling older people with CI for synthesis. A detailed summary of intervention characteristics from these studies is presented in Appendix 3.
Study and Sample Characteristics
Table 1 outlines the characteristics of the studies and FRM programs. In terms of the study design, the majority were quantitative studies (n=22), including randomized controlled trials [RCTs] (n=13), non-RCTs (eg, single group pre-test/post-test design, pilot feasibility trial, n=7), descriptive study (n=1), and multi-method study (ie, RCT and non-RCT, n=1). There were also qualitative studies (n=5) and mixed-method studies (n=5). Most studies were conducted in Europe (eg, Finland, United Kingdom, n=11), Australia (n=10), and the United States (n=9), with only two programs conducted in Asia (ie, Taiwan and Indonesia). The FRM programs were primarily exercise-based (n=18) or multi-component interventions (n=4) that included exercises and other components (eg, behavioral management, home hazard reduction). Other interventions involved discussion tools, fall risk assessment and recommendations, in-home assistive-technology system installations, nutritional guidance, training on safe gait aid use, safety education, and multi-component FRM programs. Fifteen studies (46.9%) included a control group, and 14 (43.8%) had post-intervention follow-ups. Twelve studies (37.5%) reported fall outcomes (eg, rate of falls, number of falls) as a result of the FRM program: 15.6% reported a significant reduction in fall outcomes, 9.4% demonstrated significant effects for certain subgroups (eg, older people with CI who had better baseline physical function), and 9.4% reported non-significant reductions in fall outcomes.
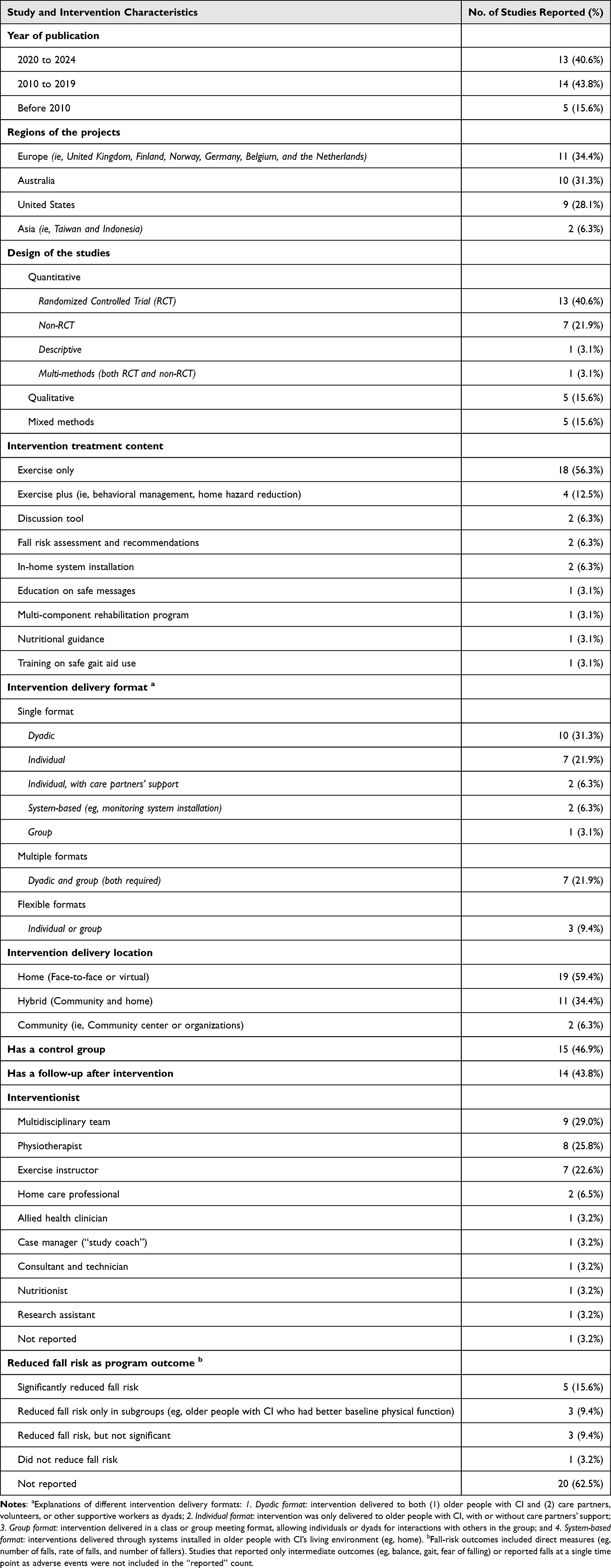 |
Table 1 Summary of Study and Intervention Characteristics (n=32) |
Table 2 presents detailed characteristics of older people with CI participants and care partners in the 29 distinct FRM programs (see footnotes for programs described in multiple studies). The sample sizes of older people with CI participants across projects ranged from 4 to 365. Based on programs with available data, older people with CI had a mean age of 79.6 years and an average of 46.4% were women. Among the 11 of 29 programs that reported race/ethnic background, the majority of participants were White/Caucasian. Regarding types of CI, eight projects were limited to participants diagnosed with Alzheimer’s Disease, and 15 included participants with different types of dementia. The stages of CI varied across projects, with five including only mild stages (eg, mild cognitive impairment, mild Alzheimer’s Disease), four including mild to moderate stages only, and five including a mix of mild, moderate, and severe stages. Over half of the projects reported participants’ fall history at baseline (55.2%) and mobility status at baseline (55.2%). Regarding care partners, a majority of programs (72.4%) included only informal caregivers (eg, spouses, adult children, and other family members), while three programs included both informal and paid caregivers. Based on studies with available data, care partners had an average age of 66.9 years and an average of 70.1% were women.
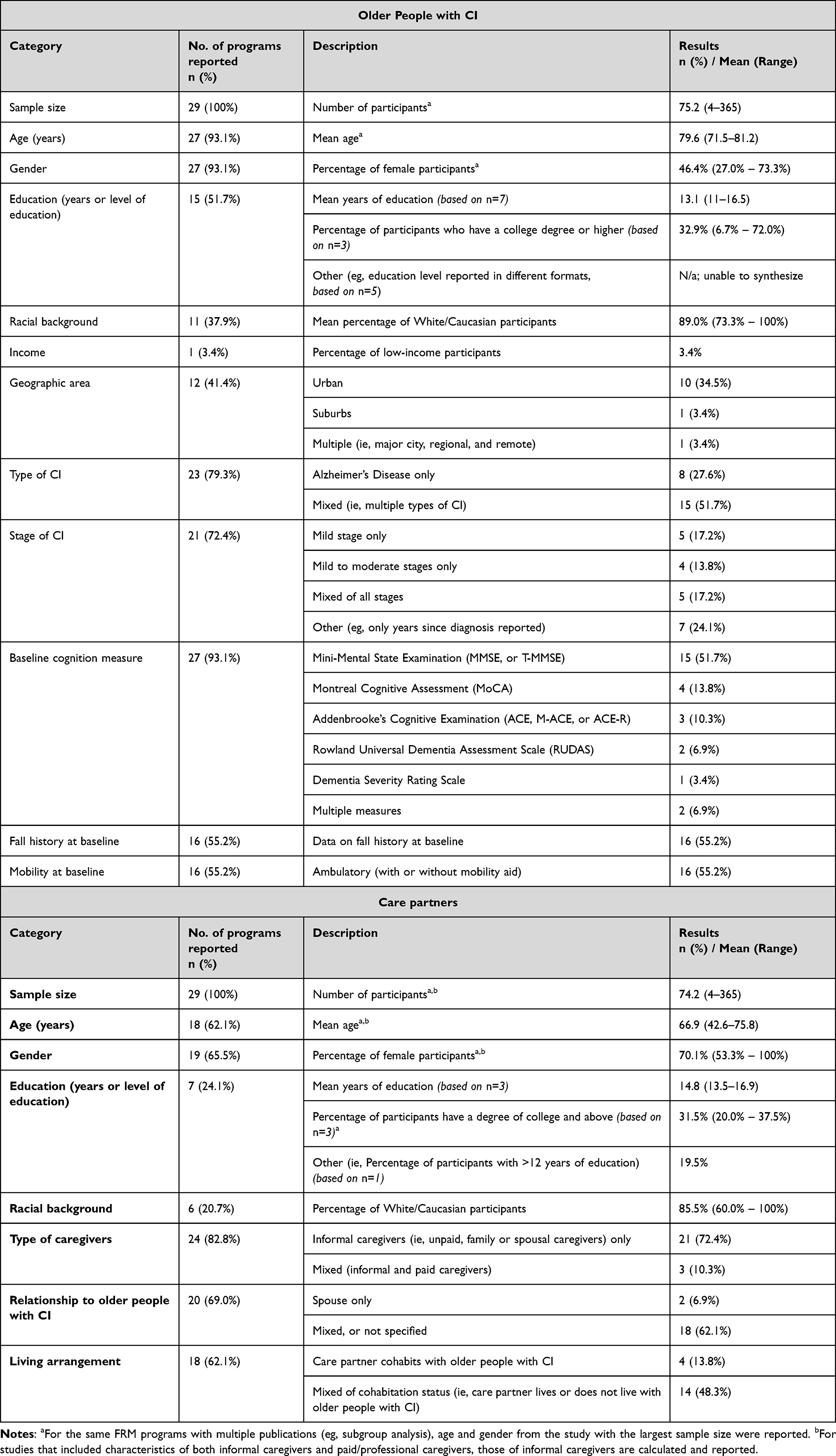 |
Table 2 Characteristics of Older People with Cognitive Impairment (CI) and Care Partners in 29 Unique Fall Risk Management (FRM) Programs |
Quality Appraisal of CPE-Specific Data
Appendix 5 summarizes the results of the quality appraisal of CPE-specific data collection and analysis methods using the adapted MMAT. Although only two studies explicitly posed research questions about CPE, over 80% of the included studies contained data sufficient to address all three aims of this review. All studies included a qualitative component of CPE data, enabling analysis aligned with our research questions; however, 37.5% did not employ appropriate qualitative data collection or analysis methods. The overall quality of the qualitative component is relatively low (lower than 50% of “Yes”). Regarding the quantitative component, a limited number of studies had RCT component (n=1) or non-RCT component (n=4) in reporting CPE-related data, though the data quality was relatively high. Eight studies contained quantitative descriptive data related to CPE, which also demonstrated relatively high quality (more than 50% of “Yes”), except for measurement appropriateness (0% of “Yes”). Among the 13 studies that contained mixed methods components reporting CPE data, none provided an adequate rationale for using mixed-methods approach, and few demonstrated a high quality in both qualitative and quantitative approaches. Nevertheless, most studies effectively integrated qualitative and quantitative findings in ways that were adequate to address our research aims. Overall, the content-specific data quality within the quantitative components was relatively high.
Aim 1: Terms and Measures of CPE
We identified multiple terms across the five CPE components from 24 out of 32 studies, reflecting care partners’ roles, behaviors, and status of behavioral participation in FRM programs (see Table 3). However, none of these studies attempted to define CPE. Terms reflected substantial variability, with most studies including terms that fell within our definitions of care partners’ active participation (75.0%) and completion (62.5%) components. Fewer studies reported the enrollment (28.1%), attendance (18.8%), and maintenance of FRM practice (18.8%) components. Notably, the term “adherence” was commonly used to describe CPE across multiple components, without specifying which particular aspects of CPE were referred to.
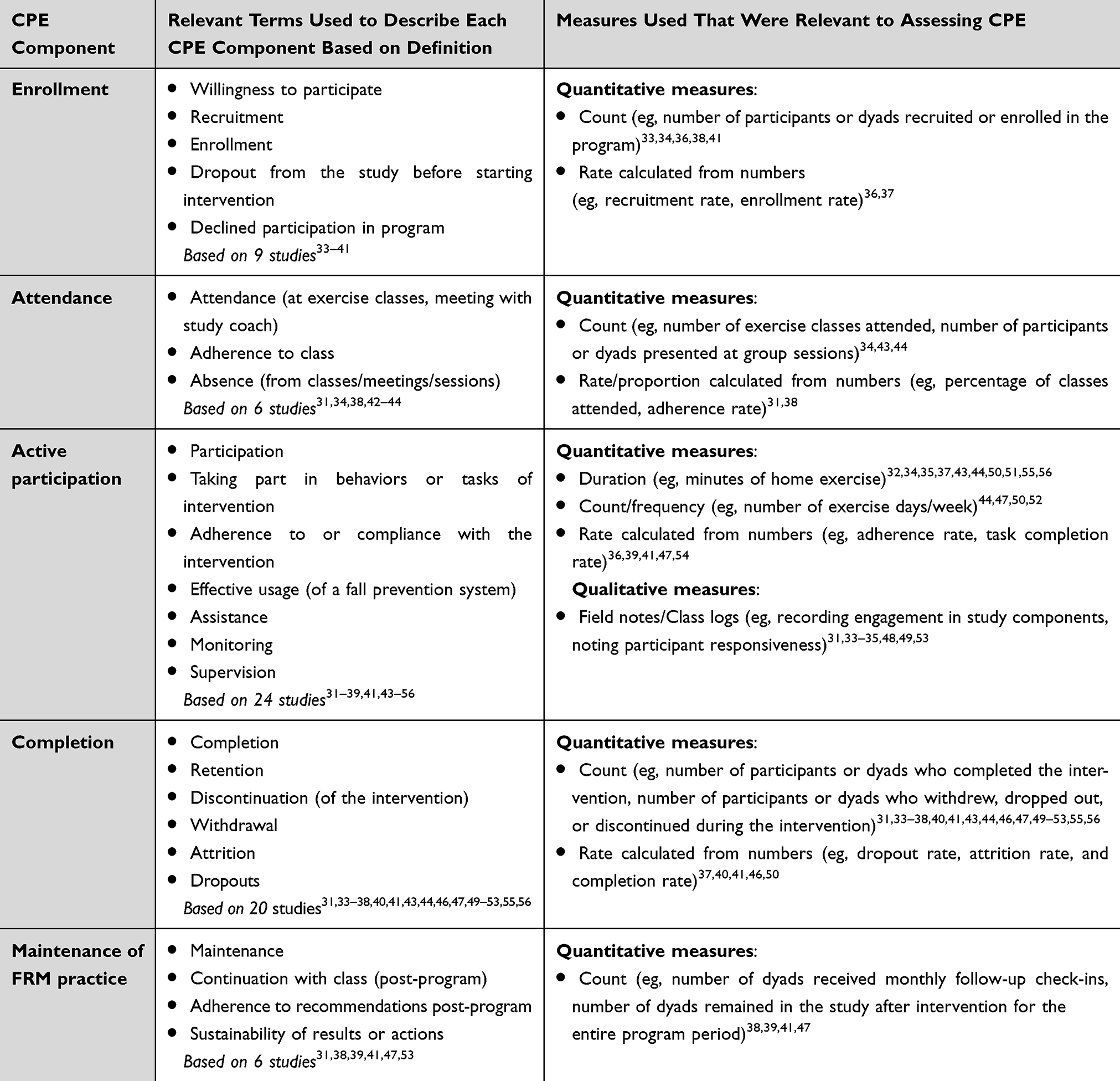 |
Table 3 Terms and Measures of Care Partner Engagement (CPE) Reported in Studies (n=32) |
CPE was measured both quantitatively and qualitatively in the studies (n=24). Quantitative measures of CPE included counts, frequencies, duration, and rates that reflected care partners’ behaviors. Examples of these measures include the number of care partners (and older people with CI) enrolled, the total number of minutes of a fall prevention system, and the percentage of participants who completed the tasks required by the FRM program. Quantitative measures were found across all five CPE components. Qualitative measures of CPE were only found in care partners’ active participation component, usually in the format of an observational diary recorded by care partners or subjective rating/field notes based on observations from program staff.
Aim 2: Facilitators and Barriers Associated with CPE
Table 4 presents a thematic summary of facilitators and barriers associated with CPE from 29 studies, with key findings organized into three categories: (1) older people with CI, (2) care partners, and (3) service providers (including interventionists and other program staff), programs, or organizations.
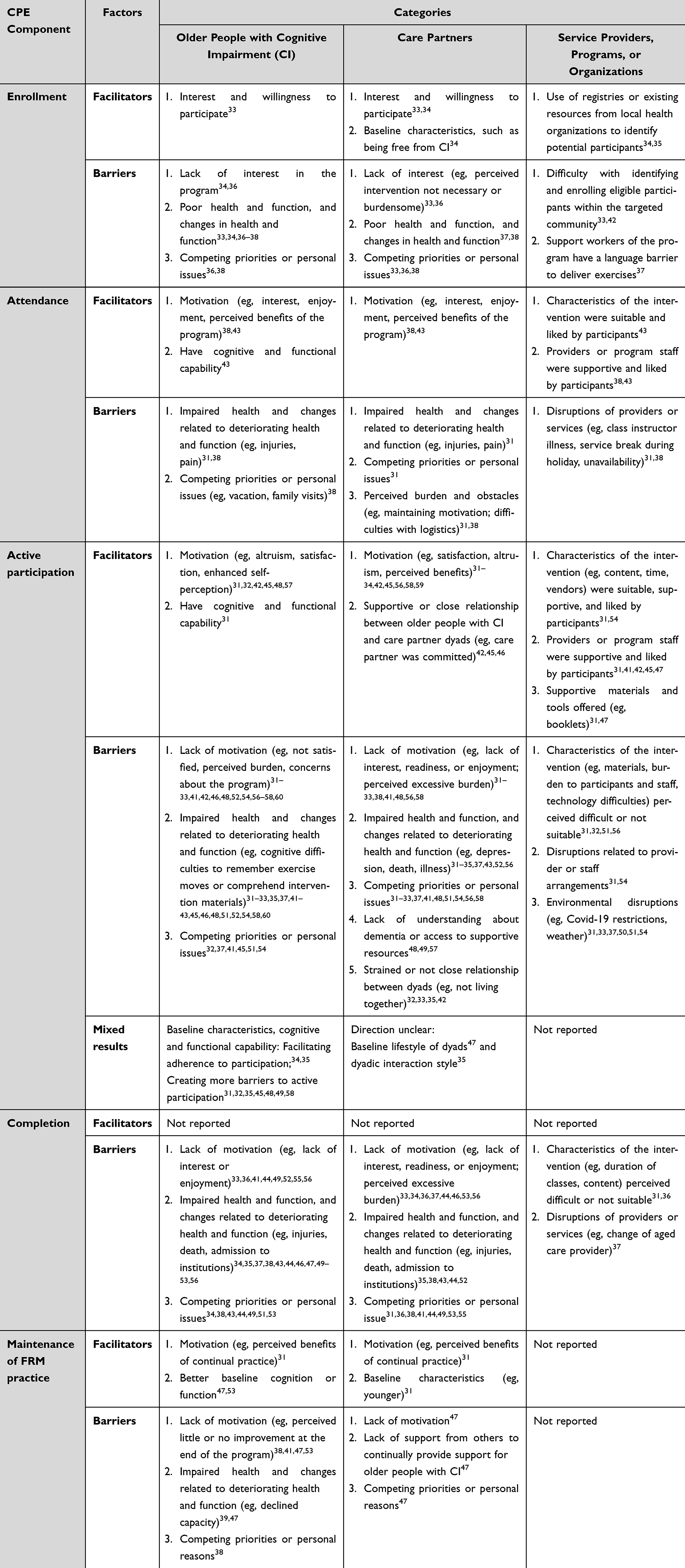 |
Table 4 Summary of Facilitators and Barriers to Care Partner Engagement (CPE) Reported in Studies (n=32) |
Results revealed similar patterns and themes of facilitators and barriers across the five CPE components, especially among care partners’ attendance, active participation, and completion. Themes that emerged in care partners’ enrollment and maintenance of FRM practice were distinct from themes related to the other three CPE components (ie, attendance, active participation, and completion). Meanwhile, a few factors (eg, older people with CI’s baseline high cognitive and functional capability, baseline healthy lifestyle of care partner and older people with CI dyads) yielded mixed or unclear results as CPE facilitators or barriers.
Care Partners’ Enrollment
Facilitators for care partners’ enrollment included the interest and willingness to participate in the FRM programs for both older people with CI33 and care partners.33,34 Baseline characteristics, such as the absence of CI for care partners, were an additional facilitator.34 For service providers, programs, or organizations, having established registries or existing resources for older people with CI in the community facilitated enrollment because those resources helped identify potentially eligible dyads.34,35
Some barriers to enrolling care partners (and older people with CI) were a lack of interest in the program,33,34,36 impaired health and function at baseline,33,34,36,37 changes in health and function (eg, medical illness and comorbidities that made them unable to enroll in the program),34,38 and competing priorities (eg, scheduling conflicts, time constraints).33,36,38 Another barrier to care partners’ enrollment was the difficulty programs and organizations faced in identifying eligible older people with CI and their care partners, particularly among underserved populations (eg, those with specific language needs) within service catchment areas or geographically isolated communities.33,37,42
Care Partners’ Attendance
Facilitators for care partners’ attendance were older people with CI and care partners’ motivation, including multiple aspects such as interest, enjoyment, and perceived benefits from the program.38,43 Unique facilitators included older people with CI’s cognitive and functional ability to carry out the intervention.43 For service providers, programs, or organizations, specific intervention design features (eg, structured group sessions, weekly monitoring calls) and additional support for staff time needed for program implementation contributed to greater buy-in for the program.38,43
The barriers to care partners’ attendance were similar to those for enrollment for both older people with CI and care partners, except for a lack of interest in the program, as this component focused on care partners’ presence at one or more program sessions rather than the entire FRM program. A unique barrier to care partners’ attendance was care partners’ perceived burden and obstacles to attend program sessions, for example, perceived challenges with following study logistics and maintaining their motivation.31,38 Disruptions of service providers or programs, such as service breaks during holidays and instructors’ illness or unavailability, also served as a barrier to care partners’ attendance.31,38
Care Partners’ Active Participation
Similar to attendance, themes for facilitators and barriers emerged in care partners’ active participation. Unique facilitators relevant to older people with CI included certain baseline characteristics that enhanced care partners’ motivation, such as older age, higher fall risk, and more advanced CI.34,35 Care partners’ commitment, cooperation, supportive nature, and positive relationship or close contact (eg, living together, frequent visits) with older people with CI served as important facilitators for active participation.42,45,46 An additional facilitator was the supportive materials and tools (eg, booklets, DVDs demonstrating exercise moves, a discussion tool) offered to care partners by the service providers or programs.32,47
In contrast to facilitators mentioned above, certain baseline characteristics of older people with CI, such as being older, more sedentary, and having elevated fall risk at baseline, were reported as barriers to care partners’ active participation.31,32,35,45,48,49,58 Unique barriers for care partners were their lack of understanding about dementia or limited access to resources and support,48,49,57 as well as strained relationships or not co-residing with older people with CI.32,33,35 Environmental disruptions such as weather changes and COVID-19 restrictions emerged as factors hindering care partners’ active participation.39,50,51
Care Partners’ Completion
No facilitators for care partners’ completion were identified. Similar to care partners’ attendance, barriers to care partners’ completion were the lack of motivation for both older people with CI and care partners. Care partners’ declining health and function, as well as transitioning to an institutional setting, also impeded their completion of the program.35,38,43,44,52 For service providers, programs or organizations, some barriers were the (1) intervention design features perceived by care partners as not suitable or difficult (eg, Tai Chi was perceived as a boring activity by some dyads) and (2) disruptions in service coverage where FRM programs were embedded, which hindered program completion.31,36,39
Care Partners’ Maintenance of FRM Practice
Facilitators for care partners’ maintenance of FRM practice include older people with CI and care partners’ motivation, such as their perceived benefits of continuing FRM behaviors and recommendations following the program completion.31 Certain baseline characteristics of older people with CI (eg, higher cognitive functioning and better health) and care partners (eg, younger age) also facilitated the maintenance of FRM practice.31,47,53
Barriers to care partners’ maintenance of FRM practice were similar to those associated with other components of CPE. A unique barrier for this CPE component was a lack of support from others to continue supporting older people with CI after the intervention commenced.47 The included studies did not report any facilitators or barriers to care partners’ maintenance of FRM practice that were relevant to service providers, programs, or organizations.
Aim 3: Strategies for and Their Effects on Enhancing CPE
We identified a total of 18 strategies relevant to CPE that were reported or discussed across 26 studies (see Table 5). However, none of these studies explicitly claimed that these strategies were employed with the intention of enhancing CPE within FRM programs. Therefore, it was often unclear whether these effects were directly attributable to the reported strategies. We found positive effects reported on four strategies. Seven strategies yielded mixed effects. The remaining seven strategies had no reported effects.
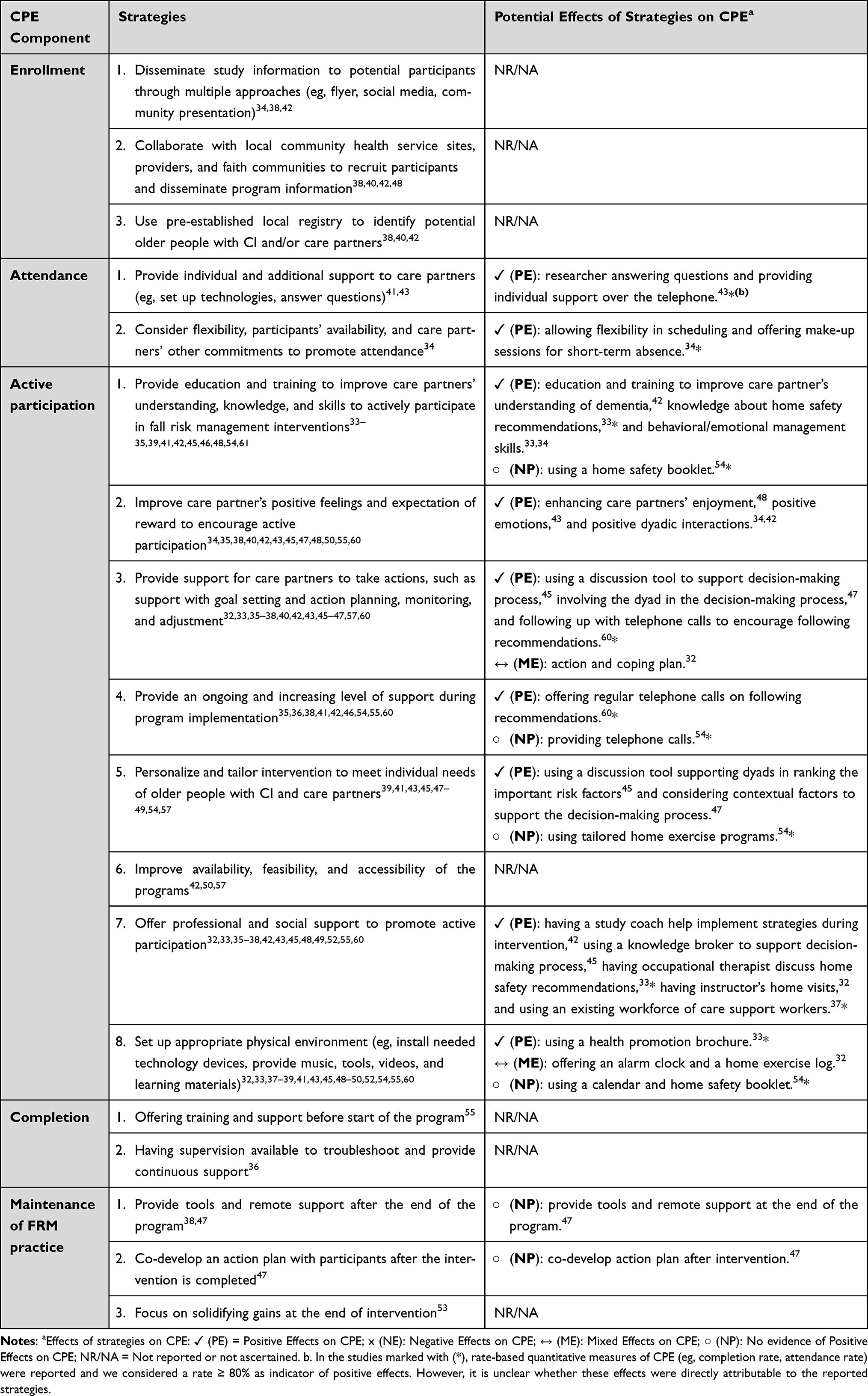 |
Table 5 Strategies Used That Were Relevant to Care Partner Engagement (CPE) and Effects |
Care Partners’ Enrollment
Multiple recruitment strategies were reported to enhance care partners’ enrollment. These strategies included (1) disseminating study information via various venues (eg, distributing flyers, presenting program information at caregiver support groups) to reach care partners in the community;34,38,42 (2) collaborating with local service agencies to develop recruitment resources and brainstorm strategies for disseminating program information,38,40,42,48 and (3) using pre-established registries to identify potential older people with CI and/or care partners.38,40,42 No studies examined or reported the effects of these strategies on CPE.
Care Partners’ Attendance
Strategies relevant to care partners’ attendance included providing assistance and offering support to care partners to promote attendance.41,43 An additional strategy to improve attendance was offering flexibility in program schedules and having make-up sessions for short-term absences for appropriate reasons.34 We found positive effects of all these strategies on enhancing attendance of care partners and older people with CI dyads.
Care Partners’ Active Participation
Compared to other CPE components, a majority of identified strategies fell under care partners’ active participation. Most strategies involved behavioral change techniques, which are “observable and replicable components” designed for behavior changes, such as goal setting and restructuring the physical environment.62 We identified eight key behavioral change strategies for care partners’ active participation.
Although only 11 studies examined or reported the effects of these strategies on CPE, we identified positive effects reported on seven out of eight strategies. One study adopted multiple strategies but reported no evidence of positive effects.54 In another study, care partners expressed different opinions (eg, helpful vs burdensome) on several strategies, such as action plans and the use of an alarm clock.32
Care Partners’ Completion
Two main strategies were identified as relevant to care partners’ completion. The first strategy involved providing training and assistance to older people with CI and care partners with program setups, orientation on system use, and answering questions at the beginning of the program.55 The second strategy was to offer regular supervision and technical support throughout the entire program implementation to troubleshoot any issues.36 The effects of these strategies on CPE were not reported in the studies.
Care Partners’ Maintenance of FRM Practice
Three strategies were identified relevant to care partners’ maintenance of FRM practice, including (1) providing tools and support, such as offering an illustrated brochure with the movement exercises practiced in class, and maintaining phone contact if needed;38,47 (2) co-developing an action plan with older people with CI and care partners to maintain actions;47 and (3) focusing on solidifying gains from the program to motivate their continual maintenance.53 One study examined the effects of the maintenance strategies, but it did not endorse any positive effect on CPE.47
Discussion
This systematic review provides a comprehensive overview of current evidence on CPE in FRM programs for community-dwelling older people with CI. Our examination of CPE terms and measures revealed conceptual ambiguity and heterogeneity in the definition and measurement of CPE. Our proposal of a five-component CPE conceptual framework addressed these gaps, providing a foundation for future research and intervention design that engages care partners. Facilitators and barriers to CPE were identified and categorized into three groups, with some factors shared across multiple CPE components (eg, care partners’ attendance, active participation, and completion) and others unique to specific components. Additionally, various strategies to enhance CPE were summarized, some of which demonstrated positive effects in improving CPE. Despite the common practice of involving care partners in these programs, facilitators, barriers, and CPE enhancement strategies remain underrecognized and inconsistently evaluated, underscoring the need for more rigorous and systematic investigation in this area.
Aim 1: Terms and Measures of CPE
Although engaging care partners in FRM programs for older people with CI is a common practice, our review revealed persistent conceptual ambiguity in how CPE was defined and measured. This lack of clarity, reflected in considerable heterogeneity in CPE terms used, may stem from the diverse and evolving roles that care partners assume in FRM throughout the caregiving trajectory,16 as well as from differences in FRM program targets, each addressing distinct fall risk factors and thereby requiring varying forms of CPE.10 For example, exercise programs may require care partners to attend exercise classes and supervise the safe movement of older people with CI,37,41 while home hazard reduction programs may involve care partners actively identifying and modifying fall risk in the home environment.33 Additionally, certain terms, adherence in particular, were applied across multiple CPE components without explicit definitions, making it difficult to discern the specific behaviors of CPE. As such, our proposed definitions of CPE and its five components contribute to the field by offering a novel conceptual framework to distinguish and characterize CPE in FRM programs with different foci.
Similarly, there was a considerable variability in how CPE was assessed across FRM programs. The reliance on unvalidated, self-reported measures completed by care partners or observational notes from program staff may place additional burdens on care partners and program staff and introduce potential biases (eg, recall bias, social desirability bias). Capturing CPE as the joint behavioral participation of older people with CI and care partner dyads reflected the relational nature of CPE described in prior studies.14–16 However, this dyadic approach may obscure the distinct assessment of care partners’ individual engagement levels.54 Failing to measure the care partner’s role independently can limit our understanding of how their specific actions and motivations contribute to intervention outcomes. Therefore, future research should consider incorporating individual-level metrics to more accurately capture care partners’ unique engagement patterns.
Aim 2: Facilitators and Barriers Associated with CPE
The grouping of facilitators and barriers to CPE into three categories (ie, older people with CI, care partners, and service providers or programs) highlights the relational and multi-dimensional nature of CPE.16 This shows that interventions that incorporate CPE must be designed with an appreciation for individual, relational, and systemic factors. In addition, four recurring patterns (ie, motivation, support, health and function status or changes, intervention characteristics) emerged across multiple CPE components (ie, care partners’ attendance, active participation, and completion), while the care partners’ enrollment component received less attention and was associated with a unique set of factors, such as difficulty with participant identification and recruitment from targeted community.
Our findings highlighted motivation as a critical driver for enhancing CPE for both older people with CI and their care partners. Motivation refers to all those brain processes that energize and direct behaviors, including habitual processes, emotional responding, and analytical decision-making.63 Prior research has emphasized the role of motivation for older people with CI, especially perceived benefits and support of FRM programs, as a key enabler to their active participation in FRM programs;64 however, our review expands this perspective by demonstrating that care partners’ motivations are also influential. Importantly, our review identified various types of motivations, such as interest, willingness, enjoyment, satisfaction, and perceived benefits. This echoes findings from a prior review suggesting that varying motivations were reported by care partners when supporting FRM for older people with CI.13 These motivators include maintaining or improving the health and well-being of both older people with CI and care partners themselves, improving their care relationship, and having some practical support that strengthens older people with CI’s confidence and independence. However, these motivators were not always directly relevant to reducing their risk of falls and fall-related injuries.13
Support, in its many forms and sources, is another essential determinant for sustaining the engagement of care partners across the FRM programs. Support was multi-faceted, encompassing physical, educational, professional, and social dimensions. This finding is consistent with existing research that, while care partners play an important role in facilitating the participation of older people with CI in FRM programs, they often struggle with their responsibilities due to limited access to external support resources,13,64 need multiple sources of support,65 and experience inadequate support from healthcare and service providers.66 Without sufficient support and training, care partners may face various challenges in selecting and adopting FRM strategies that are the most appropriate and effective,12 and could even cause injuries to themselves.67 Another recent study also supported our findings, revealing that care partners often experience a gradual and continuing negative impact of falls on their emotional, physical, and financial well-being, calling for more comprehensive services and supports, such as mental health services, caregiving training, affordable home modification programs, and resources to access paid clinical care.68 Addressing these gaps could mitigate the multifaceted burden experienced by care partners and improve outcomes for both care partners and older people with CI.
Health-related factors of both older people with CI and care partners (eg, their illness, declines in health and function, transition to residential care, and death) can disrupt CPE across multiple phases of the programs. The dual burden of care partners managing their own health while supporting the complex needs of older people with CI is often under-recognized in program design.69,70 Our study findings underscore the necessity for programs to have integrated and coordinated service systems that address the complex health and care needs of older people with CI, while also offering comprehensive training and support for care partners.70 Future programs may consider comorbidity management approaches and provide care partners with opportunities to share their concerns and priorities related to FRM and broader caregiving responsibilities, collaborate with service providers to agree on acceptable levels of burden and risk, receive support in coordinating care across clinical and community-based service settings, and be equipped with resources to strengthen their capacity for FRM.71,72
Our study findings also revealed the influence of service provider-, program-, and organization-level factors in either facilitating or hindering CPE. Earlier CPE frameworks like Carman et al’s advocated for integrating patient and care partners’ values and perspectives into the organizational design and program development,16 yet the perceived fit and suitability of the program (eg, program design, content, and support received from program or service staff) can be highly subjective and based on their specific situations. This points to a critical need for greater flexibility in program design and a person-centered approach to tailoring program offerings to the diverse needs of participants.70,73,74 Moreover, persistent barriers to service access existed, including technology difficulties, transportation challenges, financial burden, and time constraints, highlighting the systemic inequities that disproportionately impact older people with CI and care partners with limited resources. These barriers are not only common in the broader characteristics of FRM programs for older adults,75 but are also evident in our included studies, where older people with CI and care partners from racial/ethnic minoritized groups, living in rural areas, or having lower socioeconomic status were underrepresented. Addressing these gaps requires increased and continuous support from service providers, programs, or organizations to ensure equitable access and engagement in services.
We also identified that two components—care partners’ enrollment and maintenance of FRM practices—are underexplored in the intervention studies and are associated with unique sets of factors. The unique challenges for FRM programs and providers to identify and enroll care partners from geographically isolated areas or within minoritized communities are significant,33,37,42 suggesting that current interventions may not be sufficiently designed to reach these underserved populations. Our findings also indicate the necessity of continued support to motivate and enable care partners to sustain behavioral engagement following the conclusion of services and support.41 These findings underscore the importance of distinguishing between behavioral initiation and behavioral maintenance in engaging care partners in FRM,76 particularly in the context of the prolonged caregiving trajectory associated with CI.77
Aim 3: Strategies for and Their Effects on Enhancing CPE
While our review identified a variety of strategies aimed at enhancing CPE, from boosting motivation and providing multidimensional support to facilitating goal setting and participation monitoring, the effectiveness of these approaches appears highly dependent on the context. The interconnection between strategies and the previously identified facilitators and barriers points to multiple promising mechanisms of behavior change that warrant further investigation.78
Notably, several other strategies yielded mixed effects or had no evidence of positive effects, particularly those that involved providing care partners with specific tools or materials. This pattern raises an important consideration: the design of FRM programs needs to adequately consider the cognitive capacity and emotional load of older people with CI and care partners, without overburdening participants with excessive information and stringent requirements.33,37,38 As suggested by prior studies, intervention designers must improve the program’s user-friendliness to enable care partners to provide more effective and sustained support to older people with CI.11,56,79 Simplifying program logistics presents a promising avenue for enhancing engagement; studies that introduced flexible scheduling and integrated interventions into daily caregiving routines reported better adherence and fewer disruptions.32,34
We also found that care partners’ enrollment and maintenance of FRM practice were associated with unique CPE enhancement strategies. However, none of these strategies was particularly evaluated. Without targeted approaches to support the initial and sustained engagement, FRM programs may fail to achieve their intended reach, impact, and sustainability.
Overall Discussion Across Study Aims
Across all three study aims, our review revealed a general lack of systematic examination and discussion of CPE in the existing literature. Only two studies explicitly identified facilitators and barriers to CPE as part of their primary research questions, indicating that care partners’ roles and engagement are often under-recognized in these programs. In many cases, facilitators and barriers were reported only briefly and ambiguously, often noted as annotations in study flowcharts (eg, “personal reasons”, “other reasons”) without further elaboration or contextualization. This lack of detail limits the interpretability of the findings. This pattern is also noted through the uneven attention given to different CPE components; for example, no facilitators were mentioned under the care partners’ completion component, and organizational factors were not identified in the maintenance of FRM practice component. Furthermore, evaluation of strategies to enhance CPE was similarly limited, with promising effects often mentioned only briefly in discussion sections of the included studies and rarely supported by robust empirical evidence. These gaps suggest that the effectiveness of CPE enhancement strategies remains underexplored and underreported, raising concerns about the reliability and generalizability of current recommendations. Importantly, the majority of findings in this review were derived from the qualitative study components, many of which were of relatively low methodological quality. Collectively, these findings underscore the urgent need for more systematic, high-quality research in this area.
Implications
The current systematic review points out critical gaps in the literature concerning CPE in FRM programs for community-dwelling older people with CI. First, the heterogeneity and inconsistency in how CPE was defined and measured reflect the complexity of the construct and the need for conceptual clarity in its application within FRM programs. Although our proposed CPE framework is an attempt to provide a conceptual foundation for harmonizing different studies, future research should further validate and expand our proposed conceptual framework to ensure a comprehensive understanding of CPE. The improved framework can also inform the development and validation of brief and clinically practical measures of CPE, without assuming concordance within dyads. Future research is also needed to develop and validate objective and multimodal measures of CPE (eg, technology-based behavioral tracking data, video, or sensory data) that integrate multiple data sources to enhance measurement reliability, along with reducing the reporting burden on care partners.80,81
Second, future research should further examine how different types of motivations, supports, comorbidity management approaches, and access to services can facilitate or hinder CPE in FRM programs for older people with CI. To better understand the factors influencing care partners’ enrollment in FRM programs and the maintenance of their practice post-intervention, future research should examine how various factors are associated with both behavioral initiation and maintenance among care partners.76
Third, our review identified a range of promising mechanisms of behavioral changes (ie, strategies to enhance motivations and provide multidimensional support) for CPE that require further examination in future FRM programs. Given the importance of both the intervention features and implementation processes to optimize CPE in FRM programs, care partners and older people with CI should be involved in co-developing and implementing these FRM programs.82 Conceptual frameworks of Intervention Taxonomy83 may be used to describe and refine intervention design and implementation strategies. Importantly, rigorous evaluations are needed to assess how different engagement strategies impact CPE and how CPE may serve as a critical mechanism that improves older people with CI’s adherence, long-term improvements in fall-related outcomes, and overall well-being for both older people with CI and their care partners.
Fourth, in terms of enrollment, strategies to proactively identify and reach care partners are urgently needed, especially for those who may not be aware of fall risk among older people with CI and those who are underserved. A public health approach may be utilized, such as enhancing access to cognitive screening, improving the availability and visibility of local community programs, and increasing public awareness about dementia and fall risk, which may facilitate earlier identification and support of at-risk dyads and encourage care partners’ enrollment in FRM programs.84
Lastly, the lack of attention on supporting care partners’ maintenance of FRM practice post-intervention calls for a paradigm shift. FRM programs should not be treated as “one and done” interventions.84 In order to ensure a supportive environment and promote long-term success, FRM programs should incorporate follow-up support, longitudinal engagement, capacity building for care partners and older people with CI, and connecting care partners with external support systems, such as secondary care partners, community volunteers, and online support programs.
Limitations
Our review has several limitations. First, we extracted the CPE terms, measures, factors, and strategies based solely on what was explicitly reported in the included studies, which were often insufficiently described. As a result, we could not analyze information that was not systematically collected and reported in these FRM programs. For studies that only reported CPE-related information on the dyadic level, our extraction and analyses were limited as we used dyad-level information as a proxy for CPE. Second, we conducted the analysis based on our predefined CPE concept and components based on existing literature. Other care partners’ behaviors that were not aligned with our conceptual framework were not included in our analysis. For example, some care partners may notice certain parts of FRM programs not working well and find alternatives on their own.85,86 Such behaviors may not be captured under our current framework. Third, our search was limited to English-language publications, and mostly were programs from countries in the Global North. As a result, we may have excluded evidence from programs developed and implemented in non-English-speaking regions and practices in diverse cultural and healthcare contexts. Lastly, given the limited research and the moderate to low methodological quality of the primarily qualitative data analyzed, our findings should be interpreted with caution (eg, the use of a threshold of 80% to determine effectiveness was arbitrary87) and require further validation through future mixed-methods research aimed at developing and testing strategies to enhance CPE in FRM programs for older people with CI.
Conclusion
Despite the scarcity of systematic investigations on CPE in FRM programs for community-dwelling older people with CI, this review introduces a novel conceptual framework that clarifies the multidimensional nature of CPE and guides the inquiry. By identifying terms and measures used to characterize CPE, delineating facilitators and barriers to CPE, and summarizing strategies employed to enhance CPE within FRM programs for older people with CI, we achieved our three study aims and highlighted the under-recognized engagement of care partners in FRM programs for older people with CI. Our findings advance theoretical understanding of CPE, inform the design of care-partner-engaged FRM programs for community-dwelling older people with CI, and offer valuable implications for developing and implementing evidence-based strategies that foster care partner engagement in dementia care.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Web–based Injury Statistics Query and Reporting System (WISQARS). Available from: https://wisqars.cdc.gov/.
2. Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL. Interventions to prevent falls in older adults: updated evidence report and systematic review for the US preventive services task force. JAMA. 2018;319(16):1705. doi:10.1001/jama.2017.21962
3. Minta K, Colombo G, Taylor WR, Schinazi VR. Differences in fall-related characteristics across cognitive disorders. Front Aging Neurosci. 2023;15:1171306. doi:10.3389/fnagi.2023.1171306
4. Muir SW, Gopaul K, Montero Odasso MM. The role of cognitive impairment in fall risk among older adults: a systematic review and meta-analysis. Age Ageing. 2012;41(3):299–308. doi:10.1093/ageing/afs012
5. Racey M, Markle-Reid M, Fitzpatrick-Lewis D, et al. Fall prevention in community-dwelling adults with mild to moderate cognitive impairment: a systematic review and meta-analysis. BMC Geriatr. 2021;21(1):689. doi:10.1186/s12877-021-02641-9
6. Allan LM, Ballard CG, Rowan EN, Kenny RA. Incidence and prediction of falls in dementia: a prospective study in older people. PLoS One. 2009;4(5):e5521. doi:10.1371/journal.pone.0005521
7. Ansai JH, Andrade LPD, Masse FAA, et al. Risk factors for falls in older adults with mild cognitive impairment and mild Alzheimer Disease. J Geriatr Phys Ther. 2019;42(3):E116–E121. doi:10.1519/JPT.0000000000000135
8. Zhou Y, Choi NG, Sadak T, Ghosh N, Phelan EA. Association between pain and fall worry among community-dwelling older people with cognitive impairment in the United States. Innov Aging. 2023;7(10):igad100. doi:10.1093/geroni/igad100
9. Peek K, Bryant J, Carey M, et al. Reducing falls among people living with dementia: a systematic review. Dementia. 2020;19(5):1621–1640. doi:10.1177/1471301218803201
10. Zhou Y, Berridge C, Hooyman NR, Sadak T, Mroz TM, Phelan EA. Development of a behavioural framework for dementia care partners’ fall risk management. BMC Geriatr. 2022;22(1):975. doi:10.1186/s12877-022-03620-4
11. Sultana M, Alexander N, Pierucini-Faria F, et al. Involvement of informal caregivers in preventing falls in older adults with cognitive impairment: a rapid review. J Alzheimers Dis. 2023;92(3):741–750. doi:10.3233/JAD-221142
12. Zhou Y, Berridge C, Hooyman N, et al. Care partners’ engagement in preventing falls for community-dwelling older people with dementia. Gerontologist. 2024;64(8):gnae064. doi:10.1093/geront/gnae064
13. Zhou Y, Strayer AT, Phelan EA, Sadak T, Hooyman NR. A mixed methods systematic review of informal caregivers’ experiences of fall risk among community‐dwelling elders with dementia. Health Soc Care Community. 2021;29(4):1126–1144. doi:10.1111/hsc.13148
14. Levoy K, Rivera E, McHugh M, Hanlon A, Hirschman KB, Naylor MD. Caregiver engagement enhances outcomes among randomized control trials of transitional care interventions: a systematic review and meta-analysis. Med Care. 2022;60(7):519–529. doi:10.1097/MLR.0000000000001728
15. Todorova I, Turner H, Castaneda-Sceppa C, Young D, Bonner A. “I do it with love”: engagement in caring for people with dementia. Glob Qual Nurs Res. 2016;3:2333393616668634. doi:10.1177/2333393616668634
16. Carman KL, Dardess P, Maurer M, et al. Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Affairs. 2013;32(2):223–231. doi:10.1377/hlthaff.2012.1133
17. Haine-Schlagel R, Dickson KS, Lind T, et al. Caregiver participation engagement in child mental health prevention programs: a systematic review. Prev Sci. 2022;23(2):321–339. doi:10.1007/s11121-021-01303-x
18. Holmes Rovner M, French M, Sofaer S, Shaller D, Kanouse D, Prager D. A new definition of patient engagement: what is engagement and why is it important? In: Center for Advancing Health. Washington, DC; 2010.
19. Staudt M. Treatment engagement with caregivers of at-risk children: gaps in research and conceptualization. J Child Fam Stud. 2007;16(2):183–196. doi:10.1007/s10826-006-9077-2
20. Noonan MC, Wingham J, Dalal HM, Taylor RS. Involving caregivers in self‐management interventions for patients with heart failure and chronic obstructive pulmonary disease. A systematic review and meta‐analysis. J Adv Nurs. 2019;75(12):3331–3345. doi:10.1111/jan.14172
21. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
22. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:n71. doi:10.1136/bmj.n71.
23. Garcia L, Mendonça G, Benedetti TRB, et al. Barriers and facilitators of domain-specific physical activity: a systematic review of reviews. BMC Public Health. 2022;22(1):1964. doi:10.1186/s12889-022-14385-1
24. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
25. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
26. Stern C, Lizarondo L, Carrier J, et al. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid Synth. 2020;18(10):2108–2118. doi:10.11124/JBISRIR-D-19-00169
27. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45. doi:10.1186/1471-2288-8-45
28. Burnier M. Is there a threshold for medication adherence? Lessons learnt from electronic monitoring of drug adherence. Front Pharmacol. 2019;9:1540. doi:10.3389/fphar.2018.01540
29. Mercadante AR, Lee S, Uh K, et al. Impact of adherence goal awareness intervention on PDC in various settings: does awareness help modify medication-taking behavior? Explor Res Clin Soc Pharm. 2021;4:100072. doi:10.1016/j.rcsop.2021.100072
30. Hong QN, Fàbregues S, Bartlett G, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. EFI. 2018;34(4):285–291. doi:10.3233/EFI-180221
31. Barrado-Martín Y, Heward M, Polman R, Nyman SR. Adherence to the class-based component of a Tai Chi exercise intervention for people living with dementia and their informal carers. J Aging Phys Act. 2021;29(5):721–734. doi:10.1123/japa.2020-0119
32. Barrado-Martín Y, Heward M, Polman R, Nyman SR. People living with dementia and their family carers’ adherence to home-based Tai Chi practice. Dementia. 2021;20(5):1586–1603. doi:10.1177/1471301220957758
33. Wesson J, Clemson L, Brodaty H, et al. A feasibility study and pilot randomised trial of a tailored prevention program to reduce falls in older people with mild dementia. BMC Geriatr. 2013;13(1):89. doi:10.1186/1471-2318-13-89
34. Yao L, Giordani BJ, Algase DL, You M, Alexander NB. Fall risk-relevant functional mobility outcomes in dementia following dyadic Tai Chi exercise. West J Nurs Res. 2013;35(3):281–296. doi:10.1177/0193945912443319
35. Teri L, McCurry SM, Buchner DM, et al. Exercise and activity level in Alzheimer’s disease: a potential treatment focus. J Rehabil Res Dev. 1998;35.
36. Park J, Heilman KJ, Sullivan M, et al. Remotely supervised home-based online chair yoga intervention for older adults with dementia: feasibility study. Complement Ther Clin Pract. 2022;48:101617. doi:10.1016/j.ctcp.2022.101617
37. Lee DCA, Haines TP, Callisaya ML, Hill KD. A scalable program for improving physical activity in older people with dementia including culturally and linguistically diverse (CALD) groups who receive home support: a feasibility study. IJERPH. 2023;20(4):3662. doi:10.3390/ijerph20043662
38. Mehling WE, Scott TM, Duffy J, et al. Dyadic group exercises for persons with memory deficits and care partners: mixed-method findings from the paired preventing loss of Independence through exercise (PLIÉ) randomized trial. JAD. 2020;78(4):1689–1706. doi:10.3233/JAD-200713
39. Lee DCA, Burton E, Meyer C, et al. The potential for effect of a six-week training program for gait aid use in older people with dementia with unsteadiness of gait: a pilot study. JCM. 2023;12(4):1574. doi:10.3390/jcm12041574
40. Goldberg SE, Van Der Wardt V, Brand A, et al. Promoting activity, Independence and stability in early dementia (PrAISED): a multisite, randomised controlled, feasibility trial. BMC Geriatr. 2019;19(1):353. doi:10.1186/s12877-019-1379-5
41. Sari YM, Burton E, Lee DCA, Hill KD. A telehealth home-based exercise program for community-dwelling older people with dementia in Indonesia: a feasibility study. IJERPH. 2023;20(4):3397. doi:10.3390/ijerph20043397
42. McCurry SM, Logsdon RG, Pike KC, LaFazia DM, Teri L. Training Area Agencies on Aging case managers to improve physical function, mood, and behavior in persons with dementia and caregivers: examples from the RDAD-northwest study. J Gerontol Soc Work. 2018;61(1):45–60. doi:10.1080/01634372.2017.1400486
43. Yao L, Giordani B, Alexander NB. Developing a positive emotion–motivated Tai Chi (PEM-TC) exercise program for older adults with dementia. Res Theory Nurs Pract. 2008;22(4):241–255. doi:10.1891/1541-6577.22.4.241
44. Nyman SR, Ingram W, Sanders J, et al. Randomised controlled trial of the effect of Tai Chi on postural balance of people with dementia. CIA. 2019;14:2017–2029. doi:10.2147/CIA.S228931
45. Meyer C, Hill S, Hill KD, Dow B. Inclusive decision making for falls prevention: a discussion tool for use with people with dementia and their caregivers. J Aging Phys Act. 2019;27(5):711–718. doi:10.1123/japa.2018-0167
46. Suttanon P, Hill KD, Said CM, et al. Feasibility, safety and preliminary evidence of the effectiveness of a home-based exercise programme for older people with Alzheimer’s disease: a pilot randomized controlled trial. Clin Rehabil. 2013;27(5):427–438. doi:10.1177/0269215512460877
47. Meyer C, Hill KD, Hill S, Dow B. Falls prevention for people with dementia: a knowledge translation intervention. Dementia. 2020;19(7):2267–2293. doi:10.1177/1471301218819651
48. Francis-Coad J, Weselman T, Burton E, Beilby J, Hill AM. Fall prevention education co-designed and evaluated with community-dwelling older people living with dementia and their caregivers: a feasibility study. Health Soc Care Community. 2023;2023:1–13. doi:10.1155/2023/9965507
49. Suominen MH, Puranen TM, Jyväkorpi SK, et al. Nutritional guidance improves nutrient intake and quality of life, and may prevent falls in aged persons with Alzheimer disease living with a spouse (NuAD trial). J Nutr Health Aging. 2015;19(9):901–907. doi:10.1007/s12603-015-0558-0
50. Harwood RH, Goldberg SE, Brand A, et al. Promoting activity, Independence and stability in early dementia and mild cognitive impairment (PrAISED): a randomised controlled trial. BMJ. 2023;2023:382. doi:10.1136/bmj-2023-074787
51. Taylor ME, Close JCT, Lord SR, et al. Pilot feasibility study of a home‐based fall prevention exercise program (StandingTall) delivered through a tablet computer (iPad) in older people with dementia. Australas J Ageing. 2020;39(3). doi:10.1111/ajag.12717
52. Pitkälä KH, Pöysti MM, Laakkonen ML, et al. Effects of the Finnish Alzheimer Disease exercise trial (FINALEX): a randomized controlled trial. JAMA Intern Med. 2013;173(10):894. doi:10.1001/jamainternmed.2013.359
53. Teri L, Gibbons LE, McCurry SM, et al. Exercise plus behavioral management in patients with Alzheimer Disease: a randomized controlled trial. JAMA. 2003;290(15):2015. doi:10.1001/jama.290.15.2015
54. Taylor ME, Wesson J, Sherrington C, et al. Tailored exercise and home hazard reduction program for fall prevention in older people with cognitive impairment: the i-FOCIS randomized controlled trial. J Gerontol Biol Sci Med Sci. 2021;76(4):655–665. doi:10.1093/gerona/glaa241
55. Padala KP, Padala PR, Lensing SY, et al. Home-based exercise program improves balance and fear of falling in community-dwelling older adults with mild Alzheimer’s Disease: a pilot study. JAD. 2017;59(2):565–574. doi:10.3233/JAD-170120
56. Hattink BJJ, Meiland FJM, Overmars-Marx T, et al. The electronic, personalizable Rosetta system for dementia care: exploring the user-friendliness, usefulness and impact. Disabil Rehabil Assist Technol. 2016;11(1):61–71. doi:10.3109/17483107.2014.932022
57. Mackintosh SF, Sheppard LA. A pilot falls-prevention programme for older people with dementia from a predominantly Italian background. Hong Kong Physiother J. 2005;23(1):20–26. doi:10.1016/S1013-7025(09)70055-7
58. Chou HK, Yan SH, Lin IC, Tsai MT, Chen CC, Woung LC. A pilot study of the telecare medical support system as an intervention in dementia care: the views and experiences of primary caregivers. J Nurs Res. 2012;20(3):169–180. doi:10.1097/jnr.0b013e318263d916
59. Taraldsen K, Boulton E, Helbostad JL, Saltvedt I, Granbo R. Client, caregiver, volunteer, and therapist views on a voluntary supported group exercise programme for older adults with dementia. BMC Geriatr. 2020;20(1):235. doi:10.1186/s12877-020-01632-6
60. Mahoney JE, Shea TA, Przybelski R, et al. Kenosha County falls prevention study: a randomized, controlled trial of an intermediate‐intensity, community‐based multifactorial falls intervention. J Am Geriatr Soc. 2007;55(4):489–498. doi:10.1111/j.1532-5415.2007.01144.x
61. Perttila NM, Öhman H, Strandberg TE, et al. Effect of exercise on drug-related falls among persons with Alzheimer’s Disease: a secondary analysis of the FINALEX study. Drugs Aging. 2018;35(11):1017–1023. doi:10.1007/s40266-018-0594-7
62. Michie S, Wood CE, Johnston M, Abraham C, Francis JJ, Hardeman W. Behaviour change techniques: the development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol Assess. 2015;19(99):1–188. doi:10.3310/hta19990
63. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):42. doi:10.1186/1748-5908-6-42
64. Booth V, Harwood R, Hancox JE, Hood-Moore V, Masud T, Logan P. Motivation as a mechanism underpinning exercise-based falls prevention programmes for older adults with cognitive impairment: a realist review. BMJ Open. 2019;9(6):e024982. doi:10.1136/bmjopen-2018-024982
65. Meyer C, Dow B, Hill KD, Tinney J, Hill S. “The right way at the right time”: insights on the uptake of falls prevention strategies from people with dementia and their caregivers. Front Public Health. 2016;4. doi:10.3389/fpubh.2016.00244
66. Zhou Y, Thakkar N, Phelan EA, et al. How do care partners overcome the challenges associated with falls of community-dwelling older people with dementia? A qualitative study. Dementia. 2024;23(7):1152–1171. doi:10.1177/14713012241267137
67. Gomes NP, Pedreira LC, Gomes NP, Fonseca EDOS, Reis LAD, Santos ADA. Health-related consequences of caring for dependent relatives in older adult caregivers. Rev Esc Enferm USP. 2019; 53:e03446. doi:10.1590/s1980-220x2018002303446
68. Zhou Y, Meyer K, Irani E, Liu X, Choi N. Change in fall status of older people with dementia and caregiving difficulties: moderation effects of living arrangements. J Am Geriatr Soc. 2025;
69. Layton N, Lalor A, Slatyer S, et al. Who cares for the carer? Codesigning a carer health and wellbeing clinic for older care partners of older people in Australia. Health Expect. 2023;26(6):2644–2654. doi:10.1111/hex.13863
70. Fields B, Golden BP, Perepezko K, Wyman M, Griffin JM. Optimizing better health and care for older adults and their family caregivers: a review of geriatric approaches. J Am Geriatr Soc. 2024;72(12):3936–3940. doi:10.1111/jgs.19061
71. Handley M, Windle G, Mathie E, et al. Living with dementia and other long-term conditions: what works for patient-caregiver dyads? A realist review. Aging Mental Health. 2025:1–11. doi:10.1080/13607863.2025.2478168.
72. Ma D, Wang Y, Zhao Y, et al. How to manage comorbidities in people with dementia: a scoping review. Ageing Res Rev. 2023;88:101937. doi:10.1016/j.arr.2023.101937
73. Hackett K, Sabat SR, Giovannetti T. A person-centered framework for designing music-based therapeutic studies in dementia: current barriers and a path forward. Aging Mental Health. 2022;26(5):940–949. doi:10.1080/13607863.2021.1931029
74. Wu Q, Qian S, Deng C, Yu P. Understanding interactions between caregivers and care recipients in person-centered dementia care: a rapid review. Clin Interv Aging. 2020;15:1637–1647. doi:10.2147/CIA.S255454
75. Malik H, Virag B, Fick F, Hunter PV, Kaasalainen S, Dal Bello-Haas V. Fall prevention program characteristics and experiences of older adults and program providers in Canada: a thematic content analysis. J Appl Gerontol. 2020;39(10):1124–1133. doi:10.1177/0733464819874600
76. Rothman A, Baldwin AS, Hertel AW, Fuglestad PT. Self-regulation and behavior change: disentangling behavioral initiation and behavioral maintenance. In: Handbook of Self-Regulation: Research, Theory, and Applications. The Guilford Press; 2011:106–125.
77. Gallagher-Thompson D, Choryan Bilbrey A, Apesoa-Varano EC, Ghatak R, Kim KK, Cothran F. Conceptual framework to guide intervention research across the trajectory of dementia caregiving. Siegel EO, ed. Gerontologist. 2020;60(Supplement_1):S29–S40. doi:10.1093/geront/gnz157
78. Onken LS, Carroll KM, Shoham V, Cuthbert BN, Riddle M. Reenvisioning clinical science: unifying the discipline to improve the public health. Clin Psychol Sci. 2014;2(1):22–34. doi:10.1177/2167702613497932
79. Peach T, Pollock K, Van Der Wardt V, Das Nair R, Logan P, Harwood RH. Attitudes of older people with mild dementia and mild cognitive impairment and their relatives about falls risk and prevention: a qualitative study. PLoS One. 2017;12(5):e0177530. doi:10.1371/journal.pone.0177530
80. Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. JMDH. 2016;211. doi:10.2147/JMDH.S104807
81. Demiris G, Harrison S, Sefcik J, Skubic M, Richmond T, Hodgson N. Feasibility and acceptability of a technology mediated fall risk prevention intervention for older adults with mild cognitive impairment. J Gerontol Biol Sci Med Sci. 2025;glaf043. doi:10.1093/gerona/glaf043
82. Juckett LA, Bunger AC, Jarrott SE, et al. Determinants of fall prevention guideline implementation in the home- and community-based service setting. Gerontologist. 2021;61(6):942–953. doi:10.1093/geront/gnaa133
83. Schulz R. Intervention taxonomy (ITAX): describing essential features of interventions. AJHB. 2010;34(6). doi:10.5993/AJHB.34.6.15
84. Vincenzo JL, Bergen G, Casey CM, Eckstrom E. Reframing fall prevention and risk management as a chronic condition through the lens of the expanded chronic care model: will integrating clinical care and public health improve outcomes? Gerontologist. 2024;64(6):gnae035. doi:10.1093/geront/gnae035
85. Anantapong K, Davies N, Chan J, McInnerney D, Sampson EL. Mapping and understanding the decision-making process for providing nutrition and hydration to people living with dementia: a systematic review. BMC Geriatr. 2020;20(1):520. doi:10.1186/s12877-020-01931-y
86. Schumacher KL, Stewart BJ, Archbold PG, Dodd MJ, Dibble SL. Family caregiving skill: development of the concept. Res Nurs Health. 2000;23(3):191–203
87. Baumgartner PC, Haynes RB, Hersberger KE, Arnet I. A systematic review of medication adherence thresholds dependent of clinical outcomes. Front Pharmacol. 2018;9:1290. doi:10.3389/fphar.2018.01290
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.