Back to Journals » Vascular Health and Risk Management » Volume 20
Cardiovascular Risk in People Living with Human Immunodeficiency (HIV) Viremia Suppression in a Young, Mid-Eastern European Population - Preliminary Study
Authors Jachymek M, Wójcik Ł, Peregud-Pogorzelska M, Parczewski M, Dembowska A, Aksak-Wąs BJ ![]()
Received 5 June 2024
Accepted for publication 16 August 2024
Published 21 September 2024 Volume 2024:20 Pages 435—445
DOI https://doi.org/10.2147/VHRM.S472328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Magdalena Jachymek,1 Łukasz Wójcik,2 Małgorzata Peregud-Pogorzelska,1 Miłosz Parczewski,3 Aneta Dembowska,3 Bogusz Jan Aksak-Wąs3
1Department of Cardiology, Pomeranian Medical University, Szczecin, 70-111, Poland; 2Department of Radiology, Pomeranian Medical University, Szczecin, 70-111, Poland; 3Department of Infectious, Tropical Diseases and Immune Deficiency, Pomeranian Medical University, Szczecin, 71-455, Poland
Correspondence: Bogusz Jan Aksak-Wąs, Department of Infectious, Tropical Diseases and Immune Deficiency, Pomeranian Medical University, Szczecin, 71-455, Poland, Email [email protected]
Purpose: People living with HIV are twice as likely to develop cardiovascular diseases (CVDs) and myocardial infarction related to atherosclerosis than the uninfected population. This study aimed to evaluate the prevalence of subclinical atherosclerosis in a young, mid-eastern European population of PLWH receiving ART for undetectable viremia.
Patients and Methods: This was a single-centre study. We included 34 patients below 50 years old, treated in Szczecin, Poland, with confirmed HIV-1 infection, treated with antiretroviral therapy (ART), and undetectable viremia. All patients underwent coronary artery computed tomography (CACT), carotid artery intima-media thickness (IMT) evaluation, and echocardiography.
Results: In the primary assessment, only two (5.8%) patients had an increased CVD risk calculated using the Framingham Risk Score (FRS), but we identified coronary or carotid plaques in 26.5% of the patients. Neither traditional risk factors nor those associated with HIV significantly influenced the presence of the plaque. IMT was significantly positively correlated with age and the FRS (R=0.38, p=0.04). Relative wall thickness assessed in echocardiography was higher in those with plaque (0.49 vs 0.44, p=0.04) and significantly correlated with IMT (R=0.38, p=0.04).
Conclusion: In our population, more than a quarter of PLWH with undetectable viremia had subclinical atherosclerosis in either the coronary or carotid arteries. The FRS underpredicted atherosclerosis in this population. The role of RWT as a possible early marker of atherosclerosis needs further studies.
Keywords: cardiovascular disease, echocardiography, coronary artery computed tomography, intima media thickness, people living with human immunodeficiency virus
Introduction
Modern antiretroviral treatment (ART) for human immunodeficiency virus (HIV) infection has changed the long-term prognosis of people living with HIV (PLWH). There has been a significant decrease in the mortality rate of patients living with HIV, as well as a decrease in the incidence of AIDS-defying illnesses. A significant improvement is also observed in both the life expectancy of patients and their quality of life, including significantly fewer HIV-related both cardiovascular and neurodegenerative diseases. Nevertheless, PLWH are more likely to develop cardiovascular diseases (CVDs) than the uninfected population with incidence of cardiovascular disease being 61.8 (95% CI, 45.8–83.4), in comparison with non-HIV population where hazard ratio was 2.16 (95% CI, 1.68–2.77) per 10000 person-years.1 There is also higher risk of myocardial infarction related to atherosclerosis in PLWH with hazard ratio (HR) of 2.57 (95% CI, 2.30–2.86) per 1000 person-years, with comparison to non-HIV population with HR of 1.30 (95% CI, 1.09–1.56) per 1000 person-years.2 The global burden of HIV-associated CVDs has tripled over the past two decades.1
The mechanism underlying atherosclerosis is multifactorial and includes inflammation caused by HIV infection or residual viremia (persisting despite ART), high prevalence of traditional CVD risk factors, unfavorable effects of ART on the metabolic profile, endothelial dysfunction, and increased pro-thrombotic activity.3 CVDs were the fourth leading cause of death in the French HIV-infected population, following non-acquired immunodeficiency syndrome (AIDS), nonviral hepatitis-related malignancies, non-AIDS infections, and AIDS.4 The importance of cardiovascular diseases in the risk of death in patients living with HIV was also confirmed in multicenter cohorts: EUROSIDA and D:A:D.5
The prevalence of subclinical atherosclerosis is high, ranging from 12% to 70.3%.6–10 However, some studies showed the incidence comparable to that in matched uninfected controls.6,10 HIV infection may be associated with more prevalent uncalcified plaques10,11 and more rapid progression of atherosclerosis.12 Moreover, it seems that the HIV infection itself plays the leading role in atherosclerosis development since increased atherosclerosis can occur in so-called HIV controllers, that is, untreated PLWH with undetectable viremia.13
Subclinical atherosclerosis in younger PLWH (precisely age <50 years) with or without other cardiovascular risk factors has not been excessively examined. This study aimed to evaluate the prevalence of subclinical atherosclerosis in a young, mid-eastern European population of PLWH receiving ART for undetectable viremia.
Material and Methods
Study Population
We conducted a single-center study of patients treated at the local Department of Infectious and Tropical Diseases and Immune Deficiencies. We invited volunteers to participate in a comprehensive cardiovascular risk assessment using coronary artery computed tomography (CACT), carotid artery ultrasonography, and echocardiography.
Table 1 shows the inclusion and exclusion criteria. Baseline CD4+ count data were retrospectively obtained from the records. Data regarding the actual viral load, CD4+ count, comorbidities, total cholesterol (TC) and high density cholesterol (HDL) concentrations, treatment, and informed consent were collected during routine follow-up visits. BMI was calculated with standard equation and reported in kg/m2. Framingham Risk Score (FRS) was calculated on-line using following variables: age, gender, smoking status, TC and HDL cholesterol concentrations, systolic BP or hypertension treatment.
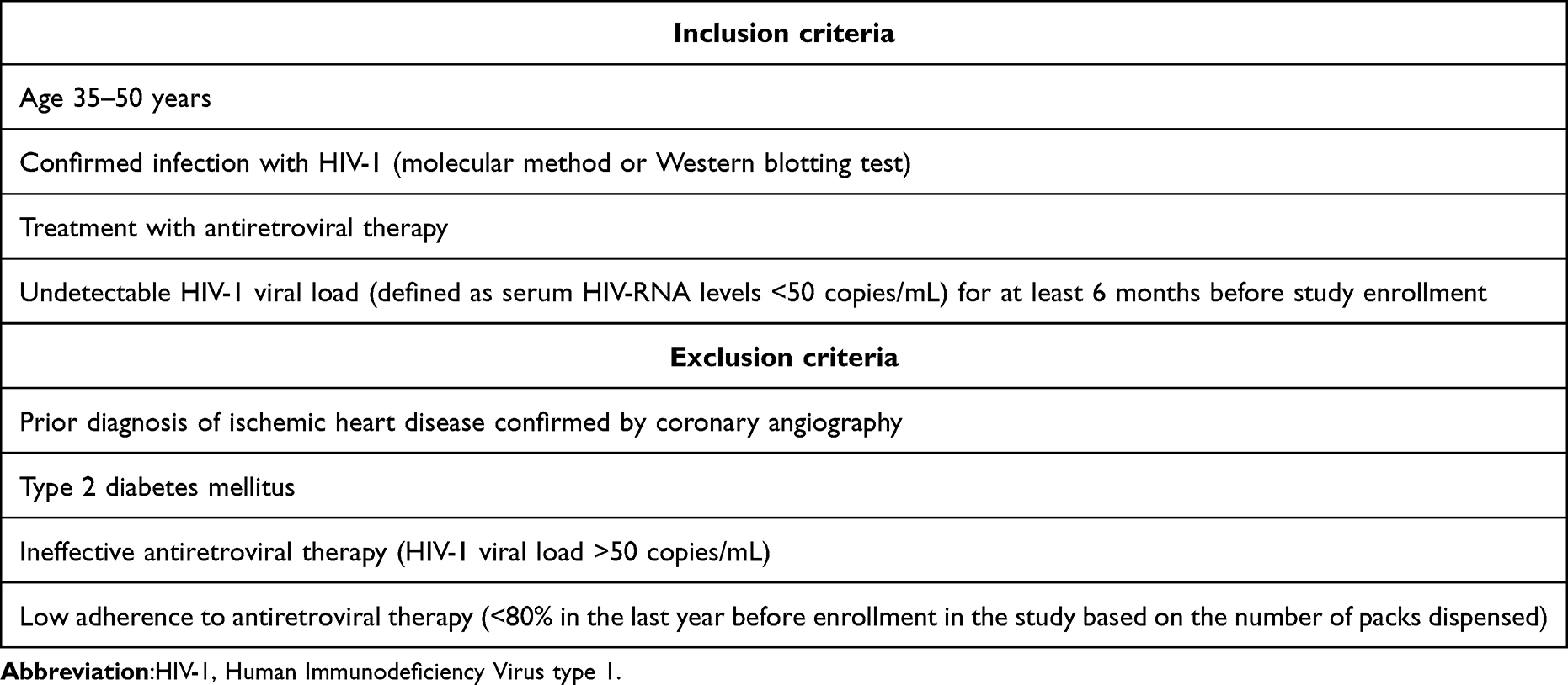 |
Table 1 The Inclusion and Exclusion Criteria Used in the Study |
In this study, we focused on subclinical atherosclerosis diagnosed using CACT, particularly the calcium score (coronary artery calcification [CAC]), carotid intima-media thickness (IMT), and the presence of atherosclerotic plaque in the carotid arteries. We also investigated the relationship between subclinical atherosclerosis and echocardiographic abnormalities.
The study protocol was approved by the local bioethics committee (KB-006/28/2022, 18 May 2022). The study received funding from the “Regional Initiative of Excellence” during 2019–2022, project number 002/RID/2018/19.
Coronary Artery Computed Tomography
Coronary artery computed tomography was performed by a 128-slice multidimensional computed tomography scanner Siemens Somatom Edge Plus (Siemens AG, Erlangen, Germany), using non-contrast and contrast retrospective electrocardiography-gated acquisition. The acquisition was made using coronary presets with a slice thickness of 0.6 mm. A single radiologist well trained in CTA analyzed scans of left main coronary artery, left anterior descending artery, left circumflex coronary artery, right coronary artery, and posterior descending artery on Syngo. via software in CT Cardiac application (Siemens AG, Erlangen, Germany). Stenosis severity was reported using Coronary Artery Disease – Reporting and Data System 2.0 (CAD-RADS) categories (score from 0 to 5).
Intima Media Thickness (IMT)
Carotid artery ultrasonography was performed using a linear probe with Philips Epiq 7C (software version 3.0.3; Philips Ultrasound Inc., Bothell, WA, USA). All sub-cranial segments of the common carotid artery, bulb, internal, and external carotid arteries were visualized whenever possible. IMT, defined as the distance between the leading edge of the first and second echogenic lines of the far wall of the common carotid artery (CCA), was measured in B-mode imaging>1 cm below the bulb in the CCA using automatic software on both sides, and the mean value was calculated. The IMT measurement was performed in plaque-free segments. Blood flow was evaluated using color and pulse-wave Doppler in all visible segments of the carotid artery. Plaque was defined as increase in IMT by >1.5 mm in any segment of the carotid artery. All examinations were performed by the same examiner.
Echocardiography
All the patients underwent transthoracic echocardiography, performed by two echocardiographers using Philips Epiq 7C and GE Vivid E95 (software version 202; GE Vingmed Ultrasound AS, Horten, Norway). Standard echocardiographic measurements were obtained in two dimensions and with Doppler to assess cardiac muscle size, function, and valve sufficiency. The analysis of echocardiography findings and the exact methodology have been described elsewhere.14
Statistical Analyses
Statistical analyses were performed using Statistica 13 (StatSoft, Inc., Tulsa, OK, USA). Quantitative data are presented as means with standard deviations or medians with interquartile ranges, depending on the distribution, and were compared using Student’s t-test or Mann–Whitney U-test. Qualitative data were compared using the chi-squared test with Fisher’s correction. Logistic regression was used to determine the odds ratios. The Spearman correlation coefficient was used to determine the correlation between two quantitative variables. Statistical significance was set at p<0.05. Graphs were created using Microsoft Excel (version 16.48).
Results
Study Population
Table 2 presents the demographic and clinical characteristics of the analytic sample of the study, which consists of 34 patients living with HIV. The mean age was 41.2 years and the mean BMI was 25.65 (±4.1) kg/m2. The table also shows the results of other variables that are related to cardiovascular risk, such as smoking, blood pressure, TC, HDL, and variables related to HIV infection history and actual status, such as baseline CD4+ count, actual CD4+ count, cellular reconstruction and time from diagnosis (Table 2). We evaluated the baseline cardiovascular risk using the Framingham Risk Score (FRS). According to the FRS, only one patient had a medium risk (10–20%), and one had a high risk (>20%).
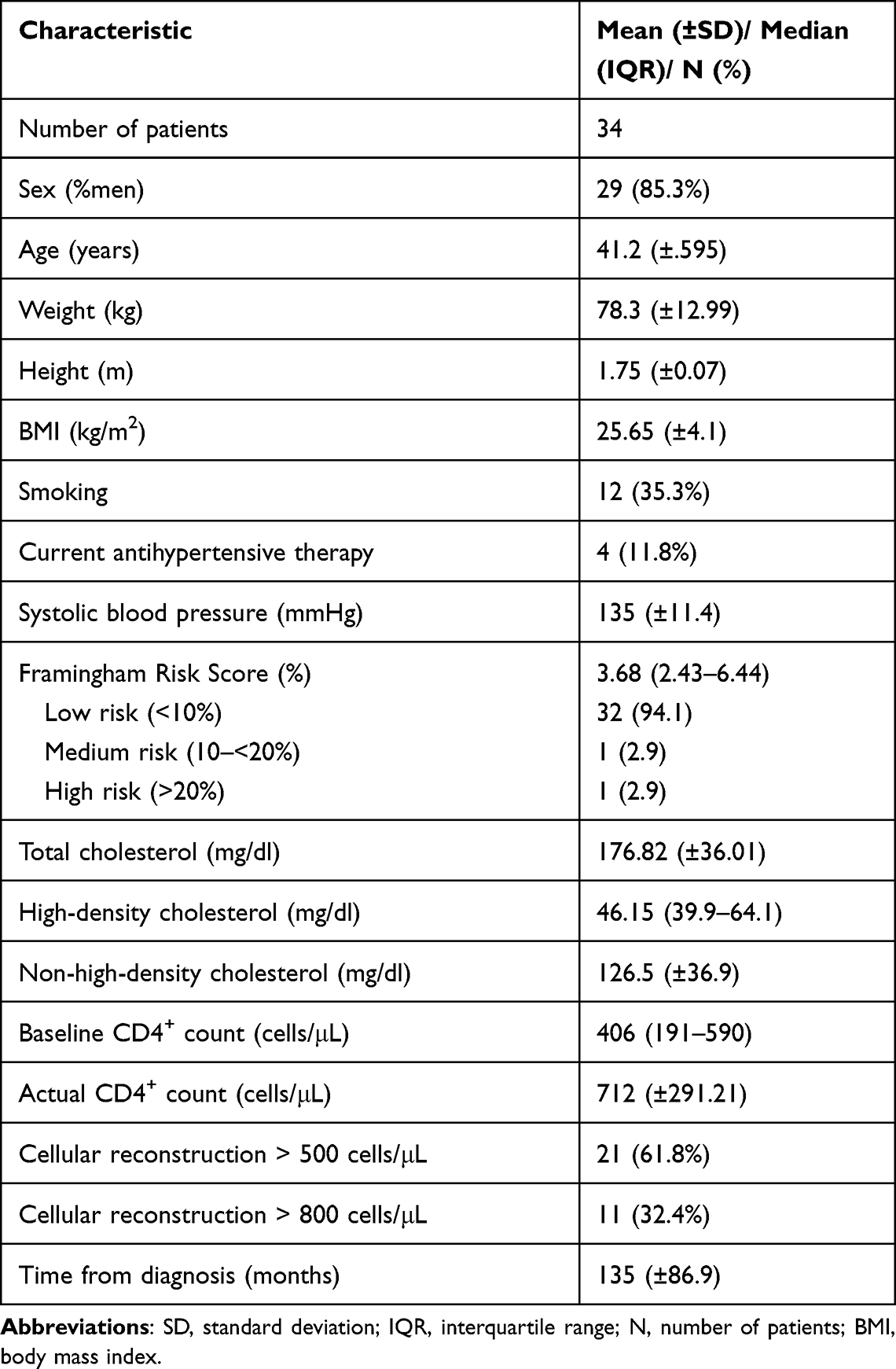 |
Table 2 Demographics and Cardiovascular Risk Factors of the Study Population |
CT scans were available for 33 participants (one reported echocardiography and CA ultrasonography but not CACT); six participants did not undergo CA ultrasonography. Seven (21%) participants had CAC>0 (range, 0.1–85.3), five (17.8%) participants had a CA plaque, and two participants had both. None of the participants with an elevated FRS had visible plaques on CACT or CA USG (Figure 1).
 |
Figure 1 The study population with marked baseline calculated cardiovascular risk in terms of the Framingham Risk Score (FRS), coronary artery calcium score (CAC)>0, plaques in carotid artery ultrasonography, and unavailable data. |
Plaque Presence
Six (18.2%) participants had a Coronary Artery Disease-Reporting and Data System (CAD-RAD) score of 1 (minimal stenosis or plaques with no stenosis), and two had a CAD-RAD score of 2 (mild stenosis). In two participants, narrowing of the coronary artery (up to 20 and 50%) was caused by cardiac muscle bridging without plaque (one participant with a CAD-RAD score of 2 and one with a CAD-RAD score of 1). The most severe was narrowing of the proximal left anterior descending artery by up to 40–50% (CAC, 85.5). In the plaque analysis we included 28 patients with the results of both examinations.
Nine (32.1) patients had plaques in the arteries (both coronary and/or carotid arteries). Table 3 shows a comparison between patients with and without plaques. We compared the demographics and cardiac risk factors between both groups (with and without plaques) and did not find any significant differences.
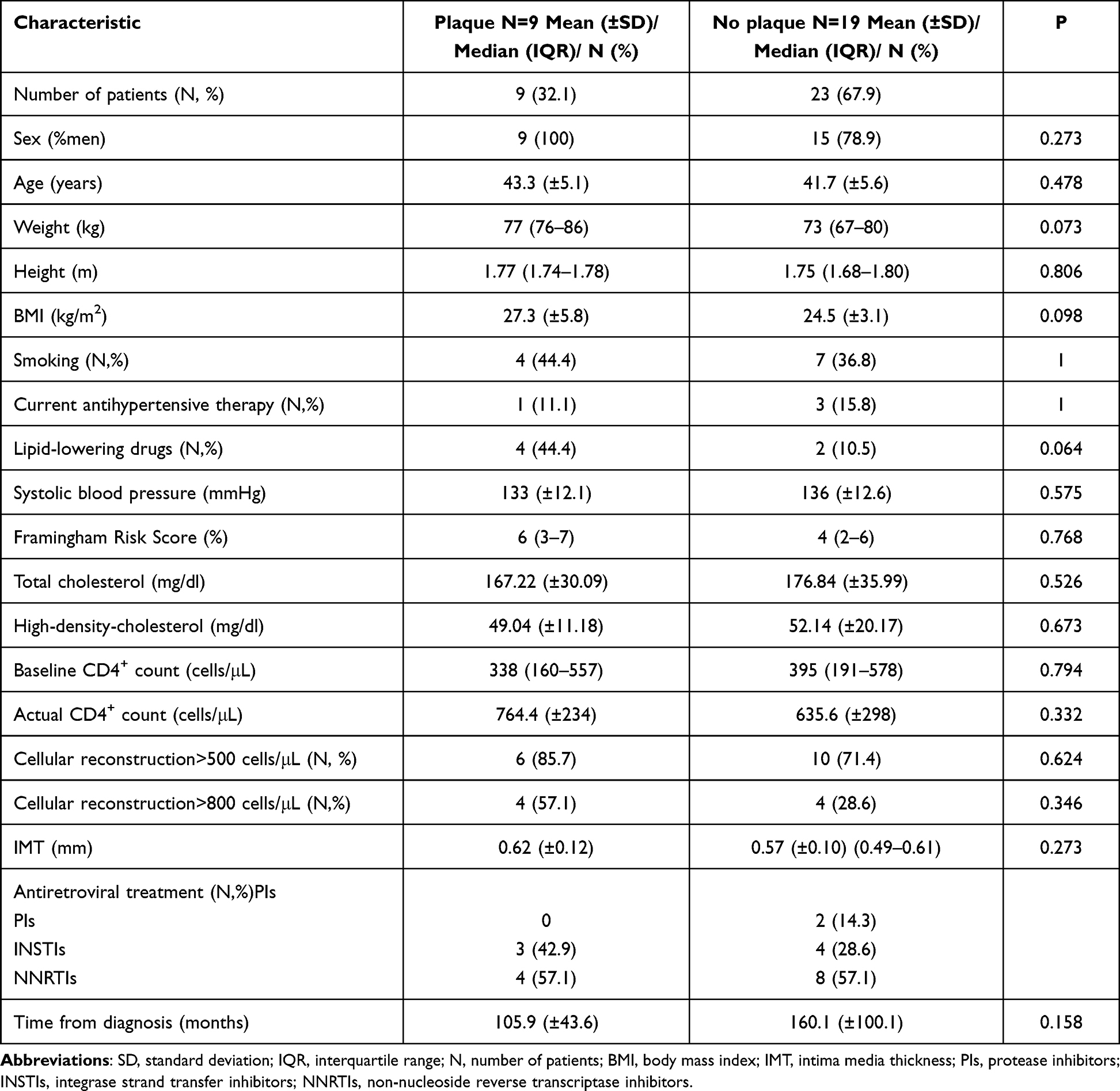 |
Table 3 The Comparison of Variables Between Patients with and without Plaques in Arteries |
The univariate logistic regression showed that neither traditional risk factors nor those associated with HIV significantly influenced the presence of the plaque (Figure 2).
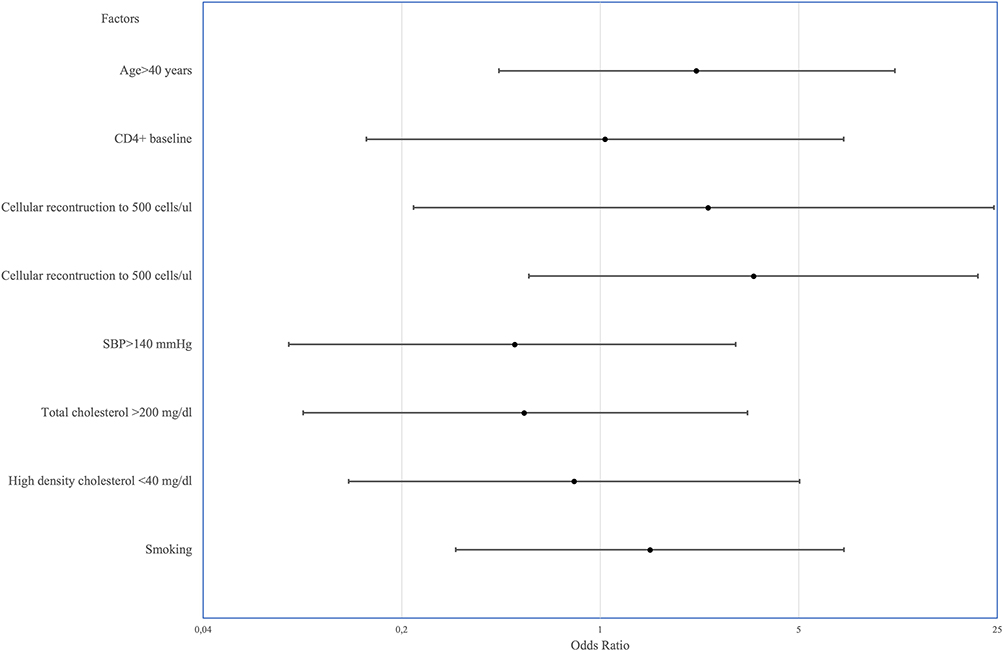 |
Figure 2 The influence of traditional and human immunodeficiency virus-related risk factors on the presence of plaque. Univariate logistic regression. Odds ratio with 95% confidence interval. |
Intima Media Thickness
There was no difference in IMT between participants with and without plaques. We analyzed the correlation of the IMT with traditional and HIV-related risk factors. IMT was significantly positively correlated only with age and the FRS (Table 4).
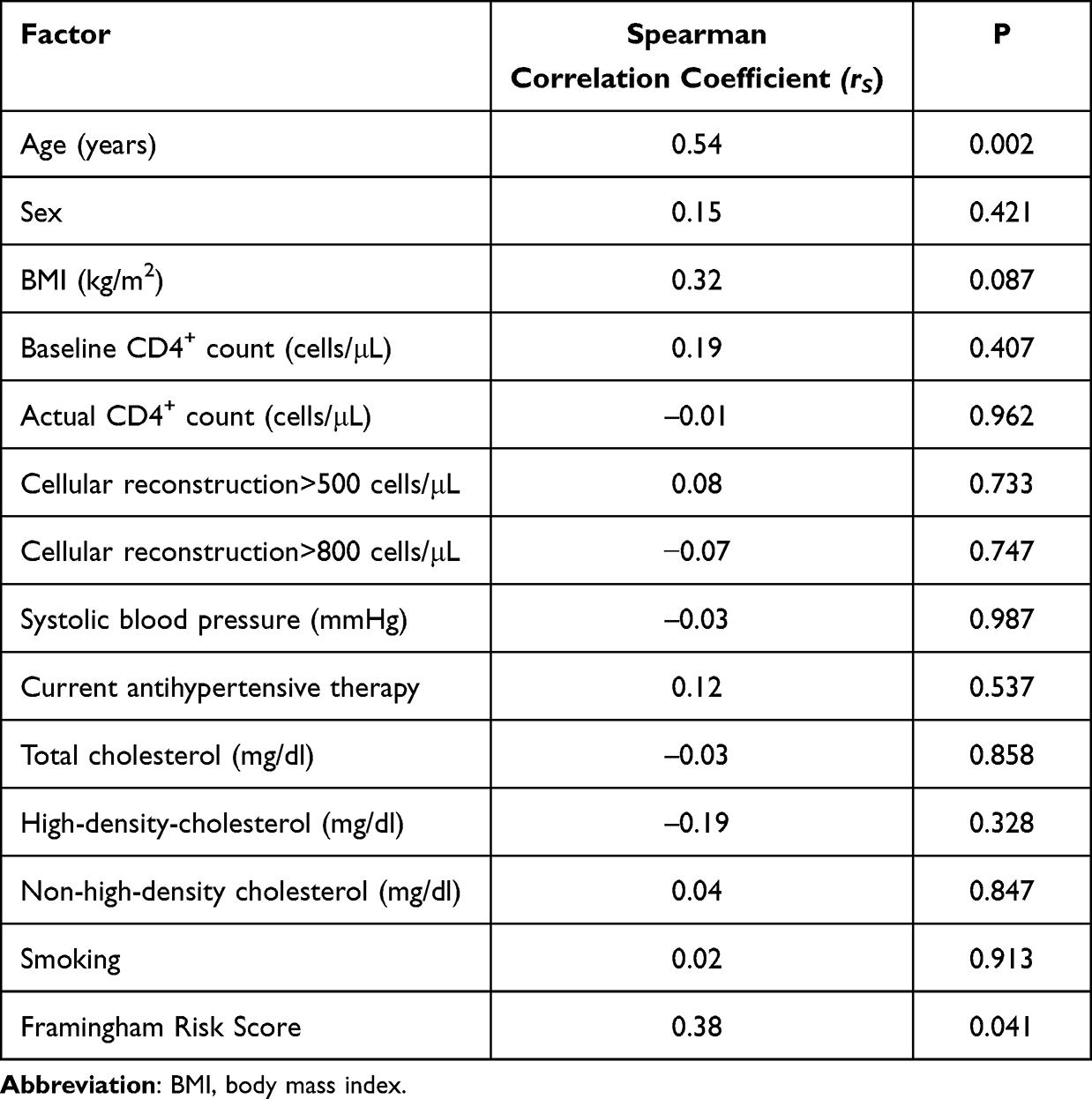 |
Table 4 Correlation Between Carotid Intima-Media Thickness and Traditional and Human Immunodeficiency Virus-Related Risk Factors |
Echocardiography
Echocardiography was performed to assess the size and function of the cardiac muscle, focusing on left ventricular hypertrophy, remodeling, and diastolic function. We have already reported that most participants had concentric remodeling (based on relative wall thickness [RWT] measurements); none had diastolic dysfunction, but one-fifth had left atrium enlargement, which was significantly associated with worse immune reconstruction (data published elsewhere).14 We analyzed the correlation of echocardiographic results with the presence of IMTs and plaques. Increased RWT was associated with the presence of plaque and significantly correlated with IMT (Table 5).
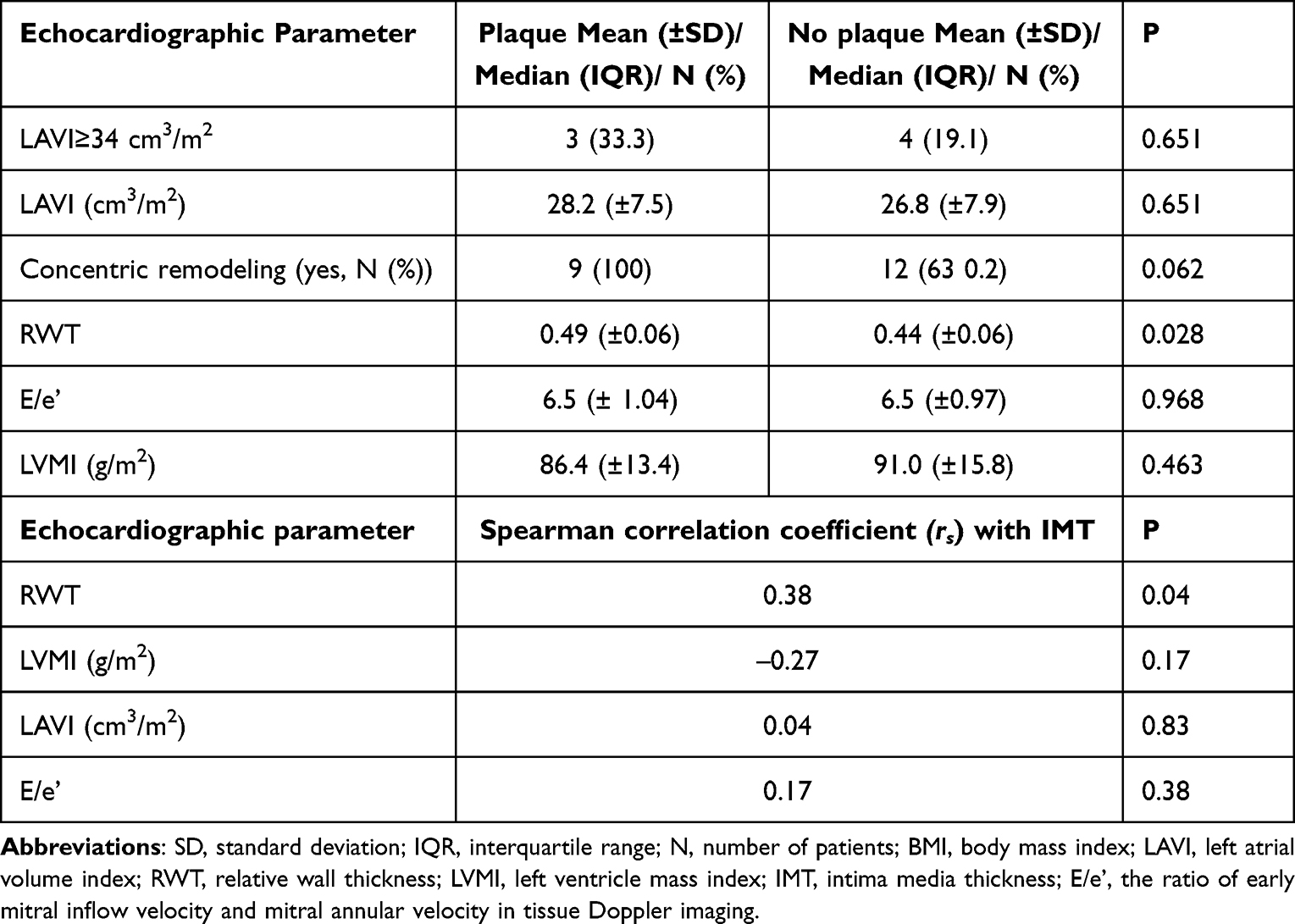 |
Table 5 The Association Between Echocardiographic Parameters of Diastolic Function and Remodeling |
Discussion
In this study, we analyzed the cardiovascular risk in young PLWH. In the primary assessment, only two (5.8%) patients had an increased CVD risk calculated using the FRS, but we identified coronary or carotid plaques in 26.5% of the patients. Notably, those with an elevated FRS had no plaques. We were unable to identify the significant factors associated with plaque formation. IMT was significantly correlated with age and the FRS. The echocardiographic parameter RWT, which describes left ventricle remodeling, was associated with both the presence of plaque and IMT.
A healthy lifestyle should be advised to all individuals as part of cardiovascular prevention. To identify individuals with greater CVD risk and therefore implement more intensive prophylactics or treatment strategies, including lipid or hypertension management, the American Heart Association and European Society of Cardiology (ESC) recommends using validated risk scores.15,16 According to the 2021 ECS CVD prevention guidelines,16 Poland is considered a country with a high CVD risk, and the use of the SCORE2 chart is recommended. The SCORE2 scale has been validated for individuals aged > 40 years and age is a leading risk modifier. The FRS can be used in younger populations (30+). The FRS considers age, sex, total cholesterol and high-density cholesterol levels, smoking, systolic blood pressure, and antihypertensive therapy and estimates the 10-year risk of cardiovascular events.17 Other calculators can be used to assess cardiovascular risk in a cohort of patients living with HIV. For example, the REPRIEVE cohort evaluating the effectiveness of pitavastatin in preventing cardiovascular risk used the American Heart Association and American College of Cardiology 2013 Pooled Cohort Equation risk calculator.18,19 Some cohorts, such as D:A:D or EUROSIDA, use other risk calculators, such as Framingham risk score, or create their own.20 Results of a recent systematic review and meta-analysis comparing the outcomes of the general population and HIV-specific CVD risk models tended to underpredict the risk with general risk scores. However, the FRS had the highest discrimination performance.21 Approximately 20% of patients with FRS>10% have no detectable calcifications in CACT, and almost 20% of those with low risk (FRS<10%) have CAC>0.22 In our study group, the FRS and CAC>0 did not match at all.
The prevalence of subclinical atherosclerosis measured using CACT in PLWH depends on the population ethnicity and inclusion criteria. It is lower in patients with a lower burden of traditional risk factors. For example, a study comparing the prevalence of CAC>0 in Uganda and the USA reported a significantly lower prevalence of atherosclerosis in Uganda than in the USA (12% vs 47%).12 In an Asian population, CAC>0 was found in 50% of patients,7 similar to that in the Danish population of PLWH without viral replication in which almost half had angiographically verified atherosclerosis.23 In a Canadian study, the plaques were present in 70.3% of CACTs, with a higher incidence of uncalcified plaques in the HIV+ population.10 In our population, 21% of the patients had CAC>0, which is a significantly lower incidence than that previously reported, but our population was restricted to young patients with or without few other CVD risk factors.
Several HIV-related factors are associated with plaques in CACT: nadir CD4+ count, soluble intercellular adhesion molecules, soluble CD163, oxidized low-density lipoprotein levels,6 and CD4/CD8 ratio <0.7.8 However, results of studies on the role of ART in plaque formation differ. Treatment with protease inhibitors may be associated with a higher volume of plaque,10 but the duration and type of antiretroviral therapy do not influence the prevalence of atherosclerosis.24,25 Traditional risk factors play a dominant role in CVD risk. The factors considered in FRS and associated with atherosclerosis are age, smoking, and hypercholesterolemia.8,24 In our cohort none of them met statistical significance.
The rapid progression of atherosclerotic plaques may also increase the risk of CVD. In a longitudinal study from Switzerland, the FRS was associated with the progression of subclinical atherosclerosis; however, HIV infection itself was not.26 Suboptimal HIV infection suppression may mediate more rapid artery stenosis progression.12 Age, low-density lipoprotein cholesterol level, visceral abdominal fat, and current T-helper cell count were significantly associated with absolute CAC progression.27 The risk of disease progression and subclinical coronary stenosis also increases in long-term cocaine users.28,29
Ultrasonography of carotid arteries is a less invasive and easily accessible diagnostic test for detecting atherosclerosis. The incidence rate of plaques in the carotid arteries in PLWH ranges from 15 to 83%.8,9,30 In our study, two out of five patients with plaques present in the carotid artery also had CAC>0, but the median IMT did not differ between patients with and without plaques. In a meta-analysis of studies on this topic, HIV-positive patients demonstrated significantly elevated IMT, which was higher in patients receiving ART than in ART-naïve patients, suggesting a role for ART in the thickening of CIMT.31 In another study, the current use of raltegravir was associated with a higher prevalence of pathological findings in the carotid artery, in addition to traditional (age, sex, dyslipidemia) and HIV-related (nadir CD4+ count<200 cells/μ) risk factors.9 From traditional risk factors, age, Black race, body mass index, type 2 diabetes, and smoking (pack-years) were positively associated with higher IMT, but only age and prior myocardial infarction were positively associated with the presence of a carotid plaque in PLWH.30
There are little data connecting atherosclerosis to echocardiographic results, although the mechanism underlying myocardial injury seems similar to that of atherosclerotic plaque formation and includes inflammation, microvascular dysfunction, and endothelial injury.32 In a study by Athanasiadi et al, early left ventricular systolic dysfunction, defined as a global longitudinal strain≥18%, was associated with diastolic dysfunction, left ventricular hypertrophy, increased RWT, and any carotid atherosclerosis.33 In our study, RWT was associated with the presence of plaques and increased IMT. Further studies are necessary to evaluate the usefulness of RWT as an early marker of atherosclerosis.
This study has some limitations. Our main limitation was the small sample size. We did not compare HIV-negative sex and age-matched controls, but multiple data sources have already shown a greater frequency of atherosclerosis in HIV cohorts. Employing “elite” controllers who naturally control virus replication without ART might have served as a valuable control group in this study. Ultrasonography is not a perfect technique, and the measurements and interpretation vary across readers. To reduce the possibility of bias, two independent clinicians were employed to evaluate echocardiography and one to assess IMT with a standardized automatic method. A lot of additional risk factors may contribute to cardiovascular risk—we do not have the data on drug usage, lifestyle choices, diet, or physical activity, but tracking them retrospectively was impossible. Our study is unique because it combines two methods for establishing atherosclerosis diagnosis with echocardiographic measurements.
Conclusion
In our population, more than a quarter of PLWH with undetectable viremia had subclinical atherosclerosis in either the coronary or carotid arteries. The FRS underpredicted atherosclerosis in this population; none of the participants with plaques had an FRS>10%. RWT was correlated with both CIMT and plaque presence, and its role as an early marker of atherosclerosis should be established in further studies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shah ASV, Stelzle D, Lee KK, et al. Global burden of atherosclerotic cardiovascular disease in people living with HIV: systematic review and meta-analysis. Circulation. 2018;138(11):1100–1112. doi:10.1161/CIRCULATIONAHA.117.033369
2. Drozd DR, Kitahata MM, Althoff KN, et al. Increased risk of myocardial infarction in HIV-infected individuals in North America compared with the general population. J Acquir Immune DeficSyndr. 2017;75(5):568–576. doi:10.1097/QAI.0000000000001450
3. Jachymek M, Braksator M, Parczewski M, Peregud-Pogorzelska M, Kaźmierczak J. Cardiovascular disease and HIV infection. AIDS Rev Int J HIV-Related Probl. 2021;20(2):85–89. doi:10.5114/hivar.2021.107234
4. Sellier P, Alexandre-Castor G, Brun A, et al. Updated mortality and causes of death in 2020–2021 in people with HIV: a multicenter study in France. AIDS. 2023;37(13):2007–2013. doi:10.1097/QAD.0000000000003645
5. Petoumenos K, Kuwanda L, Ryom L, et al. Effect of changes in body mass index on the risk of cardiovascular disease and diabetes mellitus in HIV-positive individuals: results from the D:A:D study. J Acquir Immune Defic Syndr. 2021;86(5):579–586. doi:10.1097/QAI.0000000000002603
6. Alencherry B, Erem G, Mirembe G, et al. Coronary artery calcium, HIV and inflammation in Uganda compared with the USA. Open Heart. 2019;6(1):e001046. doi:10.1136/openhrt-2019-001046
7. Chattranukulchai P, Vassara M, Siwamogsatham S, et al. High-sensitivity troponins and subclinical coronary atherosclerosis evaluated by coronary calcium score among older Asians living with well-controlled human immunodeficiency virus. Open Forum Infect Dis. 2023;10(7):1–8. doi:10.1093/ofid/ofad234
8. Fernández Soto J, Romero-Jiménez MJ, Alarcón García JC, Bonet Estruch E, Sánchez Ramos JL, Má CL. Predictors of subclinical atherosclerosis in HIV. BMC Infect Dis. 2023;23(1):1–8. doi:10.1186/s12879-022-07976-1
9. Maggi P, Ricci ED, Muccini C, et al. Subclinical atherosclerosis as detected by carotid ultrasound and associations with cardiac and HIV-specific risk factors; the archi-prevaleat project. HIV Med. 2023;24(5):596–604. doi:10.1111/hiv.13448
10. Boldeanu I, Sadouni M, Mansour S, et al. Prevalence and characterization of subclinical coronary atherosclerotic plaque with CT among individuals with HIV: results from the Canadian HIV and aging cohort study. Radiology. 2021;299(3):571–580. doi:10.1148/radiol.2021203297
11. Post WS, Budoff M, Kingsley L, et al. Associations between HIV infection and subclinical coronary atherosclerosis. Ann Intern Med. 2014;160(7):458–467. doi:10.7326/M13-1754
12. Post WS, Haberlen SA, Witt MD, et al. Suboptimal HIV suppression is associated with progression of coronary artery stenosis: the multicenter AIDS cohort study (MACS) longitudinal coronary CT angiography study. Atherosclerosis. 2022;353:33–40. doi:10.1016/j.atherosclerosis.2022.04.019
13. Hsue PY, Hunt PW, Schnell A, et al. Role of viral replication, antiretroviral therapy, and immunodeficiency in HIV-associated atherosclerosis. AIDS. 2009;23(9):1059–1067. doi:10.1097/QAD.0b013e32832b514b
14. Jachymek M, Peregud-Pogorzelska M, Parczewski M, et al. Unveiling the heart of the matter: echocardiographic insights into diastolic function and left ventricular and atrial changes in hiv patients with controlled Viremia. J Clin Med. 2024;13(2):463. doi:10.3390/jcm13020463
15. Arnett DK, Blumenthal RS, Albert MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;140(11):e596–e646. doi:10.1161/CIR.0000000000000678
16. Visseren F, Mach F, Smulders YM, et al. ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–3337. doi:10.1093/eurheartj/ehab484
17. D’Agostino RB, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation. 2008;117(6):743–753. doi:10.1161/CIRCULATIONAHA.107.699579
18. Grinspoon SK, V. FK, Zanni MV, et al. Pitavastatin to prevent cardiovascular disease in HIV infection. N Engl J Med. 2023;389(8):687–699. doi:10.1056/nejmoa2304146
19. Goff DCJ, Lloyd-Jones DM, Bennett G, et al. ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American college of cardiology/American heart association task force on practice guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2935–2959. doi:10.1016/j.jacc.2013.11.005
20. Friis-Møller N, Ryom L, Smith C, et al. An updated prediction model of the global risk of cardiovascular disease in HIV-positive persons: the Data-collection on Adverse Effects of Anti-HIV Drugs (D:A:D) study. Eur J Prev Cardiol. 2016;23(2):214–223. doi:10.1177/2047487315579291
21. Soares C, Kwok M, Boucher KA, et al. Performance of cardiovascular risk prediction models among people living with HIV: a systematic review and meta-analysis. JAMA Cardiol. 2023;8(2):139–149. doi:10.1001/jamacardio.2022.4873
22. Pereira B, Mazzitelli M, Milinkovic A, et al. Use of coronary artery calcium scoring to improve cardiovascular risk stratification and guide decisions to start statin therapy in people living with HIV. J Acquir Immune DeficSyndr. 2020;85(1):98–105. doi:10.1097/QAI.0000000000002400
23. Knudsen AD, Fuchs A, Benfield T, et al. Coronary artery disease in persons with human immunodeficiency virus without detectable viral replication. Open Forum Infect Dis. 2023;10(7):ofad298. doi:10.1093/ofid/ofad298
24. Monteiro VS, Lacerda HR, Uellendahl M, et al. Calcium score in the evaluation of atherosclerosis in patients with HIV/AIDS. Arq Bras Cardiol. 2011;97(5):427–433. doi:10.1590/s0066-782x2011005000094
25. Thomas GP, Li X, Post WS, et al. Associations between antiretroviral use and subclinical coronary atherosclerosis. AIDS. 2016;30(16):2477–2486. doi:10.1097/QAD.0000000000001220
26. Tarr PE, Ledergerber B, Calmy A, et al. Longitudinal progression of subclinical coronary atherosclerosis in Swiss HIV-positive compared with HIV-negative persons undergoing coronary calcium score scan and CT angiography. Open Forum Infect Dis. 2020;7(10):ofaa438. doi:10.1093/ofid/ofaa438
27. Guaraldi G, Zona S, Orlando G, et al. Progression of coronary artery calcium in men affected by human immunodeficiency virus infection. Int J Cardiovasc Imaging. 2012;28(4):935–941. doi:10.1007/s10554-011-9898-y
28. Kolossváry M, Fishman EK, Gerstenblith G, et al. Cardiovascular risk factors and illicit drug use may have a more profound effect on coronary atherosclerosis progression in people living with HIV. Eur Radiol. 2021;31(5):2756–2767. doi:10.1007/s00330-021-07755-7
29. Lai H, Moore R, Celentano DD, et al. HIV infection itself may not be associated with subclinical coronary artery disease among African Americans without cardiovascular symptoms. J Am Heart Assoc. 2015;5(3):1–16. doi:10.1161/JAHA.115.002529
30. Blaauw MJT, Berrevoets MAH, Vos WAJW, et al. Traditional cardiovascular risk factors are stronger related to carotid intima-media thickness than to presence of carotid plaques in people living with HIV. J Am Heart Assoc. 2023;12(20):e030606. doi:10.1161/JAHA.123.030606
31. Sun D, Wu Y, Yuan Y, Wang Y, Liu W, Yang J. Is the atherosclerotic process accentuated under conditions of HIV infection, antiretroviral therapy, and protease inhibitor exposure? Meta-analysis of the markers of arterial structure and function. Atherosclerosis. 2015;242(1):109–116. doi:10.1016/j.atherosclerosis.2015.06.059
32. Ntsekhe M, Baker JV. Cardiovascular disease among persons living with HIV: new insights into pathogenesis and clinical manifestations in a global context. Circulation. 2023;147(1):83–100. doi:10.1161/CIRCULATIONAHA.122.057443
33. Athanasiadi E, Bonou M, Basoulis D, et al. Subclinical left ventricular systolic dysfunction in HIV patients: prevalence and associations with carotid atherosclerosis and increased adiposity. J Clin Med. 2022;11(7):1804. doi:10.3390/jcm11071804
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.