Back to Journals » Clinical and Experimental Gastroenterology » Volume 13
Cardiovascular Risk in Individuals with Inflammatory Bowel Disease
Authors Biondi RB ![]() , Salmazo PS
, Salmazo PS ![]() , Bazan SGZ
, Bazan SGZ ![]() , Hueb JC, Paiva SAR
, Hueb JC, Paiva SAR ![]() , Sassaki LY
, Sassaki LY ![]()
Received 24 December 2019
Accepted for publication 8 April 2020
Published 24 April 2020 Volume 2020:13 Pages 107—113
DOI https://doi.org/10.2147/CEG.S243478
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Everson Artifon
Robertha Baccaro Biondi, Pericles Sidnei Salmazo, Silméia Garcia Zanati Bazan, João Carlos Hueb, Sergio Alberto Rupp de Paiva, Ligia Yukie Sassaki
Department of Internal Medicine, Botucatu Medical School at Sao Paulo State University (UNESP), Botucatu, Brazil
Correspondence: Ligia Yukie Sassaki
Department of Internal Medicine, São Paulo State University (UNESP), Medical School, Botucatu CEP 18618-970, Brazil
Tel +5514 38801171
Fax +55 14 38801667
Email [email protected]
Background: Inflammatory bowel disease (IBD) patients present a higher risk of developing cardiovascular diseases due to the presence of chronic inflammation, which plays an essential role in atherogenesis. Therefore, the aim of the study was to evaluate the cardiovascular risk between patients with IBD and healthy control individuals.
Materials and Methods: A total of 52 consecutive IBD outpatients from a tertiary hospital and 37 healthy controls were enrolled. Data collected included age, sex, smoking status, presence of comorbidities, disease activity, ongoing medical treatment, body mass index, arterial blood pressure, and cardiovascular risk. The cardiovascular risk was based on the Framingham risk score and ultrasonography variables, such as the carotid intima-media thickness and the presence of atherosclerotic plaque in the carotid. Multivariate logistic regression or multiple linear regression analysis was performed at a significance level of 5%.
Results: No differences were observed between groups with regard to age, sex, smoking status, comorbidities, blood pressure, body mass index, lipid profile, and Framingham risk score. In the IBD group, fasting glucose [95 (86.2– 107.3) mg/dL vs 86 (79– 100) mg/dL, p=0.041], carotid intima-media thickness (0.69± 0.12 mm vs 0.63± 0.12 mm, p=0.031), and atherosclerotic carotid plaque (25% vs 5.4%, p=0.032) were higher compared with those in the control group. Multivariate logistic regression analysis showed that patients with IBD presented a 6.45-fold higher risk of carotid atherosclerotic plaque (odds ratio: 6.45; 95% confidence interval: 1.035– 40.216; p< 0.046).
Conclusion: Patients with IBD are at an increased risk of atherosclerosis and, consequently, an increased risk for cardiovascular diseases.
Keywords: cardiovascular risk, carotid artery diseases, carotid intima-media thickness, inflammatory bowel disease
Introduction
Inflammatory bowel disease (IBD) is a group of chronic inflammatory disorders that affect the gastrointestinal tract and comprises Crohn’s disease and ulcerative colitis. As observed in other chronic inflammatory diseases, patients with IBD present a higher risk of developing cardiovascular diseases because chronic inflammation plays an essential role in atherogenesis.1,2 The inflammatory process induces aggression to the vascular endothelium, leading to endothelial dysfunction and, consequently, carotid intima-media thickness and arterial stiffness, both considered subclinical manifestations of atherosclerosis.2
Despite the increased risk of atherosclerosis due to chronic inflammation and the increased frequency of risk factors such as overweight and obesity in this population,3,4 studies on cardiovascular risk in patients with IBD presented conflicting results. Two retrospective cohort studies involving approximately 17,000 and 25,000 individuals showed that the risk of myocardial infarction in patients with IBD is similar to that in the control group.5,6 However, a Danish cohort study including 28,833 IBD individuals found an increased risk of cardiovascular events (risk ratio [RR]=2.13, 95% confidence interval [CI]: 1.91 to 2.38), particularly in the first year after the IBD diagnosis.7
Atherosclerotic cardiovascular disease is the leading cause of morbidity and mortality worldwide, which may be attributed to uncontrolled exposure to risk factors, in addition to the lack of efficient strategies of disease prevention.8 Patients with IBD are at a high risk of developing cardiovascular disease due to the presence of chronic inflammation and exposure to risk factors such as the presence of metabolic disease. In the present study, we aimed to evaluate the cardiovascular risk in patients with IBD compared with the healthy control group.
Materials and Methods
Study Design and Population
A case–control study was conducted on 52 outpatients with Crohn’s disease and ulcerative colitis and 37 healthy individuals between April 2016 and October 2017. The diagnosis of IBD was based on clinical, endoscopic, and histological parameters. The inclusion criteria for the IBD group were age ≥18 years and the evaluation of the carotid arteries by ultrasonography. Exclusion criteria were gestation or breastfeeding; previous history of cardiovascular disease; diagnosis of acquired immunodeficiency syndrome; presence of renal, rheumatic, or hepatic disease or previous bariatric surgery; and impossibility of carotid artery evaluation due to technical difficulty related to the ultrasonography exam.
The control group was composed of healthy volunteer blood donors from the institution’s blood bank. The donors were invited to participate in the study during their appointment for blood donation. They were evaluated through a questionnaire interview, physical examination including weight and height, and blood pressure measurement, and blood sample was collected for laboratory tests. The control group was chosen using the same age group as the IBD group, those individuals who did not fit the age group of the disease group were excluded.
Clinical Evaluation
Data such as age, sex, smoking status, presence of comorbidities, disease duration, and medication were evaluated, and blood pressure was measured. The extent of the disease was classified according to the Montreal classification9 for patients with Crohn’s disease and according to the extent of the inflammatory process (proctitis, left-sided colitis, or extensive/pancolitis)10 for patients with ulcerative colitis. Disease activity was assessed using the Crohn’s disease activity index11 for Crohn’s disease and the Mayo score12 for ulcerative colitis. To assess the endoscopic activity of the disease for the calculation of the Mayo score, the endoscopic examination performed from 0 to 6 months before or after the study evaluation was considered.
Anthropometric Evaluation
Anthropometric evaluation consisted of body weight, height, and body mass index (BMI). Nutritional status was classified according to the points proposed by the World Health Organization13 and Pan American Health Organization (OPAS)14 for adults and elderly (≥60 years), respectively.
Cardiovascular Risk
Cardiovascular risk was based on the Framingham risk score and ultrasonography variables, such as the carotid intima-media thickness and the presence of carotid atherosclerotic plaque. Ultrasonography examination of the carotid arteries was performed by the same trained and qualified cardiologist using the General Electric Vivid S6, equipped with a 7.0-MHz linear ultrasonic transducer and an image recording system. Measurements were performed at the posterior wall of the distal third 10-mm segment of the left and right common carotids, preceding the carotid bulb (5 mm), considering the distance between the lumen-intima and media-adventitia interfaces. Such measurements were performed at the R wave peak of the electrocardiogram. The mean values between the two carotids were considered. Presence of atherosclerotic plaque was defined as focal thickening of ≥50% of the intima-media thickness of the vessel wall environment or carotid intima-media thickness greater than 1.5 mm.15–17
Biochemical Evaluation
A sample of a 12-hour fasting peripheral blood was obtained from the IBD and control groups to evaluate fasting glucose, high-sensitivity C-reactive protein, total cholesterol, high-density lipoprotein cholesterol, and triglycerides. Low-density lipoprotein cholesterol was estimated using the Friedewald equation when the triglyceride level was less than 400 mg/dL.
Statistical Analysis
For sample size calculation, the chi-square test with the Yates’ correction was used for two independent proportions, considering samples of different sizes. In a previous study, Salmazo et al18 verified the frequency of atherosclerotic plaque in 4% of the subjects in the control group versus 37% of the HIV-infected patients. Considering the hypothesis of a lower frequency of atherosclerotic plaque in the carotid in patients with IBD compared with patients with HIV (approximately 20%) and considering the desired power of 0.8 and alpha of 0.05, we obtained a sample size of 76 individuals for the study.
Of the 103 individuals with IBD invited to participate in this study, 14 were excluded for presenting exclusion criteria such as cardiovascular disease (n=9), liver or renal disease (n=4), or previous bariatric surgery (n=1). Finally, 89 individuals were included in the analysis, with 52 in the IBD group and 37 in the matched control group.
Data are presented as mean and standard deviation and median and quartile 1 and quartile 3. Student’s t-test and Mann–Whitney test were used to compare the groups. To verify which factors explain the presence of cardiovascular risk, multivariate logistic regression or multiple linear regression analysis was performed. The regression model was adjusted for age, sex, smoking status, fasting glucose, LDL-cholesterol, triglycerides, and BMI. A significance level of 5% was used. All analyses were performed with Sigma Plot for Windows v12.0 (Systat Software Inc., San Jose, CA, USA).
Ethical Considerations
The study was approved by the local ethics committee (CAAE: 58127316.9.0000.5411). All subjects were informed about the objectives of the study and included after they signed the written informed consent form.
Results
Fifty-two individuals with IBD (Crohn’s disease: 32.7%; ulcerative colitis: 67.3%) were evaluated. The mean age was 49.2±11.4 years, and 51.9% were female. The disease duration was 9.9±7.2 years, and the majority (57.7%) of the individuals were in clinical remission. The high-sensitivity C-reactive protein was 2.8±5.6 mg/dL.
Among patients with ulcerative colitis, the mean age was 50.6±10.5 years, 54.3% were female, and 57.1% were in disease remission. According to the extent of the inflammation, 57.1% of the patients presented pancolitis, followed by left-sided colitis (22.9%). Most used 5-aminosalicylic acid derivatives (54.3%), followed by biological therapy (20%) and corticosteroids (14.3%). The median of the total Mayo score was 2 (1–4) points, and the median of the endoscopic Mayo score was 1 (1–2) point. Among Crohn’s disease patients, the mean age was 46.3±13.1 years, 47% were female, and 58.8% were in disease remission. Most were diagnosed at aged between 17 and 40 years (56.9%). The ileal (35.3%) and ileocolic (35.3%) regions were the main inflammation-affected areas, and the predominant behavior was penetrating (52.9%), followed by stenosing (29.4%). Perianal disease was observed in 47% of the patients. The majority received biological therapy (70.6%), followed by azathioprine (64.7%) and corticosteroids (5.8%). The control group consisted of 37 individuals with a mean age of 45.5 (±10.1) years and a predominance of women (59.4%).
Cardiovascular Risk
No difference was found in clinical variables between the IBD and control groups (Table 1). The BMI was 26.5±3.8 kg/m2 in the IBD group and 27.1±5.5 kg/m2 in the control group (p=0.236), and the majority of the individuals were overweight or obese (IBD 53.8% vs control 59.4%).
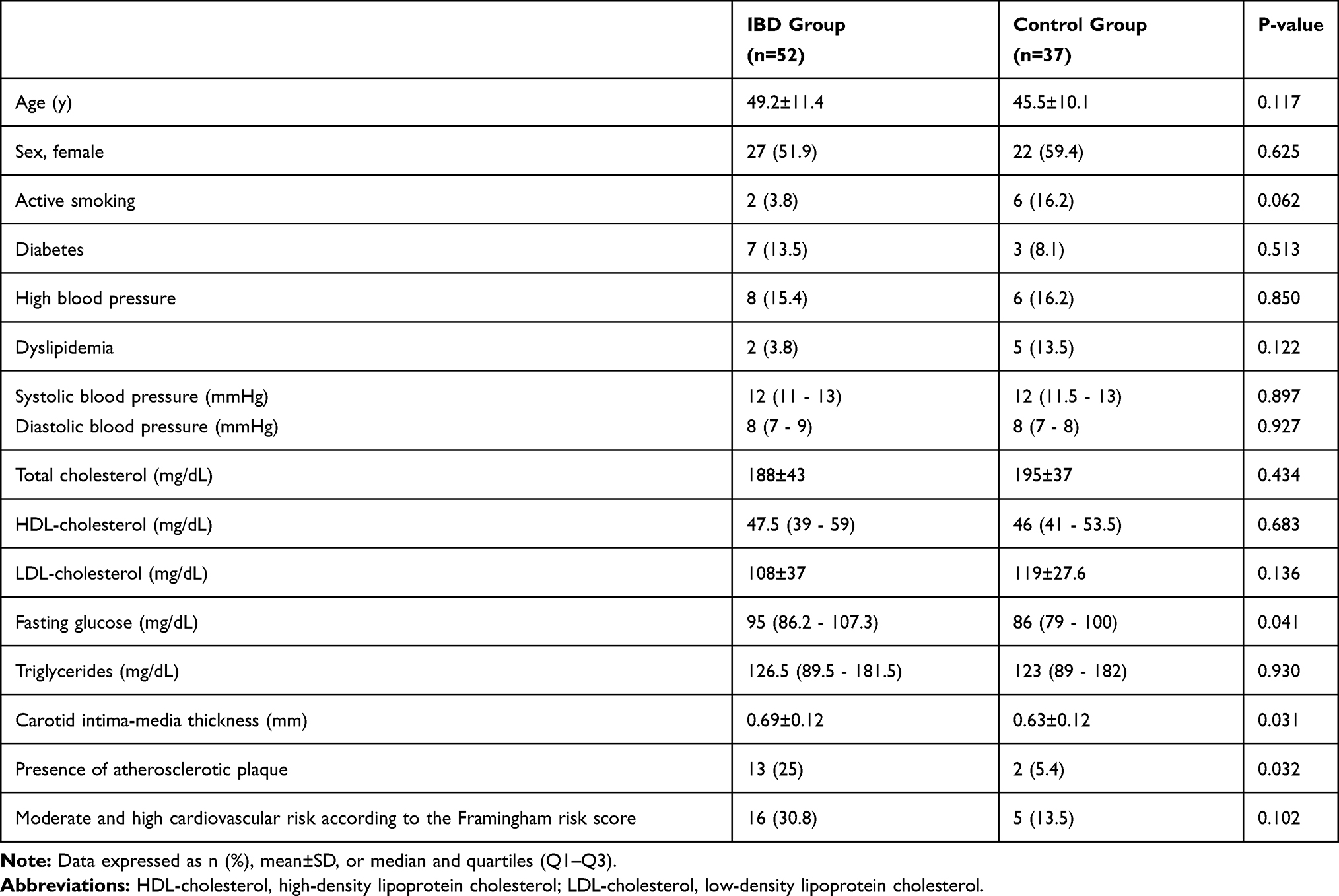 |
Table 1 Clinical Variables and Risk Factors for Cardiovascular Disease in the IBD and Control Groups |
The IBD group presented higher fasting glucose (p=0.041), higher carotid intima-media thickness (p=0.031), and higher percentage of atherosclerotic plaque in the carotid (p=0.032) compared with the control group (Table 1). Despite these findings, the presence of moderate and high cardiovascular risks according to the Framingham risk score did not differ between the groups (30.8% in the IBD group vs 13.5% in the control group, p=0.102; Table 1).
Multivariate logistic regression analysis showed that the presence of IBD, even adjusted for age, sex, smoking status, fasting glucose, LDL-cholesterol, triglycerides, and BMI, increased the risk of carotid atherosclerotic plaque by 6.45 times (Table 2). According to the linear regression model, an association was found between the presence of IBD and the carotid intima-media thickness (p=0.031), but the association became non-significant (p=0.176) when adjusted (Table 2).
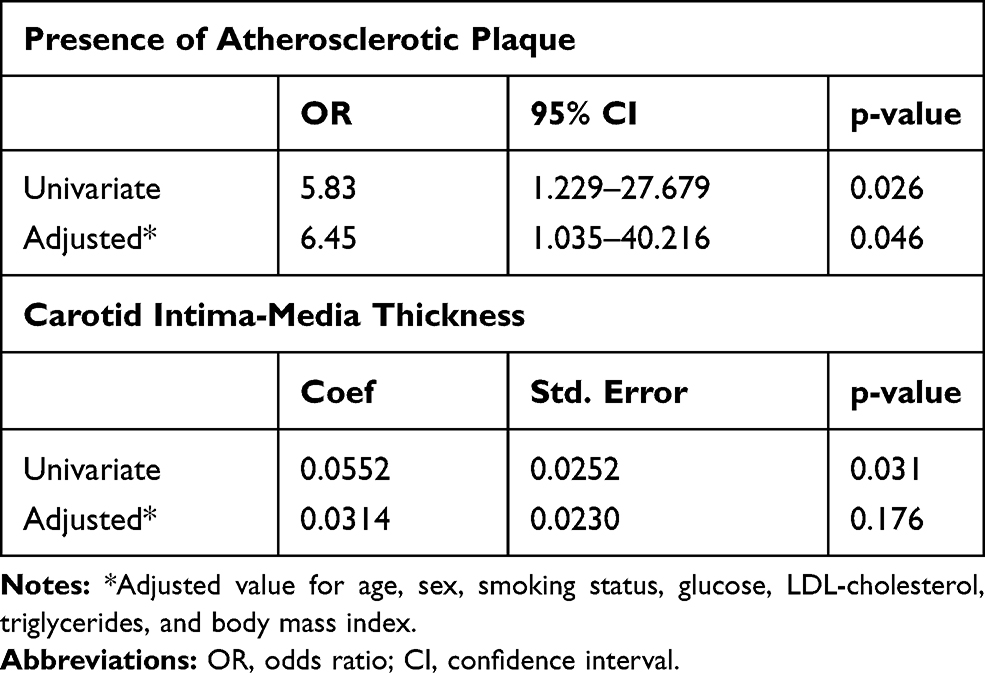 |
Table 2 Logistic Regression for the Presence of Atherosclerotic Plaque and Linear Regression for Carotid Intima-Media Thickness in the IBD Group |
Discussion
In recent years, evidence has emerged on the association between IBD and the increased risk of cardiovascular events. A systematic review included six studies and observed 6478 coronary events in 123,907 patients with IBD and a risk increase of 19% in coronary artery disease, particularly among women and individuals younger than 40–50 years.19 Kristensen et al20 found that individuals with IBD present an increased risk of stroke (RR=1.15, 95% CI: 1.05–1.27) and hospitalization for heart failure (RR 1.37, 95% CI 1.26–1.49) when compared with the matched controls.
Therefore, evaluating cardiovascular risk in this population periodically and throughout life is important. Cardiovascular risk assessment is based on clinical scores, such as the Framingham risk score, which is used worldwide and estimates the likelihood of occurrence of or death from coronary disease within a period of 10 years in individuals without prior clinical atherosclerosis. The score assesses the cardiovascular risk based on the presence of risk factors such as systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol, and smoking. The Framingham risk score was not originally proposed to evaluate cardiovascular risk in the IBD population, but it is a well-established score in literature and globally used to estimate cardiovascular risk in populations of interest.21–23
In the present study, no significant difference was found in cardiovascular risk calculated using the Framingham risk score between the IBD and matched control groups. Considering that patients with IBD presented a higher percentage of atherosclerotic plaque in the carotid, the Framingham risk score was possibly not a good tool to detect the risk in this population, probably because it does not consider the presence of systemic inflammation. In addition, the low age of the patients may have contributed to this finding. Similarly, Rungoe et al24 observed that the Framingham risk score is lower in patients with IBD, even in those with coronary artery disease, compared with individuals with coronary artery disease (8.1±3.47 vs 10±3.75, p=0.002).
Therefore, previous studies suggested the use of other methods of risk assessment, such as evaluation of carotid intima-media thickness by ultrasonography. Carotid ultrasound is the standard tool in clinical practice for the detection and estimation of the severity of carotid atherosclerosis.25 It is a non-invasive, reproducible, and relatively inexpensive method that provides quantitative measurements of structural changes in the arterial wall. It allows the diagnosis of atherosclerosis in its subclinical phase, permitting early intervention, thereby contributing to reduced incidence of unfavorable outcomes.26 The exam should be considered in high-risk groups for cardiovascular disease,27 such as in patients with IBD.
Patients with IBD presented a higher risk of carotid atherosclerotic plaque even when adjusted for other risk factors for cardiovascular disease. With regard to the carotid intima-media thickness, although the IBD group presented greater thickness compared with the control group, this result was not significant when adjusted for other variables. Emphasizing that the carotid intima-media thickness and the carotid plaque seem to be distinct manifestations of the arterial wall thickening process is important.28 However, the presence of carotid plaque is more strongly associated with coronary artery disease and is a better predictor of cardiovascular events compared with the carotid intima-media thickness.29 Notably, when both of them are visualized, the cardiovascular risk is higher.27
Chronic inflammation may contribute to the development of atherosclerosis and atherosclerotic plaque rupture. Inflammatory cytokines, such as tumor necrosis factor-α, reduce the expression of enzyme nitric oxide synthase, decreasing nitric oxide bioavailability and impairing endothelium vasodilation.30 Inflammatory cytokines are also largely responsible for the increased production of reactive oxygen species capable of activating nuclear kappa factor, which increases the expression of cell adhesion molecules by stimulating leukocyte migration to the subendothelial space, a key process in initiation and maintenance of atherosclerosis.30
Despite the association between chronic inflammation and cardiovascular diseases, few studies evaluated the effects of drug treatment aiming to control the inflammatory process to reduce the risk of cardiovascular events in patients with IBD.7 With the advent of new drugs that enable better control of inflammatory activity and the establishment of treatment strategies with defined therapeutic targets, a reduction of the cardiovascular risk in this population is expected. A study conducted by Paschou et al31 observed a decrease in insulin levels and homeostatic model assessment for insulin resistance index in patients with IBD after receiving treatment with biological therapy for a period of six months. These data suggest that clinical treatment can promote not only controlling intestinal inflammation, but also controlling risk factors for cardiovascular disease, resulting in the reduction of the overall risk of cardiovascular events in the long term. However, prospective studies are needed to prove these effects in the general IBD population.
The present study has some limitations including small sample size and cross-sectional design, indicating that prospective and longitudinal studies are necessary, particularly to clarify the impact of active intestinal inflammation on the development of cardiovascular disease. In addition, future studies should investigate the relationship between disease remission and cardiovascular risk modification. We also acknowledge that other methods of body composition evaluation, such as computed tomography and dual-energy X-ray absorptiometry, more accurately reflect visceral and mesenteric adiposity compared with BMI, an important risk factor for cardiovascular disease. Despite these limitations, our study suggests that patients with IBD present a higher risk of developing atherosclerotic plaque in the carotid arteries and, consequently, a higher risk of cardiovascular diseases when compared with the matched control group.
Conclusion
Patients with IBD are at an increased risk of atherosclerosis and, consequently, an increased risk for cardiovascular diseases. Strategies should be implemented to promote control of the cardiovascular risk factors aiming cardiovascular risk reduction in this population.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics and Consent Statement
The study was approved by the Botucatu Medical School Research Ethics Committee (protocol number 58127316.9.0000.5411). The authors confirm that all research was performed in accordance with relevant regulations. All subjects were informed about the objectives of the study and included after they signed the written informed consent form.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no competing interests to disclose.
References
1. Roifman I, Beck PL, Anderson TJ, Eisenberg MJ, Genest J. Chronic inflammatory diseases and cardiovascular risk: a systematic review. Can J Cardiol. 2011;27:174–182. doi:10.1016/j.cjca.2010.12.040
2. Singh S, Kullo IJ, Pardi DS, Loftus EV. Epidemiology, risk factors and management of cardiovascular diseases in IBD. Nat Rev Gastroenterol Hepatol. 2015;12:26–35. doi:10.1038/nrgastro.2014.202
3. Seminerio JL, Koutroubakis IE, Ramos-Rivers C, et al. Impact of obesity on the management and clinical course of patients with inflammatory bowel disease. Inflamm Bowel Dis. 2015;21:2857–2863. doi:10.1097/MIB.0000000000000560
4. Moran GW, Dubeau MF, Kaplan GG, Panaccione R, Ghosh S. The increasing weight of Crohn’s disease subjects in clinical trials: a hypothesis-generatings time-trend analysis. Inflamm Bowel Dis. 2013;19:2949–2956. doi:10.1097/MIB.0b013e31829936a4
5. Ha C, Magowan S, Accortt NA, Chen J, Stone CD. Risk of arterial thrombotic events in inflammatory bowel disease. Am J Gastroenterol. 2009;104:1445–1451. doi:10.1038/ajg.2009.81
6. Osterman MT, Yang YX, Brensinger C, Forde KA, Lichtenstein GR, Lewis JD. No increased risk of myocardial infarction among patients with ulcerative colitis or Crohn’s disease. Clin Gastroenterol Hepatol. 2011;9:875–880. doi:10.1016/j.cgh.2011.06.032
7. Rungoe C, Basit S, Ranthe MF, Wohlfahrt J, Langholz E, Jess T. Risk of ischaemic heart disease in patients with inflammatory bowel disease: a nationwide Danish cohort study. Gut. 2013;62:689–694. doi:10.1136/gutjnl-2012-303285
8. American Heart Association. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease; 2019. Available from: https://www.ahajournals.org/doi/suppl/10.1161/CIR.0000000000000678.
9. Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a working party of the 2005 Montreal world congress of gastroenterology. Can J Gastroenterol. 2005;19:5A–36A. doi:10.1155/2005/269076
10. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55:749–753. doi:10.1136/gut.2005.082909
11. Best WR, Becktel JM, Singleton JW, Jr KF. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology. 1976;70:439–444. doi:10.1016/S0016-5085(76)80163-1
12. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317:1625–1629. doi:10.1056/NEJM198712243172603
13. World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Geneva: WHO; 1998:8–9.
14. Organización Panamericana de la Salud (OPAS). XXXVI Reunión del Comitê Asesor de Investigaciones en Salud – Encuestra Multicêntrica – Salud Beinestar y Envejecimeiento (SABE) en América Latina e el Caribe – Informe preliminar; 2002 [XXXVI Meeting of the Advisory Committee on Health Research - Survey Multicenter - Health Well-being and Aging (SABE) in Latin America and the Caribbean – Preliminary report; 2002]. Spanish.
15. Touboul PG, Hennerici MG, Meairs S, et al. Mannheim carotid intima-media thickness consensus (2004–2006). An update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Cerebrovasc Dis. 2007;23:75–80. doi:10.1159/000097034
16. Gray-Weale AC, Graham JC, Burnett JR, Lusby RJ. Carotid artery atheroma: comparison of preoperative B-mode ultrasound appearance with carotid endarterectomy specimen pathology. J Cardiovasc Surg. 1988;29:676–681.
17. Stein JH, Korcarz CE, Hurst RT, et al; American Society of Echocardiography Carotid Intima-Media Thickness Task Force Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21:93–111. doi:10.1016/j.echo.2007.11.011
18. Salmazo PS, Bazan SGZ, Shiraishi FG, Bazan R, Okoshi K, Hueb JC. Frequency of subclinical atherosclerosis in Brazilian HIV-infected patients. Arq Bras Cardiol. 2018;110:402–410. doi:10.5935/abc.20180058
19. Singh S, Singh H, Loftus EV, Pardi DS. Risk of cerebrovascular accidents and ischemic heart disease in patients with inflammatory bowel disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2014;12:382–393. doi:10.1016/j.cgh.2013.08.023
20. Kristensen SL, Ahlehoff O, Lindhardsen J, et al. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death: a Danish nationwide cohort study. PLoS One. 2013;8:e56944. doi:10.1371/journal.pone.0056944
21. Anderson TJ, Grégoire J, Pearson GJ, et al. 2016 Canadian Cardiovascular Society Guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol. 2016;32:1263–1282. doi:10.1016/j.cjca.2016.07.510
22. National Cholesterol Education Program (NCEP). Third report of the expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III: final report). Circulation. 2002;106:3145–3146.
23. Sociedade Brasileira de Cardiologia. Departamento de Aterosclerose da Sociedade Brasileira de Cardiologia. IV Diretriz Brasileira Sobre Dislipidemias e Prevenção da Aterosclerose [IV Brazilian Guideline on Dyslipidemias and Atherosclerosis Prevention]. Arq Bras Cardiol. 2007;88:2–19. Portuguese. doi:10.1590/S0066-782X2007000700002
24. Rungoe C, Nynne AN, Jess T. Inflammatory bowel disease and risk of coronary heart disease. Trends Cardiovasc Med. 2015;25:699–704. doi:10.1016/j.tcm.2015.03.010
25. Gallino A, Aboyans V, Diehm C; European Society of Cardiology Working Group on Peripheral Circulation, et al. Non-coronary atherosclerosis. Eur Heart J. 2014;35:1112–1119. doi:10.1093/eurheartj/ehu071
26. Zaid M, Fujiyoshi A, Kadota A, Abbott RD, Miura K. Coronary artery calcium and carotid artery intima media thickness and plaque: clinical use in need of clarification. J Atheroscler Thromb. 2017;24:227–239. doi:10.5551/jat.RV16005
27. Nambi V, Chambless L, Folsom AR, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (atherosclerosis risk in communities) study. J Am Coll Cardiol. 2010;55:1600–1607. doi:10.1016/j.jacc.2009.11.075
28. Rundek T, Gardener H, Della-Morte D, et al. The relationship between carotid intima-media thickness and carotid plaque in the Northern Manhattan study. Atherosclerosis. 2015;241:364–370. doi:10.1016/j.atherosclerosis.2015.05.027
29. Simon A, Megnien JL, Chironi G. The value of carotid intima-media thickness for predicting cardiovascular risk. Arterioscler Thromb Vasc Biol. 2010;30:182–185. doi:10.1161/ATVBAHA.109.196980
30. Steyers CM, Miller FJ
31. Paschou SA, Kothonas F, Lafkas A, et al. Favorable effect of anti-TNF therapy on insulin sensitivity in nonobese, nondiabetic patients with inflammatory bowel disease. Int J Endocrinol. 2018;2018:6712901. doi:10.1155/2018/6712901
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.