Back to Journals » International Journal of Women's Health » Volume 17
Cardiovascular Health Optimization Through Life’s Essential 8 Scores Reduces Gestational Diabetes Risk: Mediation by Platelet Activity and Inflammatory Pathways in a Nationwide Cohort
Authors Li X ![]() , Yang Q
, Yang Q ![]() , Zhang X, He L, Chen C
, Zhang X, He L, Chen C ![]() , Wu J
, Wu J
Received 23 April 2025
Accepted for publication 2 August 2025
Published 11 August 2025 Volume 2025:17 Pages 2511—2522
DOI https://doi.org/10.2147/IJWH.S536082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Xuemei Li,1,2,* Qimei Yang,3,* Xia Zhang,1,2 Lidan He,1,2 Chen Chen,4,5 Jianbo Wu1,2
1Department of Obstetrics and Gynecology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 2Department of Obstetrics and Gynecology, National Regional Medical Center, Binhai Campus of The First Affiliated Hospital, Fujian Medical University, Fuzhou, People’s Republic of China; 3Department of Obstetrics, The First People’s Hospital of Yunnan, Kunming, People’s Republic of China; 4Nutrition Department, The First Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 5Nutrition Department, National Regional Medical Center, Binhai Campus of The First Affiliated Hospital, Fujian Medical University, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chen Chen, Nutrition Department, The First Affiliated Hospital of Fujian Medical University, ChaZhong Road 20, Fuzhou, 350000, People’s Republic of China, Email [email protected] Jianbo Wu, Department of Obstetrics and Gynecology, The First Affiliated Hospital of Fujian Medical University, ChaZhong Road 20, Fuzhou, 350000, People’s Republic of China, Email [email protected]
Objective: This study explores the relationship between Life’s Essential 8 (LE8) score and gestational diabetes mellitus (GDM), subsequent diabetes, and mortality, and analyzes the mediating effects of platelet-related indicators and inflammatory markers.
Methods: The study utilized cohort, data from the Nutrition Examination Survey (NHANES), applying logistic regression models and mediation effect analysis to assess the associations between LE8 score and GDM. Potential confounding factors such as age, race, education, PIR, health insurance, and access to healthcare were adjusted to ensure the reliability of the results. Linear mediation analysis, conducted using the “mediation” package with 1000 bootstrap replications, quantified the mediating roles of mean platelet volume (MPV), white blood cell (WBC), and lymphocyte (LYM) counts.
Results: We analyzed data from the NHANES from 2007 to 2018, involving 59,842 participants. Among them, 858 had a history of GDM. Each unit increase in LE8 score reduced GDM odds by 3%. High Cardiovascular health (CVH) individuals exhibited 70% lower GDM risk versus low CVH. WBC (5.8%), LYM (4.8%), and MPV (0.6%) partially mediated LE8-GDM associations, highlighting inflammation’s mechanistic role. High LE8 scores predicted 94% lower diabetes risk post-GDM. Mortality analysis revealed a U-shaped association between LE8 scores and mortality risk, with borderline evidence of nonlinearity (P = 0.069).
Conclusion: As the first study to integrate CVH metrics with platelet/inflammatory biomarkers in GDM pathogenesis, our findings demonstrate that optimizing LE8 scores, particularly through BMI, blood pressure, and lipid control, significantly mitigates GDM risk and complications. Integrating LE8 assessment at first prenatal visit may enable early risk stratification and personalized interventions.
Keywords: gestational diabetes mellitus, life’s essential 8 score, mean platelet volume, inflammatory biomarkers, mediation effect analysis
Introduction
Gestational diabetes mellitus (GDM) is a common metabolic disorder during pregnancy, affecting approximately 2% to 10% of pregnant women worldwide.1 GDM is closely linked to maternal and fetal complications during pregnancy, such as hypertension, preterm birth, and large-for-gestational-age infants, and it also increases the risk of developing type 2 diabetes in the future for the mother.2–4 With the rising global prevalence of diabetes, the prevention and early detection of GDM have become increasingly important issues in public health and clinical medicine.5 However, current GDM screening methods typically focus on monitoring blood glucose levels during pregnancy, often overlooking other factors influencing glucose metabolism, particularly Cardiovascular health (CVH).
The Life’s Essential 8 (LE8) score is a new CVH assessment tool recently introduced.6–8 It evaluates individual CVH by comprehensively assessing eight core health indicators: diet, physical activity, body weight, blood sugar, lipid levels, blood pressure, smoking status, and sleep quality.9 Compared to previous Life’s Simple 7 models, the LE8 score provides a more comprehensive and updated framework that considers sleep and improves diet and glycaemic control indicators, particularly relevant factors during pregnancy.10 Increasing research indicates that good CVH effectively reduces the risk of cardiovascular diseases (CVD) and may also play a positive role in preventing metabolic conditions such as diabetes.11 GDM shares many pathophysiological pathways with CVD, including insulin resistance, chronic inflammation, endothelial dysfunction, and dyslipidemia.12,13 Recent studies have preliminarily demonstrated an association between optimal CVH and a lower prevalence of GDM.14,15 Therefore, risk prediction models incorporating CVH indicators may improve the early identification and prevention of GDM.
Although CVH metrics like LE8 are known to influence the risk of diabetes,16 the specific mediating biological pathways that link them to the pathogenesis of GDM are unknown. As a crucial regulatory factor in metabolic diseases, platelet activity has been confirmed to be abnormally activated throughout the entire diabetes development.17 Basic research indicates that platelets, through the release of active mediators such as thromboxane A2 and P-selectin,18,19 not only directly participate in insulin resistance and vascular endothelial dysfunction but also form a bidirectional regulatory network with chronic low-grade inflammation20—a pathological feature highly overlapping with the core pathogenesis of GDM.21 Notably, biological markers reflecting platelet production rate and activation status, such as mean platelet volume (MPV), potentially exacerbate glucose metabolic disorders through enhanced platelet-endothelial cell interactions.15 Further research reveals that abnormal platelet activity, in conjunction with the synergistic elevation of inflammatory factors, constitutes a typical microenvironment characteristic of GDM,22,23 with this platelet-inflammatory axis playing a key bridging role in mediating the association between CVH and GDM risk.24 Critically, our study identifies and mechanistically demonstrates for the first time the platelet-inflammation axis as a central, novel bridge between CVH (quantified by LE8) and increased GDM risk.
This study investigates the association between LE8 scores and GDM through the NHANES conducted from 2007 to 2018. It also analyzes whether platelet-related indicators and inflammatory markers mediate the relationship between LE8 scores and GDM. Additionally, the study explores the relationship between LE8 scores and the combined risk of GDM with type 2 diabetes mellitus (T2DM) and post-GDM mortality. We hypothesize that improving CVH (increasing LE8 scores) can indirectly reduce the risk of GDM and help lower the risk of T2DM and mortality following GDM. The goal is to provide clinicians with more comprehensive tools for GDM screening, particularly by integrating CVH assessments, platelet activity markers, and inflammatory markers to offer more precise strategies for personalized prevention and management of gestational diabetes.
Methods
Study Population
This study’s data were sourced from the NHANES, a comprehensive population-based survey designed to collect data on the civilian noninstitutionalized US population. Since 1999, NHANES has collected data from approximately 10,000 individuals every two years, utilizing a multi-stage probability sampling design to obtain a representative sample of noninstitutionalized American households.25 The current study’s population is drawn from four “continuous NHANES” cycles (2007/2008, 2009/2010, 2011/2012, 2013/2014, 2015/2016, 2017/2018), with an initial cohort of 59,842 participants. First, individuals younger than 20 years (n = 41,935) were excluded, leaving 17,907 females aged ≥20 years or older. Next, participants without data on a history of gestational diabetes mellitus (GDM) were excluded (n = 5097), resulting in 12,810 individuals with GDM history data. Subsequently, those lacking data on Life’s Essential 8 were excluded (n = 1811), yielding a final primary analysis sample of 10,999 participants. Within this final sample, 858 participants had a history of GDM, while 10,141 participants had no history of GDM (Figure 1).
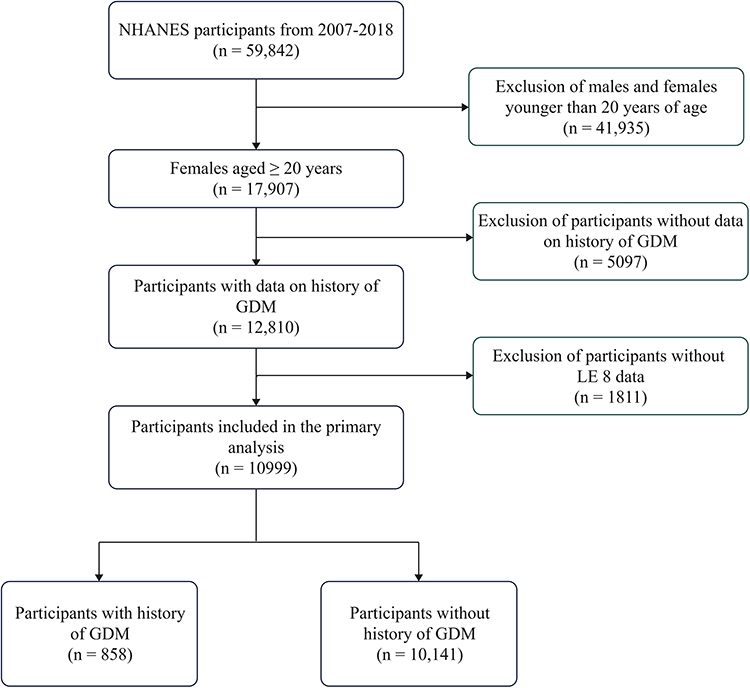 |
Figure 1 Flow chart for the selection of participants in this study. Abbreviations: NHANES, Nutrition Examination Survey; LE8, Life’s Essential 8; GDM, gestational diabetes mellitus. |
Definition of Gestational Diabetes
The reproductive health questionnaire in NHANES defines GDM. GDM is diagnosed based on the question, “During your pregnancy, was a doctor or other health professional ever told you that you had diabetes, sugar diabetes, or gestational diabetes?” Additionally, the questionnaire specifies, “Please do not include diabetes that you may have known about before your pregnancy”. Women are considered to have GDM if they answer “yes” when asked if they were previously diagnosed with GDM during a medical screening or if they were told by a health professional that they had GDM.26
Definition of Diabetes with a GDM History
Based on previous research,27 among individuals not currently pregnant, diabetes is diagnosed if any of the following conditions are met: (1) answering “Yes” to the questionnaire item “Apart from during pregnancy, has a doctor or healthcare professional ever told you that you have diabetes or sugar diabetes?”; (2) HbA1c level ≥ 6.5%; (3) fasting glucose (mmol/L) ≥ 7.0; (4) two-hour oral glucose tolerance test (OGTT) blood glucose (mmol/L) ≥ 11.1.
Definition of Death
The mortality follow-up data in this study were obtained from the death records database publicly released by the National Health Center (NHC) in 2019.28 The follow-up period was calculated from when the participants completed their baseline examination at the Mobile Examination Center (MEC) to the date of death or the end of follow-up (December 31, 2019), whichever occurred first.
Measurement of Life’s Essential 8 Scores
The LE8 score includes four health behaviors (diet, physical activity, nicotine exposure, and sleep health) and four health factors (body mass index, non-high-density lipoprotein cholesterol, blood glucose, and blood pressure).29 The LE8 scores for each indicator, calculated using NHANES data, have been previously published.30 The detailed algorithm for calculating the LE8 score has been thoroughly described in previous literature.31 First, each CVH metric is scored on a scale of 0 to 100. Second, the overall LE8 score is the arithmetic mean of these eight metrics, ranging from 0 to 100. Participants are then categorized into three LE8 health categories: 80–100 is considered high CVH, 50–79 is considered moderate CVH, and 0–49 indicates low CVH. Health behavior and health factor classifications are also determined using the aforementioned method.
Dietary scores are assessed using the Healthy Eating Index-2015 (HEI-2015) quintile. HEI-2015 scores are calculated based on dietary intake, with data collected through two 24-hour nutritional recalls combined with United States Department of Agriculture(USDA) food pattern equivalents. Per week, physical activity scores are measured by self-reported minutes of moderate (or higher) intensity activity, derived from frequency and duration of vigorous or moderate level activities over the past 30 days. Nicotine exposure scores are calculated based on smoking status (never smoker, former smoker, and current smoker) and years since quitting smoking. Sleep health scores are measured by self-reported average hours of sleep per night. The four health factors are scored according to their respective criteria. Height, weight, and blood pressure are measured during physical examination. BMI is calculated as weight (kg) divided by height (m) squared. Blood pressure is determined by the average reading of three consecutive measurements. Blood lipid, plasma glucose, and HbA1c determinations are based on blood samples analyzed at a central laboratory.32
Measurement of Mediators
According to the NHANES protocol for the 2007–2018 cycle, peripheral blood samples obtained from the NHANES Mobile Examination Centers (MEC) were analyzed for hematocrit counts using Beckman Coulter counting and sorting methods, combined with automated dilution and mixing equipment, and hemoglobin measurements using a single-beam photometer. In this study, inflammatory biomarkers of the examined participants included white blood cell (WBC) count, neutrophil (NEU) count, lymphocyte (LYM) count, platelet (PC) count, and mean platelet volume (MPV). The LYM, NEU, and PC count units were 109 cells/L.33
Covariates
This study collected sociodemographic and lifestyle factors and adjusted sociodemographic characteristics, including age, race, education, access to healthcare, health insurance, and the ratio of household income to the poverty threshold (PIR). Racial categories include Mexican American, non-Hispanic Black, non-Hispanic White, other Hispanic, and multiracial. Educational attainment categories include less than 9th grade, 9th to 11th grade, high school graduate/GED or equivalent, some college or associate degree, and college graduate or higher.
Statistical Analysis
Categorical variables were reported as percentages, and differences between groups were compared using chi-square tests. Continuous variables that did not meet standard distribution criteria were presented as a median and interquartile range [median (25th, 75th)], with group differences assessed using the Wilcoxon rank-sum test. Multiple imputation by chained equations (MICE) to impute missing covariate data. Initially, we evaluated the association between LE8 score and GDM history using logistic regression with three models: Crude model (unadjusted), Model 1 (adjusted for age), and Model 2 (further adjusted for race, education, PIR, health insurance, and access to healthcare). The LE8 score was analyzed as a continuous and three-category variable, with results presented as odds ratios (ORs) and 95% confidence intervals (CIs). Restricted cubic splines (RCS) were used further to investigate potential nonlinear associations between LE8 score and GDM.
Additionally, the study examined the potential mediating effects of a series of clinical indicators (MPV, PC, WBC, LYM, NEU count) on the association between LE8 score and GDM, using the “mediation” package for mediation analysis, with 1000 bootstrap applications. We systematically tested the fundamental assumptions of the mediation model. Specifically: (1) The assumption of linearity between variables was tested using regression analysis, and the results indicated that the prerequisite for a linear model was met. (2) Guided by existing literature and theory, we included a series of potential confounding variables as covariates in the mediation model to reduce potential bias from omitted variables. Considering the relationship between GDM history and subsequent diabetes, the association between LE8 score and post-GDM diabetes risk was further analyzed using logistic regression and RCS. We also conducted a Cox proportional hazards regression model to explore the association between LE8 score and subsequent mortality risk in GDM patients, presenting results as hazard ratios (HRs) and 95% CIs. The proportional hazards assumption of the Cox model was tested using Schoenfeld residuals, which were satisfied. Furthermore, we performed subgroup analyses and assessed interactions between stratification variables and LE8 scores concerning outcomes. This study used R software (version 4.3.1) for data analysis, with a two-sided P value < 0.05 indicating statistical significance.
Result
Baseline Data and Population Characteristics
This study included 10,999 participants (858 in the GDM group and 10,141 in the non-GDM group). The median age of the GDM group (45 years) was significantly lower than that of the non-GDM group (54 years) (P < 0.001). Participants in the GDM group were more likely to be non-Hispanic white or Mexican American and had higher educational levels (P < 0.05). Additionally, the rate of healthcare access was slightly lower in the GDM group compared to the non-GDM group (88.1% vs 90.3%, P = 0.049). The total LE8 score was significantly lower in the GDM group compared to the non-GDM group (62.82 vs 65.52, P < 0.001). Regarding inflammatory markers, the GDM group had substantially higher MPV (8.29 fl vs 8.21 fl, P = 0.028), PC, WBC, LYC, and NEU count (P < 0.001) (Table 1).
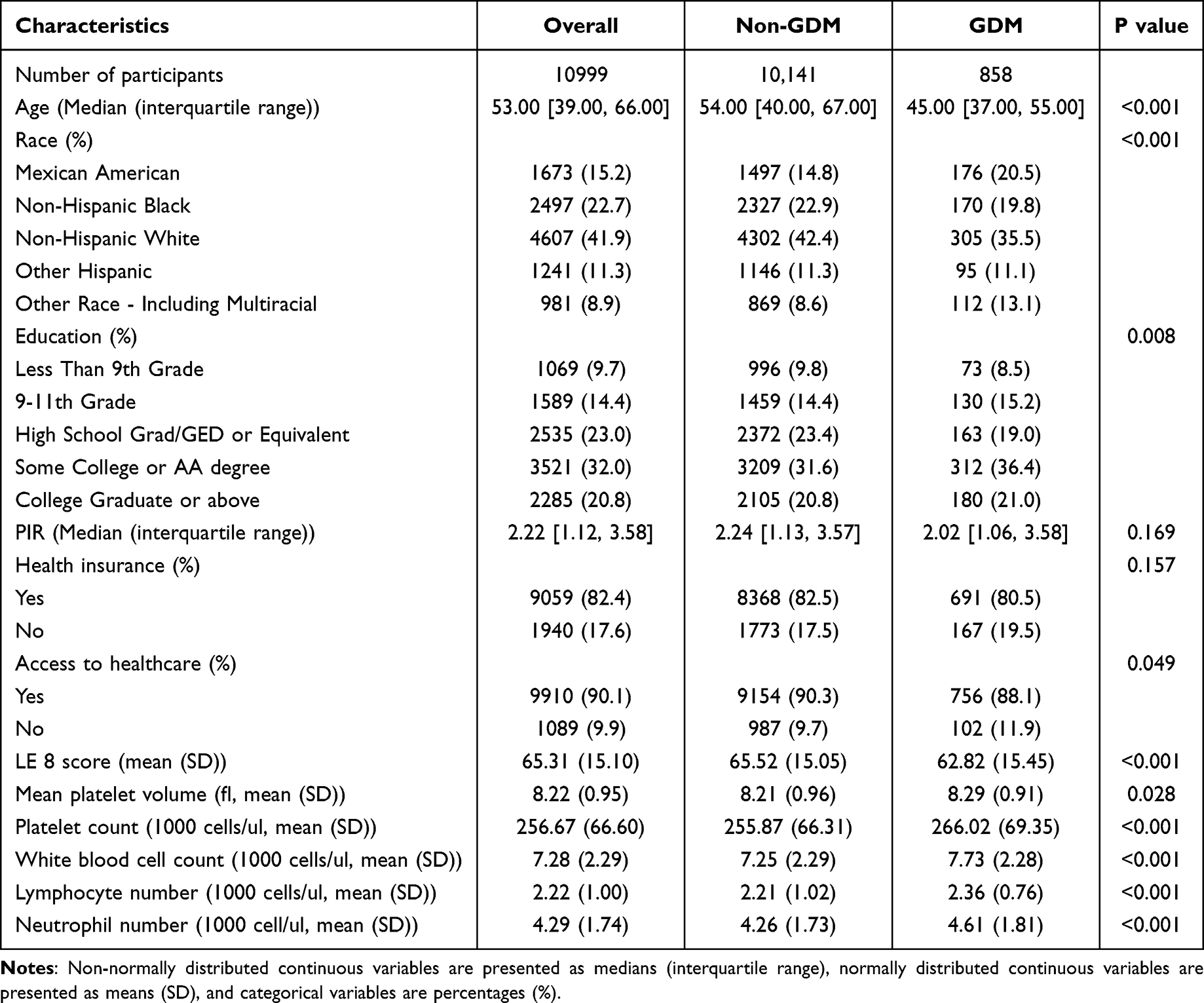 |
Table 1 Basic Characteristics and Laboratory Data for Study Population Stratified by History of GDM |
Analysis of the Association Between LE8 and GDM Risk
Table 2 presents the association between LE8 scores and GDM history. After adjusting for multiple confounding factors, it was found that with increasing LE8 scores, the prevalence of GDM significantly decreased (OR = 0.97). When the LE8 score was treated as a categorical variable, the likelihood of high CVH was reduced by 70% compared to the low CVH group (OR = 0.30). Further analysis using restricted cubic splines (RCS) to explore the relationship between LE8 scores and GDM revealed a clear linear association (P for overall < 0.0001, nonlinear association was observed = 0.3803) (Figure 2A). When analyzing based on the eight components of LE8, more pronounced associations were observed between lipid levels, blood pressure, BMI, and GDM history (Figure 3 and Supplementary Table 1). In subgroup analyses (Figure 4), the relationship between LE8 scores and GDM history across different populations was examined. This analysis found no significant differences in the protective effect of LE8 on GDM risk among subgroups defined by age, education level, PIR, health insurance, and access to healthcare services (P for interaction > 0.05), providing evidence for regression model development.
 |
Table 2 Association of LE 8 Score and History of Gestational Diabetes (n = 10,999) |
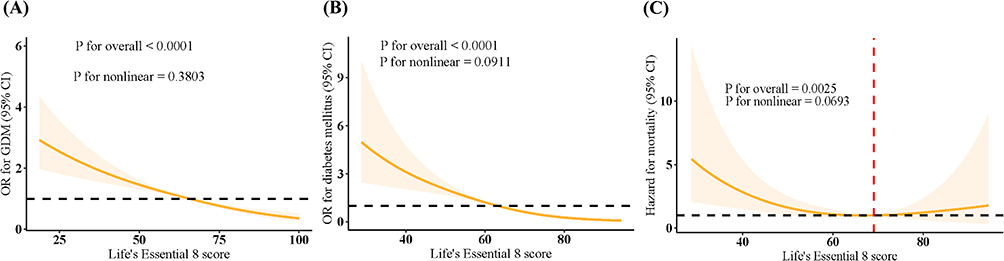 |
Figure 2 Analysis of the association between LE8 score and the prevalence of (A) GDM, (B) diabetes mellitus among women with a history of GDM, and (C) mortality risk in women with a history of GDM using the restricted cubic spline. Model adjusted for age, race, education, PIR, health insurance, and access to healthcare. |
 |
Figure 3 Association of each component of LE 8 with the history of GDM. Model adjusted for age, race, education, PIR, health insurance, and access to healthcare. |
 |
Figure 4 Subgroup analysis of the association between LE8 score and history of GDM. |
This trend is also observed in diabetic patients with a history of GDM. Upon further analysis of the association between LE8 scores and the presence of diabetes mellitus in female participants with a history of GDM, it was similarly found that the high CVH group had a significantly lower prevalence of diabetes compared to the low CVH group (OR = 0.06). The trend remains significant after adjusting for potential confounders such as age, race, education, PIR, health insurance, and access to healthcare services. RCS analysis reveals a linear association (P < 0.001) (Table 3). This significant linear association was also observed between the two in the RCS (Figure 2B).
 |
Table 3 Association of LE 8 Score and the Presence of Diabetes Mellitus in Female Participants with a History of GDM (n = 835) |
The Intermediary Effect of Inflammatory Mediators
In the mediation analysis, it was observed that MPV, WBC count, and LYM count exhibited significant mediating effects on the association between LE8 score and history of GDM (P < 0.05). The proportion mediated by WBC count was the highest at 5.8%, followed by LYM count at 4.8% and MPV at 0.6% (Figure 5).
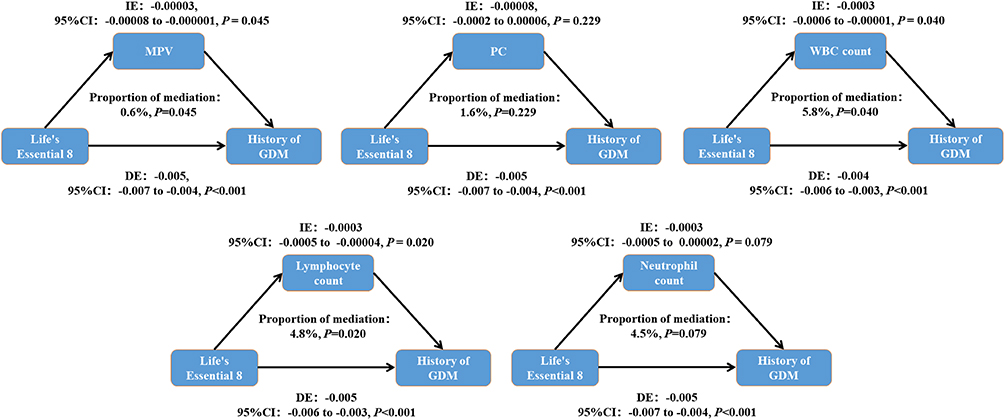 |
Figure 5 The role of a series of CBC results in mediating the association between LE8 score and GDM. IE is the estimate of the indirect effect; DE is the estimate of the direct effect. Model adjusted for age, race, education, PIR, health insurance, and access to healthcare. |
Long-Term Prognosis Outcome Tracking
Table 4 demonstrates the association between LE8 scores and mortality risk among participants with a history of GDM. In unadjusted models (HR=0.95, 95% P<0.001), age-adjusted models (HR=0.96, P<0.001), and further adjusted models accounting for race, education, and health insurance (HR=0.97, P=0.005), LE8 scores consistently showed significant protective effects. Compared to moderate CVH (50–79), individuals with low CVH (0–49) exhibited significantly increased mortality risk (HR=3.09). However, those with high CVH did not show a significant change in mortality risk compared to those with moderate CVH (P>0.05). RCS showed a U-shaped trend between LE8 and mortality risk in GDM patients (P for overall=0.003, P for non-linearity=0.069) (Figure 3C).
 |
Table 4 LE 8 Score and Risk of Mortality in Female Participants with a History of GDM (n = 835) |
Discussion
This study systematically elucidates the complex association between the LE8 score and the risk of GDM and its related prognostic outcomes for the first time. Through multidimensional analysis of 10,999 samples from the US NHANES cohort, we confirmed a significant negative correlation between LE8 score and GDM, with this protective effect being particularly pronounced in the low BMI subgroup. Inflammatory biomarkers (MPV, WBC, NEU, and NLR count) were significantly elevated in women with a history of GDM, highlighting the critical role of inflammation in developing GDM. More importantly, inflammatory biomarkers were found to mediate the association between LE8 and GDM, providing new biological insights into the pathological mechanisms by which CVH impacts glucose metabolism. Additionally, this study found that improving CVH (by increasing the LE8 score) is crucial for preventing GDM and its long-term consequences, including diabetes and mortality, through reducing inflammation.
Previous studies have primarily focused on the impact of single metabolic indicators on GDM,34,35 and earlier studies on CVH and GDM mainly relied on the LE 7 framework.15 In contrast, our study represents the first application of the updated LE8 score in GDM pathogenesis. The LE8’s novel inclusion of sleep health provides a more granular assessment of metabolic vulnerabilities during pregnancy. Our findings indicate that BMI, blood pressure control, and lipid metabolism indicators in the LE8 score contribute most significantly to predicting GDM risk, highlighting the central role of body composition regulation and vascular homeostasis in maintaining glucose tolerance during pregnancy.
Previous research has established a connection between CVH and diabetes, but detailed mechanistic explorations on how improving CVH can reduce the risk of GDM are lacking.13,36 Unlike LE7 studies that focused on CVD endpoints,15 we mechanistically linked LE8 to GDM through platelet-immune crosstalk (MPV/WBC-mediated effects), a pathway previously unexplored in gestational metabolic dysregulation. It has been shown that GDM is a chronic low-grade inflammation in the pathophysiologic process.37 Most studies support that a significant increase in WBC in early and mid-pregnancy may be a clinical feature of abnormal glucose metabolism.38 Inflammation can trigger vascular injury and dysfunction, and activate platelet activation and aggregation. Therefore, platelet-related indicators may indirectly reflect the inflammatory state. Current studies have shown that platelets are not significantly correlated with GDM.39 Instead, MPV may be a potential early predictor of GDM as an indicator for evaluating platelet morphology and activity; Elevated MPV (>7.38 fl) in early pregnancy was found to be a valid predictor of GDM (AUC 0.577 and 0.704, respectively).40 Elevated MPV at 24–28 weeks of gestation was an independent risk factor for the development of GDM (OR 1.56 and 4.0, AUC = 0.639, respectively).41,42 We observed by mediation analysis that MPV, WBC count, and LYM count exhibited significant mediation in the association between LE8 score and history of GDM (P < 0.05), with the highest proportion of mediation by WBC count (5.8%), 4.8% by LYM count, and 0.6% by MPV, further suggesting that improvement in cardiovascular health may be achieved by in turn reducing vascular endothelial damage and inflammatory responses, ultimately reducing the incidence of GDM. This finding provides a novel clinical perspective, suggesting that in the prevention and treatment of gestational diabetes mellitus, the assessment of cardiovascular health and inflammatory indicators should be emphasized in addition to routine glucose monitoring. Our mediation analysis further establishes that LE8’s protective effects against GDM are partially (5.8–0.6%) but mechanistically driven by inflammatory biomarkers. This proposes a new paradigm for targeting platelet activity and subclinical inflammation in GDM prevention.
This study also revealed that the LE8 score was significantly and negatively associated with the risk of all-cause mortality in patients with a history of GDM and concomitant diabetes. Our finding mechanistically echoes several essential studies. The Prognostic Nutritional Index (PNI), a composite indicator of immuno-inflammatory and nutritional status, is significantly negatively associated with the risk of all-cause mortality (HR=0.90, 95% CI:0.84–0.96) and cardiovascular disease (CVD) mortality (HR=0.91, 95% CI:0.88–0.94) in GDM patients.43 LE8, as a health scoring system covering 8 dimensions such as diet, exercise, and BMI, may play a protective role by improving the above pathways (elevating serum albumin levels and modulating lymphocyte-mediated inflammatory responses). Longitudinal cohort studies have shown that a history of GDM increases women’s future risk of type 2 diabetes 7–10 fold and is independently associated with cardiovascular mortality (HR=1.59, 95% CI:1.03–2.47).44 This association stems from standard pathological mechanisms such as insulin resistance and endothelial dysfunction caused by GDM, and health behaviors (tobacco control, blood pressure management) in the LE8 score may reduce risk by intervening in these mechanisms. Notably, a history of GDM alone was weakly associated with mortality, but the risk of all-cause mortality (HR=2.11, 95% CI:1.21–3.68) and cardiac death (HR=2.46, 95% CI:1.66–3.64) was significantly elevated when progressing to overt diabetes.45 The study suggests that the modulation of metabolic status by LE8 score may achieve mortality reduction by delaying the progression of diabetes, especially in the high-risk subgroup of combined gestational hypertension and low birth weight.43 Similar to the threshold phenomenon (75% risk reduction at PNI=50.75) found in the PNI study,43 similar thresholds (≤60) may exist for LE8 scores, which can be used to identify high-risk populations for prioritized intervention. This stratified management strategy has been validated in patients with chronic kidney disease (CKD), with each 10-point improvement in LE8 reducing the risk of all-cause mortality by 17%,46 suggesting its potential application in the GDM population.
Our findings support using the LE8 score as a practical early GDM risk assessment tool. Because the LE8 contains modifiable behavioral and metabolic risk factors, it can be integrated into routine antenatal care, especially for women who benefit from targeted lifestyle or medical interventions early in pregnancy. Clinicians can implement the LE8 assessment using standardized tools, such as lifestyle factors (diet, activity, sleep), via patient questionnaires and clinical measures (BMI, blood pressure, lipids, glucose) from routine laboratory work and physical examination. Embedding the LE8 score in the electronic health record could further facilitate its use in risk stratification and care planning. In addition, our study highlights MPV as a potentially helpful biomarker reflecting underlying inflammatory or thrombotic activity. MPV can be obtained from standard complete blood counts and monitored alongside LE8 metrics to provide a more nuanced risk map for GDM. In high-risk patients, continuous MPV tracking may help guide the timing and intensity of preventive interventions. Therefore, combining LE8 scores with traditional GDM screening methods provides a more comprehensive and effective evaluation system for clinical use, enabling early identification and personalized intervention to reduce the incidence of GDM and subsequent metabolic disease risks.
Although this study ensured robust results through strict multivariable adjustments (including PIR, healthcare accessibility, and other social determinants), several limitations should be noted. The cross-sectional design makes it difficult to rule out reverse causality. It necessitates prospective cohort validation with pre-pregnancy baseline data, particularly examining how the LE8 score functions within intervention measures (diet, exercise, and pharmacotherapy). Additionally, exploring the relationship between the LE8 score and other diabetes-related biomarkers (insulin resistance and insulin secretion) could deepen our understanding of the pathophysiology of GDM. The sample primarily consists of individuals from the United States, necessitating race-specific validation in regions with high GDM incidence rates, such as Asia, to further validate the universal applicability of the relationship between CVH and GDM. Future efforts should establish dynamic intervention models based on the LE8 score. Moreover, our mediation analysis indicates that improved CVH may reduce GDM incidence by modulating platelet activation levels, thereby decreasing vascular endothelial damage and inflammatory responses. This finding offers a new perspective for clinical practice, suggesting that in preventing and treating GDM, attention should be given to routine blood glucose monitoring and assessing CVH and inflammatory indicators.
Conclusion
This study reveals a negative correlation between good CVH and the risk of GDM as the first study to integrate and explore the mediating role of MPV and a series of inflammatory cell markers in this process. It also identifies that good CVH is associated with better outcomes in GDM patients, such as reduced mortality and lower subsequent incidence of diabetes. The findings provide a theoretical basis for applying interventions to improve CVH in preventing and managing GDM, emphasizing the importance of CVH assessment in prenatal diabetes screening. This discovery offers new directions for future clinical management and preventive strategies of GDM and has significant public health implications.
Data Sharing Statement
The data were publicly available from NHANSE (https://www.cdc.gov/nchs/nhanes/).
Ethics Approval and Consent to Participate
This study utilized de-identified data from the National Health and Nutrition Examination Survey (NHANES), which has been ethically approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board (ERB). All participants provided written informed consent. According to Article 32 (Items 1 and 2) of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, our use of this anonymized secondary data is exempt from further ethical review.
Acknowledgments
The authors expressed gratitude to NHANES for data collection and quality control.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bauer ST, Cate J, Whitsel AI, Combs CA. Society for maternal-fetal medicine special statement: quality metric on the rate of postpartum diabetes screening after pregnancies with gestational diabetes mellitus. Am J Obstet Gynecol. 2023;228(4):B2–B9. doi:10.1016/j.ajog.2022.12.315
2. Geetha KSRC, Sakshi R, Chandana T. Risk of cardiovascular diseases in women with gestational diabetes. Int J Health Sci Res. 2023;13(12):215–222. doi:10.52403/ijhsr.20231226
3. Moon JH, Jang HC. Gestational diabetes mellitus: diagnostic approaches and maternal-offspring complications. Diabetes Metab J. 2022;46(1):3–14. doi:10.4093/dmj.2021.0335
4. Siddiqui K, George TP. The potential impact of gestational diabetes mellitus on long-term kidney disease: a narrative review. European Med J Diabetes. 2024;57–64.
5. Gallagher C, Hill J. Gestational diabetes mellitus prevention: a commentary. Pract Midwife. 2024;27(5):24–28. doi:10.55975/TPDP7486
6. Li X, Ma H, Wang X, Feng H, Qi L. Life’s essential 8, genetic susceptibility, and incident cardiovascular disease: a prospective study. Arterioscler Thromb Vasc Biol. 2023;43(7):1324–1333. doi:10.1161/ATVBAHA.123.319290
7. Ma H, Wang X, Xue Q, et al. Cardiovascular health and life expectancy among adults in the United States. Circulation. 2023;147(15):1137–1146. doi:10.1161/CIRCULATIONAHA.122.062457
8. Isiozor NM, Kunutsor SK, Voutilainen A, Laukkanen JA. Life’s essential 8 and the risk of cardiovascular disease death and all-cause mortality in Finnish men. Eur J Prev Cardiol. 2023;30(8):658–667. doi:10.1093/eurjpc/zwad040
9. Rempakos A, Prescott B, Mitchell GF, Vasan RS, Xanthakis V. Association of life’s essential 8 with cardiovascular disease and mortality: the Framingham heart study. J Am Heart Assoc. 2023;12(23):e30764. doi:10.1161/JAHA.123.030764
10. Wang Q, Schmidt AF, Lennon LT, Papacosta O, Whincup PH, Wannamethee G. Association of life’s simple 7 lifestyle metric with cardiometabolic disease-free life expectancy in older British men. Commun Med. 2024;4(1):104. doi:10.1038/s43856-024-00534-7
11. Zhang Y, Liu C, Xu Y, et al. The management correlation between metabolic index, cardiovascular health, and diabetes combined with cardiovascular disease. Front Endocrinol. 2022;13:1036146. doi:10.3389/fendo.2022.1036146
12. Sharma AK, Singh S, Singh H, et al. Deep insight of the pathophysiology of gestational diabetes mellitus. Cells-Basel. 2022;11(17):2672.
13. McElwain CJ, Tuboly E, McCarthy FP, McCarthy CM. Mechanisms of endothelial dysfunction in pre-eclampsia and gestational diabetes mellitus: windows into future cardiometabolic health? Front Endocrinol. 2020;11:655. doi:10.3389/fendo.2020.00655
14. Qin L, Fan Z, Shi Q, et al. Relationship between life’s essential 8 and the risk of gestational diabetes among us adults. J Matern Fetal Neonatal Med. 2024;37(1):2407037. doi:10.1080/14767058.2024.2407037
15. Sadiq R, Broni EK, Levine LD, Retnakaran R, Echouffo-Tcheugui JB. Association of ideal cardiovascular health and history of gestational diabetes mellitus in NHANES 2007-2018. Diabet Res Clin Pract. 2024;217:111857. doi:10.1016/j.diabres.2024.111857
16. Tian X, Chen S, Xu Q, et al. Longitudinal cardiovascular health measured by life’s essential 8 metrics with incident diabetes: a 13-year prospective cohort study. Diabetes Metab Res Rev. 2024;40(3):e3757. doi:10.1002/dmrr.3757
17. Gulia M, Gupta M, Singh LS, Singla M, Tahlan A, Kaur J. Mean platelet volume and glycaemic control in patients with new-onset Type 2 diabetes mellitus. J R Coll Physicians Edinb. 2022;52(2):105–109. doi:10.1177/14782715221107948
18. Izzi B, Gialluisi A, Gianfagna F, et al. Platelet distribution width is associated with P-selectin dependent platelet function: results from the moli-family cohort study. Cells-Basel. 2021;10(10):2737.
19. Liu W, Pircher J, Schuermans A, et al. Jak2 V617F clonal hematopoiesis promotes arterial thrombosis via platelet activation and cross talk. Blood. 2024;143(15):1539–1550. doi:10.1182/blood.2023022260
20. Moin A, Al-Qaissi A, Sathyapalan T, Atkin SL, Butler AE. Platelet protein-related abnormalities in response to acute hypoglycemia in type 2 diabetes. Front Endocrinol. 2021;12:651009. doi:10.3389/fendo.2021.651009
21. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287(19):2570–2581. doi:10.1001/jama.287.19.2570
22. Sun X, Sun H, Li P. Association of circulating inflammatory cells and platelets with gestational diabetes and pregnancy outcomes. Clin Chim Acta. 2021;523:87–96. doi:10.1016/j.cca.2021.09.004
23. Xiao Y, Zhang H, An S, et al. Single and joint associations between blood cell-based inflammatory indicator in early pregnancy and risk of gestational diabetes mellitus (GDM): a prospective cohort study. Am J Reprod Immunol. 2024;92(6):e70021. doi:10.1111/aji.70021
24. Feng Y, Lin H, Tan H, Liu X. Life’s essential 8 metrics and mortality outcomes in insulin resistance: the role of inflammation, vascular aging, and gender. Clin Nutr ESPEN. 2024;61:131–139. doi:10.1016/j.clnesp.2024.03.004
25. Liu F, You F, Yang L, et al. Nonlinear relationship between oxidative balance score and hyperuricemia: analyses of NHANES 2007-2018. Nutr J. 2024;23(1):48. doi:10.1186/s12937-024-00953-1
26. Zeng Y, Piao Y. Association analysis of dietary inflammatory index and gestational diabetes mellitus: based on national health and nutrition examination survey database. Exp Clin Endocrinol Diabetes. 2024;132(8):453–462. doi:10.1055/a-2293-7983
27. Wei Y, Lin Y, Huang L, Wang C, Li R. Association between mean platelet volume and the risk of type 2 diabetes mellitus among women with history of gestational diabetes mellitus. Bmc Endocr Disord. 2024;24(1):159. doi:10.1186/s12902-024-01693-3
28. Lin F, Shi Y, Zou X, et al. Coffee consumption and all-cause and cardiovascular mortality in older adults: should we consider cognitive function? Front Nutr. 2023;10:1150992. doi:10.3389/fnut.2023.1150992
29. Lloyd-Jones DM, Allen NB, Anderson C, et al. Life’s essential 8: updating and enhancing the American heart association’s construct of cardiovascular health: a presidential advisory from the American heart association. Circulation. 2022;146(5):e18–e43. doi:10.1161/CIR.0000000000001078
30. Ma R, Song J, Ding Y. Associations between Life’s Essential 8 and post-stroke depression and all-cause mortality among US adults. Eur J Med Res. 2024;29(1):229. doi:10.1186/s40001-024-01834-3
31. Ren Y, Cai Z, Guo C, et al. Associations between life’s essential 8 and chronic kidney disease. J Am Heart Assoc. 2023;12(24):e30564. doi:10.1161/JAHA.123.030564
32. Pang S, Wang Y, Sun S, et al. Associations between life’s essential 8 and insulin resistance among nondiabetic adults. J Am Heart Assoc. 2024;13(13):e33997. doi:10.1161/JAHA.123.033997
33. Zhang H, Liu X, Wang X, Jiang Y. Association of two novel systemic inflammatory biomarkers and frailty based on NHANES 2007-2018. Front Public Health. 2024;12:1377408. doi:10.3389/fpubh.2024.1377408
34. An Z, Niu T, Lu Y, et al. Nonlinear association between alanine aminotransferase to high-density lipoprotein cholesterol ratio and risk of gestational diabetes mellitus. Sci Rep. 2024;14(1):24872. doi:10.1038/s41598-024-76656-8
35. Henriksson P, Sandborg J, Soderstrom E, et al. Associations of body composition and physical fitness with gestational diabetes and cardiovascular health in pregnancy: results from the HealthyMoms trial. Nutr Diabetes. 2021;11(1):16. doi:10.1038/s41387-021-00158-z
36. Nakshine VS, Jogdand SD. A comprehensive review of gestational diabetes mellitus: impacts on maternal health, fetal development, childhood outcomes, and long-term treatment strategies. Cureus. 2023;15(10):e47500. doi:10.7759/cureus.47500
37. Seyhanli Z, Seyhanli A, Aksun S, Pamuk BO. Evaluation of serum Angiopoietin-like protein 2 (ANGPTL-2), Angiopoietin-like protein 8 (ANGPTL-8), and high-sensitivity C-reactive protein (hs-CRP) levels in patients with gestational diabetes mellitus and normoglycemic pregnant women. J Matern Fetal Neonatal Med. 2022;35(25):5647–5652. doi:10.1080/14767058.2021.1888919
38. Baki YS, Bezirganoglu AN, Bayoglu TY. Monocyte-to-lymphocyte ratio in the early second trimester is a predictor of gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2024;37(1):2371979. doi:10.1080/14767058.2024.2371979
39. Simsek D, Akselim B, Altekin Y. Do patients with a single abnormal OGTT value need a globally admitted definition such as “borderline GDM”? Pregnancy outcomes of these women and the evaluation of new inflammatory markers. J Matern Fetal Neonatal Med. 2021;34(22):3782–3789. doi:10.1080/14767058.2021.1946779
40. Huang Y, Chen X, You ZS, et al. The value of first-trimester platelet parameters in predicting gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2022;35(11):2031–2035. doi:10.1080/14767058.2020.1774543
41. Fashami MA, Hajian S, Afrakhteh M, Khoob MK. Is there an association between platelet and blood inflammatory indices and the risk of gestational diabetes mellitus? Obstet Gynecol Sci. 2020;63(2):133–140. doi:10.5468/ogs.2020.63.2.133
42. Liu W, Lou X, Zhang Z, Chai Y, Yu Q. Association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, mean platelet volume with the risk of gestational diabetes mellitus. Gynecol Endocrinol. 2021;37(2):105–107. doi:10.1080/09513590.2020.1780579
43. Cao J, Bu X, Chen J, Zhang X. Associations of prognostic nutritional index with risk of all-cause and cardiovascular disease mortalities in persons with gestational diabetes mellitus: a NHANES-based analysis. Diab Vasc Dis Res. 2024;21(5):1507127097. doi:10.1177/14791641241284409
44. Christensen MH, Rubin KH, Petersen TG, et al. Cardiovascular and metabolic morbidity in women with previous gestational diabetes mellitus: a nationwide register-based cohort study. Cardiovasc Diabetol. 2022;21(1):179. doi:10.1186/s12933-022-01609-2
45. Ying Q, Xu Y, Zhang Z, Cai L, Zhao Y, Jin L. Gestational diabetes mellitus and risk of long-term all-cause and cardiac mortality: a prospective cohort study. Cardiovasc Diabetol. 2024;23(1):47. doi:10.1186/s12933-024-02131-3
46. Chen H, Tang H, Huang J, Luo N, Zhang X, Wang X. Life’s essential 8 and mortality in US adults with chronic kidney disease. Am J Nephrol. 2023;54(11–12):516–527. doi:10.1159/000533257
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.