Back to Journals » Cancer Management and Research » Volume 11
Cardiovascular disease-related chronic conditions among Veterans Affairs nonmetastatic colorectal cancer survivors: a matched case–control analysis
Authors Zullig LL, Smith VA, Lindquist JH, Williams CD, Weinberger M, Provenzale D, Jackson GL, Kelley MJ ![]() , Danus S, Bosworth HB
, Danus S, Bosworth HB ![]()
Received 16 October 2018
Accepted for publication 29 May 2019
Published 22 July 2019 Volume 2019:11 Pages 6793—6802
DOI https://doi.org/10.2147/CMAR.S191040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rituraj Purohit
Leah L Zullig,1,2 Valerie A Smith,1,2 Jennifer H Lindquist,1 Christina D Williams,3,4 Morris Weinberger,1,5 Dawn Provenzale,1,4 George L Jackson,1,2 Michael J Kelley,6–8 Susanne Danus,1 Hayden B Bosworth1,2,9
1Center for Health Services Research in Primary Care, Durham Veterans Affairs Health Care System, Durham, NC, USA; 2Department of Population Health Sciences, Duke University, Durham, NC, USA; 3Division of Medical Oncology, Department of Medicine, Duke University, Durham, NC, USA; 4Cooperative Studies Program Epidemiology Center, Durham, NC, USA; 5Department of Health Policy and Management, University of North Carolina, Chapel Hill, NC, USA; 6Office of Specialty Care Services, Department of Veterans Affairs, Washington, DC, USA; 7Hematology-Oncology Service, Durham Veterans Affairs Medical Center, Durham, NC, USA; 8Department of Medicine, Duke University, Durham, NC, USA; 9Departments of Psychiatry and School of Nursing, Duke University, Durham, NC, USA
Purpose: The growing number of colorectal cancer (CRC) survivors often have multiple chronic conditions. Comparing nonmetastatic CRC survivors and matched noncancer controls, our objectives were to determine the odds of CRC survivors being diagnosed with cardiovascular disease (CVD)-related chronic conditions and their likelihood of control during the year after CRC diagnosis.
Patients and methods: We retrospectively identified patients diagnosed with nonmetastatic CRC in the Veterans Affairs health care system from fiscal years 2009 to 2012 and matched each with up to 3 noncancer control patients. We used logistic regression to assess differences in the likelihood of being diagnosed with CVD-related chronic conditions and control between nonmetastatic CRC survivors and noncancer controls.
Results: We identified 9,758 nonmetastatic CRC patients and matched them to 29,066 noncancer controls. At baseline, 69.4% of CRC survivors and their matched controls were diagnosed with hypertension, 52.4% with hyperlipidemia, and 36.7% with diabetes. Compared to matched noncancer controls, CRC survivors had 57% higher odds of being diagnosed with hypertension (OR=1.57, 95% CI=1.49–1.64) and 7% higher odds of controlled blood pressure (OR=1.07, 95% CI 1.02, 1.13) in the subsequent year. Compared to matched noncancer control patients, CRC survivors had half the odds of being diagnosed with hyperlipidemia (OR=0.50, 95% CI=0.48–0.52) and lower odds of low-density lipoprotein (LDL) control (OR 0.88, 95% CI 0.81–0.94). There were no significant differences between groups for diabetes diagnoses or control.
Conclusion: Compared to noncancer controls, nonmetastatic CRC survivors have 1) greater likelihood of being diagnosed with hypertension and worse blood pressure control in the year following diagnosis; 2) lower likelihood of being diagnosed with hyperlipidemia or LDL control; and 3) comparable diabetes diagnoses and control. There may be a need for hypertension control interventions targeting cancer survivors.
Keywords: Veterans Affairs, colorectal neoplasms, cancer survivors, cardiovascular disease, comorbidity, chronic disease management
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in the US as well as users of the Veterans Affairs (VA) health care system.1–4 CRC survival rates are improving, resulting in a large population of CRC survivors.5,6 There are an estimated 750,000 living CRC survivors in the US.7 With this increased survivability of CRC, many CRC survivors must also focus on and manage other chronic conditions.
In addition to their CRC, many survivors are also diagnosed with multiple chronic conditions.8 For cardiovascular disease (CVD), the presence of CVD-related chronic conditions may be partially attributed to shared risk factors such as obesity, physical inactivity, diet, and other lifestyle behaviors.9–12 When combined, these behavioral factors may synergistically impact health.13
Among CRC survivors, CVD is a leading cause of death.14–16 Emerging evidence suggests that CRC survivors may be more likely to develop diabetes in the five years following their cancer diagnosis.17 However, there is a paucity of research about control of CVD-related chronic conditions among CRC survivors. Understanding the control of CVD-related chronic conditions following CRC diagnosis is critical to ensure survivors’ optimal health.
The VA is a national, high-volume provider of CRC care, and the prevalence of CVD is high among veterans.3 Thus, we compared VA nonmetastatic CRC survivors and matched noncancer controls to accomplish two objectives: (1) determine the odds of nonmetastatic CRC survivors being diagnosed with CVD-related chronic conditions (eg, hypertension, diabetes, hyperlipidemia) and (2) determine their likelihood of CVD-related chronic condition control, each over 12 months following CRC diagnosis or identification.
Patients and methods
This is a retrospective, matched case–control cohort study that was approved by Durham VA Health Care System Institutional Review Board (IRB). The study data contained personally identifiable health information. The IRB granted a waiver of informed consent and HIPAA authorization. The waiver was granted because these analyses used existing, retrospective data originating from the electronic health record and it would not be feasible to recontact every patient, many of whom were deceased.
Nonmetastatic CRC survivor case eligibility criteria
Nonmetastatic CRC survivors were identified from the VA Central Cancer Registry (VACCR), a database capturing information on cancer cases diagnosed and/or treated at any VA facility nationwide.3,18 We identified patients diagnosed with CRC at any VA hospital nationwide from fiscal years 2009 to 2012 (ie, October 1, 2008, through September 30, 2012). To be eligible, CRC survivors must have been newly diagnosed with invasive, stages I, II, or III) at a VA facility during the study time frame and have had at least one primary care or oncology visit in the year prior to their CRC diagnosis. Nonmetastatic CRC survivors were excluded if we were unable to link their VACCR record with VA administrative data sources, had insufficient data to construct covariates, or were not matched with a noncancer control patient (Figure 1).
 |
Figure 1 Patient flow diagram. |
Noncancer control eligibility criteria
Potential noncancer control patients were identified through VA electronic health record (EHR) data via the VA Informatics and Computing Infrastructure.19 To match nonmetastatic CRC survivors and noncancer control patients, we used sequential stratification exact matching.20,21 This technique allowed for multiple anchor dates and time-varying characteristics, for example, longitudinal variation in body mass index (BMI). These time-varying characteristics may affect patterns of health care utilization and diagnoses with CVD-related chronic conditions (eg, more frequent interaction with health care system leads to more opportunities to be diagnosed), so properly accounting for them via a longitudinal matching process that allowed for these characteristics changing over time was critical. In order to be eligible to match to a nonmetastatic CRC survivor, potential noncancer controls could have no history of any cancer from five years prior until that CRC survivor’s diagnosis date and must have had one or more primary care visits in the previous six months. We chose five years as a threshold because evidence suggests that a pattern of stability emerges by that time.22
Case–control matching process
Nonmetastatic CRC survivors and noncancer control patients were first exact matched on the following characteristics: sex; race (white, non-white); age (within 5 years of the age of the matched case at time of diagnosis), copayment status (no copayment because of disability, no copayment because of low-income, must pay); Veterans Integrated Service Network geographic area; distance to VA healthcare; and health care use (high users [≥3 outpatient visits in the 14 months to 2 months prior to their CRC diagnosis], low users [<3 outpatient visits in the same period]). We used the period from 14 months to 2 months prior to their CRC diagnosis to avoid measuring a temporary increase in health services use related to obtaining a CRC diagnosis. CRC cases and noncancer control patients were matched on three BMI categories (underweight or healthy [BMI<24.9], overweight [25≤BMI≤29.9]), and obesity [BMI≥30.0] using the closest BMI to the case’s diagnosis date between 2 and 14 months prior to diagnosis (1 year for controls). Because CRC patients may experience weight changes around the time of diagnosis that might influence BMI, we excluded measurements within the 2 months prior to diagnosis. Additionally, CRC survivors and noncancer control patients were matched on the presence of CVD-related chronic conditions (hypertension, hyperlipidemia, diabetes diagnoses) between 2 and 26 months prior to the CRC survivor’s diagnosis date (2 years for controls).
After exact matching on the above characteristics, matching was further refined by selecting control patients closest to each CRC survivor based on minimizing the Mahalanobis distance function23 including the continuous variables of age and distance to VA health care. Based on the smallest variance that enabled the balance of covariates while minimizing the loss of potential controls, up to three matches were selected for each CRC survivor. An anchor date was established for all patients. For CRC cases, the date of CRC diagnosis was the anchor date. For matched, noncancer controls, the anchor date was the closest primary care visit date that occurred prior to and within six months of the corresponding CRC case’s diagnosis date.
Outcome measures
The three primary outcomes of interest were dichotomous measures of diagnosis of hypertension, diabetes, and/or hyperlipidemia in the first year following CRC diagnosis (or anchor date for matched noncancer controls). The three secondary outcomes of interest were time-varying binary indicators from CVD-related chronic disease control based on clinical practice guidelines that covered the study period: blood pressure (for nondiabetic patients <150/90 mm Hg, for diabetic patients <140/90 mm Hg),24 diabetes (A1c <7% vs ≥7%),25 and hyperlipidemia [low-density lipoprotein (LDL) <100 mg/dL vs ≥100 mg/dL].26 Chronic disease control outcomes were collected from EHR data measured in outpatient clinics over the year following the anchor date; diabetes diagnosis in the pre-period was used to define the blood pressure threshold. If an individual had multiple measurements of an outcome per day, the average measurement for the day was used.
Statistical analysis
We used logistic regression to assess associations between CRC survivors’ and matched noncancer controls prevalence of hypertension, diabetes, and hyperlipidemia diagnoses. Odds of control of BP, A1c, and LDL were estimated using a generalized linear mixed model for each outcome, with an individual-level random intercept to account for correlation among multiple measures per person. The model included an indicator for whether a patient was a CRC survivor vs a matched noncancer control, continuous time from anchor date, and their interaction. Statistical analyses were conducted using SAS Enterprise Guide 7.1 and SAS 9.4 (SAS Institute Inc., Cary, NC) with a priori two-sided statistical significance level set at 0.05.
Additional analyses
We conducted a sensitivity analysis, using stratified age as an interaction term, examining whether the associations found varied by categorical age group. Given the differences in hypertension control, we conducted a post-hoc analysis to evaluate differences in polypharmacy and antihypertensive medication-taking behaviors. We report the overall number of oral cardiovascular medications patients were prescribed. To assess adherence to antihypertensive medications, we calculated Medication Possession Ratio (MPR), a pharmacy refill-based measure of medication adherence, for patients prescribed metoprolol tartrate in the outpatient setting in the year following the anchor date.27,28 Due to the MPR not being normally distributed, a difference in MPR between cases and controls was checked using the Wilcoxon Rank Sum test, a nonparametric test.
Results
Patient sample
We identified 15,218 CRC survivors who were diagnosed during the study period. After applying exclusion criteria (eg, stage IV, diagnosed outside of study time frame), 9,758 CRC survivors and 29,066 matched noncancer control patients were included in the analytic sample (Figure 1).
Patient characteristics
Baseline characteristics for CRC survivors and matched noncancer control patients, including presence of CVD risk factors, are presented in Table 1. Most cases were white (79.3%), males (97.7%). Patients were commonly married (48.9%), overweight (BMI 25.0–29.9; 29.7%), or obese (BMI ≥30; 32.5%). Most patients received VA health care without a copay (78.9%) because of either low annual income (44.3%) or military service-related disability (34.6%).
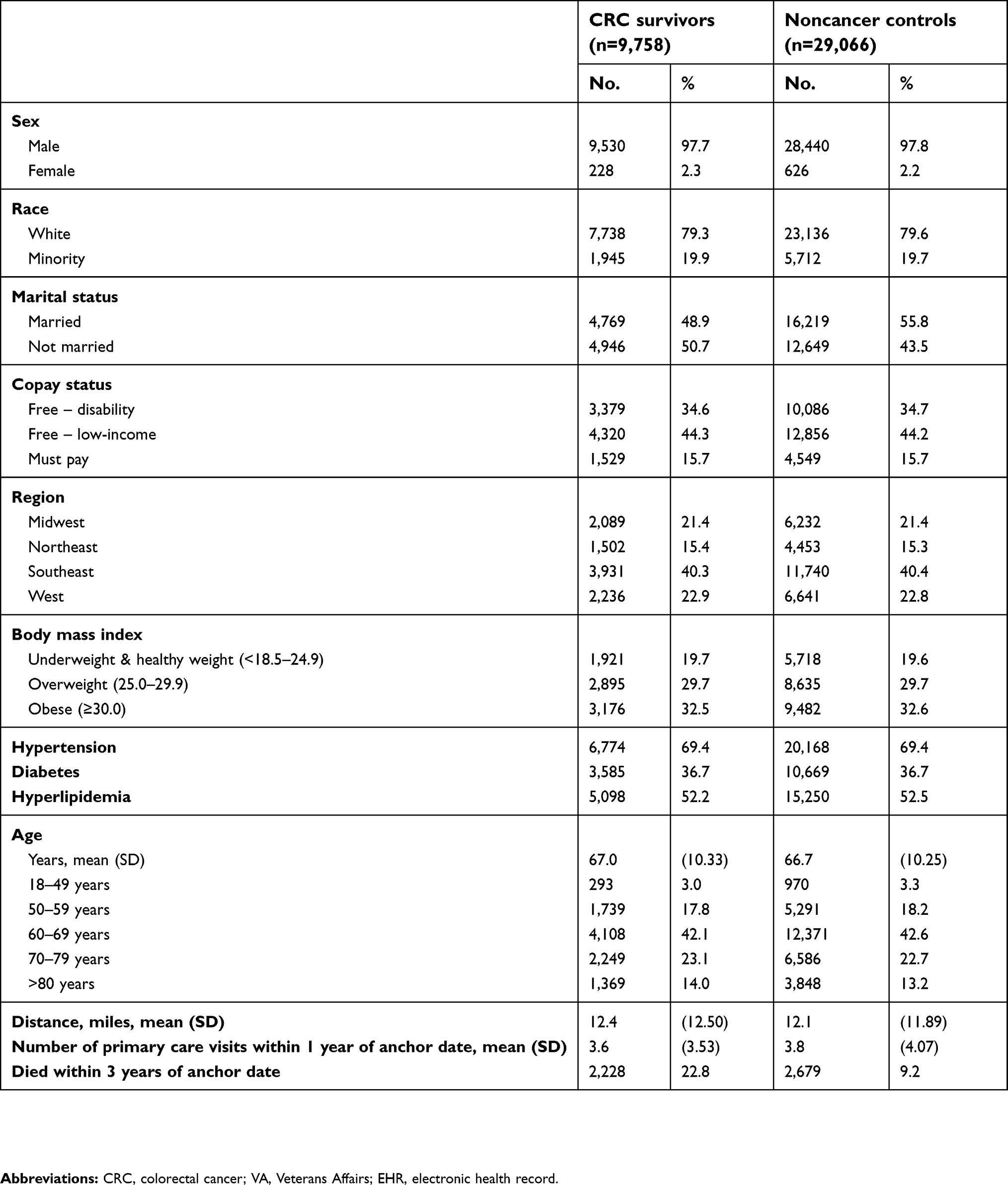 |
Table 1 Demographic characteristics of patient sample |
Among CRC cases, the mean age at diagnosis was 67.0 years. A larger proportion of CRC cases died within three years of the anchor date compared to the noncancer control patients (22.83 vs 9.22%, respectively).
Presence of CVD-related chronic conditions among CRC survivors
At baseline, 69.4% of CRC survivors were diagnosed with hypertension, 36.7% with diabetes, and 52.2% with hyperlipidemia. In the post-period, approximately 7% of cases and 11% of controls had newly diagnosed hypertension; 6% and 24% of cases and controls, respectively, had newly diagnosed hyperlipidemia; and 5% and 4% of cases and controls, respectively, had newly diagnosed diabetes. In the year following the anchor date, compared to matched noncancer control patients (Table 2), CRC survivors had 57% higher odds of being diagnosed with hypertension (OR=1.57, 95% CI=1.49–1.64). This includes all diagnoses of hypertension in the sample (ie, not limited to new diagnosis). Also, at 1 year post-anchor date, we identified no difference between CRC survivors and controls regarding diabetes diagnoses (OR=0.97, 95% CI=0.93–1.02). Compared to matched noncancer control patients, CRC survivors had half the odds of being diagnosed with hyperlipidemia (OR=0.50, 95% CI=0.48–0.52).
 |
Table 2 Model-estimated odds ratios of being diagnosed CVD risk factors post-CRC diagnosis (CRC survivors vs matched noncancer controls) |
CVD-related chronic condition control
Twelve months post-anchor date (Table 3), CRC cases experienced 7% higher odds of good blood pressure control (OR=1.07, 95% CI 1.02–1.13) and 12% lower odds of LDL control (OR=0.88, 95% CI 0.81–0.94) compared to matched noncancer controls. There was no significant difference between CRC cases and matched controls in odds of A1c control at 12 months.
 |
Table 3 Model-estimated odds ratios of CVD risk factor control 1-year post-CRC diagnosis |
Sensitivity analysis for age stratification
There was minor variation by age group, but the magnitude and direction of the associations were consistent (Table 4). We also report age-stratified analysis with regard to CVD risk factor control (Table 5).
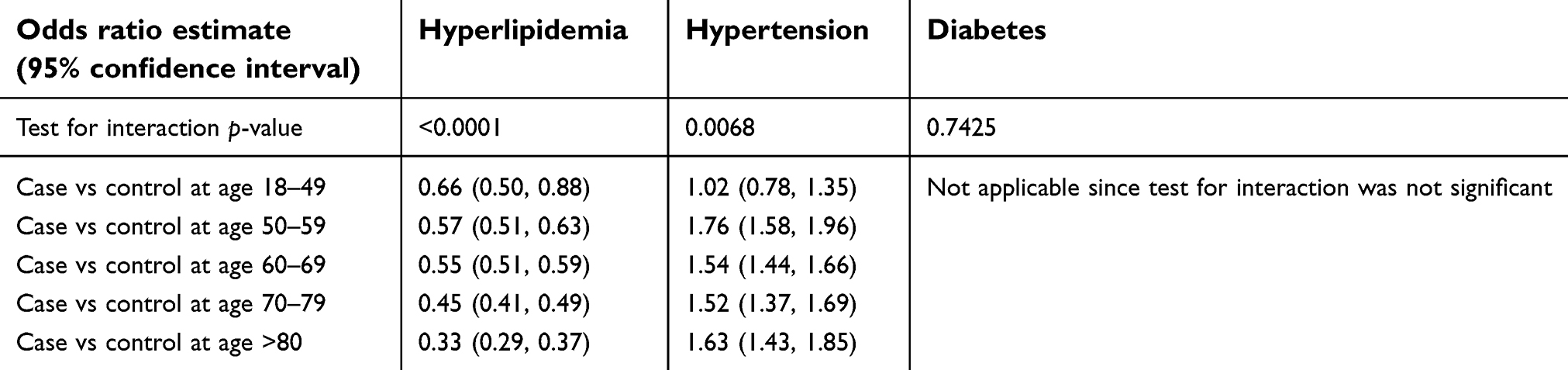 |
Table 4 Age-stratified analysis of being diagnosed CVD risk factors post-CRC diagnosis (CRC survivors vs matched noncancer controls) |
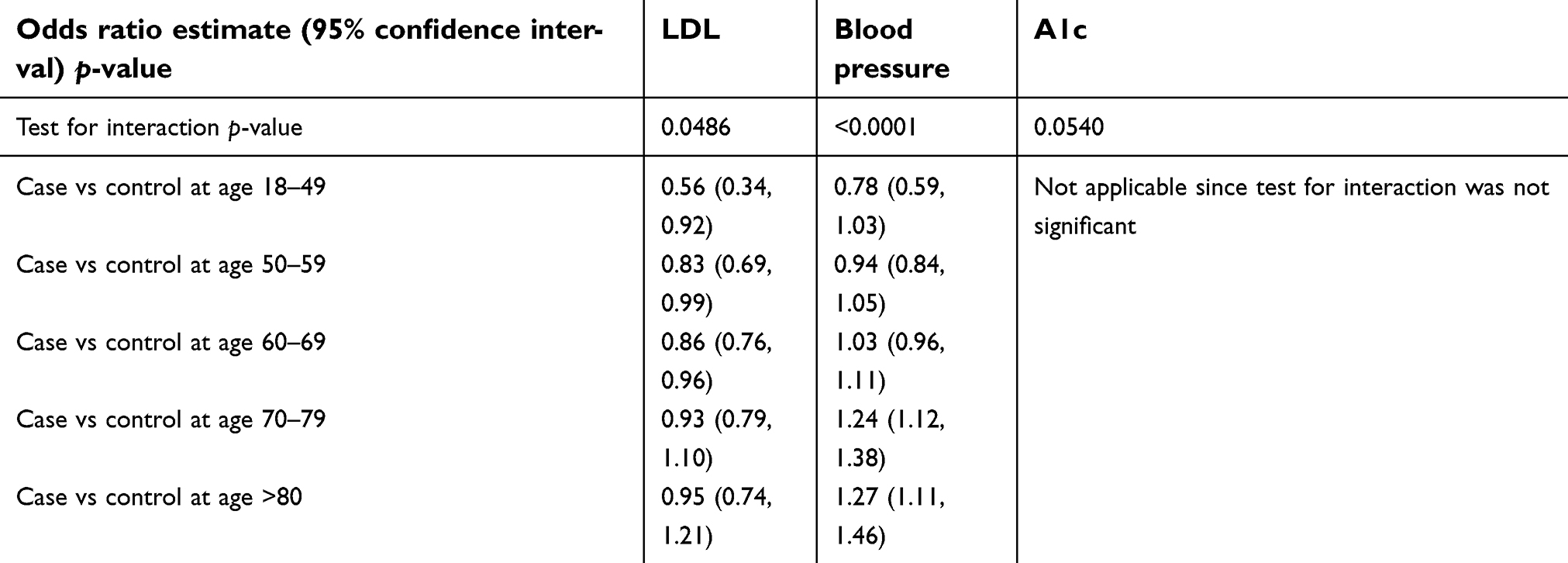 |
Table 5 Age-stratified analysis of CVD risk factor control 1-year post-CRC diagnosis |
Polypharmacy and differences in medication adherence
Regarding polypharmacy, CRC survivors and matched noncancer controls were prescribed similar numbers of overall oral medications (CRC cases, mean =4.21, SD 3.70; matched noncancer controls, mean 4.13, SD 3.67). Based on pharmacy refill data, adherence was significantly lower among CRC survivors compared with matched noncancer controls (mean MPR 85% and 93%, respectively, p<0.001).
Discussion
Our analysis suggests that, compared to matched peers, nonmetastatic CRC survivors may be more likely to be diagnosed with hypertension. While the magnitude of the effect appears relatively small, we assert that this is still an important difference when considered from a population health perspective. It is also worth noting that nonmetastatic CRC survivors and controls had very similar rates of primary care visits in the three years post-anchor date and, as a result, similar opportunities to receive a hypertension diagnosis. Specifically, CRC survivors had a mean of approximately 9 primary care visits over the three years post-anchor date (SD 8) and controls had a mean of 8 primary care visits (SD 7). CRC and hypertension share common risk factors (eg, sedentary behavior, poor quality diet, noncompliance with healthy behaviors).29,30 Prolonged sedentary time is associated with increased risk of developing both CRC30 and hypertension, as well as poor blood pressure control.31–33 Among CRC survivors, sedentary time is associated with decreased health-related quality of life34 and higher CRC-specific mortality.35 Although the relationship between risk factors is similar for hyperlipidemia, we saw the opposite association with the likelihood of being diagnosed with hyperlipidemia and/or cholesterol control. While beyond the scope of this project, it is possible that patients who do not follow CRC screening guidelines may have both a higher risk of CRC and be less likely to be compliant with other health behaviors, like blood pressure management. Hyperlipidemia among CRC survivors merits additional study.
Of note, hypertension is a transient side effect of certain chemotherapy regimens, such as bevacizumab for the treatment of metastatic CRC. While our sample includes patients with nonmetastatic disease, we were concerned that some patients might have been prescribed bevacizumab for disease progression. We reviewed VA administrative health data and found that only 7 CRC cases and 11 controls were exposed to bevacizumab during their first year post-anchor date. These small numbers suggest that bevacizumab exposure is not a driver of our results.
In contrast to a prior analysis,17 we did not find more diabetes diagnoses among CRC survivors in the year following their CRC diagnosis. This may be because the VA patient population, irrespective of cancer status, has a higher prevalence of diabetes (16%) compared to the US (7.2%).36,37 The VA has a strong history of diabetes risk reduction research38–40 and has nationally disseminated two programs targeting diabetes. These programs include the Veterans Affairs Diabetes Prevention Program (VA-DPP) and MOVE! weight management program.41,42 We did not have data about whether people in our cohort participated in these programs.
The association between nonmetastatic CRC and CVD risk-related chronic conditions, such as hypertension, is complex. CRC and CVD share common behavioral risk factors including obesity, physical inactivity, diet, and other lifestyle behaviors.9–12 In Australia, Hawkes and colleagues conducted a telephone-based behavioral change intervention targeting improved dietary habits, increased physical activity, smoking cessation, and alcohol moderation among CRC survivors.43 The intervention improved CRC survivors’ physical activity, dietary habits, and BMI, as well as their psychosocial outcomes.43,44 While this is a promising beginning, there is a need for additional interventions of this type, particularly those targeting hypertension management among CRC survivors. In addition to addressing traditional healthy lifestyle behaviors, future self-management interventions should address medication adherence.
Medication therapy is often necessary to achieve therapeutic goals for CVD-related chronic conditions and maximum clinical effectiveness.45 Medication nonadherence for chronic disease medications among people with cancer has been documented potentially harming their cardiovascular health.46,47 Therefore, we examined adherence to antihypertensive medications. In our study, we found that CRC survivors had lower adherence to a commonly prescribed antihypertensive medication compared to controls. Because we observed poorly managed hypertension and suboptimal medication adherence among CRC survivors, improving medication adherence may be an area for future interventional work in this population.
Our analysis had several limitations. We studied users of the VA health care system who are, on average, older, sicker, and engage in different health behaviors than the general US population.37,48 This may impact the generalizability of study findings including generalizing to metastatic CRC, other cancers, or patient populations with a higher proportion of women. Additionally, we did not have data on lifestyle behaviors (eg, diet and physical activity) that might impact CRC and CVD-related chronic conditions. Instead, we relied on BMI prior to diagnosis as a proxy measure. Because we relied on BMI measured in the last six months, we could have missed the inclusion of healthier controls who had no visits and therefore no recent BMI measurements. We also did not have access to information about patients’ diet quality, tobacco, alcohol use, or cancer-related therapies that they received. We considered outcomes within the first year after CRC diagnosis. It is probable that there will be variation at different points in the survivorship trajectory. Despite these limitations, our analysis also had several advantages. We used a national cohort with a large sample size. Additionally, we exactly matched on a myriad of variables that might not be possible in other large administrative datasets (eg, distance from care).
Conclusions
We identified no difference in the presence of diabetes or diabetes control between CRC cases and matched controls in the year following CRC diagnosis. During the same time period, we found that hyperlipidemia was better controlled among CRC survivors. This may merit additional study. However, we found that CRC survivors may be more likely to have hypertension and may be more likely to struggle with blood pressure control in the years following their CRC diagnosis.
There may be a need to address care for hypertension, a CVD-related chronic condition, among CRC survivors, and to understand the impact of CRC treatment on development and management of hypertension. Future studies should evaluate adherence to antihypertensives medications and how the management of hypertension among CRC survivors is relative to their peers. There may be a need for blood pressure control interventions targeted toward cancer survivors.
Acknowledgments
We thank the Veterans Affairs cancer registrars and VA Central Cancer Registry staff for their data collection and related efforts. This study is supported by a VA Health Services Research and Development (HSR&D) Career Development Award (CDA 13-025) awarded to Dr Leah L Zullig. This study is also supported by a Veterans Affairs Health Services Research and Development Senior Career Scientist Award (HSRD 08-027) awarded to Dr Hayden B Bosworth. This work was supported by the Center of Innovation for Health Services Research in Primary Care (CIN 13-410) at the Durham VA Health Care System. This work was previously presented at the American Society of Medical Oncology (ASCO) Cancer Survivorship Symposium in March 2018; the abstract was published in a supplemental issue of the Journal of Clinical Oncology.
Disclosure
Dr Leah L Zullig reports grants from Department of Veterans Affairs, during the conduct of the study. Dr George L Jackson reports grants from Department of Veterans Affairs, during the conduct of the study and grants from Bristol-Myers Squibb Foundation, outside of the submitted work. Dr Hayden B Bosworth reports grants from Johnson & Johnson, Improve Patient Outcomes, Cover MyMeds, and Omnicell. He also received grants and personal fees from Otsuka and Sanofi, outside of the submitted work. The authors report no other conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67(3):177–193.
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. doi:10.3322/caac.21387
3. Zullig LL, Jackson GL, Dorn RA, et al. Cancer incidence among patients of the U.S. veterans affairs health care system. Mil Med. 2012;177(6):693–701. doi:10.7205/milmed-d-11-00434
4. Zullig LL, Smith VA, Jackson GL, et al. Colorectal cancer statistics from the veterans affairs central cancer registry. Clin Colorectal Cancer. 2016. doi:10.1016/j.clcc.2016.04.005
5. Byers T, Wender RC, Jemal A, Baskies AM, Ward EE, Brawley OW. The American Cancer Society challenge goal to reduce US cancer mortality by 50% between 1990 and 2015: results and reflections. CA Cancer J Clin. 2016;66(5):359–369. doi:10.3322/caac.21348
6. Howlader N, Ries LA, Mariotto AB, Reichman ME, Ruhl J, Cronin KA. Improved estimates of cancer-specific survival rates from population-based data. J Natl Cancer Inst. 2010;102(20):1584–1598. doi:10.1093/jnci/djq366
7. Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66(4):271–289. doi:10.3322/caac.21349
8. Kenzik KM, Kent EE, Martin MY, Bhatia S, Pisu M. Chronic condition clusters and functional impairment in older cancer survivors: a population-based study. J Cancer Surviv. 2016. doi:10.1007/s11764-016-0553-4
9. Giovannucci E, Ascherio A, Rimm EB, Colditz GA, Stampfer MJ, Willett WC. Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med. 1995;122(5):327–334.
10. Giovannucci E, Rimm EB, Stampfer MJ, et al. A prospective study of cigarette smoking and risk of colorectal adenoma and colorectal cancer in U.S. men. J Natl Cancer Inst. 1994;86(3):183–191.
11. Potter J, Brown L, Williams RL, Byles J, Collins CE. Diet quality and cancer outcomes in adults: a systematic review of epidemiological studies. Int J Mol Sci. 2016;17(7). doi:10.3390/ijms17071052
12. Potter JD. Nutrition and colorectal cancer. Cancer Causes & Control. 1996;7(1):127–146.
13. Aleksandrova K, Pischon T, Jenab M, et al. Combined impact of healthy lifestyle factors on colorectal cancer: a large European cohort study. BMC Med. 2014;12:168. doi:10.1186/s12916-014-0141-2
14. Armenian SH, Xu L, Ky B, et al. Cardiovascular disease among survivors of adult-onset cancer: a community-based retrospective cohort study. J Clin Oncol. 2016;34(10):1122–1130. doi:10.1200/JCO.2015.64.0409
15. van Erning FN, van Steenbergen LN, Lemmens VE, et al. Conditional survival for long-term colorectal cancer survivors in the Netherlands: who do best? Eur J Cancer (Oxford, England: 1990). 2014;50(10):1731–1739. doi:10.1016/j.ejca.2014.04.009
16. Weaver KE, Foraker RE, Alfano CM, et al. Cardiovascular risk factors among long-term survivors of breast, prostate, colorectal, and gynecologic cancers: a gap in survivorship care? J Cancer Surviv. 2013;7(2):253–261. doi:10.1007/s11764-013-0267-9
17. Singh S, Earle CC, Bae SJ, et al. Incidence of diabetes in colorectal cancer survivors. J Natl Cancer Inst. 2016;108(6):djv402. doi:10.1093/jnci/djv402
18. Zullig LL, Sims KJ, McNeil R, et al. Cancer incidence among patients of the U.S. veterans affairs health care system: 2010 update. Mil Med. 2017;182(7):e1883–e1891. doi:10.7205/MILMED-D-16-00371
19. VA informatics and computing infrastructure (VINCI), VA HSR HIR 08-204, U.S. Department of Veterans Affairs; 2008. Available from: https://vawww.VINCI.med.va.gov Accessed November 12, 2018.
20. Kennedy EH, Taylor JM, Schaubel DE, Williams S. The effect of salvage therapy on survival in a longitudinal study with treatment by indication. Stat Med. 2010;29(25):2569–2580. doi:10.1002/sim.4017
21. Schaubel DE, Wolfe RA, Port FK. A sequential stratification method for estimating the effect of a time‐dependent experimental treatment in observational studies. Biometrics. 2006;62(3):910–917. doi:10.1111/j.1541-0420.2006.00527.x
22. Andersen BL, Goyal NG, Westbrook TD, Bishop B, Carson WE
23. Rosenbaum PR, Rubin DBJTAS. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am Stat. 1985;39(1):33–38.
24. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth Joint National Committee (JNC 8). Jama. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
25. Association AD. 6. Glycemic targets. Diabetes Care. 2015;38(Supplement 1):S33–S40. doi:10.2337/dc15-S009
26. Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Circulation. 2014;129:S1–S45. doi:10.1161/01.cir.0000437738.63853.7a
27. Steiner JF, Koepsell TD, Fihn SD, Inui TS. A general method of compliance assessment using centralized pharmacy records. Description and validation. Med Care. 1988;26(8):814–823.
28. Steiner JF, Prochazka AV. The assessment of refill compliance using pharmacy records: methods, validity, and applications. J Clin Epidemiol. 1997;50(1):105–116.
29. Hang J, Cai B, Xue P, et al. The joint effects of lifestyle factors and comorbidities on the risk of colorectal cancer: a large chinese retrospective case-control study. PLoS One. 2015;10(12):e0143696. doi:10.1371/journal.pone.0143696
30. Ma P, Yao Y, Sun W, Dai S, Zhou C. Daily sedentary time and its association with risk for colorectal cancer in adults: A dose-response meta-analysis of prospective cohort studies. Medicine. 2017;96(22):e7049. doi:10.1097/MD.0000000000007049
31. Beunza JJ, Martinez-Gonzalez MA, Ebrahim S, et al. Sedentary behaviors and the risk of incident hypertension: the SUN cohort. Am J Hypertens. 2007;20(11):1156–1162. doi:10.1016/j.amjhyper.2007.06.007
32. Martinez-Gomez D, Tucker J, Heelan KA, Welk GJ, Eisenmann JC. Associations between sedentary behavior and blood pressure in young children. Arch Pediatr Adolesc Med. 2009;163(8):724–730. doi:10.1001/archpediatrics.2009.90
33. Whitaker KM, Buman MP, Odegaard AO, et al. Sedentary behaviors and cardiometabolic risk, an isotemporal substitution analysis. Am J Epidemiol. 2018;187(2):181–189.
34. van Roekel EH, Winkler EA, Bours MJ, et al. Associations of sedentary time and patterns of sedentary time accumulation with health-related quality of life in colorectal cancer survivors. Prev Med Rep. 2016;4:262–269. doi:10.1016/j.pmedr.2016.06.022
35. Cao Y, Meyerhardt JA, Chan AT, Wu K, Fuchs CS, Giovannucci EL. Television watching and colorectal cancer survival in men. Cancer Causes & Control. 2015;26(10):1467–1476. doi:10.1007/s10552-015-0645-x
36. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. Jama. 2001;286(10):1195–1200.
37. Reiber GE, Koepsell TD, Maynard C, Haas LB, Boyko EJ. Diabetes in nonveterans, veterans, and veterans receiving department of veterans affairs health care. Diabetes Care. 2004;27(Suppl 2):B3–B9. doi:10.2337/diacare.27.suppl_2.b3
38. Crowley MJ, Edelman D, McAndrew AT, et al. Practical telemedicine for veterans with persistently poor diabetes control: a randomized pilot trial. Telemedicine J E-Health. 2016;22(5):376–384. doi:10.1089/tmj.2015.0145
39. Edelman D, Fredrickson SK, Melnyk SD, et al. Medical clinics versus usual care for patients with both diabetes and hypertension: a randomized trial. Ann Intern Med. 2010;152(11):689–696. doi:10.7326/0003-4819-152-11-201006010-00001
40. Jackson GL, Yano EM, Edelman D, et al. Veterans affairs primary care organizational characteristics associated with better diabetes control. Am J Manag Care. 2005;11(4):225–237.
41. Damschroder LJ, Moin T, Datta SK, et al. Implementation and evaluation of the VA DPP clinical demonstration: protocol for a multi-site non-randomized hybrid effectiveness-implementation type III trial. Implementation Science. 2015;10:68. doi:10.1186/s13012-015-0250-0
42. Moin T, Damschroder LJ, AuYoung M, et al. Diabetes prevention program translation in the veterans health administration. Am J Prev Med. 2017;53(1):70–77. doi:10.1016/j.amepre.2016.11.009
43. Hawkes AL, Chambers SK, Pakenham KI, et al. Effects of a telephone-delivered multiple health behavior change intervention (CanChange) on health and behavioral outcomes in survivors of colorectal cancer: a randomized controlled trial. J Clin Oncol. 2013;31(18):2313–2321. doi:10.1200/JCO.2012.45.5873
44. Hawkes AL, Pakenham KI, Chambers SK, Patrao TA, Courneya KS. Effects of a multiple health behavior change intervention for colorectal cancer survivors on psychosocial outcomes and quality of life: a randomized controlled trial. Ann Behav Med. 2014;48(3):359–370. doi:10.1007/s12160-014-9610-2
45. Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119(23):3028–3035. doi:10.1161/CIRCULATIONAHA.108.768986
46. Santorelli ML, Steinberg MB, Hirshfield KM, et al. Effects of breast cancer on chronic disease medication adherence among older women. Pharmacoepidemiol Drug Saf. 2016;25(8):898–907. doi:10.1002/pds.3971
47. Tan X, Feng X, Chang J, Higa G, Wang L, Leslie D. Oral antidiabetic drug use and associated health outcomes in cancer patients. J Clin Pharm Ther. 2016;41(5):524–531. doi:10.1111/jcpt.12430
48. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at veterans affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21):3252–3257.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.