Back to Journals » Journal of Asthma and Allergy » Volume 19
Cardiorespiratory and Glycaemic Changes Following Prehospital Nebulised Salbutamol in Acute Asthma: A Mixed Retrospective and Prospective Observational Study
Authors Mortimer C ![]() , Nikoletou D, Ooms A, Williams J
, Nikoletou D, Ooms A, Williams J
Received 3 March 2026
Accepted for publication 14 May 2026
Published 3 June 2026 Volume 2026:19 605135
DOI https://doi.org/10.2147/JAA.S605135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Craig Mortimer,1,2 Dimitra Nikoletou,3 Ann Ooms,2 Julia Williams1
1Research and Development Department, South East Coast Ambulance Service NHS Foundation Trust, Crawley, UK; 2Faculty of Health, Science, Social Care and Education, Kingston University London, London, UK; 3School of Health and Medical Sciences (SHMS), City St George’s, University of London, London, UK
Correspondence: Craig Mortimer, Research and Development Department, South East Coast Ambulance Service NHS Foundation Trust, Crawley, UK, Tel +44 7733302897, Email [email protected]
Purpose: In 2010, the Global Strategy for Asthma Management and Prevention recommended reducing the reliance on treating acute asthma exacerbations with short-acting β2 agonists (SABAs) given potential adverse effects. However, more than a decade later, SABAs, particularly nebulised salbutamol, remain at the forefront of acute asthma care. This study examined the physiological effects of nebulised salbutamol in patients experiencing moderate to severe asthma exacerbations.
Methods: A six month, prospective and retrospective observational study was undertaken involving prehospital asthma patients treated with nebulised salbutamol. Data were analysed using descriptive and inferential statistics, including paired comparisons and exploratory subgroup analyses, to identify relevant trends and variability.
Results: Among 176 eligible patients, reductions were observed in heart rate (mean − 3 beats/min) and respiratory rate (mean − 5 breaths/min), with modest improvement in peripheral oxygen saturation (+2%). Capillary blood glucose (CBG) analysis was conducted on a small prospective subgroup (n=8). A mean increase of +0.375 mmol/L was observed. When one clinically atypical outlier was excluded (n=7), the increase reached statistical significance. Albeit interpretation is limited by the small sample size.
Conclusion: Administration of ≥ 5mg nebulised salbutamol in acute asthma exacerbations was transiently associated with improved peripheral oxygen saturation and respiratory parameter changes during the prehospital treatment period. No clinically significant increase in heart rate was observed overall. A small rise in CBG was observed in a small prospectively monitored subgroup. However, the clinical significance of this finding remains uncertain. Larger, adequately powered prospective studies are required to confirm these findings. The present findings are insufficient to recommend changes to current glucose monitoring practices in non-diabetic patients.
Keywords: asthma, beta-agonist, hyperglycaemia, capillary blood glucose, emergency care
Introduction
Asthma remains a significant global public health concern, associated with substantial morbidity, mortality, and healthcare utilisation despite advances in pharmacological management. Acute exacerbations continue to account for considerable emergency healthcare attendance and ambulance service utilisation worldwide.1,2 Asthma is a complex, heterogeneous inflammatory disease shaped by diverse phenotypes, endotypes, disease mechanisms, and individual patient profiles.1–3 This heterogeneity influences disease presentation, progression, and response to treatment.4 Clinical outcomes may be influenced by variation in healthcare professional’s assessment, treatment approaches, and patient perception of symptoms.3,5,6
Understanding asthma pathophysiology, triggers, and patient specific factors can support tailored management strategies aimed at reducing exacerbations, morbidity, and mortality.7,8 However, acute exacerbations may still occur despite preventative strategies and can occasionally become life-threatening.9
β2 agonists remain a mainstay of acute asthma management because of their bronchodilator effects on smooth muscle.10,11 Nebulised salbutamol is widely used in prehospital and emergency care settings to relieve bronchospasm and improve airflow during acute exacerbations, although variability in individual clinical response is recognised.12 As a β2 adrenergic agonist, salbutamol may also exert systemic physiological effects, including transient changes in heart rate and glucose regulation through sympathomimetic stimulation and glycogenolysis.13,14 Consequently, cardiorespiratory observations such as respiratory rate (RR), heart rate (HR), and peripheral oxygen saturation (SpO2), alongside metabolic indicators including capillary blood glucose (CBG), may provide clinically relevant markers of treatment response and physiological effect. While systemic β2 agonists are associated with recognised metabolic effects, previous studies examining inhaled salbutamol at standard therapeutic doses have generally not demonstrated clinically significant hyperglycaemia. The metabolic effects observed with oral or intravenous administration appear less pronounced with inhaled therapy. Current asthma guidance has also moved away from SABA monotherapy, emphasising anti-inflammatory reliever strategies. Nevertheless, nebulised salbutamol remains widely used in prehospital asthma care, although physiological responses during acute exacerbations are not fully understood.
Intrinsic and extrinsic factors may further disrupt asthma exacerbation severity and treatment response.15,16 Respiratory infections, including influenza and pharyngitis, alongside chronic conditions such as diabetes and cardiovascular disease, may compound asthma severity and complicate acute management.17,18
This study aimed to characterise immediate physiological and metabolic responses following nebulised salbutamol in acute asthma within a real world prehospital setting.
Materials and Methods
Study Design
This pragmatic observational study incorporated both prospective and retrospective components to evaluate changes in CBG and cardiorespiratory parameters, including HR, RR, and SpO2 following nebulised salbutamol administration. This design allowed data collection during routine care without altering standard clinical practice, thus enhancing validity and minimising bias.19–22 Both pre and post treatment comparisons were undertaken within an acute emergency setting to assess physiological changes during routine care.22,23
The prospective component enabled collection of additional variables not routinely recorded, including paired CBG measurements. Inclusion and exclusion criteria, aligned with a preceding systematic review,2 ensured uniformity and consistency in data collection, and facilitated comparison across datasets.20,24
A schematic overview of the study design and data collection processes is presented in Figure 1.
 |
Figure 1 Schematic overview of study design and data collection processes. |
Study Setting
The study was conducted within a single NHS ambulance service Foundation Trust, serving multiple counties in the United Kingdom. Conducting the research within a single service enabled consistency in clinical protocols, care delivery, and data capture, thereby limiting confounding variability across sites.25
Paramedics followed Trust clinical guidelines for acute asthma management, typically including the administration of 5 mg nebulised salbutamol driven by oxygen, repeated at clinician discretion. Supplemental oxygen was titrated to maintain SpO2 ≥94% in most adults unless otherwise indicated. Corticosteroid administration was not routinely undertaken prehospital but was recorded where applicable. No additional standardisation of treatment was undertaken.
Sampling Strategy
A non-probability, purposive sampling strategy with criterion based selection was employed to ensure relevance to the study objectives.26 Recruitment reflected the operational realities of emergency ambulance services, including seasonal variation and healthcare system pressures. These factors affected patient availability and condition mix (eg, Chronic Obstructive Pulmonary Disease) during the study period.27–29
Sample Size Estimation
A priori power analysis using G*Power determined that a minimum of 107 participants were required to detect statistically significant effects (power: 80%, α: 0.05). This calculation assumed a moderate within subject effect size for paired physiological comparisons. Based on historical data,30 recruitment of this sample was deemed feasible over a six-month period, even when accounting for anticipated attrition due to exclusion criteria and operational variability. While 176 patients met inclusion criteria, complete paired physiological data were available for 100 participants, and paired CBG data for eight. Therefore, analyses involving these subsets should be interpreted cautiously relative to the original power calculation.
Data Collection and Recruitment
Phase 1: Prospective Data Collection
From 10th March to 9th September 2023, study-trained paramedics identified eligible asthma patients during routine emergency calls. Following patient stabilisation and confirmation of eligibility, informed electronic consent was obtained via a secure application on a work issued device prior to study-specific data collection. Paramedics were instructed to collect paired observations, including CBG, HR, RR, and SpO2, before and after nebulisation, along with additional study specific clinical details, including history of diabetes.
Pre-treatment physiological values were defined as the final complete set of observations recorded immediately prior to administration of the first nebulised salbutamol dose. Post-treatment values were defined as the first complete observation set recorded following completion of nebulised therapy during the prehospital encounter (typically within 20–30 minutes). Where multiple post-treatment readings were available, the earliest complete dataset following nebulisation was used for analysis.
Phase 2: Retrospective Data Collection
All patients treated with nebulised salbutamol during the same time period were identified via the Trust’s Business Intelligence Department. This approach increased sample size but relied on routine clinical documentation and was therefore more susceptible to missing or inconsistent data31 Anonymised data were filtered using the same inclusion criteria as the prospective phase, enabling comparison between routinely collected and prospectively gathered datasets within the same operational setting.32
Electronic Recruitment Strategy
A bespoke electronic enrolment and consent form was created to work with the electronic Patient Clinical Record (ePCR) system to support real time screening and data capture. This minimised duplication and aligned with routine clinical workflows.
Condensed Patient Information Sheets (PIS) were provided for patients without Email access. The recruitment process was ethically approved and compliant with NHS research governance requirements.33
Paramedic Training
Participating paramedics completed a 30-minute online training package covering study procedures, recruitment, and ethical considerations. The training was pilot tested and refined with input from the Trust’s Clinical Education Department.34 Ongoing support was provided throughout the recruitment period.35
Inclusion and Exclusion Criteria
Selection criteria are outlined in Table 1. Prospective recruitment excluded non-English speakers and individuals with significant communication barriers, where inclusion could risk compromising patient care or increase anxiety.36,37 While interpretation services were available, their use was judged impractical in time sensitive emergency settings.
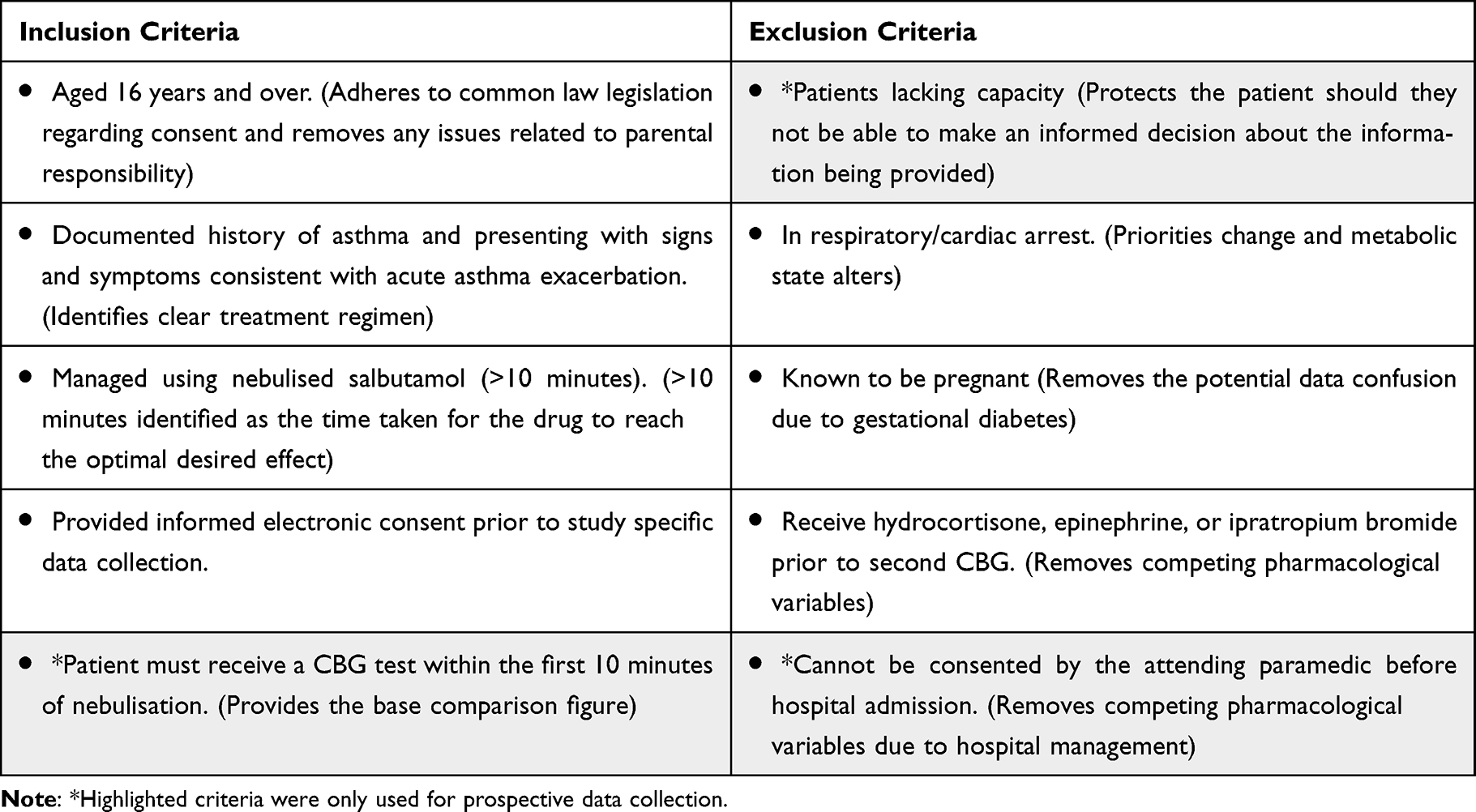 |
Table 1 Inclusion and Exclusion Criteria |
Data Management and Statistical Analysis
Data Handling
The CI manually entered data to ensure consistency in cleaning and verification.38 Missing data were common in the retrospective dataset, while no missing primary data were identified in the prospective phase.
Study Population
During the six-month study period, 2412 patients with documented asthma received nebulised salbutamol. From this population:
- Target Population (n=176): Patients meeting study inclusion criteria identified through anonymised retrospective record review. These data were extracted from routine clinical documentation and did not require individual patient consent under Health Research Authority approval.
- Per-Protocol Subset (n=100): Patients within the target population with complete paired pre and post treatment HR, RR and SpO2 data.
- Prospective CBG Subgroup (n=8): A subset of patients meeting the same inclusion criteria who were recruited prospectively and provided informed electronic consent for additional structured data collection, including paired pre and post nebulisation CBG measurements.
All remaining asthma patients treated during the same period formed a contextual retrospective cohort to assess representativeness.
Statistical Analysis
Data were analysed using SPSS and G*Power. Cardiorespiratory parameters (HR, RR, and SpO2) were considered the primary observational outcomes, while paired CBG analysis was considered exploratory given anticipated limitations in prospective recruitment and paired glucose data availability.39,40 Percentages were used to improve interpretability.41,42
Paired t-tests were used to assess within-subject differences in physiological variables before and after salbutamol administration. Normality was assessed visually because of the small subgroup sizes. Given the limited sample sizes, inferential findings should be viewed as exploratory.43 The absence of a control group restricted causal inference. However, pre and post treatment comparisons provided insight into transient associations.44,45
Given the small size of the prospective CBG subgroup (n=8), assumptions of normality and robustness of parametric testing may not be fully satisfied. Inferential statistics in this subgroup were therefore interpreted with caution and considered exploratory. No formal correlation coefficients were calculated and observed relationships between physiological variables are described descriptively rather than as statistically confirmed correlations.
Ethical and Regulatory Considerations
The study and all components therein were conducted in accordance with the principles of the Declaration of Helsinki, Good Clinical Practice guidelines and applicable governmental regulatory standards as stated below.
This article uses the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidance.46 The study was approved by the Health Research Authority (IRAS 32068) with ethics approval from the East of England - Cambridgeshire and Hertfordshire Research Ethics Committee (REC 22/EE/0267). Further ethical approval (KU3202) was obtained from Kingston University, London. Local research governance and Capacity and Capability (C&C) approval was gained from the participating NHS Trust. In the prospective component, participants provided informed electronic consent prior to additional study-specific data collection. Retrospective anonymised data were extracted under Health Research Authority approval and did not require individual patient consent.
Although individuals aged 16–17 years were eligible for recruitment within the prospective cohort, no participants under 18 years were enrolled. Any data relating to individuals under 18 years occurred only from retrospectively collected datasets that were fully anonymised prior to analysis, therefore individual consent was not required in accordance with applicable ethical guidelines.
Results
Retrospective Data Analysis
The retrospective review of ambulance clinical records over a six-month period showed that nebulised salbutamol was administered across a range of presenting conditions beyond asthma alone. During this period 7426 patients received nebulised salbutamol, of which 2412 (32.5%) had a documented history of asthma. The top ten presenting conditions for patients receiving nebulised treatment, including those with and without a history of asthma, are detailed in Table 2. Although some patients may report asthma without a definitive diagnosis, the study relies on documented clinical records as an accurate representation of patient status, consistent with existing literature and the treatments administered.
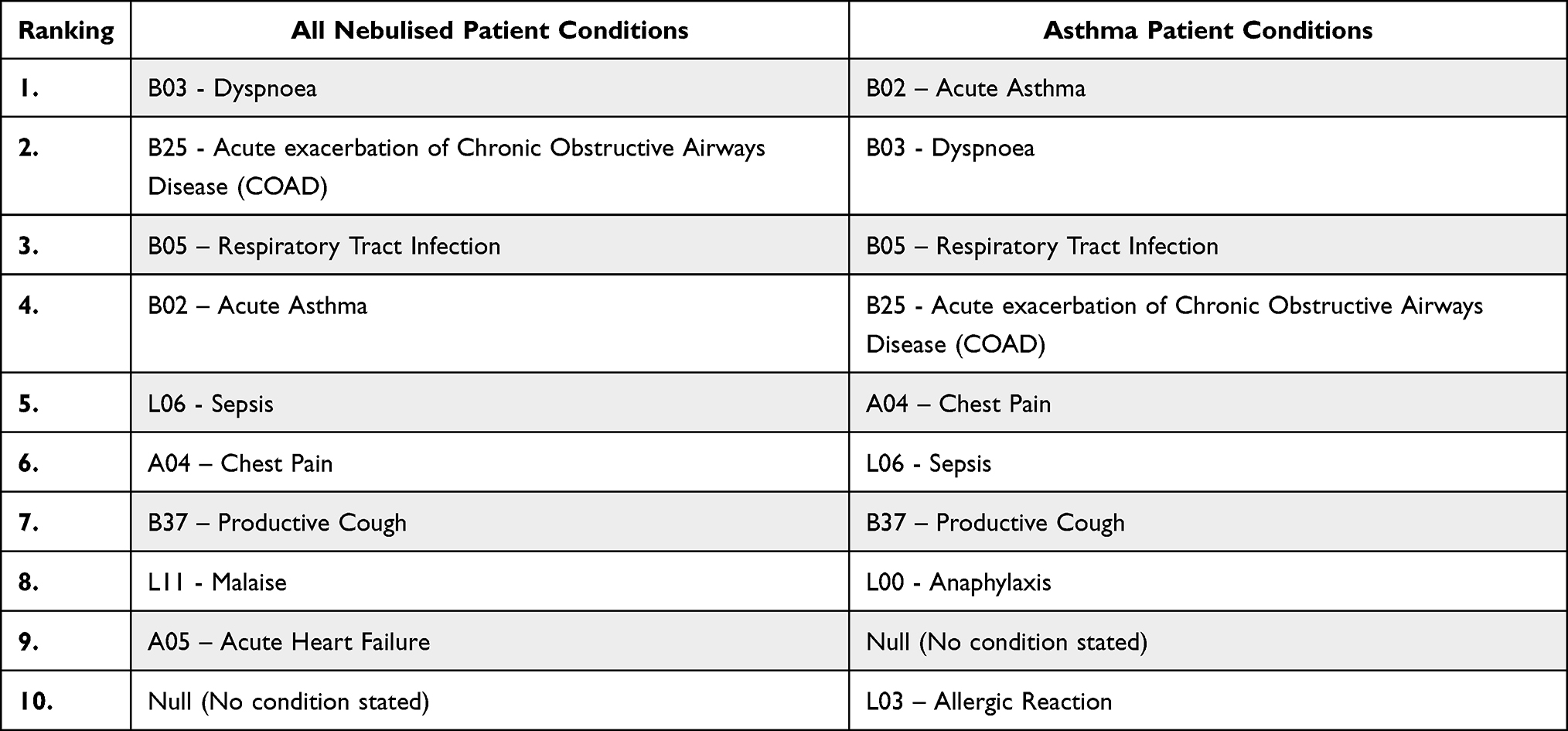 |
Table 2 Top ten Presenting Conditions for Nebulised Patients, With and Without a Documented History of Asthma |
Due to limitations in condition coding within the ePCR system, asthma was not consistently recorded as the primary diagnosis in all cases where nebulised salbutamol was administered. In some instances, asthma may have been recorded as a secondary or associated condition. Additionally, generic symptom coding, such as “sepsis”, may mask underlying respiratory complications requiring bronchodilation, thereby complicating data interpretation.
Demographic data for both the “Asthma Population” and the broader “Target Population” were analysed to establish representativeness and relevance. Although the primary research focus is not demographic based, this contextual information supports the contextual relevance of the findings within the study setting. Demographic data for both the asthma population and the target population are presented in Table 3 to provide context for the study example.
 |
Table 3 Demographic Characteristics of Study Populations (Age, Gender, Ethnicity) |
Call volumes remained relatively stable across the six-month period, averaging 29 patients per month.
Analysis of pharmacological treatment revealed that a cumulative dose of 5 mg of nebulised salbutamol was most common, administered to nearly 90% of patients, while higher doses (10 mg and 15 mg) were less frequent, reflecting standard dosing practices and clinical judgment.
Detailed patient observations conducted by paramedics provide insight into physiological changes following nebulised salbutamol administration. Out of 176 patients, 141 had at least two sets of clinical observations recorded, allowing for evaluation of changes over time. Distribution figures are presented to illustrate variability and directionality of individual patient changes beyond summary statistics. The interval between initial and final observations averaged just under 23 minutes, providing an appropriate window to observe acute physiological responses.
Baseline HR values ranged from 50–148 beats/min and showed a modest overall reduction following treatment (Figure 2). Among patients with paired HR measurements (n=112), 32.1% showed an increase, 4.5% remained unchanged, and 63.4% showed a decrease. The mean heart rate decreased from 101 to 98 beats/min, with a mean change of −3 beats/min, median of −4 beats/min, and modal value of −2 beats/min.
 |
Figure 2 Distribution of heart rate changes (y-axis: frequency of patients; x-axis: change in beats/minute from pre to post nebulisation). |
Among patients with paired RR measurements (n=120), 76.7% showed a reduction, 19.2% remained unchanged, and 4.2% increased (Figure 3). Mean RR decreased from 25 to 20 breaths/min (mean change −5), with a median change of −4 and a modal value of 0.
 |
Figure 3 Distribution of respiratory rate changes pre and post treatment (y-axis: frequency of patients; x-axis: change in breaths/min from pre to post nebulisation). |
Peripheral oxygen saturation (SpO2) increased from a mean of 95% to 98% (Figure 4). Among patients with follow-up measurements, 60.4% showed an increase, 25.4% remained unchanged, and 14.2% showed a decrease. Changes ranged from −5% to +30%, with a mean increase of 2%.
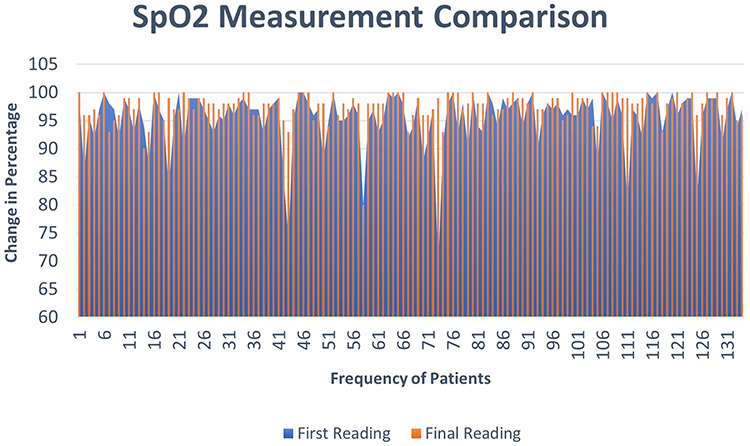 |
Figure 4 Distribution of oxygen saturation changes pre and post treatment (y-axis: frequency of patients; x-axis: change in percentage from pre to post nebulisation). |
CBG measurements were recorded in 81 patients with values ranging from 4.1 to 26 mmol/L (Figure 5). Most pre-treatment values were below 7.8 mmol/L, with a smaller proportion ≥7.8 mmol/L and ≥11.1 mmol/L. Post treatment values showed a similar distribution. Only a small number of paired CBG measurements were available.
 |
Figure 5 Distribution of capillary blood glucose values recorded during the study period where paired data were unavailable, post-nebulisation values are shown in Group 1 and pre-nebulisation values in Group 2 (y-axis: frequency of patients; x-axis: capillary blood glucose (mmol/L)). |
Peak Expiratory Flow Rate (PEFR) data were insufficient for meaningful analysis, with only four patients measured and no follow-ups recorded.
Within the subset of 100 patients with complete paired data, decreases in HR and RR were observed in 65.0% and 74.0% of patients, respectively, with concurrent decreases in both parameters in 48.0%. SpO2 increased in 59.0% of patients. Descriptive patterns of concurrent physiological changes are presented in Table 4.
 |
Table 4 Descriptive Patterns of Concurrent Changes in HR, RR, and SpO2 |
Among this subset, capillary blood glucose data after salbutamol administration revealed that 56.0% of patients had glucose levels below 7.8 mmol/L, generally accompanied by decreased HR and RR, and stable or increased SpO2. Elevated glucose levels (≥7.8 mmol/L) were recorded in 28.0% of patients, with some exceeding 11.1 mmol/L (Table 5). These elevated values occurred across varied clinical presentations.
 |
Table 5 Mean, Median, and Modal Changes in Physiological Parameters |
 |
Table 6 Prospective Data (Demographic and Vital Signs) |
Prospective Data Analysis
In the prospective subgroup (n=8), HR decreased in 62.5% of patients, RR decreased in 87.5%, and SpO2 increased in 75.0%. Mean changes were −0.38 beats/min (HR), −2.5 breaths/min (RR), and +3.8% (SpO2). Physiological changes post salbutamol (SLB) administration are presented in Table 6.
In the prospective subgroup, CBG increased in most patients, with a mean change of +0.375 mmol/L. A sensitivity analysis excluding one clinically atypical outlier case demonstrated statistical significance (Table 7). However, given the small subgroup size, these findings should be viewed as exploratory.
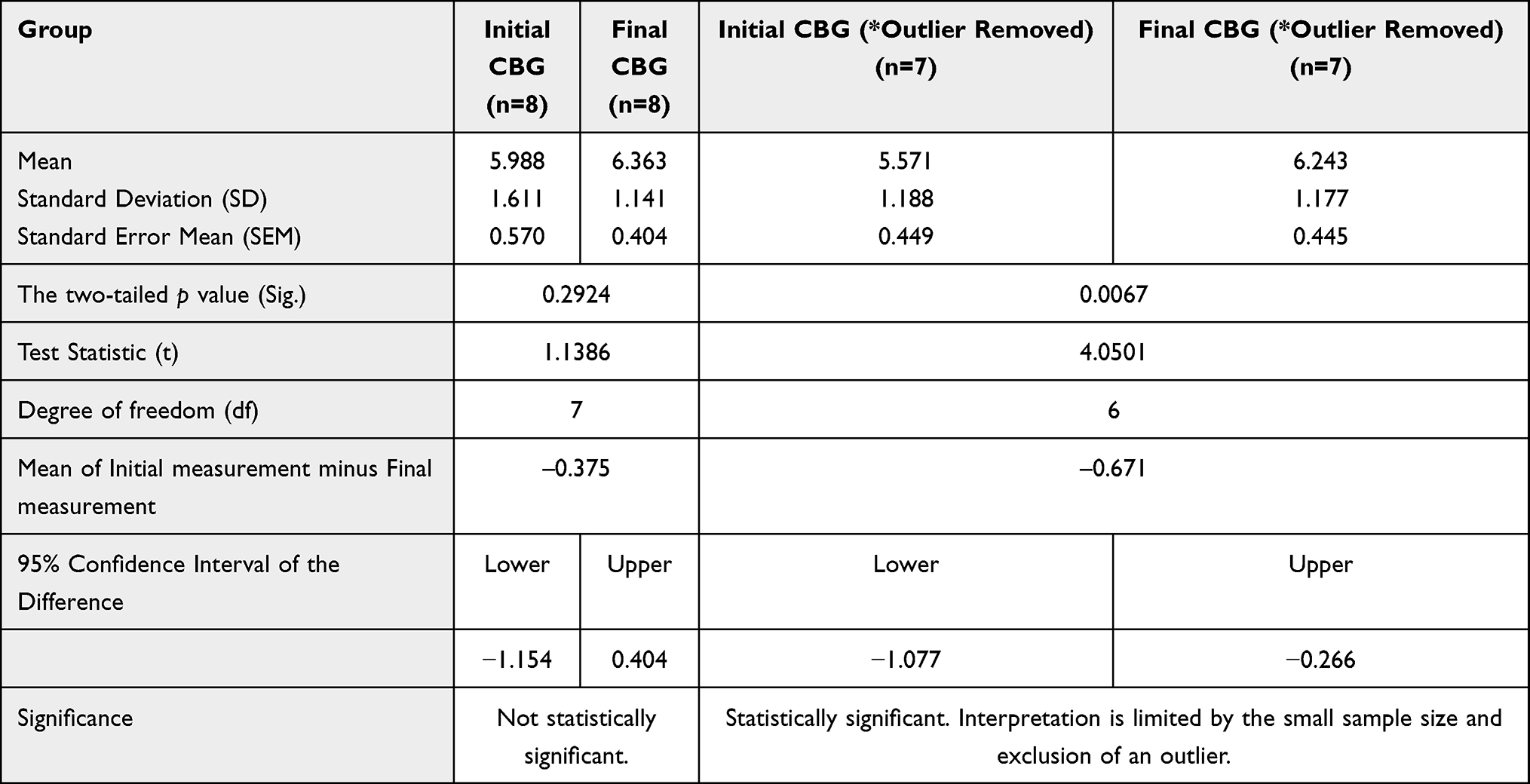 |
Table 7 Inferential Analysis of Pre and Post Nebulisation (CBG) |
Discussion
This study investigated the physiological and metabolic effects of nebulised salbutamol administration in adult asthma patients treated by ambulance services. In this cohort, nebulised salbutamol was consistent with reductions in HR and RR, alongside improvements in SpO2. A modest rise in CBG was also observed following treatment. Most patients showed improved cardiorespiratory observations during the treatment period, although individual metabolic response was varied.
The reductions in RR and HR observed following treatment are consistent with relief of bronchospasm and reduced physiological stress associated with improvement in respiratory distress. These findings align with previous literature describing the bronchodilation effects of β2-agonists on airway smooth muscle and their influence on sympathetic activity.47,48 Nonetheless, the level and direction of HR change varied between patients, with a subset showing an increase in HR following treatment. This variability may reflect differences in exacerbation severity, anxiety, recovery from hypoxia, or individual cardiovascular sensitivity to β2-agonists.49,50 These findings highlight the variability of physiological responses during acute asthma management.
SpO2 increased in most patients during the treatment period. However, this finding should be interpreted cautiously. Nebulised salbutamol was administered using supplemental oxygen, and ambulance protocols targeted oxygen saturations above 94%. Consequently, some of the observed improvement in oxygenation may reflect supplemental oxygen administration rather than bronchodilator therapy alone. Incomplete follow-up observations in some cases further limit definitive interpretation of treatment related oxygenation changes. A proportion of patients also showed inconsistent physiological responses, including cases where SpO2 did not increase despite reductions in HR and RR. This likely reflects the heterogeneous nature of acute asthma exacerbations and the influence of factors such as pre-existing oxygen therapy, co-existing pathology, or variation in treatment response.
A modest rise in CBG was observed within the prospective subgroup. Although β2-agonists are recognised to influence glycogenolysis and gluconeogenesis,51 the small subgroup size and presence of multiple confounding variables preclude attribution of glucose changes solely to salbutamol administration. Acute physiological stress, corticosteroid use, and pre-existing metabolic disease may also contribute to transient glycaemic variation during asthma exacerbations. Most glucose values remained within clinically acceptable ranges.
The present findings are broadly consistent with previous studies reporting improvements in RR and SpO2 following inhaled salbutamol treatment in acute asthma. The mean reduction in RR observed within this cohort (−5 breaths/min) and mean increase in SpO2 (+2%) are comparable with previously reported short-term physiological improvements following bronchodilator therapy in acute asthma management.52,53 The findings are also consistent with reports describing circadian influences on asthma exacerbation patterns, including increased early morning presentations.54,55 Furthermore, the predominance of female patients and broad age distribution observed within this cohort are consistent with recognised demographic trends in asthma populations.56,57 The observed variability in CBG values is also consistent with literature describing heterogeneous metabolic responses to physiological stress and medication exposure.58,59
A strength of this study lies in its use of routine ambulance service data, allowing evaluation of asthma management within a routine emergency care setting. Yet several limitations should be acknowledged, including missing follow-up observations, particularly PEFR measurements and limited assessment of treatment response. PEFR data were available for only four patients and therefore could not contribute meaningfully to asthma specific physiological assessment. Although PEFR measurement is recommended in asthma guidelines,60 operational constraints likely contributed to its limited use in the prehospital setting. Additionally, incomplete documentation relating to medication history and oxygen therapy status limited contextual interpretation of physiological and metabolic findings.
The prospective subgroup represented only a small proportion of the overall cohort, limiting statistical power and generalisability. Several important confounders, including supplemental oxygen therapy, corticosteroid administration, baseline asthma severity, and anxiety-related physiological responses, could not be fully controlled, meaning they may have also influenced HR, SpO2, and CBG levels.
As a whole, this study observed modest improvements in respiratory parameters following prehospital nebulised salbutamol administration, while metabolic findings remained exploratory given limited paired glucose data.
Conclusion and Recommendations
In this observational prehospital study, nebulised salbutamol was associated with modest improvements in respiratory parameters in most patients experiencing acute asthma exacerbations. Respiratory rate generally decreased following treatment, while oxygen saturation improved in many patients during their prehospital care. No clinically significant increase in heart rate was observed overall.
Small increases in capillary blood glucose were identified within the prospectively monitored subgroup, although the limited sample size restricts interpretation of this finding. Variability in physiological response between patients likely reflects the heterogeneous nature of acute asthma presentations encountered during routine ambulance care.
Further research should focus on larger prospective studies with more consistent physiological monitoring and standardised timing of measurements. Improved collection of PEFR data and medication history would also strengthen future analyses of prehospital asthma management and the systemic effects of inhaled β2-agonists.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank all paramedics from the South East Coast Ambulance Service NHS Foundation Trust who contributed to this study, as well as the patients who kindly agreed to participate. We are also grateful to Peter Eaton-Williams for his valuable support in reviewing and editing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific funding.
Disclosure
All authors declare no competing interests in this work.
References
1. Kuruvilla ME, Lee FE, Lee GB. Understanding asthma phenotypes, endotypes, and mechanisms of disease. Clin Rev Allergy Immunol. 2019;56(2):219–16. doi:10.1007/s12016-018-8712-1
2. Mortimer C, Nikoletou D, Ooms A, Williams J. The effects of nebulised beta-2 agonists on clinical observations in asthma exacerbations. J Paramed Pract. 2023;15:1–11. doi:10.12968/jpar.2023.15.2.CPD1
3. Mortimer C, Nikoletou D, Ooms A, Williams J. Clinical reasoning amongst paramedics using nebulised β2 agonists. NPJ Prim Care Respir Med. 2024;34:24. doi:10.1038/s41533-024-00383-w
4. Sengler C, Lau S, Wahn U, Nickel R. Gene–environment interactions in asthma. Respir Res. 2002;3:7. doi:10.1186/rr179
5. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care. Ann Intern Med. 2005;142(4):260–273. doi:10.7326/0003-4819-142-4-200502150-00008
6. Andersson U, Maurin Söderholm H, Wireklint Sundström B, Andersson Hagiwara M, Andersson H. Clinical reasoning in the emergency medical services: an integrative review. Scand J Trauma Resusc Emerg Med. 2019;27(1):76. doi:10.1186/s13049-019-0646-y
7. Bush A. Pathophysiological mechanisms of asthma. Front Pediatr. 2019;7:68. doi:10.3389/fped.2019.00068
8. Hizawa N. The understanding of asthma pathogenesis in the era of precision medicine. Allergol Int. 2023;72(1):3–10. doi:10.1016/j.alit.2022.09.001
9. Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical review: severe asthma. Crit Care. 2002;6(1):30–44. doi:10.1186/cc1451
10. Sellers WFS. Inhaled and IV treatment in acute severe asthma. Br J Anaesth. 2013;110:183–190. doi:10.1093/bja/aes444
11. Almadhoun K, Sharma S. Bronchodilators. In: StatPearls. StatPearls Publishing; 2020. Available from. https://www.ncbi.nlm.nih.gov/books/NBK519028/.
12. Castillo JR, Peters SP, Busse WW. Asthma exacerbations: pathogenesis, prevention, and treatment. J Allergy Clin Immunol Pract. 2017;5(4):918–927. doi:10.1016/j.jaip.2017.05.001
13. Sampson BG, Bersten AD. Therapeutic approach to bronchospasm and asthma. In: Webb A, Angus D, Finfer S, Gattinoni L, Singer M, editors. Oxford Textbook of Critical Care.
14. Torres RM, Souza MDS, Coelho ACC, de Mello LM, Souza-Machado C. Association between asthma and type 2 diabetes mellitus: mechanisms and impact on asthma control-a literature review. Can Respir J. 2021;2021:8830439. doi:10.1155/2021/8830439
15. Nunes C, Pereira AM, Morais-Almeida M. Asthma costs and social impact. Asthma Res Pract. 2017;3:1. doi:10.1186/s40733-016-0029-3
16. Singh AM, Busse WW. Asthma exacerbations. 2: aetiology. Thorax. 2006;61(9):809–816. doi:10.1136/thx.2005.045179
17. Ansari SF, Memon M, Kumar R, Rizwan A. Risk factors associated with frequent acute exacerbations of asthma. Cureus. 2020;12(10):e11090. doi:10.7759/cureus.11090
18. Uppal P, Mohammed SA, Rajashkar S, et al. Type 2 diabetes mellitus, and asthma. Cureus. 2023;15:e36047. doi:10.7759/cureus.36047
19. Bosdriesz JR, Stel VS, van Diepen M, et al. Evidence-based medicine-When observational studies are better than randomized controlled trials. Nephrology. 2020;25(10):737–743. doi:10.1111/nep.13742
20. Song JW, Chung KC. Observational studies: cohort and case-control studies. Plast Reconstr Surg. 2010;126(6):2234–2242. doi:10.1097/PRS.0b013e3181f44abc
21. Paneth N, Joyner M. The use of observational research to inform clinical practice. J Clin Invest. 2021;131(2):e146392. doi:10.1172/JCI146392
22. Eyisi D. Usefulness of qualitative and quantitative approaches in researching problem-solving ability. J Educ Pract. 2016;7:91–100.
23. Ravitch MM. Subjectivity in decision making: common problems and limitations. World J Surg. 1989;13:281–286.
24. Setia MS. Cohort studies. Ind J Dermatol. 2016;61:21–25. doi:10.4103/0019-5154.174011
25. Clarke M. Standardising outcomes in paediatric clinical trials. PLoS Med. 2008;5(4):e102. doi:10.1371/journal.pmed.0050102
26. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
27. Adams RJ, Smith BJ, Ruffin RE. Factors associated with hospital admissions and repeat emergency department visits for adults with asthma. Thorax. 2000;55:566–573. doi:10.1136/thorax.55.7.566
28. Turner J, Jaques R, Crum A, et al. Ambulance Response Programme: final Report. NHS England. 2017. Available from: https://www.england.nhs.uk/wp-content/uploads/2017/07/ARPReport_Final.pdf.
29. Al Amiry A, Maguire BJ. Emergency medical services (EMS) calls during COVID-19: early lessons learned for systems planning. Open Access Emerg Med. 2021;13:407–414. doi:10.2147/OAEM.S324568
30. Mortimer C. A preliminary study to determine the effects of nebulised salbutamol on blood glucose levels during an acute asthma exacerbation. Eur Respir J. 2019;54:PA4243.
31. Hess DR. Retrospective studies and chart reviews. Respir Care. 2004;49(10):1171–1174. doi:10.4187/respcare.04491171
32. Cole SR, Chu H, Allison PD, Gange SJ. Combined analysis of retrospective and prospective occurrences in cohort studies: HIV-1 serostatus and incident pneumonia. Int J Epidemiol. 2006;35(6):1442–1446. doi:10.1093/ije/dyl176
33. Collin M, Manson J, Morris C. Joint statement on seeking consent by electronic methods v1.2. 2018. Available from: https://www.hra.nhs.uk/about-us/news-updates/hra-and-mhra-publish-joint-statement-seeking-and-documenting-consent-using-electronic-methods-econsent/.
34. S FAA, Ahmad S. Stimulating training motivation using the right training characteristic. Ind Commer Train. 2011;43:53–61. doi:10.1108/00197851111098171
35. Prout H, Tod A, Neal R, Nelson A. Maximising recruitment of research participants into a general practice based randomised controlled trial concerning lung diagnosis-staff insights from an embedded qualitative study. Trials. 2022;23(1):225. doi:10.1186/s13063-022-06125-y
36. Slade D, Scheeres H, Manidis M, et al. Emergency communication in emergency departments. Discourse Commun. 2008;2:271–298. doi:10.1177/1750481308091910
37. Pun JK, Chan EA, Murray KA, Slade D, Matthiessen CM. Complexities of emergency communication: clinicians’ perceptions of communication challenges in a trilingual emergency department. J Clin Nurs. 2017;26(21–22):3396–3407. doi:10.1111/jocn.13699
38. Valencia Morales DJ, Bansal V, Heavner SF, et al. Validation of automated data abstraction for SCCM discovery VIRUS COVID-19 registry: practical EHR export pathways (VIRUS-PEEP). Front Med. 2023;10:1089087. doi:10.3389/fmed.2023.1089087
39. Loeb S, Dynarski S, McFarland D, Morris P, Reardon S, Reber S. Descriptive analysis in education. NCEE. 2017;4023. Available from https://files.eric.ed.gov/fulltext/ED573325.pdf.
40. Kaliyadan F, Kulkarni V. Types of variables, descriptive statistics, and sample size. Indian Dermatol Online J. 2019;10(1):82–86. doi:10.4103/idoj.IDOJ_468_18
41. P.a B. Problems with rates based on small numbers. Statistical Primer No. 12. North Carolina Department of Health and Human Services. 2008. Available from: https://schs.dph.ncdhhs.gov/schs/pdf/primer12_2.pdf.
42. Sinayev A, Peters E, Tusler M, Fraenkel L. Presenting numeric information with percentages and descriptive risk labels: a randomized trial. Med Decis Making. 2015;35(8):937–947. doi:10.1177/0272989X15584922
43. Ghasemi A, Zahediasl S. Normality tests for statistical analysis: a guide for non-statisticians. Int J Endocrinol Metab. 2012;10(2):486–489. doi:10.5812/ijem.3505
44. Kamper SJ. Control groups: linking evidence to practice. J Orthop Sports Phys Ther. 2018;48(11):905–906. doi:10.2519/jospt.2018.0706
45. Caughlin DE. Evaluating a pre-test/post-test without control group design. R for HR An introduction to human resource analytics using R. 2024. Available from: https://rforhr.com/pretestposttest.html.
46. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
47. Miyasaka T, Dobashi-Okuyama K, Takahashi T, Takayanagi M, Ohno I. The interplay between neuroendocrine activity and psychological stress-induced exacerbation of allergic asthma. Allergol Int. 2018;67:32–42. doi:10.1016/j.alit.2017.04.013
48. Higgins ET, Davidson RJ, Busse WW, et al. Clinically relevant effects of mindfulness-based stress reduction in individuals with asthma. Brain Behav Immun Health. 2022;25:100509. doi:10.1016/j.bbih.2022.100509
49. Tiwari R, Kumar R, Malik S, Raj T, Kumar P. Analysis of heart rate variability and implication of different factors on heart rate variability. Curr Cardiol Rev. 2021;17(5):e160721189770. doi:10.2174/1573403X16999201231203854
50. Togher FJ, O’Cathain A, Phung VH, Turner J, Siriwardena AN. Reassurance as a key outcome valued by emergency ambulance service users: a qualitative interview study. Health Expect. 2015;18(6):2951–2961. doi:10.1111/hex.12279
51. Wong H, Singh J, Go RM, Ahluwalia N, Guerrero-Go MA. The effects of mental stress on non-insulin-dependent diabetes: determining the relationship between catecholamine and adrenergic signals from stress, anxiety, and depression on the physiological changes in the pancreatic hormone secretion. Cureus. 2019;11(8):e5474. doi:10.7759/cureus.5474
52. Hodder R, Lougheed MD, Rowe BH, FitzGerald JM, Kaplan AG, McIvor RA. Management of acute asthma in adults in the emergency department: nonventilatory management. CMAJ. 2010;182(2):55–67. doi:10.1503/cmaj.080072
53. van Wamel A, Procter S. Why take a peak flow in asthma? J Paramed Pract. 2010;2:56–62. doi:10.12968/jpar.2010.2.2.46760
54. Hetzel MR, Clark TJ, Houston K. Physiological patterns in early morning asthma. Thorax. 1977;32(4):418–423. doi:10.1136/thx.32.4.418
55. Lodhi S, Smith JA, Satia I, Holt KJ, Maidstone RJ, Durrington HJ. Cough rhythms in asthma: potential implication for management. J Allergy Clin Immunol Pract. 2019;7(6):2024–2027. doi:10.1016/j.jaip.2018.12.020
56. Zein JG, Erzurum SC. Asthma is different in women. Curr Allergy Asthma Rep. 2015;15(6):28. doi:10.1007/s11882-015-0528-y
57. Cukic V, Lovre V, Dragisic D, Ustamujic A. Asthma and COPD — differences and similarities. Mater Sociomed. 2012;24:100–105. doi:10.5455/msm.2012.24.100-105
58. Schneider H, Shaw J, Zimmet P. Guidelines for the detection of diabetes mellitus--diagnostic criteria and rationale for screening. Clin Biochem Rev. 2003;24(3):77–80.
59. Weinisch P, Fiamoncini J, Schranner D, et al. Dynamic patterns of postprandial metabolic responses to three dietary challenges. Front Nutr. 2022;9:933526. doi:10.3389/fnut.2022.933526
60. Joint Royal Colleges Ambulance Liaison Committee. JRCALC clinical practice guidelines. 2022. Available from: https://aace.org.uk/clinical-practice-guidelines/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.