Back to Journals » International Medical Case Reports Journal » Volume 17
Busin Glide-Assisted Pull-Through Insertion of Artificial Corneal Endothelium (EndoArt)
Authors Kobayashi A ![]() , Hayashi T
, Hayashi T ![]() , Igarashi A, Shimizu T, Yokogawa H
, Igarashi A, Shimizu T, Yokogawa H ![]() , Yuda K, Bachmann B, Yamagami S, Sugiyama K
, Yuda K, Bachmann B, Yamagami S, Sugiyama K
Received 12 July 2024
Accepted for publication 30 August 2024
Published 25 September 2024 Volume 2024:17 Pages 795—800
DOI https://doi.org/10.2147/IMCRJ.S482261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Busin glide-assisted pull-through insertion of EndoArt - Supplementary Video [482261]
Views: 186
Akira Kobayashi,1 Takahiko Hayashi,2 Ami Igarashi,2 Toshiki Shimizu,2 Hideaki Yokogawa,1 Kentaro Yuda,3 Björn Bachmann,4 Satoru Yamagami,2 Kazuhisa Sugiyama1
1Department of Ophthalmology, Kanazawa University Hospital, Ishikawa, Japan; 2Department of Ophthalmology and Department of Visual Sciences, Nihon University School of Medicine, Itabashi, Tokyo, Japan; 3Kikuna Yuda Eye Clinic, Yokohama, Japan; 4Department of Ophthalmology, University of Cologne, Faculty of Medicine and University Hospital Cologne, Cologne, Germany
Correspondence: Akira Kobayashi, Department of Ophthalmology, Kanazawa University Graduate School of Medical Science, Takara-machi 13-1, Kanazawa, Ishikawa-ken, 920-8641, Japan, Tel +81-76-265-2403, Fax +81-76-222-9660, Email [email protected]
Background: Currently, the push-in technique through the corneal tunnel using a blunt-tip spatula is used to insert an artificial corneal endothelium (EndoArt) into the anterior chamber (AC). The device is useful for patients with bullous keratopathy; however, it may be difficult to manipulate the very thin implant through hazy cornea. Unlike DMEK graft, it cannot be stained and the F-mark is faint. So, visualizing and orienting the implant is a real challenge especially through a hazy cornea and inadequate AC visualization. Therefore, alternative EndoArt implantation techniques are needed in patients with advanced endothelial dysfunction to avoid complications.
Purpose: To report an alternative technique for EndoArt implantation using a Busin glide.
Technique: The EndoArt was loaded onto the Busin glide with the concave side of the EndoArt facing upward and was then pulled/pushed into the Busin glide opening. After the Descemet’s membrane and endothelium were detached and removed in a circular fashion in a patient with advanced corneal endothelial decompensation, the Busin glide was inserted into the corneal incision, and the EndoArt was slowly pulled into the AC using retractor forceps. Finally, the air was injected into the AC.
Conclusion: The Busin glide-assisted pull-through technique smoothly and securely inserted the EndoArt into the AC without upside-down attachment. This alternative technique can be useful for patients with a history of repeat intraocular surgeries or trauma with severe corneal edema to avoid potential complications such as epithelial implantation cysts or downgrowth.
Keywords: endothelial keratoplasty, artificial corneal endothelium, EndoArt, bullous keratopathy, Descemet’s membrane endothelial keratoplasty
Introduction
To date, endothelial keratoplasty (EK) techniques, such as Descemet’s stripping automated EK (DSAEK) and Descemet’s membrane EK (DMEK), are favorably used to treat all types of corneal endothelial dysfunction.1 The advantages of EK compared to penetrating keratoplasty (PK) include less invasiveness or corneal graft rejection and faster visual acuity with less astigmatism. By 2022, in the United States, 89.9% of patients with corneal endothelial dysfunction had undergone DSAEK or DMEK.1 In Germany, EK accounted for approximately 60% of all keratoplasties in 2016, 92% of which were DMEK.2 Although the overall success rate of DSAEK/DMEK is quite high,3–5 several factors are considered as negative prognostic factors for graft survival after EK; these include prior graft failure, bullous keratopathy, glaucoma, and previous complicated anterior segment surgery.3
To circumvent these difficulties, a novel artificial corneal endothelium (EndoArt, EyeYon Medical, Israel) device was developed.6 EndoArt is a CE-approved device for the treatment of corneal edema, comprising an acrylic hydrophilic, flexible material measuring 30–50 µm in thickness and 6.0–8.0 mm in diameter, shaped according to the posterior corneal curvature, which acts as an artificial fluid barrier to replace the function of the diseased corneal endothelium. Once the device adheres to the inner corneal surface, aqueous penetration of the central corneal stroma is prevented, reducing stromal edema and improving corneal transparency.
Currently, the push-in technique through the corneal tunnel using a blunt-tip spatula is mainly used to insert the EndoArt into the anterior chamber.6,7 The device is useful for patients with bullous keratopathy; however, it may be difficult to manipulate the very thin implant through hazy cornea. Unlike DMEK graft, it cannot be stained and the F-mark is faint. So, visualizing and orienting the implant is a real challenge especially through a hazy cornea and inadequate anterior chamber (AC) visualization. Therefore, there is a need for alternative techniques for corneal implantation in patients with advanced endothelial dysfunction to avoid upside-down attachment. Additionally, avoiding direct contact between the EndoArt and conjunctiva may prevent bacterial contamination between the EndoArt and host stroma.
Herein, we describe the use of Busin glide-assisted pull-through insertion of an EndoArt as a novel alternative technique for EndoArt implantation.
Case Reports and Techniques
An 82-year-old female was referred to our clinic complaining of eye pain and decreased visual acuity in her left eye. The patient had been previously diagnosed with Fuchs’ corneal endothelial dystrophy with numerous characteristic guttae on corneal specular microscopy. Cataract surgery and intraocular lens implantation were performed elsewhere prior to her referral to our clinic. Slit-lamp examination revealed a beaten-metal appearance, characteristic of Fuchs’ corneal endothelial dystrophy in both eyes, and epithelial bullae in her left eye. The intraocular pressure was within normal limits in both eyes. The best-corrected visual acuities were 0.5 (decimal) and 0.1 in the right and left eye, respectively. DMEK was performed in 2019 to improve visual acuity and alleviate eye pain. Postoperatively, the visual acuity in her left eye improved from 0.1 to 0.2, despite the presence of a dense epiretinal membrane. However, repeated endothelial rejection occurred during the postoperative course, resulting in late endothelial failure and decreased visual acuity during hand motion. Slit-lamp examination of the left eye revealed bullous keratopathy with diffuse significant corneal edema. Band-shaped keratopathy also occurred in the eye.
To prevent further rejection, EndoArt was considered as a surgical therapy to alleviate ocular pain and promote visual rehabilitation. Severe corneal opacity with band keratopathy prevented maneuver visualization in the AC. After a detailed consultation, the patient agreed to undergo EndoArt implantation. To circumvent the difficulty of poor visualization of the AC, an alternative novel surgical technique, Busin glide-assisted pull-through insertion, was used to implant the EndoArt (Figure 1A–F, Supplementary Video). Briefly, three paracentesis incisions were made at the 1, 9, and 10 o’clock positions, and a 2.7-mm clear corneal incision was made at the 3 o’clock position. An AC maintainer was inserted into the AC through the 10 o’clock paracentesis. After removing the corneal epithelium and band keratopathy to improve visualization, a failed 8-mm-diameter DMEK graft was removed using a reverse Sinskey hook (#19091, Moria, Antony, France). EndoArt was spread over the spatula of a Busin glide (#19098, Moria). To ensure correct orientation, a letter “F” symbol (Figure 1A and B), which was also visible using an endo-illuminator light, was used as a reference owing to its asymmetrical characteristics. Viscoelastic material was not used throughout the procedure because there were no viable endothelial cells on the EndoArt. The EndoArt was then pulled into the glide opening (Figure 1C). The glide was inverted and positioned at the entrance of the nasal corneal tunnel. A 25-G DSAEK forceps (AE-4221, ASICO, Westmont, IL) was passed through a temporal paracentesis wound across the anterior chamber, and the edge of the EndoArt was grasped (Figure 1D). An AC maintainer was placed at the 10 o’clock position with minimal continuous irrigation. The EndoArt was pulled into the AC (Figure 1E). The device was left to unfold spontaneously under continuous irrigation. After securing the wound with a 10–0 nylon suture, air was injected to attach the EndoArt to the posterior stromal surface. A reverse Sinskey hook was used to place the EndoArt at the desired central position of the cornea. One 10–0 nylon suture at the 12 o’clock position was used to anchor the device to the stroma (Figure 1F). EndoArt attachment was confirmed by intraoperative spectral-domain optical coherence tomography using ARTEVO800 (Carl Zeiss Meditec, Jena, Germany) (Figure 2A and B). The AC was left full of gas (20% SF6), and the patient was instructed to lie on her back for 6–8 h. On day one postoperatively, the EndoArt device was partially detached, additional air was injected into the AC, and the device was completely attached. No complications occurred during the surgical procedures. The postoperative topical regimen included a topical antibiotic drop four times daily for 2 weeks and a low-dose corticosteroid drop four times daily as long-term treatment. The patient was followed-up for 3 months; corneal edema gradually improved over time, and all epithelial bullae resolved. The central corneal thickness (CCT) decreased from 845 μm to 530 μm (Figure 3A and B). The best-corrected visual acuity improved from hand motion to 0.01 (decimal), which was due to circumvention of the dense epiretinal membrane with cystoid macular edema that existed preoperatively. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board/Ethics Committee of the Kikuna Yuda Eye Clinic in Yokohama, Japan (#2023-2, UMIN000051282). Written informed consent to publish the case details and accompanying images was obtained prior to the surgery. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research. Institutional approval was not required to publish the case details.
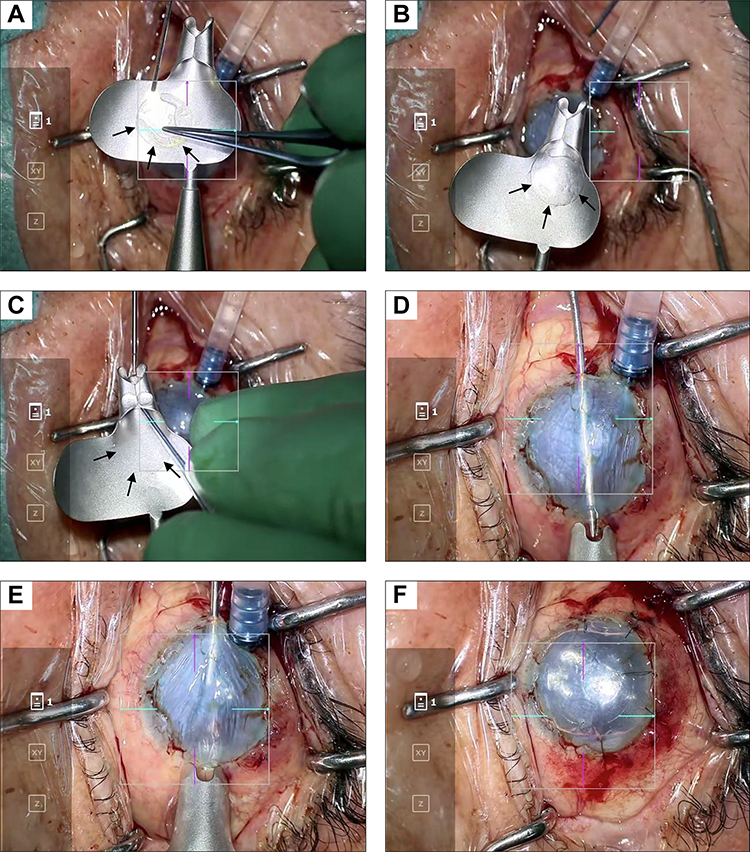 |
Figure 1 (A and B) The EndoArt (arrows) was spread over the spatula of the Busin glide to ensure correct orientation through an irreversible F letter; however, this is not very much visible in this video/screenshots. (C) The EndoArt was then pulled into the glide opening. (D) The glide was then inverted and positioned at the entrance of a nasal corneal tunnel. A 25-G Descemet’s stripping automated endothelial keratoplasty (DSAEK) forceps was passed through a temporal paracentesis wound across the anterior chamber and grasped the edge of the EndoArt. (E) The donor lamella was pulled into the anterior chamber. The donor lamella was left to unfold spontaneously under continuous irrigation. (F) After securing the wound using a single 10–0 nylon suture, air was injected to attach the EndoArt to the posterior stromal surface. The reverse Sinskey hook was used to place the EndoArt to the desired central position of the cornea. One 10–0 Nylon suture was used to anchor the device to the stroma. |
 |
Figure 2 (A and B) EndoArt attachment was confirmed using intraoperative spectral domain optical coherence tomography. |
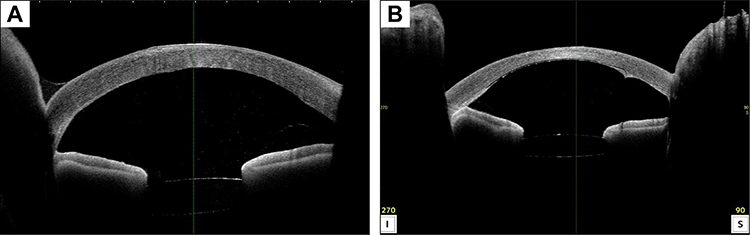 |
Figure 3 (A) Anterior segment optical coherence tomography image showing bullous keratopathy before surgery. The corneal thickness was 753 µm. (B) Postoperatively, the corneal thickness reduced to 530 µm with clearance of corneal edema. The eye pain also disappeared. |
The techniques described herein were also successfully performed in more cases by different surgeon (B.B). and its usefulness has been confirmed.
Discussion and Conclusion
In this report, we demonstrated an alternative EndoArt insertion technique using a Busin glide, which we have termed the Busin glide-assisted pull-through insertion technique. We tried several more cases and confirmed the usefulness of this technique. An initial report by Auffarth and coworkers showed that EndoArt was placed in the cartridge of an intraocular lens injector, Accuject (Medicel AG, Altenrhein, Switzerland), and manually implanted into the AC using the push-in technique.6 Subsequently, Fontana et al reported early outcomes of the EndoArt after failed repeat EK.7 They used a blunt-tip spatula (Janach Srl, Como, Italy) to push the device through the corneal tunnel, promoting device coiling during the passage. Although this push-in technique worked well in most cases, we found it difficult to confirm the correct orientation of the EndoArt in cases of severe corneal edema.
In contrast to that in Western countries, the incidence of Fuchs’ corneal endothelial dystrophy as a cause of corneal endothelial dysfunction is relatively low in Japan. Instead, argon laser-induced corneal endothelial decompensation, bullous keratopathy, and post-glaucoma surgery account for most of the causes; they tend to show severe corneal edema with inadequate AC visualization.8 We have previously shown the usefulness of an endo-illuminator for DSAEK and DMEK to improve visualization of the graft in the AC.9 Additionally, we used an intraocular lens glide together with a Busin glide to safely insert DSAEK graft and called the procedure the Kobayashi double-glide method.10 Therefore, using the Busin glide to insert EndoArt in eyes with severe corneal edema is convenient. Using an endo-illuminator, the F letter symbol on the EndoArt was clearly visible on the Busin glide and after attachment behind the posterior stroma, confirming the correct orientation.
Recently, Abusayf et al reported the usefulness of pull-through insertion to implant the EndoArt in complex eyes, especially in Asian eyes with unstable iris lens diaphragm.11 They also described multiple sutures to the EndoArt to decrease the likelihood of postop detachment. We find this technique to be both elegant and effective, and further augmented the pull-through technique using a Busin glide. Additionally, using a Busin glide to insert the device may avoid direct contact of EndoArt with the conjunctiva, reducing the potential risk of epithelial implantation cysts or downgrowth, which are serious complications seen in DMEK in our experience. Furthermore, transfection of bacteria residing in the conjunctiva into the space between the host tissue and the graft might be prevented. Another consideration for using the Busin glide-assisted insertion technique would be for aphakic eyes or in eyes with incomplete iris, as a DSAEK/DMEK/EndoArt can be lost to the posterior segment if inserted with an injector or push through method.
With the Busin glide it is held in place by the forceps in the AC and air can be injected underneath before the forceps is removed.
In conclusion, the Busin glide-assisted pull-through technique smoothly and securely inserted the EndoArt into the AC without upside-down attachment. This alternative technique can be useful for patients with a history of repeat intraocular surgeries or trauma with severe corneal edema to avoid potential complications such as epithelial implantation cysts or downgrowth.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to disclose regarding any of the products mentioned in this article.
References
1. Eye Bank Association of America. 2022 Eye Banking Statistical Report. Available from: https://restoresight.org/members/publications/statisticalreport/.
2. Flockerzi E, Maier P, Böhringer D, et al. All German keratoplasty registry contributors. Trends in corneal transplantation from 2001 to 2016 in Germany: a report of the DOG-section cornea and its keratoplasty registry. Am J Ophthalmol. 2018;188:91–98. doi:10.1016/j.ajo.2018.01.018
3. Zafar S, Wang P, Woreta FA, et al. Risk factors for repeat keratoplasty after endothelial keratoplasty in the medicare population. Am J Ophthalmol. 2021;221:287–298. doi:10.1016/j.ajo.2020.08.006
4. Birbal RS, Ni Dhubhghaill S, Bourgonje VJA, et al. Five-year graft survival and clinical outcomes of 500 consecutive cases after Descemet membrane endothelial keratoplasty. Cornea. 2020;39:290–297. doi:10.1097/ICO.0000000000002120
5. Ang M, Soh Y, Htoon HM, et al. Five-year graft survival comparing Descemet stripping automated endothelial keratoplasty and penetrating keratoplasty. Ophthalmology. 2016;123:1646–1652. doi:10.1016/j.ophtha.2016.04.049
6. Auffarth GU, Son HS, Koch M, et al. Implantation of an artificial endothelial layer for treatment of chronic corneal edema. Cornea. 2021;40:1633–1638. doi:10.1097/ICO.0000000000002806
7. Fontana L, Di Geronimo N, Cennamo M, et al. Early outcomes of an artificial endothelial replacement membrane implantation after failed repeat endothelial keratoplasty. Cornea. 2023;2023:10–1097. Online ahead of print.
8. Nishino T, Kobayashi A, Yokogawa H, et al. Changing indications and surgical techniques for keratoplasty during a 16-year period (2003-2018) at a tertiary referral hospital in Japan. Clin Ophthalmol. 2019;13:1499–1509. doi:10.2147/OPTH.S214515
9. Kobayashi A, Yokogawa H, Yamazaki N, et al. The use of endoillumination probe-assisted Descemet membrane endothelial keratoplasty for bullous keratopathy secondary to argon laser iridotomy. Clin Ophthalmol. 2015;9:91–93. doi:10.2147/OPTH.S74981
10. Kobayashi A, Yokogawa H, Sugiyama K. Descemet stripping with automated endothelial keratoplasty for bullous keratopathies secondary to argon laser iridotomy--preliminary results and usefulness of double-glide donor insertion technique. Cornea. 2008;27 Suppl 1:S62–S69. doi:10.1097/ICO.0b013e31817f38e9
11. Abusayf MM, Tan GS, Jodhbir S, et al. Pull-through insertion of EndoArt for complex eyes. Am J Ophthalmol Case Rep. 2023;32:101878. doi:10.1016/j.ajoc.2023.101878
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Outcomes of Synthetic Corneal Endothelial Implant in Patients with Corneal Oedema with or without Prior Endothelial Keratoplasty: A Case Series
Levy I, Mukhija R, Nanavaty MA
Clinical Ophthalmology 2026, 20:604707
Published Date: 3 June 2026