Back to Journals » International Journal of Women's Health » Volume 18
Burden and Risk Factor Patterns of Reproductive System Tumors and Non-Tumor Diseases Among Asian Women, 1990–2021: Evidence from the GBD Study
Authors Xiong X ![]() , Yao Y, Yang G, Lin C
, Yao Y, Yang G, Lin C
Received 7 October 2025
Accepted for publication 3 February 2026
Published 11 February 2026 Volume 2026:18 572535
DOI https://doi.org/10.2147/IJWH.S572535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Xinyi Xiong,1,2,* Yuming Yao,2,3,* Guang Yang,2,3 Chiayen Lin2,4– 6
1Department of Infectious Diseases, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 3Department of Orthopedics, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 4Department of General Surgery, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 5Hunan Provincial Clinical Medical Research Centre for Thyroid Diseases, Changsha, Hunan, People’s Republic of China; 6Hunan Engineering Research Central for Thyroid and Related Diseases Diagnosis and Treatment Technology, Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chiayen Lin, Email [email protected]
Background: Female reproductive system diseases, including malignant tumors such as breast, ovarian, and uterine cancers, and non-neoplastic disorders such as uterine fibroids, endometriosis, polycystic ovary syndrome (PCOS), infertility, and premenstrual syndrome (PMS), represent major health challenges in Asia. While malignant diseases receive considerable attention due to high mortality, the long-term burden of non-malignant conditions affecting fertility, psychological well-being, and quality of life remains underestimated.
Methods: Data from the Global Burden of Disease (GBD) 2021 were used to quantify the burden of female reproductive system diseases in 47 Asian countries and territories from 1990 to 2021. Incidence, prevalence, mortality, and disability-adjusted life years (DALYs) were analyzed, together with age-standardized rates. Temporal trends were assessed using estimated annual percentage change (EAPC), and disease burden patterns were examined across Socio-demographic Index (SDI) levels. Associations between major modifiable risk factors and disease burden were described.
Results: In 2021, female reproductive system diseases accounted for over 33 million DALYs and approximately 600,000 deaths in Asia. Breast and cervical cancers were the leading contributors to mortality and DALYs, whereas PMS and infertility accounted for a substantial burden among younger women. From 1990 to 2021, absolute case numbers and deaths increased with population growth and aging, while most age-standardized rates declined, particularly for cervical cancer. In contrast, PCOS and infertility showed the fastest increases. High body mass index and elevated fasting glucose were strongly associated with breast and uterine cancer burden, while smoking was closely associated with cervical cancer burden.
Conclusion: Female reproductive system diseases impose a substantial and heterogeneous burden across Asia. Although malignant cancers remain the main contributors to mortality and DALYs, non-malignant disorders increasingly affect reproductive health, particularly among younger women. Prevention strategies tailored to SDI levels and major risk factors are needed to reduce the overall disease burden across the region.
Keywords: female reproductive system diseases, global burden of disease, Asia, disability-adjusted life years, risk factors, women
Introduction
Female reproductive system diseases have emerged as a pressing global public health concern, posing significant challenges not only to physical health but also to broader aspects of women’s well-being.1 These conditions encompass both malignant tumors, such as breast and ovarian cancers, and a diverse spectrum of non-malignant gynecological disorders, including endometriosis, infertility, and uterine fibroids.2 Collectively, these diseases have profound consequences: they compromise fertility,3,4 generate substantial psychological and emotional stress, and negatively influence women’s roles within families, their participation in social life, and their economic opportunities. Unlike malignancies such as breast cancer, which have been extensively studied and prioritized in public health agendas, non-cancerous gynecological conditions often receive insufficient attention.2,5,6 Because these disorders rarely result in immediate mortality, their impact tends to be underestimated, and the allocation of health resources and policy efforts does not adequately reflect the true burden they impose on women’s health and quality of life.7
The Global Burden of Disease (GBD) study offers a comprehensive and standardized framework for evaluating disease burden worldwide. The most recent dataset, GBD 2021, includes information from 204 countries and territories spanning the period from 1990 to 2021.8,9 This resource provides detailed insights into long-term epidemiological trends, health outcomes, and attributable risk factors, making it particularly valuable for understanding the patterns of female reproductive system diseases.10 While several studies have examined the global burden of specific conditions or analyzed trends in selected countries,2,11–14 systematic evaluations of the overall burden of female reproductive system diseases in Asia remain limited. Asia is the world’s most populous region and hosts a substantial proportion of the global female population.15 Rapid demographic and epidemiological transitions, including population aging, declining fertility, delayed childbearing, and lifestyle changes, are reshaping the burden and distribution of reproductive system diseases across many Asian countries.16 These transitions have been accompanied by increasing risks of hormone-related cancers and metabolic conditions.17 Meanwhile, marked heterogeneity in health system capacity, screening coverage, and sociocultural contexts across Asia may contribute to delayed diagnosis and underestimation of non-malignant gynecological disorders. Given the increasing recognition of women’s health issues across Asian countries, where rapid demographic, economic, and social transitions are also reshaping health needs, the lack of comprehensive data represents an important knowledge gap.
To address this, our study systematically analyzes the epidemiological characteristics and temporal trends of female reproductive system diseases across five Asian regions and 47 countries from 1990 to 2021.18 By stratifying results by geographic area, age group, period, and sociodemographic index (SDI), we assess incidence, prevalence, mortality, and disability-adjusted life years (DALYs), providing a multidimensional view of disease burden. Furthermore, we describe patterns of disease burden in relation to major risk factors and present their associations with overall disease outcomes. Together, these analyses aim to generate robust and regionally relevant evidence that can guide health policy, inform prevention strategies, and ultimately reduce the burden of reproductive system diseases among Asian women.
Materials and Methods
Overview
The GBD 2021 study provided standardized and comparable estimates of the burden of 371 diseases and injuries across 204 countries and territories from 1990 to 2021, with detailed findings published in the core GBD reports.19–21 The study integrated multiple data sources, including population censuses, civil registration systems, health surveys, and epidemiological surveillance, and applied DisMod-MR 2.1, a Bayesian meta-regression tool, to adjust for bias and conduct model-based estimations. DisMod-MR 2.1 synthesizes heterogeneous epidemiological data sources, including incidence, prevalence, remission, and mortality data, and generates internally consistent estimates by borrowing strength across locations, age groups, and time; corresponding uncertainty intervals were derived through posterior sampling from the Bayesian model. The complete methodological framework is described in detail in the GBD 2021 publications.20 All publicly available data can be accessed via the Global Health Data Exchange platform (http://ghdx.healthdata.org/gbd-results-tool).
Disease Burden Analysis
This study examined five categories of female reproductive system diseases: breast cancer, cervical cancer, uterine cancer, ovarian cancer, and gynecological disorders. The latter category was further subdivided into endometriosis, female infertility, genital prolapse, polycystic ovary syndrome (PCOS), premenstrual syndrome (PMS), uterine fibroids, and other gynecological conditions. Detailed definitions of each disease and the corresponding International Classification of Diseases (ICD) codes are provided in Supplementary Materials 1 and 2. It should be noted that non-malignant gynecological conditions may be subject to misclassification or underestimation in some settings, particularly in regions with limited access to health care or incomplete diagnostic reporting.
To better reflect geographic and sociocultural characteristics of Asia, we reclassified countries into subregions commonly used in regional analyses. Based on geographic proximity, 47 Asian countries were classified into five subregions, namely East Asia, South Asia, West Asia, Central Asia, and Southeast Asia. It should be noted that the regional classification adopted in GBD 2021 does not fully correspond to that used in this study. For instance, in the GBD database, the “Southeast Asia” region includes countries such as Seychelles and Mauritius, which are located outside Asia, while data for West Asia are unavailable. The regional classification applied in this analysis is presented in Table S1. To enhance comparability across regions, age-standardized rates (ASRs) were calculated using the direct standardization method based on the GBD 2021 global standard population.22,23
Within the GBD 2021 framework, the major risk factors for female reproductive system diseases were defined as follows: breast cancer was mainly associated with high red meat intake, elevated fasting plasma glucose, high body mass index (BMI), low physical activity, second-hand smoke exposure, active smoking, and alcohol consumption; cervical cancer was linked to unsafe sexual practices and smoking; and both uterine and ovarian cancers were related to high BMI, with ovarian cancer additionally associated with occupational asbestos exposure. Risk factor attribution was conducted in accordance with the GBD 2021 comparative risk assessment framework.
To quantify the contribution of these risk factors to disease burden, we employed the population-attributable fraction (PAF) method. Attributable DALYs were calculated by multiplying the total DALYs of each disease by the corresponding PAF value. The PAF represents the proportion of disease burden that could be avoided if exposure levels were reduced to the theoretical minimum risk exposure level. Furthermore, the relative contribution of each risk factor was evaluated by dividing its attributable age-standardized DALY rate by the total age-standardized DALY rate of the respective disease. Due to the uneven economic development across Asian regions, this study incorporates the SDI into the analysis framework to account for socio-economic variations in disease burden.24 According to the official GBD methodology, countries and territories were classified into five socio-demographic index levels based on their relative level of socio-demographic development, including low, low-middle, middle, high-middle, and high SDI categories.25
Data on incidence, prevalence, mortality, DALYs, ASRs, and their 95% uncertainty intervals (UIs) for females across all age groups (0–95+ years) were extracted from the GBD 2021 database for the period 1990–2021. Temporal trends between 1990 and 2021 were assessed using estimated annual percentage changes (EAPCs).26 All analyses and visualizations were performed in R software (version 4.4.0).
Results
Distribution of the Burden of Female Reproductive System Diseases (DFRS) in Asia, 2021
In 2021, the number of newly diagnosed cases of female reproductive system diseases DFRS in Asia was estimated at 393 million, while the number of existing cases reached 889 million. Overall, newly diagnosed cases were equivalent to about 17% of the total female population, while prevalent cases accounted for approximately 39%. DFRS accounted for approximately 34 million DALYs, equivalent to 5% of all DALYs among Asian women. They were also the direct cause of around 590,000 deaths, representing 4% of total female deaths in the region. After age standardization, the incidence, prevalence, and mortality rates of DFRS were 16,454, 37,124, and 28 per 100,000 population, respectively, with a DALY rate of 1332 (Table 1).
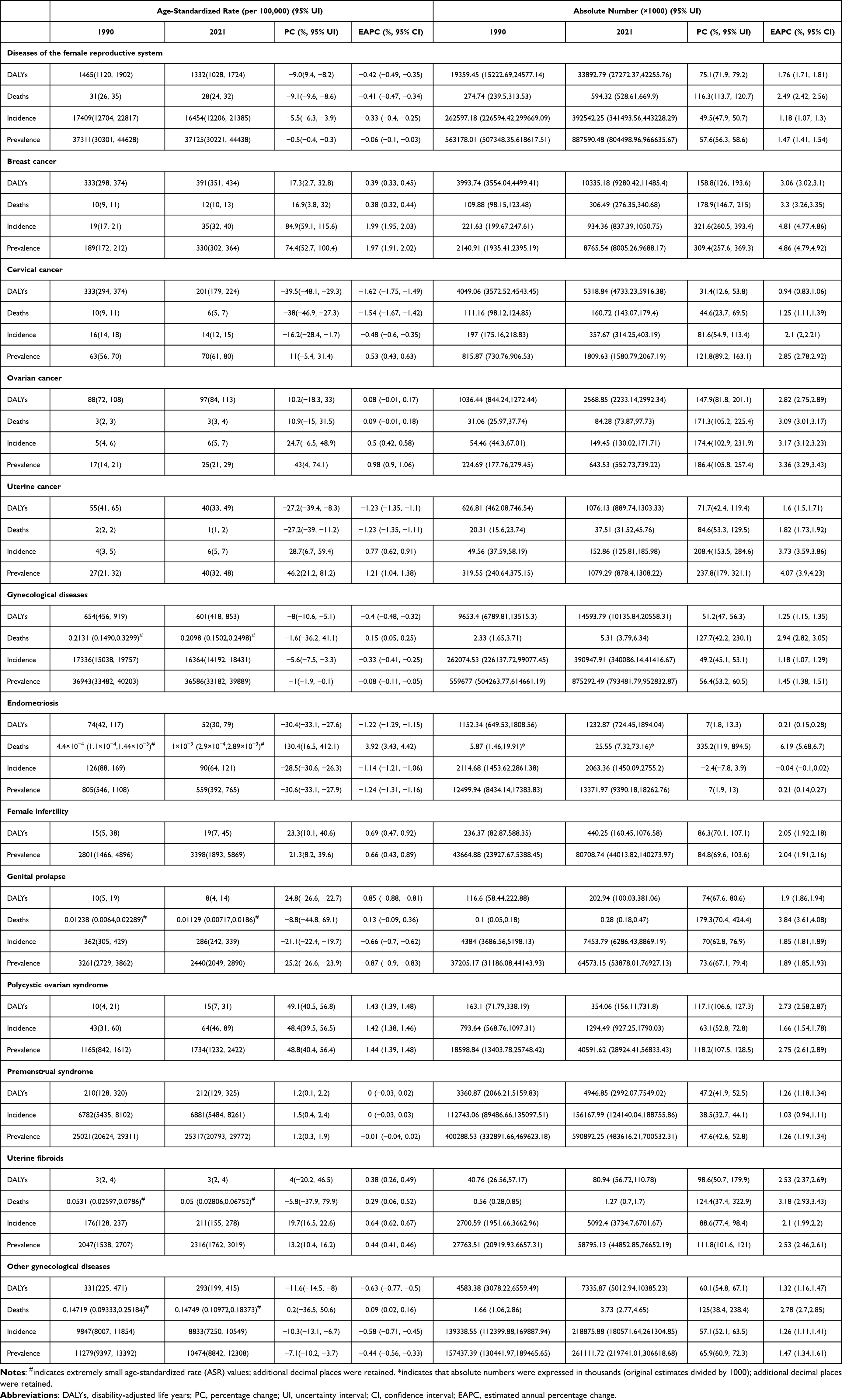 |
Table 1 Age-Standardized Rates (per100,000) and Absolute Number (×1000) of DALYs, Death, Prevalence, and Incidence by Gynecological Disorders Category in Asia, 1990–2021 |
Among the different conditions, the highest numbers of new cases in 2021 were attributed to other gynecological disorders (219 million;95% UI:181–261million), PMS (156 million;95% UI: 124–189million), and uterine fibroids (5 million;95% UI:4–7 million). For prevalence, PMS remained the leading contributor (591 million;95% UI: 484–700 million), followed by other gynecological disorders (261 million;95% UI: 220–307 million) and female infertility (81 million;95% UI: 44–140 million). By contrast, ovarian, uterine, cervical, and breast cancers accounted for relatively fewer cases but contributed disproportionately to mortality. With respect to DALYs, the top three causes were breast cancer (10 million; 95% UI: 9–11 million), other gynecological disorders (7 million;95% UI: 5–10 million), and cervical cancer (5 million; 95% UI: 5–6 million) (Table 1).
In addition, age-specific patterns of prevalence differed from those of DALYs, with the overall number of prevalent cases peaking among women aged 30–44 years, primarily driven by PMS, other gynecological disorders, and female infertility (Figure S1).
Age-Specific Burden of DFRS in Asia
The age distribution of DALYs associated with female reproductive system diseases varied substantially across disease categories, with no cases reported among girls younger than 10 years. Among women aged 10–24 years, PMS was the leading contributor to DALYs, whereas other gynecological disorders predominated among those aged 25–39 years. Beyond the age of 40 years, the DALY burden increased markedly, reflecting growing contributions from both malignant and non-malignant conditions, particularly breast cancer and cervical cancer. The highest DALY rates were observed among women aged 45–59 years. Unlike the overall unimodal distribution of DALYs, breast cancer exhibited a bimodal age pattern, with DALY rates increasing, then decreasing, and rising again at older ages. Endometriosis was mainly concentrated among women aged 15–54 years, while infertility was most prevalent among women aged 20–44 years (Figure 1).
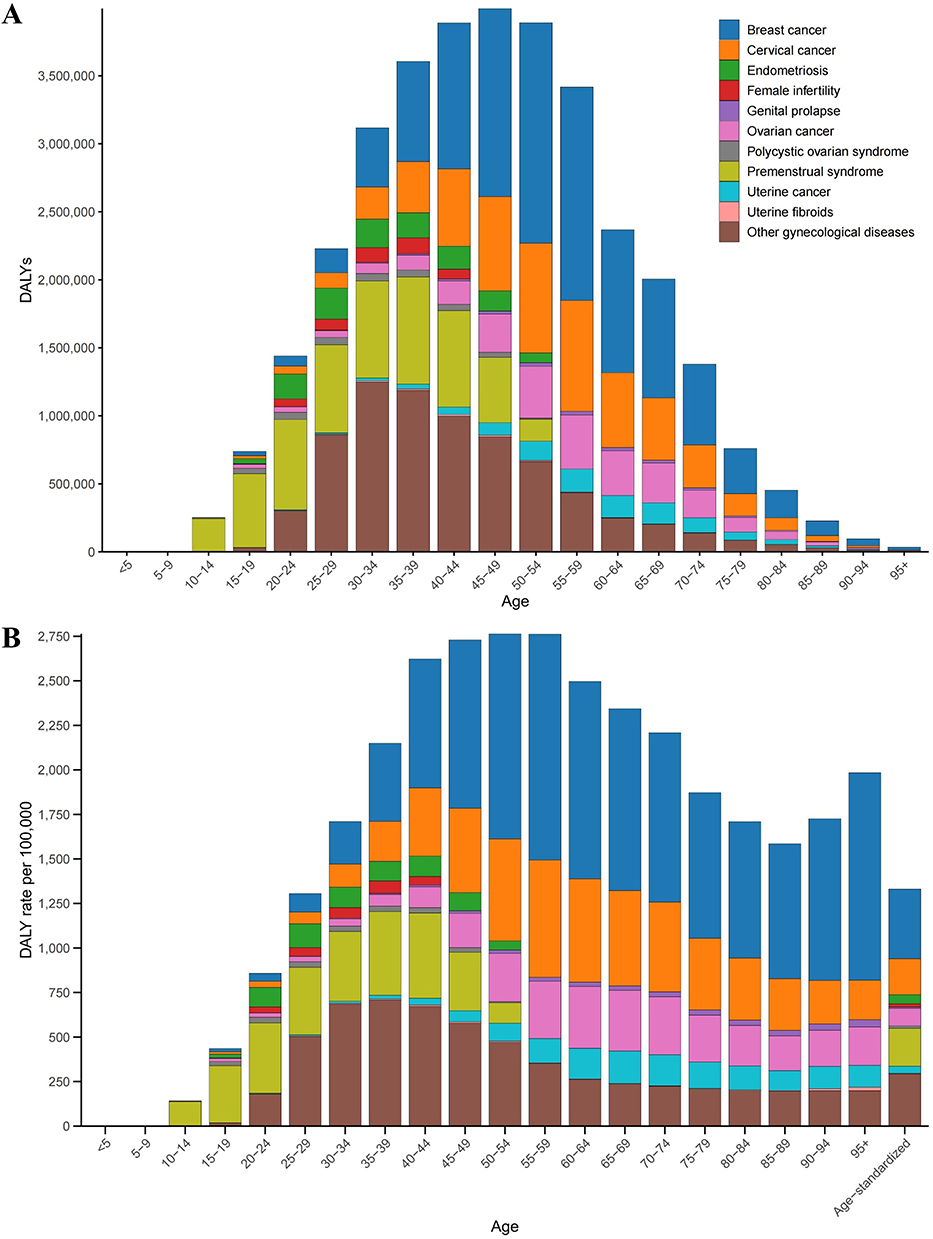 |
Figure 1 Age-specific burden of gynecological diseases. Total DALYs (A) and DALY rates per 100,000 population (B) across age groups. Colors represent breast cancer, cervical cancer, endometriosis, female infertility, genital prolapse, ovarian cancer, polycystic ovarian syndrome, premenstrual syndrome, uterine cancer, uterine fibroids, and other gynecological diseases. Abbreviation: DALY, disability-adjusted life year. |
Geographic Distribution of DFRS in Asia
In 2021, the prevalence and DALY burden of female DFRS varied considerably across Asian regions. The highest numbers of prevalent cases and DALYs were observed in South Asia, followed by East Asia, Southeast Asia, West Asia, and Central Asia. The age-standardized prevalence rate (ASPR) was highest in West Asia, whereas East Asia consistently showed the lowest levels. Similarly, the age-standardized DALY rate (ASDR) was highest in West Asia and lowest in East Asia (Figure 2).
 |
Figure 2 Geographic distribution of gynecological disease burden in Asia. Maps showing four age-standardized indicators across Asian countries: incidence rate (ASIR, (A)), prevalence rate (ASPR, (B)), mortality rate (ASMR, (C)), and DALY rate (ASDR, (D)), each expressed per 100,000 population. Darker shading indicates higher burden. Abbreviations: ASIR, age-standardized incidence rate; ASPR, age-standardized prevalence rate; ASMR, age-standardized mortality rate; ASDR, age-standardized DALY rate. |
At the subregional level, PMS and other gynecological disorders were the dominant contributors to prevalence in most regions, while breast cancer and cervical cancer accounted for the majority of DALYs. At the national level, India, China, and Indonesia bore the greatest absolute burden in terms of prevalence and DALYs, whereas Brunei, Maldives, and Bhutan carried the lowest burden. Several West Asian countries exhibited comparatively high ASDRs despite smaller population sizes. Notably, disease composition varied across countries, with PCOS contributing substantially to ASPR in Japan and cervical cancer accounting for a large share of ASDR in Nepal (Figures 2, 3 and Table S2).
 |
Figure 3 Rankings of gynecological diseases by ASDR and ASPR across Asian countries and territories. (A) Heatmap of rankings based on age-standardized DALY rates (ASDR). (B) Heatmap of rankings based on age-standardized prevalence rates (ASPR). Numbers in each cell represent the rank of a given gynecological condition within a specific country or territory, with color gradients indicating relative position (red = higher rank, blue = lower rank). Abbreviations: ASDR, age-standardized DALY rate; ASPR, age-standardized prevalence rate. |
Temporal Trends in the Burden of DFRS in Asia, 1990–2021
Between 1990 and 2021, the absolute burden of DFRS in Asia increased substantially, with the number of deaths rising by 116.3% (95% UI: 113.7–120.7). However, ASRs generally showed a downward trend. Except for endometriosis, which showed a nonsignificant decrease of 2.4% in incident cases, all other reproductive diseases exhibited increases in absolute numbers, with breast cancer showing the largest growth. In contrast, ASRs declined for most conditions except breast cancer, female infertility, PCOS, and PMS. Some diseases displayed divergent trends across indicators. For example, between 1990 and 2021, uterine cancer showed a 27.2% decline in ASDR and age-standardized mortality rate (ASMR), but its age-standardized incidence rate (ASIR) and ASPR increased by 28.7% and 46.2%, respectively (Table 1).
In terms of pace of change, PCOS-related ASDR rose most rapidly (EAPC = 1.43%, 95% CI: 1.39–1.48), while cervical cancer showed a marked decline (EAPC = –1.62%, 95% CI: –1.75 to –1.49). ASMR trends also differed across diseases. Breast cancer and PCOS showed the fastest growth in ASIR and ASPR, whereas endometriosis demonstrated the sharpest decline. Across Asia’s five subregions, ASDR and ASIR increased slightly in West Asia but decreased in the other four subregions, with East Asia showing the steepest decline. ASPR in West Asia remained essentially stable throughout the 32-year period (EAPC = 0.00, 95% CI: –0.01 to 0.01) (Tables 1, S3 and S4).
Distribution of DFRS in Asia Burden Across SDI Levels
In 2021, the burden of female reproductive system diseases in Asia demonstrated clear variation across SDI levels. (Figure 4) Overall, ASMR declined with increasing SDI, whereas ASIR and ASPR were elevated in both low- and high-SDI settings. ASDR did not show a consistent gradient across SDI levels.
 |
Figure 4 Association between SDI and gynecological disease burden in Asia. Scatter plots showing the relationship between SDI and four age-standardized indicators: incidence rate (ASIR, (A)), prevalence rate (ASPR, (B)), mortality rate (ASMR, (C)), and DALY rate (ASDR, (D)), per 100,000 population. Each dot represents a country, with fitted curves illustrating the overall trend. Abbreviations: SDI, Socio-demographic Index; ASIR, age-standardized incidence rate; ASPR, age-standardized prevalence rate; ASMR, age-standardized mortality rate; ASDR, age-standardized DALY rate. |
At the country level, low-SDI countries such as Afghanistan and Yemen exhibited high ASIR, ASPR, ASMR, and ASDR. Middle-SDI countries presented a comparatively lower overall burden across all indicators. Among high-SDI countries, Japan, South Korea, and Singapore showed elevated ASIR and ASPR, while their ASMR and ASDR were substantially lower than those in low-SDI countries. The United Arab Emirates, despite its high SDI level, recorded unusually high ASMR and ASDR compared with other high-SDI countries (Figure 4).
Risk Factors for DFRS in Asia, 2021
For breast cancer, high red meat intake accounted for the largest proportion of the ASDR (10.5%), followed by elevated fasting plasma glucose (3.8%), high BMI (3.4%), low physical activity (1.9%), second-hand smoke exposure (1.7%), alcohol consumption (1.1%), and active smoking (0.8%). For cervical cancer, smoking accounted for 5.2% of the ASDR. In uterine cancer, high BMI accounted for 25.1% of the ASDR, whereas in ovarian cancer, high BMI and occupational asbestos exposure accounted for 6.0% and 0.7% of the ASDR, respectively.
At the national level, the proportion of breast cancer ASDR attributable to red meat intake was lower than the Asian average in Bangladesh (6.2%), Bhutan (10.2%), India (4.9%), Indonesia (9.4%), Iraq (9.9%), Maldives (8.6%), and Sri Lanka (4.8%). In contrast, several West Asian countries, including Jordan, Kuwait, Yemen, and the United Arab Emirates, showed a relatively higher proportion of breast cancer ASDR attributable to high BMI. Alcohol consumption accounted for a comparatively higher proportion of breast cancer ASDR in Japan (7.9%) and South Korea (6.0%).
For cervical cancer, smoking accounted for a particularly high proportion of ASDR in Israel (18.7%) and Lebanon (27.1%). In Jordan, Kuwait, Qatar, and Saudi Arabia, high BMI represented the largest proportion of ASDR for both uterine and ovarian cancers. In Armenia (5.6%) and Turkey (3.9%), occupational asbestos exposure accounted for a relatively higher proportion of ovarian cancer ASDR (Figure 5).
 |
Figure 5 Contribution of risk factors to the burden of gynecological cancers in Asia. Heatmaps show the proportion of disease burden attributable to major risk factors for (A) breast cancer, (B) cervical cancer, (C) ovarian cancer, and (D) uterine cancer across countries and territories. Color intensity indicates the relative magnitude of risk factor contribution, with darker red representing higher values. |
Discussion
This study, using GBD 2021 estimates, assessed the long-term trends of female reproductive system diseases in Asia. Despite progress in prevention and treatment, these conditions continue to exert a substantial public health impact, affecting nearly 40% of women and contributing significantly to mortality and DALYs.7 Breast and cervical cancers remain the leading causes of death and disability.27 In contrast, disorders such as PMS,28 infertility,29 and other gynecological conditions account for most cases. Non-neoplastic diseases rarely threaten survival, yet they profoundly influence fertility, psychological health, and daily life.2 Their burden, however, has historically received limited attention in policy and funding decisions. Particularly concerning is the rapid rise of infertility and PCOS, a trend echoed in other epidemiological studies, pointing to their growing role as public health priorities.
Marked regional heterogeneity in the burden of female reproductive system diseases across Asia reflects the combined influence of demographic transitions, health system capacity, sociocultural factors, and lifestyle patterns. In South Asia, the absolute number of cases is the highest, not only due to its large population base but also because of insufficient public health coverage, limited allocation of women’s health resources, and underdeveloped screening systems, which delay timely detection and intervention.30 West Asia records the highest ASPR and DALYs, largely attributable to the high prevalence of obesity and metabolic disorders; restrictions on women’s physical activity imposed by sociocultural norms further exacerbate these risks.31,32 In contrast, East Asia demonstrates comparatively lower standardized rates, reflecting the effectiveness of long-standing cervical cancer screening and HPV vaccination programs supported by relatively robust health systems.33–35 However, Japan and South Korea show disproportionately high burdens of infertility and PCOS,36,37 likely explained by widespread postponement of childbearing, higher average maternal age, and the availability of advanced diagnostic practices and assisted reproductive technologies that increase case detection.38 Southeast Asia faces the dual challenge of malignant and non-neoplastic diseases, driven by economic disparities and persistent gaps in health service delivery between urban and rural populations.39,40 At the national level, Nepal stands out with a disproportionately high burden of cervical cancer, largely reflecting inadequate screening, low HPV vaccine coverage, and limited health system resources.41,42 Although nationwide HPV vaccination has recently been initiated with partial progress, historical deficits and fluctuating financial and logistical capacity continue to shape the short-term burden profile.43
The temporal trends reveal both progress and new concerns. While absolute case numbers and deaths have risen steadily, particularly for breast cancer, infertility and PCOS, the overall age-standardized rates have declined. Population growth and aging largely explain this paradox and offset improvements from prevention programs.44 The persistent decline in cervical cancer highlights the success of HPV vaccination and screening efforts.45 By contrast, the rapid increase in infertility and PCOS underscores gaps in prevention and long-term care. Regionally, East Asia has shown the most consistent reductions, whereas West Asia has remained stable or worsened, reinforcing the association between health system strength and population outcomes.46 Taken together, these findings indicate that incremental measures are no longer sufficient. Broader strategies are needed, including expansion of cancer screening and vaccination programs, integration of infertility and PCOS into public health priorities, and stronger primary healthcare systems. For aging populations, developing long-term management pathways that link reproductive and chronic disease care will be especially important.47
Risk factor analysis offers further guidance for prevention. Breast cancer risk is shaped by high red meat intake, elevated BMI, and raised fasting glucose. Cervical cancer remains closely tied to unsafe sexual practices and smoking.48 Uterine and ovarian cancers, in turn, are strongly linked to obesity. Rising BMI, now a central driver in West Asia and several high-income countries,49 reflects broader dietary and lifestyle transitions, as well as limited opportunities for women to engage in physical activity.50 In Japan and South Korea, alcohol contributes significantly to breast cancer burden, consistent with changing social norms and increased alcohol consumption among women.51,52 These findings emphasize the need for strategies tailored to local realities rather than uniform regional approaches. Promoting weight management and physical activity should be prioritized in West Asia, while in East Asia, alcohol control and public education are more pressing. South and Southeast Asia, meanwhile, would benefit most from scaling up HPV vaccination, tobacco control, and sexual health education.
From a policy standpoint, resources should be more evenly distributed between malignant and non-malignant gynecological diseases. Breast and cervical cancers have historically received greater attention because of their lethality,53,54 whereas conditions such as infertility, PCOS, and PMS remain insufficiently prioritized. Although these disorders do not directly threaten survival, their effects on fertility, psychological health, and quality of life are considerable,52 and their economic and social consequences justify stronger policy responses. Strengthening primary healthcare is a critical step,55 with community-level services playing a central role in early screening, health education, and timely intervention, while access to diagnostic and treatment services must be extended to rural and disadvantaged populations.56,57 Developing tiered healthcare systems could also relieve the overconcentration of high-quality resources in large urban centers and improve equity of access. At the same time, addressing modifiable risk factors such as obesity, smoking, and alcohol use requires coordinated action across multiple sectors, including education, agriculture, and food policy, with measures ranging from the promotion of healthy diets and regular physical activity to adolescent-focused programs on tobacco and alcohol prevention.58 Regional and cross-national cooperation will further enhance prevention and control by supporting shared databases, multinational studies, and the exchange of experience in screening and vaccination, thereby helping to narrow disparities between countries.59–61 Ultimately, policies should move beyond narrow disease-centered approaches toward integrated strategies that link gynecological disease management with chronic disease care and mental health support,62 as such comprehensive measures will be crucial for reducing the long-term burden of reproductive system diseases and improving women’s health outcomes across Asia. However, this study has several limitations. First, although GBD 2021 provides standardized and comparable estimates, the results rely on modeling assumptions and data synthesis procedures that may introduce uncertainty, particularly in settings with sparse data. Second, limitations in national disease registries and surveillance systems in some Asian countries may lead to underreporting and greater reliance on modeled estimates. Third, certain non-malignant gynecological conditions may be underestimated due to non-standardized diagnostic criteria and incomplete reporting. Finally, this analysis focused on major risk factors within the GBD framework and did not account for comorbidities or psychosocial influences.
Conclusion
The findings highlight the substantial burden and mark regional disparities of reproductive system tumors and non-tumor diseases among Asian women from 1990 to 2021. Malignant cancers remain the leading causes of death and disability, while non-neoplastic conditions such as infertility and polycystic ovary syndrome showed the most notable increasing trends and substantially affected quality of life. Policy responses should balance attention to both cancerous and non-cancerous diseases. In lower SDI settings, priorities include improving access to basic health services, early detection, and vaccination programs. In higher SDI settings, prevention strategies targeting modifiable metabolic and lifestyle risk factors, as well as better management of chronic non-malignant conditions, are warranted to reduce the overall burden and improve women’s health outcomes.
Abbreviations
APC, age-period-cohort; ASDR, age-standardized DALYs rate; ASIR, age-standardized incidence rate; ASMR, age-standardized mortality rate; ASPR, age-standardized prevalence rate; ASR, age-standardized rates; BMI, body mass index; CI, confidence interval; DALYs, disability-adjusted life years; DFRS, Distribution of the Burden of Female Reproductive System Diseases; EAPC, estimated annual percentage change; GBD, global burden of disease; PCOS, polycystic ovary syndrome; PMS, premenstrual syndrome; UIs, uncertainty intervals; WHO, World Health Organization.
Data Sharing Statement
The data utilized in this study can be accessed from the GBD 2021 (Available at: https://vizhub.healthdata.org/gbd-results/).
Ethics Declarations
This study was based on publicly available, anonymized, and aggregated data from the GBD 2021 database and did not involve identifiable individual-level information. According to the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects of the People’s Republic of China, such studies are exempt from ethical review. The Ethics Committee of Xiangya Hospital, Central South University confirmed that ethical approval and informed consent were not required.
Consent for Publication
All authors have read and approved the final manuscript and consent to its publication.
Acknowledgments
We acknowledge the Institute for Health Metrics and Evaluation (IHME) for providing access to the Global Burden of Disease Study 2021 data used in this analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Cao Y, Guo Y, Long Z, et al. The global burden of gynecological diseases from 1990 to 2019. Am J Prev Med. 2024;67(5):698–17. doi:10.1016/j.amepre.2024.06.022
2. Gu D, Qi M, Gui R, et al. Global burden of non-neoplastic gynecological diseases in women: a 32-year analysis with projections to 2100. Am J Prev Med;2025. 108099. doi:10.1016/j.amepre.2025.108099
3. Liu J, Qin Y, Liu H, et al. Global, regional, and national burden of female infertility and trends from 1990 to 2021 with projections to 2050 based on the GBD 2021 analysis. Sci Rep. 2025;15(1):17559. doi:10.1038/s41598-025-01498-x
4. Don EE, Mijatovic V, Huirne JAF. Infertility in patients with uterine fibroids: a debate about the hypothetical mechanisms. Hum Reprod. 2023;38(11):2045–2054. doi:10.1093/humrep/dead194
5. Wijeratne D, Gibson JFE, Fiander A, Rafii-Tabar E, Thakar R. The global burden of disease due to benign gynecological conditions: a call to action. Int J Gynaecol Obstet. 2024;164(3):1151–1159. doi:10.1002/ijgo.15211
6. Liu Y, Shi W, Mubarik S, Wang F. Assessment of secular trends of three major gynecologic cancers burden and attributable risk factors from 1990 to 2019: an age period cohort analysis. BMC Public Health. 2024;24(1):1349. doi:10.1186/s12889-024-18858-3
7. Gao Y, Wang X, Wang Q, et al. Rising global burden of common gynecological diseases in women of childbearing age from 1990 to 2021: an update from the global burden of disease study 2021. Reprod Health. 2025;22(1):57. doi:10.1186/s12978-025-02013-1
8. Ferrari AJ, Santomauro DF, Aali A, et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
9. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
10. Bhattacharjee NV, Schumacher AE, Aali A, et al. Global fertility in 204 countries and territories, 1950–2021, with forecasts to 2100: a comprehensive demographic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2057–2099. doi:10.1016/S0140-6736(24)00550-6
11. Chai O, Feng X, Tang N, et al. Global and regional burden of polycystic ovary syndrome, 1990–2021: a systematic analysis of the global burden of disease study 2021. BMC Womens Health. 2025;25(1):437. doi:10.1186/s12905-025-03976-w
12. Yin B, Zhou H. Burden and trends of ovarian and uterine cancer due to high body mass index from 1990 to 2021: an age-period-cohort study based on the GBD 2021, and projections through 2036. Front Oncol. 2025;15:1647757. doi:10.3389/fonc.2025.1647757
13. Zhang Z, Huang H, Jiang K, Liu W, Xuan Y, Lu W. Global, regional and national uterine fibroid burdens from 1990 to 2021 and projections until 2050: results from the GBD study. BMC Womens Health. 2025;25(1):423. doi:10.1186/s12905-025-03974-y
14. Huang M, Guan M, Rao Q, et al. Long-term trends and projections of ovarian cancer burden in China (1990 to 2040): an age-period-cohort analysis based on GBD 2021 data. Front Oncol. 2025;15:1652347. doi:10.3389/fonc.2025.1652347
15. Division UP. World population prospects. 2022. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL.FE.ZS.
16. Youlden DR, Cramb SM, Yip CH, Baade PD. Incidence and mortality of female breast cancer in the Asia-Pacific region. Cancer Biol Med. 2014;11(2):101–115. doi:10.7497/j.issn.2095-3941.2014.02.005
17. Sha R, Kong XM, Li XY, Wang YB. Global burden of breast cancer and attributable risk factors in 204 countries and territories, from 1990 to 2021: results from the global burden of disease study 2021. Biomark Res. 2024;12(1):87. doi:10.1186/s40364-024-00631-8
18. Yang M, Xuan F, Wang L, Lou Y, Yu S. Spatial patterns and temporal trends of tracheal, bronchus, and lung cancer attributed to particulate matter pollution in Asia and its 34 countries and territories, 1990–2021. Front Public Health. 2025;13:1602454. doi:10.3389/fpubh.2025.1602454
19. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
20. Fay MP, Feuer EJ. Confidence intervals for directly standardized rates: a method based o n the gamma distribution. Stat Med. 1997;16(7):791–801.
21. Brauer M, Roth GA, Aravkin AY, et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024;403(10440):2162–2203.
22. Ferrari AJ, Santomauro DF, Aali A, et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. The Lancet. 2024;403(10440):2133–2161.
23. Selvin S. Statistical Analysis of Epidemiologic Data. Vol. 35. Oxford University Press; 2004.
24. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2024;74(3):229–263. doi:10.3322/caac.21834
25. Vos T, Lim SS, Abbafati C, etal. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
26. Yu J, Yang X, He W, Ye W. Burden of pancreatic cancer along with attributable risk factors in Eu rope between 1990 and 2019, and projections until 2039. Int J Cancer. 2021;149(5):993–1001. doi:10.1002/ijc.33617
27. Force LM, Kocarnik JM, May ML, et al. The global, regional, and national burden of cancer, 1990–2023, with forecasts to 2050: a systematic analysis for the global burden of disease study 2023. Lancet. 2025;406:1565–86.
28. Liu X, Li R, Wang S, Zhang J. Global, regional, and national burden of premenstrual syndrome, 1990–2019: an analysis based on the global burden of disease study 2019. Hum Reprod. 2024;39(6):1303–1315. doi:10.1093/humrep/deae081
29. Cheng X, Ma J, Wang W, et al. Global, regional, and national burden and trend of infertility and its subtypes from 1990 to 2021, with projections to 2035. J Assist Reprod Genet. 2025;42(10):3409–3428. doi:10.1007/s10815-025-03592-5
30. Sun J, Zhu Y, Huang D, et al. Burden of female diseases among adolescents and young adults aged 10–24 years in South Asia and Sub-Saharan Africa, 1990–2021: a systematic analysis from the global burden of disease study 2021. J Adv Res. 2025. doi:10.1016/j.jare.2025.05.048
31. Sharara E, Akik C, Ghattas H, Makhlouf Obermeyer C. Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC Public Health. 2018;18(1):639. doi:10.1186/s12889-018-5472-z
32. Chaabane S, Chaabna K, Abraham A, Mamtani R, Cheema S. Physical activity and sedentary behaviour in the Middle East and North Africa: an overview of systematic reviews and meta-analysis. Sci Rep. 2020;10(1):9363. doi:10.1038/s41598-020-66163-x
33. Yagi A, Ueda Y, Kakuda M, et al. Cervical cancer protection in Japan: where are we? Vaccines. 2021;9(11):1263. doi:10.3390/vaccines9111263
34. Chen Q, Wang S, Lin Q, Zhang G. Temporal changes in prevalence and geographical distribution of human papillomavirus infection in mainland China: a systematic review and analysis of 1.07 million females from 2010 to 2021. BMC Public Health. 2025;25(1):3083. doi:10.1186/s12889-025-24323-6
35. Prem K, Cernuschi T, Malvolti S, Brisson M, Jit M. Optimal human papillomavirus vaccination strategies in the context of vaccine supply constraints in 100 countries. EClinicalMedicine. 2024;74:102735. doi:10.1016/j.eclinm.2024.102735
36. Sun F, Wang W, Ding G, et al. Disease burden of infertility in five East Asian countries from 1990 to 2021 and prediction for 2050: an analysis of the global burden of disease study 2021. PLoS One. 2025;20(9):e0331617. doi:10.1371/journal.pone.0331617
37. Chen Q, Zhao J, Wu X, Xie X, Liu M. Temporal trends of polycystic ovary syndrome burden in the East and Southeast Asia from 1990 to 2021: an analysis from the global burden of disease study 2021. Int J Womens Health. 2025;17:2097–2108. doi:10.2147/IJWH.S523350
38. Kim JH, Jung MH, Hong SH, Moon N, Kang DR. Age-adjusted prevalence and characteristics of women with polycystic ovarian syndrome in Korea: a nationwide population-based study (2010–2019). Yonsei Med J. 2022;63(8):794–798. doi:10.3349/ymj.2022.63.8.794
39. Yang Y, Miao R, He H, et al. The burden and trends of gynecological cancers in Asia from 1980 to 2021, with projections to 2050: a systematic analysis for the global burden of disease study 2021. Curr Oncol. 2025;32(6):298. doi:10.3390/curroncol32060298
40. Sisubalan N, Sivamaruthi BS, Kesika P, Chaiyasut C. Addressing health inequities in Southeast Asia: challenges and opportunities. Lancet Reg Health Southeast Asia. 2024;28:100455. doi:10.1016/j.lansea.2024.100455
41. Narasimhamurthy M, Kafle SU. Cervical cancer in Nepal: current screening strategies and challenges. Front Public Health. 2022;10:980899. doi:10.3389/fpubh.2022.980899
42. Dangal G, Dhital R, Dwa YP, Poudel S, Pariyar J, Subedi K. Implementation of cervical cancer prevention and screening across five tertiary hospitals in Nepal and its policy implications: a mixed-methods study. PLOS Glob Public Health. 2024;4(1):e0002832. doi:10.1371/journal.pgph.0002832
43. Paudel P. Human papillomavirus vaccine: a welcome addition to the national immunisation schedule in Nepal. BMJ Glob Health. 2025;10(3).
44. Xi JY, Liang BH, Zhang WJ, et al. Effects of population aging on quality of life and disease burden: a population-based study. Glob Health Res Policy. 2025;10(1):2. doi:10.1186/s41256-024-00393-8
45. Zeitouni J, Osazuwa-Peters N, Dundar Y, Zimet G, Varvares MA. Two decades of the HPV vaccine: its promise, progress, prospects, projections, and posterity. Lancet Reg Health Am. 2025;51:101243. doi:10.1016/j.lana.2025.101243
46. Huo M, Wang Y, Yuan X, Yuan Y, Zhang X. Changing trends in the global burden of polycystic ovarian syndrome-related infertility over the past 30 years: retrospective data analysis of the global burden of disease study 2019. BMC Womens Health. 2025;25(1):35. doi:10.1186/s12905-024-03537-7
47. World Health Organization. Primary health care. Available from: https://www.who.int/news-room/fact-sheets/detail/primary-health-care?utm_source=chatgpt.com.
48. Islami F, Marlow EC, Thomson B, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States, 2019. CA Cancer J Clin. 2024;74(5):405–432. doi:10.3322/caac.21858
49. Xie F, Xiong F, Yang B, et al. Global, regional, and national burden of mortality and DALYs attributable to high body mass index from 1990 to 2021 with projections to 2036. BMC Public Health. 2025;25(1):2053. doi:10.1186/s12889-025-23237-7
50. Hyde ET, Bandoli GE, Zou J, et al. Prospective associations between accelerometer-measured physical activity, sedentary behavior, and healthy longevity: the women’s health accelerometry collaboration. J Gerontol a Biol Sci Med Sci. 2025;80(12). doi:10.1093/gerona/glaf206
51. Jung KJ, Lee K, Song DS, et al. Alcohol consumption and cancer risk in South Korea and the UK: prospective cohort studies. Int J Epidemiol. 2025;54(4). doi:10.1093/ije/dyaf108
52. Satoh M, Sato N, Sekino M. Behavioral economics, lifestyle, and health-related factors associated with participation in breast and cervical cancer screenings: a cross-sectional analysis of Japanese women. Prev Med Rep. 2025;59:103249. doi:10.1016/j.pmedr.2025.103249
53. World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. 2020. Available from: https://www.who.int/news/item/17-11-2020-a-cervical-cancer-free-future-first-ever-global-commitment-to-eliminate-a-cancer?utm_source=chatgpt.com.
54. World Health Organization. The Global Breast Cancer Initiative. 2022. Available from: https://cdn.who.int/media/docs/default-source/documents/health-topics/cancer/the-global-breast-cancer-initiative-flyer-june-2022.pdf?sfvrsn=c4756174_3&download=true.
55. Ibrahim N, Da Silva RB, Agyepong AI, Novignon J, Ensor T. Health facility capacity and technical efficiency in the provision of adolescent sexual and reproductive health services in Niger. BMC Public Health. 2025;25(1):3200. doi:10.1186/s12889-025-24442-0
56. Chan M. Primary health care as a route to health security. Lancet. 2009;373(9675):1586–1587. doi:10.1016/S0140-6736(09)60003-9
57. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
58. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384(9945):766–781. doi:10.1016/S0140-6736(14)60460-8
59. Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P. WHO European review of social determinants of health and the health divide. Lancet. 2012;380(9846):1011–1029. doi:10.1016/S0140-6736(12)61228-8
60. World Health Organization. Global status report on alcohol and health 2018. 2018. Available from: https://iris.who.int/server/api/core/bitstreams/9530de1c-1fd2-4c20-a167-ec6ba7cb00c3/content.
61. World Health Organization. Who report on the global tobacco epidemic, 2021. 2021. Available from: https://iris.who.int/server/api/core/bitstreams/d6747635-8c77-431e-9554-b3a2cd4d21a1/content.
62. Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018;392(10157):1553–1598. doi:10.1016/S0140-6736(18)31612-X
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.