Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Bullous Pilomatricoma After Influenza Vaccination
Authors Zhang H ![]() , Jin J, Chen X, Cai L, Zhang J, Wen G
, Jin J, Chen X, Cai L, Zhang J, Wen G
Received 5 March 2022
Accepted for publication 7 April 2022
Published 13 April 2022 Volume 2022:15 Pages 657—660
DOI https://doi.org/10.2147/CCID.S364850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Heng Zhang, Jiang Jin, Xue Chen, Lin Cai, Jianzhong Zhang, Guangdong Wen
Department of Dermatology, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China
Correspondence: Guangdong Wen, Department of Dermatology, Peking University People’s Hospital, # 11. Xizhimen South St, Beijing, 100044, People’s Republic of China, Tel +86 10 88325472, Fax +86 10 88325474, Email [email protected]
Abstract: Pilomatricoma, also known as “benign calcifying epithelioma”, is an uncommon slow-growing benign adnexal skin tumor, which originates from primitive cells of the hair matrix and usually appears as a solitary, firm, and asymptomatic nodule beneath the skin. Bullous pilomatricoma is a rare form of pilomatricoma, always presenting with firm subcutaneous nodules with a bullous appearance. In this study, we report a 9-year-old Chinese presenting girl with bullous pilomatricoma after influenza vaccination.
Keywords: bullous pilomatricoma, calcifying epithelioma of Malherbe, influenza vaccination
Introduction
Pilomatricoma is a benign skin neoplasm that arises from hair follicle matrix cells. It usually occurs on the head, neck, and upper extremities. The etiology of pilomatricoma is unknown. Trauma, insect bites, or surgery are thought to be antecedent events to the onset of the tumors.1 Pilomatricoma has other rare variants such as multiple pilomatricoma,2 perforating pilomatricoma,3 and bullous pilomatricoma.4 Bullous pilomatricoma is a very rare form of pilomatricoma with a prevalence of 3%-6%.4
Influenza vaccination is extremely common, with many patients receiving the vaccine on an annual basis. Complications are usually mild and self-limiting. Here we described a case of bullous pilomatricoma arising after influenza vaccination. Although there has been a report about an association between bullous pilomatricoma and hepatitis A vaccination,5 an association with influenza vaccination has not been reported previously.
Case Report
A 9-year-old girl presented with a solitary nodule on her left upper arm. Nine months ago, she received her routine influenza vaccination in the left upper arm. A soy-bean size nodule developed on the vaccination site without any symptoms. The nodule enlarged gradually, and a bullous appearance was detected one month earlier. The patient did not have any family history of such or mechanical trauma. Dermatological examination revealed a pink-colored, 1.0 cm × 0.5 cm-sized, thick-walled, and semi-translucent blister on the extensor aspect of the left upper arm. A 1.5 cm × 1 cm-sized and well-demarcated firm nodule was detected underneath the blister (Figure 1). An incisional biopsy was performed. Histopathology showed a marked lymphoedema and increased numbers of dilated lymphatics filled with eosinophilic lymph fluid in the superficial dermis and the deep dermis. The tumor nests were composed of eosinophilic shadow cells and basophilic cells surrounded by a fibrous capsule (Figure 2). Based on these findings, the lesion was diagnosed as a “bullous pilomatricoma.”
 |
Figure 1 A pink-colored, 1.0 cm × 0.5 cm-sized, thick-walled, and semi-translucent blister on the extensor aspect of the left upper arm. A 1.5 cm × 1 cm-sized and well-demarcated firm nodule was detected underneath the blister. |
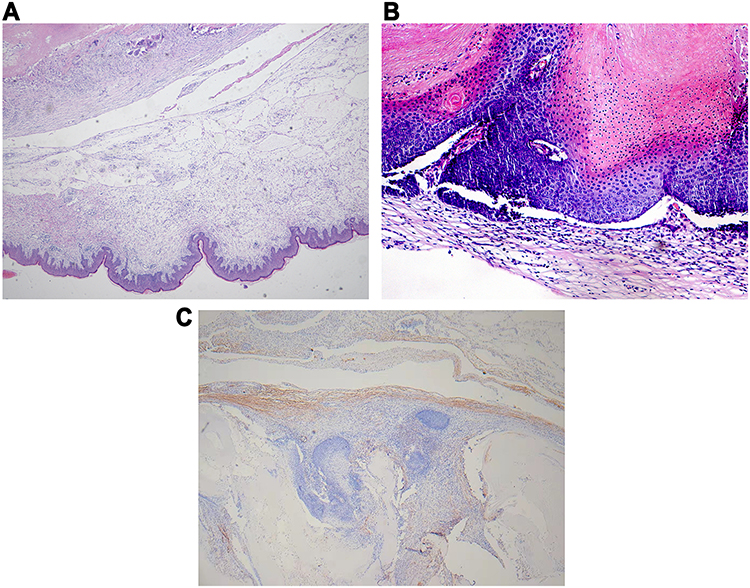 |
Figure 2 The histopathology of the skin lesions showed expanded lymphatic vessels and lymph fluid in the dermis (40×, A), tumor masses composed of eosinophilic shadow cells and basophils were seen (200×, B) and positive D2-40 (200×, C). |
Discussion
Pilomatricoma, also known as calcifying epithelioma of Malherbe, is a benign calcifying tumor that arises from the hair matrix and presents as a slow-growing dermal or subcutaneous mass.6 Pilomatricoma mainly occurs in children and adolescents. Another small onset peak is between the ages of 50 and 70 years.7 Pilomatricoma has other rare variants such as multiple pilomatricoma,2 perforating pilomatricoma,3 and bullous pilomatricoma.4 The subtypes are usually defined by clinical features, the multiple pilomatricoma always presents with 2 or more lesions; the perforating pilomatricoma is characterized by the process of tumor cells perforating the epidermis; the bullous pilomatricoma always presents with firm subcutaneous nodules with a bullous appearance.
Bullous pilomatricoma is rare, and its incidence is between 3% and 6%.4 Although pilomatricoma can be associated with other disorders such as Steinert disease, Gardner syndrome, Turner syndrome, Sotos syndrome, 21 Rubinstein-Taybi syndrome, medullary thyroid carcinoma, and sarcoidosis,1 the bullous variant has not been associated with these disorders. The bullous lesions are located primarily on the shoulder and upper extremity.8 Clinical characteristics reported include semi-transparent, erythematous, bluish or skin-colored, heavily folded or striae-like, flaccid blisters overlying a solitary, firm-to-hard nodule.8,9
Theories have been proposed to explain the bullous appearance seen on pilomatricoma. The prominent bullous appearance is attributed to lymphatic obstruction, which results in dilating lymphatic vessels, the leakage of lymphatic fluid, and edema in the dermis surrounding the tumor.10 Another theory suggests that the tumor cells or infiltrating inflammatory cells can produce elastolytic enzymes, which disrupt collagen fibers, destruct and dilate lymphatic vessels; hence, the dermis is filled with lymph fluid and the bullous appearance is formed.10,11 Tumors found in vaccination sites could be induced by trauma, persistent inflammation, or the inoculated attenuated agent itself.12,13
Histopathologically, eosinophilic shadow cells, basophilic cells, foreign body cells, calcified focus, or even ossification can be seen.1 In a perforating pilomatricoma, the unique features of tumor mass extruded to the skin surface through the perforated epidermal channel can be found.3 In a bullous pilomatricoma, in addition to these findings, lymphoedema and dilated lymphatic vessels in the superficial dermis can be found in most cases.5,8 These lymphatic findings have been described as standard pathologic features.
Pilomatricoma is still frequently misdiagnosed. Ultrasound is a valuable diagnostic tool in pilomatricoma.14 One study showed that the rate of preoperative diagnostic accuracy is less than 49%.12 Pilomatricoma is difficult to diagnose because of its varying morphology and unusual appearance. Furthermore, as vaccination-induced pilomatricoma is a rare event, differential diagnosis under such settings can be more difficult. Therefore, histopathologic examinations are required for its final diagnosis.
Bullous Pilomatricoma does not regress spontaneously, and surgical excision is the treatment of choice because recurrence is rare. The limitation of our study was that the patient did not have an ultrasound. A major limitation of this study is the lack of ultrasound finding, as that was not routinely performed in all the patients.
Conclusion
Bullous pilomatricoma, although rare, has been reported worldwide. Clinicians should be aware that bullous pilomatricoma may occur after vaccination. The prominent bullous appearance is probably attributed to lymphatic obstruction or elastolytic enzymes, however, the exact mechanism needs further study. Ultrasound, as a noninvasive examination, is a valuable diagnostic tool in pilomatricoma, but the final diagnosis and treatment requires surgical resection.
Ethics and Consent Statements
Written informed consent was provided by the parent of the patient to have the case details and any accompanying images published. Institutional approval was not required to publish the case details.
Funding
National Natural Science Foundation of China (81402588).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hernández-Núñez A, Nájera Botello L, Romero Maté A, et al. Retrospective study of pilomatricoma: 261 tumors in 239 patients. Actas Dermosifiliogr. 2014;105(7):699–705. doi:10.1016/j.ad.2014.01.003
2. King I, Rahman K, Henderson A, Ragbir M. Multiple familial pilomatrixomas in three generations: an unusual clinical picture. Pediatr Dermatol. 2015;32(1):97–101. doi:10.1111/pde.12353
3. Watabe D, Mori S, Akasaka T, Motegi S, Ishikawa O, Amano H. Six cases of perforating pilomatricoma: anetodermic changes with expression of matrix metalloproteinases. J Dermatol. 2020;47(1):82–85. doi:10.1111/1346-8138.15138
4. de Giorgi V, Alfaioli B, Massi D, et al. Bullous pilomatricoma: a particular and rare dermal bullous disorder. Acta Derm Venereol. 2009;89(2):189–190. doi:10.2340/00015555-0442
5. Tas B, Tas E, Sar M. A bullous pilomatricoma developed after Hepatitis A vaccination. West Indian Med J. 2015;64(2):166–167. doi:10.7727/wimj.2013.304
6. Jeon H, Jeong S, Dhong E, Han S. Pilomatricoma arising at an influenza vaccination site. Arch Plast Surg. 2014;41(6):775–777. doi:10.5999/aps.2014.41.6.775
7. Lan M, Lan M, Ho C, Li W, Lin C. Pilomatricoma of the head and neck: a retrospective review of 179 cases. Arch Otolaryngol–Head Neck Surg. 2003;129(12):1327–1330. doi:10.1001/archotol.129.12.1327
8. Chen S, Wu F, Qian Y, Zhu L, Tu Y, Huang C. Pilomatricoma with bullous appearance: a case report and review of literature. Int J Dermatol. 2011;50(5):615–618. doi:10.1111/j.1365-4632.2010.04586.x
9. Bhushan P, Hussain S. Bullous pilomatricoma: a stage in transition to secondary anetoderma? Indian J Dermatol Venereol Leprol. 2012;78(4):484–487. doi:10.4103/0378-6323.98081
10. Fetil E, Soyal M, Menderes A, Lebe B, Güneş A, Ozkan S. Bullous appearance of pilomatricoma. Dermatol surg. 2003;29(10):1066–1067. doi:10.1046/j.1524-4725.2003.29304.x
11. Inui S, Kanda R, Hata S. Pilomatricoma with a bullous appearance. J Dermatol. 1997;24(1):57–59. doi:10.1111/j.1346-8138.1997.tb02741.x
12. Pirouzmanesh A, Reinisch J, Gonzalez-Gomez I, Smith E, Meara J. Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg. 2003;112(7):1784–1789. doi:10.1097/01.PRS.0000091160.54278.64
13. Malpathak V, Zawar V, Chuh A, Ghadi P. Giant pilomatricoma (pilomatrixoma) following an intramuscular injection. J Dermatol Case Rep. 2008;2(1):11–13. doi:10.3315/jdcr.2008.1005
14. Giacalone S, Spigariolo C, Brena M, Nazzaro G. The role of high-frequency ultrasound in the clinical management of multiple pilomatricomas. Int J Dermatol. 2022. doi:10.1111/ijd.16100
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.