Back to Journals » Clinical Interventions in Aging » Volume 21
Bronchial Arterial Chemoembolization with versus without Anlotinib in Elderly Patients with Advanced Non-Small Cell Lung Cancer: A Retrospective Case-Control Study
Authors Lai L, Si T, Yao H, Gong S, Duan X, Jin ZC, Zhang D, Ji J ![]() , Tu J
, Tu J
Received 16 December 2025
Accepted for publication 7 May 2026
Published 19 May 2026 Volume 2026:21 585561
DOI https://doi.org/10.2147/CIA.S585561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Linqiang Lai,1,* Tongguo Si,2,* Hongxiang Yao,3 Shaolin Gong,4 Xuhua Duan,5 Zhi-Cheng Jin,6 Dengke Zhang,1 Jiansong Ji,1 Jianfei Tu1
1Department of Thoracic Center, The Fifth Affiliated Hospital of Wenzhou Medical University, Lishui, Zhejiang, 323000, People’s Republic of China; 2Interventional Radiology Department, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China; 3Interventional Radiology Department, The Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China; 4Interventional Radiology Department, The First Affiliated Hospital of Zhejiang University, Hangzhou, Zhejiang, 310000, People’s Republic of China; 5Interventional Radiology Department, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450000, People’s Republic of China; 6Center of Interventional Radiology and Vascular Surgery, Department of Radiology, Zhongda Hospital, Southeast University, Nanjing, Jiangsu, 210009, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiansong Ji, Email [email protected] Jianfei Tu, Email [email protected]
Purpose: To compare bronchial arterial chemoembolization (BACE) plus anlotinib versus BACE alone for advanced non-small cell lung cancer (NSCLC) in the elderly.
Patients and Methods: We screened all elderly patients (≥ 75 years of age) receiving BACE (75 mg/m2 cisplatin and 1000 mg/m2 gemcitabine via feeding arteries and then embolization using microspheres) plus anlotinib (21-day cycles, 12 mg/day on the first 14 days of each cycle) or BACE alone for advanced NSCLC (stage III and IV) with no driver gene mutations at the participating centers from January 2018 to December 2023. Overall survival (OS) was analyzed in the overall and propensity score-matched (PSM) (1:1 ratio with 0.05 caliper width) cohorts, adjusting for confounders via PSM and stabilized inverse probability of treatment weighting (sIPTW).
Results: The final analysis included 95 patients: 33 and 62 in the BACE/anlotinib and BACE groups, respectively. The median lines of previous anti-tumor therapy was 1 (range, 1– 3) and 1 (range, 1– 3) in the BACE/anlotinib and BACE groups, respectively. The median OS was 39 months and 18.9 months in the BACE/anlotinib and BACE groups, respectively (hazard ratio 0.12, 95% confidence interval 0.06– 0.24; P < 0.001). In multivariate Cox regression analysis, BACE plus anlotinib was associated with lower risk of death versus BACE alone (hazard ratio 0.15, 95% confidence interval 0.08– 0.29; P < 0.001). Longer OS in the BACE/anlotinib group was also evident in the PSM and sIPTW analyses. The rate of grade ≥ 3 adverse events was 24.2% in the BACE/anlotinib group versus 12.9% in the BACE group (P = 0.16).
Conclusion: In comparison to BACE, BACE plus anlotinib was associated with improved OS in elderly patients with NSCLC.
Keywords: anlotinib, bronchial arterial chemoembolization, elderly population, non-small cell lung cancer
Introduction
Non-small cell lung cancer (NSCLC) accounts for approximately 85% of lung cancers,1 with 30–40% occurring in elderly patients.2 Elderly NSCLC patients frequently present with poor performance status, comorbidities and exhibit poor tolerance to chemotherapy. Targeted therapy3,4 (for driver gene-positive cases) and immunotherapy3,5,6 (for patient with high programmed death-ligand 1 (PD-L1) expression) represent standard treatments for advanced NSCLC, but their clinical utility remains restricted in driver gene-negative and PD-L1-low populations.
Bronchial arterial chemoembolization (BACE) delivers chemotherapeutic agents directly into the tumors through feeding arteries, followed by embolization with microspheres to block tumor blood supply, and could achieve high concentration in the tumors with reduced systemic exposure. A series of retrospective studies in patients undergoing BACE reported 21.6%-80.0% objective response rate (ORR), 66.7%-100% disease control rate (DCR), 4.3–8.4 month median progression-free survival (PFS) and 12.6–28.5 month median overall survival (OS).7–16 BACE is particularly useful in controlling the symptoms of hemoptysis or respiratory difficulties.17
Anlotinib, a multi-target tyrosine kinase inhibitor (TKI) that inhibits vascular endothelial growth factor receptor (VEGFR) / fibroblast growth factor receptor (FGFR) / platelet-derived growth factor receptor (PDGFR),18 has shown efficacy in refractory NSCLC (ALTER0303 trial: median PFS 5.4 versus 1.4 months with placebo; median OS 9.6 versus 6.3 months with placebo) with favorable safety.19 In a retrospective study in patients with advanced NSCLC, anlotinib plus BACE achieved a median OS of 18.4 months, median PFS of 8.4 months, with 15.7% grade ≥ 3 adverse events (AEs).12 In patients with hepatocellular carcinoma (HCC), anlotinib promotes the therapeutic action of transarterial chemoembolization (TACE) by inhibiting post-procedural hypoxia-induced VEGF upregulation and compensatory angiogenesis.20
Elderly NSCLC patients often have poor performance status and comorbidities, leading to suboptimal treatment tolerance. However, limited studies have specifically addressed this population. While our previous findings21 that BACE combined with chemotherapy improves efficacy over chemotherapy alone but is often poorly tolerated in elderly NSCLC patients. To address this, we conducted a retrospective study to examine a modified approach by replacing intravenous chemotherapy with oral anlotinib and compares the efficacy and safety of BACE plus anlotinib versus BACE alone in elderly patients with NSCLC.
Materials and Methods
Study Design and Patients
The retrospective case-control study was approved by the Institutional Review Board of author’s Hospital, and conducted in compliance to the 1964 Declaration of Helsinki and its later amendments. The requirement for informed consent was waived by the Institutional Review Board because of the retrospective nature of the study. All patient data were anonymized and to protect patient privacy. We screened all elderly patients (≥75 years of age) undergoing either BACE plus anlotinib or BACE alone for pathologically confirmed NSCLC at the participating centers from January 2018 to December 2023. Inclusion criteria were: (1) absence of driver gene mutations (including epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), c-ros oncogene 1 (ROS1), and other actionable mutations); (2) presence of at least one measurable lesion according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1;22 (3) intolerance to standard chemotherapy or immunotherapy, or refusal of such treatments after being fully informed of potential benefits and risks. Exclusion criteria were: (1) presence of driver gene mutations; (2) concurrent malignancy requiring active treatment; (3) incomplete clinical or follow-up data (Figure 1).
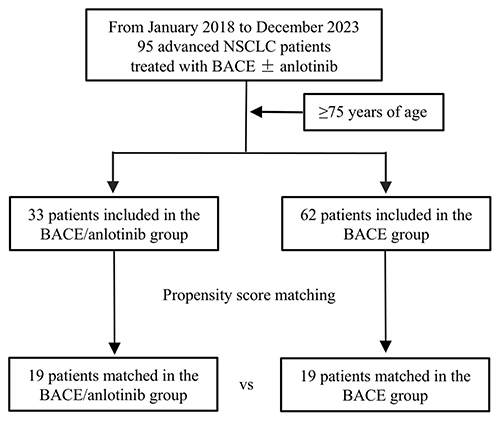 |
Figure 1 Patient flow through the study. Abbreviations: NSCLC, non-small cell lung cancer; BACE, bronchial arterial chemoembolization. |
Treatments
BACE consisted of cisplatin at a dose of 75 mg/m2 and gemcitabine at 1000 mg/m2 through the feeding arteries followed by embolization using microspheres. Blood supply to the lesions was delineated using chest computed tomography (CT) scan and CT angiography. The femoral artery was accessed using the Seldinger technique under local anesthesia. A 5F RLG or Cobra catheter (Asahi, Japan) was navigated through a 5F femoral sheath to the intended artery. Subsequently, a 1.9F microcatheter (Asahi, Japan) was positioned super-selectively within the feeding artery guided by angiography and intraoperative cone-beam CT. Cisplatin and gemcitabine were infused over a 30-minute period. The feeding artery was then embolized with microspheres (300–500 μm; Embospheres Beads, Meriton Co., USA). In cases with two or more feeding arteries, the total dosage was divided according to the volume of tumor supplied by each artery, estimated via intraoperative cone-beam CT. Reflux was prevented by maintaining an infusion rate of 400 mL/h with an infusion pump. The angiographic criterion for procedure completion was the stasis of the embolized artery or the non-visualization of tumor blush within 5 cardiac cycles (Figure 2). BACE was repeated in patients who achieved initial response but had residual viable tumor on follow-up chest CT performed three weeks after the procedure, provided that performance status was adequate. The procedure was performed by interventional radiologists with a minimum of 10 years of experience.
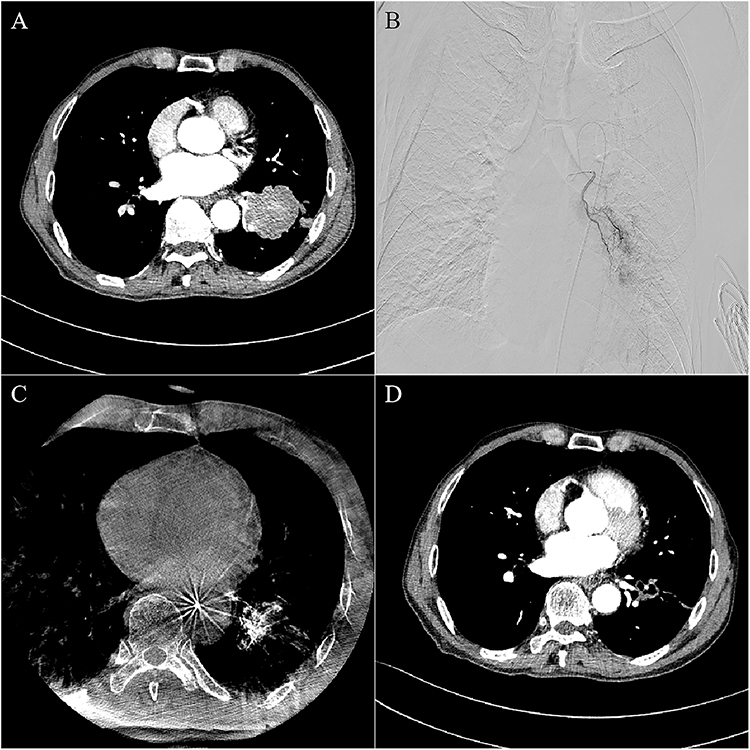 |
Figure 2 Treatment response in a 78-year-old male with stage IIIA lung squamous cell carcinoma receiving BACE plus anlotinib. (A) Pre-operative contrast-enhanced CT shows a left lower lobe mass (50 mm × 46 mm). (B) Intraoperative DSA demonstrates tumor-feeding left bronchial artery. (C) Intraoperative CB-CT confirms tumor vascular supply from the same artery. (D) Postoperative contrast-enhanced CT showing the shrinking of the tumor (23 mm × 24 mm). Abbreviations: BACE, bronchial arterial chemoembolization; DSA, digital subtraction angiography; CB-CT, cone beam computed tomography. |
Anlotinib treatment commenced one week after BACE, and was given at a daily dose of 12 mg for the first 14 days of each 21-day cycle until disease progression or intolerable side effects. In cases that patients could not tolerate anlotinib, the dosage was reduced in 2-mg steps until 8 mg/day and discontinued if anlotinib could not be tolerated anlotinib at 8 mg/day.
Assessments
The follow-up was conducted at the end of anlotinib cycle following BACE and every 3–6 months thereafter, and consisted of blood routines, liver and kidney functions, and coagulation function. Tumor response evaluation was conducted per RECIST v1.122 by two independent radiologists with more than ten years of experience; inconsistency was resolved by discussion with a third radiologist with more than ten years of experience in diagnostic radiology. Survival outcomes (OS and PFS) were calculated from start of the treatment. ORR was defined as the proportion of patients who achieved CR or PR. DCR was defined as the proportion of patients who achieved CR, PR, or SD. Anlotinib-related adverse effects were assessed per NCI Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.23 BACE-related complications were categorized into embolization-related (graded by Society of Interventional Radiology [SIR] Standards)24 and chemotherapy-related (assessed per NCI-CTCAE version 5.0).
Statistical Analysis
To compare baseline characteristics between the two groups, continuous variables were analyzed using Student’s t-test if normally distributed or Mann–Whitney U-test otherwise. Categorical variables were compared using the chi-squared test or Fisher’s exact test as appropriate. OS and PFS were compared using the Log rank test, and Kaplan–Meier survival curves were constructed. Hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated using the Cox proportional hazards model. Propensity score matching (PSM) and stabilized inverse probability of treatment weighting (sIPTW) were conducted as sensitivity analyses. Covariates in the analyses included age, sex, Eastern Cooperative Oncology Group (ECOG) performance status, TNM stage, pathological histology (squamous cell carcinoma versus adenocarcinoma), smoking history, and lines of treatment. Due to the retrospective nature of this study, power calculation was not conducted. P < 0.05 (2-sided) was considered statistically significant. All statistical analyses were conducted using R software (version 4.3.1) and PASS (version 15.0.5).
Results
Patient Characteristics
The final analysis included 95 patients (median age: 79 years; 78 man): 33 in the BACE/anlotinib group and the remaining 62 in the BACE group. Technical success rate for BACE was 100% in both groups. Demographical and baseline characteristics of the two groups are shown in Table 1. The median lines of previous anti-tumor therapy was 1 (range, 1–3) and 1 (range, 1–3) in the BACE/anlotinib and BACE groups, respectively.
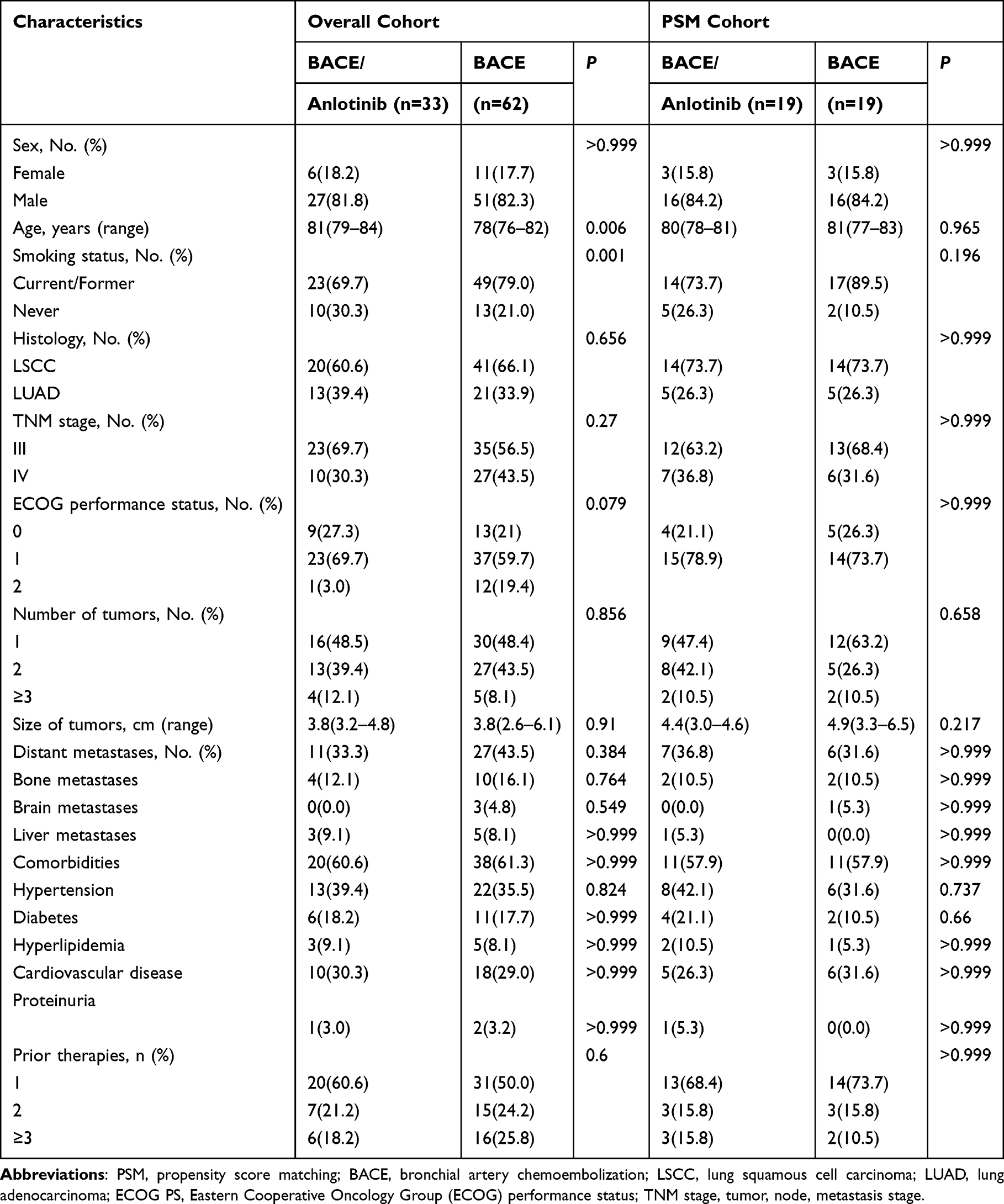 |
Table 1 Demographic and Baseline Characteristics |
Analysis of the Overall Cohort
In the crude analysis of the overall cohort, the median OS was 39 months (95% CI 31.8–47.2) in the BACE/anlotinib group versus 18.9 months (95% CI 17.8–22.8) in the BACE group (HR 0.12, 95% CI 0.06–0.24; P < 0.001; Figure 3A); the median PFS was 13 months (95% CI 10.3–16.4) in the BACE/anlotinib group versus 5.5 months (95% CI 4.4–7.2) in the BACE group (HR 0.19, 95% CI 0.11–0.35; P < 0.001; Figure 3D). In the sIPTW analysis, the median OS was 39.5 months (95% CI 31.5–47.2) in the BACE/anlotinib group versus 19.7 months (95% CI 17.8–22.8) in the BACE group (HR 0.16, 95% CI 0.08–0.33; P < 0.001; Figure 3B); the median PFS was 11.6 months (95% CI 8.9–17.6) in the BACE/anlotinib group versus 5.6 months (95% CI 4.4–7.8) in the BACE group (HR 0.22, 95% CI 0.12–0.40; P < 0.001; Figure 3E). In the multivariate COX regression, improved OS was independently associated with earlier TNM stage (HR 0.43, 95% CI 0.28–0.68, P < 0.001), and BACE plus anlotinib (HR 0.15, 95% CI 0.08–0.29; P < 0.001; Table 2). Improved PFS was independently associated with BACE plus anlotinib (HR 0.19, 95% CI 0.11–0.35, P < 0.001; Table 2). The BACE/anlotinib group had higher ORR (66.7% versus 40.3%, P = 0.018) and DCR (87.9% versus 61.3%, P = 0.009; Table 3).
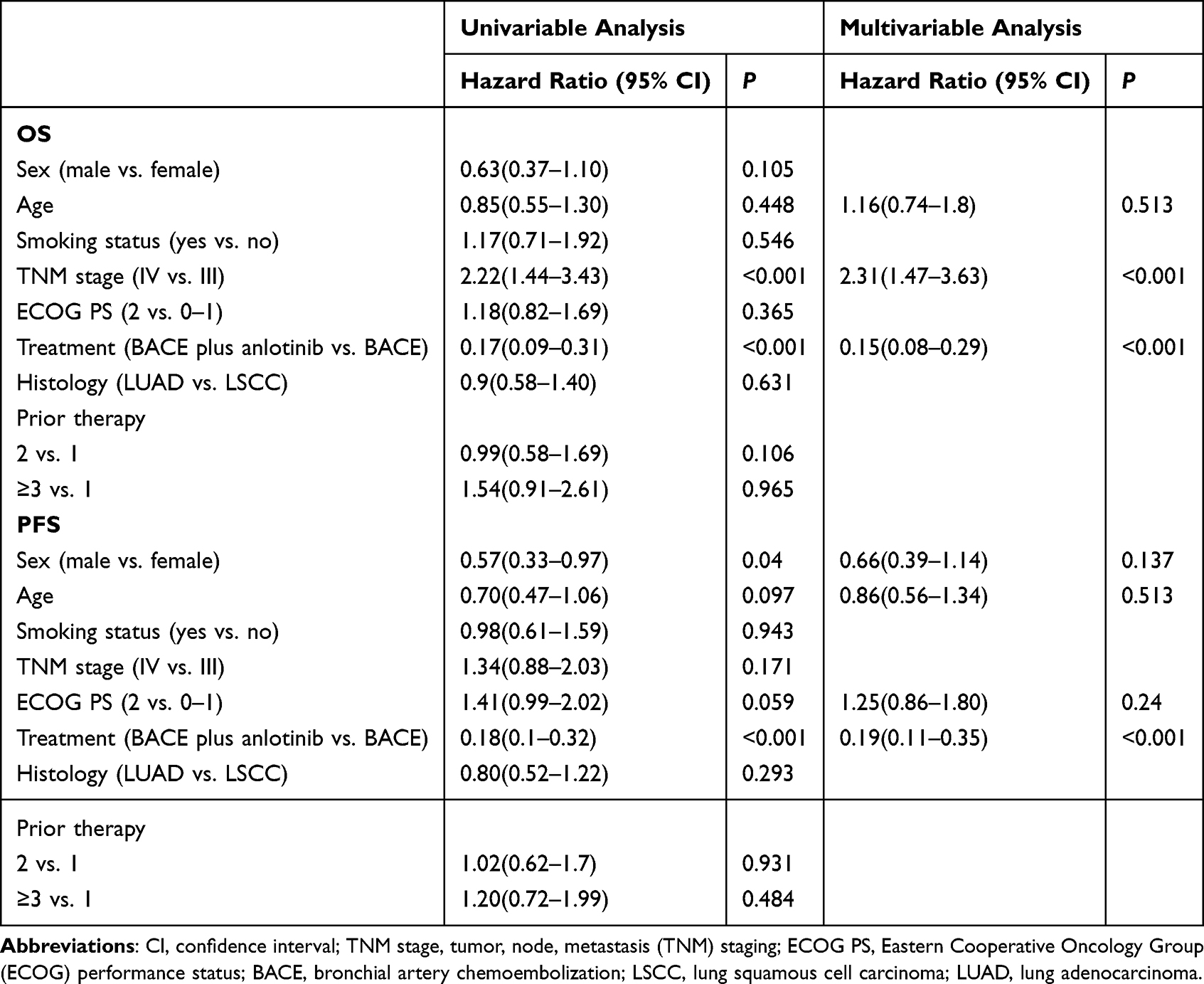 |
Table 2 Cox Regression Analysis of the Overall Survival and Progression-Free Survival in the Overall Cohort |
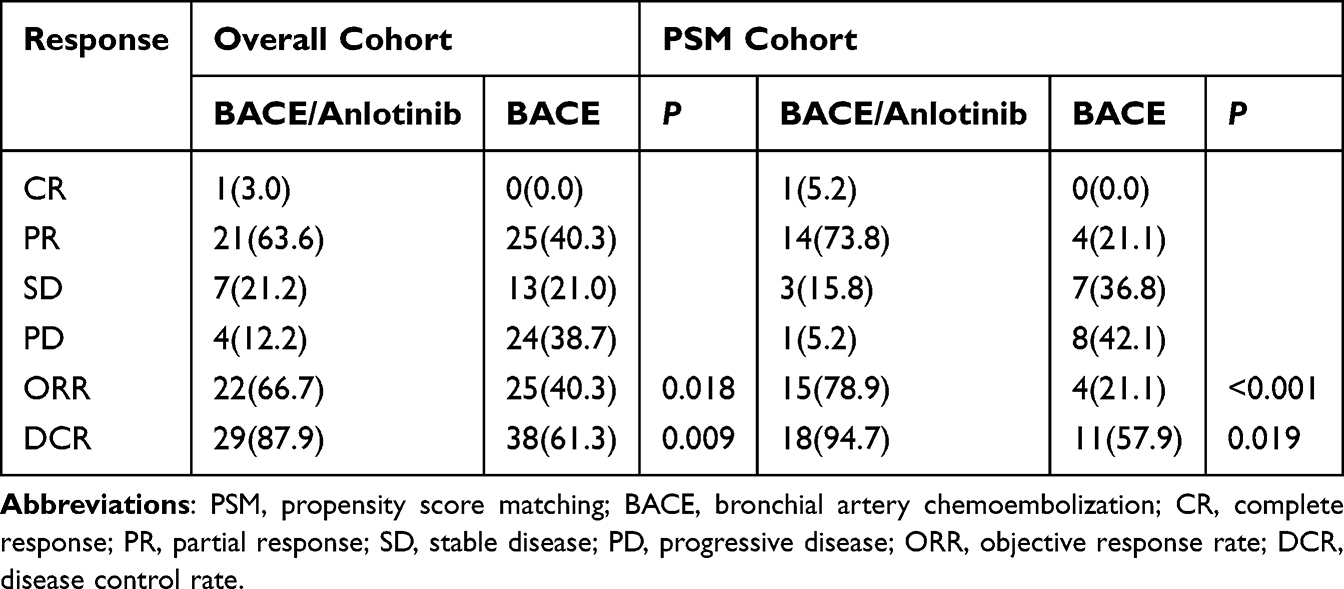 |
Table 3 Best Tumor Response According to RECIST Standard |
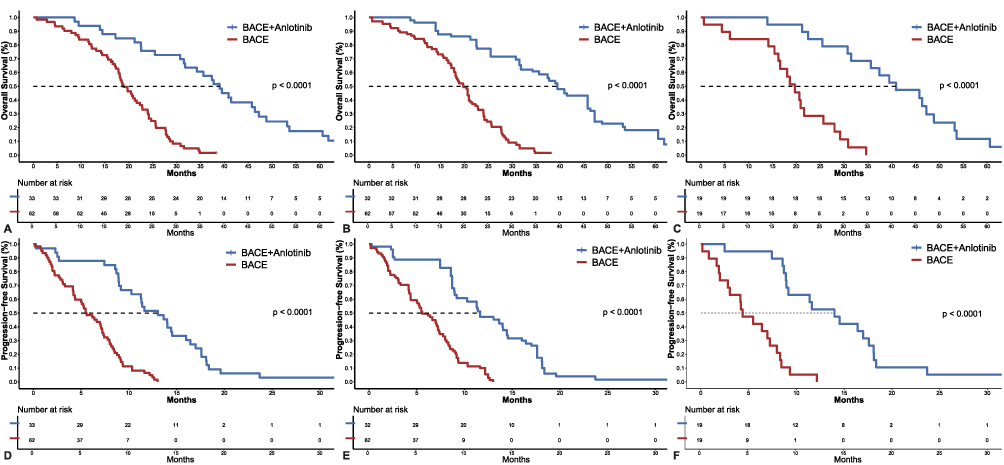 |
Figure 3 Survival outcomes in different cohorts: (A) OS in the overall cohort, (B) OS in the sIPTW-adjusted analysis, (C) OS in the PSM cohort, (D) PFS in the overall cohort, (E) PFS in the sIPTW-adjusted analysis, (F) PFS in the PSM cohort. Abbreviations: OS, Overall survival; PFS, progression-free survival; SIPTW, stabilized inverse probability of treatment weighting; PSM, propensity score-matched. |
Complications related to BACE did not differ between the two groups (Table 4). No spinal cord injury and cerebral embolism was observed in any patients. The rate of AEs of any grade was 93.9% in the BACE/anlotinib group versus 79.0% in the BACE group (P = 0.077); grade ≥ 3 AEs was 24.2% in the BACE/anlotinib group versus 12.9% in the BACE group (P = 0.16). The BACE/anlotinib group had higher rate of hypertension (60.6% versus 35.5%, P = 0.029), hand-foot syndrome (36.4% versus 0%, P < 0.001), hypertriglyceridemia (33.3% versus 8%, P = 0.003), proteinuria (33.3% versus 3.2%, P < 0.001), and oral mucositis (9.1% versus 0%, P = 0.032) (Table 4).
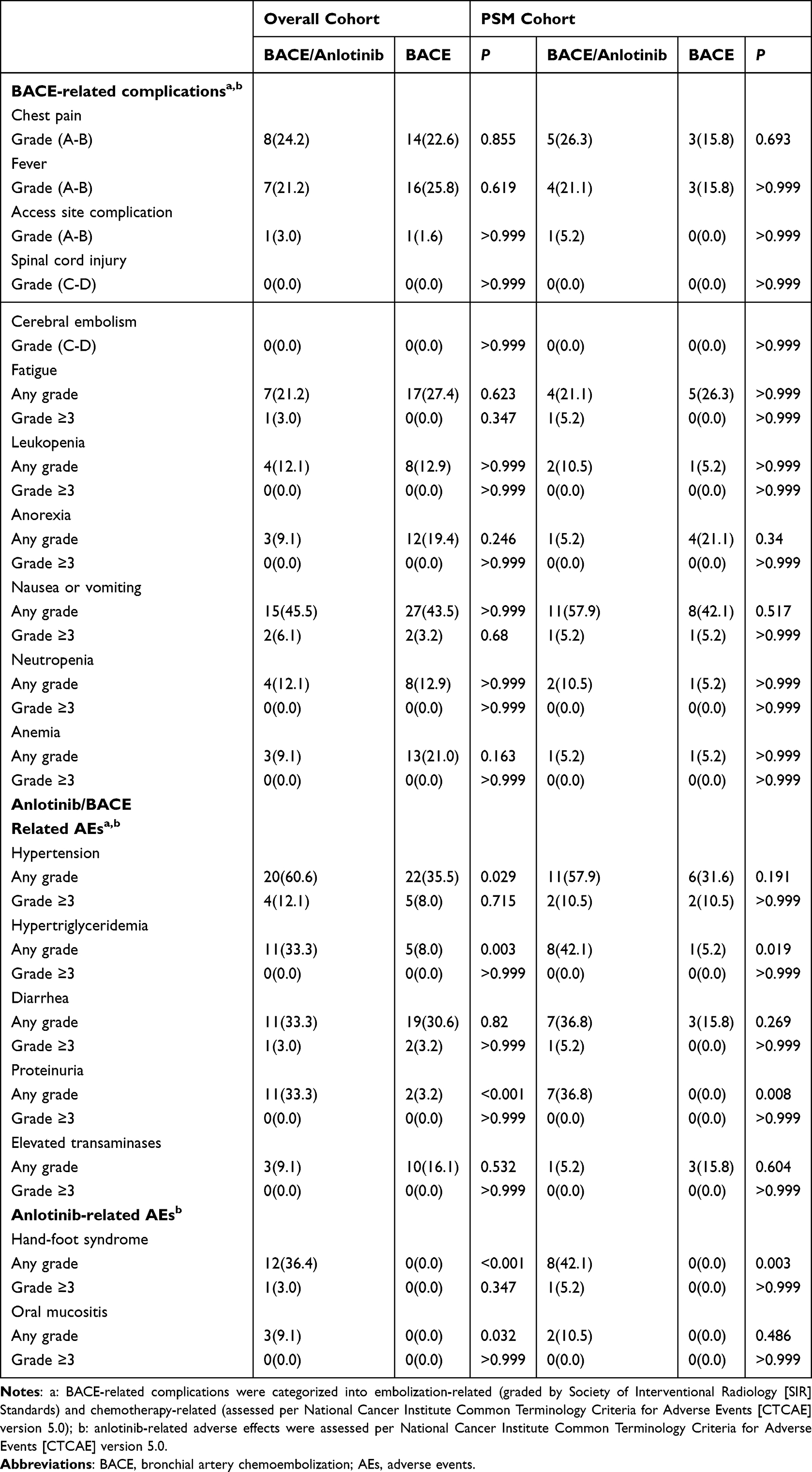 |
Table 4 Treatment-Emergent Adverse Events |
PSM Analysis
The PSM analysis included 19 patients in each group. The median OS was 40.9 months (95% CI 35.6–53.2) in the BACE/anlotinib group versus 19.7 months (95% CI 16.6–28.0) in the BACE group (HR 0.12, 95% CI 0.04–0.34; P < 0.001; Figure 3C). The median PFS was 14 months (95% CI 9.2–18.1) in the BACE/anlotinib group versus 4.4 months (95% CI 3.0–8.3) in the BACE group (HR 0.13, 95% CI 0.05–0.33; P < 0.001; Figure 3F). The BACE/anlotinib group had higher ORR (78.9% [1CR + 14 PR] versus 21.1% [4 PR], P < 0.001; Table 3) and DCR (94.7% [1 CR + 14 PR + 3 SD] versus 57.9% [4 PR + 7 SD], P = 0.019). Complications related to BACE did not differ between the two groups (Table 4). The rate of AEs of any grade was 100% in the BACE/anlotinib group versus 78.9% in the BACE group (P = 0.105), the rate of grade ≥3 AEs was 26.3% in the BACE/anlotinib group versus 15.8% in the BACE group (P = 0.434). The BACE/anlotinib group had higher rate of hand-foot syndrome (42.1% versus 0%, P = 0.003), hypertriglyceridemia (42.1% versus 5.2%, P = 0.019) and proteinuria (36.8% versus 0%, P = 0.008) (Table 4).
Discussions
Chemotherapy combined with immunotherapy are the standard first-line treatment for advanced NSCLC patients with driver gene-negative status. However, elderly patient population often could not tolerate systemic chemotherapy due to limited organ reserve and co-morbidities. Locoregional therapies (eg., BACE) have favorable safety profile, and thus represent important alternatives for this patient population.
In the current study, the BACE/anlotinib group had longer median OS (39 versus 18.9 months in the BACE group) as well as median PFS (13 versus 5.5 months in the BACE group). The sIPTW analysis confirmed longer OS and PFS in the BACE/anlotinib group. In the multivariate COX regression, BACE/anlotinib was independently associated with improved OS and PFS. In the PSM analysis, the BACE/anlotinib group also had longer median OS (40.9 months versus 19.7 months) and PFS (14 months versus 4.4 months). There was a statistically non-significant trend for higher AEs in the BACE/anlotinib group (93.9% versus 79.0% in the BACE group, P = 0.077). The BACE/anlotinib group also seemed to have higher grade ≥3 AEs (24.2% in the BACE/anlotinib group versus 12.9% in the BACE group; P = 0.16). The BACE/anlotinib group had higher rate of AEs known to associate with anlotinib, including hypertension, hand-foot syndrome, hypertriglyceridemia, proteinuria and oral mucositis.
The median OS and PFS in the BACE/anlotinib group (OS: 39 months in overall cohort and 40.9 months in the PSM cohort; PFS: 13 months in the overall cohort and 14 months in the PSM cohort) are numerically longer than that reported for anlotinib monotherapy (median OS: 6.44–12.78 months; median PFS: 3.52–9.23 months).25–27 Notably, the median OS and PFS in the BACE group of the current study (OS: 18.9 months in overall cohort and 19.7 months in the PSM cohort; PFS: 5.5 months in the overall cohort and 4.4 months in the PSM cohort) were consistent with that reported in previous studies of BACE,7–16 supporting longer median OS and PFS with BACE/anlotinib versus wither BACE or anlotinib alone. The therapeutic synergy of this combination can be attributed to the fact that increased VEGFR expression and the proliferation of new blood vessels in response to local ischemia and hypoxia after BACE is inhibited by anlotinib.20,28
There was a statistically non-significant trend for higher rate of grade ≥3 AEs in the BACE/anlotinib group in both the overall analysis (24.2% versus 12.9% in the BACE group, P = 0.16) and PSM analysis (26.3% versus 15.8% in the BACE group, P = 0.434). The BACE/anlotinib group also had higher rate of hypertension, hand-foot syndrome, hypertriglyceridemia, proteinuria, and oral mucositis. These findings were consistent with that reported by previous large-scale clinical trials of anlotinib in lung cancer, including those by Chen et al,25 Zhou et al,26 and Li et al27 Complications related to BACE in the current study were consistent with previous literature,7–16 and did not differ between the two groups No spinal cord injury or cerebral embolism occurred, confirming the overall safety of the procedure.
This study had several limitations. First, this is a retrospective study, and thus is subject to selection bias, despite of the use of PSM and IPTW. Second, detailed data on systemic therapy regimens after BACE were not available. Third, our findings are limited to elderly patients with advanced NSCLC who are not suitable candidates for systemic chemotherapy. Fourth, the sample size (particularly the PSM cohort) may not be sufficient to detect differences of AEs. As a matter of fact, we failed to show statistically significant differences in overall rate of AEs despite of higher rate of specific AEs that are known to be associated with anlotinib (eg. hypertension, hand-foot syndrome, and oral mucositis). Future studies with larger sample sizes and comparator arms are needed to validate the findings and to assess the generalizability of the results. Fifth, BACE was gemcitabine-based in this study. Whether the results apply to other chemotherapeutic regimens requires further investigation. Last, PD-L1 status was not collected, and no patients in this cohort received immunotherapy due to financial restriction; accordingly, relevance to current practice (chemoimmunotherapy as the standard treatment for NSCLC with no driver gene mutations) requires further investigation.
Conclusion
In conclusion, BACE plus anlotinib was associated with survival benefits in elderly patients with advanced NSCLC.
Data Sharing Statement
Deidentified individual patient data are available upon request.
The data that support the findings of this study are available from the corresponding author, Jianfei Tu, upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Fifth Affiliated Hospital of Wenzhou Medical University (#202517101), and conducted in compliance with the Declaration of Helsinki and its later amendments. The requirement for informed consent was waived by the Institutional Review Board because of the retrospective nature of the study.
Funding
This study was funded by Zhejiang Medical Association Clinical Medicine Special Fund Project (2022ZYC-A263), Medical and Health Science and Technology Planning Project of Zhejiang Province (2022PY031 and WKJ-ZJ-1932).
Disclosure
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–11. doi:10.3322/caac.21660
2. Gridelli C, Balducci L, Ciardiello F, et al. Treatment of elderly patients with non–small-cell lung cancer: results of an international expert panel meeting of the Italian association of thoracic oncology. Clin Lung Cancer. 2015;16(5):325–333. doi:10.1016/j.cllc.2015.02.006
3. Riely GJ, Wood DE, Ettinger DS, et al. Non-small cell lung cancer, version 4.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2024;22(4):249–274. doi:10.6004/jnccn.2204.0023
4. Kumarakulasinghe NB, van Zanwijk N, Soo RA. Molecular targeted therapy in the treatment of advanced stage non-small cell lung cancer (NSCLC). Respirology. 2015;20(3):370–378. doi:10.1111/resp.12490
5. Trebeschi S, Drago SG, Birkbak NJ, et al. Predicting response to cancer immunotherapy using noninvasive radiomic biomarkers. Ann Oncol. 2019;30(6):998–1004. doi:10.1093/annonc/mdz108
6. Nikolich-žugich J. The twilight of immunity: emerging concepts in aging of the immune system. Nat Immunol. 2018;19(1):10–19. doi:10.1038/s41590-017-0006-x
7. Ren K, Wang J, Li Y, et al. The efficacy of drug-eluting bead transarterial chemoembolization loaded with oxaliplatin for the treatment of stage III-IV non-small-cell lung cancer. Acad Radiol. 2022;29(11):1641–1646. doi:10.1016/j.acra.2022.01.015
8. Bie Z, Li Y, Li B, Wang D, Li L, Li X. The efficacy of drug-eluting beads bronchial arterial chemoembolization loaded with gemcitabine for treatment of non-small cell lung cancer. Thorac Cancer. 2019;10(9):1770–1778. doi:10.1111/1759-7714.13139
9. Liu X-F, Lin H, Wang Q, et al. Drug-eluting bead bronchial arterial chemoembolization vs. chemotherapy in treating advanced non-small cell lung cancer: comparison of treatment efficacy, safety and quality of life. Eur Rev Med Pharmacol Sci. 2021;25(6):2554–2566. doi:10.26355/eurrev_202103_25419
10. Yu G, Shen Y, Chen L, Xu X, Yang J. Drug-eluting beads bronchial arterial chemoembolization vs. conventional bronchial arterial chemoembolization in the treatment of advanced non-small cell lung cancer. Front Med. 2023;10:1201468. doi:10.3389/fmed.2023.1201468
11. He G, Yang K, Zhang X, et al. Bronchial artery chemoembolization with drug-eluting beads versus bronchial artery infusion followed by polyvinyl alcohol particles embolization for advanced squamous cell lung cancer: a retrospective study. Eur J Radiol. 2023;161:110747. doi:10.1016/j.ejrad.2023.110747
12. Liu J, Zhang W, Ren J, et al. Efficacy and safety of drug-eluting bead bronchial arterial chemoembolization plus anlotinib in patients with advanced non-small-cell lung cancer. Front Cell Dev Biol. 2021;9:768943. doi:10.3389/fcell.2021.768943
13. Zeng Y, Yin M, Zhao Y, et al. Combination of bronchial arterial infusion chemotherapy plus drug-eluting embolic transarterial chemoembolization for treatment of advanced lung cancer—a retrospective analysis of 23 patients. J Vasc Interv Radiol. 2020;31(10):1645–1653. doi:10.1016/j.jvir.2020.06.007
14. Liu X, Lin H, Wang Q, et al. Drug-eluting beads bronchial arterial chemoembolization plus intercostals arterial infusion chemotherapy is effective and well- tolerated in treating non-small cell lung cancer patients with refractory malignant pleural effusion. J Thorac Dis. 2021;13(4):2339–2350. doi:10.21037/jtd-20-1603
15. Bi Y, Zhang B, Ren J, Han X, Wu W. Clinical outcomes of gemcitabine-loaded callispheres drug-eluting beads for patients with advanced and inoperable lung cancer: a case series study. Front Pharmacol. 2022;13:992526. doi:10.3389/fphar.2022.992526
16. Boas FE, Kemeny NE, Sofocleous CT, et al. Bronchial or pulmonary artery chemoembolization for unresectable and unablatable lung metastases: a phase I clinical trial. Radiology. 2021;301(2):474–484. doi:10.1148/radiol.2021210213
17. Xiaobing L, Meipan Y, Pengfei X, et al. Bronchial artery chemoembolization for hemoptysis in advanced primary lung cancer. Clin Lung Cancer. 2022;23(3):e203–e209. doi:10.1016/j.cllc.2021.10.011
18. Shen G, Zheng F, Ren D, et al. Anlotinib: a novel multi-targeting tyrosine kinase inhibitor in clinical development. J Hematol Oncol. 2018;11(1):120. doi:10.1186/s13045-018-0664-7
19. Han B, Li K, Wang Q, et al. Effect of anlotinib as a third-line or further treatment on overall survival of patients with advanced non–small cell lung cancer. JAMA Oncol. 2018;4(11):1569–1575. doi:10.1001/jamaoncol.2018.3039
20. Zeng H, Shao G. Efficacy and safety of TACE combined with anlotinib compared with TACE alone among patients with intermediate or advanced hepatocellular carcinoma (HCC): a randomized, controlled, Phase II clinical study. J Clin Oncol. 2023;41(4_suppl):581. doi:10.1200/JCO.2023.41.4_suppl.581
21. Lai L, Xu F, Zhang D, et al. Bronchial arterial chemoembolization with drug-eluting beads plus sequential chemotherapy for the treatment of stage III and IV lung squamous cell carcinoma. Eur J Radiol. 2024;175:111398. doi:10.1016/j.ejrad.2024.111398
22. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
23. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. CTCAE versión 5.0. Evaluación de la gravedad de los eventos adversos dermatológicos de las terapias antineoplásicas. Actas Dermosifiliogr. 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
24. Khalilzadeh O, Baerlocher MO, Shyn PB, et al. Proposal of a new adverse event classification by the society of interventional radiology standards of practice committee. J Vasc Interv Radiol. 2017;28(10):1432–1437.e3. doi:10.1016/j.jvir.2017.06.019
25. Chen X-Z. Anlotinib for refractory advanced non–small cell lung cancer in China. JAMA Oncol. 2019;5(1):116–117. doi:10.1001/jamaoncol.2018.5526
26. Zhou M, Chen X, Zhang H, et al. China national medical products administration approval summary: anlotinib for the treatment of advanced non-small cell lung cancer after two lines of chemotherapy. Cancer Commun. 2019;39(1):36. doi:10.1186/s40880-019-0383-7
27. Li Z, Hou X, Yang L, et al. EP08.02-033 Anlotinib in elderly patients with advanced non-squamous NSCLC who had not received systemic chemotherapy: a single-arm, phase II study. J Thorac Oncol. 2022;17(9):S412. doi:10.1016/j.jtho.2022.07.715
28. Li X, Feng G-S, Zheng C-S, Zhuo C-K, Liu X. Influence of transarterial chemoembolization on angiogenesis and expression of vascular endothelial growth factor and basic fibroblast growth factor in rat with walker-256 transplanted hepatoma: an experimental study. World J Gastroenterol. 2003;9(11):2445–2449. doi:10.3748/wjg.v9.i11.2445
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.