Back to Journals » International Journal of Nanomedicine » Volume 21
Bridging Preclinical and Clinical Gaps in Ocular Therapeutics: Hydrogel Drug Delivery and 3D Tissue Models
Authors Barar J, Aliakbari A, Omidi Y
Received 15 January 2026
Accepted for publication 22 April 2026
Published 3 June 2026 Volume 2026:21 555555
DOI https://doi.org/10.2147/IJN.S555555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Eng San Thian
Jaleh Barar, Anali Aliakbari, Yadollah Omidi
Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL, 33328, USA
Correspondence: Jaleh Barar, Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, Florida, 33328, USA, Email [email protected] Yadollah Omidi, Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, Florida, 33328, USA, Email [email protected]
Abstract: Affecting over 2.2 billion people globally, ocular diseases represent a profound public health challenge, with vision loss projected to increase by 55% by 2050. Ocular drug delivery is fundamentally constrained by the eye’s anatomical and physiological barriers, limiting bioavailability and necessitating repeated invasive administration. Hydrogel-based drug delivery systems (DDSs) have emerged as transformative platforms offering controlled drug release, mucoadhesive precorneal retention, and stimulus-responsive phase transitions for anterior and posterior segment diseases. Formulated from natural biopolymers (e.g., hyaluronic acid, chitosan, gelatin, and alginate) and synthetic platforms (e.g., thermosensitive poloxamers, pH-responsive carbomers, and photo-crosslinked polyethylene glycol systems), these networks sustain therapeutic concentrations while reducing the burden of invasive procedures. Despite these advances, clinical translation remains critically impeded by the limited predictive capacity of conventional two-dimensional cell cultures and animal models, which fail to replicate human ocular tissue architecture, barrier integrity, and disease pathophysiology. Three-dimensional (3D) ocular organoids (e.g., corneal epithelial, lens, lacrimal gland, and retinal constructs derived from patient-specific induced pluripotent stem cells) alongside eye-on-a-chip microfluidic platforms provide human-relevant microphysiological systems for evaluating hydrogel performance, drug transport, efficacy, and biocompatibility under normal conditions. Critically, the integration of hydrogel-based DDSs with advanced 3D tissue models offers a transformative strategy to bridge the persistent preclinical-to-clinical translation gap in ocular therapeutics. Herein, we critically appraise the current landscape of hydrogel-based ocular DDSs and their integration with 3D organoid and organ-on-chip platforms, identifying key opportunities and barriers along the translational pathway toward next-generation therapeutics for vision-threatening ocular diseases.
Keywords: ocular hydrogel drug delivery, ocular organoids, eye-on-a-chip, sustained release systems, microphysiological platforms, patient-derived models
Introduction
Ocular diseases impose an extraordinary global health burden, affecting approximately 2.2 billion people worldwide with near or distance vision impairment (including 1.1 billion with distance vision loss), of whom at least 1 billion cases could have been prevented or remain unaddressed (Figure 1A).1,2 In 2020, an estimated 43.3 million people were blind, and 295 million experienced moderate to severe vision impairment globally. The economic impact is staggering, with the annual global cost of productivity losses attributed to vision impairment estimated at US$411 billion.3–5 This escalating burden underscores the urgent need for advanced drug delivery technologies, including hydrogel-based systems capable of overcoming the eye’s formidable anatomical and physiological barriers. Both anterior and posterior segment diseases contribute substantially to this burden. Among the leading causes of preventable blindness, cataract accounts for 17.0 million (39.6%) cases and 83.5 million (28.3%) cases of moderate to severe vision impairment, followed by uncorrected refractive error affecting 88.4 million people, age-related macular degeneration impacting 8 million individuals, glaucoma affecting 7.7 million people, and diabetic retinopathy contributing to vision loss in 3.9 million individuals (Figure 1B).1,3–8 Notably, diabetic retinopathy was the only major cause of blindness to show an increase in global prevalence from 1990 to 2020, with an estimated 103.12 million adults worldwide affected, representing 22.27% of all adults with diabetes.6 This escalating burden is projected to worsen substantially, with vision loss predicted to increase by 55% by 2050, potentially affecting 1.8 billion people globally (Figure 1C).8 Ocular diseases represent a significant global health burden, with conditions affecting both the anterior and posterior segments of the eye, constituting major causes of vision impairment and irreversible blindness worldwide. For instance, presbyopia, as an age-related loss of the eye’s ability to focus on nearby objects, occurs naturally as part of the aging process, typically becoming noticeable after age 40, when the lens of the eye becomes less flexible, and the muscles controlling lens shape weaken. This makes it difficult to see things up close, such as reading small print, using a smartphone, or doing detailed work. Presbyopia affects nearly everyone as they age and is corrected with reading glasses, bifocals, multifocal contact lenses, or progressive lenses. Figure 1 represents global vision loss and the magnitude and contributing factors.
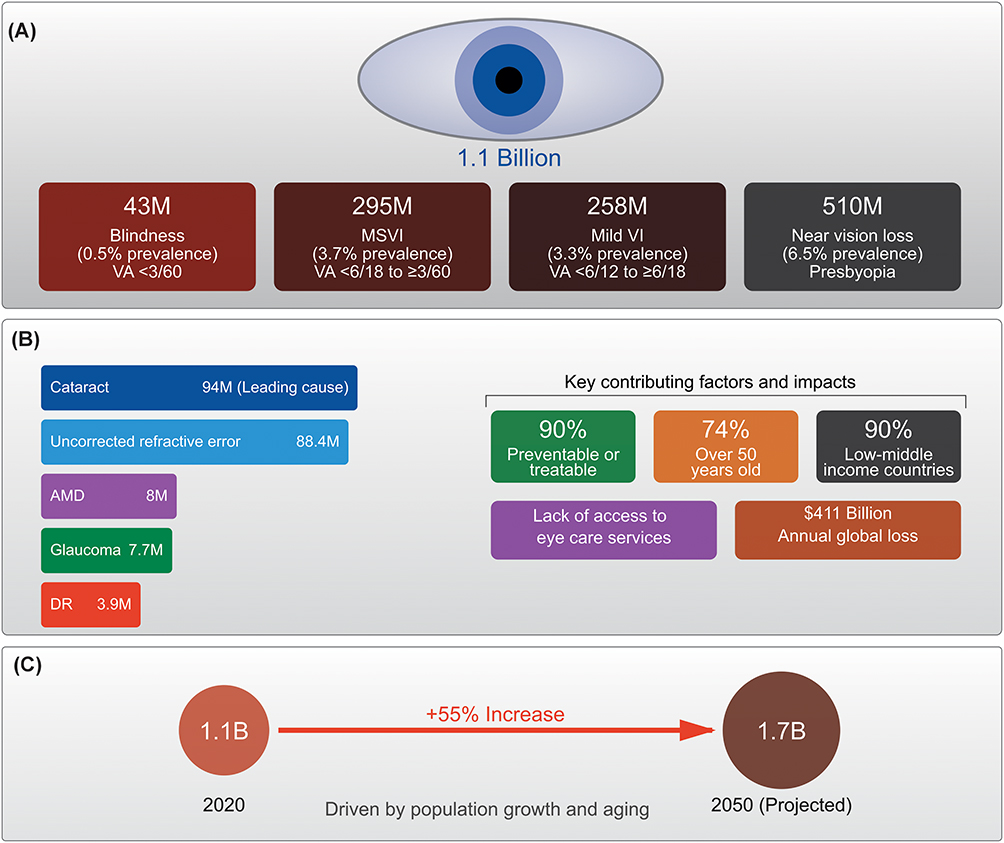 |
Figure 1 Schematic illustration of the global vision loss and the magnitude and contributing factors. (A) People living with vision loss. The global burden of vision loss, affecting 1.1 billion people worldwide, in which the leading causes are predominantly treatable. (B) Leading causes of vision loss. Cataract represents the greatest impact on vision loss worldwide. (C) Projected growth of vision loss by 2050. Without adequate intervention and improved access to eye care services, the burden is projected to increase by 55%. For detailed information, readers are directed to Vision Atlas.8 Abbreviations: MSVI, Moderate to severe visual impairment; VI, Visual impairment; AMD, Age-related macular degeneration; DR, Diabetic retinopathy; VA, Visual Acuity (used in the infographic to denote vision measurements). |
The eye possesses one of the most sophisticated and complex physiological defense systems in the human body, comprising multiple anatomical barriers that, while essential for protecting delicate ocular tissues, simultaneously present formidable challenges for effective therapeutic intervention.9,10 These barriers include the corneal epithelium, blood-aqueous barrier (BAB), blood-retinal barrier (BRB), and various tight junction complexes that collectively restrict drug penetration and limit bioavailability of therapeutic agents.10 Consequently, the development of effective ocular drug delivery systems (DDSs) remains one of the most challenging endeavors in pharmaceutical sciences, with conventional approaches often failing to achieve adequate therapeutic concentrations at target sites while minimizing systemic exposure and adverse effects.11
Traditional ocular drug delivery modalities, including topical administration through eye drops and ointments, intravitreal injections, and systemic routes, each present distinct limitations that compromise therapeutic efficacy and patient compliance. Topical formulations, while non-invasive and convenient, suffer from extremely low bioavailability; typically, less than 5% of the administered dose reaches intraocular tissues due to rapid precorneal clearance, nasolacrimal drainage, and limited corneal permeability.9,10,12 Intravitreal injections, though effective for posterior segment diseases, require repeated invasive procedures that carry risks of endophthalmitis, retinal detachment, and patient discomfort. Furthermore, the difficulty in monitoring antibiotic dosage and duration of therapy in topical preparations, combined with the potential for disrupting normal ocular microflora, raises concerns about antimicrobial resistance and therapeutic outcomes.13–16 These limitations underscore an urgent need for innovative drug delivery platforms that can overcome anatomical barriers, provide sustained therapeutic concentrations, and improve patient adherence.11
Hydrogel-based DDSs have emerged as promising candidates to address these challenges, offering unique advantages derived from their biocompatibility, tunable mechanical properties, and capacity for controlled drug release of multiple drugs.17–19 Polysaccharide-based hydrogels, in particular, have gained considerable attention due to their outstanding biodegradability and versatility in fabrication.20,21 These materials can be engineered as injectable in situ gelling systems, which become gel within seconds to minutes following administration, with storage moduli ranging from 102 to 104 Pa, indicating excellent injectability and adjustable mechanical strength suitable for various ocular applications.20 Stimulus-responsive cellulose hydrogels represent a particularly sophisticated approach, capable of responding to environmental stimuli (e.g., pH variations, temperature fluctuations, and light exposure), thereby enabling targeted drug release and resulting in an optimized treatment outcome.22 These systems have been optimized for ocular administration, demonstrating enhanced corneal permeability, prolonged retention time, and sustained release profiles that address the pharmacokinetic limitations observed with conventional formulations, as reported for curcumin formulations.23 The integration of nanocarrier technologies with hydrogel platforms further enhances their potential, offering low toxicity, high efficiency, and superior stability for targeted delivery to both anterior and posterior eye segments.24 Despite these advances, a critical bottleneck remains in translating preclinical findings into successful clinical outcomes. High attrition rates in ocular drug development reflect the limitations of conventional preclinical models. Two-dimentional (2D) cell models fail to replicate the architecture and microenvironment of native ocular tissues, while animal models are constrained by interspecies differences in anatomy and drug disposition. This translational gap drives substantial resource waste on candidates that fail in clinical trials, underscoring the need for more predictive, human-relevant platforms. Three-dimensional (3D) tissue models and organoids have emerged as transformative tools to bridge this divide.25 These advanced in vitro systems recapitulate key structural and functional characteristics of native ocular tissues, including cellular organization, extracellular matrix composition, barrier properties, and disease-relevant pathophysiology.26 When integrated with hydrogel-based drug delivery platforms, 3D tissue models offer physiologically relevant environments for evaluating drug penetration, efficacy, and toxicity, enabling mechanistic insights, formulation optimization, and improved clinical outcome prediction. However, translating these systems faces key challenges, including manufacturing scalability, characterization limitations, in vivo instability, safety concerns, and incomplete understanding of nanoformulation biophysical and chemical interactions.27 For stimuli-responsive hydrogels specifically, challenges related to immune compatibility, long-term stability, and scalability in production remain significant barriers to clinical translation.22,28–30 Standardization and validation of 3D models, maintenance of long-term cultures, incorporation of vascularization and innervation, and establishment of regulatory pathways for these novel testing platforms represent additional hurdles. Quality-by-design (QbD) approaches, process analytical methods, and microfluidics offer promising solutions to accelerate translation, though these technologies require further development and regulatory guidance.27 This review critically examines hydrogel-based DDSs and 3D tissue models as synergistic platforms for overcoming translational barriers in ocular therapeutics. By evaluating recent advances, integration strategies, and key knowledge gaps, it offers a framework for designing next-generation ocular systems that bridge preclinical innovation and clinical impact.
A Glance at Diseases, Microanatomy, and Physiological Barriers of the Eye
Ocular diseases encompass a broad spectrum of conditions affecting both the anterior and posterior segments of the eye,31 each presenting distinct pathophysiological mechanisms, target tissues, and therapeutic challenges that collectively demand innovative drug delivery solutions. Anterior segment disorders, including dry eye disease (DED), infectious keratitis, and cataract, primarily compromise the corneal and conjunctival surfaces, the lacrimal apparatus, and the crystalline lens, whereas posterior segment pathologies such as age-related macular degeneration, diabetic retinopathy, and retinitis pigmentosa threaten the structural and functional integrity of the retina, choroid, and optic nerve. Conditions such as glaucoma and uveitis span multiple anatomical compartments, further compounding therapeutic complexity. Despite significant advances in pharmacological and surgical management, the majority of these conditions remain inadequately controlled by conventional treatment modalities, largely due to the eye’s formidable anatomical barriers, the chronic and progressive nature of most ocular diseases, and the absence of disease-modifying therapies for several major indications. Table 1 summarizes the key pathophysiological features, primary target tissues, and unmet therapeutic needs across the major ocular diseases discussed throughout this review.
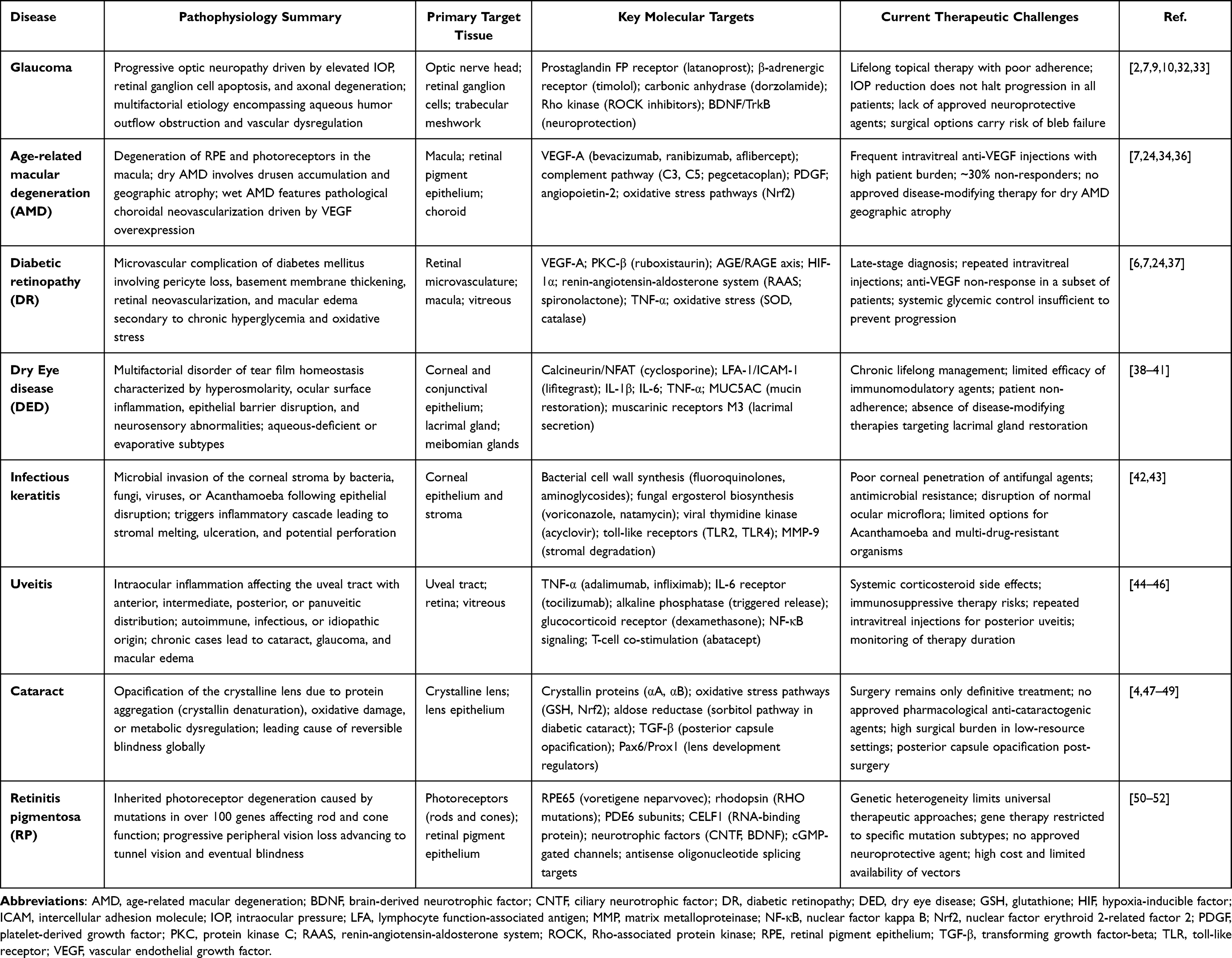 |
Table 1 Major Ocular Diseases: Pathophysiology, Primary Target Tissues, Key Molecular Targets, and Current Therapeutic Challenges |
The eye represents an extraordinarily complex organ whose visual function depends on the intricate coordination between specialized cellular components and optically transparent tissues. Central to maintaining ocular homeostasis is a sophisticated network of biological barriers that regulate the movement of molecules between systemic circulation and intraocular compartments.10 These barriers, while essential for preserving visual integrity and protecting delicate ocular structures, simultaneously present formidable obstacles to therapeutic agent penetration, which is a challenge that necessitates innovative drug delivery strategies for effective pharmacological intervention.53
As shown in Figure 2, ocular homeostasis is maintained through a multi-component barrier system, comprising the BAB and the BRB, which collectively govern molecular trafficking between the vasculature and intraocular tissues.9–12 Such barrier architectures serve multiple critical functions by (i) preserving the unique biochemical composition of ocular fluids through specific/selective molecular trafficking, (ii) maintaining appropriate intraocular pressure via regulated aqueous humor dynamics, and (iii) shielding sensitive neural tissues from potentially harmful blood-borne substances. For systemically or topically administered therapeutics to reach target sites within the posterior segment, they must successfully navigate these highly selective barriers, which significantly limits bioavailability and therapeutic efficacy of conventional formulations. Locally, in addition to the tear film, the corneal epithelial barrier is the outermost barrier (Figure 2Ai). In the following sections, we highlight the most important biological structure of the ocular barrier from a drug delivery and targeting standpoint.
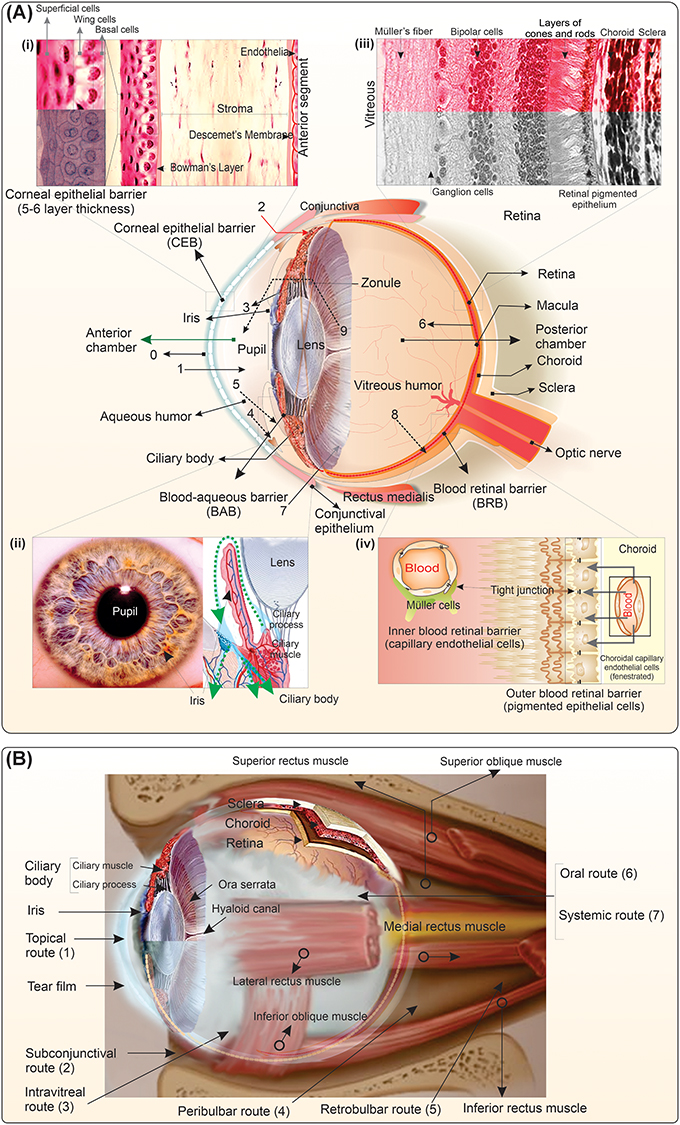 |
Figure 2 Anatomical illustration of ocular biological membranes and barrier systems. (A) Barriers of the eye, including (i) the corneal epithelial barrier (CEB), (ii) the blood-aqueous barrier (BAB), (iii) the retinal biological architecture, and (iv) the blood-retinal barrier (BRB) comprising both the inner endothelial and outer pigmented epithelial components. Multiple static and dynamic barriers orchestrate the maintenance of ocular homeostasis through coordinated regulatory functions. Various mechanisms are involved in the maintenance of vision function. (0) The precorneal tear layer constitutes the initial physiological barrier encountered by topically administered pharmaceutical formulations. (1) The stratified corneal structure presents a formidable obstacle that restricts penetration of topically applied therapeutics into the anterior chamber. (2) The conjunctival-scleral pathway offers the most permeable route for hydrophilic compounds and large molecular weight substances to bypass corneal barriers. (3) Following systemic administration, small molecular weight agents can traverse the fenestrated iris vasculature to access the anterior chamber compartment. (4) Pharmaceutical agents entering the anterior chamber undergo continuous elimination via aqueous humor drainage pathways. (5) Compounds present in the anterior chamber may be cleared into systemic venous circulation through diffusion across the iris surface – a function mediated by the blood-aqueous barrier. (6) Systemically delivered therapeutics must successfully penetrate dual blood-retinal barrier components: the outer barrier formed by retinal pigment epithelium (RPE) and the inner barrier constituted by retinal capillary endothelium (RCE). (7) Direct intravitreal injection enables pharmaceutical delivery directly into the vitreous cavity, bypassing anterior barriers. (8) Clearance of intravitreally administered agents occurs through uptake into retinal microvascular circulation. (9) Vitreal drug diffusion toward the anterior chamber represents an additional elimination pathway from the posterior segment. (B) The main routes for the administration of ophthalmologic drugs. Adapted with permission from.11 |
Blood-Aqueous Barrier
The BAB comprises two primary cellular components, which work synergistically to regulate molecular trafficking between systemic circulation and the anterior chamber (Figure 2Aii).54,55 The epithelial component consists of non-pigmented ciliary epithelial cells located in the ciliary body, which are interconnected by tight junctions (zonulae occludens) and actively participate in aqueous humor production while restricting paracellular diffusion. The vascular component is formed by the continuous, non-fenestrated endothelium of iris blood vessels, which exhibits tight junction complexes and demonstrates greater restrictiveness to molecular passage compared to ciliary body vasculature. Additional barrier-contributing structures include the posterior iris epithelium, a pigmented epithelial layer that reinforces barrier function in the iris region, and the inner wall endothelium of Schlemm’s canal, which forms part of the aqueous outflow pathway and regulates fluid egress from the anterior chamber. This multi-layered architectural arrangement ensures precise control of aqueous humor composition, maintains optical transparency, and protects the anterior segment from blood-borne pathogens and potentially harmful molecules. Located in the anterior eye, the BAB effectively restricts paracellular diffusion of hydrophilic molecules while maintaining the optical clarity and ionic homeostasis of aqueous humor. Notably, the permeability characteristics of these components differ substantially, in which iris vasculature excludes macromolecules exceeding 40 kDa, and ciliary body capillaries exhibit fenestrations that facilitate solute efflux toward systemic circulation. This asymmetry in permeability influences drug pharmacokinetics, with small lipophilic compounds experiencing rapid clearance (pilocarpine clearance: 13.0 µL/min in rabbit models) compared to larger hydrophilic molecules whose elimination approximates aqueous humor turnover rates (3.0–4.7 µL/min).55–58
Blood-Retinal Barrier
The posterior segment is protected by an even more restrictive barrier composed of inner and outer components (Figure 2 Aiii-Aiv). The inner BRB is formed by retinal capillary endothelial cells joined by continuous tight junctions with high transendothelial electrical resistance, functionally analogous to blood-brain barrier architecture. The outer barrier comprises retinal pigment epithelial cells with apical tight junctions that seal the subretinal space. Together, these barriers create a formidable impediment to drug penetration, evidenced by the substantially lower drug concentrations achieved in vitreous humor compared to aqueous humor following systemic administration.10,59–61 This differential permeability reflects the critical protective function of the BRB in preserving the metabolic sanctuary required for photoreceptor function yet simultaneously represents the primary bottleneck in posterior segment drug delivery (Figure 2B).
Multi-Layered Defense Through Active Barrier Mechanisms
The challenge of achieving therapeutic drug concentrations in target ocular tissues extends beyond anatomical barriers to encompass three integrated levels of protection. Static barriers include the stratified cellular architecture of cornea, sclera, conjunctiva, and the barrier-forming epithelia and endothelia described above. Each tissue layer presents distinct physicochemical properties; the corneal epithelium favors lipophilic penetration, while the underlying stroma permits hydrophilic diffusion, creating a biphasic permeability requirement that few molecules satisfy. Dynamic barriers continuously reduce drug bioavailability through physiological clearance mechanisms. Tear film turnover (16–20% per minute), conjunctival lymphatic drainage, nasolacrimal duct clearance, and high choroidal blood flow (the highest perfusion rate per tissue mass in the body) collectively eliminate the majority of topically applied drugs within minutes, limiting precorneal residence time and reducing absorption to typically less than 5% of the administered dose.9,10,62 Active efflux systems further restrict drug accumulation through ATP-binding cassette transporters, particularly P-glycoprotein and multidrug resistance-associated proteins, which are abundantly expressed in corneal and retinal epithelia, ciliary body, and vascular endothelia.63 These efflux pumps actively export a broad spectrum of therapeutic compounds, including many chemotherapeutics, antivirals, and corticosteroids, back into the tear film or systemic circulation. This multilayered barrier architecture, while varying in restrictiveness across ocular regions, collectively presents an enormous challenge to drug delivery that conventional formulations cannot adequately overcome (Figure 2B).
Current Landscape of Ocular Drug Delivery
The therapeutic management of ocular diseases relies predominantly on the established delivery routes, each with distinct advantages and limitations (Table 2). Topical administration through eye drops, ointments, and emulsions represents the most common approach due to its non-invasive nature, ease of self-administration, and patient acceptance.9,10 However, topical formulations face severe bioavailability challenges, with less than 5% of the administered dose penetrating intraocular tissues due to rapid precorneal clearance, nasolacrimal drainage, tear turnover, and the formidable barrier properties of the human corneal epithelium with relatively high transepithelial electrical resistance (TEER) value of ~300–500 Ω·cm2, and a permeability coefficient of ~1–5 × 10−6 cm/s for hydrophilic compounds.9,10 Intravitreal injections have become the gold standard for treating posterior segment diseases, particularly diabetic retinopathy and age-related macular degeneration, enabling direct delivery of therapeutic agents to the vitreous cavity and bypassing anterior barriers.24 Despite their efficacy, repeated intravitreal administrations carry significant risks, including endophthalmitis, retinal detachment, vitreous hemorrhage, and substantial patient burden. Systemic approaches through oral or intravenous routes offer convenience but necessitate high systemic doses to achieve therapeutic intraocular concentrations, leading to poor ocular bioavailability, potential systemic toxicity, and off-target effects. Additionally, intraocular implants and contact lens-based DDSs have been explored as alternative strategies, though each presents implementation challenges related to invasiveness, foreign body sensation, or limited drug loading capacity.11,64–66 The inadequacy of conventional delivery modalities has created substantial unmet clinical needs in ocular therapeutics. Critical limitations include inefficient drug delivery to posterior ocular segments, poor patient compliance with frequent dosing regimens, drug-related cytotoxicity to sensitive ocular tissues, and inability to maintain sustained therapeutic concentrations. The difficulty in monitoring dosage and therapy duration with topical preparations, combined with the potential disruption of resident ocular microflora, raises concerns about antimicrobial resistance development and treatment outcomes.67
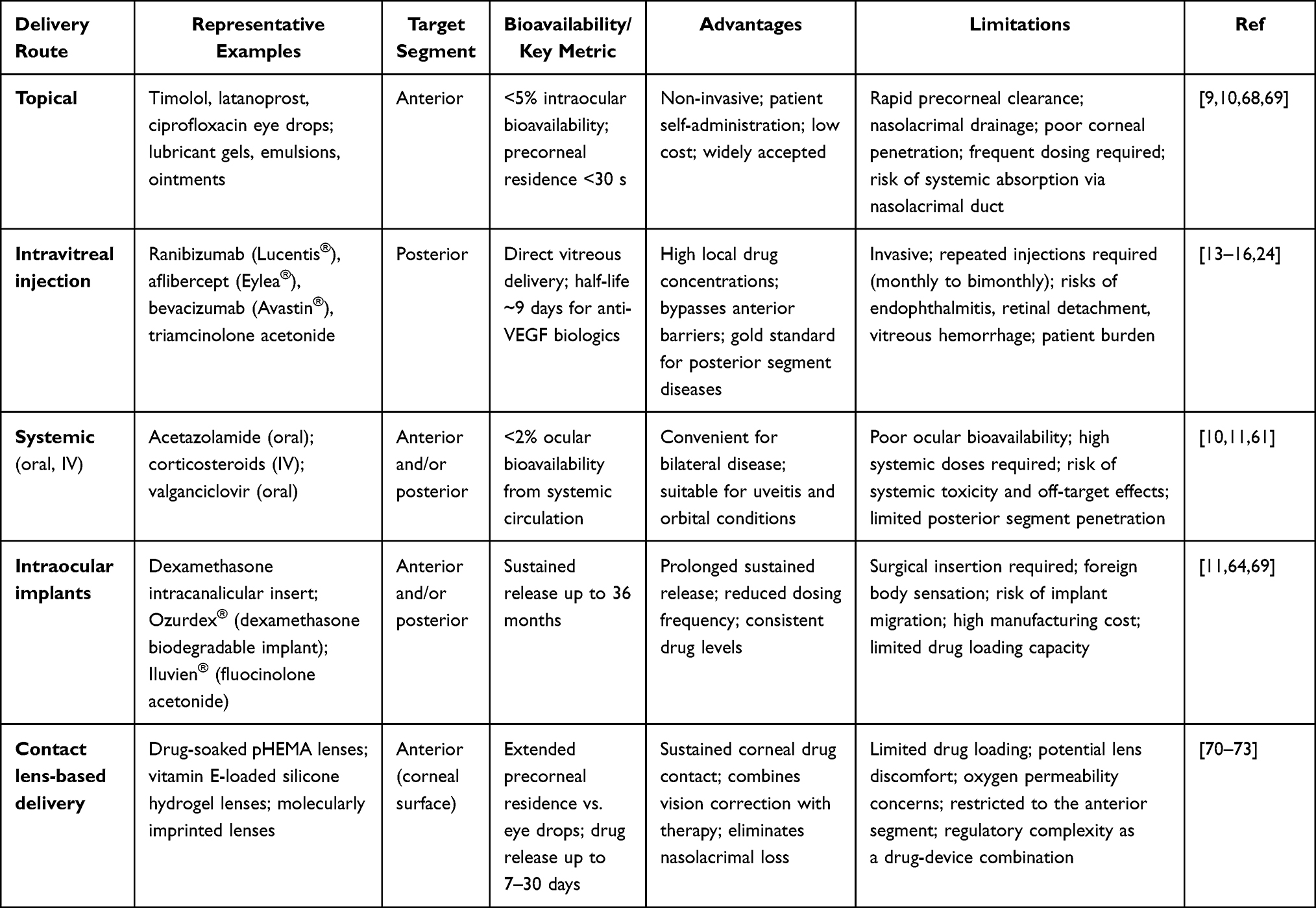 |
Table 2 Comparative Overview of Conventional Ocular Drug Delivery Routes: Advantages, Limitations, and Key Pharmacokinetic Parameters |
Many promising therapeutic agents, such as curcumin and other natural compounds with anti-inflammatory, antioxidant, and neuroprotective properties, remain clinically underutilized due to poor aqueous solubility, limited bioavailability, and rapid systemic elimination.23 These challenges necessitate innovative delivery platforms capable of overcoming anatomical barriers, providing controlled and sustained release, minimizing invasive procedures, and improving therapeutic outcomes across diverse ocular pathologies. Recent advances in biomaterial science and nanotechnology have catalyzed the development of next-generation ocular DDSs designed to address conventional limitations. Nanocarrier-based platforms (e.g., nanoparticles (NPs), nanosuspensions, nanofibers, nanogels, liposomes, micelles, and dendrimers) offer enhanced drug solubility, improved ocular penetration, and controlled release kinetics. Of these advancements, hydrogel systems have emerged as particularly promising candidates, with polysaccharide-based injectable hydrogels demonstrating excellent biocompatibility, tunable mechanical properties, and capacity for ocular barrier penetration.20 Remarkably, stimulus-responsive cellulose hydrogels represent a sophisticated evolution, capable of responding to environmental cues such as pH, temperature, and light to enable targeted drug release and tissue regeneration.22 These systems have been optimized for oral, nasal, and ocular administration, with emerging applications in advanced disease-specific therapies. Hybrid platforms combining nanocarriers with mucoadhesive hydrogels, cyclodextrin complexes, and biodegradable matrices enable sustained release and enhanced retention, supporting treatment of both anterior conditions like keratitis and dry eye syndrome, and posterior diseases including diabetic retinopathy and macular degeneration.
Hydrogel-Based Ocular DDSs
The development of effective ocular DDSs represents a persistent challenge in pharmaceutical sciences, primarily due to the eye’s sophisticated protective mechanisms and unique anatomical features. Conventional topical formulations, particularly eye drops, demonstrate remarkably poor bioavailability, typically below 5% of the administered dose, attributable to rapid precorneal clearance, tear film dilution, and nasolacrimal drainage. To overcome these limitations, a broad spectrum of nanotechnology-based platforms has been investigated, including liposomes, polymeric nanoparticles,NPs nanoemulsions, micelles, and dendrimers.66,68,74–78 While liposomes offer favorable biocompatibility and the capacity to encapsulate both hydrophilic and lipophilic drugs, they are limited by physical instability, drug leakage, and short precorneal residence time. Polymeric NPs, particularly poly(lactic-co-glycolic acid) (PLGA)-based systems, provide tunable and sustained drug release with excellent biodegradability, yet their small size, while advantageous for tissue penetration, limits bulk drug loading and extends manufacturing complexity.79,80 Nanoemulsions enhance corneal permeability through improved wettability and spreading but offer limited control over release kinetics.81–83 Dendrimers, despite their precise architecture and surface-functionalization potential, raise cytotoxicity concerns at higher generations that restrict clinical translation. In this context, hydrogel-based DDSs have emerged as particularly compelling platforms, uniquely combining mucoadhesive precorneal retention, stimuli-responsive in situ gelation, and the capacity to serve as macroscale depots for nanocarrier incorporation — advantages that individually available nanosystems cannot fully recapitulate. This synergistic versatility positions hydrogels not as replacements for nanocarrier technologies, but as integrative matrices that amplify their therapeutic potential within the demanding ocular microenvironment.68,69 These limitations necessitate frequent administration schedules, potentially compromising patient adherence and therapeutic outcomes. Hydrogels have emerged as transformative platforms for ocular therapeutics, offering distinctive advantages through their 3D crosslinked polymeric networks capable of retaining substantial quantities of water or biological fluids while maintaining structural integrity.84 Remarkably, the fundamental appeal of hydrogels in ophthalmic applications stems from their capacity to address multiple challenges simultaneously. These systems provide extended precorneal residence time through mucoadhesive interactions, enable controlled and sustained drug release kinetics, protect encapsulated therapeutic agents from degradation, and demonstrate excellent biocompatibility with ocular tissues.85 Furthermore, hydrogels can be engineered to respond to physiological stimuli, transforming from liquid to gel states upon exposure to specific triggers such as temperature, pH, or ionic strength changes, thereby facilitating ease of administration while ensuring prolonged retention at the target site.21 Figure 3 schematically illustrates composite hydrogels and gelation mechanisms.
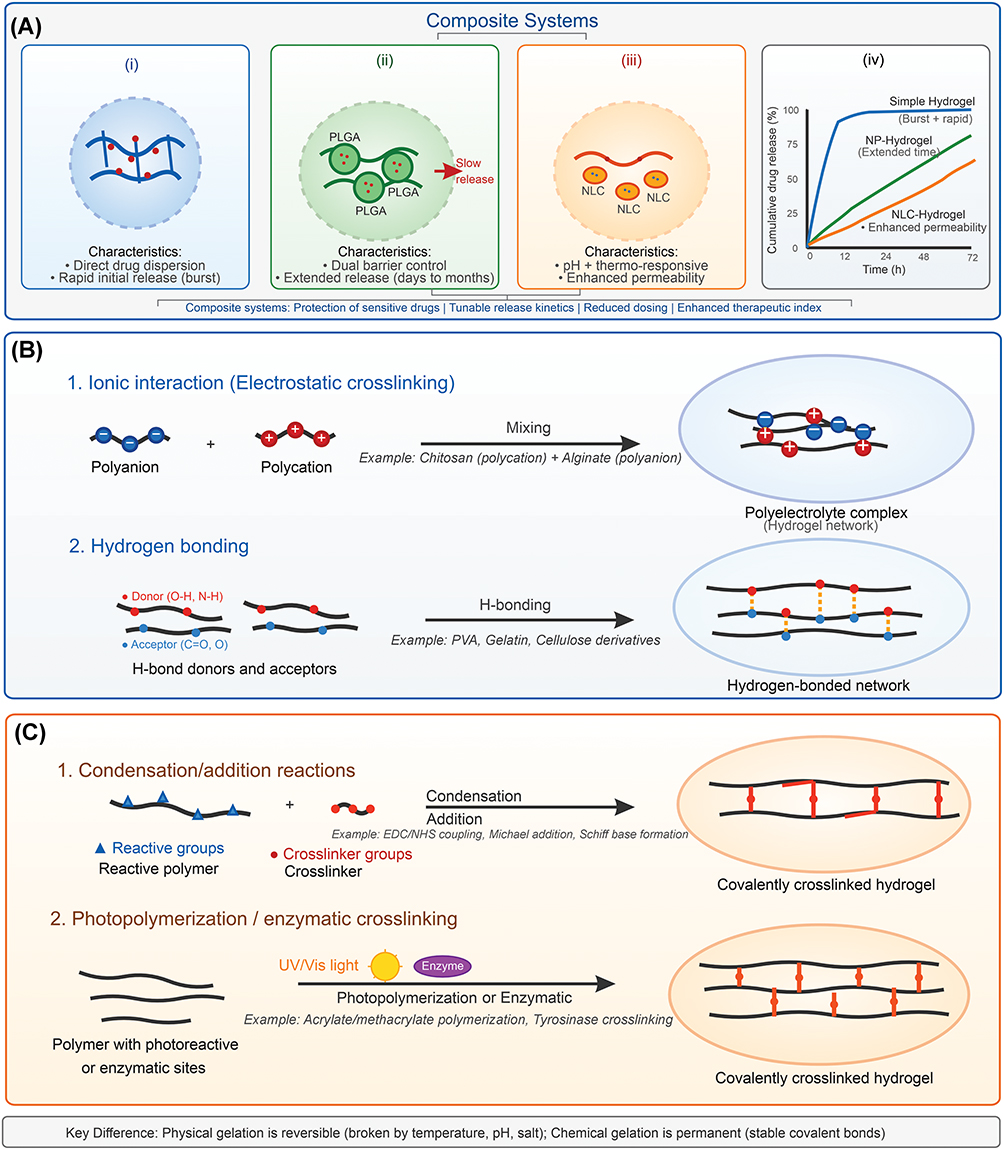 |
Figure 3 Composite hydrogels and gelation mechanisms. (A) Main categories of hydrogels, including (i) simple hydrogel with direct drug dispersion and rapid burst release, and composite systems comprising (ii) nanoparticle (NP)-loaded hydrogel with dual-barrier extended release, and (iii) nanostructured lipid carrier (NLC)-hydrogel with pH/thermo-responsive behavior, alongside comparative cumulative drug release profiles (iv). (B) Physical gelation mechanisms: 1. Ionic crosslinking, where polyanions (−) and polycations (+) interact electrostatically to form polyelectrolyte complexes; 2. Hydrogen bonding, where donors (red) and acceptors (blue) associate via H-bonds (dashed Orange lines), as seen in PVA, gelatin, and cellulose derivatives — both mechanisms being reversible. (C) Chemical gelation mechanisms: 1. Condensation/addition reactions, where distinguished reactive groups and bifunctional crosslinkers form permanent covalent networks via EDC/NHS coupling, Michael addition, or Schiff base formation; 2. Photopolymerization or enzymatic crosslinking, achieved through UV/Vis light activation or enzyme-mediated reactions at specific polymer sites, both yield irreversible, covalently crosslinked hydrogel networks. |
Classification and Design Strategies
Hydrogel-based ocular DDSs can be categorized according to several criteria, including polymer composition, crosslinking methodology, and responsiveness to environmental stimuli (Figure 3A). Table 3 represents selective polymers/biomaterials used in the formulation of ocular hydrogels. Natural polymer-based hydrogels, derived from materials such as chitosan, hyaluronic acid, alginate, gelatin, and cellulose, offer inherent biocompatibility, biodegradability, and minimal immunogenic potential.84,86 Chitosan-based formulations have garnered particular attention due to their cationic nature, which facilitates electrostatic interactions with negatively charged mucin layers, thereby enhancing corneal adhesion and penetration (Figure 3B).87,88 Hyaluronic acid, a naturally occurring component of ocular tissues, provides exceptional viscoelastic properties and promotes wound healing, making it particularly suitable for anterior segment applications.89 Synthetic polymer-based hydrogels, including those derived from poly(N-isopropylacrylamide), polyethylene glycol (PEG), poly(2-hydroxyethyl methacrylate) (pHEMA), and poloxamer formulations, offer advantages in terms of reproducible synthesis, tunable physicochemical properties, and predictable degradation profiles (Figure 3B).70,90 Thermosensitive hydrogels, particularly those based on Pluronic F-127 (poloxamer 407), demonstrate sol-gel phase transitions at physiologically relevant temperatures, existing as free-flowing solutions at ambient conditions while forming semi-solid gels at ocular surface temperatures.91,92 This temperature-responsive behavior facilitates straightforward instillation as liquid drops that subsequently gel in situ, significantly extending drug residence time without causing application discomfort. Collectively, natural hydrogels offer superior biocompatibility, biodegradability, and cell-interactive properties. They also might have some limitations, including batch-to-batch variability, limited mechanical tunability, and potential immunogenicity from animal-derived sources. Synthetic hydrogels offer reproducible synthesis, precise tuning of crosslinking density and degradation, while their limitations include potential cytotoxicity of monomers, non-degradability of some variants, and lack of intrinsic bioactivity.
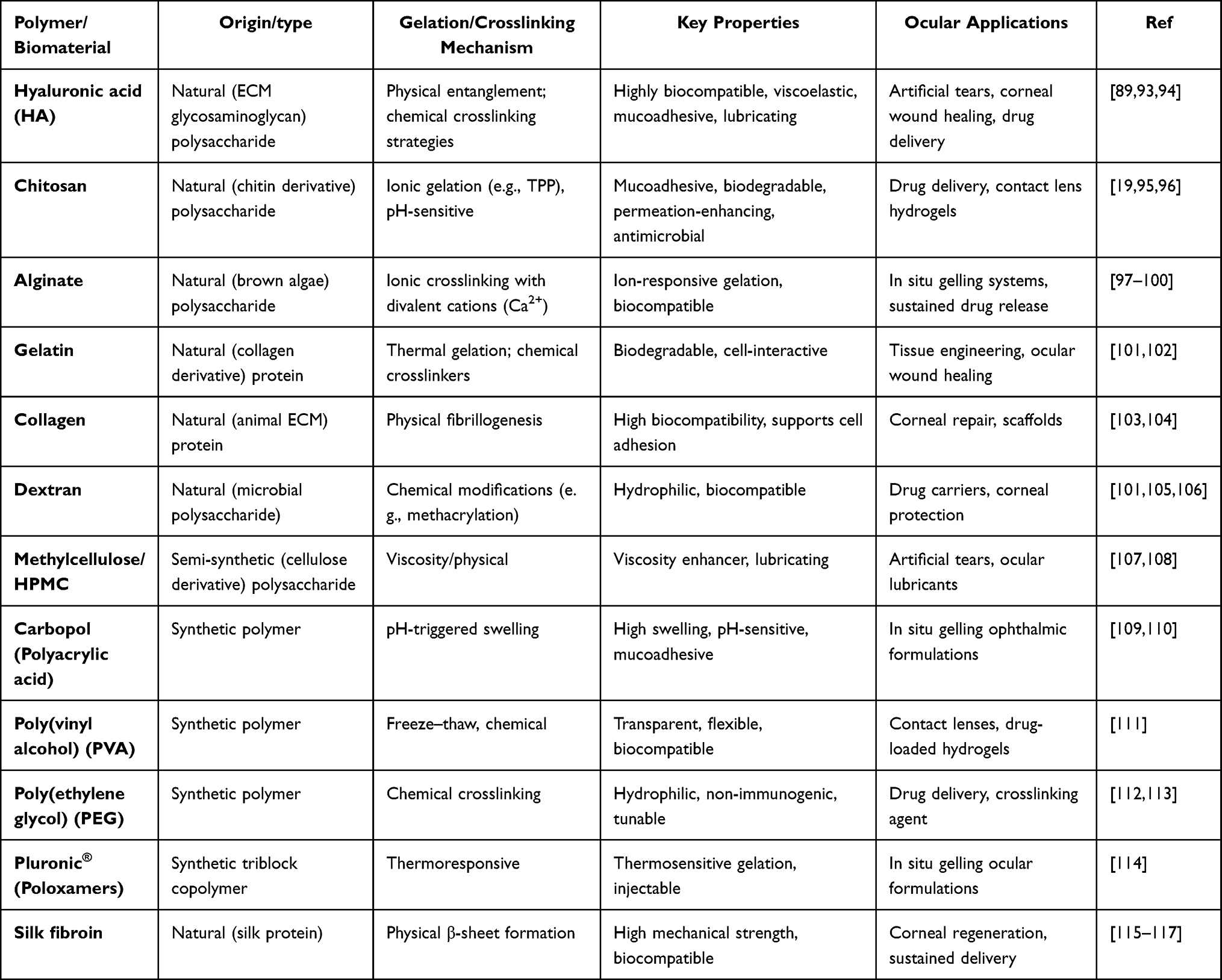 |
Table 3 Physicochemical Properties and Ocular Applications of Selected Polymers and Biomaterials Used in Hydrogel Development |
Preparation and Fabrication Techniques
Ionic Crosslinking
Ionic crosslinking is among the most widely employed and scalable strategies for fabricating ocular hydrogels, exploiting electrostatic interactions between oppositely charged polymer chains or between polyanionic polymers and multivalent cations to form physically crosslinked networks without cytotoxic chemical agents. Alginate hydrogels are prototypically prepared through exposure to divalent calcium ions (Ca2⁺), which coordinate with guluronate blocks to yield stable gel matrices suitable for vitreous substitution and sustained drug release.98,118 Gellan gum undergoes in situ ionic gelation upon contact with cations naturally present in tear fluid (Na⁺, K⁺, Ca2⁺, Mg2⁺), enabling seamless sol-to-gel transition on the ocular surface following instillation.98 Chitosan-based systems are similarly crosslinked using tripolyphosphate (TPP) or through polyelectrolyte complexation with anionic polymers such as hyaluronic acid, yielding NPs or hydrogel matrices with favorable mucoadhesive and permeation-enhancing properties relevant to anterior segment drug delivery.88
Photopolymerization
Photopolymerization enables rapid, spatially controlled covalent crosslinking of functionalized polymer precursors upon UV or visible light exposure, producing hydrogels with precisely tunable mechanical properties and network density for in vitro and in vivo applications.71,119 Methacrylated derivatives of hyaluronic acid and polyethylene glycol diacrylate (PEGDA) are the most frequently employed precursors, forming crosslinked networks within seconds to minutes in the presence of photoinitiators such as lithium phenyl-2,4,6-trimethylbenzoylphosphinate (LAP).120,121 For intravitreal applications, this approach enables in situ depot formation following injection of a liquid precursor, with subsequent UV-triggered crosslinking producing mechanically stable systems capable of releasing therapeutic agents over periods exceeding 90 days.121 Critical formulation considerations include photoinitiator cytotoxicity, light penetration depth through ocular tissues, and the degree of polymer functionalization, which collectively govern crosslink density, equilibrium swelling, and drug diffusion kinetics.120
Thermosensitive Sol-Gel Methods
Thermosensitive hydrogel systems exploit the lower critical solution temperature (LCST) behavior of specific polymers to undergo reversible sol-to-gel transitions driven by the temperature differential between ambient conditions (~25°C) and the ocular surface (32–35°C). Poloxamer 407 is the archetypal thermogelling polymer for ophthalmic formulation, forming packed micellar networks at concentrations of 15–25% w/v as the temperature exceeds its critical micelle temperature.92 To mitigate the ocular irritation associated with high poloxamer concentrations, combinatorial systems incorporating hydroxypropyl methylcellulose (HPMC) or Carbopol 940 as viscosity-enhancing co-polymers have been developed to reduce individual component concentrations while preserving gelation performance. 92 Biodegradable triblock systems such as PLGA-PEG-PLGA undergo thermally driven gelation at physiological temperatures, with the added benefit of hydrolytic erosion contributing to sustained drug release profiles over days to weeks.91 Chitosan-based thermosensitive formulations incorporating β-glycerophosphate as a gelation mediator achieve sol-gel transitions at near-neutral physiological pH, overcoming the acid-solubility limitation of native chitosan and enabling sustained drug release profiles extending beyond 120 hours.87
Electrospinning for Nanofiber Hydrogels
Electrospinning generates ultrafine polymer fibers with diameters ranging from tens of nanometers to several micrometers through the application of high-voltage electric fields to polymer solutions, producing fibrous scaffolds with high surface area-to-volume ratios, interconnected porosity, and structural resemblance to native extracellular matrix. In ocular drug delivery, electrospun matrices fabricated from biocompatible polymers (e.g., PLGA, poly(ε-caprolactone) (PCL), gelatin, and silk fibroin) have been investigated as sustained-release platforms for corneal wound healing, conjunctival delivery, and subconjunctival implantation.68 Upon hydration, these fibrous scaffolds transition into hydrogel-like states with tunable swelling and drug release characteristics governed by fiber diameter, polymer molecular weight, and drug-polymer miscibility. Co-axial electrospinning, which produces core-shell fiber architectures, enables independent optimization of drug loading in the core and release-modulating shell composition, providing an additional degree of formulation control critical for achieving desired ocular pharmacokinetic profiles.122 Key process parameters, including applied voltage, polymer flow rate, needle-to-collector distance, and solution concentration, must be rigorously optimized to ensure reproducible fiber morphology and homogeneous drug distribution.
Microfluidic-Assisted Preparation of Nanocomposite Systems
Microfluidic platforms have emerged as powerful tools for preparing drug-loaded nanocarriers and nanocomposite hydrogel systems with superior size uniformity, reproducibility, and scalability compared to conventional bulk nanoprecipitation or emulsification methods.123,124 By precisely controlling fluid flow through engineered microscale channels, these devices enable continuous, high-throughput production of lipidic and polymeric NPs, and liposomes with narrow polydispersity indices (PDI < 0.15) and reproducible surface charge profiles, which are parameters directly influencing ocular permeability and precorneal retention.20 Droplet-based microfluidic systems employing immiscible fluid streams generate monodisperse emulsion droplets that serve as templates for microsphere fabrication, which are subsequently embedded within thermosensitive or photopolymerizable hydrogel matrices to produce nanocomposite intravitreal depot systems with precisely controlled initial burst and sustained release phases.125 The integration of inline process analytical technology (PAT) within microfluidic workflows, including real-time dynamic light scattering (DLS) and UV absorbance monitoring, enables continuous quality verification consistent with QbD principles, supporting regulatory compliance and future scale-up translation.27
Characterization Techniques for Ocular Hydrogel Drug Delivery Systems
Physicochemical and Colloidal Characterization
Comprehensive physicochemical characterization of ocular hydrogel DDSs and their incorporated nanocarriers is fundamental to establishing structure–property–performance relationships that govern clinical outcomes. Particle size, size distribution, and polydispersity index (PDI) are routinely determined by DLS, with nanocarriers intended for corneal penetration generally requiring mean hydrodynamic diameters below 200 nm and PDI values below 0.2 to ensure homogeneous tissue distribution and avoid aggregation-mediated clearance.125 Zeta potential measurement, likewise performed by laser Doppler electrophoresis, provides critical information regarding colloidal stability and mucoadhesive potential; cationic surfaces (typically +15 to +30 mV) promote electrostatic interaction with negatively charged mucin glycoproteins, enhancing precorneal retention.88 Drug encapsulation efficiency and loading capacity are quantified by indirect methods following nanocarrier separation via ultracentrifugation or ultrafiltration, using UV–Vis spectrophotometry or high-performance liquid chromatography (HPLC) as appropriate to the physicochemical properties of the encapsulated agent.68
Rheological Characterization
Rheological assessment is indispensable for thermosensitive and in situ gelling systems, as it directly determines injectability, gelation kinetics, and mechanical durability under physiological conditions. Oscillatory amplitude and frequency sweep experiments yield the storage modulus (G′) and loss modulus (G″), with the sol-to-gel transition temperature identified at the G′/G″ crossover point; ocular hydrogels typically require G′ values in the range of 102 to 104 Pa following gelation to resist precorneal clearance while maintaining tissue compliance.126 Viscosity profiling under increasing shear rates characterizes shear-thinning behavior, a property essential for formulations requiring passage through fine-gauge needles (27–30 G) during intravitreal administration without mechanical disruption of the gel network.127 Temperature ramp experiments conducted between 20°C and 37°C at a fixed oscillatory frequency confirm appropriate sol-gel transition windows relative to ambient instillation and ocular surface temperatures.92
Morphological and Optical Characterization
Scanning electron microscopy (SEM) and transmission electron microscopy (TEM) provide direct visualization of hydrogel microarchitecture, pore size distribution, nanoparticle morphology, and homogeneity of nanocarrier dispersion within the hydrogel matrix — parameters that collectively govern drug diffusion pathways and release kinetics.126 Atomic force microscopy complements electron microscopy by quantifying surface topography and nanomechanical properties under hydrated conditions, more accurately reflecting the in situ state of the hydrogel. For formulations intended for anterior segment application, optical transparency is an essential functional parameter assessed by UV–Vis transmittance spectroscopy at wavelengths spanning the visible spectrum (400–700 nm), with clinically acceptable systems typically demonstrating transmittance exceeding 90%.19,66 Refractive index measurements using Abbe refractometry further confirm that incorporated nanocarriers and polymer matrices do not introduce optical distortions incompatible with corneal or contact lens applications.
Drug Release, Permeation, and in vivo Evaluation
In vitro drug release studies employing simulated tear fluid (STF, pH 7.4, 37°C) or phosphate-buffered saline in dialysis membrane assemblies or Franz diffusion cells provide foundational pharmacokinetic data, with release profiles fitted to mathematical models (e.g., zero-order, Higuchi, and Korsmeyer–Peppas equations) to elucidate dominant release mechanisms such as diffusion, erosion, or anomalous transport.34 Ex vivo transcorneal permeation studies using freshly excised porcine or bovine corneas mounted in modified Franz diffusion cells yield apparent permeability coefficients (Papp) that more accurately reflect the barrier properties of native tissue compared to membrane-based assays, enabling direct formulation comparison under physiologically relevant conditions.128 Cytotoxicity assessment employing MTT (3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium Bromide) cell viability, live/dead, and annexin V/propidium iodide assays on human corneal epithelial cell lines (HCE-T), human umbilical vein endothelial cells (HUVECs), or retinal pigment epithelial cells (ARPE-19) confirms the tolerability of hydrogel components and degradation products at clinically anticipated concentrations.18 In vivo pharmacokinetic evaluation in rabbit models, the regulatory standard for ocular formulation assessment, involves serial sampling of aqueous humor and vitreous humor at predetermined intervals following topical or intravitreal administration, with drug quantification by LC-MS/MS enabling determination of area under the curve (AUC), maximum concentration (Cmax), and ocular half-life (t½) parameters essential for clinical dose projection.129
Thermosensitive in situ Gelling Systems
Thermosensitive hydrogels represent one of the most extensively investigated platforms for ophthalmic delivery, with poloxamer-based formulations demonstrating particular clinical promise. However, the high polymer concentrations (20–25% w/v) traditionally required for adequate gelation can induce ocular irritation. Consequently, researchers have developed combinatorial approaches incorporating poloxamer with complementary polymers to reduce individual component concentrations while maintaining or enhancing gelling capacity.92 For instance, the integration of hydroxypropyl methylcellulose (HPMC) as a viscosity-enhancing agent, or pH-sensitive polymers such as Carbopol 940, enables formulation optimization with reduced side effect profiles.32
Chitosan-based thermosensitive systems, particularly those incorporating β-glycerophosphate or disodium α-D-glucose 1-phosphate as gelation mediators, have demonstrated remarkable efficacy in preclinical evaluations. Chen et al (2012) reported that chitosan/disodium α-D-glucose 1-phosphate hydrogels exhibited appropriate sol-gel transition temperatures, maintained physiological pH ranges, and achieved sustained release profiles extending beyond 120 hours.87 These formulations demonstrated significantly prolonged ocular residence times and enhanced corneal penetration of model drugs compared to conventional aqueous solutions. For glaucoma management, chitosan-based thermosensitive hydrogels loaded with latanoprost maintained therapeutic intraocular pressure reduction for up to 21 days following a single topical application in triamcinolone-induced ocular hypertension models.129
Triblock copolymer systems, particularly those incorporating biodegradable segments, offer additional advantages for sustained intraocular delivery. PEG-polycaprolactone-PEG (PECE) thermosensitive hydrogels demonstrate sol-gel transitions near physiological temperatures while providing extended drug release profiles. Luo et al (2016) demonstrated that 30% (w/v) PECE hydrogels containing diclofenac sodium achieved sustained release over seven days, with pharmacokinetic studies revealing 1.6-fold enhancement in area under the curve compared to commercial eye drops.130 More sophisticated designs incorporating poly(trimethylene carbonate) segments have achieved even longer degradation times exceeding two weeks, making them particularly suitable for post-surgical applications such as glaucoma filtration surgery where controlled release of mitomycin C can prevent excessive scarring.131
Contact Lens-Based Drug Delivery Platforms
Therapeutic contact lenses represent an innovative approach to ocular drug delivery, combining vision correction functionality with sustained pharmaceutical release capabilities. Both conventional hydrogel and silicone hydrogel contact lenses have been investigated as drug delivery vehicles, with various strategies employed to enhance drug loading capacity and extend release duration. Silicone hydrogel lenses, composed of materials such as bitelechelic methacrylated polydimethylsiloxanes and N,N-dimethylacrylamide (i.e., with reactive functional groups at both chain ends), offer superior oxygen permeability compared to conventional hydrogels, an essential consideration for maintaining corneal health during extended wear.71 Drug loading methodologies for contact lens systems include soaking lenses in drug solutions, incorporating drug-loaded NPs within the lens matrix, or chemical modification of lens materials to enhance drug-matrix interactions. Lee et al (2016) demonstrated that co-loading lipophilic vitamins, specifically vitamin E, into pHEMA-hydrogel contact lenses significantly increased loading capacity for hydrophilic drugs such as timolol and brimonidine by 19.1% and 18.7%, respectively.72 This enhancement stems from the creation of additional hydrophobic domains within the hydrogel matrix that can sequester hydrophilic drugs through altered partition coefficients. More sophisticated approaches incorporate drug-loaded nanocarriers within contact lens matrices, creating composite systems that provide enhanced control over release kinetics. Lu et al (2013) developed pHEMA-based hydrogels containing silica shell cross-linked micelles loaded with dexamethasone acetate, achieving sustained release extending up to 30 days while maintaining optical transparency suitable for vision applications.70 The rod-like morphology of the silica shell cross-linked micelles contributed to prolonged release by creating tortuous diffusion pathways within the hydrogel network. Molecular imprinting techniques have also been employed to create binding sites with specific affinity for target drugs, as demonstrated by Varela-Garcia et al (2020) who developed cytosine-functionalized hydrogels for controlled release of transferulic acid, an antioxidant compound with therapeutic potential for age-related ocular diseases.73
Nanocomposite Hydrogel Systems
The integration of drug-loaded NPs within hydrogel matrices represents an advanced strategy that combines the advantages of both nanoscale and macroscale DDSs (Figure 3). Nanocarrier design parameters critically govern ocular permeability and therapeutic performance within composite hydrogel systems. Particle size is a primary determinant of corneal penetration, with sub-200 nm NPs demonstrating favorable transcorneal transport, while particles exceeding 500 nm are largely restricted by tight junction complexes of the corneal epithelium.10,125 Surface charge similarly influences tissue interactions, as cationic NPs bearing positive zeta potentials interact electrostatically with negatively charged mucin glycoproteins, enhancing mucoadhesion and prolonging precorneal retention;87,88 for instance, the dexamethasonloaded chitosan NPs (DEX-CSNPs) incorporated in our poloxamer 407/gellan gum hydrogel system exhibited a zeta potential of +20.3 mV, supporting favorable corneal adhesion.18 Anionic NPs, by contrast, may exploit alternative transcorneal transport pathways, including transcytosis and lipid membrane interactions.88,95 Drug loading parameters, specifically encapsulation efficiency and loading capacity, directly determine the therapeutic dose achievable per administration and the magnitude of initial burst release; the DEX-CSNPs reported in our formulation achieved an EE of 29.4% and LC of 6.5%, values that governed the biphasic release profile observed within the hydrogel matrix.18,34 Collectively, rational optimization of these physicochemical parameters is essential for designing nanocomposite hydrogels that balance sustained drug release with adequate ocular bioavailability.125
These nanocomposite platforms provide dual control over drug release, with nanoparticle encapsulation protecting drugs from premature degradation while the hydrogel matrix extends precorneal retention and provides an additional diffusion barrier.125 PLGA NPs have been extensively employed due to their FDA-approved status, tunable degradation profiles, and capacity for sustained drug release. Several research groups have demonstrated the efficacy of microsphere-hydrogel composite systems for treating posterior segment diseases. Osswald et al (2017) developed an injectable system combining ranibizumab-loaded PLGA microspheres within a poly(N-isopropylacrylamide)-based thermosensitive hydrogel, achieving bioactive drug release for approximately 200 days in vitro.132 In a laser-induced choroidal neovascularization model, this system reduced lesion areas by 60% compared to non-treated controls, achieving superior therapeutic efficacy with drug quantities one order of magnitude lower than required for bolus injections. The controlled release profile minimized peak drug concentrations while maintaining therapeutic levels throughout the treatment period, potentially reducing toxicity concerns associated with high-dose bolus administrations.133 Biodegradable hydrogel designs incorporating degradable crosslinkers further enhance the sustainability of drug release. Liu et al (2019b) synthesized poly(ethylene glycol)-co-(L-lactic acid) diacrylate/N-isopropylacrylamide hydrogels with varying crosslinker concentrations, demonstrating that systems with 3 mM crosslinker concentration achieved optimal balance between injectability through 28-gauge needles, appropriate mechanical properties, and degradation-mediated drug release (Figure 3C, mechanism 1).127 These formulations released bioactive aflibercept in a controlled manner over six months, with in vitro assays confirming maintenance of anti-VEGF activity throughout the release period. Hybrid systems incorporating both nanostructured lipid carriers and stimuli-responsive hydrogels have demonstrated synergistic benefits for anterior segment applications. In this line, photopolymerization and enzymatic crosslinking (Figure 3C, mechanism 2) represent two distinct yet complementary strategies for generating permanent covalent hydrogel networks, achieved respectively through UV/Vis light-induced radical initiation at photoactive polymer sites and enzyme-catalyzed bond formation under physiologically mild conditions. Yu et al (2019, 2020) developed genipin-crosslinked carboxymethyl chitosan/poloxamer 407 hydrogels containing baicalin-loaded nanostructured lipid carriers, achieving both pH and temperature responsiveness.128,134 The dual-sensitive nature enabled triggered release in response to inflammatory conditions while maintaining prolonged precorneal retention. Ex vivo permeation studies revealed 4.46-fold enhancement in apparent permeability coefficient compared to conventional eye drops, attributed to the combined effects of nanocarrier-mediated transcorneal penetration and hydrogel-mediated residence time extension.128
Supramolecular and Cyclodextrin-Based Hydrogels
Supramolecular hydrogels, formed through non-covalent interactions such as host-guest inclusion complexes, hydrogen bonding, or π-π stacking, offer unique advantages including reversibility, self-healing properties, and injectability without requiring chemical crosslinking agents. Zhang et al (2016) fabricated micellar supramolecular hydrogels composed of low-molecular-weight methoxy polyethylene glycol block polymers and α-cyclodextrin, achieving gelation through host-guest inclusion of polymer chains within cyclodextrin cavities.122 These systems exhibited thixotropic behavior, enabling them to flow under shear stress during instillation while recovering gel structure upon rest, thereby extending corneal surface retention. In vivo pharmacokinetic studies demonstrated significant improvements in ocular bioavailability compared to micellar formulations without the hydrogel component. Cyclodextrin-based hydrogels offer additional functionality through their capacity to form inclusion complexes with hydrophobic drugs, enhancing solubility and stability. Glisoni et al (2013) developed β-cyclodextrin-conjugated pHEMA soft contact lenses for delivery of antimicrobial thiosemicarbazones, demonstrating controlled release extending over two weeks with drug concentrations maintained within the therapeutic window.135 The inclusion complex formation protected the drug from degradation while modulating release kinetics. Super-hydrophilic hydrogels composed of directly crosslinked hydroxypropyl-β-cyclodextrin provided even higher drug loading capacities, though with more rapid release profiles due to their enhanced swelling behavior. Prodrug supramolecular hydrogels represent an innovative approach where the drug molecule itself participates in hydrogel network formation. Zhang et al (2018) synthesized succinated dexamethasone derivatives capable of self-assembling into nanofibrous supramolecular hydrogels through π-π stacking and hydrophobic interactions.136 These systems provided dual release of both the prodrug and the active dexamethasone generated through hydrolytic cleavage of the succinate ester. The pH-dependent hydrolysis rate enabled modulation of the ratio between prodrug and active drug released, with initial pH values significantly influencing release profiles. This “self-delivery” approach eliminated the need for carrier polymers, potentially reducing manufacturing complexity and regulatory requirements.
Characterization and Performance Evaluation
Comprehensive characterization of hydrogel-based ocular DDSs encompasses multiple parameters essential for predicting clinical performance (Figure 4). Rheological characterization, including determination of sol-gel transition temperatures, gelation kinetics, storage and loss moduli, and shear-thinning behavior, provides critical insights into injectability and in situ gel formation capacity (Figure 4A).126 Thermosensitive hydrogels must exhibit appropriate viscosity at room temperature for ease of instillation while achieving sufficient gel strength at ocular temperatures (32–35°C) to resist clearance mechanisms. Morphological characterization through scanning electron microscopy reveals hydrogel microstructure, including pore size distribution, network architecture, and distribution of incorporated nanocarriers (Figure 4B). Pore size significantly influences drug diffusion coefficients and release kinetics, with larger pores generally facilitating more rapid release.90 Optical properties, particularly transparency and refractive index, are critical for formulations intended for application on optically active surfaces such as the cornea or integration into contact lenses (Figure 4B). Mechanical testing, including compressive strength and elastic modulus measurements, ensures formulations can withstand physiological stresses without mechanical failure. Swelling studies quantify hydrogel hydration capacity and dimensional changes in response to aqueous environments, parameters that directly impact drug loading capacity and release mechanisms (Figure 4C). Drug release characterization typically employs in vitro dissolution studies using simulated tear fluid or phosphate-buffered saline, with sampling at predetermined intervals to construct release profiles. Mathematical modeling of release data using equations such as the Higuchi model, Korsmeyer-Peppas model, or zero-order kinetics provides mechanistic insights into release mechanisms, distinguishing between diffusion-controlled, erosion-controlled, or combined release patterns (Figure 4D).34 Ex vivo transcorneal permeation studies using excised animal corneas mounted in Franz diffusion cells provide more physiologically relevant data regarding drug penetration through ocular barriers (Figure 4D). Most importantly, bioactivity assays confirm that released therapeutics retain pharmacological potency following encapsulation and release from the hydrogel matrix, a critical requirement particularly for protein-based agents (e.g., anti-VEGF biologics and corticosteroids) vulnerable to conformational destabilization or aggregation during fabrication and storage. Functional validation employs cell-based proliferation inhibition assays, receptor-binding affinity measurements, and immunoreactivity quantification to confirm preserved molecular integrity throughout the release period (Figure 4E). Complementing these in vitro assessments, preclinical in vivo studies in rabbit and rodent models utilize serial aqueous and vitreous humor sampling to construct pharmacokinetic profiles, benchmarking hydrogel formulations against conventional approaches (Figure 4F). Ocular safety is evaluated through slit-lamp biomicroscopy, intraocular pressure monitoring, electroretinography, and optical coherence tomography, identifying potential inflammatory or structural sequelae arising from polymer constituents or degradation byproducts. Disease-specific efficacy is substantiated through quantifiable endpoints, including intraocular pressure reduction in glaucoma models, neovascular lesion suppression in choroidal neovascularization paradigms, and retinal architecture preservation in diabetic retinopathy models, collectively establishing the preclinical evidentiary foundation necessary to advance these platforms toward clinical translation.137
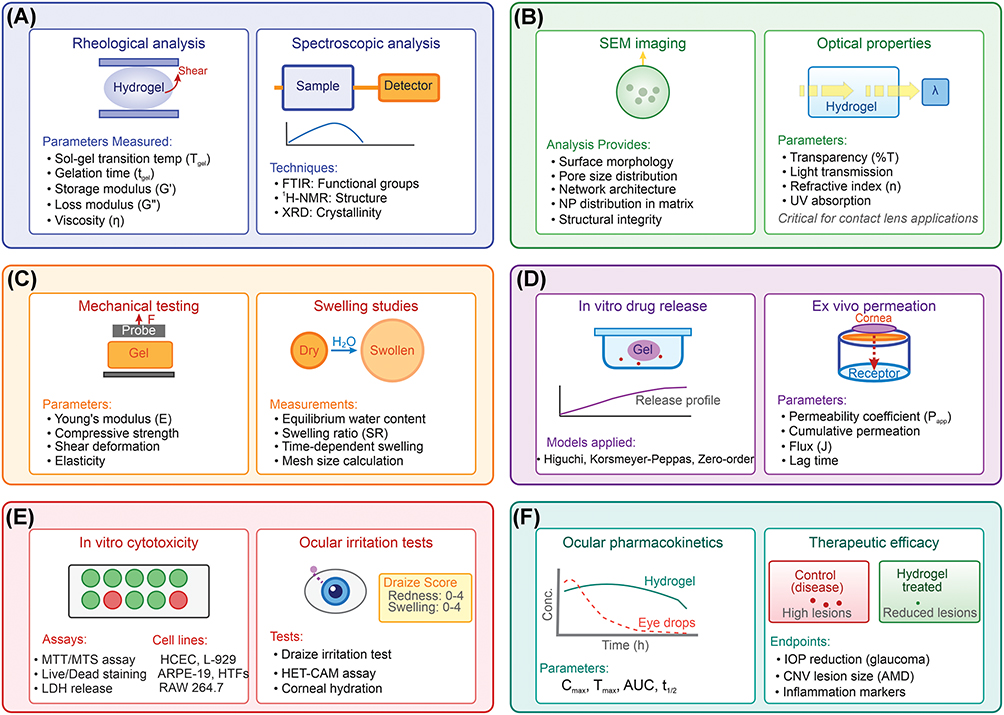 |
Figure 4 Characterization and evaluation methods for ocular hydrogels. (A) Physicochemical characterization. (B) Morphological and optical characterization (arrow indicates light absorption/transmission). (C) Mechanical and swelling properties. (D) Drug release and permeation analyses. (E) Biocompatibility and safety evaluation. (F) In vivo evaluation. |
Hydrogel Applications in Ocular Diseases
The distinctive 3D, highly hydrated polymeric network of hydrogels, combined with their inherent biocompatibility, tunable mechanical properties, and capacity to mimic the viscoelastic nature of native ocular tissues, has positioned them as versatile platforms for ophthalmic applications. Accordingly, a broad spectrum of natural, synthetic, and hybrid hydrogel formulations has been investigated both as DDSs, enabling controlled and sustained release of therapeutic agents to anterior and posterior ocular compartments, and as biomatrices for ocular tissue engineering, where they provide a structurally supportive microenvironment conducive to the adhesion, proliferation, and differentiation of corneal, trabecular, and retinal cell populations. In this line, to analyze the impacts of ophthalmic DDSs, various 3D models have been developed (Table 4).
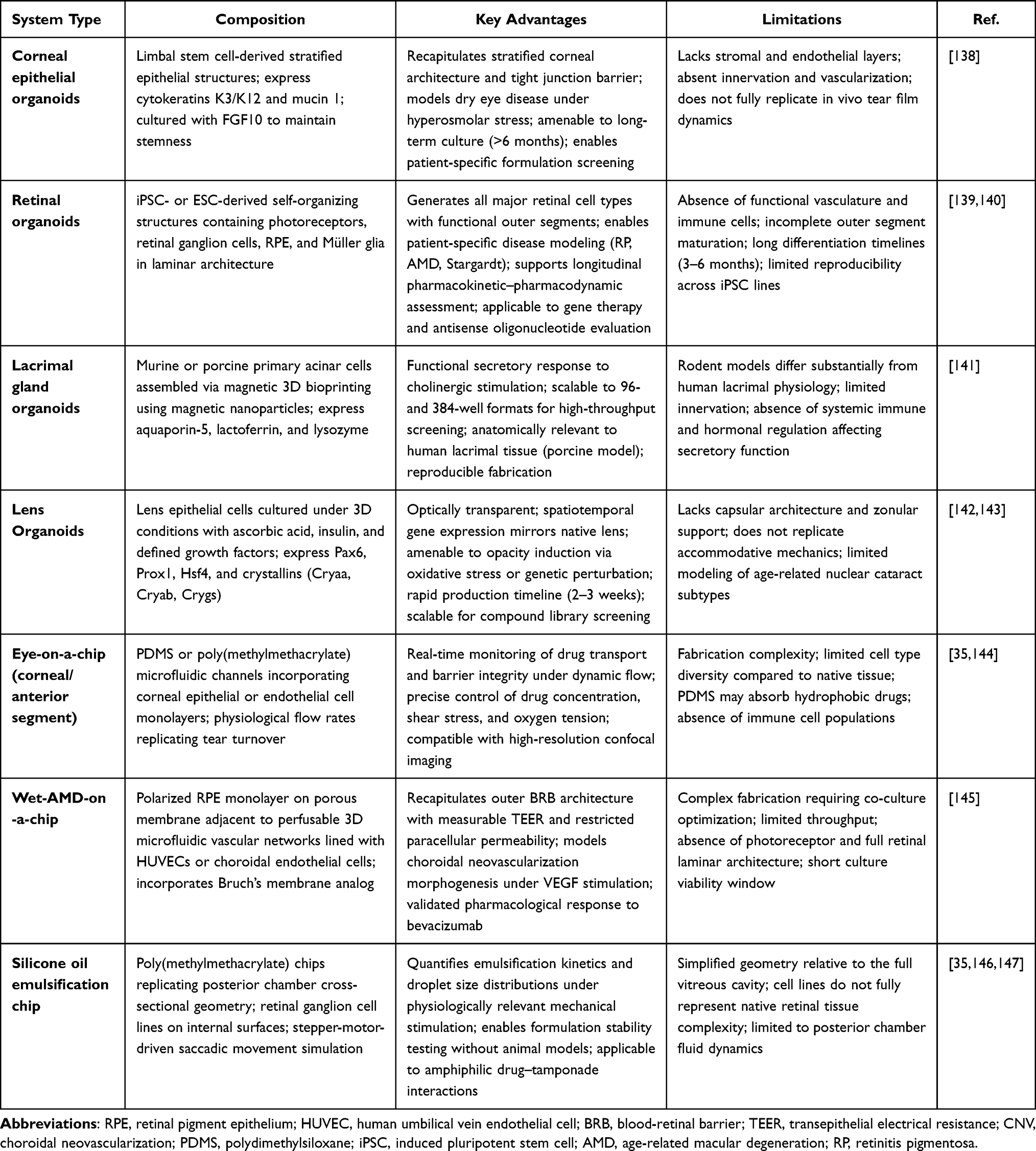 |
Table 4 Summary of Transformative 3d Ocular Tissue Models for Drug Delivery Research |
Anterior Segment Diseases
Hydrogel-based delivery systems have demonstrated particular efficacy for treating anterior segment conditions, including glaucoma, DED, bacterial and fungal infections, and inflammatory disorders. For glaucoma management, sustained delivery of intraocular pressure-lowering medications such as latanoprost, timolol, and brimonidine have been achieved through various hydrogel formulations. Pakzad et al (2020) developed quaternized chitosan-based thermosensitive hydrogels for timolol maleate delivery, addressing common limitations of chitosan systems, including opacity and prolonged gelation times.19 The quaternization process enhanced chitosan solubility and transparency while maintaining thermosensitive properties, with the addition of sodium hydrogen carbonate synergistically enhancing gelation kinetics. In vitro release studies demonstrated initial burst release followed by steady, sustained release over one week, with cytotoxicity assays confirming excellent biocompatibility. For infectious keratitis, hydrogel formulations containing antimicrobial agents provide advantages over conventional eye drops through prolonged corneal contact time and sustained drug concentrations. Wang et al (2021) fabricated natural hybrid hydrogels comprising decellularized porcine cornea, gelatin, and voriconazole-loaded microspheres for antifungal applications. This system demonstrated excellent antifungal activity against Fusarium solani and Aspergillus fumigatus while simultaneously providing a scaffold for corneal stromal regeneration in defect models.37 Ex vivo studies using rabbit corneas infected with fungal pathogens showed significant reductions in colony-forming units after 24 hours of treatment with the antifungal hydrogel compared to non-treated or drug-free controls.37
Combinatorial approaches delivering both antibiotics and corticosteroids address the dual therapeutic needs in many anterior segment inflammatory and infectious conditions. As shown in Figure 5, we previously developed poloxamer 407 (PM)/gellan gum (GG)-based in situ hydrogels containing dexamethasone-loaded chitosan NPs alongside neomycin sulfate and polymyxin B sulfate, achieving localized co-delivery with prolonged release profiles.18 In this study, a novel ophthalmic drug delivery platform was created using a dual-polymer hydrogel matrix (PM-GG) to simultaneously administer anti-inflammatory and antimicrobial agents for eye infections (Figure 5A). The CS nanocarriers encapsulating dexamethasone demonstrated dimensions of 286 nm, positive surface charge of 20.3 mV, drug capture rate of 29.4%, and payload capacity of 6.5%. Formulation optimization revealed that combining 0.1% GG with 16.5% PM substantially enhanced the system’s thickness relative to using 16.5% PM as a single component. Microscopic examination via SEM showed that incorporating GG reduced the cavity dimensions within the gel structure (Figure 5B–D), while the PM-GG composite formulation exhibited diminished water uptake compared to the PM-only version due to its enhanced rheological properties. The therapeutic agents (NMS, PMB, and DEX) were released gradually over time while maintaining bactericidal activity (Figure 5E). Cytotoxicity evaluation using HUVECs confirmed the formulation’s safety profile, showing no detrimental cellular effects, thereby supporting its potential as an innovative ophthalmic treatment system for bacterial infections accompanied by inflammation.
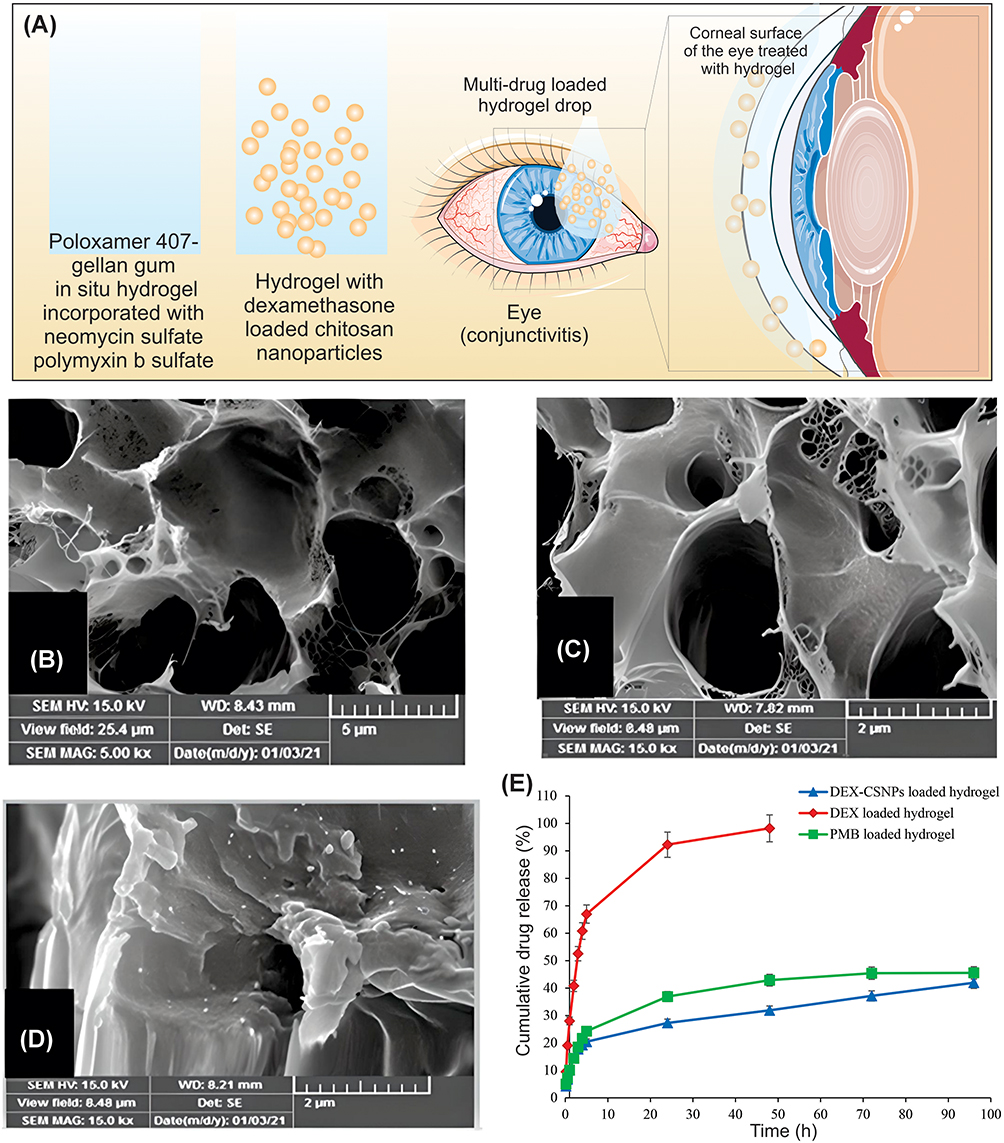 |
Figure 5 Poloxamer 407/gellan gum-based in situ hydrogels for ocular co-delivery of antibiotics and corticosteroids. (A) Proposed hydrogel formulation and application. (B) SEM micrograph of PM. (C) SEM micrograph of PM-GG. (D) SEM micrograph of DEX-CSNPs loaded PM-GG in situ hydrogels. (E) Cumulative profile of in vitro drug release from in situ hydrogels containing DEX, DEX-CSNPs, and PMB in STF at 37 °C. Data adapted with permission from.18 |
The nanoparticle encapsulation of dexamethasone provided protection and controlled release, while the antibiotics remained dispersed within the hydrogel matrix for immediate antimicrobial action. Cell viability assays confirmed the formulation’s tolerability, positioning such hybrid systems as promising alternatives to multiple separate formulations currently required for managing complex ocular conditions.
Posterior Segment Diseases
Intravitreal injection of hydrogel-based delivery systems offers significant potential for managing posterior segment diseases, particularly age-related macular degeneration and diabetic retinopathy, which currently require frequent anti-VEGF injections. The primary advantage of hydrogel depots lies in their capacity to maintain therapeutic drug concentrations over extended periods, potentially reducing injection frequency from monthly to quarterly or even less frequent intervals. Kabiri et al (2018) developed stimulus-responsive hyaluronic acid/methylcellulose hydrogels laden with poly(ethylene oxide)-poly(lactic acid) NPs loaded with cannabigerolic acid, demonstrating over 300% enhancement in transcorneal penetration compared to control formulations in whole-eye experiments.30 Biodegradable microsphere-hydrogel systems specifically designed for intravitreal administration have demonstrated particularly promising results. Liu et al (2019a) characterized ranibizumab-loaded PLGA microsphere-hydrogel systems fabricated using PEG-PLLA-DA/NIPAAm hydrogels, systematically evaluating thermal responsive behavior, swelling ratios, mechanical properties, and degradation kinetics.127 These systems maintained injectability through 28-gauge needles while providing volume phase transition temperatures appropriate for ocular application. The aflibercept-loaded microsphere-hydrogel system achieved 6-month sustained release (0.07–0.15 μg/day) of bioactive drug with tunable initial burst release (37.35–74.56 μg), potentially reducing treatment from 12 monthly injections to 1 single injection over 6 months while maintaining therapeutic efficacy and demonstrating no cytotoxicity. Similar approaches have been successfully applied to aflibercept delivery, with bioactivity assays confirming that the released drug maintained therapeutic efficacy throughout the release period.133 Light-responsive hydrogel systems offer additional control over gelation timing and degradation. Cheruvu et al (2025) synthesized methacrylated hyaluronic acid hydrogels for spironolactone delivery targeting the renin-angiotensin-aldosterone system in diabetic retinopathy.121 Upon UV crosslinking following intravitreal injection, these systems formed stable depots releasing drug over 90 days in vitro, with in vivo ocular residence studies confirming depot retention exceeding 60 days. The targeting of non-VEGF pathways addresses the growing challenge of anti-VEGF non-responder populations, potentially providing alternative therapeutic mechanisms for managing refractory cases. Alkaline phosphatase-responsive hydrogels represent an innovative approach leveraging disease-specific biomarkers for triggered drug release. Li et al (2025) developed dexamethasone sodium phosphate hydrogels for autoimmune uveitis management, capitalizing on elevated alkaline phosphatase levels in inflamed intraocular tissues.148 The ionic crosslinking approach enabled incorporation of adalimumab, creating a synergistic combination therapy within a single injectable formulation. In experimental autoimmune uveitis models, single intravitreal injections significantly attenuated inflammatory cell infiltration, suppressed pro-inflammatory cytokines, and preserved BRB integrity while demonstrating excellent biocompatibility.
Clinical Translation, Emerging Technologies, and Market Perspectives
Despite extensive preclinical development, relatively few hydrogel-based ocular delivery systems have achieved clinical approval and commercialization. Notable exceptions include DEXTENZA®, a dexamethasone-loaded intracanalicular insert utilizing hydrogel technology for sustained corticosteroid delivery following ophthalmic surgery, and ReSure® Sealant, a PEG-based hydrogel for sealing clear corneal incisions.69 Clinical translation of hydrogel-based delivery systems faces multiple hurdles. Regulatory pathways depend on intended use, duration of application, and drug-device classification, with intraocular systems subject to more rigorous scrutiny than topical formulations. Sterilization poses a distinct challenge, as terminal methods such as autoclaving may compromise gelation behavior, mechanical integrity, or drug stability, while aseptic manufacturing, though a viable alternative, adds cost and complexity. Economically, the higher manufacturing costs of hydrogel systems must be offset by demonstrable clinical benefits, including improved efficacy, reduced adverse effects, better patient compliance, or fewer clinic visits. Patient acceptance of novel delivery modalities also remains a barrier. Future directions center on stimuli-responsive “smart” hydrogels with integrated biosensing for closed-loop drug delivery, such as glucose-responsive systems for diabetic retinopathy or inflammation-triggered release for uveitis management.149 The development of such intelligent systems requires sophisticated molecular design integrating sensing elements with responsive drug release mechanisms while maintaining biocompatibility and manufacturing feasibility. Remarkably, 3D bioprinting technologies offer potential for creating patient-specific hydrogel constructs with precisely controlled geometries, internal architectures, and drug distribution patterns.150 This approach could enable personalized medicine strategies, tailoring delivery systems to individual patient anatomy and disease characteristics. Integration of multiple drugs within spatially distinct hydrogel regions could provide sequential or simultaneous delivery of complementary therapeutics, addressing complex multifactorial diseases through coordinated pharmacological interventions. Further, nanotechnology integration continues to advance with the development of multifunctional nanocarriers incorporating imaging agents, targeting ligands, and therapeutic payloads within hydrogel matrices.82 Such theranostic platforms could enable real-time monitoring of drug distribution and therapeutic responses, facilitating treatment optimization. The incorporation of cell-based therapies within hydrogel scaffolds represents another frontier, with applications in retinal regeneration and stem cell delivery showing promise for treating currently intractable degenerative conditions.151 However, these advanced approaches must overcome substantial technical, regulatory, and economic hurdles before achieving clinical realization.
Transformative 3D Ocular Organoids and Eye-on-a-Chip Platforms
The development of effective ocular therapeutics remains exceptionally challenging, in large part due to the eye’s unique anatomical barriers, specialized cellular microenvironments, and complex physiological processes. Traditional preclinical drug development paradigms, which predominantly rely on 2D cell cultures and animal models, have demonstrated inadequate predictive capacity for human therapeutic responses, contributing to attrition rates exceeding 90% during clinical trials. Two-dimensional culture systems fundamentally fail to recapitulate the 3D architecture, intercellular communication networks, extracellular matrix composition, and biomechanical cues that govern cellular behavior in native ocular tissues.25 While animal models provide whole-organism contexts, substantial interspecies differences in ocular anatomy, physiology, drug metabolism, and immune responses frequently result in poor translation of preclinical findings to clinical outcomes. This persistent translational gap has catalyzed intensive efforts to develop physiologically relevant experimental platforms that authentically replicate human ocular biology at multiple scales of organization. The convergence of induced pluripotent stem cell technology, advanced tissue engineering, microfluidics, biomaterials science, and 3D bioprinting has enabled unprecedented innovations in modeling ocular tissues ex vivo.144,152 Ocular 3D organoid cultures and organ-on-a-chip systems are two complementary technological approaches that have emerged as particularly transformative. For instance, Hau et al evaluated antisense oligonucleotide splicing modulation using patient-derived retinal organoids, confirming gene-corrected photoreceptor rescue, demonstrating direct therapeutic efficacy assessment in a human-relevant model.139 For mechanistic drug delivery investigation, remarkably, 3D organoid cultures self-organize into complex tissue structures and microfluidic organ-on-a-chip systems recreate functional tissue units within precisely controlled microenvironments. Wan et al (2024) study more explicitly, noting quantitative outcomes: elevated IL-6/IL-8/TNF-α under hyperosmolar stress, reduced colony-forming efficiency, and pharmacological responses to dexamethasone and cyclosporine as validated efficacy readouts.138 These platforms offer opportunities to investigate drug delivery mechanisms, evaluate therapeutic efficacy, model disease pathogenesis, and predict safety profiles with fidelity approaching native human tissues while maintaining experimental control impossible to achieve in vivo. Recognizing the revolutionary potential of these technologies, the National Eye Institute and National Center for Advancing Translational Science have established strategic initiatives specifically targeting the advancement of 3D ocular organoid and microphysiological systems.144 These coordinated efforts aim to provide vision researchers with sophisticated tools that augment traditional experimental approaches, enabling investigations of developmental processes, disease mechanisms, and therapeutic interventions previously impossible to conduct systematically. Beyond fundamental biology, these platforms promise to transform pharmaceutical screening by facilitating high-throughput evaluation of thousands of therapeutic candidates in human-relevant contexts, potentially reducing drug development timelines from over a decade to just a few years while simultaneously improving clinical success rates.
3D Ocular Organoids as Advanced Platforms for Drug Delivery Research
Unlike flat monolayer cultures that fail to recapitulate the complex cellular interactions, spatial organization, and extracellular matrix composition of actual tissues, organoid systems self-assemble into multilayered structures exhibiting appropriate cell type diversity, polarity, and functional characteristics essential for evaluating drug penetration, distribution, and therapeutic efficacy.26
Anterior segment organoid models address distinct challenges in topical drug delivery, where rapid clearance through nasolacrimal drainage and limited corneal penetration severely restrict bioavailability. Human corneal epithelial organoids recapitulate the stratified architecture and barrier properties of native cornea, maintaining hierarchical cell lineages with basal stem cells, transit-amplifying populations, and differentiated superficial cells expressing appropriate cytokeratins and mucins.138 These organoids enable evaluation of topical formulations, including nanosuspensions, mucoadhesive polymers, and contact lens-based delivery systems under physiologically relevant conditions. Hyperosmolar stress-induced DED models demonstrate inflammatory responses, stem cell dysfunction, and mucin reduction characteristic of clinical pathology, validating their utility for screening anti-inflammatory therapeutics and tear supplements.138 The ability to generate patient-specific organoids facilitates personalized therapeutic selection, particularly valuable given the heterogeneous etiology of ocular surface disorders. Human corneal epithelial organoids established from limbal stem cells demonstrate remarkable structural and functional fidelity to native corneal epithelium, recapitulating hierarchical cell lineage organization with basal progenitor cells, transit-amplifying cells, and differentiated superficial cells expressing appropriate cytokeratins (K3, K12) and mucin-1.138 These 3D structures can be maintained in long-term culture exceeding six months while retaining proliferative capacity and differentiation potential, with addition of FGF10 specifically inhibiting premature differentiation and maintaining stemness. The organoids successfully model dry eye disease when subjected to hyperosmolar stress (450–500 mOsm), inducing pathophysiologically relevant responses (e.g., elevated inflammatory cytokine secretion (IL-6, IL-8, TNF-α), compromised stem cell function with reduced colony-forming efficiency, and diminished mucin-1 expression), which are the clinical hallmark features of this disease. Importantly, organoids demonstrate appropriate pharmacological responses to dexamethasone and cyclosporine, validating their utility as ex vivo drug testing platforms that may predict clinical efficacy more accurately than animal models suffering from anatomical and immunological differences. Corneal epithelial organoids enable systematic evaluation of topical drug delivery formulations, including nanosuspensions, liposomal preparations, mucoadhesive polymeric systems, and contact lens-based delivery under physiologically relevant 3D conditions maintaining tissue architecture and cellular differentiation.138 Assessment of drug penetration through stratified epithelium using confocal microscopy, effects on tight junction integrity measured by impedance spectroscopy, impacts on mucin production quantified by immunofluorescence, and modulation of inflammatory responses evaluated by multiplex cytokine assays provide comprehensive information critical for formulation optimization. The capacity to generate organoids from individual patients enables personalized therapeutic screening particularly relevant for heterogeneous conditions like dry eye disease, where different etiological subtypes (aqueous deficient versus evaporative, inflammatory versus neuropathic) may respond differently to available therapeutics.
Lens organoids provide unique platforms for cataract research, displaying optical transparency and spatiotemporal gene expression patterns matching native lens tissue.142 High-throughput RNA sequencing confirms appropriate expression of developmental regulators and crystallin proteins, while functional assays demonstrate susceptibility to opacity induction. The rapid production timeline and scalability position these organoids for systematic screening of anti-cataractogenic compounds, potentially identifying pharmacological alternatives to surgical intervention. Lacrimal gland organoids address critical needs for modeling aqueous-deficient DED, with magnetic 3D bioprinting technology enabling reproducible fabrication of functional secretory structures.141 Porcine models offer anatomical and physiological similarities to human lacrimal tissue, providing relevant platforms for identifying therapeutics that restore tear production or protect against glandular dysfunction. Lens organoids represent another frontier in anterior segment modeling, offering opportunities to study cataract formation mechanisms and evaluate anti-cataractogenic compounds.142,143 Generated by culturing lens epithelial cells under defined 3D conditions with ascorbic acid, insulin, and appropriate growth factors, these organoids display optical transparency and spatiotemporal gene expression patterns characteristic of native lens tissue. High-throughput RNA sequencing of laser-capture-microdissected organoid regions confirms appropriate expression of key lens developmental regulators (Pax6, Prox1) and differentiation markers (Hsf4, crystallins including Cryaa, Cryab, Crygs) with spatial gradients matching in vivo patterns. The organoids are amenable to opacity induction through oxidative stress, calcium dysregulation, or genetic perturbation, providing functional readouts for screening anti-cataractogenic compounds. Knockdown of Celf1, encoding an RNA-binding protein implicated in cataract pathogenesis, successfully induces opacities validating the platform’s utility for identifying genes and therapeutic targets relevant to lens biology. The rapid production timeline (2–3 weeks) and scalability of these organoids position them as viable platforms for high-throughput screening of chemical libraries to identify compounds preventing or reversing lens opacity.
Lacrimal gland organoids address the critical unmet need for models of tear production and aqueous-deficient DED, affecting millions worldwide.141 Using magnetic 3D bioprinting technology that employs magnetic NPs to assemble cells into spheroids, investigators have successfully generated functional lacrimal gland organoids from murine and porcine primary cells. The porcine model offers particular advantages due to greater anatomical and physiological similarities to human lacrimal glands compared to rodent models, including acinar cell organization, innervation patterns, and secretory protein profiles. These organoids express appropriate markers including aquaporin-5, lactoferrin, and lysozyme, and maintain secretory function in response to cholinergic stimulation. The magnetic bioprinting platform provides scalability and reproducibility essential for high-throughput drug screening applications, enabling consistent fabrication of large organoid arrays (96-well or 384-well formats) suitable for systematic compound evaluation to identify therapies that restore tear production, protect against oxidative damage, or modulate inflammatory responses in lacrimal insufficiency.
The utility of organoid platforms for pharmaceutical development is substantially enhanced through integration with sophisticated imaging technologies and computational analysis methods addressing inherent challenges of 3D tissue visualization and quantification. Notably, 3D tissues pose significant optical challenges due to light scattering, absorption by chromophores, and refractive index mismatches that limit penetration depth in conventional microscopy. Tissue clearing techniques employing organic solvents (3DISCO, iDISCO), aqueous media (CLARITY, CUBIC), or hydrogel embedding (PACT, ExM) render tissues optically transparent by matching refractive indices among tissue components, enabling deep imaging of intact organoids with subcellular resolution.25 Combined with advanced microscopy modalities including light-sheet fluorescence microscopy, which illuminates samples from the side while detecting orthogonally to minimize photobleaching and phototoxicity, and multiphoton microscopy utilizing near-infrared excitation for deep tissue penetration, these approaches allow comprehensive 3D visualization of drug distribution, cellular responses, and tissue architecture throughout entire organoids.
Retinal organoids have emerged as particularly valuable tools for investigating therapeutic strategies targeting posterior segment diseases including age-related macular degeneration, diabetic retinopathy, retinitis pigmentosa, and Stargardt disease.26,140 These self-organizing structures recapitulate the spatiotemporal differentiation sequence of retinogenesis, generating all major retinal cell types arranged in laminar architecture with functional photoreceptors possessing rudimentary outer segments. The 3D organization enables authentic assessment of how therapeutic agents penetrate through multiple retinal layers, a critical consideration for optimizing intravitreal drug delivery formulations including sustained-release implants, biodegradable microspheres, and nanoparticle systems. Patient-derived induced pluripotent stem cell lines allow generation of disease-specific organoids carrying pathogenic mutations, providing ideal platforms for testing antisense oligonucleotides, gene therapy vectors, and personalized pharmacological interventions in the correct genomic and cellular context.139 The capacity to model disease progression and evaluate therapeutic responses longitudinally within the same organoid overcomes limitations of endpoint-only analyses, enabling pharmacokinetic-pharmacodynamic studies that reveal temporal drug action profiles.
Beyond genetic disorders, retinal organoids serve as platforms for screening compounds targeting complex multifactorial diseases. Organoids subjected to disease-relevant stressors such as oxidative damage, inflammatory cytokines, or hyperglycemic conditions faithfully model pathological states, allowing systematic evaluation of neuroprotective agents, anti-inflammatory compounds, and antioxidant formulations.140 The integration of retinal organoids with brain tissue in optic vesicle-containing organoids further expands modeling capabilities, enabling investigation of visual pathway development and assessment of systemically administered drugs that must traverse the blood-brain barrier to reach ocular targets.153 These complex assembloids provide unprecedented opportunities to study interorgan communication relevant to neurological disorders with ocular manifestations.
Advanced organoid protocols incorporating retinal pigment epithelium and choroid-like vascular structures enable modeling of drusen formation, complement activation, and choroidal neovascularization (i.e., all critical features of AMD pathophysiology), providing more comprehensive disease models for therapeutic evaluation. Recent innovations have produced optic vesicle-containing brain organoids that integrate eye primordia with forebrain structures, recapitulating embryonic eye-brain connectivity.153 These complex assembloids are generated through carefully timed modulation of morphogen gradients (Wnt, BMP, FGF) that pattern anterior neural tissue into forebrain and optic vesicle domains. The resulting organoids contain bilateral eye structures with primitive corneal epithelium, lens-like structures, retinal pigment epithelia, and photoreceptor progenitors connected to brain tissue through axon-like projections, enabling investigation of visual pathway development and potentially facilitating studies of systemically administered drugs that must penetrate the blood-brain barrier before reaching retinal targets. These sophisticated models open possibilities for studying neurodevelopmental disorders affecting both eye and brain, as well as neurodegenerative diseases with ocular manifestations.
Eye-on-a-Chip Microfluidic Platforms
Eye-on-a-chip technologies represent sophisticated microfluidic platforms that recreate specific ocular anatomical compartments, physiological processes, and pathological conditions within precisely engineered microenvironments fabricated using photolithography and soft lithography techniques. These microsystems utilize materials such as polydimethylsiloxane (PDMS), poly(methylmethacrylate), and other biocompatible polymers to create channels, chambers, and interfaces that mimic ocular structures at physiologically relevant length scales, typically ranging from tens of micrometers to several millimeters. The integration of living cells, tissue explants, or miniaturized organoids within these devices enables real-time monitoring of drug-tissue interactions, transport kinetics, barrier function integrity, and cellular responses under dynamic conditions that closely approximate in vivo scenarios while maintaining optical transparency for high-resolution imaging. A pioneering application of eye-on-a-chip methodology involved developing a microfluidic platform to investigate silicone oil emulsification following vitreoretinal surgery, where silicone oil serves as long-term intraocular tamponade.146 Further, poly(methylmethacrylate) chips replicating the posterior chamber cross-section, lined with retinal ganglion cells, were subjected to stepper-motor-driven saccadic movements for four days to assess silicone oil emulsification across viscosities of 5–5000 centistokes (cSt). Lower viscosity oils (5 cSt) emulsified significantly more than higher viscosity alternatives (500–5000 cSt), yielding quantitative data on droplet formation and size distribution. This work established microfluidic eye-on-a-chip platforms as tools for evaluating intraocular formulation stability under physiological mechanical stimulation, later extended to assess amphiphilic additives in silicone oil as sustained-release reservoirs for lipophilic agents requiring long-term intraocular delivery.35 Three silicone-oil-soluble surfactants (i.e., DC749, MQ1640, and FZ2233) served as model amphiphilic additives representing potential drug molecules. Systematic characterization revealed that amphiphilic substances substantially increased emulsification rates through mechanisms not directly correlated with interfacial tension or bulk viscosity changes. Remarkably, these additives promoted formation of water-in-oil droplets within the silicone oil phase in addition to conventional oil-in-water emulsions, a phenomenon entirely absent with unmodified silicone oil controls. These findings carry profound implications for developing silicone oil-based sustained-release drug delivery systems, as amphiphilic therapeutic agents, representing a substantial fraction of ophthalmic pharmaceuticals, might compromise formulation stability, alter pharmacokinetic release profiles, and reduce optical clarity causing visual disturbances. The capability to identify such complications ex vivo prior to clinical implementation exemplifies the value of microfluidic platforms in de-risking therapeutic development and optimizing formulation parameters before committing resources to expensive animal studies and clinical trials. The most sophisticated eye-on-a-chip application reported to date involves modeling the outer BRB and choroidal neovascularization, representing key pathophysiological features of wet age-related macular degeneration.145 This organotypic “wet-AMD-on-a-chip” platform reconstructs the RPE-choroid complex using a polarized RPE monolayer on a porous membrane adjacent to perfusable 3D microfluidic vascular networks lined with HUVECs or choroidal endothelial cells. The system maintains intact barrier function, confirmed by TEER measurements and restricted paracellular permeability, while preserving cellular polarization, tight junction protein expression (e.g., ZO-1, occludin, claudins), and basement membrane interactions. Critically, the platform recapitulates choroidal neovascularization when exposed to pro-angiogenic stimuli, demonstrating endothelial sprouting, VEGF-guided tip cell migration, and Bruch’s membrane penetration with RPE disruption. It also exhibits dose-dependent responsiveness to bevacizumab, validating its utility for anti-angiogenic drug screening. This capacity to model disease progression and quantitatively assess therapeutic interventions represents a major advancement in drug evaluation methodology, enabling mechanistic dissection of how anti-VEGF agents, corticosteroids, or novel therapeutics modulate pathological angiogenesis at cellular and molecular resolution. Furthermore, integration of transparent materials with real-time confocal or multiphoton imaging enables longitudinal tracking of drug molecules, NPs, or therapeutic proteins across tissue barriers and cellular compartments without destructive sampling.154 Microfluidic control enables precise manipulation of drug concentrations, exposure profiles, and washout kinetics while maintaining physiological shear stress, perfusion, and oxygen tension. These systems support systematic investigation of formulation parameters (e.g., viscosity, osmolarity, pH, and particulate characteristics) on drug bioavailability, permeation, and therapeutic outcomes. Integration of patient-derived induced pluripotent stem cells further enables precision medicine approaches, allowing prediction of individual therapeutic responses and adverse reactions prior to clinical administration.
Final Remarks and Conclusion
Hydrogel-based DDSs have fundamentally transformed ocular therapeutics by overcoming persistent challenges of inadequate bioavailability, rapid precorneal clearance, and insufficient therapeutic duration that have long compromised conventional treatment approaches. These sophisticated polymeric networks, encompassing natural biopolymers (e.g., hyaluronic acid, chitosan, gelatin, and alginate) alongside synthetic platforms (i.e., thermosensitive poloxamer copolymers, pH-responsive carbomer derivatives, and photo-crosslinked polyethylene glycol systems), facilitate sustained drug release profiles extending from several days to multiple months while maintaining therapeutic concentrations at target sites. The versatility of hydrogels to undergo phase transitions in response to physiological stimuli, establish intimate contact with ocular surfaces through mucoadhesive interactions, traverse anatomical barriers via enhanced penetration mechanisms, and function as controlled-release reservoirs for diverse therapeutic cargo (e.g., small molecules, biologics, and nucleic acid therapeutics) has established them as indispensable technologies for managing anterior segment disorders such as glaucoma, keratitis, and ocular surface disease, as well as posterior segment pathologies including age-related macular degeneration, diabetic retinopathy, and proliferative vitreoretinopathy.
The emergence of 3D ocular organoids and eye-on-a-chip microphysiological platforms has fundamentally redefined the developmental trajectory for hydrogel-based DDSs, providing human-relevant testing environments that dramatically improve predictive accuracy for clinical translation. These platforms overcome inherent limitations of conventional 2D monolayer cultures and cross-species variability in animal models by authentically recreating human tissue architecture, multicellular complexity, physiological barrier properties, and disease-specific pathological features. Retinal organoids differentiated from patient-derived induced pluripotent stem cells offer unprecedented opportunities to evaluate intravitreal hydrogel depot systems, biodegradable microsphere suspensions, and sustained-release implant technologies under conditions that replicate drug distribution through stratified neural retina, therapeutic interactions with photoreceptor subtypes and retinal pigment epithelium, and efficacy against patient-specific genetic mutations. Corneal epithelial organoids exhibiting authentic stratified architecture and tight junction barrier function enable systematic evaluation of thermosensitive in situ gelling formulations, mucoadhesive polymer modifications, and penetration enhancers that improve drug flux without inducing cytotoxicity. Eye-on-a-chip microfluidic devices recreating the outer blood-retinal barrier or corneal-aqueous interface facilitate mechanistic investigation of how hydrogel viscosity, polymer concentration, and degradation kinetics influence drug residence time and permeation under dynamic flow conditions approximating physiological tear turnover or aqueous humor circulation.
Despite these advances, several critical barriers continue to impede clinical translation of hydrogel-based ocular therapeutics. Reproducible manufacturing and scalable production remain primary bottlenecks, as the physicochemical properties of stimuli-responsive hydrogels are highly sensitive to minor variations in polymer molecular weight, crosslinking density, and processing conditions, necessitating robust QbD frameworks and process analytical technologies to ensure batch-to-batch consistency. Long-term in vivo stability presents a parallel challenge, particularly for intravitreally administered depot systems, where sustained mechanical integrity, predictable biodegradation, and preservation of drug bioactivity must be demonstrated without inducing chronic inflammatory responses or fibrotic encapsulation. Sterilization compatibility constitutes another underappreciated obstacle, as terminal sterilization methods such as autoclaving or gamma irradiation frequently alter hydrogel crosslink density and release kinetics, while aseptic manufacturing alternatives substantially increase production complexity and cost. Biocompatibility assessment in 3D tissue contexts, particularly for nanocomposite formulations incorporating metallic or lipid-based carriers, requires evaluation beyond conventional cytotoxicity assays to capture complement activation, macrophage polarization, and foreign body responses relevant to the immunoprivileged ocular environment. Regulatory pathway ambiguity for combination drug-device hydrogel products further complicates development timelines, as classification uncertainties require early and iterative engagement with regulatory agencies.
Against this backdrop, several future research directions hold particular promise for accelerating next-generation ocular hydrogel translation. First, closed-loop stimuli-responsive platforms integrating biosensing elements with programmable drug release mechanisms (eg, glucose-responsive hydrogels for diabetic retinopathy or inflammation-triggered systems for uveitis) represent a transformative frontier aligning therapeutic output with real-time disease biomarkers, potentially eliminating fixed dosing schedules. Second, 3D bioprinting of patient-specific hydrogel constructs with spatially controlled drug distribution and anatomically precise geometries offers a precision medicine paradigm simultaneously addressing formulation optimization and personalized therapeutic matching. Third, theranostic nanocomposite hydrogel platforms integrating imaging contrast agents, therapeutic payloads, and targeting ligands within unified polymeric matrices would enable concurrent treatment monitoring and dose adjustment. Fourth, AI-assisted high-throughput screening of hydrogel formulation parameters using organoid and organ-on-chip readouts, coupled with machine learning algorithms for pharmacokinetic-pharmacodynamic modeling, promises to compress optimization cycles from years to months. Fifth, cell-laden hydrogel scaffolds incorporating photoreceptor precursors, retinal pigment epithelial cells, or Müller glia derived from patient-specific induced pluripotent stem cells represent an emerging frontier for currently intractable conditions such as geographic atrophy and end-stage retinitis pigmentosa.
In conclusion, the convergence of advanced biomaterials science with tissue engineering and microphysiological modeling represents the future of ocular drug delivery. Realizing this potential will require coordinated, interdisciplinary efforts spanning polymer chemistry, stem cell biology, microfluidic engineering, computational pharmacology, and regulatory science. As standardization initiatives mature and these platforms become progressively accessible, their collective influence on ocular drug development pipelines will expand substantially, ultimately delivering more effective, longer-acting, and better-tolerated therapeutic options to patients afflicted by vision-threatening diseases worldwide. Looking ahead, successful clinical translation demands coordinated resolution of persistent challenges: regulatory classification of hydrogel formulations as combination drug-device products under FDA 21 CFR Parts 3 and 820 imposes heightenedpremarket requirements, and the absence of standardized sterilization validation guidance remains a significant gap. Terminal sterilization methods such as autoclaving irreversibly alter gelation temperatures and drug release kinetics, making aseptic filtration the preferred alternative, albeit at greater manufacturing complexity, particularly for viscous nanocomposite systems prone to membrane fouling. At manufacturing scale, batch-to-batch reproducibility demands robust process analytical technology frameworks, while protein-loaded formulations require validated cold-chain infrastructure maintaining 2–8°C throughout production and distribution. Addressing these interconnected barriers through cross-disciplinary collaboration among academic institutions, industry partners, and regulatory bodies will be essential to realizing the full clinical potential of next-generation ocular hydrogel systems.
Acknowledgment
The authors would like to acknowledge the technical support provided by the College of Pharmacy at Nova Southeastern University.
Funding
This work was supported by Nova Southeastern University through the President Resarch Grant (PRG, Grant No. 334878).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Blindness and Visual Impairment; 2023.
2. Blindness GBD, Vision Impairment C, Vision Loss Expert Group of the Global Burden of Disease S. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9(2):e130–32. doi:10.1016/S2214-109X(20)30425-3
3. Vision Loss Expert Group of the Global Burden of Disease S, Blindness GBD, Vision Impairment C. Global estimates on the number of people blind or visually impaired by diabetic retinopathy: a meta-analysis from 2000 to 2020. Eye. 2024;38(11):2047–2057. doi:10.1038/s41433-024-03101-5.
4. Vision Loss Expert Group of the Global Burden of Disease S, Blindness GBD, Vision Impairment C. Global estimates on the number of people blind or visually impaired by cataract: a meta-analysis from 2000 to 2020. Eye. 2024;38(11):2156–2172. doi:10.1038/s41433-024-02961-1.
5. Vision Loss Expert Group of the Global Burden of Disease S, Blindness GBD, Vision Impairment C. Global estimates on the number of people blind or visually impaired by Uncorrected Refractive Error: a meta-analysis from 2000 to 2020. Eye. 2024;38(11):2083–2101. doi:10.1038/s41433-024-03106-0.
6. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027
7. Blindness GBD, Vision Impairment C, Vision Loss Expert Group of the Global Burden of Disease S. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/S2214-109X(20)30489-7.
8. International Agency for the Prevention of B. Vision Atlas. 2020.
9. Barar J, Asadi M, Mortazavi-Tabatabaei SA, Omidi Y. Ocular drug delivery; impact of in vitro cell culture models. J Ophthalmic Vis Res. 2009;4(4):238–252.
10. Barar J, Javadzadeh AR, Omidi Y. Ocular novel drug delivery: impacts of membranes and barriers. Expert Opin Drug Deliv. 2008;5(5):567–581. doi:10.1517/17425247.5.5.567
11. Barar J, Aghanejad A, Fathi M, Omidi Y. Advanced drug delivery and targeting technologies for the ocular diseases. Bioimpacts. 2016;6(1):49–67. doi:10.15171/bi.2016.07
12. Willoughby CE, Ponzin D, Ferrari S, Lobo A, Landau K, Omidi Y. Anatomy and physiology of the human eye: effects of mucopolysaccharidoses disease on structure and function–a review. Clin Exp Ophthalmol. 2010;38:2–11.
13. Scott IU, Flynn HW Jr. Reducing the risk of endophthalmitis following intravitreal injections. Retina. 2007;27(1):10–12. doi:10.1097/IAE.0b013e3180307271
14. Patel SN, Storey PP, Kim JS, et al. Systemic immunosuppression and risk of endophthalmitis after intravitreal anti-vascular endothelial growth factor injections. Ophthalmic Surg Lasers Imaging Retina. 2021;52(S1):S17–S22. doi:10.3928/23258160-20210518-04
15. Israilevich RN, Mansour H, Patel SN, et al. Risk of endophthalmitis based on cumulative number of anti-VEGF intravitreal injections. Ophthalmology. 2024;131(6):667–673. doi:10.1016/j.ophtha.2023.12.033
16. Comcali S, Tasci YY, Onen M, et al. Endophthalmitis following intravitreal injections at a tertiary center: real-life data on incidence, risk factors, management strategies, and visual outcomes. BMC Ophthalmol. 2025;25(1):278. doi:10.1186/s12886-025-04093-w
17. Lotfi M, Nakhlband A, Doustmihan A, Omidi Y, Fathi M, Adibkia K. Formulation and evaluation of in-situ forming poloxamer-based hydrogel containing thiolated chitosan nanoparticles as intranasal galantamine delivery system. Int J Biol Macromol. 2025;320(Pt 1):145647. doi:10.1016/j.ijbiomac.2025.145647
18. Marandi MF, Safary A, Abdolahinia ED, Fathi M, Barar J, Omidi Y. Poloxamer407/gellan gum-based in situ hydrogels for ocular co-delivery of antibiotics and corticosteroids. Eur J Pharm Biopharm. 2025;213:114739. doi:10.1016/j.ejpb.2025.114739
19. Pakzad Y, Fathi M, Omidi Y, Mozafari M, Zamanian A. Synthesis and characterization of timolol maleate-loaded quaternized chitosan-based thermosensitive hydrogel: a transparent topical ocular delivery system for the treatment of glaucoma. Int J Biol Macromol. 2020;159:117–128. doi:10.1016/j.ijbiomac.2020.04.274
20. Liao X, Lu J, Yao J, et al. Polysaccharide-based injectable hydrogels for targeted drug delivery: advances and challenges. Int J Pharm. 2025:126536. doi:10.1016/j.ijpharm.2025.126536.
21. Fathi M, Barar J, Aghanejad A, Omidi Y. Hydrogels for ocular drug delivery and tissue engineering. Bioimpacts. 2015;5(4):159–164. doi:10.15171/bi.2015.31
22. Xue H, Zhu C, Wang Y, et al. Stimulus-responsive cellulose hydrogels in biomedical applications and challenges. Mater Today Bio. 2025;32:101814. doi:10.1016/j.mtbio.2025.101814
23. Ribeiro A, Oliveira D, Cabral-Marques H. Curcumin in ophthalmology: mechanisms, challenges, and emerging opportunities. Molecules. 2025;30(3). doi:10.3390/molecules30030457
24. Al Yabhouni SA, Mozumder MS, Hassan N, Mourad AI, Issa TM. Nanocarrier-based, ocular drug delivery: challenges, prospects, and the therapeutic landscape in the United Arab Emirates. Int J Pharm. 2024;667(Pt B):124899. doi:10.1016/j.ijpharm.2024.124899
25. Boutin ME, Hampton C, Quinn R, Ferrer M, Song MJ. 3D engineering of ocular tissues for disease modeling and drug testing. Adv Exp Med Biol. 2019;1186:171–193. doi:10.1007/978-3-030-28471-8_7
26. Ma SC, Xie YL, Wang Q, Fu SG, Wu HZ. Application of eye organoids in the study of eye diseases. Exp Eye Res. 2024;247:110068. doi:10.1016/j.exer.2024.110068
27. Agrahari V, Agrahari V. Facilitating the translation of nanomedicines to a clinical product: challenges and opportunities. Drug Discov Today. 2018;23(5):974–991. doi:10.1016/j.drudis.2018.01.047
28. Lin D, Lei L, Shi S, Li X. Stimulus-responsive hydrogel for ophthalmic drug delivery. Macromol Biosci. 2019;19(6):e1900001. doi:10.1002/mabi.201900001
29. Soppimath KS, Aminabhavi TM, Dave AM, Kumbar SG, Rudzinski W. Stimulus-responsive “smart” hydrogels as novel drug delivery systems. Drug Dev Indust Pharm. 2002;28(8):957–974. doi:10.1081/ddc-120006428
30. Kabiri M, Kamal SH, Pawar SV, et al. A stimulus-responsive, in situ-forming, nanoparticle-laden hydrogel for ocular drug delivery. Drug Deliv Transl Res. 2018;8(3):484–495. doi:10.1007/s13346-018-0504-x
31. Cassel GH. The Eye Book: A Complete Guide to Eye Disorders and Health. A Johns Hopkins Press Health Book. Johns Hopkins University Press; 2021.
32. Deepthi S, Jose J. Novel hydrogel-based ocular drug delivery system for the treatment of conjunctivitis. Int Ophthalmol. 2019;39(6):1355–1366. doi:10.1007/s10792-018-0955-6
33. Li J, Hao H, Yu B, Xin M, Sun Y, Xing X. Advancing glaucoma treatment through materials science: a bibliometric analysis. J Curr Ophthalmol. 2025;37(2):183–193. doi:10.4103/joco.joco_116_25
34. Moreno M, Pow PY, Tabitha TST, et al. Modulating release of ranibizumab and aflibercept from thiolated chitosan-based hydrogels for potential treatment of ocular neovascularization. Expert Opin Drug Deliv. 2017;14(8):913–925. doi:10.1080/17425247.2017.1343297
35. Lu Y, Chan YK, Lau LH, et al. Amphiphilic additives in silicone oil tamponade and emulsification: an eye-on-a-chip study. Acta Ophthalmol. 2020;98(2):e232–e237. doi:10.1111/aos.14212
36. Sahu A, Patel AR, Shetty KH, et al. Revolutionizing age-related macular degeneration treatment: advances and future directions in non-invasive retinal drug delivery systems. Int J Pharm. 2025;683:126009. doi:10.1016/j.ijpharm.2025.126009
37. Wang F, Zhao L, Song F, Wu J, Zhou Q, Xie L. Hybrid natural hydrogels integrated with voriconazole-loaded microspheres for ocular antifungal applications. J Mater Chem B. 2021;9(15):3377–3388. doi:10.1039/d1tb00263e
38. Colligris B, Crooke A, Huete-Toral F, Pintor J. An update on dry eye disease molecular treatment: advances in drug pipelines. Expert Opinion Pharmacother. 2014;15(10):1371–1390.
39. Elhusseiny AM, Khalil AA, El Sheikh RH, Bakr MA, Eissa MG, El Sayed YM. New approaches for diagnosis of dry eye disease. Int J Ophthalmol. 2019;12(10):1618–1628. doi:10.18240/ijo.2019.10.15
40. Khanal S, Tomlinson A, McFadyen A, Diaper C, Ramaesh K. Dry eye diagnosis. Invest Ophthalmol Vis Sci. 2008;49(4):1407–1414. doi:10.1167/iovs.07-0635
41. Li Q, Cao Y, Wang P. Recent advances in hydrogels for the diagnosis and treatment of dry eye disease. Gels. 2022;8(12). doi:10.3390/gels8120816
42. Cabrera-Aguas M, Khoo P, Watson SL. Infectious keratitis: a review. Clin Exp Ophthalmol. 2022;50(5):543–562. doi:10.1111/ceo.14113
43. Stapleton F. The epidemiology of infectious keratitis. Ocul Surf. 2023;28:351–363. doi:10.1016/j.jtos.2021.08.007
44. Gupta A. Current perspective on infectious uveitis. Ind J Ophthalmol. 2026. doi:10.4103/IJO.IJO_3289_25.
45. Han J, Harper J, Copland DA, Maghsoudlou P. The immunopathogenesis of uveitis. Front Med. 2026;13:1717056. doi:10.3389/fmed.2026.1717056
46. Chen KY, Chan HC, Chan CM. What are the key predictors of visual function recovery in uveitis? A systematic review and meta-analysis unraveling structural, genetic, and immunological determinants. Inflamm Res. 2026;75(1). doi:10.1007/s00011-025-02130-4
47. Zhang X, Yu Y, Yao K. Advances in cataract surgery: is a new era on the horizon? Curr Opin Ophthalmol. 2026. doi:10.1097/ICU.0000000000001219
48. Jin L, Wu Y, Zhang F, et al. Interocular agreement and differences of ocular growth in cataract patients. Sci Rep. 2026;16(1):6095. doi:10.1038/s41598-026-36134-9
49. Aune D, Jayedi A, Kazemi A, Soltani S, Rezaei F, Leitzmann MF. Physical activity and the risk of cataract and age-related macular degeneration: a systematic review and meta-analysis of cohort studies. BMC Ophthalmol. 2026. doi:10.1186/s12886-026-04721-z
50. Karuntu JS, Almushattat H, Nguyen XT, et al. Syndromic retinitis pigmentosa. Prog Retin Eye Res. 2025;107:101324. doi:10.1016/j.preteyeres.2024.101324
51. Janaky M, Braunitzer G. Syndromic retinitis pigmentosa: a narrative review. Vision. 2025;9(1). doi:10.3390/vision9010007
52. Mihalache A, Huang RS, Grad J, et al. Adaptive optics in retinitis pigmentosa: a systematic review. Retina. 2025. doi:10.1097/IAE.0000000000004475
53. Visor GC. Drug design strategies for ocular therapeutics. Adv Drug Delivery Rev. 1994;14(2–3):269–279.
54. Coca-Prados M. The blood-aqueous barrier in health and disease. J Glaucoma. 2014;23(8 Suppl 1):S36–8. doi:10.1097/IJG.0000000000000107
55. Raviola G. The structural basis of the blood-ocular barriers. Exp Eye Res. 1977;25 Suppl:27–63. doi:10.1016/s0014-4835(77)80009-2
56. Toris CB, Yablonski ME, Wang YL, Camras CB. Aqueous humor dynamics in the aging human eye. Am J Ophthalmol. 1999;127(4):407–412. doi:10.1016/s0002-9394(98)00436-x
57. Brubaker RF. Flow of aqueous humor in humans [The Friedenwald Lecture]. Invest Ophthalmol Vis Sci. 1991;32(13):3145–3166.
58. Conrad JM, Robinson JR. Aqueous chamber drug distribution volume measurement in rabbits. J Pharm Sci. 1977;66(2):219–224. doi:10.1002/jps.2600660222
59. Zhou LY, Liu ZG, Sun YQ, Li YZ, Teng ZQ, Liu CM. Preserving blood-retinal barrier integrity: a path to retinal ganglion cell protection in glaucoma and traumatic optic neuropathy. Cell Regen. 2025;14(1):13. doi:10.1186/s13619-025-00228-y
60. Braunger BM, Giessl A, Schlotzer-Schrehardt U. The blood-ocular barriers and their dysfunction: anatomy, physiology, pathology. Klin Monbl Augenheilkd. 2023;240(5):650–661. Die Blut-Augen-Schranken und ihre Storungen: Anatomie, Physiologie, Pathologie. doi:10.1055/a-2063-8957
61. Sarkar T, Gogoi NR, Jana BK, Mazumder B. Formulation advances in posterior segment ocular drug delivery. J Ocul Pharmacol Ther. 2025;41(3):101–130. doi:10.1089/jop.2024.0153
62. Garaszczuk IK, Montes Mico R, Iskander DR, Exposito AC. The tear turnover and tear clearance tests - a review. Expert Rev Med Devices. 2018;15(3):219–229. doi:10.1080/17434440.2018.1435271
63. Chen P, Chen H, Zang X, et al. Expression of efflux transporters in human ocular tissues. Drug Metab Dispos. 2013;41(11):1934–1948. doi:10.1124/dmd.113.052704
64. Barar J, Omidi Y. Nanoparticles for ocular drug delivery. Nanomed Drug Delivery. 2013;287:1.
65. Omidi Y, Barar J, Hamzeiy H. Nanomedicines impacts in ocular delivery and targeting. In: Nanotechnology in Health Care. Pan Stanford Publishing Pte. Ltd.; 2012:43–106.
66. Pakzad Y, Fathi M, Omidi Y, Zamanian A, Mozafari M. Nanotechnology for ocular and optic drug delivery and targeting. In: Nanoengineered Biomaterials for Advanced Drug Delivery. Elsevier; 2020:499–523.
67. Ray P, Singh S, Gupta S. Topical antimicrobial therapy: current status and challenges. Ind J Med Microbiol. 2019;37(3):299–308. doi:10.4103/ijmm.IJMM_19_443
68. Sabbagh F, Zargarian SS, Kosik-Koziol A, Nakielski P, Pierini F. Hydrogel-based ocular drug delivery systems. J Mater Chem B. 2025;13(46):14982–15006. doi:10.1039/d5tb01575h
69. Fang G, Yang X, Wang Q, Zhang A, Tang B. Hydrogels-based ophthalmic drug delivery systems for treatment of ocular diseases. Mater Sci Eng C Mater Biol Appl. 2021;127:112212. doi:10.1016/j.msec.2021.112212
70. Lu C, Yoganathan RB, Kociolek M, Allen C. Hydrogel containing silica shell cross-linked micelles for ocular drug delivery. J Pharm Sci. 2013;102(2):627–637. doi:10.1002/jps.23390
71. Xu J, Li X, Sun F. In vitro and in vivo evaluation of ketotifen fumarate-loaded silicone hydrogel contact lenses for ocular drug delivery. Drug Deliv. 2011;18(2):150–158. doi:10.3109/10717544.2010.522612
72. Lee D, Cho S, Park HS, Kwon I. Ocular drug delivery through pHEMA-hydrogel contact lenses co-loaded with lipophilic vitamins. Sci Rep. 2016;6:34194. doi:10.1038/srep34194
73. Varela-Garcia A, Concheiro A, Alvarez-Lorenzo C. Cytosine-functionalized bioinspired hydrogels for ocular delivery of antioxidant transferulic acid. Biomater Sci. 2020;8(4):1171–1180. doi:10.1039/c9bm01582e
74. Sahoo SK, Dilnawaz F, Krishnakumar S. Nanotechnology in ocular drug delivery. Drug Discov Today. 2008;13(3–4):144–151. doi:10.1016/j.drudis.2007.10.021
75. Nakhlband A, Barar J. Impacts of nanomedicines in ocular pharmacotherapy. Bioimpacts. 2011;1(1):7–22. doi:10.5681/bi.2011.003
76. Omidi Y, Barar J, Hamzeiy H. Nanomedicines impacts in ocular delivery and targeting. Nanotechnol Health Care. 2012;43:1.
77. Ahmed S, Amin MM, Sayed S. Ocular drug delivery: a comprehensive review. AAPS PharmSciTech. 2023;24(2):66. doi:10.1208/s12249-023-02516-9
78. Wu Y, Tao Q, Xie J, et al. Advances in nanogels for topical drug delivery in ocular diseases. Gels. 2023;9(4):292. doi:10.3390/gels9040292
79. Almeida H, Amaral MH, Lobao P, Silva AC, Loboa JM. Applications of polymeric and lipid nanoparticles in ophthalmic pharmaceutical formulations: present and future considerations. J Pharm Pharm Sci. 2014;17(3):278–293. doi:10.18433/j3dp43
80. Bharali DJ, Armstrong D, Mousa SA. Hybrid polymeric nanoparticles: potential candidate for ophthalmic delivery. Methods Mol Biol. 2013;1028:279–286. doi:10.1007/978-1-62703-475-3_18
81. Fardous J, Inoue Y, Yoshida K, Ono F, Higuchi A, Ijima H. Delivery of hydrophobic drugs to the posterior ocular region by gel-in-water nanoemulsion. Transl Vis Sci Technol. 2022;11(5):16. doi:10.1167/tvst.11.5.16
82. Arabpour Z, Salehi M, An S, et al. Exploring hydrogel nanoparticle systems for enhanced ocular drug delivery. Gels. 2024;10(9). doi:10.3390/gels10090589
83. Qi Q, Su D, Zhuang S, et al. Progress in nanotechnology for treating ocular surface chemical injuries: reflecting on advances in ophthalmology. Adv Sci. 2025;12(6):e2407340. doi:10.1002/advs.202407340
84. Lynch CR, Kondiah PPD, Choonara YE, du Toit LC, Ally N, Pillay V. Hydrogel biomaterials for application in ocular drug delivery. review. Front Bioeng Biotechnol. 2020;8:228. doi:10.3389/fbioe.2020.00228
85. Cooper RC, Yang H. Hydrogel-based ocular drug delivery systems: emerging fabrication strategies, applications, and bench-to-bedside manufacturing considerations. J Control Release. 2019;306:29–39. doi:10.1016/j.jconrel.2019.05.034
86. Yu C, Xu J, Heidari G, et al. Injectable hydrogels based on biopolymers for the treatment of ocular diseases. Int J Biol Macromol. 2024;269(Pt 1):132086. doi:10.1016/j.ijbiomac.2024.132086
87. Chen X, Li X, Zhou Y, et al. Chitosan-based thermosensitive hydrogel as a promising ocular drug delivery system: preparation, characterization, and in vivo evaluation. J Biomater Appl. 2012;27(4):391–402. doi:10.1177/0885328211406563
88. Dmour I. Absorption enhancement strategies in chitosan-based nanosystems and hydrogels intended for ocular delivery: latest advances for optimization of drug permeation. Carbohydr Polym. 2024;343:122486. doi:10.1016/j.carbpol.2024.122486
89. Widjaja LK, Bora M, Chan PN, Lipik V, Wong TT, Venkatraman SS. Hyaluronic acid-based nanocomposite hydrogels for ocular drug delivery applications. J Biomed Mater Res A. 2014;102(9):3056–3065. doi:10.1002/jbm.a.34976
90. Lu C, Zahedi P, Forman A, Allen C. Multi-arm PEG/silica hydrogel for sustained ocular drug delivery. J Pharm Sci. 2014;103(1):216–226. doi:10.1002/jps.23777
91. Gao Y, Sun Y, Ren F, Gao S. PLGA-PEG-PLGA hydrogel for ocular drug delivery of dexamethasone acetate. Drug Dev Ind Pharm. 2010;36(10):1131–1138. doi:10.3109/03639041003680826
92. Shastri D, Patel L, Parikh R. Studies on in situ hydrogel: a smart way for safe and sustained ocular drug delivery. J Young Pharm. 2010;2(2):116–120. doi:10.4103/0975-1483.63144
93. Liu B, Wang M, Tan L, et al. Hyaluronic acid hydrogel as a retinal patch in the treatment of rhegmatogenous retinal detachment: a multicenter randomised parallel-controlled trial. Clin Exp Ophthalmol. 2025;53(8):946–955. doi:10.1111/ceo.14570
94. Yang C, Xin M, Jiang Y, et al. Injectable hyaluronic acid hydrogels crosslinked by structure-engineered aldehyde-functionalized beta-cyclodextrin derivatives for long-term controlled voriconazole delivery. AAPS PharmSciTech. 2025;27(1):18. doi:10.1208/s12249-025-03212-6
95. Cheng YH, Chang YF, Ko YC, Liu CJ. Development of a dual delivery of levofloxacin and prednisolone acetate via PLGA nanoparticles/thermosensitive chitosan-based hydrogel for postoperative management: an in-vitro and ex-vivo study. Int J Biol Macromol. 2021;180:365–374. doi:10.1016/j.ijbiomac.2021.03.017
96. Ghanavi M, Khoshandam A, Aslzad S, et al. Injectable thermosensitive PEG-g-chitosan hydrogel for ocular delivery of vancomycin and prednisolone. J Drug Delivery Sci Technol. 2023;83:104385.
97. Schulz A, Rickmann A, Wahl S, et al. Alginate- and hyaluronic acid-based hydrogels as vitreous substitutes: an in vitro evaluation. Transl Vis Sci Technol. 2020;9(13):34. doi:10.1167/tvst.9.13.34
98. Kurl S, Mittal N, Kaur G. Advancing Ocular Therapeutics: the role of alginate hydrogels in overcoming drug delivery barriers - A review. Int J Biol Macromol. 2025;321(Pt 2):146319. doi:10.1016/j.ijbiomac.2025.146319
99. Li B, Shemkai JC, Zhang Q, et al. Fabrication of an alginate-poloxamer 407 thermosensitive carboxymethyl chitosan stabilized nanosuspension hydrogel for enhanced ocular delivery of clobetasol propionate in uveitis management. Int J Biol Macromol. 2025;319(Pt 1):145356. doi:10.1016/j.ijbiomac.2025.145356
100. Xiao X, Zhou Y, Lin S, Chen H, Dai R. Evaluation of calcium alginate hydrogel for suprachoroidal buckling in a rabbit model-a pilot study on efficacy and biocompatibility. Front Med. 2025;12:1632889. doi:10.3389/fmed.2025.1632889
101. Ge Z, Long L, Zhang F, et al. Development of an injectable oxidized dextran/gelatin hydrogel capable of promoting the healing of alkali burn-associated corneal wounds. Int J Biol Macromol. 2024;273(Pt 1):132740. doi:10.1016/j.ijbiomac.2024.132740
102. Shajari G, Erfan-Niya H, Fathi M, Amiryaghoubi N. Gellan gum/gelatin Schiff-base hydrogel for ocular drug delivery of timolol maleate. BMC Biotechnol. 2025;25(1):118. doi:10.1186/s12896-025-01056-3
103. Liu W, Griffith M, Li F. Alginate microsphere-collagen composite hydrogel for ocular drug delivery and implantation. J Mater Sci Mater Med. 2008;19(11):3365–3371. doi:10.1007/s10856-008-3486-2
104. Chae JJ, Mulreany DG, Guo Q, et al. Application of a collagen-based membrane and chondroitin sulfate-based hydrogel adhesive for the potential repair of severe ocular surface injuries. Mil Med. 2014;179(6):686–694. doi:10.7205/MILMED-D-13-00360
105. Maia J, Ribeiro MP, Ventura C, Carvalho RA, Correia IJ, Gil MH. Ocular injectable formulation assessment for oxidized dextran-based hydrogels. Acta Biomater. 2009;5(6):1948–1955. doi:10.1016/j.actbio.2009.02.008
106. An B, Deng Y, Cui H, et al. Redox dextran-based self-adapting adhesive hydrogels for subconjunctival injury to alleviate inflammation and accelerate healing. Biomacromolecules. 2025;26(11):7909–7922. doi:10.1021/acs.biomac.5c01399
107. Zhang T, Han X, Zhong Y, et al. Regulatory T cell intravitreal delivery using hyaluronan methylcellulose hydrogel improves therapeutic efficacy in experimental autoimmune uveitis. Biomater Adv. 2023;151:213496. doi:10.1016/j.bioadv.2023.213496
108. Block M, Giorgio G, Saal C, et al. Design of an in situ forming methylcellulose hydrogel as universal vehicle for preclinical intravitreal injection of particulate formulations. Eur J Pharm Sci. 2026;217:107346. doi:10.1016/j.ejps.2025.107346
109. De TK, Rodman DJ, Holm BA, Prasad PN, Bergey EJ. Brimonidine formulation in polyacrylic acid nanoparticles for ophthalmic delivery. J Microencapsul. 2003;20(3):361–374. doi:10.1080/0265204031000093591
110. Dalei G, Das S. Polyacrylic acid-based drug delivery systems: a comprehensive review on the state-of-art. J Drug Delivery Sci Technol. 2022;103988. doi:10.1016/j.jddst.2022.103988
111. Wong JHM, Ting Tan RP, Chang JJ, et al. Dynamic grafting of carboxylates onto Poly(Vinyl Alcohol) polymers for supramolecularly-crosslinked hydrogel formation. Chem Asian J. 2022;17(20):e202200628. doi:10.1002/asia.202200628
112. Anumolu SS, DeSantis AS, Menjoge AR, et al. Doxycycline loaded poly(ethylene glycol) hydrogels for healing vesicant-induced ocular wounds. Biomaterials. 2010;31(5):964–974. doi:10.1016/j.biomaterials.2009.10.010
113. Pritchard CD, Crafoord S, Andreasson S, et al. Evaluation of viscoelastic poly(ethylene glycol) sols as vitreous substitutes in an experimental vitrectomy model in rabbits. Acta Biomater. 2011;7(3):936–943. doi:10.1016/j.actbio.2010.11.013
114. Villapiano F, Silvestri T, Lo Gatto C, et al. Thermosensitive in situ gelling poloxamers/hyaluronic acid gels for hydrocortisone ocular delivery. Gels. 2024;10(3). doi:10.3390/gels10030193
115. Bhattacharjee P, Ahearne M. Silk fibroin based interpenetrating network hydrogel for corneal stromal regeneration. Int J Biol Macromol. 2022;223(Pt A):583–594. doi:10.1016/j.ijbiomac.2022.11.021
116. Liu J, Liu W, Zhang Y, et al. Injectable high-adhesion fibrinogen-silk fibroin hydrogel loaded with curcumin accelerates pterygium repair via dual anti-inflammatory/antiproliferative mechanisms. ACS Appl Mater Interfaces. 2025;17(37):51805–51819. doi:10.1021/acsami.5c12778
117. Gong B, Liu Y, Li H, et al. A silk fibroin nanoparticle hydrogel loaded with NK1R antagonist has synergistic anti-inflammatory and reparative effects on dry eye disease. Adv Sci. 2025;12(15):e2404835. doi:10.1002/advs.202404835
118. Fathi M, Alami-Milani M, Geranmayeh MH, Barar J, Erfan-Niya H, Omidi Y. Dual thermo-and pH-sensitive injectable hydrogels of chitosan/(poly(N-isopropylacrylamide-co-itaconic acid)) for doxorubicin delivery in breast cancer. Int J Biol Macromol. 2019;128:957–964. doi:10.1016/j.ijbiomac.2019.01.122
119. Nie X, Wang L, Xu Z, et al. 3D-bioprinted biomimetic epithelial-stromal hydrogel construct with in situ photocrosslinkable bioadhesive for suture-free corneal regeneration. Adv Healthc Mater. 2025:e04578. doi:10.1002/adhm.202504578.
120. Nguyen KT, West JL. Photopolymerizable hydrogels for tissue engineering applications. Biomaterials. 2002;23(22):4307–4314. doi:10.1016/s0142-9612(02)00175-8
121. Cheruvu SS, Merugu S, Malani M, Kulkarni O, Nirmal J. Hyaluronic acid based light responsive long acting hydrogel for the intraocular delivery of spironolactone. Int J Biol Macromol. 2025;321(Pt 4):146451. doi:10.1016/j.ijbiomac.2025.146451
122. Zhang Z, He Z, Liang R, et al. Fabrication of a micellar supramolecular hydrogel for ocular drug delivery. Biomacromolecules. 2016;17(3):798–807. doi:10.1021/acs.biomac.5b01526
123. Prina E, Mistry P, Sidney LE, et al. 3D microfabricated scaffolds and microfluidic devices for ocular surface replacement: a review. Stem Cell Rev Rep. 2017;13(3):430–441. doi:10.1007/s12015-017-9740-6
124. Dong L, Agarwal AK, Beebe DJ, Jiang H. Adaptive liquid microlenses activated by stimuli-responsive hydrogels. Nature. 2006;442(7102):551–554. doi:10.1038/nature05024
125. Hsu XL, Wu LC, Hsieh JY, Huang YY. Nanoparticle-hydrogel composite drug delivery system for potential ocular applications. Polymers. 2021;13(4). doi:10.3390/polym13040642
126. Das S, Saha D, Majumdar S, Giri L. Imaging methods for the assessment of a complex hydrogel as an ocular drug delivery system for glaucoma treatment: opportunities and challenges in preclinical evaluation. Mol Pharm. 2022;19(3):733–748. doi:10.1021/acs.molpharmaceut.1c00831
127. Liu W, Borrell MA, Venerus DC, Mieler WF, Kang-Mieler JJ. Characterization of biodegradable microsphere-hydrogel ocular drug delivery system for controlled and extended release of ranibizumab. Transl Vis Sci Technol. 2019;8(1):12. doi:10.1167/tvst.8.1.12
128. Yu Y, Feng R, Li J, et al. A hybrid genipin-crosslinked dual-sensitive hydrogel/nanostructured lipid carrier ocular drug delivery platform. Asian J Pharm Sci. 2019;14(4):423–434. doi:10.1016/j.ajps.2018.08.002
129. Cheng YH, Tsai TH, Jhan YY, et al. Thermosensitive chitosan-based hydrogel as a topical ocular drug delivery system of latanoprost for glaucoma treatment. Carbohydr Polym. 2016;144:390–399. doi:10.1016/j.carbpol.2016.02.080
130. Luo Z, Jin L, Xu L, et al. Thermosensitive PEG-PCL-PEG (PECE) hydrogel as an in situ gelling system for ocular drug delivery of diclofenac sodium. Drug Deliv. 2016;23(1):63–68. doi:10.3109/10717544.2014.903535
131. Xi L, Wang T, Zhao F, et al. Evaluation of an injectable thermosensitive hydrogel as drug delivery implant for ocular glaucoma surgery. PLoS One. 2014;9(6):e100632. doi:10.1371/journal.pone.0100632
132. Osswald CR, Guthrie MJ, Avila A, Valio JA Jr, Mieler WF, Kang-Mieler JJ. In vivo efficacy of an injectable microsphere-hydrogel ocular drug delivery system. Curr Eye Res. 2017;42(9):1293–1301. doi:10.1080/02713683.2017.1302590
133. Liu W, Lee BS, Mieler WF, Kang-Mieler JJ. Biodegradable microsphere-hydrogel ocular drug delivery system for controlled and extended release of bioactive aflibercept in vitro. Curr Eye Res. 2019;44(3):264–274. doi:10.1080/02713683.2018.1533983
134. Yu Y, Xu S, Yu S, et al. A hybrid genipin-cross-linked hydrogel/nanostructured lipid carrier for ocular drug delivery: cellular, ex vivo, and in vivo evaluation. ACS Biomater Sci Eng. 2020;6(3):1543–1552. doi:10.1021/acsbiomaterials.9b01800
135. Glisoni RJ, Garcia-Fernandez MJ, Pino M, et al. beta-Cyclodextrin hydrogels for the ocular release of antibacterial thiosemicarbazones. Carbohydr Polym. 2013;93(2):449–457. doi:10.1016/j.carbpol.2012.12.033
136. Zhang Z, Yu J, Zhou Y, et al. Supramolecular nanofibers of dexamethasone derivatives to form hydrogel for topical ocular drug delivery. Colloids Surf B Biointerfaces. 2018;164:436–443. doi:10.1016/j.colsurfb.2018.01.051
137. Ilochonwu BC, van der Lugt SA, Annala A, et al. Thermo-responsive Diels-Alder stabilized hydrogels for ocular drug delivery of a corticosteroid and an anti-VEGF fab fragment. J Control Release. 2023;361:334–349. doi:10.1016/j.jconrel.2023.07.052
138. Wan X, Gu J, Zhou X, et al. Establishment of human corneal epithelial organoids for ex vivo modelling dry eye disease. Cell Prolif. 2024;57(11):e13704. doi:10.1111/cpr.13704
139. Hau KL, Lane A, Guarascio R, Cheetham ME. Eye on a dish models to evaluate splicing modulation. Methods Mol Biol. 2022;2434:245–255. doi:10.1007/978-1-0716-2010-6_16
140. Arthur P, Muok L, Nathani A, et al. Bioengineering human pluripotent stem cell-derived retinal organoids and optic vesicle-containing brain organoids for ocular diseases. Cells. 2022;11(21). doi:10.3390/cells11213429
141. Rodboon T, Yodmuang S, Chaisuparat R, Ferreira JN. Development of high-throughput lacrimal gland organoid platforms for drug discovery in dry eye disease. SLAS Discov. 2022;27(3):151–158. doi:10.1016/j.slasd.2021.11.002
142. Duot M, Viel R, Viet J, et al. Eye lens organoids made simple: characterization of a new three-dimensional organoid model for lens development and pathology. Cells. 2023;12(20). doi:10.3390/cells12202478
143. Duot M, Viel R, Viet J, et al. Eye lens organoids going simple: characterization of a new 3-dimensional organoid model for lens development and pathology. bioRxiv. 2023. doi:10.1101/2023.07.12.548679
144. Wright CB, Becker SM, Low LA, Tagle DA, Sieving PA. Improved ocular tissue models and eye-on-a-chip technologies will facilitate ophthalmic drug development. J Ocul Pharmacol Ther. 2020;36(1):25–29. doi:10.1089/jop.2018.0139
145. Chung M, Lee S, Lee BJ, Son K, Jeon NL, Kim JH. Wet-AMD on a chip: modeling outer blood-retinal barrier in vitro. Adv Healthc Mater. 2018;7(2). doi:10.1002/adhm.201700028
146. Chan YK, Sy KH, Wong CY, Man PK, Wong D, Shum HC. In vitro modeling of emulsification of silicone oil as intraocular tamponade using microengineered eye-on-a-chip. Invest Ophthalmol Vis Sci. 2015;56(5):3314–3319. doi:10.1167/iovs.15-16728
147. Lu Y, Chan YK, Lau LH, et al. Adhesion of silicone oil and emulsification: an in vitro assessment using a microfluidic device and ‘Eye-on-a-Chip’. Acta Ophthalmol. 2019;97(3):313–318. doi:10.1111/aos.13982
148. Li Y, Lin D, Chen J, et al. Alkaline phosphatase-responsive hydrogel for efficient management of autoimmune intraocular inflammation. J Control Release. 2025;387:114229. doi:10.1016/j.jconrel.2025.114229
149. Yang M, Chen X, Chen Z, et al. Thermoresponsive antioxidant metal-free carbon nanodot hydrogel: an effective therapeutic approach for ocular surface disease. Sci Adv. 2025;11(30):eadt8775. doi:10.1126/sciadv.adt8775
150. Rafael D, Guerrero M, Marican A, et al. Delivery systems in ocular retinopathies: the promising future of intravitreal hydrogels as sustained-release scaffolds. Pharmaceutics. 2023;15(5). doi:10.3390/pharmaceutics15051484
151. Ibeas Moreno E, Alonso MJ, Abbadessa A. Intraocular injectable hydrogels for the delivery of cells and nanoparticles. Mater Today Bio. 2025;32:101767. doi:10.1016/j.mtbio.2025.101767
152. Achberger K, Probst C, Haderspeck J, et al. Merging organoid and organ-on-a-chip technology to generate complex multi-layer tissue models in a human retina-on-a-chip platform eLife. 2019 8 e46188. doi:10.7554/eLife.46188
153. Gabriel E, Albanna W, Pasquini G, et al. Generation of iPSC-derived human forebrain organoids assembling bilateral eye primordia. Nat Protoc. 2023;18(6):1893–1929. doi:10.1038/s41596-023-00814-x
154. Zuo R, Wei S, Wang Y, Irsch K, Kang JU. High-resolution in vivo 4D-OCT fish-eye imaging using 3D-UNet with multi-level residue decoder. Biomed Opt Express. 2024;15(9):5533–5546. doi:10.1364/BOE.532258
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.