Back to Journals » International Journal of Women's Health » Volume 18
Bridging Knowledge Gaps: Prenatal Education Acquisition and Its Determinants Among Expectant Mothers in Northwestern China
Authors Yang X, Ning Y, He Y, Wan Nordin N, Chen XW ![]()
Received 7 January 2026
Accepted for publication 16 March 2026
Published 24 March 2026 Volume 2026:18 579836
DOI https://doi.org/10.2147/IJWH.S579836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Xiali Yang,1,2 Yanhua Ning,3 Ying He,1 Nadzratulaiman Wan Nordin,4 Xin Wee Chen2
1Department of Maternal and Infant Nursing, School of Nursing, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 2Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Selangor, Malaysia; 3Department of Community Nursing, School of Nursing, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 4Department of Obstetrics and Gynaecology, Faculty of Medicine, Universiti Teknologi MARA, Selangor, Malaysia
Correspondence: Xin Wee Chen, Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Selangor, Malaysia, Tel + 603-6126 7187, Email [email protected]
Introduction: High-risk pregnancies (HRPs) remain a significant global public health issue, notably increasing maternal and neonatal morbidity and mortality. Prenatal education is crucial in mitigating the risks associated with HRPs by providing expectant mothers with essential health information. This study aims to investigate the factors associated with frequent acquisition of prenatal knowledge.
Methods: A multicentre cross-sectional study was conducted between March and October 2023 involving 1211 pregnant women from three hospitals in Northwestern China. Data were collected via a self-administered questionnaire. Frequent prenatal knowledge acquisition was defined as seeking information at least three times per week. Both simple and multivariate logistic regression analyses were performed to identify determinants. Crude odds ratios (ORs) and adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated, and model discrimination was assessed using the area under the receiver operating characteristic curve (AUC).
Results: Approximately 69.5% of participants reported regularly seeking prenatal information. Healthcare professionals were the most cited information source (64.7%). The multivariate logistic regression model demonstrated good discrimination (AUC = 0.75). Six factors were significantly associated with frequent knowledge acquisition: high-risk pregnancy (AOR=1.49, 95% CI: 1.15– 1.94), higher household income (AOR=1.45, 95% CI: 1.06– 1.98), shorter distance to healthcare facilities (AOR=2.65, 95% CI: 1.80– 3.91 for < 30 min), public sector employment (AOR=2.04, 95% CI: 1.40– 2.99), attending ≥four antenatal visits (AOR=2.49, 95% CI: 1.27– 4.89), and being in a long-distance marriage (AOR=2.21, 95% CI: 1.40– 3.51).
Conclusion: The acquisition of prenatal knowledge is influenced by high-risk pregnancy status and multiple sociodemographic factors. Priority interventions should target underserved groups, particularly low-income families, women in remote areas, and those with high-risk pregnancies. Health systems should enhance equitable access by combining digital platforms for urban populations with community-based outreach (e.g, mobile clinics, health workers) for marginalized communities.
Plain Language Summary: Some pregnancies carry higher risks, potentially leading to health issues. Prenatal education helps expectant mothers recognise problems early and make informed decisions.
This study looked at how often pregnant women learn new information and the factors that affect their learning. 1211 women completed a survey during their first antenatal visit.
About 70% regularly sought information on pregnancy health. Factors enabling this included a high-risk pregnancy, higher household income, living closer to healthcare facilities, public-sector employment, attending ≥ 4 antenatal visits, or being in a long-distance marriage. Healthcare professionals were the most trusted information source.
The findings highlight the need to improve access to reliable prenatal education, especially for women in underserved settings.
Keywords: high-risk pregnancy, prenatal care, health knowledge, attitudes, practice, information-seeking behaviour, sociodemographic factors
Introduction
High-risk pregnancies (HRPs) remain a major global public health issue due to their association with increased maternal and neonatal morbidity and mortality.1 These pregnancies often require intensified monitoring, timely interventions, and informed decision-making throughout the antenatal period. Consequently, acquiring comprehensive prenatal knowledge is crucial, as it equips women with the information needed to identify complications, adhere to medical advice, and adopt healthier behaviors.2 Research has consistently demonstrated that well-informed pregnant women are more likely to engage in proactive health-seeking behaviors and seek prompt medical attention when needed.3
Globally, the frequency and sources of prenatal knowledge acquisition vary considerably across settings. In high-income countries such as Sweden, Australia, and the United States, widespread use of digital health technologies, robust healthcare infrastructure, and regular contact with medical professionals contribute to prenatal knowledge acquisition rates exceeding 80%.4–6 In these contexts, mobile applications and online platforms have become increasingly prominent information sources alongside traditional healthcare providers.7 Conversely, in many low- and middle-income countries, including Bangladesh and Papua New Guinea, weak health systems, limited digital infrastructure, and lower health literacy result in significantly lower engagement with prenatal information, often below 50%.8,9 Despite these global disparities, healthcare providers are consistently regarded as the most trusted source of prenatal information across all settings, while digital and print media vary considerably in quality and accuracy.3
In China, prenatal education is recognized as a critical component of maternal health policy; however, significant inequalities persist in both access to and participation in prenatal knowledge acquisition. Pregnant women in urban areas typically benefit from better access to health resources, regular antenatal care, and diverse educational opportunities.10 In contrast, those in rural and less developed regions, particularly in Northwestern China, face substantial barriers to acquiring essential knowledge.11 These challenges include inadequate healthcare infrastructure, lower health literacy levels, geographic isolation, limited interaction with qualified healthcare professionals, and cultural and linguistic diversity among ethnic minority populations.10–12 Migration-related family separation, common in rural Northwest China, further impedes the sharing of health information within households.13
While previous studies have examined prenatal information-seeking in various contexts, several knowledge gaps remain. Most research has focused either on clinical outcomes of high-risk pregnancies or on general patterns of information source utilization, with limited integration of high-risk pregnancy status as a potential determinant of active information-seeking behavior.1,2 Although spatial accessibility to healthcare facilities is known to influence service utilization, its association with the frequency of knowledge acquisition remains underexplored, particularly in geographically remote regions.14 The rapid proliferation of digital health information sources warrants updated investigation into how pregnant women navigate and integrate multiple information channels including healthcare providers, mobile applications, social media, and traditional media in their efforts to obtain reliable prenatal guidance.6,7 Furthermore, few studies have simultaneously examined the relative contributions of clinical, spatial, and sociodemographic factors using multivariate modeling in a large, representative sample from an underserved region.3,15
Guided by Andersen’s Behavioral Model16 and health literacy theory,17 this study investigated the frequency and determinants of prenatal knowledge acquisition among pregnant women in Northwestern China. Using a large representative sample (N=1211), we aimed to determine the prevalence of frequent knowledge acquisition ≥three times/week);18 and identify factors associated with frequent information-seeking. We hope to have a better insight regarding prenatal information seeking among the expectant mothers, given that Northwestern China is one of China’s smallest and less economically developed regions. The findings are expected to inform the creation of more equitable, effective, and contextually appropriate strategies for maternal health education.
Methods
Study Design
This multicentre study was conducted from March to October 2023 in the Ningxia Hui Autonomous Region, north-western China, involving 1211 pregnant women. Participants were chosen from those attending antenatal check-ups at three hospitals: Ningxia Medical University General Hospital, Ningxia Hui Autonomous Region People’s Hospital, and Yinchuan First People’s Hospital.
Study Population
Pregnant women admitted to the obstetric ward were consecutively recruited by the research team using a systematic random sampling method at an interval of k=3. The inclusion criteria were: (i) women who had delivered between March and October 2023; (ii) residents of Ningxia who remained in the region throughout their pregnancy; and (iii) those who received antenatal care at the same hospital where they delivered. The exclusion criteria included: (i) individuals with communication difficulties (eg, inability to understand Chinese, requiring intensive medical monitoring, or diagnosed with cognitive impairments); (ii) those who did not give consent; and (iii) patients referred to other healthcare facilities for ongoing treatment.
Sample Size Estimation
The sample size was calculated using the following formula:  .19 Based on an expected 50% prevalence of knowledge acquisition (a conservative estimate),3 with a 5% margin of error and a 95% confidence level, the minimum sample required was 1211 (including a 10% non-response rate).
.19 Based on an expected 50% prevalence of knowledge acquisition (a conservative estimate),3 with a 5% margin of error and a 95% confidence level, the minimum sample required was 1211 (including a 10% non-response rate).
Data Collection
Data were collected using a structured, self-administered questionnaire administered during participants’ initial antenatal visits. Trained research assistants were present during data collection to clarify any questions/minimise information bias and ensure completeness of responses. Participants were assured of the anonymity and confidentiality of their responses to encourage honest reporting to minimise social desirability bias.
The proforma checklist was developed based on an extensive literature review of similar studies on prenatal health information-seeking behavior3,5,18 and adapted to the local context of Northwestern China. The instrument consisted of three main sections: (1) sociodemographic characteristics (age, education, occupation, household income, marital status, distance to healthcare facilities); (2) pregnancy-related factors (number of antenatal care visits, high-risk pregnancy status); and (3) patterns of knowledge acquisition (frequency of seeking information, sources of health information).
A pilot study was conducted with 50 pregnant women not included in the main study sample to assess the questionnaire’s clarity, comprehensibility, and internal consistency. The Cronbach’s alpha coefficient for the knowledge acquisition section was 0.82, indicating good reliability. Minor wording adjustments were made based on the pilot results to enhance clarity.
Study Tools and Variables
The primary outcome variable was the frequency of prenatal knowledge acquisition, categorised as frequent (≥3 times per week) or infrequent (<3 times per week).18
High-risk pregnancy status (yes/no) at booking was defined using a standardised five-colour risk assessment tool (green, yellow, orange, red, purple) implemented in Chinese maternal health services.20 To enhance efficiency in clinical and research settings, green was categorized as non-high-risk, while all other colors were classified as high-risk. This risk assessment tool stratifies pregnancies based on established clinical and obstetric risk criteria, including individual and sociodemographic factors, past obstetric history, gynecological history, internal medicine conditions, and pregnancy-related complications.1,2
Sources of knowledge included healthcare workers, books, antenatal classes, mobile applications, television, and relatives or friends. Independent variables comprised sociodemographic factors (education, household income, distance to healthcare facilities, occupation, presence of long-distance marriage) and pregnancy-related factors (number of antenatal care visits, high-risk pregnancy status).
Statistical Analysis
Descriptive statistics were used to summarise participants’ characteristics and the frequencies of knowledge acquisition. Categorical variables were presented as frequencies and percentages. The chi-square test was employed to examine differences between groups.
Simple logistic regression analysis was conducted to explore the relationships between independent variables and frequent knowledge acquisition, with crude odds ratios (OR) and 95% confidence intervals (CI) calculated. Variables with p-values less than 0.25 in the simple logistic regression were then included in the multivariate binary logistic regression model using backward stepwise selection to calculate adjusted odds ratios (AOR) with 95% CI. The threshold of 0.25 was chosen as a conservative criterion to avoid excluding potentially important variables that might be significant after adjusting for confounders.19
For categorical variables, thresholds were selected based on clinically meaningful cut-offs or distribution in the data. Distance to healthcare facilities was categorized as <30 minutes, 30–60 minutes, and ≥60 minutes based on previous studies indicating that travel time significantly impacts healthcare access and utilization.8 The cut-off of ≥4 antenatal care visits align with the World Health Organization’s recommended minimum number of visits for standard antenatal care.1
The model’s goodness-of-fit was assessed using the Hosmer-Lemeshow test; a p-value >0.05 indicates adequate fit. Discrimination was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC), with values above 0.70 considered acceptable To assess internal validity, bootstrap resampling with 1000 replications was performed to calculate bias-corrected confidence intervals for the AORs, confirming the stability of estimates. Multicollinearity was assessed using variance inflation factors (VIFs), with all VIF values <2.0, indicating no significant multicollinearity. A p-value of less than 0.05 was regarded as statistically significant. All statistical analyses were performed using SPSS software, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Participant Characteristics
A total of 1300 pregnant women were recruited; however, only 1211 met the study’s criteria and were enrolled. The participation rate was 100%, with 1211 women recruited and analysed. The women included in the analysis ranged in age from 17 to 43 years. They had a mean (standard deviation, SD) age of 29.9 (4.74) years.
The study showed a high level of prenatal knowledge acquisition, with 842 participants (69.5%) reporting frequent information-seeking (≥3 times per week; 95% CI: 66.9%, 72.1%). Table 1 presents the characteristics of pregnant women stratified by frequency of knowledge acquisition. Among participants, 721 (59.5%) had tertiary education qualifications (junior college or bachelor’s degree or above), while 847 households (69.9%) reported monthly incomes exceeding 4000 yuan. Medical facilities were accessible within 30 minutes for 698 women (57.6%). Notably, 1176 participants (97.1%) completed four or more antenatal care visits. A total of 567 women (46.8%) were classified as having high-risk pregnancies. Regarding marital circumstances, 1065 women (87.9%) were in non-long-distance marriages. Employment was distributed across sectors, with the largest proportions working in private enterprises (29.0%) and as housewives (25.7%), followed by civil service or public sector roles (21.9%).
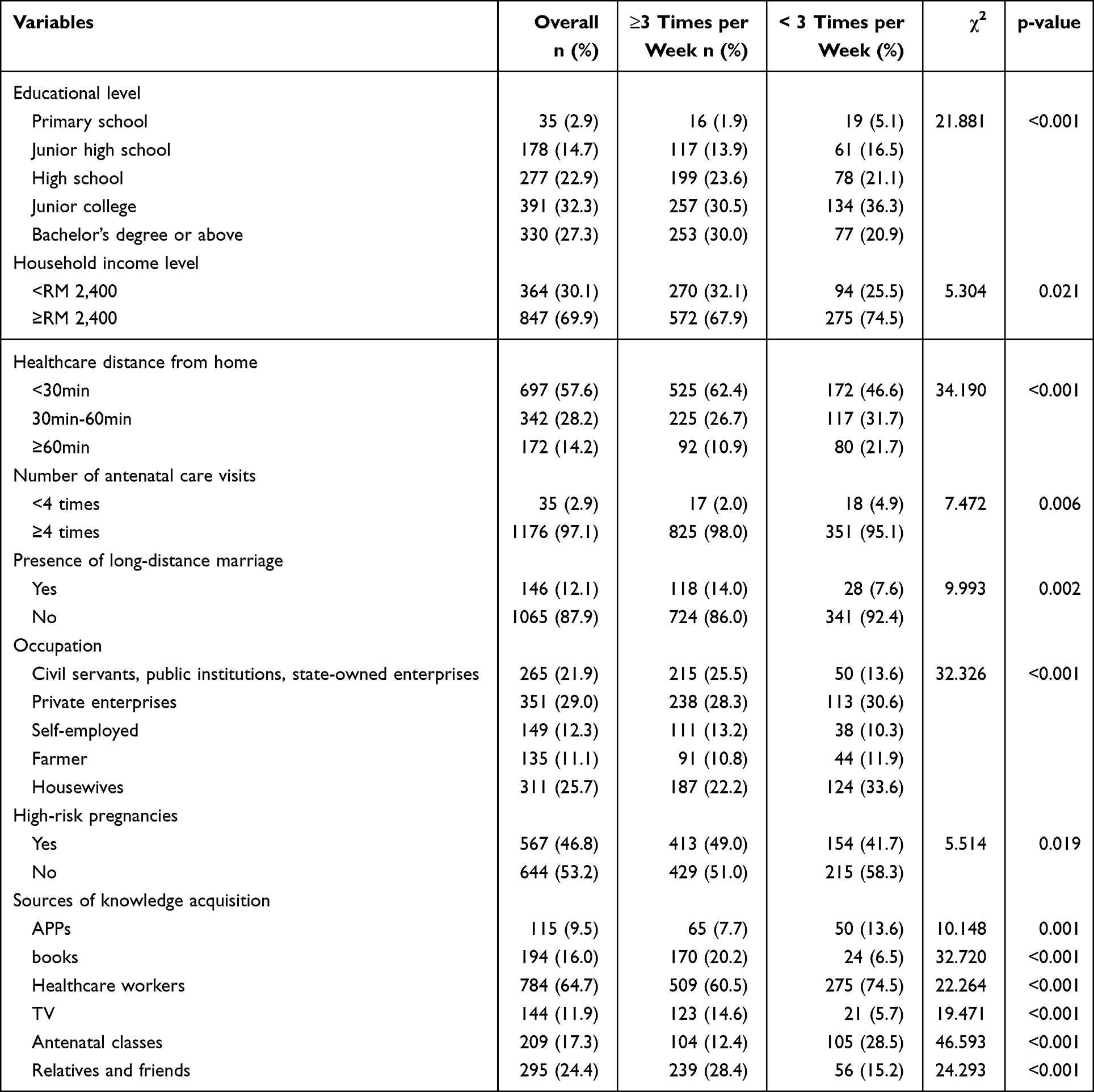 |
Table 1 Knowledge Acquisition Frequency During Pregnancy Among Study Participants (n=1211) |
Sources of Prenatal Information
When asked about their main sources of prenatal information, participants reported various methods and channels. Healthcare workers were the most frequently cited source, mentioned by 784 women (64.7%), highlighting the importance of clinical encounters in health education during pregnancy. Relatives and friends (24.4%) and books (16.0%) served as key secondary sources, especially for informal and supplementary information. Mobile applications (9.5%) and antenatal classes (17.3%) were also used, but to a lesser degree.
Notable differences in how people use information sources appeared when comparing frequent and infrequent knowledge seekers. Women who reported more frequent knowledge gathering were significantly more likely to use books (20.2% vs. 6.5%, p < 0.001) and to rely on relatives or friends (28.4% vs. 15.2%, p < 0.001) compared to those who sought information less often. Conversely, infrequent seekers depended more on healthcare workers (74.5% vs. 60.5%, p < 0.001) and antenatal classes (28.5% vs. 12.4%, p < 0.001). This pattern indicates that frequent information seekers take a more varied and active approach, combining professional advice with informal and self-directed learning, while infrequent seekers rely more on formal, structured sources.
Factors Associated with Frequent Knowledge Acquisition
Table 2 presents the results of the logistic regression analysis. In the simple logistic regression, seven factors were significantly associated with frequent acquisition of prenatal knowledge: high-risk pregnancy, higher household income, shorter distance to healthcare facilities, attending four or more antenatal care visits, being in a long-distance marriage, employment in the public sector, and higher educational attainment.
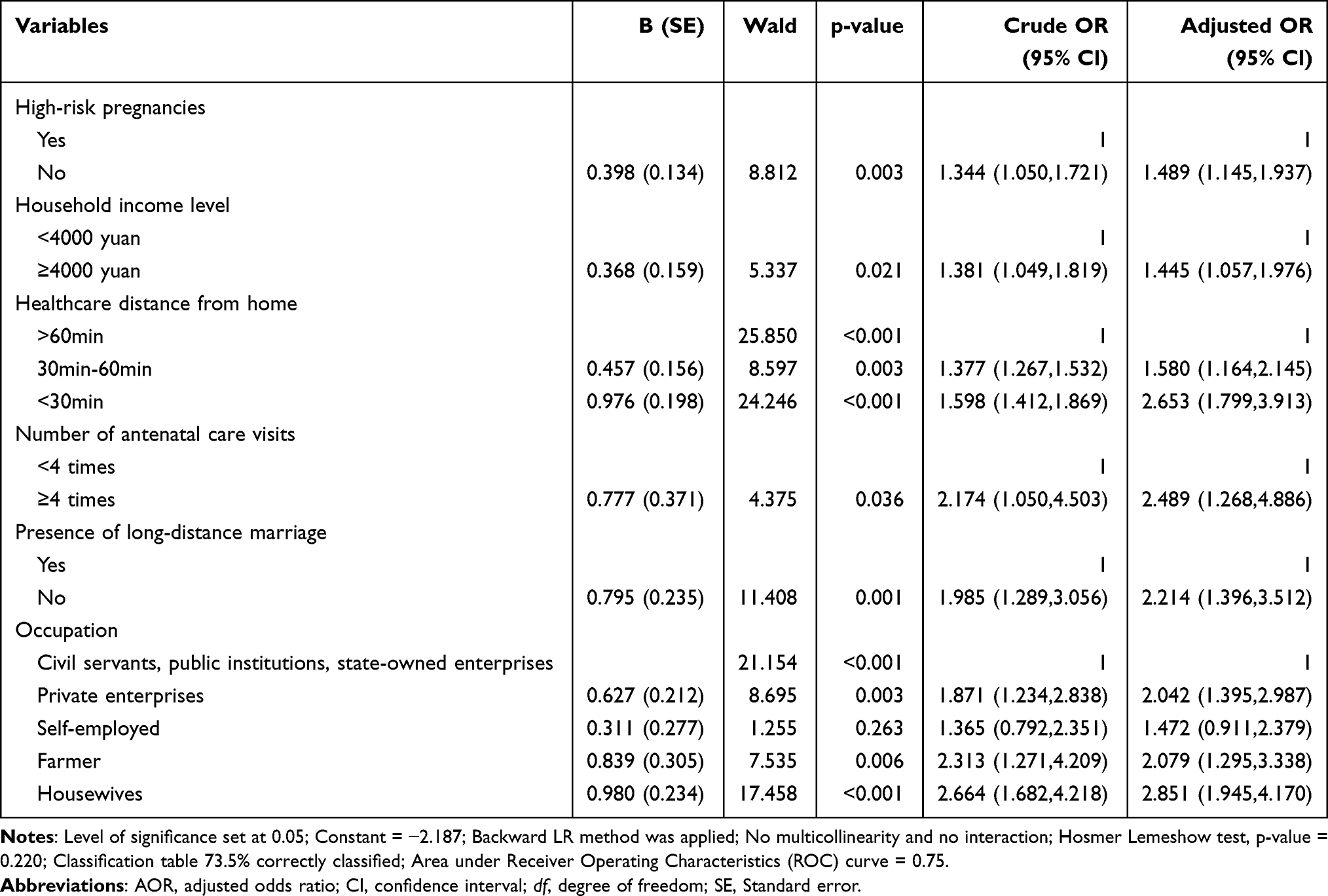 |
Table 2 Factors Associated with Frequent Knowledge Acquisition During Pregnancy Using Simple and Binary Logistic Regression Analysis (n=1211) |
After adjusting for potential confounders in the multivariate model, six factors remained statistically significant. Women with high-risk pregnancies were more likely to report frequent knowledge acquisition (AOR=1.49, 95% CI: 1.15–1.94). Higher household income (≥4000 yuan per month) was positively associated with frequent information seeking (AOR=1.45, 95% CI: 1.06–1.98). Shorter distance to healthcare facilities showed a graded association: compared to women living ≥60 minutes away, those residing within 30–60 minutes (AOR=1.58, 95% CI: 1.16–2.15) and those within 30 minutes (AOR=2.65, 95% CI: 1.80–3.91) had progressively higher odds of frequent knowledge acquisition. Attending four or more antenatal care visits was strongly associated with frequent information seeking (AOR=2.49, 95% CI: 1.27–4.89). Women in long-distance marriages were more likely to seek information frequently (AOR=2.21, 95% CI: 1.40–3.51). Compared to housewives, women employed in the public sector (civil servants, public institutions, state-owned enterprises) had higher odds of frequent knowledge acquisition (AOR=2.04, 95% CI: 1.40–2.99), as did farmers (AOR=2.08, 95% CI: 1.30–3.34).
The multivariate model demonstrated good fit (Hosmer-Lemeshow test, p=0.220) and acceptable discrimination, with an area under the ROC curve of 0.75, indicating that the model correctly classified 75% of participants. Bootstrap resampling with 1000 replications confirmed the stability of the estimates, with bias-corrected confidence intervals consistent with the original analysis.
Discussion
This study aimed to investigate the frequency of prenatal knowledge acquisition and its determinants among pregnant women in Northwestern China. Two main findings emerged: (i) 842 (69.5%) women reported frequently acquiring prenatal knowledge (defined as at least three times per week), and (ii) various socio-demographic factors, such as high-risk pregnancy, higher household income, shorter distance to medical facilities, attending four or more ANC visits, being in a long-distance marriage, and working in the public sector, were significantly associated with this behaviour.
Among the 1211 women surveyed, 842 (69.5%) reported regularly acquiring prenatal knowledge, defined as accessing maternal health information at least three times per week. This prevalence rate sits at an intermediate position in the global landscape, substantially exceeding rates reported in low- and middle-income countries such as Bangladesh and Papua New Guinea (often below 50%),8,9 while remaining below the over 80% level typical of high-income countries such as Sweden, Australia, and the United States.4–6 This probably demonstrates China’s ongoing progress in expanding access to antenatal care, adopting mobile health solutions, and implementing community education initiatives; nonetheless, it also highlights that further improvements depend on addressing region-specific barriers, particularly in underdeveloped western regions, for rural, ethnic minority, and low-income populations.10–12
Geographic proximity and socioeconomic status impact maternal health knowledge through different but related pathways. Shorter distances to healthcare facilities encourage more prenatal visits and direct communication with providers.3,11,14 In our study, this graded association was clearly demonstrated (compared to women living ≥60 minutes away, those residing within 30–60 minutes and those within 30 minutes) had progressively higher odds of frequent knowledge acquisition. Women with higher incomes find it easier to overcome geographic barriers by using private transportation and digital tools.21–23 Conversely, women in rural areas and ethnic minorities face ongoing access challenges due to infrastructural limitations.9,11,12 Urban residents benefit from improved access and additional resources, which support increased knowledge.5–7 Studies across diverse settings affirm the consistent influence of spatial and socioeconomic factors.1,13,15,22,24,25 These factors primarily affect knowledge dissemination through increased healthcare utilization and access to digital information platforms.3,6,13,26
Educational attainment proved to be a notable factor. Women with higher levels of education demonstrated greater initiative and confidence in finding accurate health information, aligning with current concepts of health literacy.8,13 However, it is noteworthy that, although educational level was significantly associated with frequent knowledge acquisition in the univariate analysis, this association did not remain statistically significant after adjusting for other covariates in the multivariate model. This suggests that the effect of education may be mediated or confounded by other factors such as household income, employment type, and access to healthcare services, all of which remained significant in the final model. This finding agrees with previous research indicating that education enables health information seeking primarily by improving access to resources and opportunities.8,13 Perhaps integrating maternal health education into formal schooling or community-based learning platforms could be vital in raising awareness, especially among younger or first-time mothers. Such efforts might promote proactive engagement with antenatal services from early pregnancy stages.
Employment status further influenced access to information, it was found that public sector employment was associated with higher odds of frequent knowledge acquisition compared to housewives. Women working in the public sector were more likely to engage in regular knowledge acquisition, possibly because of consistent work schedules and institutional support, such as maternity leave or workplace health education programmes.8 On the other hand, women in private or informal employment often faced stricter working conditions and had limited access to health education opportunities. Offering mobile-accessible or flexible health education options could help overcome these structural barriers and expand the reach of maternal health information.7
The nature of marital relationships also plays a significant role. Women in long-distance marriages are less likely to report frequent information acquisition, which may be due to emotional stress and reduced family support in the absence of a cohabiting partner.26 Engaging spouses through telecommunication tools or remote participation in prenatal consultations could improve emotional and informational support during pregnancy.27,28 Conversely, couples living together may facilitate each other’s engagement with health education, and community-based peer support systems might strengthen this dynamic by fostering environments conducive to shared learning and emotional resilience.27
Antenatal care utilisation is closely linked to maternal knowledge acquisition, with women attending ≥4 visits engaging more actively with health information, emphasising healthcare providers’ vital educational role.1,2,4 Studies indicate that structured ANC enhances health literacy, particularly in high-risk pregnancies,2 while frequent visits raise risk awareness.1 Although the information provided by providers is highly trusted,3 women in rural areas often rely on informal networks due to access barriers. Culturally adapted programmes such as China’s Five Colour Project20 and community ANC initiatives15 effectively improve knowledge in underserved regions, especially among migrant populations.13
Women with high-risk pregnancies are less likely to gain frequent prenatal knowledge. In such cases, clinical encounters often focus on diagnostic monitoring and therapeutic interventions, leaving limited time for preventive education;1,2 communication gaps and structural challenges within care settings further deepen this imbalance, especially among disadvantaged groups.4,11 This disparity emphasises the importance of tailored educational strategies for high-risk women, focusing on recognising warning signs, self-monitoring practices, and reinforcing essential health behaviours.2 Using historical health data to develop predictive models may enable earlier detection and timely, personalised interventions.29 Furthermore, digital platforms and social media can be effective channels for disseminating maternal health information, especially among younger women who engage more with digital technology.6,7
This study indicates that maternal knowledge acquisition is significantly influenced by socioeconomic status, educational background, geographical location, and access to healthcare services. These factors directly impact antenatal health behaviours and maternal and neonatal outcomes.3,15,20,22 Addressing such inequalities should become a priority for public health. Effective strategies may include community-based outreach adapted to local contexts, accessible digital health tools, and culturally sensitive communication methods.6,13,26 Special attention should be given to women with limited financial means, those residing in remote or underserved areas, and individuals identified as high risk, as these groups encounter the greatest barriers to information and care.
This study has several limitations. The mainly urban sample (83.8%) may limit the applicability of the findings to rural populations with less access to maternal health services and information. Psychosocial factors, such as stress, social support, and mental health, were not assessed despite their potential influence on knowledge-seeking behaviours and pregnancy outcomes.3,9 The cross-sectional design restricts the ability to determine causality between the observed associations. Future research should utilise longitudinal designs to establish temporal sequences and employ mixed methods to explore how cultural, social, and experiential factors affect women’s engagement with maternal health information. Evaluating the impact of mobile education platforms, male partner involvement, and Artificial Intelligence-based risk detection could provide scalable approaches to enhance equitable access to maternal health knowledge.8,30
Conclusion
This study reveals that high-risk pregnancy status and various sociodemographic factors are significantly associated with the frequency of prenatal information seeking among pregnant women in Northwestern China. The identified factors include high-risk pregnancy, higher household income, shorter distance to healthcare facilities, attending four or more antenatal care visits, long-distance marriage, and public-sector employment. Nevertheless, these associations are correlational and do not confirm causal relationships.
On this note, a future longitudinal study that includes other potentially influential unaccounted factors (such as digital literacy, cultural attitudes, the quality of education and counselling provided) is highly recommended.17,27 Additionally, this study highlights that information is the fundamental building block that transforms maternal health from passive medical management to active, informed participation. Hence, policymakers should prioritise expanding equitable access to prenatal education for underserved groups through community-based outreach, provide economic support for transportation and digital access, and integrate structured education into high-risk care protocols. These targeted and customised strategies can help bridge the knowledge gap for low-income families, rural residents, and women experiencing geographic or social isolation.
Data Sharing Statement
The data that support the findings of this Studies are available on request from the corresponding author.
Ethics Approval Statement
This study was approved by the Human Research Ethics Committee of Ningxia Medical University (no. 2022-G019) and complied with the Declaration of Helsinki. Informed consents were obtained from the study participants prior to study commencement. Married participants under the age of 18 are granted full civil capacity upon legally contracted marriage in China and provided consent independently.31
Acknowledgments
The authors thank the Ningxia Medical University General Hospital, Ningxia Hui Autonomous Region People’s Hospital and Yinchuan First People’s Hospital for collecting data. The authors also thank all participants who participated in our research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the 2024 First Class Discipline Incubation Project of the School of Nursing, Ningxia Medical University (NYHLYB202403).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rajbanshi S, Norhayati MN, Nik Hazlina NH. High-risk pregnancies and their association with severe maternal morbidity in Nepal: a prospective cohort study. PLoS One. 2020;15(12):e0244072. doi:10.1371/journal.pone.0244072
2. Shojaeian Z, Khadivzadeh T, Sahebi A, Kareshki H, Tara F. Knowledge valuation by Iranian women with high-risk pregnancy: a qualitative content analysis. Int J Community Based Nurs Midwifery. 2020;8(3):243–10. doi:10.30476/IJCBNM.2020.83305.1139
3. Vogels-Broeke M, Daemers D, Budé L, de Vries R, Nieuwenhuijze M. Sources of information used by women during pregnancy and the perceived quality. BMC Pregnancy Childbirth. 2022;22(1):109. doi:10.1186/s12884-022-04422-7
4. Kawish AB, Umer MF, Arshed M, Khan SA, Hafeez A, Waqar S. Respectful maternal care experience in low- and middle-income countries: a systematic review. Medicina (Kaunas). 2023;59(10):1842. doi:10.3390/medicina59101842
5. Ghiasi A. Health information needs, sources of information, and barriers to accessing health information among pregnant women: a systematic review of research. J Matern Fetal Neonatal Med. 2021;34(8):1320–1330. doi:10.1080/14767058.2019.1634685
6. Fitzgerald H, Frank M, Kasula K, Krans EE, Krishnamurti T. Usability and acceptability of a pregnancy app for substance use screening and education: a mixed methods exploratory pilot study. JMIR Pediatr Parent. 2025;8:e60038. doi:10.2196/60038
7. Hochmuth A, Hochmuth AM, Dockweiler C. Digital health technologies enabling the transition from pregnancy to early parenthood: a scoping review. Z Evid Fortbild Qual Gesundhwes. 2025;193:82–92. doi:10.1016/j.zefq.2024.11.013
8. Palani D, Tucker J, Briley A. Developing antenatal education resources for CALD women: first steps, exploring what women from CALD backgrounds want and need. Midwifery. 2025;145:104367. doi:10.1016/j.midw.2025.104367
9. Abedin S, Arunachalam D. Maternal autonomy and high-risk pregnancy in Bangladesh: the mediating influences of childbearing practices and antenatal care. BMC Pregnancy Childbirth. 2020;20(1):555. doi:10.1186/s12884-020-03260-9
10. Ma Y, Gao Y, Li J, et al. Maternal health behaviors during pregnancy in rural Northwestern China. BMC Pregnancy Childbirth. 2020;20(1):745. doi:10.1186/s12884-020-03444-3
11. Huang Y, Martinez-Alvarez M, Shallcross D, et al. Barriers to accessing maternal healthcare among ethnic minority women in Western China: a qualitative evidence synthesis. Health Policy Plan. 2019;34(5):384–400. doi:10.1093/heapol/czz040
12. Wu Y, Zhou H, Wang Q, Cao M, Medina A, Rozelle S. Use of maternal health services among women in the ethnic rural areas of western China. BMC Health Serv Res. 2019;19(1):179. doi:10.1186/s12913-019-3996-2
13. Eghrari D, Scoullar MJL, Wilson AN, et al. Low knowledge of newborn danger signs among pregnant women in Papua New Guinea and implications for health-seeking behaviour in early infancy: findings from a longitudinal study. BMC Pregnancy Childbirth. 2023;23(1):71. doi:10.1186/s12884-022-05322-6
14. Jiang H, Wang Y, Cheng Y, Zhang M, Feng L, Wang S. Transport accessibility and hospital attributes: a nonlinear analysis of their impact on women’s prenatal care seeking behavior. Health Place. 2024;87:103250. doi:10.1016/j.healthplace.2024.103250
15. Yang J, Chen J, Xie Y, et al. Challenges in rural maternal health: how received public services and policy awareness affect health knowledge and practices. Front Public Health. 2025;12. 1514522. doi:10.3389/fpubh.2024.1514522
16. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10.
17. Yeo G, Reich SM, Liaw NA, Chia EYM. The effect of digital mental health literacy interventions on mental health: systematic review and meta-analysis. J Med Internet Res. 2024;26:e51268. doi:10.2196/51268
18. Sayakhot P, Carolan-Olah M. Internet use by pregnant women seeking pregnancy-related information: a systematic review. BMC Pregnancy Childbirth. 2016;16:65. doi:10.1186/s12884-016-0856-5
19. Arifin WN. Sample size calculator. 2023. Available from: http://wnarifin.github.io.
20. Qin H. Evaluation of the effectiveness of the five color project management during pregnancy and childbirth in the management of pregnant and postpartum women with syphilis infection. Chin J AIDS STD. 2022;28(11):1281–1284. doi:10.13419/j.cnki.aids.2022.11.12
21. Janevic T, Birnie L, Belfon K, et al. Immigrant inequities in uninsurance and postpartum Medicaid extension: a quasi-experimental study in New York City, 2016-2021. Am J Public Health. 2025;115(5):732–735. doi:10.2105/AJPH.2024.307968
22. Vousden N, Geddes-Barton D, Hanley SJ, Roberts N, Knight M. Interventions to reduce inequalities for pregnant women living with disadvantage in high-income countries: an umbrella review. BMC Public Health. 2025;25(1):1140. doi:10.1186/s12889-025-22283-5
23. Ajayi T, Kueper J, Ariniello L, et al. Digital health platform for maternal health: design, recruitment strategies, and lessons learned from the PowerMom observational cohort study. JMIR Form Res. 2025;9:e70149. doi:10.2196/70149
24. Iraqi S, Goldenberg S, Baer RJ, Lemus H, Bandoli G. Variations in adverse pregnancy and birth outcomes among Latin American and Caribbean-born birthing people by region of origin, California birth cohort, 2007-2020. BMC Pregnancy Childbirth. 2025;25(1):384. doi:10.1186/s12884-025-07483-6
25. Asghar Vahedi F, Gholizadeh L, Khajehei M. Knowledge and awareness of cardiovascular risk factors among women with a history of pregnancy complications in Australia: a World Heart Federation cross-sectional study. Aust N Z J Obstet Gynaecol. 2025. doi:10.1111/ajo.70026
26. Wood SN, Yirgu R, Karp C, Tadesse MZ, Shiferaw S, Zimmerman LA. The impact of partner autonomy constraints on women’s health-seeking across the maternal and newborn continuum of care. EClinicalMedicine. 2022;53:101715. doi:10.1016/j.eclinm.2022.101715
27. De Meyer F, Chambaere K, Van de Velde S, Van Assche K, Beernaert K, Sterckx S. Factors influencing obstetricians’ acceptance of termination of pregnancy beyond the first trimester: a qualitative study. BMC Med Ethics. 2025;26(1):32. doi:10.1186/s12910-025-01186-5
28. Medford E, Lane S, Sharp A, Care A. The PRECISION study protocol: can cervical stiffness in the second trimester predict preterm birth in high-risk singleton pregnancies? A feasibility cohort study. PLoS One. 2025;20(2):e0316297. doi:10.1371/journal.pone.0316297
29. Sylvain MH, Nyabyenda EC, Uwase M, Komezusenge I, Ndikumana F, Ngaruye I. Prediction of adverse pregnancy outcomes using machine learning techniques: evidence from analysis of electronic medical records data in Rwanda. BMC Med Inform Decis Mak. 2025;25(1):76. doi:10.1186/s12911-025-02921-z
30. Rafat N, Bakouei F, Delavar MA, Nikbakht HA. Preventing postpartum depression in pregnant women using an app-based health-promoting behaviors program (Pender’s health promotion model): a randomized controlled trial. BMC Psychol. 2025;13(1):243. doi:10.1186/s40359-025-02547-w
31. The Civil Code of the People’s Republic of China. (2020). China Legal Publishing House.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.