Back to Journals » Breast Cancer: Targets and Therapy » Volume 12
Breast Self-Examination Practice and Associated Factors Among Secondary School Female Teachers in Gammo Gofa Zone, Southern, Ethiopia
Authors Mekuria M, Nigusse A ![]() , Tadele A
, Tadele A ![]()
Received 22 September 2019
Accepted for publication 3 December 2019
Published 29 January 2020 Volume 2020:12 Pages 1—10
DOI https://doi.org/10.2147/BCTT.S232021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Mesele Mekuria,1 Aderajew Nigusse,2 Afework Tadele2
1Department of Public Health, Arba Minch College of Health Science, Arba Minch, Ethiopia; 2Population and Family Health, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Afework Tadele Email [email protected]
Introduction: Nowadays, breast self-examination (BSE) is a breast cancer screening method that identifies breast mass by the woman herself. However, it is not widely practiced due to various problems. This study aimed to assess the magnitude of BSE practice and associated factors among female secondary school teachers in Gammo Gofa Zone, South Ethiopia.
Methods: An institution-based cross-sectional study was conducted among 247 female secondary school teachers, from March 1 to 30, 2018. Participants were selected using the lottery method. A self-administered questionnaire was used for data collection. Data were cleaned, coded, and entered into Epi data manager 4.4 and analyzed using SPSS version 21. Binary logistic regression was employed.
Results: Of 82 respondents, 34.3% had ever performed BSE. Among these, only 32 (13.4%) had practiced BSE monthly (regularly). Being knowledgeable on BSE [AOR=2.84, 95% CI (1.41, 5.72)], ever heard about BSE [AOR=2.26, 95% CI (1.07, 4.77)], being married [AOR=4.09, 95% CI (1.64, 10.22)], having less perceived barrier to BSE [AOR=2.62, 95% CI (1.26, 5.46)], having high perceived confidence [AOR=3.63, 95% CI (1.79, 7.39)] and motivation to BSE [AOR=3.29, 95% CI (1.15, 9.45)] were significant predictors of BSE practice.
Conclusion: In this study, one in three women had ever practiced BSE, whereas about one in seven women regularly practiced BSE. The main reasons for not practicing BSE were: not knowing how to perform BSE and forgetfulness (for regular practice). Therefore, integrated work on behavioral change communication and interferences that focus on improving knowledge of BSE, and skills on how to perform BSE is needed. Additionally, the identified domains of the health belief model (perceived barrier, perceived confidence, and perceived motivation) may be the most effective strategies that should be considered by Gammo Gofa Zonal health and educational offices.
Keywords: breast self-examination, breast cancer, health belief model, South Ethiopia
Introduction
These days, an estimated 1.7 million women are diagnosed with breast cancer, and about 522,000 women die from breast cancer globally. It has been predicted that the worldwide incidence of female breast cancer will reach approximately 3.2 million new cases per year by 2050.1 However, the higher burden of cancer was observed in less-developed regions of the world, which accounts for 56% of new cancer cases and 63% of cancer deaths worldwide.2 In Sub-Saharan Africa it is estimated that the prevalence of breast cancer in women aged 15 and over was 23.5 per 100,000 women and an estimated 35,427 women died from breast cancer with a crude mortality rate of 12.8 per 100,000 women.3
While a high proportion of cancers are diagnosed at an early stage in high-income countries, they are diagnosed at more advanced and often fatal stages in developing countries. Moreover, most of the developing nations have recorded a poor outcome and high fatality rate owing to diagnosis of the breast cancer at advanced stages.4 In Ethiopia, about 42,722 incident cancer cases were diagnosed in females in 2015. Breast cancer was by far the commonest cancer, constituting 33% of the cancers in women and 23% of all cancers identified.5 It is the leading cancer among females with a 24.4% prevalence rate and 26,200 women died of breast cancer in 2014.6
Thus, morbidity and mortality associated with breast cancer can be reduced through early detection by means of screening programs, which not only increase the chances for successful treatment and cure of the disease, but also improve chances of survival and lessens the need forinvasive treatment.7 Breast self-examination (BSE) is the most important and recommended screening method for early detection of breast cancer.8 BSE is the process whereby women examine their breasts regularly to detect any breast mass in order to seek early medical attention.6 It is one of the screening methods used to detect breast-related problems such as possible lumps, distortions, or swelling2,9 and it is recommended for every woman above the age of 20 years to be done for 20 min once monthly,2 between the 7th and 10th days of the menstrual cycle (2–3 days after the menses has gone), and goes a long way in detecting breast cancer at early stages of growth when there is a low risk of spread, ensuring a better prognosis when treated.6
However, in Ethiopia, breast cancer screening practice among women was only 6.9%.10 Different studies conclude this may be due to lack of uniform information, education, and communication about the breast cancer disease, and screening methods were found to be a public health challenge.11 In addition, only 12.1% monthly in Kafa, south-west Ethiopia in 2015,12 and only 14.4% of health extension workers (HEWs) in West Gojam practiced BSE regularly;13 one-third of the participants (33.7%) only practiced regularly in 2017 by health professionals in Addis Ababa.2
Factors contributing to the low level of BSE practices as identified by different literatures where knowledge of BSE and breast cancer, income,14 level of education,17,23 ever heard about BSE,15 perception factors and others.10,16,23 However, all these studies neglected female teachers in a school setting and did not test the health belief model to identify perceptions of this population group.
As the majority of Ethiopian populations reside in the rural areas where there is no access to a health facility equipped in mammography, BSE will be the best approach for effective prevention of breast cancer and its complications.
So, this study will identify the different approach that the awareness reaches mothers via the female teachers and in the long run, the students in the school can benefit from their teachers as they can act as a model in the community. In another way, when teachers are well aware of BSE they could go out into their community to educate others. This will be an advantage for economic programs, too, through saving the cost disability-adjusted years of lives lost due to breast cancer and also the cost of health services for the treatment of other forms of breast cancer screening mechanisms.
To this effect, knowing the barriers about breast self-examination practice among study participants through study and addressing it is crucial. Therefore, this study aimed to assess the level of practice of BSE and its associated factors among female secondary school teachers to plan future interventions in this field.
Methods
Study Setting and Period: The study was conducted in Gammo Gofa Zone (GGZ),274 and 502 km from Hawassa (capital of SNNPR) and Addis Ababa (capital of Ethiopia), respectively, from its capital city Arba Minch. Administratively, GGZ is divided into 15 districts and two administrative towns. Based on the 2007 Census conducted by the Central Statistical Agency of Ethiopia (CSA), GGZ has a total population of 1,593,104, of whom 793,322 were men and 799,782 women, with an area of 18,010.99 km2. The study was conducted in GGZ from March 1 to 30, 2018.
Design: An institutionbased cross-sectional study was conducted.
Sample Size Determination
Epi-info version 7.1.1 was used for a single population proportion with the assumptions of 95% confidence level, 5% margin of error, and 10% non-response rate added. To assure sample adequacy, the sample size has been calculated for both the outcome and some of the predictor variables. Finally, the maximum sample size of 247 was used.
Sampling Technique
Of 15 districts and two administrative towns found in the GGZ, six districts and one town were selected from the total area using a simple random sampling technique (lottery method). The sampling frame was developed based on the total number of female teachers working in each of the selected districts and town, which were obtained from the GGZ educational bureau, and their numbers were rechecked from each of selected districts and town educational bureau first. Then, proportional size allocation was carried out for each of the selected districts and town based on the available numbers of female teachers.
Finally, a sampling frame was prepared from the list of selected districts and town educational bureaus. A code was given for each of the listed female teachers working in the GGZ and serial numbers were given for all. Then, a study participant was selected using the lottery method in each of the selected districts and town based on the available numbers of female teachers (see Figure 1).
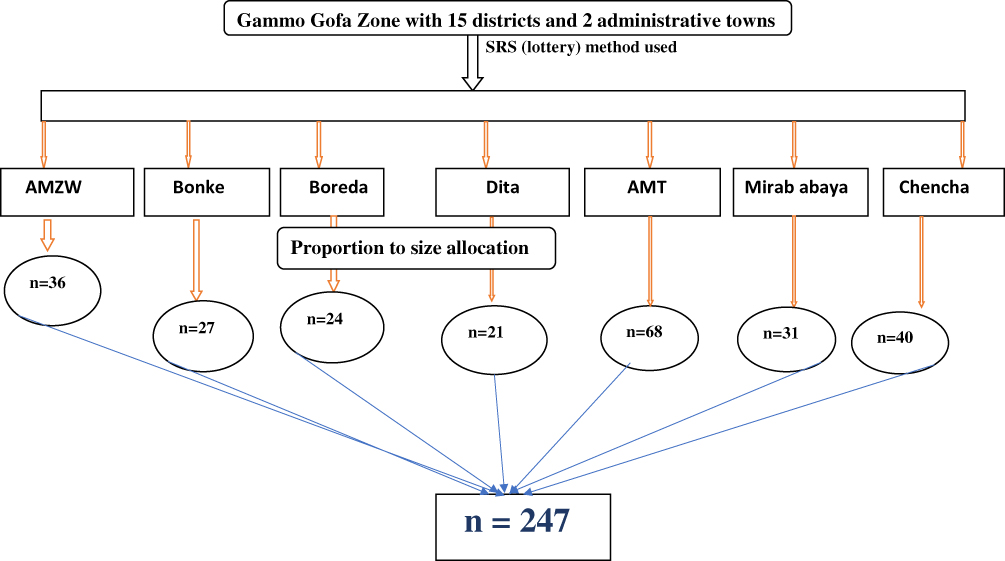 |
Figure 1 Schematic presentation of the sampling technique of female secondary school teachers who participated in the study, Gammo Gofa Zone, South Ethiopia. |
Data Collection Procedure
A total of seven HEWs and one supervisor for all selected districts and town were used as facilitators of data collection after being given two days of training. A self-administered questionnaire was used for data collection, including the socio-demographic characteristics, knowledge toward BSE and breast cancer; and the perceptions of the female teachers toward BSEs using health belief model constructs.
Measurements
A total of 34 questions was used to assess the perceptions of female teachers towards BSE practice. A five-point Likert scale response with choices ranged from “strongly disagree (scores 1 point)” to “strongly agree (scores 5 points)” was used. Based on the scales, 4, 7, 6, 7, 6, and 4 questions were asked to assess susceptibility to breast cancer, seriousness of breast cancer, benefits of BSE, barriers to BSE, self-efficacy/confidence to BSE, and motivation to BSE, respectively.
For all constructs of the health belief model, higher scores (half and above) were indicated as having a high perception toward performing BSE except for barriers to BSE, in which a higher score indicated a high barrier to performing BSE.17
Knowledge toward BSE and breast cancer was measured by total answers to 14 and 8 knowledge questions, respectively. Those who answered less than half for both BSE and breast cancer were categorized as less knowledgeable and those who answered half and above were considered as knowledgeable.17
Practices of BSE were determined from the binary outcome variable (yes, no) by using the questions “have you ever examined your breast by your hands in the last one year?” Those who responded “yes” were further asked the appropriate time to perform BSE, the right ways of performing BSE, and how frequently they did BSE. Those who responded correctly to the above questions were categorized as practiced BSE but not necessarily regularly.
Data Analysis Procedures
Data were cleaned, coded and, entered into the Epi-dataTM version 4.1 then exported to SPSS version 21 for analysis. Frequency tables, graphs, and descriptive summaries were used to describe the study variables.
Bivariable logistic regression was carried out initially to identify the candidate variables for multivariable logistic regression. All variables with a p value of <0.25 were selected as candidates. The odds ratio with 95% confidence interval was calculated and variables with p <0.05 were declared statistically significant.
The Hosmer Lame Shaw goodness-of-fit test for model fitting was conducted and the results for model prediction and overall p-value were 81.2% and 0.978, respectively. In addition to this, multicollinearity was tested and we took 0.2 as the minimum tolerance level.
Data Quality Management
First, the questionnaire was prepared in English and translated into Amharic, then retranslated back to English to check for any inconsistency. Second, two days' training was given for facilitators and the supervisor on the objective of the study, method of data collection, and content of the questionnaire to avoid any ambiguity at the time of data collection. The completeness of data was checked by facilitators during the data collection time and after data collection by the supervisor and principal investigator.
Finally, a pre-test was done on 5% of female teachers in Konso town (one of the districts of the Segen area people zone). The reliability test for each of HBM subscale, knowledge questions to BSE and breast cancer were calculated using Cronbach’s alpha. Based on the result obtained, the necessary modifications were made. The results were 0.8 and 0.79 to knowledge questions about BSE and breast cancer, respectively, whereas 0.7–0.83 for HBM constructs gave an overall alpha coefficient of 0.78, which indicates the adequate reliability of the scale.22
Results
Socio-Demographic Characteristics of the Study Participants
Two hundred thirty-nine participants responded in this study with a response rate of 96.6%. The mean (± SD) age of participants was 39.8 (± 10.4) years. Regarding marital status, more than half (59.8%) of the participants were married. The majority (55.6%) of the participants were Gammo in ethnicity, 52.3% were Orthodox religion followers followed by Protestant religion followers (see Table 1).
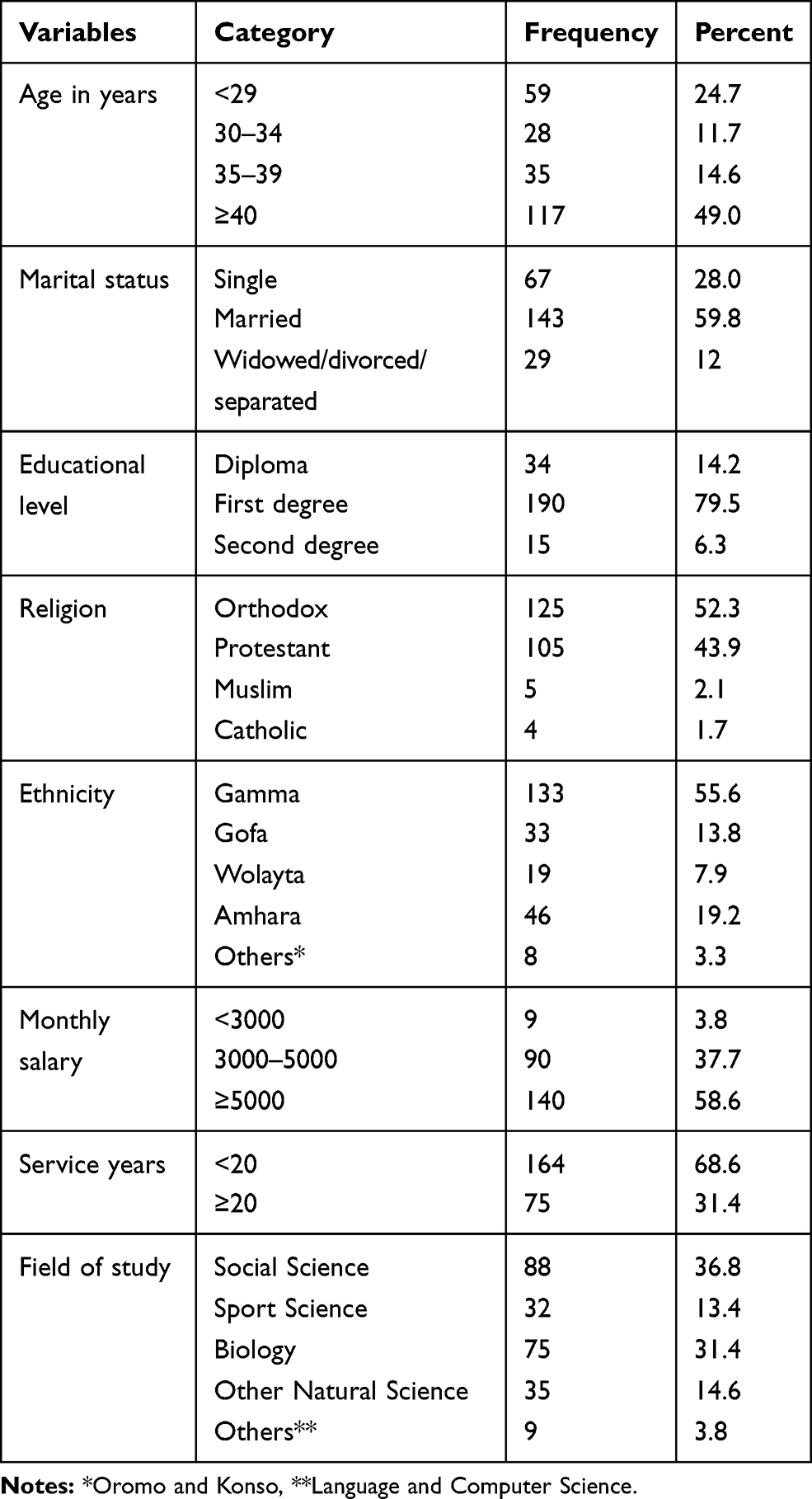 |
Table 1 Socio-Demographic Characteristics of Female Secondary School Teachers Who Were Participating in the Study, Gammo Gofa Zone, South Ethiopia (N=239) |
Knowledge, Perceptions, and Source of Information Toward Breast Self-Examination Practice
More than half (61.5%) of the study participants scored below half to knowledge questions about BSE and were considered as less knowledgeable. Regarding the perception, even though more than three-quarters of the respondents had high motivation (78.7%) to BSE practice, more than half of the participants had both low perceived confidence (56.5%) and high perceived barrier to BSE (68.2%) (see Table 2).
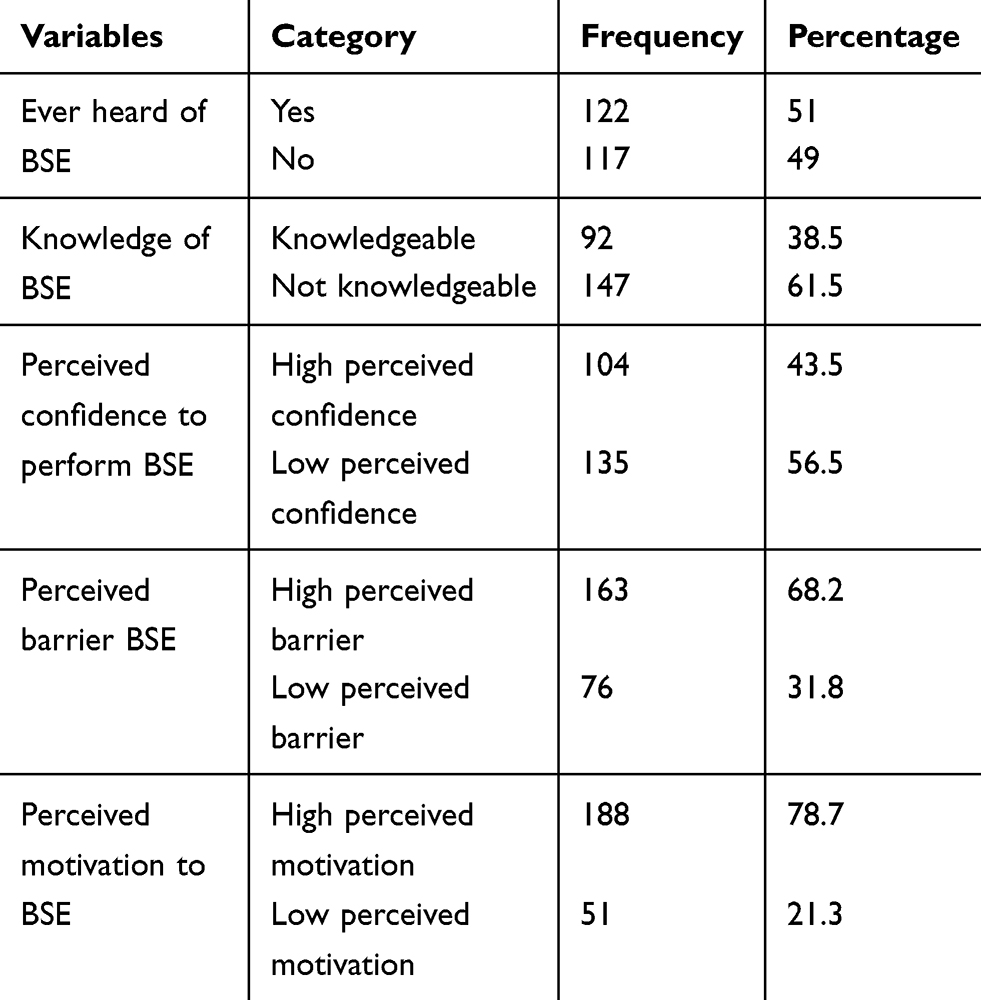 |
Table 2 Knowledge and Perception Level Toward Breast Self-Examination Practice Among Female Teachers in Gammo Gofa Zone, 2018 |
Regarding the source of information on BSE, the major source was television 80 (33.5%), radio 59 (24.7%), and health professionals 52 (21.8%), among others.
Practice of Breast Self- Examination
Of the total participants, only 82 (34.3%) had ever practiced BSE. Among these, less than a quarter (13.4%) practiced BSE on a regular (monthly) basis.
Of the total participants, the majority (65.7%) did not practice BSE and the major reasons for not practicing BSE were: not knowing how to perform BSE (49.8%), had no breast-related problems (28.5%), and considered that BSE was not beneficial (8.4%), among others.
Of the total participants, those who ever practiced BSE in the last 12 months correctly answered how BSE is performed as palpating by using the palms and three middle fingers and the appropriate time to perform BSE, which is after some days of cessation of menses (see Table 3).
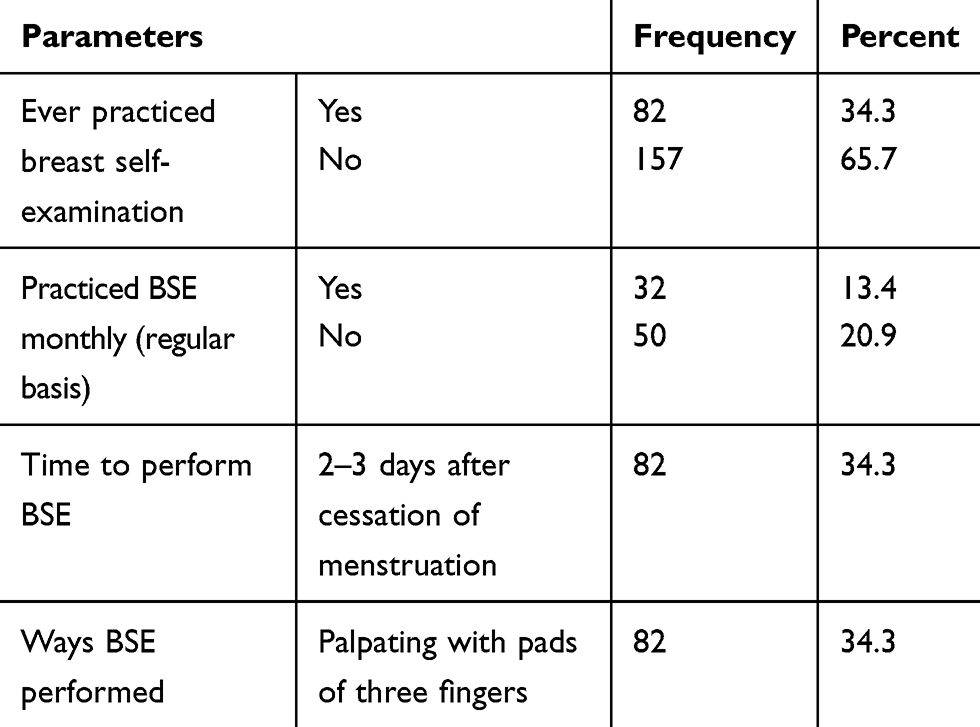 |
Table 3 Practice of Breast Self-Examination Among Female Secondary School Teachers in Gamma Gofa Zone, 2018 |
For the frequency of BSE practice which was conducted within one year by the respondents, the majority (60, 25.1%) practiced below the standard (which is 10–12) and the reasons answered by the majority for not practicing BSE regularly was forgetfulness (21.8%), among others (see Figure 2).
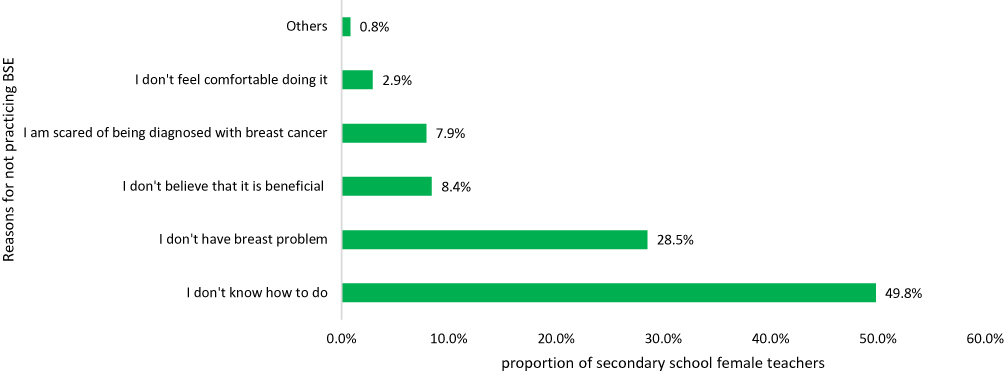 |
Figure 2 Reasons for not practicing BSE by study participants of secondary school female teachers in Gammo Gofa Zone, 2018. |
Factors Associated with the Breast Self-Examination Practice
For bivariable logistic regression analysis, a total of 18 variables was used. Among these, 16 of the variables were all candidate variables for multivariable analysis.
In multivariable logistic regression analysis, of 16 candidate variables, only six (ever heard about BSE, having knowledge of BSE practice, having less perceived barrier to BSE, having high perceived confidence and motivation to BSE and being married) were significant predictors of BSE practice. Participants who ever heard about BSE were twice as likely to practice BSE [AOR=2.26, 95% CI (1.07, 4.77)] than their counterparts. Participants having knowledge on BSE practice were three times more likely to practice BSE [AOR=2.84, 95% C. I (1.41, 5.72)] compared with those less knowledgeable. Participants having less perceived barrier to BSE were three times more likely to practice BSE [AOR=2.62, 95% C. I (1.26, 5.46)] than their counterparts. Those having high perceived confidence and motivation were four and three times more likely to practice BSE [AOR=3.63, 95% C. I (1.79, 7.39)] and [AOR=3.29, 95% CI (1.15, 9.45)] than their counterparts, respectively, and those who were married were four times more likely [AOR=4.098, 95% C. I (1.644, 10.219)] to practice than their counterparts (see Table 4).
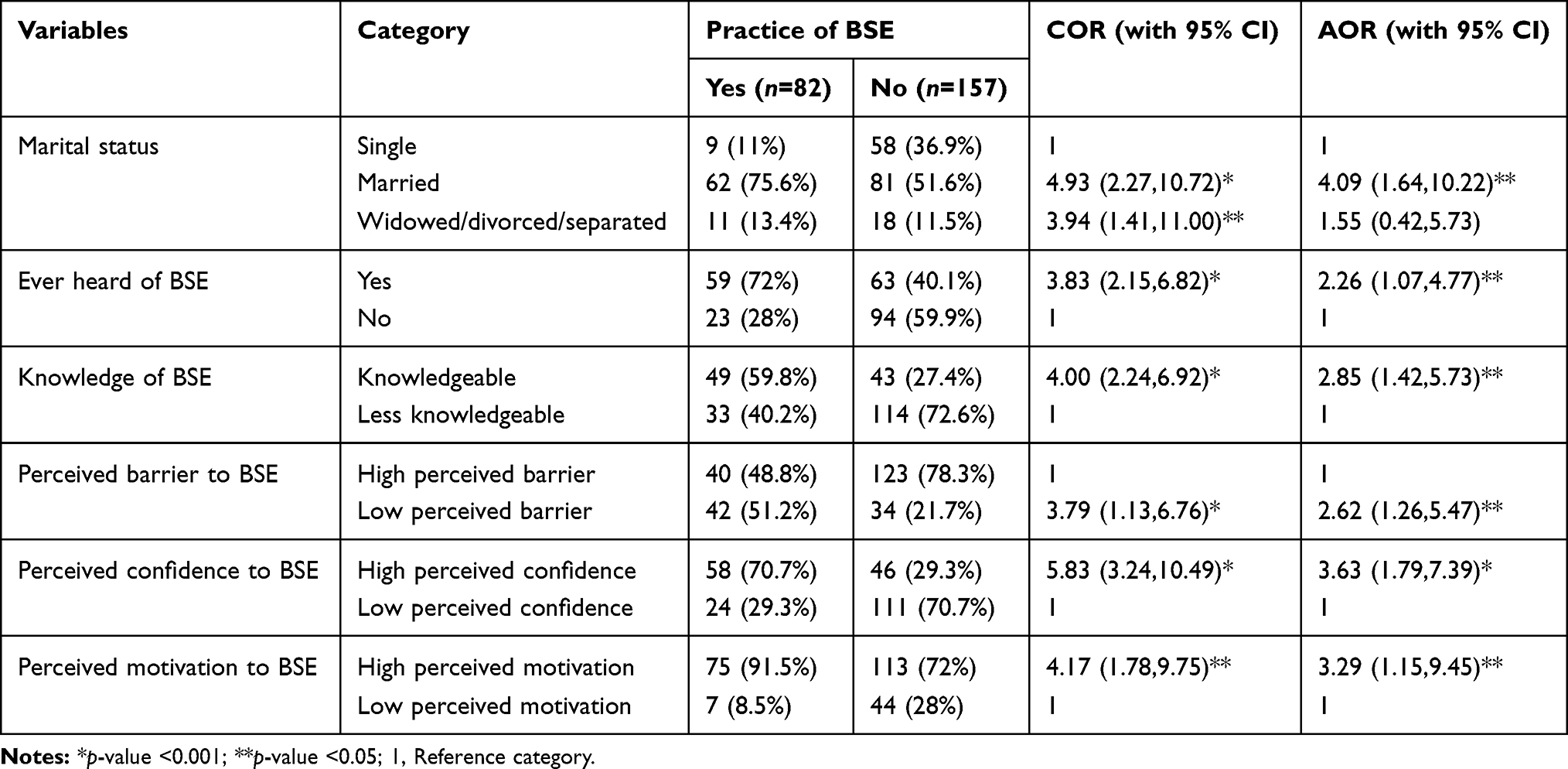 |
Table 4 Multivariable Logistic Regression Analysis Result of the Study Conducted Among Female Secondary School Teachers in GGZ, South Ethiopia, 2018 |
Discussion
It is fundamental that women should know how their breasts normally look and feel. Having good knowledge and performing regular breast self-examination is the best way to know this. Breast self-examination is one of the screening methods that helps one to become aware early of changes that may occur in the breast. Any changes from the normal look and feel can be a sign of diseases related to the breast. Thus, BSE was used to determine this breast condition early.
In this study, only 34.3% of the respondents had ever practiced breast self-examination. This finding is similar to a cross-sectional study conducted among Egyptian women in 2013 and Nigerian female teachers in 2014, which revealed that 35.3% of Egyptian women16 and 36.2% of the Nigerian female teachers18 had ever practiced breast self-examination. This similarity might be explained by the study participants in this study possibly obtain ing information on BSE from the available HEWs, health professionals and others in the community. The other possible reason might be due to similarity in some socio-demographic characteristics, such as educational level and marital status, in that the majority were married and they might have obtained information about BSE in health facilities during their ANC follow-up, family planning service and other MCH services from the available HEWs and other health professionals.
On the contrary, it is much lower than the findings from other cross-sectional studies conducted in Selangor, Malaysia in 2011, Saudi Arabia in 2015, Nigeria in 2014, Malaysia in 2012, and western Ethiopia in 2015, which revealed that 54% of Malaysian female teachers, 41.6% of Saudi women, 79.3% of Nigerian female teachers, 55% of Malaysian women, 77% of health in western Ethiopia ever practiced BSE.2,8,14,16,18,19 The possible explanation for these great differences in ever practiced breast self-examination might be due to the difference in knowledge of BSE, access to information on the screening methods, the difference in time interval between the studies, socio-economic and socio-demographic characteristics among the study population, differences in the study participants and their compositions.
The finding of this study is somehow higher than the study conducted in Mosul city among school teachers in 2013 and Jordananian women in 2001, which revealed that 26% of the participants had ever practiced BSE.15,20 This difference might be because this study was based on self-report (with no observation of performance or proficiency), so the prevalence could be an overestimation or more attention by the study participants given to BSE for the lack of accessibility of advanced screening methods in this study area though heard about BSE was lower among this study participants than Mosul and Jordan women.
For those who had ever practiced BSE in this study, less than one-quarter of the participants (13.4%) had practiced BSE on a regular (monthly) basis. This finding is similar with other cross-sectional studies among female teachers in Kafa Zone, south-west of Ethiopia in 2015 and health extension workers in west Gojam in 2013, which revealed that (12.1%) of female teachers and 14. 4% of HEWs had practiced BSE on a monthly basis.12,13 This similarity might be due to the study being conducted in the same geographical area (the same country) that made certain characteristics of this population similar. On the contrary, it is also much lower than the cross-sectional studies conducted in Selangor, Malaysia among female teachers (19%) in 2011, Saudi women (21%) in 2015, Malaysian women (28.5%) in 2012, Nigerian female teachers (19%) in 2014, and female health professionals in western Ethiopia (33.7%) in 2017.2,8,14,16,18,19 The difference observed in this study might be for the same reasons as mentioned before in ever practiced BSE.
In the current study, participants ever having heard about BSE were twice as likely to practice BSE than their counterparts. This finding is highly comparable with the cross -sectional study conducted among Thai women in 2009, which revealed that those who had ever heard of breast self-examination were more likely to practice than their counterparts.15 On the contrary, the study conducted in Selangor, Malaysia among female teachers in 2011 revealed no statistical association.14 This difference might be due to the fact that those who had ever heard about BSE in this study were given more attentions for BSE. Other possible reasons might be due to the difference in socio-economic and socio-demographic and the difference in the study period.
In many findings, the practice of BSE was determined by the knowledge of women or having information on diagnostic methods of breast cancer.11,14,21 Similarly, in the current study, participants who were knowledgeable on BSE were more likely to perform BSE. In this study, only 38.5% of the study participants were knowledgeable about BSE. This result was lower than cross -sectional studies conducted among female teachers in Nigeria (46%) in 2012, in Mosul city among school teachers (84%) in 2013, among health professionals in western Ethiopia (58%) in 2017 and Addis Ababa (77.6%) in 2012.2,11,20 The reasons for this difference might be difference in access to information, because in this study area, only half of the study participants had ever heard about BSE than the comparison groups, which might have an effect on the knowledge of BSE in this study's participants. However, it is higher than the study conducted in Nigeria among women following antenatal care (12.7%) in 2009.17 This might be due to teachers possibly having more awareness than the general population and being more open to adopting health behaviors than the others. The other possible reason might be because it was self-reported, so the study might be overestimated.
Regarding the perceptions, the current study revealed that those who had high perceived confidence were nearly four times more likely to practice BSE than their counterparts. The finding of this study is also supported by the study conducted among Iranian women on breast self-examination and breast cancer screening in 2012, in Selangor, Malaysia in 2011 among school teachers, and with Saudi Arabian women in 2015,8,15,20–22 which revealed that those who had high confidence in performing BSE were more likely to practice than their counterparts.
Similarly, those who had high perceived motivation and low perceived barriers were three times more likely to practice BSE than their counterparts. This finding is also supported by other cross-sectional studies conducted among Iranian women in 2014 on breast cancer screening methods, Saudi women in 2015, and Turkish women in 2009,8,20,22 which revealed that those with high perceived motivation and low perceived barriers were more likely to practice BSE than their counterparts. Perceived susceptibility and severity to breast cancer and perceived benefits to breast self-examination were not significantly associated with this study. Although a significant proportion of women perceived breast cancer to be serious, most of them did not perceive themselves as being susceptible. This could be due to a lack of education on breast cancer and BSE practice in the study area.
Regarding perceived severity, a previous study in Kefa, south-west Ethiopia among school teachers in 2015 suggested that BSE practice will increase with increased perceived seriousness of breast cancer and the relationship of perceived seriousness/severity of breast cancer with BSE practices.12 While similar to this study, other studies in 2015 among Saudi women, in 2011 among Malaysian female teachers, in 2001 among Jordanian women, in 2009 among Thai women, Turkish academicians and among Iranian women8,15,20–23 found that there is no association between perceived seriousness and BSE behaviors. Therefore, this indicates that teachers might have misconceptions about breast cancer and early detection methods.
In this study, the majority of women had high beliefs about the benefits of BSE, but these were not significant. Studies conducted in south-west Ethiopia among female teachers in 2015 and Jordanian women in 2001 reported a significant positive relationship between perceived benefits of screening and BSE practice,12,23 whereas similar to this study, other studies in Saudi women in 2015, Malaysian female teachers in 2011, Thaiwomen and Turkish female academics in 2009 found no significant effect.8,15,20,21 This indicates that there are no well-designed awareness programs that underline the benefits of preventive care and early screening.
Likewise, in the findings of cross-sectional studies among Iranian women in 2010 and health workers in a governmental hospital in Ethiopia in 2012,11,24 women’s marital status in this study was also found to be the predictor of BSE which revealed that those who married were four times more likely to practice BSE than their counterparts. However, this result was in contradiction with the finding of some other studies conducted among school teachers in Malaysia and Kefa Zone in south-west Ethiopia.12,14 This might be because the participants in this study might have more information about BSE that might be obtained from the available HEWs and health professionals during their ANC follow-up, family planning service and at the time of other MCH services. However; it seems that still more investigations are required in this area by using different communities with different socio-demographic characteristics.
Use of the revised champions of health belief model was the main strength of the study. However, the behavioral study outcomes are based on self-reported information, which can be affected by social desirability bias.
Conclusion
Less than a third of the participants ever practiced BSE, with only about 13% of them practicing regularly. The main reasons mentioned for not practicing BSE were not knowing how to perform BSE and forgetfulness. Being knowledgeable in BSE practice, ever heard about BSE and married and having less perceived barrier, high perceived confidence and motivation to BSE were significant predictors of BSE practice. Therefore, integrated work on behavioral change communication and interferences focusing on improving the knowledge of BSE, skills on how to perform BSE and identified domains of health belief model through training, continuous health education at school and through media to disseminate information regarding BSE may be the most effective strategies that should be considered by Zonal health and educational offices including other non-governmental organizations working on health and health-related issues. This is very important to obtain larger benefits that the teachers will contribute to the community at large and the country as well.
Abbreviations
BSE, breast self-examination; HBM, health belief model; HEWs, health extension workers; IRB, Institutional Review Board; MCH, Maternal and Child Health.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Board (IRB) of the Jimma University Institute of Health. Further information and documentation to support this will be available on reasonable request. After receiving letters of permission to carry out the study from each administrative body, verbal informed consent, which was approved by the IRB, was taken from each study subject prior to interview after the purpose of the study was explained. The respondents were informed that the data collectors were trained only to collect information, but apart from this particular research, the data were not being passed to anybody. The privacy of the respondents was maintained and confidentiality of the information was respected (personal identification and ideas were not being used in any way which might threaten the respondent). There is no payment/incentive in participating in this interview.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
MM made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. AN was involved in the design, analysis, and interpretation of data. AT was involved in drafting the manuscript or revising it critically for important intellectual content. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Tao Z, Shi A, Lu C, et al. Breast cancer: epidemiology and etiology. Cell Biochem Biophys. 2015;72:333. doi:10.1007/s12013-014-0459-6.
2. Legesse EN, Dechassa WH, Sufa AM. Assessment of breast self-examination practice and associated factors among female health professionals in Western Ethiopia: a cross sectional study. Int J Med Med Sci. 2017;9(12):148–157. doi:10.5897/IJMMS2016.1269
3. Atanga M, Atashili J, Asoh E, et al. Breast self-examination and breast cancer awareness in women in developing countries: a survey of women in Buea, Cameroon. BMC Res Notes. 2012;5(1):1.
4. Khatib OMN, Modjtabai A. Guidelines for the Early Detection and Screening of Breast Cancer. EMRO Technical Publications Series, 30. WHO World Health Organization; 2006:1–57.
5. Memirie ST, Habtemariam MK, Asefa M, Al E. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol. 2018;4:1–11. doi:10.1200/JGO.17.00175
6. Birhane K, Alemayehu M, Anawte B, et al. Practices of breast self-examination and associated factors among female Debre Berhan University Students. Int J Breast Cancer. 2017;2017:1–6. doi:10.1155/2017/8026297
7. Shrivastava SR, Shrivastava PS, Ramasamy J. Self breast examination: a tool for early diagnosis of breast cancer. Am J Public Health Res. 2013;1(6):135–139. doi:10.12691/ajphr-1-6-2
8. Abolfotouh MA, Banimustafa AA, Mahfouz AA, Al-assiri MH, Al-juhani AF, Alaskar AS. Using the health belief model to predict breast self examination among Saudi women using the health belief model to predict breast self examination among Saudi women. BMC Public Health. 2015;15. doi:10.1186/s12889-015-2510-y
9. Kassa RT, Wakjira HT, Gebremariam MB, Tullu SA, Shehissa NK. Breast cancer knowledge and breast self-examination practice among female students in Rift Valley University, Adama campus, Adama. J Women`s Heal Care. 2017;6(5).
10. Dibisa TM, Gelano TF, Negesa L, Hawareya TG, Abate D. Breast cancer screening practice and its associated factors among women in Kersa District, Eastern Ethiopia. Pan Afr Med J. 2019;33:144. doi:10.11604/pamj.2019.33.144.18062
11. Dellie ST, Neguse TM. Knowledge about breast cancer risk-factors, breast screening method and practice of breast screening among female healthcare professionals working in governmental hospitals. J Pharm Biol Sci. 2012;2(1):5–12.
12. Birhane N, Mamo A, Girma E, et al. Predictors of breast self - examination among female teachers in Ethiopia using health belief model. Arch Public Health. 2015;73(1):39. doi:10.1186/s13690-015-0087-7
13. Azage M, Abebe G, Mekonnen A. Assessment of factors associated with breast self-examination among health extension workers in West Gojjam Zone, Northwest Ethiopia. Int J Breast Cancer. 2013;2013:1–6. doi:10.1155/2013/814395
14. Parsa P, Kandiah M, Parsa N. Factors associated with breast self-examination among Malaysian women teachers. East Mediterr Health J. 2011;17(6):509–516. doi:10.26719/2011.17.6.509
15. Satitvipawee P, Promthet SS, Pitiphat W, Kalampakorn S, Parkin DM. Factors associated with breast self-examination among Thai women living in rural areas in Northeastern Thailand. J Med Assoc Thai. 2009;92(Suppl 7):S29–S35.
16. Sharaa HM. Beliefs and reported practices related to breast self examination among sample of Egyptian women. Acad J Cancer Res. 2013;6(2):99–110.
17. Onwere S, Okoro O, Chigbu B, et al. Breast self-examination as a method of early detection of breast cancer: knowledge and practice among antenatal. Pak J Med Sci. 2009;25(1):27–30.
18. Alice TE, Phiomena O. Breast self examination among secondary school teachers in South-South, Nigeria: a survey of perception and practice. Journal of Public Health and Epidemiology. 2014;6(169):169–173.
19. Al-Dubai SAR, Ganasegeran K, Alabsi AM, et al. Exploration of barriers to breast-self examination among urban women in Shah Alam, Malaysia: a cross sectional study. Asian Pac J Cancer Prev. 2012;13(4):1627–1632. doi:10.7314/APJCP.2012.13.4.1627
20. Hajian-Tilaki K, Auladi S. Health belief model and practice of breast self-examination and breast cancer screening in Iranian women. Breast Cancer. 2014;21(4):429–434. doi:10.1007/s12282-012-0409-3
21. Parsa P, Kandiah M, Zulkefli NAM, Rahman HA. Knowledge and behavior regarding breast cancer screening among female teachers in Selangor, Malaysia. Asian Pac J Cancer Prev. 2008;9(2):221–228.
22. Ceber E, Yücel U, Mermer G, Özentür KG. Health beliefs and breast self-examination in a sample of Turkish women academicians in a university. Asian Pac J Cancer Prev. 2009;10:213–218.
23. Petro-nustus W, Sc D, Mikhail BI. Factors associated with breast self-examination among Jordanian women. Public Health Nurs. 2001;19(4):263–271.
24. Noroozi A, Jomand T, Tahmasebi R. Determinants of breast self-examination performance among Iranian women: an application of the health belief model. Journal of Cancer Education. 2011; 26(2):365–74.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.