Back to Journals » Clinical Interventions in Aging » Volume 19
Blood Pressure Control for Patients with Middle Cerebral Artery Severe Stenosis or Occlusion
Authors Li Z, Duan GX, Zhang JH, Xu Y, Luo Y
Received 8 May 2024
Accepted for publication 13 November 2024
Published 18 November 2024 Volume 2024:19 Pages 1897—1905
DOI https://doi.org/10.2147/CIA.S477281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Zheng Li,1,2,* Guang-Xin Duan,3,* Jia-Hui Zhang,3 Yun Xu,3 Yun Luo3
1Department of Rehabilitation, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Rehabilitation, Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, People’s Republic of China; 3Department of Neurology, Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Xu; Yun Luo, Department of Neurology, Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, People’s Republic of China, Email [email protected]; [email protected]
Background: Chronic hypertension is an independent risk factor for ischemic stroke and worsens prognosis. However, the level of blood pressure control in hypertensive patients with severe intracranial stenosis is controversial.
Purpose: To investigate the effect of different levels of blood pressure on cerebral perfusion in patients with middle cerebral artery severe stenosis or occlusion.
Materials and methods: A total of 105 patients with isolated steno-occlusive middle cerebral artery (MCA) diagnosed by digital subtraction angiography (DSA) were enrolled, and PWI was compulsory. Relative risk factors were obtained by intergroup analysis in both hypertensive and non-hypertensive groups, and multivariable logistic regression was performed to determine whether hypertension was independently associated with PWI values. Next, the effects of different levels of blood pressure levels on cerebral perfusion as a whole and subgroup were further compared.
Results: The hypertension (HT) group (Am 1.04± 0.05, Lm 1.07± 0.06, Pm 1.07± 0.05) demonstrated lower cerebral perfusion pressure at a larger rMTT (p=0.0001, 0.004, 0.006) than the nonhypertension (NHT) group (Am 1.01± 0.21, Lm 1.04± 0.04, Pm 1.04± 0.04). After adjustment for age, diabetes, and fibrinogen (FIB), HT was independently associated with the rMTT of Am, Lm, and Pm (P=0.015, 0.001, 0.022). Significant differences were observed with HT+SBP< 140 (p=0.035, 0.048, 0.049) and HT+DBP< 80 (p=0.034, 0.045, 0.055) in rMTT compared with NHT.
Conclusion: Chronic hypertension might damage cerebral perfusion. Strictly control of blood pressure (< 140/80mmHg) in hypertensive patients with intracranial artery stenosis will further reduce ipsilateral cerebral perfusion.
Keywords: blood pressure control, isolated severe steno-occlusive, PWI, cerebral perfusion
Corrigendum for this paper has been published.
Introduction
Hypertension is an important risk factor for atherosclerosis and ischemic brain disease. Strict control of blood pressure has a preventive effect on ischemic brain disease.1 Multiple relevant research results domestically and internationally recommend that for stable stroke patients, lowering blood pressure to below 140/90mmHg can effectively reduce the recurrence rate of stroke.2–4 But should hypertensive patients with cerebral artery stenosis control their blood pressure strictly? How to reduce blood pressure? What is the target for lowering blood pressure? It has always been a focus of clinical attention and controversy. Rothwell’s study found that in patients with bilateral internal carotid artery stenosis, lower blood pressure levels are associated with an increased risk of stroke.4 But for patients with unilateral internal carotid artery stenosis, Turan’s study found that elevated blood pressure is positively correlated with increased risk of stroke.5 A multicentre, open-label, randomised controlled trial fund that intensive blood pressure lowering after endovascular therapy in acute ischaemic stroke is safe.6 Another study showed that blood pressure lowering may increase stroke risk in patients with symptomatic major cerebral artery disease and impaired perfusion.7 Jong Moon Park’s research found that strict blood pressure control may not be safe in subacute ischemic stroke caused by intracranial atherosclerosis.8 Hwa Kyoung Shin et al also found that mild hypertension can improve blood flow and oxygen metabolism in transient focal cerebral ischemia.9 While there is no high-quality evidence to suggest that maintaining slightly higher systolic blood pressure (140–159mmHg) can prevent stroke recurrence currently. In turn, hypertension will further lead to systemic atherosclerosis, leading to progressive stenosis of blood vessels. Hong Qi Li found that there was a dose-response relationship between systolic blood pressure, diastolic blood pressure and pulse pressure and the risk of intracranial atherosclerosis. Higher systolic and pulse pressures may lead to a higher burden of intracranial atherosclerosis (ICAS).10 At present, research on blood pressure management in patients with intracranial artery stenosis is mainly conducted in patients after acute ischemic events and endovascular treatment. There is no research on hypertension management in populations with severe stenosis or occlusion of the middle cerebral artery and no cerebrovascular events. This study conducted a retrospective study on the blood pressure and cerebral perfusion of this population, which has clinical significance in reducing the occurrence of acute cerebral ischemia events through appropriate blood pressure management with clear risk factors for cerebral ischemia.
Perfusion is emerging as a key variable in the outcome of acute ischemic stroke.11 Collateral status has been shown to be the strongest predictor for prognosis.12 Cerebral autoregulation refers to the ability of cerebral blood vessels to maintain stable cerebral blood flow through the adjustment of their own caliber under different peripheral blood pressure levels.13,14 This is the self-compensation ability possessed by the brain. Hypertension impairs cerebral microcirculation by causing cerebral microvascular disease, and ultimately damaging the brain tissue. Under the long-term effects of hypertension, this self-compensation ability will be impaired.15 Therefore, maintaining stable cerebral perfusion is very important for patients with hypertension. Too low will lead to cerebral infarction, and too high will lead to cerebral hemorrhage.16
The aim of our study was to investigate the association of hypertension, intracranial perfusion and collateral flow compensation in a representative population of isolated severe steno-occlusive MCA patients. The findings of the research will be utilized to further guide the management of blood pressure levels in specific populations for the prevention of acute cerebrovascular events.
Methods
Study Subjects
Clinical and imaging data were collected from hospitalized patients between May 2018 and December 2019, which was approved by the institutional committee of the Affiliated Drum Tower Hospital of Nanjing University Medical School (No. 2016–169-01). Patients or their relatives gave oral informed consent for follow-up. Inclusion criteria: (1) severe stenosis or occlusion in the MCA was vital diagnosed by DSA (>70%); (2) without acute ischemic stroke (AIS) or with AIS >1 week when DSA and High-resolution Magnetic Resonance Imaging (HR-MRI) was performed, while mechanical thrombectomy of AIS was not included in this study, regardless of whether it was induced by embolism or intracranial stenosis; (3) HR-MRI and Perfusion Weighted Imaging (PWI) was compulsory; and (4) complete clinical information and relatively complete blood detection. Additionally, exclusion criteria were defined as follows: (1) moyamoya disease diagnosed by DSA; (2) other significant stenosis (>70%) in the cervical or intracranial arteries diagnosed by DSA except for the target vessel; (3) evidence of cardioembolism in the area of the target vessel; and (4) vasculitis or arterial dissection suspected by clinical information, laboratory and imaging results. A flow chart of the study was offered is shown in Figure 1.
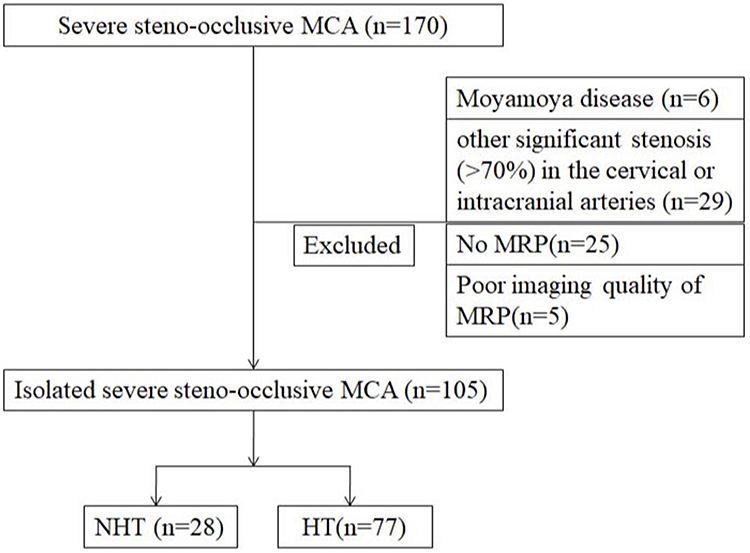 |
Figure 1 Patients inclusion flow diagram and study groups. Abbreviations: MCA, middle cerebral artery; MRP, magnetic resonance perfusion; NHT, no hypertension; HT, hypertension. |
Image Processing and Interpretation
All MRI measurements were performed on a 3.0T Magnetom Avanto Scanner (Philips, Netherlands). PWI studies were performed using a previously described protocol, with parametric maps of time to peak (TTP), mean transit time (MTT), cerebral blood flow (CBF) and cerebral blood volume (CBV). The region of interest (ROI) of this study was selected according to the ASPECT study, whose territory of the middle cerebral artery was allotted 10 points, represented as C (caudate), L (lentiform), IC (internal capsule), I (insular ribbon), M1 (anterior MCA cortex), M2 (MCA cortex lateral to insular ribbon), M3 (posterior MCA cortex) and M4, M5, M6 (anterior, lateral, and posterior MCA territories immediately superior to M1, M2, and M3, rostral to basal ganglia). According to the territory selection of M4, M5, and M6, relative territories of lentiform immediately superior to L were named L1. Data were generated from these eight ROIs including M1, M2, M3, M4, M5, M6, L and L1, which represent the perfusion of four territories named Am (anterior cortex of MCA), Lm (lateral cortex of MCA), Pm (posterior cortex of MCA) and Bm (basal ganglia of MCA). The value was calculated as follows: Am=(M1+M4)/2, Lm=(M2+M5)/2, Pm=(M3+M6)/2, Bm=(L+L1)/2.
Definition of Hypertension
Hypertension was defined as a history of hypertension or a new diagnosis according to the China hypertension standard (≥140/90 mmHg).17 New hypertension was defined as systolic blood pressure measured at least 3 times on different days after admission ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg.
Definition of Mean Systolic Blood Pressure (MSBP) and Mean Diastolic Blood Pressure (MDBP)
The blood pressure values were collected after admission at these time-points (9:00–15:00-21:00) and then taken as the average. If one of the first two points is missing, we take the blood pressure of the previous day or next day as a substitute.
Definition of rMTT
rMTT was defined as the ipsilateral/contralateral MTT.18 It showed poor collateral circulation in ipsilateral intracranial artery stenosis when rMTT was more than 1.
Statistical Analysis
Mean imputation was used for handling incomplete variables. Statistical analysis was performed with SPSS 17.0 software. The results are expressed as constituent ratios for categorical variables, and were analyzed with the χ2 test. Continuous variables were described as the mean ± SD or median (IQR); and analysed with t test and ANOVA or Mann–Whitney U-test. Logistic regression was used to determine the relative risk level of hypertension and MRP values, which was expressed as an OR and a corresponding 95% CI. The level of significance for statistical purposes was stated at p<0.05.
Results
Baseline Characteristics
Of 170 patients with severe steno-occlusive MCA in our registry, 105 patients were finally included in the trial according to the exclusion criteria (6 with Moyamoya disease, 29 combined with cervical or intracranial artery stenosis, 25 with no MRP, 5 with poor imaging quality), which was divided into a no hypertension group (NHT, n=28) and a hypertension group (HT, n=77) (Figure 1). The two groups differed significantly in age (p=0.014), diabetes (χ2=4.724, p=0.030) and FIB (p=0.012). There were no other risk factors for vascular stenosis that differed significantly between them. These results are summarized in Table 1.
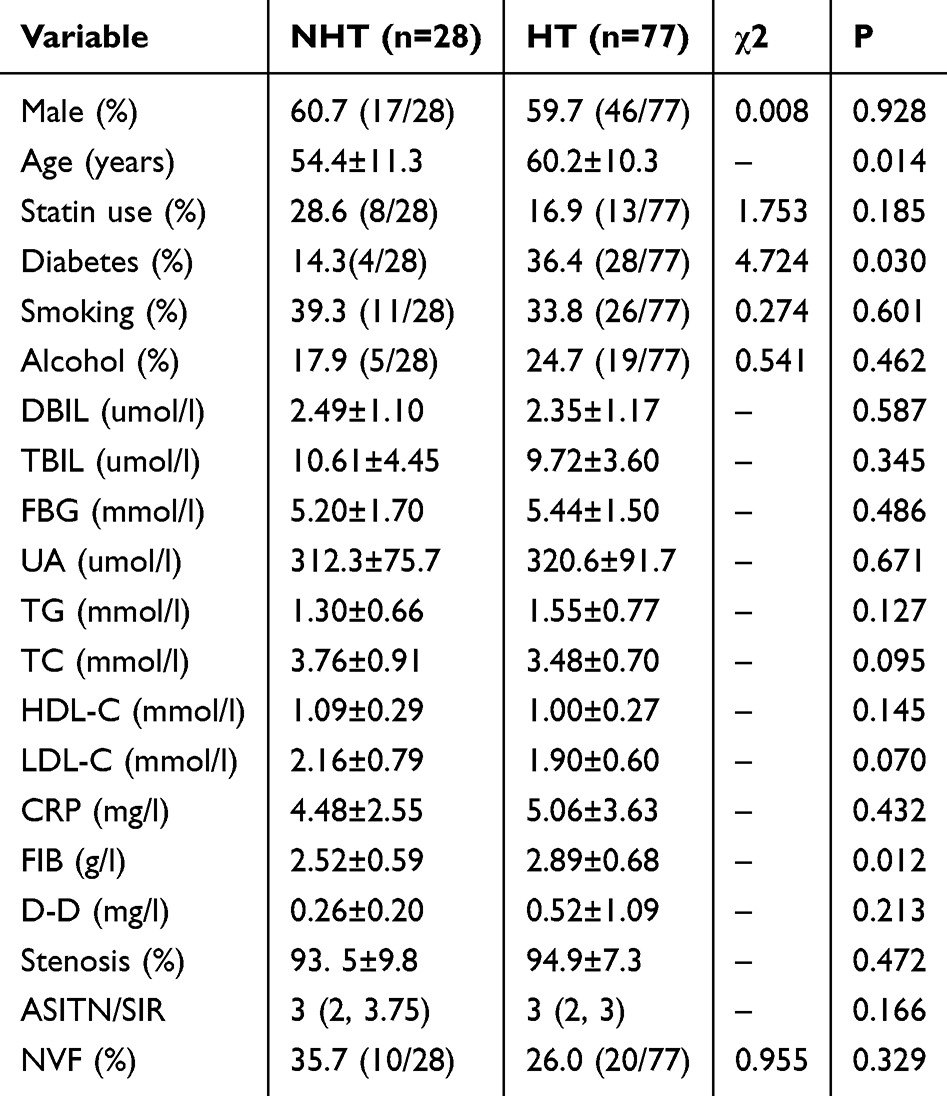 |
Table 1 Comparison of Risk Factors Between the Groups of NHT and HT |
HT Was Independently Associated with rMTT
The MTT of the HT group was lower than that of the NHT group in both the ipsilateral and contralateral sides, but the difference was not significant. Significant differences were observed between the two groups in the rMTT of Am, Lm, and Pm (Table 2). In multivariate logistic regression, we tested the association of HT and rMTT after adjustment for age, diabetes, and FIB. HT was independently associated with the rMTT of Am, Lm, Pm (P=0.015, 0.001, 0.022) (Table 3).
 |
Table 2 Comparison of MRP Values Between Groups of NHT and HT |
 |
Table 3 Relative Risk of HT versus MRP Values |
The rMTT Values at Different Blood Pressure Levels Were Not Significantly Different
All patients with severe steno-occlusive MCA were divided into three groups by different SBP/DBP levels. To study the effect of hypertension on rMTT values in our research population, which had been proven to be different in the NHT and HT groups, we compared the levels of Am-rMTT, Lm-rMTT and Pm-rMTT between different subgroups and found no significant difference (Table 4).
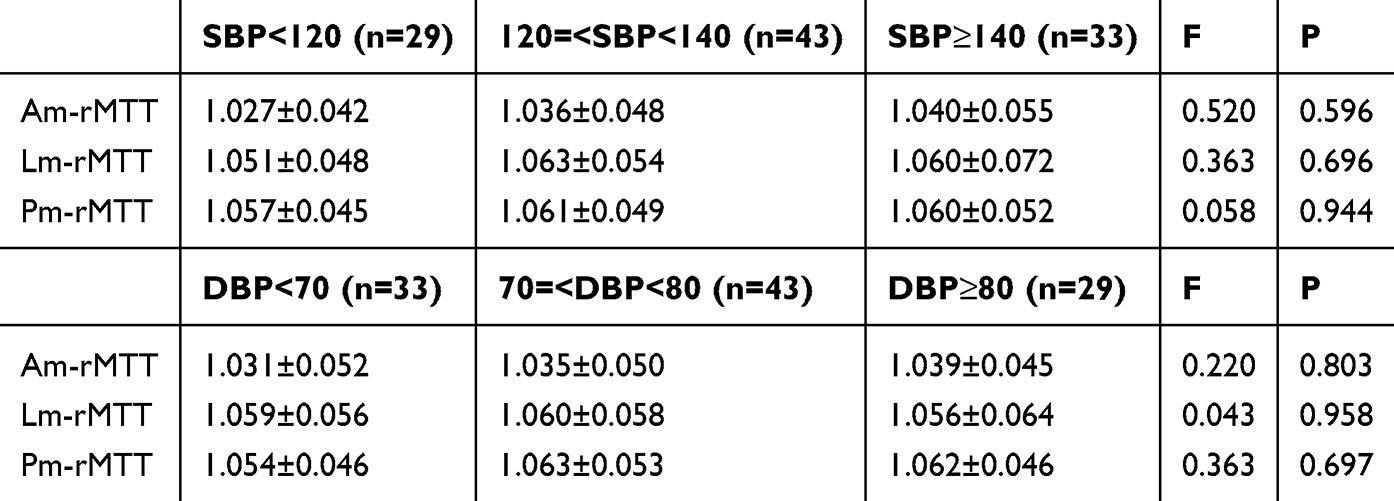 |
Table 4 Comparison of MRP Values Among the Different Blood Pressure Groups |
The Blood Pressure Control Level of Hypertensive Patients Was Related to the rMTT Values
Populations with hypertension were divided into good and poor blood pressure control according to SBP and DBP. Then, we compared the levels of Am-rMTT, Lm-rMTT and Pm-rMTT between NHT, HT+SBP<140 mmHg, HT+SBP≥140 mmHg and NHT, HT+DBP<80 mmHg, HT+DBP≥80 mmHg and found significant differences in Am-rMTT, Lm-rMTT, Pm-rMTT between theNHT and HT+SBP<140 mmHg groups. Additionally, we found differences between the NHT and HT+DBP<80 mmHg groups in Am-rMTT and Lm-rMTT (Table 5).
 |
Table 5 Comparison of MRP Values Among the NHT and Different Blood Pressure HT Groups |
Discussion
Our study revealed novel knowledge about hypertension, cerebral perfusion, collateral flow compensation and ICAS by analysing a representative population. Using PWI, significant differences were observed in HT+SBP<140 (p=0.035, 0.048, 0.049) and HT+DBP<80 (p=0.034, 0.045, 0.055) in rMTT compared with NHT. The differences in rMTT in the HT and NHT groups with different blood pressure levels suggested that strict blood pressure control in hypertensive patients with isolated severe steno-occlusive MCA would decrease perfusion.
We first confirmed that only the relative MTT values were significantly different between the NHT and HT groups. Previous studies have shown that MTT is a sensitive indicator of perfusion pressure in cerebral ischemia patients.19,20 The increase in MTT indicated a decrease in perfusion pressure. Another study also found that MTT was the most significant indicator of collateral circulation.21 Good collateral circulation can reduce the number and volume of cerebral infarction lesions by improving the perfusion area of stenosis-occlusion MCA,22 which is an important factor affecting the prognosis of patients with intracranial artery stenosis or occlusion.23 We found that hypertension was correlated with hypoperfusion in patients with severe steno-occlusive MCA, which was in accordance with Song Liu’s.24 An unusual result was that the MTT of the HT group was lower than that of the NHT group on both the ipsilateral and contralateral sides, although the difference was not significant. This phenomenon may be due to changes in the dynamics of cerebral blood vessel reactivity in patients with chronic hypertension.25 In addition, this may be related to the small sample size in our two groups, and we still expand the sample size in the future.
Considering that the baseline data of the HT and NHT groups had certain differences in age, diabetes and FIB, we next performed multivariable logistic regression adjusted for age, diabetes, and FIB. Statistical results further confirmed that Am-rMTT, Lm-rMTT and Pm-rMTT were correlated with HT. Similar views have been demonstrated in a community-based sample of Japanese individuals,26 which showed that hypertension was associated with a higher prevalence of severe-intracranial artery stenosis (ICAS).
We divided all patients into 3 subgroups according to blood pressure levels. No significant difference in rMTT was observed among the 3 subgroups. Does strict blood pressure control affect intracranial perfusion in patients with severe stenosis or chronic occlusive MCA? To answer this question, we divided the patients with hypertension into different groups and compared the MRP values. When the systolic blood pressure was set as 140 mmHg and diastolic blood pressure as 80 mmHg,27 statistically significant differences were found between subgroups. The results showed that rMTT was larger in patients with hypertension whose blood pressure was lower than 140/80 mmHg, and there was a significant difference compared with those without hypertension. MTT was defined as measuring the time between arterial inflow and venous outflow.28 A longer MTT indicates insufficient perfusion and poor microcirculation.29 rMTT was defined as the ratio of MTT ipsilateral to the contralateral side. The result showed poor collateral circulation when rMTT was greater than 1, and the larger the rMTT was, the worse the microcirculation. Our study showed that patients with hypertension whose blood pressure was strictly controlled to lower than 140/80 mmHg had worse collateral circulation than others. Hypertension was an independent factor associated with the occurrence of hypoperfusion after adjustment for other risk factors.24 In clinical work, we do not strictly control the blood pressure of patients with acute cerebrovascular disease to protect them from hypoperfusion injury. However, there were no guidelines to explain how to manage blood pressure in patients with severe intracranial vascular stenosis without acute cerebrovascular events, and doctors made the choice according to their own clinical experience. One retrospective study showed that a history of hypertension is a protective factor in patients with atherosclerotic middle cerebral artery stenosis/occlusion.30 Contrary to our research, a study found that hypertension impaired leptomeningeal collateral, and this impairment might be restored by antihypertensive treatment.31 However, this study was performed in mice, and the vascular occlusion injury was acute by surgery, which caused differences in the pathophysiological mechanism. The Carotid Occlusion Surgery Study (COSS) proved that Class III evidence that control of hypertension ≤130/85 mmHg is associated with a reduced risk of subsequent ipsilateral ischemic stroke in patients with recently symptomatic carotid occlusion.32 This difference may be caused by the fact that they selected patients with emerging symptomatic carotid artery occlusion, similar to the mouse study, while our study included patients with chronic large artery occlusion. Our study provided valid evidence that MCA severe stenosis of occlusion patients with hypertension should not strictly control their blood pressure because it would prolong the MTT value in the related blood supply area suggesting hypoperfusion.
This study had several limitations. First, it was a retrospective study, which would create a potential risk of selection bias. Second, we only investigated patients with severe stenosis of occlusion MCA. The results we obtained were not applicable to those with other intracranial or extracranial artery stenosis. Third, we did not introduce a direct assessment of the degree of collateral circulation, which might affect the outcome. We require further larger and multicenter studies to expand the applicability of this research.
Conclusion
This investigation was a retrospective study of patients with severe steno-occlusive MCA in which the correlation between intracranial perfusion and hypertension was evaluated. Relative MTT values were significantly different between the NHT and HT groups, showing that chronic hypertension might damage cerebral perfusion. The blood pressure control level of hypertensive patients is related to the rMTT value, which suggested that strict control of blood pressure in hypertensive patients with intracranial artery stenosis will further reduce ipsilateral cerebral perfusion. In conclusion, hypertensive patients with severe stenosis or occlusion of asymptomatic middle cerebral arteries should not be subjected to intensive blood pressure lowering (SBP<140 mmHg, DBP<80 mmHg). We need to individually evaluate the patient’s basical conditions before formulating a reasonable level of blood pressure to reduce the occurrence of acute cerebrovascular events.
Data Sharing Statement
Data analyzed for the current study are available from the corresponding author upon reasonable request.
Statement of Ethics
This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Nanjing Drum Tower hospital (Registration ID: No.2016-169-01). Patients or their relatives gave oral informed consent for follow-up. Written informed consents were obtained from all participants.
Statements and Declarations
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.
Acknowledgments
I would like to express my gratitude to all those who have helped me during the course of study and writing of this paper. I gratefully acknowledge the help of my colleagues who provided us with enough research objects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (81671140), Nanjing Medical Science and technique Development Foundation (QRX17002) and Nanjing Municipal Health Science and Technology Development Foundation (YKK21103).
Disclosure
The authors declare no conflicts of interest.
References
1. Bösel J. Blood pressure control for acute severe ischemic and hemorrhagic stroke. Curr Opin Crit Care. 2017;23(2):81–86. doi:10.1097/MCC.0000000000000394
2. Kitagawa K, Yamamoto Y, Arima H, et al. Effect of standard vs intensive blood pressure control on the risk of recurrent stroke: a randomized clinical trial and meta-analysis. JAMA neurol. 2019;76(11):1309–1318. doi:10.1001/jamaneurol.2019.2167
3. Lakhan SE, Sapko MT. Blood pressure lowering treatment for preventing stroke recurrence: a systematic review and meta-analysis. Int Arch Med. 2009;2(1):30. doi:10.1186/1755-7682-2-30
4. Benavente ORC, Conwit R; SPS3 StudyGroup. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial. Lancet. 2013;382:
5. Turan TN, Psychogios M-N. The CASSISS randomized clinical trial. Stroke. 2023;54(1):286–289. doi:10.1161/STROKEAHA.122.041096
6. Mazighi M, Richard S, Lapergue B, et al. Safety and efficacy of intensive blood pressure lowering after successful endovascular therapy in acute ischaemic stroke (BP-TARGET): a multicentre, open-label, randomised controlled trial. Lancet Neurol. 2021;20(4):265–274. doi:10.1016/S1474-4422(20)30483-X
7. Yamauchi H, Higashi T, Kagawa S, Kishibe Y, Takahashi M. Impaired perfusion modifies the relationship between blood pressure and stroke risk in major cerebral artery disease. J Neurol Neurosurg. 2013;84(11):1226. doi:10.1136/jnnp-2013-305159
8. Park J-M, Kim BJ, Kwon SU, et al. Intensive blood pressure control may not be safe in subacute ischemic stroke by intracranial atherosclerosis: a result of randomized trial. J Hypertens. 2018;36(9):1936–1941. doi:10.1097/HJH.0000000000001784
9. Shin HK, Nishimura M, Jones PB, et al. Mild induced hypertension improves blood flow and oxygen metabolism in transient focal cerebral ischemia. Stroke. 2008;39(5):1548–1555. doi:10.1161/STROKEAHA.107.499483
10. Li H-Q, Wang X, Wang H-F, et al. Dose-response relationship between blood pressure and intracranial atherosclerotic stenosis. Atherosclerosis. 2021;317:36–40. doi:10.1016/j.atherosclerosis.2020.12.004
11. Chan SL, Sweet JG, Bishop N, Cipolla MJ. Pial collateral reactivity during hypertension and aging understanding the function of collaterals for stroke therapy. Stroke. 2016;47(6):1618–U489. doi:10.1161/strokeaha.116.013392
12. Liebeskind DS, Jahan R, Nogueira RG, Zaidat OO, Saver JL, Investigators S. Impact of collaterals on successful revascularization in solitaire fr with the intention for thrombectomy. Stroke. 2014;45(7):2036–2040. doi:10.1161/strokeaha.114.004781
13. Tucker N, Stoffel JM, Hayes L, Jones GM. Blood pressure management following acute ischemic stroke a review of primary literature. Crit Care Nurs Q. 2020;43(2):109–121. doi:10.1097/cnq.0000000000000297
14. Tian G, Ji Z, Lin ZZ, Pan SY, Yin J. Cerebral autoregulation is heterogeneous in different stroke mechanism of ischemic stroke caused by intracranial atherosclerotic stenosis. Brain Behav. 2021;11(1):e01907. doi:10.1002/brb3.1907
15. Minhas J, Panerai R, Ghaly G, Divall P, Robinson T. Cerebral autoregulation in acute haemorrhagic stroke: a systematic review and meta-analysis of transcranial doppler studies. Eur J Neurol. 2018;25:27–28.
16. Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2018;49(3):e46–e99. doi:10.1161/STR.0000000000000158
17. Lu J, Lu Y, Wang X, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1·7 million adults in a population-based screening study (China PEACE million persons project). Lancet. 2017;390(10112):2549–2558. doi:10.1016/S0140-6736(17)32478-9
18. Chen C, Wei L, Li MT, et al. Superficial temporal artery trunk-to-middle cerebral artery bypass with short radial artery interposition graft for symptomatic internal carotid artery occlusion. World Neurosurg. 2019:127:E268–E279. doi:10.1016/j.wneu.2019.03.086
19. Sun HG, Zhang HM, Ma JP, Liu Y, Wang K, You C. Accuracy of computed tomography perfusion in detecting delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage: a meta-analysis. Neurol India. 2013;61(5):507–512. doi:10.4103/0028-3886.121922
20. González RG, Copen WA, Schaefer PW, et al. The Massachusetts general hospital acute stroke imaging algorithm: an experience and evidence based approach. J Neurointerv Surg. 2013;5(suppl 1):7–12. doi:10.1136/neurintsurg-2013-010715
21. Liu X, Pu YH, Pan YS, et al. Multi-mode CT in the evaluation of leptomeningeal collateral flow and the related factors: comparing with digital subtraction angiography. Neurological Res. 2016;38(6):504–509. doi:10.1080/01616412.2016.1187828
22. Peng G, Lu WP, Chen K, et al. Study on collateral circulation level and prognosis of acute ischemic stroke by 4D CTA-CTP integrated technology and serum S100B. Microvascular Res. 2022:140104270. doi:10.1016/j.mvr.2021.104270
23. Fanou EM, Knight J, Aviv RI, et al. Effect of collaterals on clinical presentation, baseline imaging, complications, and outcome in acute stroke. American Journal of Neuroradiology. 2015;36(12):2285–2291. doi:10.3174/ajnr.A4453
24. Liu S, Luo Y, Wang C, et al. Combination of plaque characteristics, pial collaterals, and hypertension contributes to misery perfusion in patients with symptomatic middle cerebral artery stenosis. J Magn Reson Imaging. 2020;51(1):195–204. doi:10.1002/jmri.26778
25. Malatino LS, Bellofiore S, Costa MP, et al. Cerebral blood-flow velocity after hyperventilation-induced vasoconstriction in hypertensive patients. Stroke. 1992;23(12):1728–1732. doi:10.1161/01.Str.23.12.1728
26. Shitara S, Fujiyoshi A, Hisamatsu T, et al. Intracranial artery stenosis and its association with conventional risk factors in a general population of Japanese men. Stroke. 2019;50(10):2967–2969. doi:10.1161/strokeaha.119.025964
27. Arshad Muhammad Iqbal SFJ. Essential Hypertension. In: StatPearls. Treasure Island (FL): StatPearls; 2023.
28. Todaka T, Hamada J, Kai Y, Morioka M, Ushio Y. Analysis of mean transit time of contrast medium in ruptured and unruptured arteriovenous malformations - A digital subtraction angiographic study. Stroke. 2003;34(10):2410–2414. doi:10.1161/01.Str.0000089924.43363.E3
29. Rusanen H, Saarinen JT, Sillanpää N. Collateral circulation predicts the size of the infarct core and the proportion of salvageable penumbra in hyperacute ischemic stroke patients treated with intravenous thrombolysis. Cerebrovascular Dis. 2015;40(3–4):182–190. doi:10.1159/000439064
30. Zeng Y, Li Y, Liu C, Zhang J, Huang H, Chen X. Predictors of internal borderzone infarcts in atherosclerotic middle cerebral artery stenosis. Zhonghua yi xue za zhi. 2014;94(47):3712–3716.
31. Omura-Matsuoka E, Yagita Y, Sasaki T, et al. Hypertension impairs leptomeningeal collateral growth after common carotid artery occlusion: restoration by antihypertensive treatment. J Neurosci Res. 2011;89(1):108–116. doi:10.1002/jnr.22522
32. Powers WJ, Clarke WR, Grubb RL, Videen TO, Adams HP, Derdeyn CP. Lower stroke risk with lower blood pressure in hemodynamic cerebral ischemia. Neurology. 2014;82(12):1027–1032. doi:10.1212/wnl.0000000000000238
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.