Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 13
Bispectral index in hypercapnic encephalopathy associated with COPD exacerbation: a pilot study
Authors Chalela R ![]() , Gallart L, Pascual-Guardia S
, Gallart L, Pascual-Guardia S ![]() , Sancho-Muñoz A, Gea J, Orozco-Levi M
, Sancho-Muñoz A, Gea J, Orozco-Levi M
Received 1 March 2018
Accepted for publication 15 June 2018
Published 26 September 2018 Volume 2018:13 Pages 2961—2967
DOI https://doi.org/10.2147/COPD.S167020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Video abstract presented by Roberto Chalela.
Views: 4652
Roberto Chalela,1–3 Lluis Gallart,4,5 Sergi Pascual-Guardia,1–3 Antonio Sancho-Muñoz,1,2 Joaquim Gea,1–3 Mauricio Orozco-Levi1–3
1Respiratory Medicine Department, Hospital del Mar-IMIM, Barcelona, Spain; 2Department CEXS, Universitat Pompeu Fabra, Barcelona, Spain; 3CIBERES, ISCIII, Barcelona, Spain; 4Department of Anesthesia, Hospital del Mar-IMIM, Barcelona, Spain; 5Universitat Autònoma de Barcelona, Barcelona, Spain
Background: Hypercapnic encephalopathy is relatively frequent in severe exacerbations of COPD (ECOPDs), with its intensity usually being evaluated through clinical scales. Bispectral index (BIS) is a relatively new technique, based on the analysis of the electroencephalographic signal, which provides a good approximation to the level of consciousness, having already been validated in anesthesia.
Objective: The objective of the study was to evaluate the utility of BIS in the assessment of the intensity of hypercapnic encephalopathy in ECOPD patients.
Patients and methods: A total of ten ECOPD patients were included, and the level of brain activity was assessed using BIS and different scales: Glasgow Coma Scale, Ramsay Sedation Scale (RSS), and Richmond Agitation–Sedation Scale. The evaluation was performed both in the acute phase and 3 months after discharge.
Results: BIS was recorded for a total of about 600 minutes. During ECOPD, BIS values ranged from 58.8 (95% CI: 48.6–69) for RSS score of 4 to 92.2 (95% CI: 90.1–94.3) for RSS score of 2. A significant correlation was observed between values obtained with BIS and those from the three scales, although the best fit was for RSS, followed by Glasgow and Richmond (r=-0.757, r=0.701, and r=0.615, respectively; P<0.001 for all). In the stable phase after discharge, BIS showed values considered as normal for a wake state (94.6; 95% CI: 91.7–97.9).
Conclusion: BIS may be useful for the objective early detection and automatic monitoring of the intensity of hypercapnic encephalopathy in ECOPD, facilitating the early detection and follow-up of this condition, which may avoid management problems in these patients.
Keywords: bispectral index, hypercapnic encephalopathy, exacerbation, COPD
Introduction
Exacerbations are acute situations that appear in the course of COPD (exacerbations of COPD [ECOPDs]) and condition patient prognosis and quality of life.1 When these ECOPDs are severe, they may induce hypercapnia, which in turn can lead to respiratory acidosis and neurological abnormalities, including neurological–cognitive alterations and a reduction in the level of consciousness, which is known as hypercapnic encephalopathy.2 Although the latter condition is characterized by an initial phase of psychomotor excitation, it can evolve to confusion, stupor, and finally, coma, and death.3 Moreover, the impairment in the level of consciousness can compromise airway permeability and even the patient’s life. In this regard, when the hypercapnic encephalopathy is severe, a formal contraindication for the use of non-invasive mechanical ventilation is considered,4 which may lead to the need for orotracheal intubation and invasive ventilation.5 Although the pathophysiology of hypercapnic encephalopathy is not fully understood, it appears to depend primarily on the acidosis of the cerebrospinal fluid, which is derived from the passage of CO2 through the blood–brain barrier.3,6
Despite its potential deleterious consequences for the patient, hypercapnic encephalopathy is usually evaluated qualitatively or, more rarely, with clinical scales that provide a better approximation, but has not been validated for this specific purpose. In addition, these scales do not allow automatic monitoring of the patient and, therefore, should be repeated periodically in those individuals at risk of rapid deterioration. The most commonly used scale is the Glasgow Coma Scale (GCS), which was actually developed for the assessment of patients with traumatic brain injury.7,8 Other scales that have been used for hypercapnic encephalopathy are the Ramsay Sedation Scale (RSS) and the Richmond Agitation–Sedation Scale (RASS), which were both designed primarily to assess sedation in anesthetized subjects.9,10 In contrast, the bispectral index (BIS) signal is obtained from the automatic analysis of brain activity, recorded through a series of electrodes placed on the scalp, and transformed into a numerical value ranging from 0 to 100.11 Although this technique was developed 20 years ago,11 until now it has been used mostly to assess the depth of anesthesia during surgical procedures.12–19 In fact, its use has improved the titration of neuroactive agents, also avoiding inappropriate intraoperative awakenings. However, in recent years, BIS has been extended to other fields of medicine.20–24 Interestingly, positron emission tomography has demonstrated a direct relationship between cerebral metabolic activity and values provided by BIS.14 We hypothesize that BIS may also be useful in the objective assessment and monitoring of severe respiratory patients who show, or are at the risk of developing, hypercapnic encephalopathy with depression of the level of consciousness. Consequently, the objective of the present pilot study was to evaluate the utility of BIS in the evaluation of this condition in a very frequent clinical context (ECOPD), analyzing the potential relationships of the BIS signal with the most widely used scales.
Patients and methods
This was a prospective and controlled study in which successive patients were recruited at the intermediate respiratory care unit of our center, where they were admitted for a ECOPD associating hypercapnic encephalopathy (PaCO2 >45 mmHg along with neurological–cognitive alterations and/or consciousness impairment in the absence of alternative causes as assessed by two expert pulmonologists). COPD diagnosis and assessment included forced spirometry with bronchodilator test (Datospir 92; Sibelmed®, Barcelona, Spain), determination of static lung volumes and airway resistance by body plethysmography (MasterLab; JAEGER™, Würzburg, Germany), carbon monoxide transfer (DLco, gas analyzer included in the MasterLab), and arterial blood gases (GEM Premier 3000; Instrumentation Laboratory, Bedford, MA, USA). The sample size was calculated from previous works that had used the BIS technique for other purposes.25–27
Ethics statement
The study was designed according to local and European legislation, being approved by the ethics committee at our institution (Fundació IMIM, reference 2013/5416/I). Informed written consent was obtained from all patients, who also consented to publication of their clinical data.
Protocol
At the time of inclusion, patients were monitored with a BIS device (Vista Monitoring System, BIS-XP software; Aspect Medical Systems Inc., Norwood, MA, USA). In parallel, three different clinical scales, GCS, RSS, and RASS, were repeatedly used at least at admission (first hour) and sixth hour of hospital stay, as well as immediately after the disappearance of the encephalopathy semiology (absence of flapping tremor and correct response to a standardized basic questionnaire). An additional determination of clinical scales was added at the ninth hour in three patients who showed a more persistent encephalopathy. Values provided by BIS were recorded through the same period. Finally, a new assessment (BIS and scales) was performed 3 months after discharge, with all patients in a stable phase.
Variables
BIS values were obtained for each second, and the mean, maximum, and minimum values for each minute were recorded. For the present study, the average of mean values obtained in 10 minutes following the measurement of the scales were taken. Values between 100 and 90 are typical of fully awake individuals, while those between 90 and 60 indicate a mild-to-moderate reduction in the level of consciousness (confusion to stupor), 60–40 characterized first degrees of unconsciousness, and values below 40 correspond to a deep coma.13,28,29 Regarding the three clinical scales, they were designed to assess the level of consciousness in different clinical scenarios.9,10,30–32 The GCS considers motor, verbal, and ocular reactions of the patient both spontaneously and in response to different stimuli, with its values ranging from 3 to 15.8,33 RSS, in turn, classifies the degree of sedation in six different levels, from 1 (agitation) to 6 (absence of response to intense stimuli),9 while RASS is a ten-level scale, with four levels being positive, indicating an increase in patient’s activity, a zero-value corresponding to an awake individual, and five negative levels designating progressive degrees of sedation.34
Statistical analysis
Categorical variables are expressed as absolute and relative frequencies, whereas continuous variables are described as mean (SD) or median (95% CI), as appropriate in each case. Correlations between values obtained with BIS and the scales were assessed using the Spearman correlation coefficient. The significance was defined by an alpha (P) error <0.05. Data were analyzed using the SPSS v20 program (IBM Corporation, Armonk, NY, USA).
Results
Ten consecutive COPD patients, with a net predominance of males and a severe-to-very severe disease were admitted to the emergency department of our institution with ECOPD criteria, hypercapnia, acidosis, and clinical diagnosis of secondary encephalopathy (Table 1).
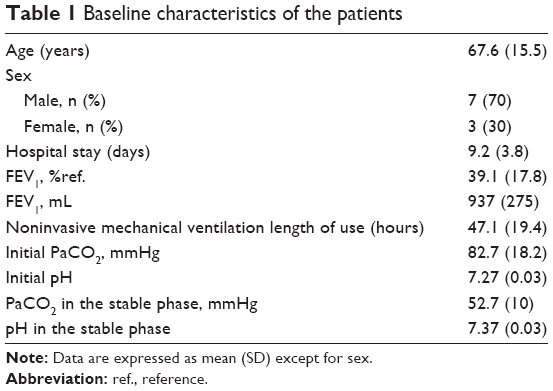 | Table 1 Baseline characteristics of the patients |
BIS assessment
The BIS signal was recorded for a total of 588 minutes, with a complete absence of local complications. The summary of these data both during admission and 3 months following discharge is shown in Figure 1. All patients showed an initial BIS of ≤90 (median, 71.0 [95% CI, 61.4–80.5]), with a variable behavior over time, although most showed an upward tendency through the hospitalization period, with normalization of BIS values in all patients in the post-discharge follow-up assessment.
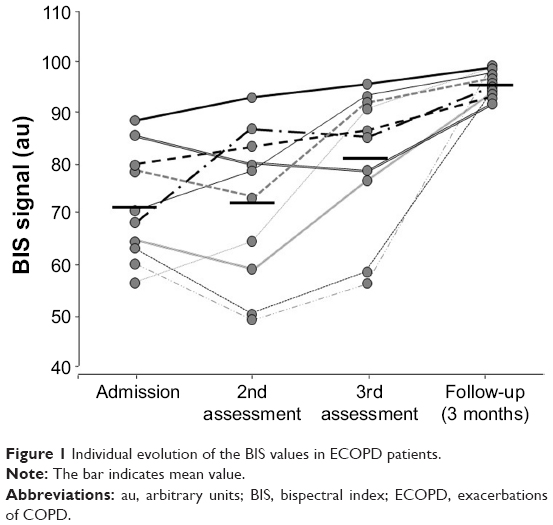 | Figure 1 Individual evolution of the BIS values in ECOPD patients. |
Comparison of BIS with clinical scales
A significant correlation was observed between BIS values and those obtained with the three scales included in the study (Figure 2). The best relationship was obtained with RSS (r=−0.757), followed by that of GCS (r=0.701) (P<0.001 in both cases). A more modest correlation was shown by RASS (r=0.615, also P<0.001). Moreover, a close relationship was observed when different categories defined by the RSS score were compared with values provided by BIS: patients with a RSS score of 2 showed a BIS value of 92.2 (95% CI, 90.1–94.3), similar to that described for awake subjects,13 whereas those with a RSS score of 3 corresponded to a BIS value of 66.1 (95% CI, 54.5–77.6), and patients with a RSS score of 4 showed a BIS value of 58.8 (95% CI, 48.6–69), which is the characteristic of sedation.13 No significant correlations were found between BIS and different lung function variables, including arterial blood gases. All patients underwent a standardized treatment for their condition, including noninvasive mechanical ventilation, nebulized and inhaled bronchodilators (beta-agonists and anticholinergics), antibiotics, and systemic steroids. The evaluation was favorable in all cases, with no need for endotracheal intubation in any of them, and patients were discharged from hospital, with subsequent controls in the outpatient clinics.
 | Figure 2 Correlation between BIS values and the scores obtained with the three clinical scales: (A) Ramsay Sedation Scale, (B) Glasgow Coma Scale, and (C) Richmond Agitation–Sedation Scale. |
In the evaluation performed 3 months after discharge, BIS value was 94.6 (95% CI, 91.7–97.9), and all three scales and physical examination showed fully awake patients, even though the majority of them (90%) still showed hypercapnia without acidosis (Table 1).
Discussion
The pilot study shows that determination of BIS can be useful to objectively assess the degree of hypercapnic encephalopathy in ECOPD patients. Its correlation with clinical scales is good, especially, with those of Ramsay and Glasgow, although the main advantages of BIS over them are that it requires no direct intervention from health professionals and permits a continuous instrumental monitoring of the patient’s consciousness level, with the potential setting of automatic alarms. This does not mean that direct surveillance of the patient should be neglected but it can facilitate its management.
The dynamic and instrumental assessment of the level of consciousness is very important in patients who, as in the case of the subjects included in the present study, can quickly move to a more critical state. In such a situation, consciousness impairment may go unnoticed by health care personnel, which can have dramatic consequences, as it can be associated with ventilatory or cardiovascular failure, or problems in airway permeability. Moreover, if the depression of consciousness is severe, the use of noninvasive mechanical ventilation will become inappropriate, involving the need for endotracheal intubation and invasive ventilatory procedures.4,5
The hypercapnic encephalopathy is a metabolic disorder with impact on the level of consciousness. Its pathophysiology is not completely known, although it seems to depend fundamentally on the presence of acidosis both in the cerebrospinal fluid and brain interstitial tissue.3,35 Moreover, both hypercapnia and the accompanying hypoxia can cause vasodilation in the cerebral vessels, increasing blood flow, and potentially generating edema and an increased intracranial pressure,36 with potential neurological effects. Finally, central nervous system acidosis appears to induce a decrease in the phosphocreatine levels, increasing glucose-6-phosphate, fructose-6-phosphate, and lactate/pyruvate ratio, which would lead to an impaired level of glucose utilization. Consequently, glutamate concentrations and acetylcholine synthesis will decrease, which can also result in decreased brain activity.3,37 In the present study, all patients with hypercapnic encephalopathy also had respiratory acidosis, which most probably were targeting their central nervous system by the abovementioned pathways.
In a simple way, BIS is based on the fact that high frequencies of the electroencephalographic signal prevail during wakefulness, while low frequencies are predominant during sleep or under anesthesia.11,37 BIS provides a continuous scale that derives from a multivariate analysis generated from neurophysiological records obtained from patients.11 The BIS signal also correlates with cerebral blood flow and indicators of local metabolic activity, such as the use of glucose.38,39 Its correlation with the level of consciousness assessed in anesthetized subjects is excellent,15,40 and therefore, the main use of BIS is in anesthesia, to assess the level of sedation of a patient, regulate the use of neuroactive drugs, or reduce inappropriate early intraoperative awakenings.41 This technique has also been occasionally used in other circumstances, such as drug abuse, pharmacological intoxications, hypothermia, hepatic encephalopathy, and transfer of patients between different care areas to alert about unexpected deteriorations.42–45 In the field of respiratory diseases, some attempts by using BIS have been made to evaluate different stages of sleep or the depth of pharmacological sedation during respiratory endoscopy.22,23 There are also three previous studies that have evaluated the utility of this technique in critically ill patients treated with and without different modalities of mechanical ventilation and different sedative drugs.20,24,46
Limitations of the study
The present study has some limitations derived from the BIS technique itself. This procedure can slightly overestimate or underestimate the actual state of consciousness in exceptional cases, with overestimation, especially, being a potential problem in severe respiratory patients, and therefore, an adequate clinical surveillance will always be necessary. It can also be a problem in anesthesia, as it may involve the use of unnecessarily high doses of neuroactive drugs. On the contrary, the underestimation of the consciousness state would only result in an oversight of patients who actually do not need it. The use of BIS in young children also constitutes a specific problem, which derives from the immaturity of their electroencephalogram signal.47 However, despite these technical limitations, it is commonly accepted that, although there are other alternatives for the assessment of response to external stimuli (such as monitoring of the autonomic nervous system with ANSiscope), the BIS seems more specific for the evaluation of consciousness levels.
Other potential limitations to the present pilot study derive from the small population included. Although the sample size was derived from the results of previous studies using BIS, our findings should be taken with the same cautions that are intrinsic of a pilot study. Certainly, further studies including large populations are needed to confirm our results. Moreover, the present study has been carried out in a very specific population (ECOPD patients with hypercapnic encephalopathy), and it would be inappropriate to extend its conclusions to other respiratory conditions associating this metabolic abnormality (such as thoracic cage or neuromuscular disorders).
As for the analysis of the relationship between BIS and the clinical scales, a correlation rather than a concordance analysis was chosen. This approach seems appropriate for a pilot study and the important differences between magnitudes obtained with the two approximations, having also been chosen by some of the previous authors.15,25 In fact, the correlations were good when obtained with either continuous or categorical values obtained with BIS and the three scales.
Conclusion
BIS seems to adequately reflect the state of consciousness in patients with hypercapnic encephalopathy secondary to ECOPD. This technique has no relevant drawbacks and maybe useful in monitoring critical respiratory patients. Broader studies are needed to confirm our findings and potentially extend our conclusions to other respiratory disorders.
Summary at glance
We evaluated the utility of BIS for the clinical assessment of hypercapnic encephalopathy in exacerbated COPD patients. A significant correlation was observed between BIS and three commonly used clinical scales, confirming that the former technique maybe useful for the objective early detection and monitoring of hypercapnic encephalopathy in such patients.
Acknowledgments
We are thankful to Jonathan McFarland for his editing aid and to Mireia Admetllo and Camino Fernández for their help in collecting clinical data. This project was funded in part by SAF SAF2014-54371, CIBERES, BRN-Pla Armengol 2014, 2014SGR424, SEPAR 2015, and SEPAR Becario 2015.
Disclosure
The authors report no conflicts of interest in this work.
References
Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. | ||
Young GB, DeRubeis DA. Metabolic encephalopathies. In: Young GB, Ropper AH, Bolton CF, editors. Coma and Impaired Consciousness: A Clinical Perspective. New York: McGraw-Hill Companies; 1998:307–392. | ||
Scala R. Hypercapnic encephalopathy syndrome: a new frontier for non-invasive ventilation? Respir Med. 2011;105(8):1109–1117. | ||
Organized jointly by the American Thoracic Society, the European Respiratory Society, the European Society of Intensive Care Medicine, and the Societé de Reanimation de Langue Francaise, and approved by ATS Board of Directors, December 2000. International consensus conferences in intensive care medicine: noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med. 2001;163(1):283–291. | ||
British Thoracic Society Standards of Care Committee. Non-invasive ventilation in acute respiratory failure. Thorax. 2002;57(3):192–211. | ||
Posner JB, Swanson AG, Plum F. Acid-base balance in cerebrospinal fluid. Arch Neurol. 1965;12:479–496. | ||
Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 2001;163(2):540–577. | ||
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81–84. | ||
Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2(5920):656–659. | ||
Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166(10):1338–1344. | ||
Sigl JC, Chamoun NG. An introduction to bispectral analysis for the electroencephalogram. J Clin Monit. 1994;10(6):392–404. | ||
Health Quality Ontario. Bispectral index monitor: an evidence-based analysis. Ont Health Technol Assess Ser. 2004;4:1–70. | ||
Rosow C, Manberg PJ. Bispectral index monitoring. Anesthesiol Clin North America. 2001;19(4):947–966. | ||
Sleigh JW, Andrzejowski J, Steyn-Ross A, Steyn-Ross M. The bispectral index: a measure of depth of sleep? Anesth Analg. 1999;88(3):659–661. | ||
Yaman F, Ozcan N, Ozcan A, Kaymak C, Basar H. Assessment of correlation between bispectral index and four common sedation scales used in mechanically ventilated patients in ICU. Eur Rev Med Pharmacol Sci. 2012;16(5):660–666. | ||
Pyeon T, Chung S, Kim I, Lee S, Jeong S. The effect of triazolam premedication on anxiety, sedation, and amnesia in general anesthesia. Korean J Anesthesiol. 2017;70(3):292–298. | ||
Dumans-Nizard V, Le Guen M, Sage E, Chazot T, Fischler M, Liu N. Thoracic epidural analgesia with levobupivacaine reduces remifentanil and propofol consumption evaluated by closed-loop titration guided by the bispectral index: a double-blind placebo-controlled study. Anesth Analg. 2017;125(2):635–642. | ||
Du Y, Shi H, Yu J. Comparison in anesthetic effects of propofol among patients with different ABO blood groups. Medicine (Baltimore). 2017;96(20):e5616. | ||
Funcke S, Sauerlaender S, Pinnschmidt HO, et al. Validation of innovative techniques for monitoring nociception during general anesthesia: a clinical study using tetanic and intracutaneous electrical stimulation. Anesthesiology. 2017;127(2):272–283. | ||
Senoglu N, Oksuz H, Dogan Z, Yildiz H, Demirkiran H, Ekerbicer H. Sedation during noninvasive mechanical ventilation with dexmedetomidine or midazolam: A randomized, double-blind, prospective study. Curr Ther Res Clin Exp. 2010;71(3):141–153. | ||
Hata K, Andoh A, Hayafuji K, et al. Usefulness of bispectral monitoring of conscious sedation during endoscopic mucosal dissection. World J Gastroenterol. 2009;15(5):595–598. | ||
Dahaba AA, Xue JX, Xu GX, Liu QH, Metzler H. Bilateral bispectral Index (BIS)-Vista as a measure of physiologic sleep in sleep-deprived anesthesiologists. Minerva Anestesiol. 2011;77(4):388–393. | ||
Hong SD, Dhong HJ, Kim HY, et al. Change of obstruction level during drug-induced sleep endoscopy according to sedation depth in obstructive sleep apnea. Laryngoscope. 2013;123(11):2896–2899. | ||
Mondello E, Siliotti R, Noto G, et al. Bispectral Index in ICU: correlation with Ramsay Score on assessment of sedation level. J Clin Monit Comput. 2002;17(5):271–277. | ||
Kasuya Y, Govinda R, Rauch S, Mascha EJ, Sessler DI, Turan A. The correlation between bispectral index and observational sedation scale in volunteers sedated with dexmedetomidine and propofol. Anesth Analg. 2009;109(6):1811–1815. | ||
LeBlanc JM, Dasta JF, Pruchnicki MC, Gerlach A, Cook C. Bispectral index values, sedation-agitation scores, and plasma Lorazepam concentrations in critically ill surgical patients. Am J Crit Care. 2012;21(2):99–105. | ||
Turan A, Dalton JE, Kasuya Y, Akça O, Sessler DI, Rauch S. Correlation between Bispectral Index, Observational Sedation Scale, and Lower Esophageal Sphincter Pressure in volunteers using dexmedetomidine or propofol. Med Sci Monit. 2012;18(10):CR593–CR596. | ||
Gan TJ, Glass PS, Windsor A, et al. Bispectral index monitoring allows faster emergence and improved recovery from propofol, alfentanil, and nitrous oxide anesthesia. BIS Utility Study Group. Anesthesiology. 1997;87(4):808–815. | ||
Roberts DJ, Haroon B, Hall RI. Sedation for critically ill or injured adults in the intensive care unit: a shifting paradigm. Drugs. 2012;72(14):1881–1916. | ||
Gotoh O, Tamura A, Yasui N, Suzuki A, Hadeishi H, Sano K. Glasgow Coma Scale in the prediction of outcome after early aneurysm surgery. Neurosurgery. 1996;39(1):19–25. | ||
Ostábal MI, Sanz C, Suárez MA, Salvo L, Millastre A. The study of prognostic factors of spontaneous subarachnoid hemorrhage. Rev Neurol. 1997;25(137):58–60. | ||
Heard K, Bebarta VS. Reliability of the Glasgow Coma Scale for the emergency department evaluation of poisoned patients. Hum Exp Toxicol. 2004;23(4):197–200. | ||
Iankova A. The Glasgow Coma Scale: clinical application in emergency departments. Emerg Nurse. 2006;14(8):30–35. | ||
Sessler CN, Grap MJ, Brophy GM. Multidisciplinary management of sedation and analgesia in critical care. Semin Respir Crit Care Med. 2001;22(2):211–226. | ||
Posner JB, Swanson AG, Plum F. Acid-base balance in cerebrospinal fluid. Arch Neurol. 1965;12:479–496. | ||
Siegel GJ, Agranoff BW, Albers RW, Fisher SK. Uhler MD, editors. Basic Neurochemistry: Molecular, Cellular and Medical Aspects. 6th ed. Philadelphia: Lippincott-Raven; 1999. | ||
Kaul HL, Bharti N. Monitoring depth of anaesthesia. Indian J Anaesth. 2002;46:323–332. | ||
Noirhomme Q, Boly M, Bonhomme V, et al. Bispectral index correlates with regional cerebral blood flow during sleep in distinct cortical and subcortical structures in humans. Arch Ital Biol. 2009;147(1–2):51–57. | ||
Alkire MT. Quantitative EEG correlations with brain glucose metabolic rate during anesthesia in volunteers. Anesthesiology. 1998;89(2):323–333. | ||
Flaishon R, Windsor A, Sigl J, Sebel PS. Recovery of consciousness after thiopental or propofol. Bispectral index and isolated forearm technique. Anesthesiology. 1997;86(3):613–619. | ||
Myles PS, Leslie K, Mcneil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet. 2004;363(9423):1757–1763. | ||
Dahaba AA, Worm HC, Zhu SM, et al. Sensitivity and specificity of bispectral index for classification of overt hepatic encephalopathy: a multicentre, observer blinded, validation study. Gut. 2008;57(1):77–83. | ||
Fatovich DM, Jacobs IG, Celenza A, Paech MJ. An observational study of bispectral index monitoring for out of hospital cardiac arrest. Resuscitation. 2006;69(2):207–212. | ||
Wennervirta J, Salmi T, Hynynen M, et al. Entropy is more resistant to artifacts than bispectral index in brain-dead organ donors. Intensive Care Med. 2007;33(1):133–136. | ||
Hernández-Gancedo C, Pestaña D, Criado A. Bispectral index monitoring during intrahospital transport. Rev Esp Anestesiol Reanim. 2007;54(3):169–172. | ||
Lu W, Fu Q, Luo X, Fu S, Hu K. Effects of dexmedetomidine on sleep quality of patients after surgery without mechanical ventilation in ICU. Medicine. 2017;96(23):e7081. | ||
Grindstaff RJ, Tobias JD. Applications of bispectral index monitoring in the pediatric intensive care unit. J Intensive Care Med. 2004;19(2):111–116. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.