Back to Journals » Clinical Ophthalmology » Volume 19
Biosimilar Versus Innovator Ranibizumab in Myopic CNVM: Comparative Real-World Outcomes- The BRIM Study
Authors Chakraborty D ![]() , Sinha TK, Sinha S, Biswas RK, Maiti A, Nandi K
, Sinha TK, Sinha S, Biswas RK, Maiti A, Nandi K ![]() , Rungta D, Bhattacharya R
, Rungta D, Bhattacharya R
Received 26 June 2025
Accepted for publication 16 September 2025
Published 10 October 2025 Volume 2025:19 Pages 3741—3747
DOI https://doi.org/10.2147/OPTH.S549744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Debdulal Chakraborty,1 Tushar Kanti Sinha,1 Sourav Sinha,2 Rupak Kanti Biswas,2 Aniruddha Maiti,3 Krishnendu Nandi,2 Dinesh Rungta,1 Ranabir Bhattacharya1
1Vitreo-Retina Services, Disha Eye Hospitals, Kolkata, WB, India; 2Vitreo-retina Services, Nethralayam Superspeciality Eye Care, Kolkata, WB, India; 3Vitreo-Retina Services Global Eye Hospital, Kolkata, WB, India
Correspondence: Debdulal Chakraborty, Vitreo-retinal Services, Disha Eye Hospitals, Kolkata, West Bengal, India, Tel +91 33 6636 0000, Email [email protected]
Purpose: To compare the efficacy and safety of biosimilar ranibizumab (Razumab®) versus innovator ranibizumab (Lucentis®/Accentrix®) in the treatment of myopic choroidal neovascular membrane (mCNVM).
Methods: This retrospective, multicenter study included treatment-naïve patients with mCNVM between January 2021 and December 2023. Patients received intravitreal injections of either innovator or biosimilar ranibizumab, following a pro re nata (PRN) protocol. Inclusion criteria were: age ≥ 18years, axial length > 26.5 mm or spherical equivalent ≥ – 6.00 D, diagnosis confirmed by multimodal imaging, and a minimum 12-month follow-up. Outcomes assessed included change in best-corrected visual acuity (BCVA; ETDRS letters), central macular thickness (CMT), intraocular pressure (IOP), injection frequency, and safety profile.
Results: A total of 80 eyes were analyzed (Group A: Innovator, n=38; Group B: Biosimilar, n=42). Mean BCVA improved from 51.0 ± 16.5 to 64.5 ± 5.5 ETDRS letters in the Innovator group and from 52.5 ± 16.5 to 64.5 ± 4.5 in the Biosimilar group at 12 months (p > 0.05). CMT reduced significantly in both groups (Innovator: from 332.03 ± 39.22 μm to 268.32 ± 18.78 μm; Biosimilar: from 315.03 ± 44.20 μm to 271.12 ± 20.39 μm; (p > 0.05). The mean number of injections was 2.68 ± 0.51 in the Innovator Ranibizumab group and 2.71 ± 0.49 in the Biosimilar Ranibizumab group. IOP remained stable in both cohorts, and no significant ocular or systemic adverse events were observed.
Conclusion: Biosimilar ranibizumab demonstrated non-inferior visual and anatomical outcomes compared to innovator ranibizumab in the treatment of mCNVM, with a similar safety profile and treatment burden.
Keywords: myopia, myopic CNVM, anti VEGF, ranibizumab, biosimilar ranibizumab
Introduction
Pathologic myopia is a major cause of irreversible visual impairment worldwide, particularly in Asian populations, and is characterized by excessive axial elongation of the globe resulting in progressive structural alterations in the retina, choroid, and sclera.1 One of the most sight-threatening complications of pathologic myopia is the development of choroidal neovascular membranes (CNVM), which typically arise due to mechanical stretching and breaks in Bruch’s membrane, known as lacquer cracks. These changes permit the growth of abnormal choroidal vessels into the subretinal space, often leading to hemorrhage, subretinal fluid, and eventual scarring if not treated promptly. Clinically, patients with myopic CNVM often present with acute onset of central visual blurring or metamorphopsia, necessitating early diagnosis and intervention to preserve visual acuity.1–3
Anti-vascular endothelial growth factor (anti-VEGF) therapy has become the standard of care for myopic CNVM.4 Ranibizumab, a monoclonal antibody fragment targeting VEGF-A, has demonstrated significant efficacy in improving visual outcomes and reducing disease activity in myopic CNVM. The RADIANCE study, a pivotal randomized controlled trial, showed that ranibizumab was superior to verteporfin photodynamic therapy, with fewer injections required and better visual recovery.5 Importantly, compared to neovascular age-related macular degeneration, myopic CNVM tends to be smaller, less exudative, and more responsive to treatment, often requiring fewer injections.3–5
In recent years, biosimilar versions of ranibizumab have emerged as more affordable therapeutic alternatives, particularly in low- and middle-income countries.6 Biosimilars are biologic products that are highly similar to approved reference products in terms of quality, efficacy, and safety. In India, a ranibizumab biosimilar (Razumab®; Intas Pharmaceuticals, Ahmedabad, India) was approved for intravitreal use by the Drug Controller General India (DCGI) in 20157 and has shown good efficacy for most retinal disorders. It has gained widespread use due to its lower cost, which has the potential to improve access to treatment in resource-constrained settings.6,7 However, despite increasing utilization, head-to-head comparative data on the efficacy and safety of biosimilar versus innovator ranibizumab specifically in myopic CNVM is lacking.
This study aims to address this gap by evaluating and comparing the visual and anatomical outcomes of innovator ranibizumab (Lucentis/Accentrix, Novartis, Mumbai, India) and biosimilar ranibizumab (Razumab, Intas pharmaceuticals, Gujarat, India) in the treatment of myopic CNVM in a real-world clinical setting. By doing so, we seek to provide evidence that may guide treatment decisions and inform healthcare policy in regions where cost remains a significant barrier to the use of anti-VEGF therapy.
Methods
This was a retrospective, comparative, multicenter study conducted across 3 eye care networks in India between Jan 2021 – Dec 2023. The study included patients diagnosed with myopic choroidal neovascular membrane (CNVM) who received intravitreal ranibizumab injections—either the innovator molecule (Lucentis/Accentrix®, Novartis, Mumbai, India) or a biosimilar formulation (Razumab®, Intas Pharmaceuticals Gujarat, India)—as part of their routine clinical care.
Inclusion criteria were: patients aged ≥18 years with a diagnosis of myopic CNVM based on multimodal imaging (including fundus fluorescein angiography and spectral domain optical coherence tomography [SD OCT]), axial length >26.5 mm or spherical equivalent ≥ −6.00 diopters, and a minimum follow-up of 12 months after initiation of anti-VEGF therapy. Eyes that received prior anti-VEGF therapy for other indications, had coexisting retinal pathologies (eg, diabetic retinopathy, age related macular degeneration, polypoidal choroidal vasculopathy), or incomplete clinical records were excluded.
Exclusion criteria: CNVM secondary to age-associated macular degradation, polypoidal choroidal vasculopathy, inflammatory disease, angioid streaks or trauma, subfoveal fibrosis or atrophy, any prior treatment such as photodynamic therapy or retinal laser photocoagulation for CNVM secondary to pathologic myopia, and systemic diseases were excluded.
Patients were divided into two cohorts based on the type of anti-VEGF therapy received:
• Group A (Innovator group): Received intravitreal innovator ranibizumab (0.5 mg in 0.05 mL).
• Group B (Biosimilar group): Received intravitreal biosimilar ranibizumab at an equivalent dose.
All injections were administered under sterile conditions following a standardized protocol in sterile operating theatre as is prevalent in India.8 Treatment regimens followed a pro re nata (PRN) approach after first injection, guided by disease activity on OCT and/or clinical examination.
Data collection included demographic details, baseline and follow-up best-corrected visual acuity (BCVA), central macular thickness (CMT) on spectral-domain OCT (Cirrus 5000, Carl Zeis, Germany), and the number of injections received over the follow-up period. The primary outcome measure was the change in BCVA from baseline to 12 months. Secondary outcomes included change in CMT, number of injections required, and the presence or resolution of subretinal or intraretinal fluid. Safety data including ocular or systemic adverse events were also recorded.
Statistical analysis was performed using SPSS version 23.0. Continuous variables were expressed as mean ± standard deviation, and categorical variables as frequencies and percentages. Intergroup comparisons were made using the independent t-test or Mann–Whitney U-test for continuous variables and the Chi-square or Fisher’s exact test for categorical variables. A p-value <0.05 was considered statistically significant.
The study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of Disha Eye Hospitals (Regn Number ECR/846/Inst/WB/2016/RR-19: EC-CT-2024-30).
Results
Both the Innovator and Biosimilar Ranibizumab groups demonstrated substantial and sustained improvement in best-corrected visual acuity (BCVA), expressed in ETDRS letter scores, across the 12-month period. In the Innovator group, mean BCVA improved from 51.0 ± 16.5 at baseline to 64.5 ± 5.5 at 12 months (p > 0.05). Similarly, the Biosimilar group showed improvement from 52.5 ± 16.5 at baseline to 64.5 ± 4.5 at 12 months (p > 0.05). The most rapid gains were seen in the first three months, with both groups reaching peak vision by 6 months (65.5 letters) and maintaining stability thereafter. At all-time points, the differences in BCVA between groups were minimal and not statistically significant, confirming the non-inferiority of biosimilar ranibizumab to its innovator counterpart in improving visual outcomes in patients with myopic CNVM. Figure 1 shows a comparative visual acuity graph. Table 1–3 contains detailed visual acuity, central macular thickness and intra ocular pressure details at various time points.
 |
Table 1 Baseline Demography |
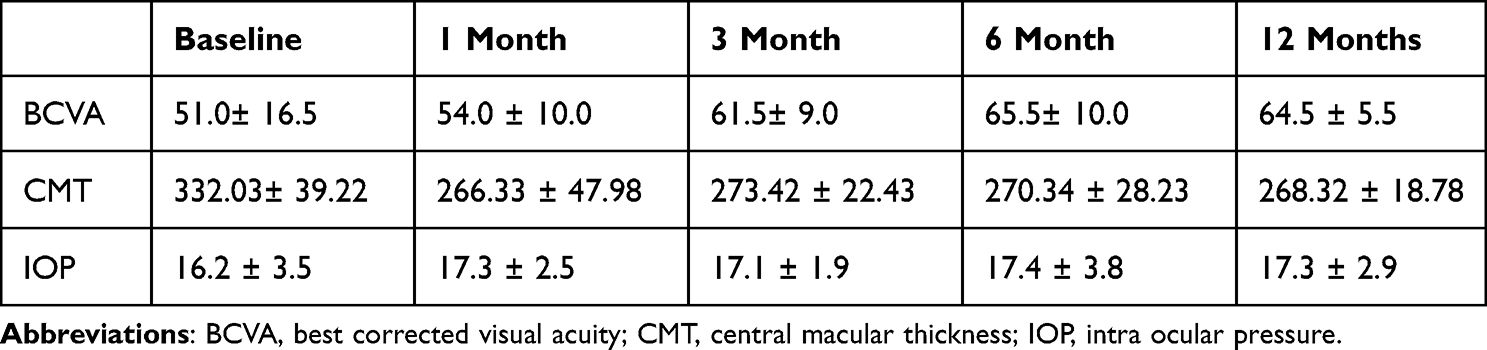 |
Table 2 Changes in BCVA,CMT & IOP in Innovator Group |
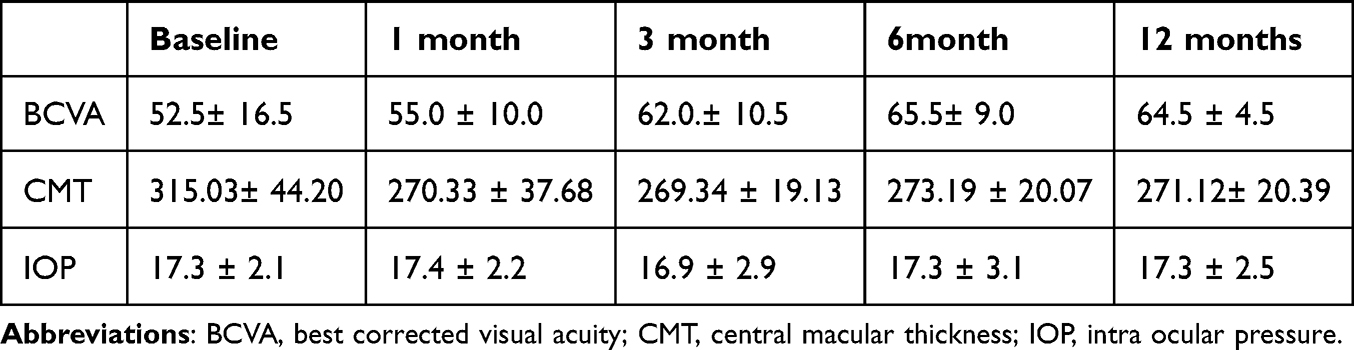 |
Table 3 Changes in BCVA,CMT & IOP in Biosimilar Ranibizumab Group |
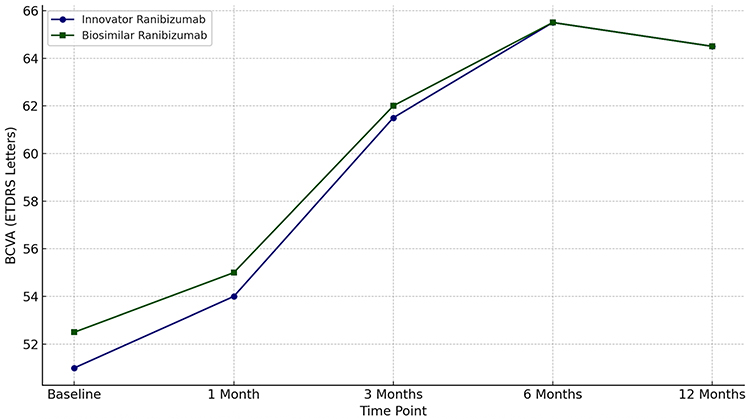 |
Figure 1 Best corrected visual acuity (ETDRS Letters) Over Time in Innovator ranibizumab vs Biosimilar ranibizumab(Razumab) Groups. |
In the Innovator group, baseline central macular thickness (CMT) was 332.03 ± 39.22 µm, which reduced to 266.33 ± 47.98 µm at 1 month. The CMT remained stable with values of 273.42 ± 22.43 µm, 270.34 ± 28.23 µm, and 268.32 ± 18.78 µm at 3, 6, and 12 months respectively (p > 0.05), demonstrating a sustained anatomical response.
In the Biosimilar group, baseline CMT was 315.03 ± 44.20 µm, reducing to 270.33 ± 37.68 µm at 1 month, and remaining stable at 269.34 ± 19.13 µm, 273.19 ± 20.07 µm, and 271.12 ± 20.39 µm at 3, 6, and 12 months, respectively (p > 0.05). No statistically significant differences were found in CMT between the two groups at any time point (all p > 0.1), again supporting the finding that biosimilar and innovator ranibizumab perform similarly in terms of anatomical improvement in myopic CNVM. Figure 2 gives a comparative graph of the CMT at different time points.
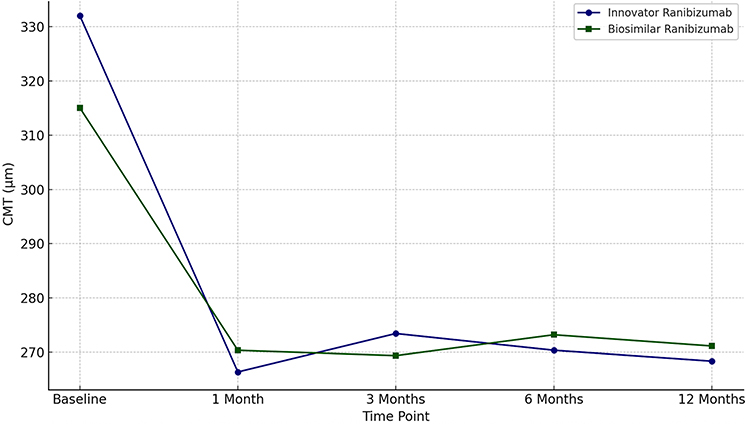 |
Figure 2 Central macular thickness Comparison Over Time: Innovator ranibizumab vs Biosimilar Ranibizumab (Razumab). |
The mean IOP in the Innovator group was 16.2 ± 3.5 mmHg at baseline, which rose slightly to 17.3 ± 2.5 mmHg at 1 month, fluctuating mildly thereafter: 17.1 ± 1.9 mmHg at 3 months, 17.4 ± 3.8 mmHg at 6 months, and 17.3 ± 2.9 mmHg at 12 months. These changes were not statistically significant (p = 0.74 overall), indicating stable IOP throughout the study duration. In the Biosimilar group, the baseline IOP was 17.3 ± 2.1 mmHg, with minimal fluctuations at 1 month (17.4 ± 2.2 mmHg), 3 months (16.9 ± 2.9 mmHg), 6 months (17.3 ± 3.1 mmHg), and 12 months (17.3 ± 2.5 mmHg). No significant changes were observed over time (p = 0.89). Intergroup comparison showed no significant difference in IOP at any time point (all p > 0.1), indicating that both treatment groups maintained stable intraocular pressure profiles over the course of treatment.
The mean number of injections administered over the 12-month period was 2.68 ± 0.51 in the Innovator Ranibizumab group and 2.71 ± 0.49 in the Biosimilar Ranibizumab group. Statistical analysis using an independent samples t-test showed no significant difference between the two groups (p = 0.76), indicating comparable injection frequencies No serious ocular or sysmentic side effects were noted in either group during the course of the study.
Discussion
This real-world, multicenter comparative study demonstrates that biosimilar ranibizumab (Razumab) is non-inferior to innovator ranibizumab in the treatment of myopic choroidal neovascular membrane (mCNVM), with comparable functional and anatomical outcomes and similar treatment burden over 12 months.
Visual Acuity Outcomes
Both groups in our study demonstrated rapid and sustained visual improvement, gaining approximately 13 ETDRS letters over 12 months, with maximal improvement observed by month 6. This aligns closely with results from the pivotal RADIANCE trial, which reported a mean gain of 10.5–10.6 letters at 3 months in patients treated with ranibizumab using PRN protocols based on disease activity or visual stability criteria.5 Similarly, the Cochrane review of anti-VEGF therapy in pathological myopia found a 13-letter gain at 2 years compared to photodynamic therapy (PDT), with a higher proportion of eyes gaining ≥3 lines of vision.9 Comparable results were also seen in studies assessing other anti-VEGF agents. Cha et al demonstrated a BCVA improvement from logMAR 0.63 to 0.39 with ranibizumab and similar gains with bevacizumab over 12 months.10 Ahmed and Howaidy, in a randomized study, showed that both aflibercept and ranibizumab led to comparable BCVA improvements (~0.15 logMAR gain) at 3 months.11 Our findings support the broad therapeutic efficacy of anti-VEGF agents across different molecular platforms and reinforce the clinical relevance of biosimilars.
The anatomical response, as measured by central macular thickness (CMT), was robust in both treatment arms. Reductions of 60–65 µm were observed within the first month, with stability thereafter. This rapid fluid resolution is characteristic of mCNVM, which typically presents with smaller lesions and less exudation compared to age-related macular degeneration. Our results are comparable to the findings of Parravano et al, who reported significantly greater and sustained CMT reduction in eyes treated with ranibizumab compared to PDT, along with better long-term visual stability.12 Ahmed and Howaidy similarly reported that both aflibercept and ranibizumab achieved significant and comparable reductions in CMT over 3 months.13 Sayanagi et al demonstrated that anti-VEGF agents, including ranibizumab, controlled lesion activity effectively.14
Our study confirms the low treatment burden typical of myopic CNVM. Patients required fewer than four injections over 12 months in both biosimilar and innovator groups, consistent with real-world patterns and trial data. The RADIANCE trial also employed a PRN regimen and showed that patients with myopic CNVM required fewer injections than those with neovascular AMD5 The RE-ENACT 2 study from India corroborates this, reporting a mean of 3–4 injections annually with biosimilar ranibizumab in various retinal indications.14 The comparable injection frequencies in our study (2.68 in the innovator group vs 2.71 in the biosimilar group; p = 0.76) highlight the biosimilar’s equivalent efficacy and durability.
Both groups maintained stable intraocular pressure (IOP) without significant changes over time. No ocular or systemic adverse events were recorded during the study. These findings are consistent with safety profiles reported in the Cochrane review, which noted rare adverse events with anti-VEGF use in mCNVM.9 Additionally, real-world pharmacovigilance studies from India and elsewhere have reported low rates of complications, including endophthalmitis and thromboembolic events, when intravitreal biosimilar ranibizumab is administered under appropriate sterile conditions.15
Although not evaluated in our study due to the 12-month follow-up period, long-term data suggest a risk of chorioretinal atrophy (CRA) in eyes treated for mCNVM. Sayanagi et al observed CRA progression in 40% of eyes over 1 year, with no significant difference between aflibercept and ranibizumab.13 Similarly, Parravano et al found greater CRA expansion in PDT-treated eyes versus those receiving ranibizumab, indicating a possible protective effect of anti-VEGF therapy.12 However, these changes may still occur despite treatment and could limit long-term visual gains, underscoring the need for extended follow-up beyond one year.
Key strengths of the present study include its multicenter design, inclusion of treatment-naïve patients, and real-world PRN treatment regimens reflective of actual clinical practice. The sample was well-matched in terms of baseline refractive error, duration of symptoms, and initial BCVA, allowing for a balanced comparison. Our study is unique in the sense that while there are studies which have demonstrated the effectiveness and safety of Biosimilar ranibizumab (Razumab) in diabetic macular edema, neovascular age related macular degeneration, literature search did not provide any studies on its use in myopic cnvm.7,16–19
Limitations include its retrospective nature and relatively short follow-up duration that precludes evaluation of atrophy progression or recurrence. Additionally, while biosimilar equivalence is demonstrated in this indication, extrapolation to other retinal diseases should be approached with caution unless supported by dedicated data.
Conclusion
In conclusion, the BRIM study demonstrates that biosimilar ranibizumab(Razumab) is clinically equivalent to innovator ranibizumab in improving visual and anatomical outcomes in myopic CNVM, with a similar safety profile and injection burden. These findings support the continued adoption of biosimilars as a cost-effective therapeutic alternative, particularly in settings where affordability remains a major barrier to sustained care. Further prospective, longer-term studies are warranted to assess recurrence patterns and CRA progression with biosimilar use in pathological myopia.
Consent to Participate
The authors confirm that all research participants provided informed consent for involvement in this study.
Acknowledgments
Dr Debasish Bhattacharya MS, Chairman, Disha Eye Hospitals, Kolkata, India.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ohno-Matsui K, Kawasaki R, Jonas JB. META-analysis for Pathologic Myopia (META-PM) Study Group, et al. International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol. 2015;159(5):877–83.e7. PMID: 25634530. doi:10.1016/j.ajo.2015.01.022
2. Cohen SY, Laroche A, Leguen Y, Soubrane G, Coscas GJ. Etiology ofchoroidal neovascularization in young patients. Ophthalmology. 1996;103(8):1241–1244. doi:10.1016/S0161-6420(96)30515-0
3. Yoshida T, Ohno-Matsui K, Yasuzumi K, et al. Myopic choroidal neovascularization: a 10-year follow-up. Ophthalmology. 2003;110(7):1297–1305. doi:10.1016/S0161-6420(03)00461-5
4. Silva RM, Ruiz-Moreno JM, Nascimento J, et al. Short-term efficacy and safety of intravitreal ranibizumab for myopic choroidal neovascularization. Retina. 2008;28(8):1117–1123. doi:10.1097/IAE.0b013e31817eda41
5. Wolf S, Balciuniene VJ, Laganovska G, et al. RADIANCE: a randomized controlled study of ranibizumab in patients with choroidal neovascularization secondary to pathologic myopia. Ophthalmology. 2014;121(3):682–92.e2. doi:10.1016/j.ophtha.2013.10.023
6. Sharma A, Kondo M, Iwahashi C, et al. Approved biosimilar ranibizumab-a global update. Eye. 2023;37(2):200–202. doi:10.1038/s41433-022-02246-5
7. Sharma A, Kumar N, Parachuri N, Bandello F, Kuppermann BD, Loewenstein A. Ranibizumab biosimilar (Razumab) vs innovator ranibizumab (Lucentis) in neovascular age-related macular degeneration (n-AMD)- efficacy and safety (BIRA study). Eye. 2022;36(5):1106–1107. doi:10.1038/s41433-021-01616-9
8. Sheth JU, Stewart MW, Khatri M, et al. Changing trends in the use of anti-vascular endothelial growth factor (anti-VEGF) biosimilars: insights from the vitreoretinal society of India biosimilars of anti-VEGF survey. Indian J Ophthalmol. 2021;69(2):352–356. doi:10.4103/ijo.IJO_2703_20
9. Zhu Y, Zhang T, Xu G, Peng L. Anti-vascular endothelial growth factor for choroidal neovascularisation in people with pathological myopia. Cochrane Database Syst Rev. 2016;12:CD011160. doi:10.1002/14651858.CD011160.pub2
10. Cha DM, Kim TW, Heo JW, et al. Comparison of 1-year therapeutic effect of ranibizumab and bevacizumab for myopic choroidal neovascularization: a retrospective, multicenter, comparative study. BMC Ophthalmol. 2014;14:69. doi:10.1186/1471-2415-14-69
11. Ahmed H, Howaidy A, Eldaly ZH. Comparison of structural and functional outcome of aflibercept versus ranibizumab in patients with myopic choroidal neovascularization. Eur J Ophthalmol. 2019;29(6):645–651. doi:10.1177/1120672118805877
12. Parravano M, Ricci F, Oddone F, et al. Long-term functional and morphologic retinal changes after ranibizumab and photodynamic therapy in myopic choroidal neovascularization. Retina. 2014;34(10):2053–2062. doi:10.1097/IAE.0000000000000201
13. Sayanagi K, Uematsu S, Hara C, et al. Effect of intravitreal injection of aflibercept or ranibizumab on chorioretinal atrophy in myopic choroidal neovascularization. Graefes Arch Clin Exp Ophthalmol. 2019;257(4):749–757. doi:10.1007/s00417-018-04214-w
14. Sharma A, Kumar N, Kuppermann BD, et al. Real-world effectiveness, safety, and tolerability of Razumab® (world’s first biosimilar ranibizumab) in wet age-related macular degeneration: RE-ENACT study. Int J Retin Vitr. 2020;6:29.
15. Rajurkar K, Mehta R, Dave VP, et al. Safety profile of intravitreal biosimilar ranibizumab (Razumab) in real-life Indian settings: a post-marketing surveillance study. Indian J Ophthalmol. 2019;67(8):1160–1165. doi:10.4103/ijo.IJO_1093_18
16. Chakraborty D, Sinha TK, Maiti A, et al. Transitioning from aflibercept to biosimilar ranibizumab in diabetic macular edema (DME): (The TRANSFORM-DME Trial) a multicenter observational study. Clin Ophthalmol. 2024;18:3449–3456. doi:10.2147/OPTH.S500912
17. Chakraborty D, Boral S, Sinha TK, et al. Transitioning from aflibercept to biosimilar ranibizumab in neovascular AMD (The TRANSFORM Trial): a multicenter observational study. Clin Ophthalmol. 2024;18:1819–1828. doi:10.2147/OPTH.S459085
18. Chakraborty D, Mondal S, Boral S, et al. Biosimilar versus InnovAtor MoLecule of RAnibizumab in Neovascular Age-Related MaCular DEgeneration (The BALANCE Trial): real-world evidence. Clin Ophthalmol. 2023;17:1067–1076. doi:10.2147/OPTH.S407219
19. Chakraborty D, Sinha TK, Mondal S, et al. Innovator ranibizumab ComparEd to Biosimilar ranibizumab in combination with Expansile gas in submaculaR HemorrhaGe: the ICEBERG study. BMC Ophthalmol. 2025;25:41. doi:10.1186/s12886-025-03846-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.