Back to Journals » Clinical Ophthalmology » Volume 19
Biomechanical Corneal Parameters in Eyes With Chronic Ocular Hypotony and in Non-Hypotonic Eyes. Self-Controlled Case Series Study
Authors Bouchikh-El Jarroudi R ![]() , Roche Fernández K
, Roche Fernández K ![]() , Romera Romero P, Croitoru-Croitoru T, Goñi-Guarro A
, Romera Romero P, Croitoru-Croitoru T, Goñi-Guarro A ![]() , Botella-Garcia J
, Botella-Garcia J ![]() , Sabala Llopart A, Loscos-Arenas J
, Sabala Llopart A, Loscos-Arenas J ![]() , Videla S
, Videla S
Received 23 November 2024
Accepted for publication 10 February 2025
Published 8 April 2025 Volume 2025:19 Pages 1237—1246
DOI https://doi.org/10.2147/OPTH.S508165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Rachid Bouchikh-El Jarroudi,1– 3,* Kolbe Roche Fernández,1,4,* Pau Romera Romero,1 Tatiana Croitoru-Croitoru,1 Anna Goñi-Guarro,1 Jessica Botella-Garcia,1 Antoni Sabala Llopart,1 Jordi Loscos-Arenas,1 Sebastian Videla5,6
1Service of Ophthalmology, Hospital Universitari Germans Trias i Pujol, Badalona, Spain; 2Department of Surgery, Universitat Autònoma de Barcelona (UAB), Barcelona, Spain; 3Evidence Based Ophthalmology Unit (Oftalmoevidencia), Scientia Clinical and Epidemiological Research Institute, Trujillo, Peru; 4Department of Medicine, Universitat Autònoma de Barcelona (UAB), Barcelona, Spain; 5Clinical Research Support Area, Clinical Pharmacology Department, Hospital Universitari Germans Trias i Pujol, Badalona, Spain; 6Department of Pharmacology, Therapeutics and Toxicology. Autonomous University of Barcelona, Bellaterra, Spain
*These authors contributed equally to this work
Correspondence: Rachid Bouchikh-El Jarroudi, Hospital Universitari Germans Trias i Pujol, Carretera de Canyet, s/n, Badalona, Barcelona, 08916, Spain, Tel +34 689 14 80 84, Fax +34 934 97 88 43, Email [email protected]
Introduction: There are no available data concerning corneal parameters in patients with chronic ocular hypotony. Our purpose is to provide evidence and clinical correlation on the biomechanical corneal changes in chronic hypotonic eyes.
Patients and Methods: A single-center, transversal, self-controlled case series study was conducted involving patients with at least one chronic hypotonic eye (defined as an intraocular pressure ≤ 6.5 mmHg measured on three separate occasions for at least three months). The chronic hypotonic eye was the case and the contralateral eye the control (non-hypotonic eye). We collected data from baseline characteristic and intraocular pressure (mmHg). Biomechanical corneal parameters measured by Corvis ST: deformation amplitude ratio (mm), Ambrósio’s relational thickness (μm), stiffness parameter at first applanation (mmHg/mm), Integrated radius (mm− 1), stress-strain index, pachymetry (μm), and in addition macular folds were recorded as well. A descriptive and exploratory analysis was performed.
Results: Between November 2021 and July 2023, a total of 16 consecutive patients (7 men, 9 women; age [median (range)]: 72 (62– 84)), diagnosed with chronic ocular hypotony in one eye were included: 16 chronic hypotonic eyes and 16 non-hypotonic eyes. Hypotonic versus non-hypotonic eyes [median (range)]: intraocular pressure: 4 (2– 6) mmHg, 16 (8– 38) mmHg; deformation amplitude ratio: 5.6 (4.3– 6.6) mm, 4.7 (3.9– 5.5) mm, p-value= 0.002; Ambrósio’s relational thickness: 482 (263– 932) μm, 530 (210– 818) μm, p-value: 0.845; stiffness parameter at first applanation: 61.5 (39– 100) mmHg/mm, 113 (68– 130) mmHg/mm, p-value: < 0.001; Integrated radius: 10.9 mm− 1 (6.3– 16.8), 7.9 mm− 1 (6.4– 10.5), p-value: < 0.001; stress-strain index: 0.7 (− 0.2– 4.9), 1.1 (− 2.7– 5.6), p-value: 0.034; pachymetry 509 (456– 617) μm, 512 (436– 775) μm, p-value: 0.637; and macular folds: 7/16, 0/16, p-value: < 0.001.
Conclusions: Chronic hypotonic eyes (eyes with a low intraocular pressure) present biomechanical corneal changes with respect to non-hypotonic eyes, mainly in deformation amplitude ratio, stiffness parameter at first applanation, stress-strain index and Ambrósio’s relational thickness parameters. These biomechanical corneal changes could reflect softer, more elastic and deformable scleras, which at its turn can bear higher risk of hypotony maculopathy.
Keywords: ocular hypotony, corneal biomechanics, macular folds
Introduction
Ocular hypotony is a condition characterized by a low intraocular pressure (IOP).1 The cause of ocular hypotony can be diverse, including ocular surgery, ocular trauma, and uveitis1,2 Likewise, although infrequent, it is a common complication after antimetabolites use in glaucoma filtering surgery.1,3 Ocular hypotony can lead to vision loss due to hypotony maculopathy and choroidal detachment.2 Ocular hypotony condition is sometimes difficult to revert, posing a medical challenge.3
Classically, the dynamics of aqueous humour (AH) have been used to explain hypotony as a result of AH production and drainage imbalance.1,4 However, IOP is not only determined by AH inflow and outflow. It has also been associated with other factors such as corneal biomechanical properties. In fact, growing interest in corneal biomechanics and their relationship with glaucoma has arisen recently.5–12 Several studies have demonstrated that stiffer corneas are both associated with faster glaucoma progression,13,14 and open-angle glaucoma.5 Nonetheless, to the best of our knowledge, there are no available scientific manuscripts concerning the corneal parameters in patients with chronic ocular hypotony.
Currently, there are two devices commercially available to evaluate corneal biomechanical properties. The first including air-jet infrared light technology (Ocular Response Analyzer, ORA; Reichert, Inc., Depew, NY, USA),15 and the second based on air-puff Scheimpflug imaging system (Corvis Scheimplug Tonometer, Corvis ST, Oculus Optikgeräte GmbH, Wetzlar, Germany)9 Corvis ST has the advantage of obtaining a real-time imaging during corneal deformation using a high-speed camera that gathers 4300 frames per second within a 100-millisecond period, obtaining 140 images of the cornea with a high resolution of 640×480 pixels. High-speed imaging enables detailed analysis of the corneal dynamics during the deformation process and hence may provide valuable information regarding biomechanical parameters of the cornea and their clinical correlation.9,16,17
Our working hypothesis was that eyes affected by chronic hypotony have biomechanical corneal changes, reflecting softer, more elastic and deformable scleras and thus increased risk of hypotony maculopathy. Therefore, the aim of this study was to provide evidence on the biomechanical corneal changes in chronic hypotonic eyes, which can arise new potential clinical correlations such as a greater need for an aggressive treatment of chronic hypotony.
Patients and Methods
Study Design
This study is a single-center, transversal, retrospective, self-controlled case series study in patients diagnosed with chronic hypotony. The eye affected by hypotony was the case and the contralateral eye was the control.
The study protocol received Institutional Review Board and Ethics Committee of the Hospital Universitari Germans Trias i Pujol approval (Reference Number: PI-24-275), and all patients included gave their written informed consent to participate. The study complied with the updated Declaration of Helsinki, Good Clinical Practice guidelines, and applicable Spanish and European regulatory requirements. Confidentiality was ensured following the European Regulation (EU) 2016/679 of the European Parliament and Council, and current Spanish law (LOPD 3/2018). This manuscript complies with the STROBE statement.
Study Population
Patients diagnosed with chronic ocular hypotony by the glaucoma unit from our Ophthalmology Department were identified and located by telephone. The study was explained to them. If they decided to participate, they were cited to sign the informed consent. The starting point of the study was November 2021, when a specific clinical database for patients treated in the glaucoma unit was created.
We included adult patients (≥18 years of age) of either sex, with a diagnosis of chronic hypotonic eye, biomechanical parameters available in the medical file, and a signed informed consent. The chronic hypotonic eye was the case and the contralateral eye the control (non-hypotonic eye). The following data was gathered: age at chronic hypotonic eye diagnosis, affected eye (right, left), cause of hypotony, sex, clinical background (hypertension, dyslipidemia, diabetes, and antecedent of heart attack. Both from hypotonic and non-hypotonic eyes IOP (mmHg) and biomechanical corneal parameters were also recorded.
Chronic Hypotonic Eye
Chronic hypotonic eye was defined as an IOP ≤6.5 mmHg measured on three separate occasions for at least three months.18 The IOP was obtained using Haag-Streit Goldmann tonometer (Model AT 900; Haag-Streit, Bern, Switzerland) and expressed in mmHg.
Non-hypotonic eye was defined as eye without a diagnosis of chronic hypotony, but this one could have been diagnosed with glaucoma or ocular hypertension.
Biomechanical Corneal Parameters
According to our clinical practice, the biomechanical corneal parameters are assessed using the Corvis ST device (Oculus Optikgerate GmbH, Wetzlar, Germany) after diagnosing a chronic hypotony eye.
The following six biomechanical corneal parameters, measured with Corvis ST, were gathered: i) Deformation amplitude ratio (DA) (mm), ii) Ambrósio’s relational thickness (ARTh) (μm), iii) Stiffness parameter at first applanation (SPA1) (mmHg/mm), iv) Integrated radius (IR) (mm−1), v) Stress-strain index (SSI) (no units apply due to its nature, the result of a mathematical algorithm in which different parameters of corneal biomechanics and IOP are analyzed),19 and vi) Pachymetry (μm). Table 1 gathers the definition and the clinical application of these biomechanical corneal parameters.
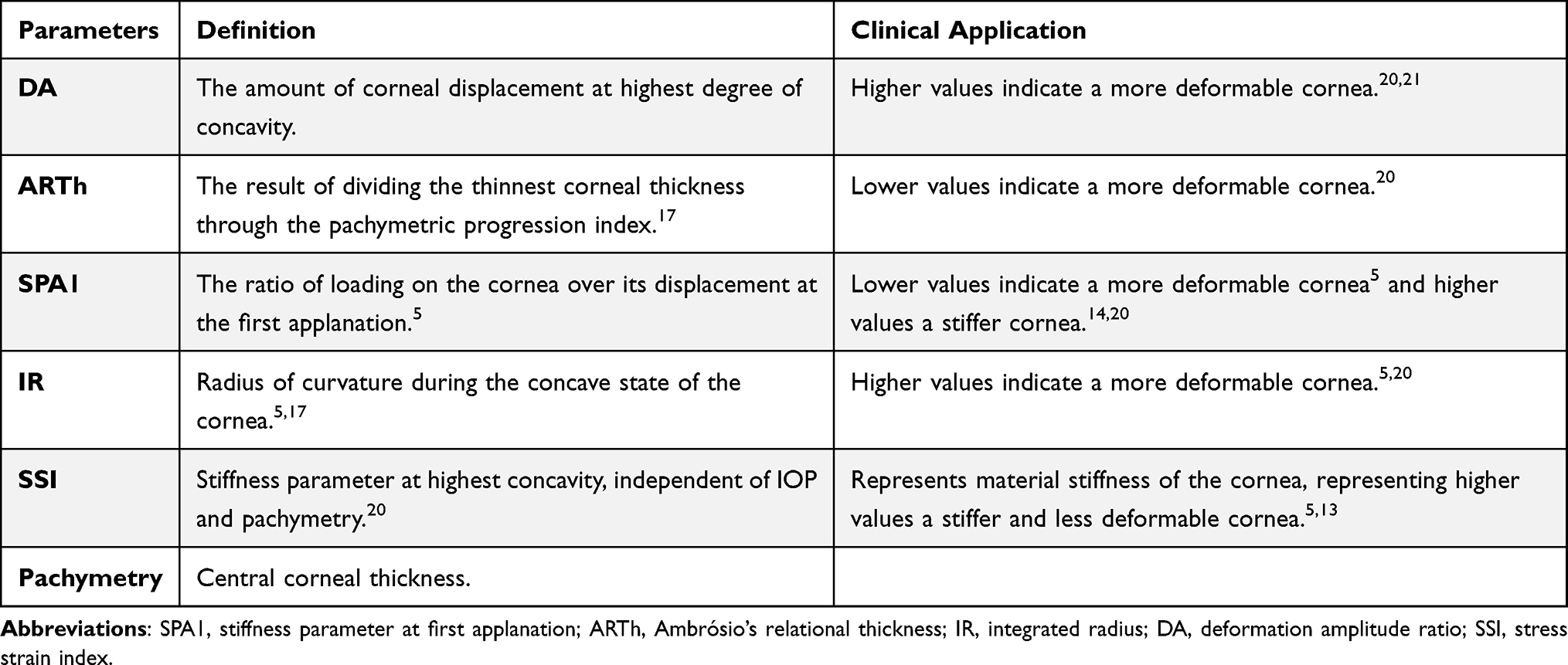 |
Table 1 Summary of Biomechanical Corneal (Corvis ST) Parameters |
In addition, macular folds were also measured. Macular folds were diagnosed on clinical grounds and then a macular scan was recorded by optical coherence tomography (OCT) scans (Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA). The presence of macular folds was recorded as a dichotomous variable.
Statistical Analysis
Given the exploratory nature of this study, no formal sample size calculation was conducted.
Categoric variables were expressed as absolute and relative frequencies. The clinical outcome assessments (quantitative variables) were expressed as medians and ranges or as means and standard deviations (SD), as applicable. A descriptive and exploratory analysis was performed. The distribution normality of measurements was assessed using the Shapiro-Wilk test. The Wilcoxon signed rank test was used to compare hypotonic and non-hypotonic eyes values of non-parametric variables (IOP, SPA1, SSI and pachymetry). The hypotonic and non-hypotonic eyes mean values of the parametric variables (DA, ARTh and IR) were compared using the paired Student t-test. The statistical significance level was set at p-value < 0.05. Data analysis was performed using Jamovi software version 2.1 (https://www.jamovi.org).
Data Availability Statement. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Results
Baseline Characteristics
Between November 2021 and July 2023, a total of 16 consecutive patients —median (range) 72 (62–84) years of age, 9 (56.3%) females and 7 (43.8%) males— were diagnosed of chronic ocular hypotony of one eye. All these patients were included in the study.
Five patients had no past medical history recorded (31,1%). Five patients (31,1%) presented hypertension and dyslipidaemia, 2 patients (12.5%) had a history of arterial hypertension and myocardial infarction, 1 case had hypertension, diabetes and dyslipidaemia, 1 case had diabetes and renal chronic disease, 1 case had folic acid deficiency and the last case had only a history of renal lithiasis.
Table 2 shows the causes of ocular hypotony. The most prevalence cause occurred after a non-perforating deep sclerectomy in 11 (68.75%) patients.
 |
Table 2 Glaucoma Treatment Received in Chronic Hypotony Eyes and Non-Hypotonic Eyes |
Biomechanical Corneal Parameters Outcomes
The median (range) of IOP was 4 (2–6) mmHg in chronic hypotonic eyes and 16 (8–38) mmHg in non-hypotonic eyes (p-value < 0,001***).
Biomechanical corneal parameters were available for 16 chronic hypotonic eyes and 16 non-hypotonic eyes. Table 3 presents the Biomechanical corneal parameters outcomes evaluated by Corvis ST and Figure 1 depicts the box plot for these results. The outcomes in IR and DA were higher and statistically significant in chronic hypotonic eyes compared to non-hypotonic eyes. SPA1 and SSI outcomes were lower and statistically significant in chronic hypotonic eyes compared to non-hypotonic eyes.
 |
Figure 1 Box plot representing the results of Corvis ST parameters in eyes with and without chronic hypotony. Abbreviations: DA, deformation amplitude ratio; ARTh, Ambrósio’s relational thickness; SPA1, stiffness parameter at first applanation; IR, integrated radius; SfSI, stress strain index. |
Table 4 compares the Biomechanical corneal parameters outcomes of chronic hypotony eyes with non-hypotonic eyes without glaucoma, being altered the same parameters previously described from Table 3.
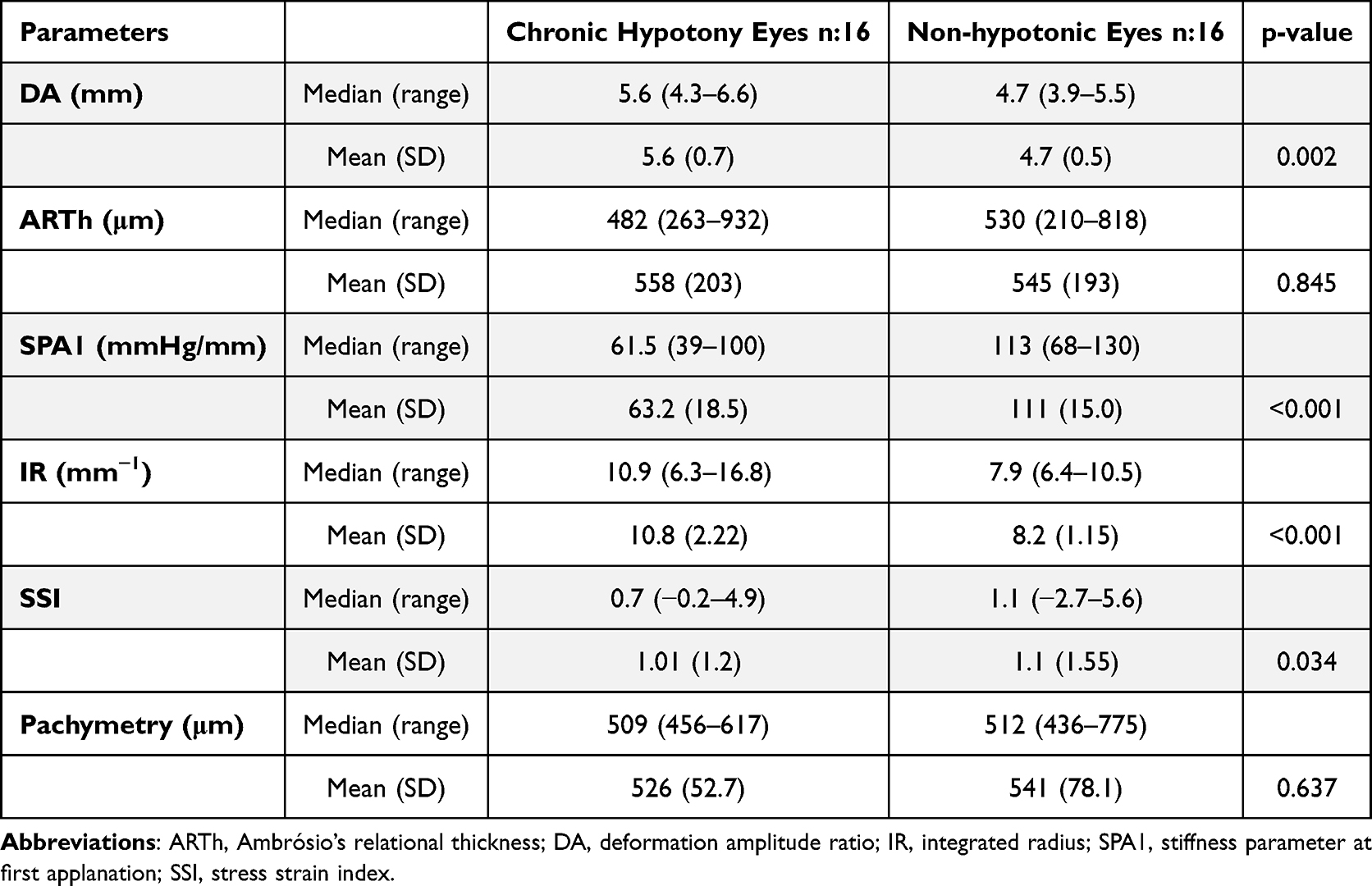 |
Table 3 Biomechanical Corneal (Corvis ST) Parameters Outcomes |
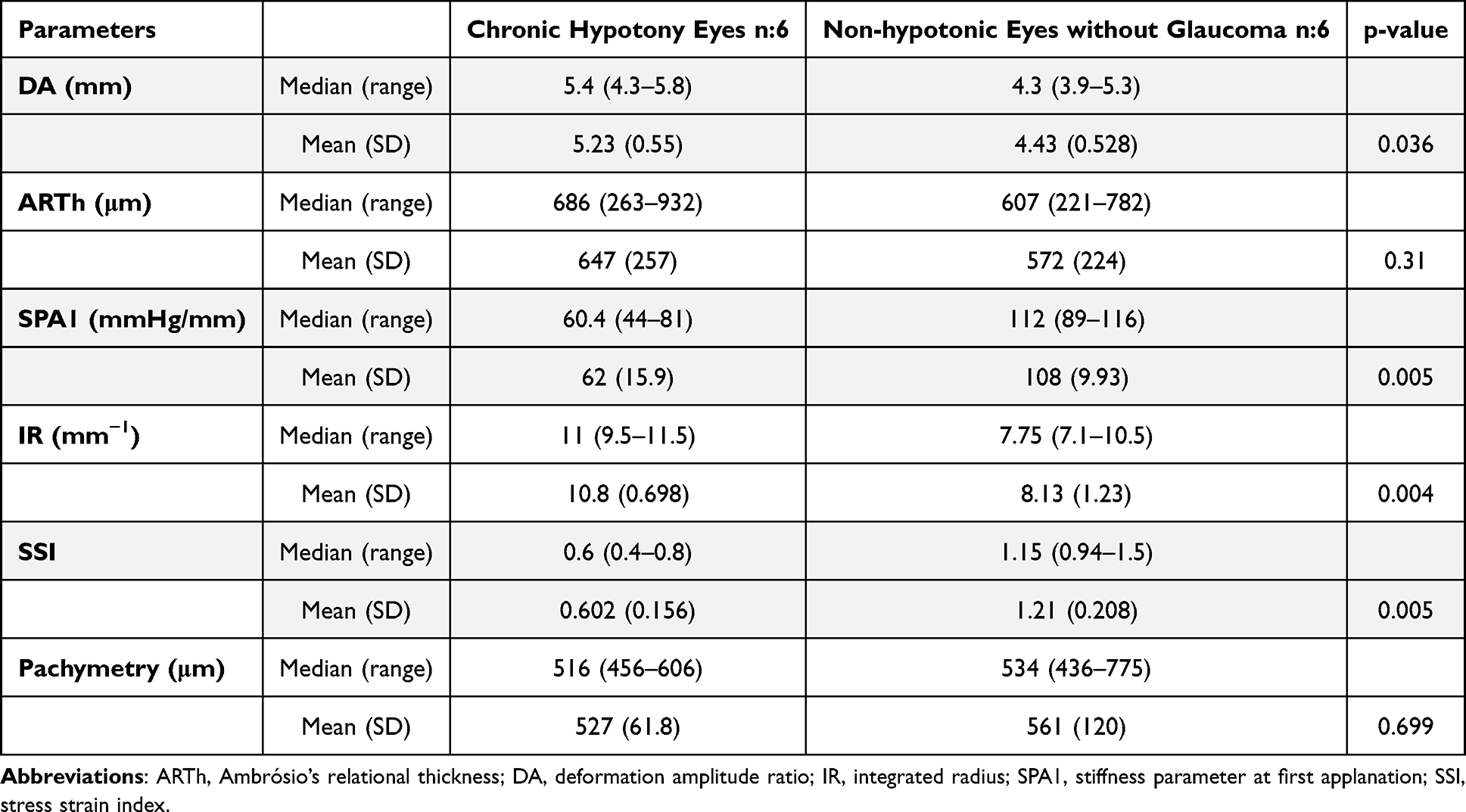 |
Table 4 Biomechanical Corneal (Corvis ST) Parameters Outcomes |
Table 5 compares the Biomechanical corneal parameters outcomes of chronic hypotony eyes with non-hypotonic eyes with glaucoma. The outcomes in IR and DA were higher and statistically significant in chronic hypotonic eyes compared to non-hypotonic eyes with glaucoma. SPA1 outcome was lower and statistically significant in chronic hypotonic eyes compared to non-hypotonic eyes with glaucoma.
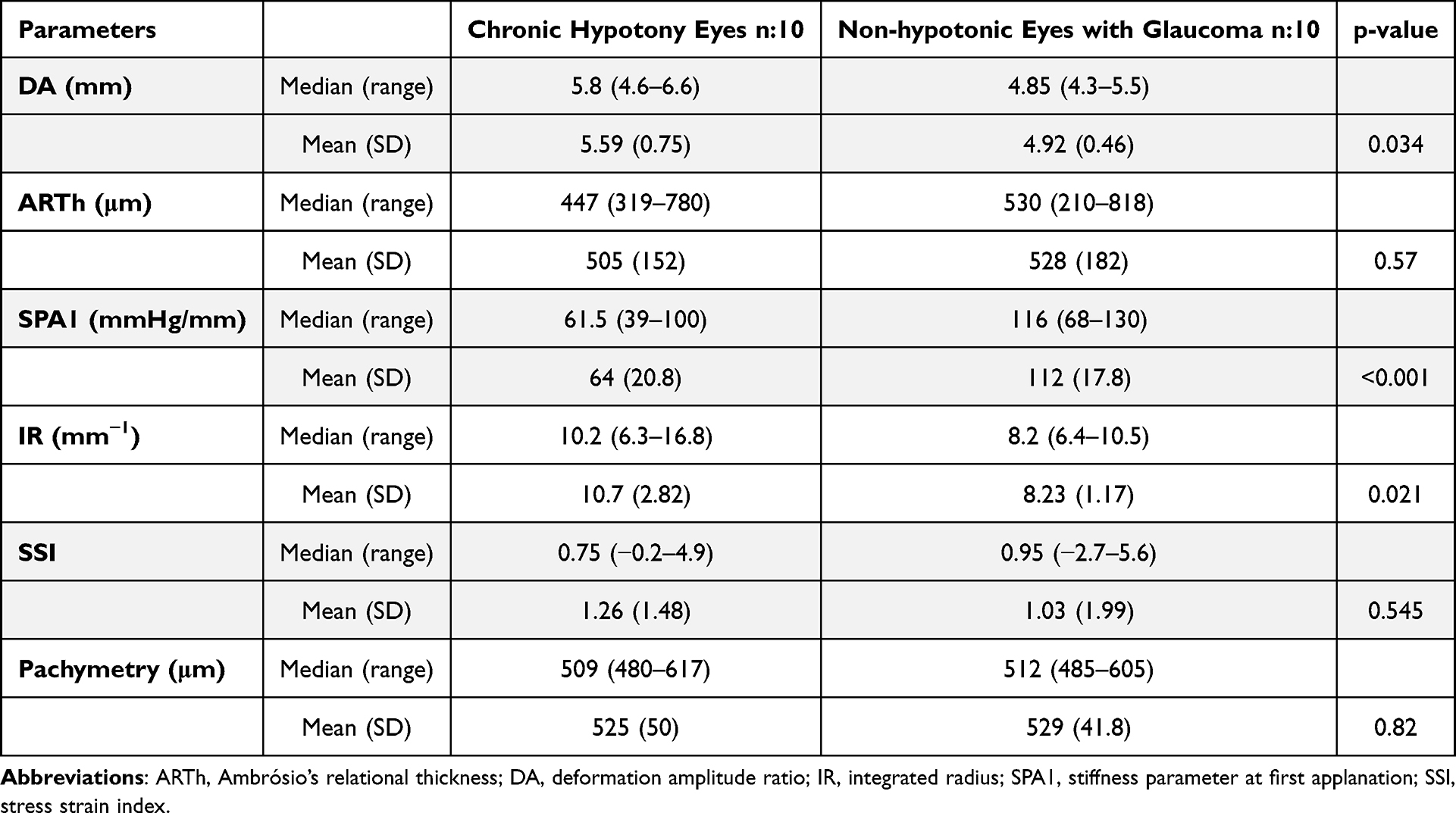 |
Table 5 Biomechanical Corneal (Corvis ST) Parameters Outcomes |
Macular folds were detected in 7 out of 16 (43.8%) chronic hypotonic eyes. Hence, 7 eyes were diagnosed as clinical hypotony. In these 7 eyes, 6 occurred in eyes that underwent deep sclerectomy, while 1 was associated with an Ahmed valve. The IOP [median (range)] in the 7 chronic hypotonic eyes with macular folds (clinical hypotony) was 5 (2–6) mmHg, and 4 (2–6) mmHg in the 9 chronic hypotonic eyes without macular folds (p-value=0.447). No macular folds were detected in non-hypotonic eyes. Table 6 shows the biomechanical corneal parameters outcomes evaluated by Corvis ST in clinical hypotonic eyes (with macular folds) and in nonclinical hypotonic eyes (without macular folds) (Figure 2).
 |
Table 6 Biomechanical Corneal (Corvis ST) Parameters Outcomes in Eyes With and Without Clinical Hypotony |
 |
Figure 2 Box plot representing the results of Corvis ST parameters in eyes with chronic hypotony, comparing eyes with clinical and nonclinical hypotony. Abbreviations: DA, deformation amplitude ratio; ARTh, Ambrósio’s relational thickness; SPA1, stiffness parameter at first applanation; IR, integrated radius; SSI, stress strain index. |
Discussion
To the best of our knowledge, our study is the first one to provide results on altered biomechanical corneal parameters in eyes diagnosed with chronic hypotonia (eyes with a low intraocular pressure during at least three months). As we suspected, chronic hypotonic eyes presented biomechanical corneal changes compared to eyes without chronic hypotonia. What we were not able to demonstrate was whether the biomechanical corneal changes observed in hypotonic eyes can predict increased risk of clinical manifestations such as hypotony maculopathy, which happens because of an increase in softness, elasticity and deformability of their scleras.
Patients with chronic ocular hypotony had a lower SPA1 and SSI, higher DA and IR values, indicating more deformable corneas and, therefore, less stiff corneas. These results are in accordance with results reported by other authors.5,13,20 Myopic eyes with a lower IOP presented a higher DA and less corneal stiffness, that is to say, a negative correlation between IOP and DA values.21 Moreover, based on Corvis parameters (parameters used in our study), eyes with primary open-angle glaucoma and lower IOP had softer corneas.22 In light of the above, corneal stiffness reduction seems to be a consequence of IOP lowering. This has been found in a prospective cohort including patients with different types of glaucoma in which a decrease in corneal stiffness was observed after IOP reduction.23
In animal models, Liu at al. showed that an increase in corneal stiffness was related with raised IOP due to reduced corneal compliance, which means a limitation of corneal capacity to accommodate sudden increases in intraocular volume, according to Hooke’s law.10 In human studies, stiffer corneas also correlate with greater increases in IOP after small volume variations. This has been investigated in patients receiving intravitreal injections of 0.05 mL bevacizumab for retinal disease, where those patients with a stiffer baseline cornea presented greater increases in post-injection IOP.24 These findings suggest that corneal stiffness is not only influenced by significant changes in IOP,23 but that variations in corneal biomechanical properties could temporarily affect IOP as well. Although Qassim et al found consistent evidence that stiffer corneas were associated with more rapid loss of retinal nerve fibers, it is yet to be further studied how do altered biomechanical properties of the cornea affect in IOP or glaucoma progression.14 To date, the only known factor affecting actual IOP remains aqueous humour production.
As we know, corneal stroma is a continuum of sclera21,25 and it has been suggested that corneal biomechanics reflect biomechanical properties of the posterior sclera.7 Macular folds are believed to be the result of scleral wall collapse under hypotonic conditions.26 A softer scleral wall could predispose to macular folds, and changes in corneal biomechanics can reflex scleral rigidity.13,21 Therefore, it would be very interesting to determine whether any corneal biomechanical parameters are altered in patients with macular folds in hypotonic eyes. These parameters could be predictive factors for macular folds development in eyes with hypotony, bringing us the possibility of selecting patients with statistical hypotonia and performing a more aggressive treatment with the purpose of preventing macular folds. It would help us identifying candidates for a more conservative approach such as a “wait and see”. Our results suggest a higher value of SSI in patients with macular folds compared to statistical hypotonia eyes, but no statistical significance was achieved, this could be explained by an insufficient sample size and open new horizons for further research.
This study may have some limitations. The study design and the small sample size could overestimate or underestimate the results found. Likewise, the different treatments used previously in case of chronic hypotonic eyes or non-hypotonic eyes could also influence the results. Another limitation is that the control group (non-hypotonic eyes) includes both patients diagnosed with glaucoma (n = 10) and patients without glaucoma (n = 6). It has been discovered that glaucoma eyes have altered biomechanical properties27 and thus may act as a confounder variable. Also, different types of glaucoma may change the pattern of altered biomechanical properties.27 We have tried to provide evidence on this issue on Table 4 and Table 5 which shows the results by “non-hypotonic eyes and glaucoma” (n = 10) and “non-hypotonic eyes without glaucoma” (n = 6). Also, the range measurement of IOP of the Corvis ST device is 6–60 mmHg and thus biomechanical parameters that include IOP in their calculation (SPA1) may include systematic error in eyes with IOP lower than 6. The lack of consensus on which parameters are ideal for studying the biomechanical properties of the cornea, and the lack of normal ranges for these parameters or which are the ranges for defining hypotony, pose as a limitation and arises new objectives for future research. The cross-sectional design prevents us from knowing whether the altered parameters are simply the consequence of hypotonia or are also part of the cause of hypotonia or from predisposed eyes with inherently softer corneas. A single-center study could also be a drawback for generalizing the results found.
Conclusions
Chronic hypotonic eyes (eyes with a low intraocular pressure) present biomechanical corneal changes in comparison with non-hypotonic eyes. The altered parameters were deformation amplitude ratio, stiffness parameter at first applanation, stress-strain index and Ambrósio’s relational thickness parameters. These changes in corneal biomechanics in chronic hypotony could reflect softer, more elastic and deformable scleras and thus higher risk for macular folds. Further research is needed in order to understand better the clinical implications of altered biomechanical corneal parameters and help improving ocular hypotonia management as well.
Abbreviations
AH, aqueous humour; ARTh, Ambrósio’s relational thickness; DA, deformation amplitude ratio; IOP, intraocular pression; IR, integrated radius; OCT, optical coherence tomography; SD, standard deviation; SPA1, stiffness parameter at first applanation; SSI, stress strain index.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. It is funded by the investigators own personal funds, who received no economic compensation for carrying out the study.
Disclosure
Jordi Loscos-Arenas and Sebastian Videla are co-senior authors for this study. The authors declare no conflict of interest related with this project.
References
1. Okonkwo ON, Tripathy K. Ocular hypotony. In: StatPearls. StatPearls Publishing; 2024.
2. Wang Q, Thau A, Levin AV, Lee D. Ocular hypotony: a comprehensive review. Surv Ophthalmol. 2019;64(5):619–638. doi:10.1016/j.survophthal.2019.04.006
3. Leen MM, Mills RP. Prevention and management of hypotony after glaucoma surgery. Int Ophthalmol Clin. 1999;39(3):87–101. doi:10.1097/00004397-199903930-00009
4. Toris CB, Pederson JE. Aqueous humor dynamics in experimental iridocyclitis. Invest Ophthalmol Vis Sci. 1987;28(3):477–481.
5. Aoki S, Asaoka R, Fujino Y, Nakakura S, Murata H, Kiuchi Y. Comparing corneal biomechanic changes among solo cataract surgery, microhook ab interno trabeculotomy and iStent implantation. Sci Rep. 2023;13(1):19148. doi:10.1038/s41598-023-46709-5
6. Kotecha A. What biomechanical properties of the cornea are relevant for the clinician?. Surv Ophthalmol. 2007;52(Suppl 2):S109–114. doi:10.1016/j.survophthal.2007.08.004
7. Congdon NG, Broman AT, Bandeen-Roche K, Grover D, Quigley HA. Central corneal thickness and corneal hysteresis associated with glaucoma damage. Am J Ophthalmol. 2006;141(5):868–875. doi:10.1016/j.ajo.2005.12.007
8. Brown KE, Congdon NG. Corneal structure and biomechanics: impact on the diagnosis and management of glaucoma. Curr Opin Ophthalmol. 2006;17(4):338. doi:10.1097/01.icu.0000233951.01971.5b
9. Salouti R, Bagheri M, Shamsi A, Zamani M, Ghoreyshi M, Nowroozzadeh MH. Corneal parameters in healthy subjects assessed by corvis ST. J Ophthalmic Vis Res. 2020;15(1). doi:10.18502/jovr.v15i1.5936
10. Liu J, He X. Corneal stiffness affects iop elevation during rapid volume change in the eye. Invest Opthalmol Vis Sci. 2009;50(5):2224. doi:10.1167/iovs.08-2365
11. Elhusseiny AM, Scarcelli G, Saeedi OJ. Corneal biomechanical measures for glaucoma: a clinical approach. Bioengineering. 2023;10(10):1108. doi:10.3390/bioengineering10101108
12. Bouchikh-El Jarroudi R, Romera-Romero P, Botella-Garcia J, Loscos-Arenas J. Multidisciplinary approach on the management of glaucoma: the role of corneal biomechanics. Arch Soc Esp Oftalmol. 2024. doi:10.1016/j.oftale.2024.10.008
13. Martinez-Sánchez MI, Bolívar G, Dastiridou A, Escámez P, Teus MA. Predictive value of dynamic corneal response parameters evaluated with scheimpflug high-speed video (Corvis ST) on the visual field progression in prostaglandin treated ocular hypertension and open-angle glaucoma patients. Ophthalmol Ther. 2023;12(6):3177–3186. doi:10.1007/s40123-023-00810-0
14. Qassim A, Mullany S, Abedi F, et al. Corneal stiffness parameters are predictive of structural and functional progression in glaucoma suspect eyes. Ophthalmology. 2021;128(7):993–1004. doi:10.1016/j.ophtha.2020.11.021
15. Kaushik S, Pandav SS. Ocular Response Analyzer. J Curr Glaucoma Pract. 2012;6(1):17–19. doi:10.5005/jp-journals-10008-1103
16. Hong J, Xu J, Wei A, et al. A new tonometer—the corvis st tonometer: clinical comparison with noncontact and Goldmann applanation tonometers. Invest Ophthalmol Vis Sci. 2013;54(1):659–665. doi:10.1167/iovs.12-10984
17. Wu N, Chen Y, Sun X. Association between ocular biomechanics measured with corvis ST and glaucoma severity in patients with untreated primary open angle glaucoma. Transl Vis Sci Technol. 2022;11(6):10. doi:10.1167/tvst.11.6.10
18. Khalil R, Dias KOM, Sutaria A, Shah D, Bokre D, Petrushkin H. Treatment options for chronic hypotony: a scoping review protocol. BMJ Open. 2024;14(12):e085968. doi:10.1136/bmjopen-2024-085968
19. Eliasy A, Chen KJ, Vinciguerra R, et al. Determination of corneal biomechanical behavior in-vivo for healthy eyes using corvis st tonometry: stress-strain index. Front Bioeng Biotechnol. 2019;7:105. doi:10.3389/fbioe.2019.00105
20. Wang X, McAlinden C, Zhang H, et al. Assessment of corneal biomechanics, tonometry and pachymetry with the Corvis ST in myopia. Sci Rep. 2021;11(1):3041. doi:10.1038/s41598-020-80915-9
21. Yu AY, Shao H, Pan A, et al. Corneal biomechanical properties in myopic eyes evaluated via Scheimpflug imaging. BMC Ophthalmol. 2020;20(1):279. doi:10.1186/s12886-020-01530-w
22. Miki A, Maeda N, Ikuno Y, Asai T, Hara C, Nishida K. Factors associated with corneal deformation responses measured with a dynamic scheimpflug analyzer. Invest Ophthalmol Vis Sci. 2017;58(1):538–544. doi:10.1167/iovs.16-21045
23. Xu Y, Ye Y, Chen Z, et al. The impact of intraocular pressure changes on corneal biomechanics in primary open-angle glaucoma. Am J Ophthalmol. 2024;269:216–225. doi:10.1016/j.ajo.2024.08.027
24. Dackowski EK, Moon JY, Wang J, Shrivastava A, Schultz JS. The relationship between corneal biomechanics and intraocular pressure dynamics in patients undergoing intravitreal injection. J Glaucoma. 2021;30(5):451–458. doi:10.1097/IJG.0000000000001833
25. McBrien NA, Gentle A. Role of the sclera in the development and pathological complications of myopia. Prog Retin Eye Res. 2003;22(3):307–338. doi:10.1016/S1350-9462(02)00063-0
26. Costa VP, Arcieri ES. Hypotony maculopathy. Acta Ophthalmol Scand. 2007;85(6):586–597. doi:10.1111/j.1600-0420.2007.00910.x
27. Liu MX, Zhou M, Li DL, Dong XX, Liang G, Pan CW. Corneal biomechanics in primary open angle glaucoma and ocular hypertension: a systematic review and meta-analysis. J Glaucoma. 2023;32(3):e24–e32. doi:10.1097/IJG.0000000000002170
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.