Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Biochemical Parameters in Cognitive Functions
Authors Popiolek AK ![]() , Chyrek-Tomaszewska A
, Chyrek-Tomaszewska A ![]() , Stachowicz-Karpińska A
, Stachowicz-Karpińska A ![]() , Bieliński MK
, Bieliński MK ![]() , Borkowska A
, Borkowska A ![]()
Received 14 June 2020
Accepted for publication 8 September 2020
Published 27 October 2020 Volume 2020:16 Pages 2479—2489
DOI https://doi.org/10.2147/NDT.S267673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Alicja Katarzyna Popiołek,1,2 Aleksandra Chyrek-Tomaszewska,1,2 Agnieszka Stachowicz-Karpińska,1,2 Maciej Kazimierz Bieliński,1,2 Alina Borkowska1
1Department of Clinical Neuropsychology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Bydgoszcz, Poland; 2Department of Vascular and Internal Diseases, Jan Biziel University Hospital No. 2 in Bydgoszcz, Bydgoszcz, Poland
Correspondence: Alicja Katarzyna Popiołek
Department of Clinical Neuropsychology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Skłodowskiej-Curie St. 75, Bydgoszcz 85-094, Poland
Tel/Fax +48 52 585 37 03
Email [email protected]
Abstract: Cognitive impairment is a common disease. Many studies attempt to explain the mechanisms of these dysfunctions formation, including correlations between cognitive functions and biochemical parameters. Scientists search for substances that would be indicators of cognitive functions and which could be determined in the cerebrospinal fluid or blood of the subjects. To date, they have isolated a few of such substances; however, research on their specificity, validity and the possibility of their use in diagnostics and prognostic assessment is still ongoing. However, there have been only few reports in the literature systematizing the existing knowledge on this subject, and they are mostly related to Alzheimer’s disease, not cognition in general, or referring only to a specific group of substances. This article discusses the most important biochemical exponents of cognitive functions.
Keywords: cognitive functions, biochemical markers, neuropsychology
Introduction
Cognitive dysfunction is an increasingly prevalent condition; incidence rate after age 65 rises exponentially. It is connected with both the physiological aging and various somatic disorders. Numerous studies seek to explain the mechanism of these dysfunctions, including interactions between them and biochemical parameters.
Given the physiology of cognitive functions, it would seem that the best markers for estimating these functions ought to be the neurotransmitters that are engaged in their creation. Impaired cognitive functions are directly related to neurotransmission disorders. Many studies support this intuition.1,2 However, under physiological conditions, the neurotransmitters in question are produced in nervous tissue, and their level in blood serum or cerebrospinal fluid (CSF) does not always correspond to their level in the brain.3 Therefore, to appraise their concentration, the rodent, postmortal or special neuroimaging experimentations must be conducted. However, such procedures are costly and hardly accessible. Scientists are thus searching for other substances that would be an indicator of cognitive functions, and be quickly detected in the CSF or blood.4 Hitherto several substances have been isolated; however, research on their specificity, validity and most importantly usefulness in diagnostics and prognosis are still ongoing. These substances are evaluated usually in subjects after stroke or craniocerebral trauma; less frequently in other disease entities not directly linked to brain damage.5
To put it simply, these substances can be divided into four groups6 (Figure 1): - inflammatory mediators – CRP, IL-1, IL-6, TNF-α, MBG;
 |
Figure 1 The most important biochemical parameters in cognitive functions. |
- neural tissue markers – S100B protein, NSE, GFAP, pNf-H, Nf-L, VILIP-1, T-tau, P-tau, beta-amyloid precursors;
- components of the coagulation and fibrinolysis systems – vWF, D-dimer, NSP; - others – BDNF, BNP/NT-proBNP, YKL40, sTREM2, NRGN and many others.
Inflammatory Mediators
Inflammation process is expressed by five features, proposed in ancient times by Celsus and Galen, that include redness, pain, increased warming, swelling and impaired functions. However, developing inflammation does not have to reveal in this fashion. There is a slight grade of subclinical inflammatory response, without the ordinary symptoms detailed above, with activation of the inflammatory cascade and increased biochemical indicators of inflammation.7 This process is related to age – is more demonstrable in older individuals and is called “inflammaging”. It is also accepted that this process may be associated with the development of illnesses that proceed with inflammation, such as atherosclerosis, diabetes, osteoporosis and Alzheimer’s disease (AD). Launching the anti-inflammatory response may have a defensive function.7 Many studies confirm the relationship between inflammation, understood in this way, and the development of many disorders, and – what is more important in this paper – cognitive impairment.8
C-reactive protein (CRP) is one of the acute phase proteins, engaged in the body’s immune response. For the wide availability and relatively low costs, with a high sensitivity of signage, it is a broadly used exponent of inflammation in a clinical practice. This protein is synthesized by the liver in response to inflammation. The increased concentration of hs-CRP (CRP determined by the high sensitivity method) is observed in people with obesity, diabetes, increased waist circumference or elevated LDL cholesterol. It is also believed that it plays an important role in the brain aging process, including the development of cognitive disorders.9–12
Chinese researchers conducted a meta-analysis of 170 studies comparing the level of various inflammatory exponents, including CRP, in healthy individuals and Alzheimer’s patients. It turned out that among subjects with Alzheimer’s dementia, CRP values were significantly higher than in healthy ones (p <0.05).13 Also in many other disease entities, CRP levels correlates with cognitive impairment – in patients with chronic kidney diseases, depression, schizophrenia, bipolar disorder, Parkinson’s disease, but also in healthy individuals.14,15
Weinstein et al conducted long-term observation of cognitive functions in subjects with chronic ischemic heart disease. They showed that the previously observed higher CRP level was associated with worse cognitive functions assessed several years later.16 Interesting studies were also carried out by Corlier and companions who, in a 9-year follow-up, evaluated the thickness of the cerebral cortex (measured in several places considered crucial for cognitive functions, inflammation and physical activity) and compared results of these measurements with the level of CRP and metabolic risk factors. According to the hypothesis, people with a higher baseline CRP had significantly thinner cerebral cortex in four regions crucial for the development of Alzheimer’s dementia in the 9th year of study. Interestingly, scientists have not observed such a direct link between metabolic risk items and brain structure.9
Interleukins (IL) belong to proteins and the cytokines that are involved in the body’s immune and hematopoietic processes. They play a role in the communication between white blood cells and originally mainly this role was seen. However, it is now recognized that they also communicate with other types of cells, not just leukocytes. This is a heterogeneous group in terms of structure and function, which is why it is divided into several subgroups. It is considered that IL-6 and IL-1 (α and β) are the most significant for acute phase regulation. Proteins from the IL-1 family show activity on almost all types of immunocompetent cells. IL-1β has the ability to pass from peripheral blood through the blood-brain barrier to the brain system. There, by stimulating macrophage-like cells, it induces the production of further interleukins. On the other hand, brain structures (such as the hippocampus) obtain signal through specific receptors for these interleukins. Persistent inflammation may thus modulate brain functions.17,18 Studies have proved that elevated stage of some interleukins is related with poorer cognitive functioning.19–21 For instance, levels of IL-6 are raised among patients with dementia and the ones with cognitive deficits in the course of cardiovascular, rheumatic or liver diseases.22 The increased IL-6 concentration corresponds with the deterioration of memory and the severity of the symptoms of chronic fatigue syndrome.18,21 Meyers et al studied patients with acute myeloid leukemia and myelodysplastic syndromes and indicated a negative correlation between IL-6 level and memory, and a positive correlation between IL-8 level and memory.23
Italiani and colleagues demonstrated similar relationships for cytokines and receptors in the IL-1 family – they observed elevated levels of both IL-1α and IL-1β in individuals with AD.24 Other researchers note the probable importance of these interleukins for the development of cognitive declines in bipolar disorder and after cerebral trauma.25,26
Scientific reports on IL-1 function are not consistent. Objective research is providing more and more evidence confirming that IL-1 is essential for memory development. Many publications also confirm their participation in opposite processes – through disturbing the consolidation of memory and hippocampal-dependent memory. An attempt to reconcile these discoveries are the results got by Goshen and colleagues, according to which exogenous IL-1β in low concentrations improves remembrance, but disturbs it in high concentrations. It seems, therefore, that it may take part in both these opposing processes and the effect of its action depends on its concentration.27
Tumor necrosis factor α (TNF-α) is a pro-inflammatory cytokine, mainly produced by monocytes and macrophages. Both forms of TNF-α – soluble and anchored – exhibit biological activity. The cells they stimulate produce a broad spectrum of cytokines, triggering a cascade of events both inducing and inhibiting the inflammatory response. This leads to mitochondrial dysfunctions, enhanced oxygen free radical production, increased proapoptotic protein generation (Bax and p53), release of cytochrome c from mitochondria, activation of caspase 3, and induction of apoptosis and cell death. In the clinical course, this may manifest cognitive impairment, especially when the above processes occur in brain cells.28 Many studies confirm the relationship between TNF-α (or its receptors) and cognitive deterioration in various disease entities.15,23,28 Increase in TNF-TNFR2 receptor concentration was observed among women receiving chemotherapy for breast cancer, which correlated with memory impairment in these cases.29 It has also been proven that treatment with TNF-α inhibitors (taken in various disease entities) is associated with the improvement of cognitive and behavioral functions.30,31
There are, however, opposite opinions – Polish researchers in a meta-analysis note that subjects with schizophrenia function better cognitively at higher levels of TNF-α.14 In the same meta-analysis, they remark that TNF-α, promotes the development of cognitive disorders among patients with bipolar disorder.14
Marinobufagenin (MBG) is a relatively new substance that seems to have a high diagnostic potential.5 It is released due to brain damage during trauma. Its increased concentration is also observed in preeclampsia and eclampsia.32 It is involved in the initiation and maintenance of the inflammatory response, secondary to increasing the permeability of brain endothelial cells and deterioration of brain functions, including cognitive functions.33
Markers of Brain Tissue Damage
Biomarkers of brain tissue damage may have a glial origin (eg, S100B protein, glial fibrillary acidic protein) or a neuronal origin (eg, tau protein, neuron special enolase). The most important of them are discussed below.
S100B protein is one of the oldest and well-tested biomarkers of brain damage. It occurs in astrocytes and it belongs to the group of calcium-binding proteins, which participate in the regulation of calcium concentration inside the cell.
It was proved that its serum concentration correlates with abnormalities in neuroimaging studies such as size and type of brain damage.34 It was also observed that it is associated with cognitive impairment, mainly in terms of attention, memory and speed of information processing.34,35 Many studies confirm its usefulness – eg, in assessing prognosis after carotid surgery, after thrombolysis, resuscitation or coronary artery bypass.36–39
On the other side, some studies emphasize the low specificity of this protein and its occurrence outside the central nervous system. This may hinder the interpretation of results and undermine their credibility.40
Neuron special enolase (NSE) is an enzyme with glycolytic activity. It occurs mainly in the cytoplasm of nerve cells, but it has also been found in erythrocytes, thrombocytes and endocrine cells. It is scattered into the extracellular space, when the cell is damaged. Its blood concentration after 72 hours since cerebral injury correlates with unfavorable prognosis.41
In 2005 Anand and Stead conducted a meta-analysis of 12 studies, which evaluated NSE in patients with a stroke (a total of 594 patients were examined). They noticed a higher NSE level in the patients’ serum in comparison to the control group. Nevertheless, it did not correlate with the clinical status of patients; also its relationship with the extent of a stroke was unclear.42 Moreover, researchers from Harvard Medical School observed that NSE level in patients undergoing cardiac surgery correlates better with cognitive deficiency than the S100B protein. Similar dependency was also noticed for tau protein which is described below.43 In addition, NSE level may be elevated in other clinical situations, not directly related to brain damage.38,39,44
Glial fibrillary acidic protein (GFAP), similar as the S100B protein, is found in astroglia; it is a part of the astrocyte cytoskeleton. Numerous studies prove that this is a good indicator of brain damage.45–47 Papa and co-authors noticed that GFAP levels were significantly different in patients after head injuries and in patients after other traumas without head injury.48 Some studies have shown correlations with distant results after cerebral trauma, but reports in this case are not consistent.46,49 Results of many studies pointed out that GFAP is a superior marker to others (in terms of correlation with imaging studies, with cognitive functions or assessment of prognosis).49,50 Herrmann et al compared results of biochemical tests (of protein S100B and GFAP) with results of neuroimaging tests and clinical condition after strokes at the time of admission to hospitals and during four following days of hospitalization.50 It turned out that the constellation of these proteins’ levels correlated with stroke type and prognosis. Particularly characteristic was the system of proteins in lacunar stroke, in which high GFAP levels were observed at the time of admission to hospital with its gradual decrease to the physiological level on the second day. Such dynamic of changes was associated with better prognosis. GFAP turned out to be a very sensitive marker, especially at small cerebral infarcts.50
Phosphorylated neurofilament heavy chain (pNf-H) and neurofilament light chain (NfL) are components of neurofilaments – specific proteins in the cytoskeleton of neurons, found mainly in myelinated axons. They are released into the CSF and then into the blood during axon damage. Their concentration in CSF is elevated after brain injury.51,52 In studies conducted among children, who experienced brain traumas, the level of Nf-H correlated with the severity of brain damage and distant results.53 Its elevated levels are also observed in patients undergoing chemotherapy for breast cancer or in postoperative delirium.54,55 Research to date suggests that also plasma NfL may be a good biomarker of cognitive function in patients with AD and in people with Parkinson’s disease and other neurological disorders.51,56,57
Visinin-like protein 1 (VILIP-1) belongs to a group of neuronal calcium sensors and it is a marker of cognitive deterioration. Previously, it was only evaluated in the CSF, but recently it is also tested in blood serum.58 It has also been proven to affect AD, what is probably associated with impaired calcium homeostasis and apolipoprotein E in CSF.59,60 This exact mechanism was described by Polish researchers who noticed that VILIP-1 affects intercellular neuronal signaling pathways in the central nervous system (cyclic nucleotide cascades and nicotinergic signaling), leading to neuronal loss.61 Its increased concentration is observed among others, after ischemic stroke and after cerebral trauma.58
Tau Protein (T-tau and P-tau) is an axonal stabilizing microtubule protein found in both the brain and the spinal cord.62 Its phosphorylation is crucial in regulating tau function at different neuronal locations, eg, stability of the neuronal cytoskeleton, axonal transport or cell signaling.63 However, excessive phosphorylation of tau protein is associated with neuron death and it occurs in neurodegenerative diseases, postoperative cognitive impairment, cerebral trauma, and cerebral ischemia.62 Therefore, total tau (T-tau) in CSF is thought to be a general marker of axonal damage in the brain tissue. Phosphorylated tau (P-tau) then is suggested to be a more specific marker for neurodegenerative tauopathies, including AD.64
T-tau in CSF is also a prognostic factor for increased intracranial pressure and clinical status of patients after cerebral trauma.65 While the level of t-tau in the blood after cerebral injury was significantly increased, it did not correlate with the clinical state.65
Beta-amyloid precursors. Beta-amyloid is a well-known component of amyloid plaques, found in AD. It has been noticed that also after craniocerebral trauma there is a rapid increase in the amount of amyloid plaques in the brain. It has also been proven that such trauma is a risk factor for AD. It is believed that it is probably associated with impaired beta-amyloid catabolism and an increase in the concentration of its precursors.66 Until recently, beta-amyloid assessment was only possible using specialized neuroimaging methods (positron emission tomography) or assessment of its concentration in the CSF. Latest reports indicate the isolation of beta-amyloid precursors from blood (APP)669–711/amyloid-β (Aβ)1–42 and Aβ1-40/Aβ1-42). It was estimated that their level correlates with the concentration of beta-amyloid in CSF and in neuroimaging studies.67 It should be emphasized that the plasma level of amyloid-β strongly correlates with the risk of developing dementia.57
Components of the Coagulation and Fibrinolysis Systems
The von Willebrand factor (vWF) is a plasma glycoprotein involved in the process of primary as well as secondary hemostasis. It is responsible for protecting factor VIII from degradation by forming a complex with it; also allowing platelets to adhere to the collagen at the place of damage. Moreover, research has shown that VWF is involved in the pathogenesis of an early brain damage after an injury.68 Higher levels of vWF are also observed in patients with ischemic stroke than in the control group. Such a dependency was observed in the acute phase of stroke and three months after the episode.69 VWF concentration also correlates with cognitive functions and untimely death of patients.70,71
D-dimers are fibrin degradation products. It has been proven that their higher concentration correlates with cognitive deterioration and with an increased risk of stroke and cardiovascular events.70,72 However, it should be emphasized, that it is a marker with very low specificity. That is why possibilities of its use in research and diagnostics are limited. Increased levels of D-dimers are observed, among others, in venous thromboembolism, intravascular coagulation syndrome, after injuries and operations, in stroke, inflammation, cancer, pregnancy, coronary artery disease, atrial fibrillation and aortic diseases.73
Neuroseprin (NSP) is an inhibitor of tissue plasminogen activator. It participates in brain development and plays a neuroprotective role.74 Although this is a relatively new marker of brain damage, and its meaning is not fully known, research using it seems to be promising. During brain damage in the course of ischemic stroke, its level is higher than among the subjects from the control group. Moreover, it was proved that the higher concentration of this neuroprotective marker was, the better the long-term results were obtained.75 Its elevated level was also observed by Polish researchers among patients after cardiac surgery, what may be related to perioperative brain damage that occurs during such procedures.5
Other Biochemical Markers
Brain-derived neurotrophic factor (BDNF) is a protein belonging to the group of neurotrophins – their role is to regulate short term and prolonged potentials, which stimulate and inhibit various regions of the brain, thus affect the creation of long-term memory.76 BDNF is a strong modulator of synaptic transmission, it also participates in the processes of maturation, differentiation and apoptosis of nerve cells, contributing to the formation of the central nervous system in embryogenesis and the plasticity of synaptic connections in the mature brain.77,78 Numerous studies prove that BDNF plays a key role in the long-term potentiation of the hippocampus (LTP), which underlies learning and memory processes.79 In animal tests, BNDF has been shown to have neuroprotective effects in subjects after ischemic-hypoxic episodes. It has also been proven that deficiencies in BDNF signaling contribute to the pathogenesis of many different diseases and disorders, such as depression and AD.79
Brain natriuretic peptide is a protein belonging to natriuretic peptides. There are also atrial natriuretic peptide (ANP) and natriuretic peptides type C and D (CNP, DNP). NT-proBNP is the N-terminal fragment of its prohormone – BNP. In clinical practice, they are routinely used to diagnose heart failure. They are produced, among others, by cardiomyocytes, in response to an increase in their tension caused by increased preload or afterload. They cause the increase of diuresis and natriuresis, have sympatholytic activity, inhibit the RAA system and also reduce the activity of baroreceptors. All of these activities lead to the reduction of blood pressure and the reduction of pre- and afterload of the ventricles. BNP and NT-proBNP are also thought to be sensitive indicators of brain damage that may be useful in clinical assessment, prognosis, and risk of death after stroke. It has been shown that increased BNP plasma levels in patients after a stroke incident can predict mortality with sensitivity and specificity close to 75%.80 In another analysis, the specificity and sensitivity in predicting death were 88.9% and 98.2%.81 Interesting studies on a large population were carried out by German scientists. They examined 419 patients with mild cognitive impairment and 1206 people without cognitive impairment and they correlated cognitive testing results with NT-proBNP levels. It turned out that cognitive functions correlated, regardless of other factors, with the level of this marker.82 A similar relationship in the five-year observation of patients after 85 years of age was observed by Dutch scientists.83
Discussion
The most relevant information, summarizing this article, is outlined in Table 1.
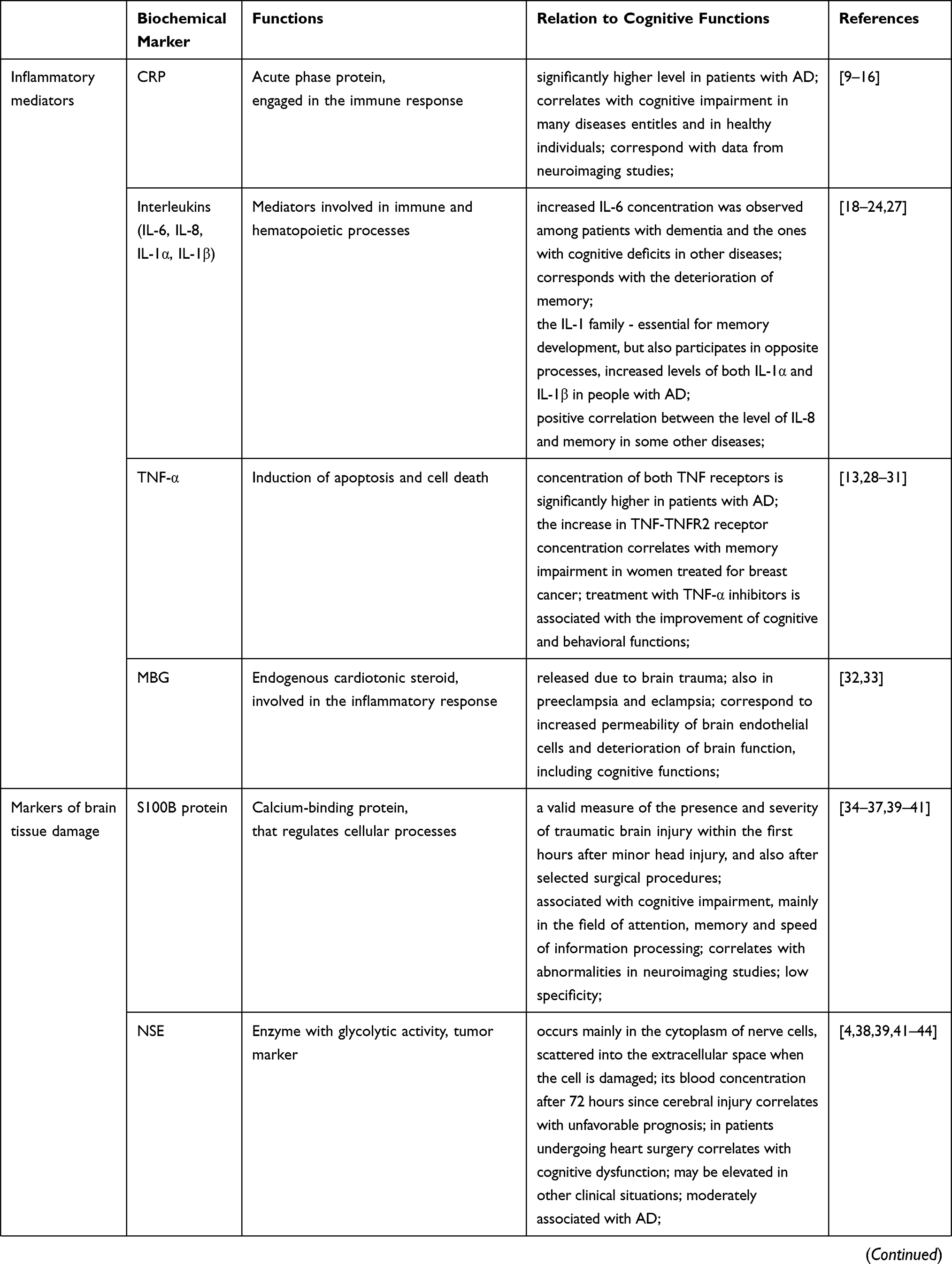 | 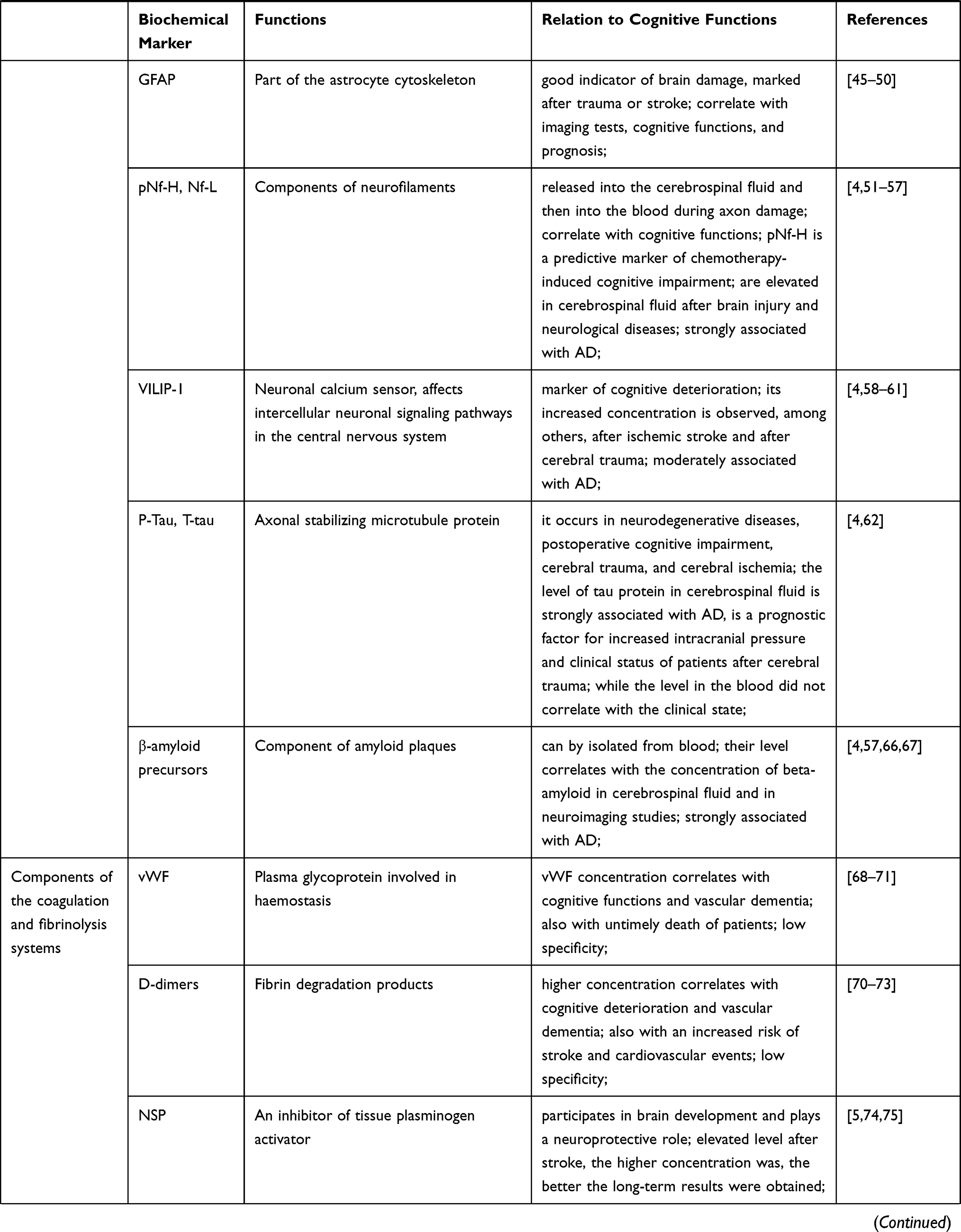 | 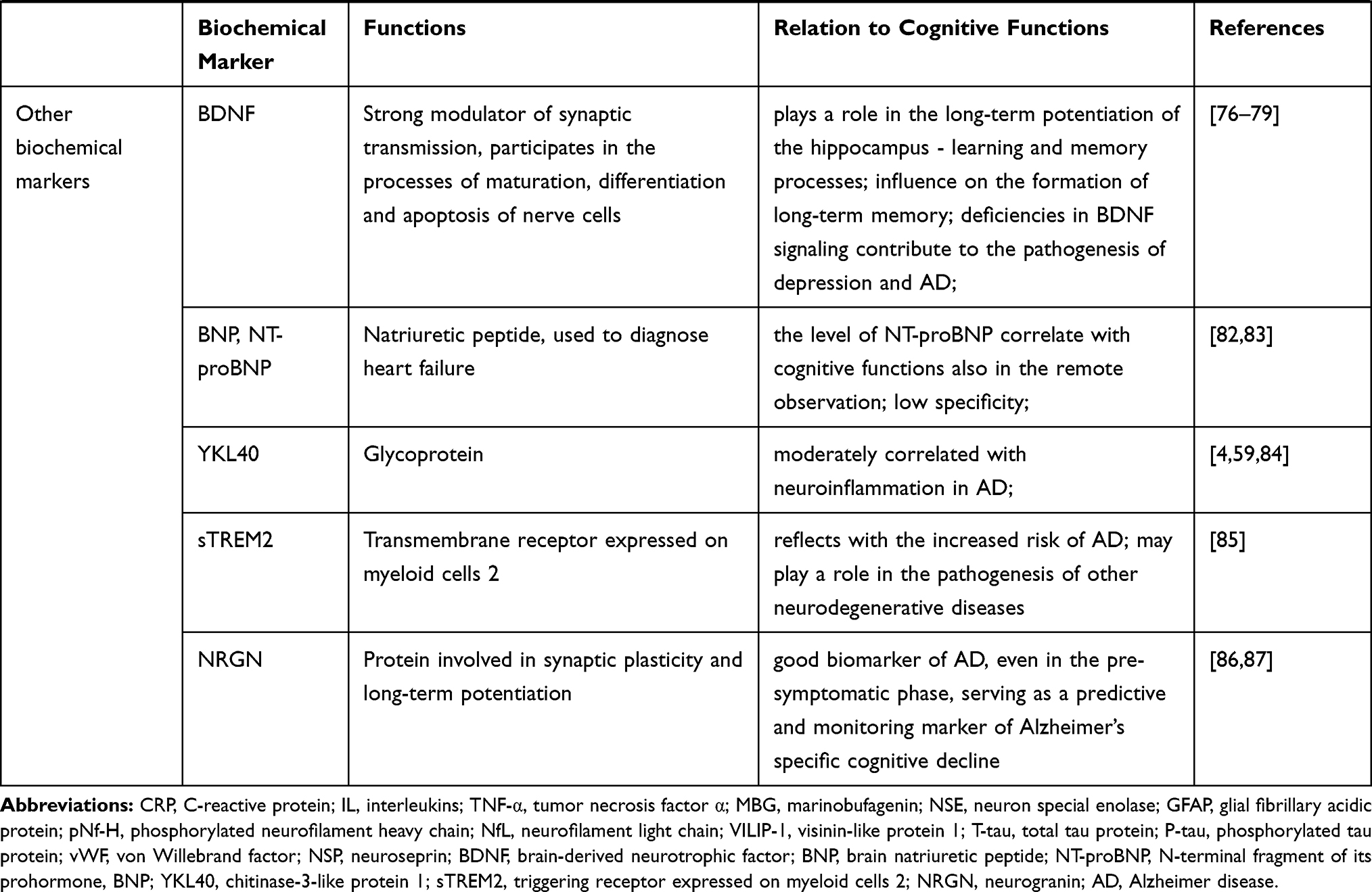 |
Table 1 The Most Important Biomarkers of Cognitive Performance, Their Functions and Relation to Cognitive Functions |
It should be emphasized that the content of the article, based on numerous citations, indicates little significant clinical and scientific usefulness of factors from groups of inflammatory mediators and coagulation/fibrinolysis components. Testing the level of markers of nerve tissue damage, in particular Tau Protein (T-tau and P-tau), is much more valuable. The existing evidence, in line with the current biochemical research on the basis of cognitive impairment, concerns many parameters. However, research using biochemical markers in diseases with accompanying cognitive dysfunctions other than Alzheimer’s dementia seems to be particularly promising.
However, it should be also emphasized that in this report we have not exhausted the topic of biochemical parameters of cognitive functions. There are more substances that should be pointed out for completeness. These include chitinase-3-like protein 1 (YKL-40), a glycoprotein correlated with neuroinflammation in AD.59,84 Another marker, triggering receptor expressed on myeloid cells 2 (sTREM2) reflects with increased risk of AD and also may play a role in the pathogenesis of other neurodegenerative diseases.85 Neurogranin (NRGN) is a postsynaptic protein involved in synaptic plasticity and long-term potentiation. It appears to be a good biomarker of AD, even in the pre-symptomatic phase, serving as a predictive and monitoring marker of Alzheimer’s cognitive decline.86,87 Besides, new reports on this issue still appear.88,89
Conclusion
In summary, more and more, is known about substances that correlate with cognitive dysfunctions. Despite this, there is a lack of convincing data indicating the clear association of any substance with the assessment of cognitive functions that would be sensitive and specific enough to be able to use it in practice. Further research is needed to deepen existing knowledge on this subject.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Garcia-Esparcia P, Diaz-Lucena D, Ainciburu M, et al. Glutamate transporter GLT1 expression in alzheimer disease and dementia with lewy bodies. Front Aging Neurosci. 2018;10:122. doi:10.3389/fnagi.2018.00122
2. Volk L, Chiu S-L, Sharma K, Huganir RL. Glutamate synapses in human cognitive disorders. Annu Rev Neurosci. 2015;38(1):127–149. doi:10.1146/annurev-neuro-071714-033821
3. Bak LK, Schousboe A, Waagepetersen HS. The glutamate/GABA-glutamine cycle: aspects of transport, neurotransmitter homeostasis and ammonia transfer. J Neurochem. 2006;98(3):641–653. doi:10.1111/j.1471-4159.2006.03913.x
4. Olsson B, Lautner R, Andreasson U, et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: a systematic review and meta-analysis. Lancet Neurol. 2016;15(7):673–684.
5. Szwed K, Słomka A, Pawliszak W, et al. Novel markers for predicting type 2 neurological complications of coronary artery bypass grafting. Ann Thorac Surg. 2020;110(2):599–607.
6. Gliński P, Rak-Pasikowska A, Czapla A, Sapa-Wojciechowska A. Usefulness of selected laboratory markers in stroke diagnosis. Diagn Lab. 2018;54(4):275–284.
7. Giunta B, Fernandez F, Nikolic WV, et al. Inflammaging as a prodrome to Alzheimer’s disease. J Neuroinflammation. 2008;5:51.
8. Tegeler C, O’Sullivan JL, Bucholtz N, et al. The inflammatory markers CRP, IL-6, and IL-10 are associated with cognitive function-data from the Berlin Aging Study II. Neurobiol Aging. 2016;38:112–117.
9. Corlier F, Hafzalla G, Faskowitz J, et al. Systemic inflammation as a predictor of brain aging: contributions of physical activity, metabolic risk, and genetic risk. Neuroimage. 2018;172:118–129.
10. Kuo H-K, Yen C-J, Chang C-H, Kuo C-K, Chen J-H, Sorond F. Relation of C-reactive protein to stroke, cognitive disorders, and depression in the general population: systematic review and meta-analysis. Lancet Neurol. 2005;4(6):371–380. doi:10.1016/S1474-4422(05)70099-5
11. Rosebud OR, Geda YE, Knopman DS, et al. Association of C-reactive protein with mild cognitive impairment Alzheimers Dement. Front Neurosci. 2009;5(5):398–405.
12. Noble JM, Manly JJ, Schupf N, Tang MX, Mayeux R, Luchsinger JA. Association of C-Reactive Protein With Cognitive Impairment. Arch Neurol. 2010;67(1):87–92. doi:10.1001/archneurol.2009.308
13. Shen X-N, Niu L-D, Wang Y-J, et al. Inflammatory markers in Alzheimer’s disease and mild cognitive impairment: a meta-analysis and systematic review of 170 studies. J Neurol Neurosurg Psychiatry. 2019;90(5):590–598. doi:10.1136/jnnp-2018-319148
14. Misiak B, Stańczykiewicz B, Kotowicz K, Rybakowski JK, Samochowiec J, Frydecka D. Cytokines and C-reactive protein alterations with respect to cognitive impairment in schizophrenia and bipolar disorder: A systematic review. Schizophr Res. 2018;192:16–29. doi:10.1016/j.schres.2017.04.015
15. Stenfors CUD, Jonsdottir IH, Magnusson Hanson LL, Theorell T. Associations between systemic pro-inflammatory markers, cognitive function and cognitive complaints in a population-based sample of working adults. J Psychosom Res. 2017;96:49–59. doi:10.1016/j.jpsychores.2017.03.010
16. Weinstein G, Lutski M, Goldbourt U, Tanne D. C-reactive protein is related to future cognitive impairment and decline in elderly individuals with cardiovascular disease. Arch Gerontol Geriatr. 2017;69:31–37. doi:10.1016/j.archger.2016.11.002
17. Singhal G, Jaehne EJ, Corrigan F, Toben C, Baune BT. Inflammasomes in neuroinflammation and changes in brain function: a focused review. Front Neurosci. 2014;8:315. doi:10.3389/fnins.2014.00315
18. Bower JE, Ganz PA, Irwin MR, Castellon S, Arevalo J, Cole SW. Cytokine genetic variations and fatigue among patients with breast cancer. J Clin Oncol. 2013;31(13):1656–1661. doi:10.1200/JCO.2012.46.2143
19. Mooijaart SP, Sattar N, Trompet S, et al. PROSPER Study Group. Circulating interleukin-6 concentration and cognitive decline in old age: the PROSPER study. J Intern Med. 2013;274(1):77–85. doi:10.1111/joim.12052
20. McAfoose J, Baune BT. Evidence for a cytokine model of cognitive function. Neurosci Biobehav Rev. 2009;33(3):355–366. doi:10.1016/j.neubiorev.2008.10.005
21. Wright CB, Sacco RL, Rundek TR, Delman JB, Rabbani LE, Elkind MSV. Interleukin-6 is associated with cognitive function: the Northern Manhattan Study. J Stroke Cerebrovasc Dis. 2006;15(1):34–38. doi:10.1016/j.jstrokecerebrovasdis.2005.08.009
22. Trapero I, Cauli CO. Interleukin 6 and cognitive dysfunction. Metab Brain Dis. 2014;29(3):593–608. doi:10.1007/s11011-014-9551-2
23. Meyers CA, Albitar M, Estey EE. Cognitive impairment, fatigue, and cytokine levels in patients with acute myelogenous leukemia or myelodysplastic syndrome. Cancer. 2005;104(4):788–793. doi:10.1002/cncr.21234
24. Italiani P, Puxeddu I, Napoletano S, et al. Circulating levels of IL-1 family cytokines and receptors in Alzheimer’s disease: new markers of disease progression? J Neuroinflammation. 2018;15(1):342. doi:10.1186/s12974-018-1376-1
25. Lotrich FE, Butters MA, Aizenstein H, Marron MM, Reynolds CF, Gildengers AG. The relationship between interleukin-1 receptor antagonist and cognitive function in older adults with bipolar disorder. Int J Geriatr Psychiatry. 2014;29(6):635–644. doi:10.1002/gps.4048
26. Samatra DPG, Pratiwi NMD, Widyadharma IPE. High Il-1β Serum as a Predictor of Decreased Cognitive Function in Mild Traumatic Brain Injury Patients. Open Access Maced J Med Sci. 2018;6(9):1674–1677. doi:10.3889/oamjms.2018.390
27. Goshen I, Kreisel T, Ounallah-Saad H, et al. A dual role for interleukin-1 in hippocampal-dependent memory processes. Psychoneuroendocrinology. 2007;32(8–10):1106–1115.
28. Belarbi K, Jopson T, Tweedie D, et al. TNF-α protein synthesis inhibitor restores neuronal function and reverses cognitive deficits induced by chronic neuroinflammation. J Neuroinflammation. 2012;9(1):23. doi:10.1186/1742-2094-9-23
29. Pomykała KL, Ganz PA, Bower JE, et al. The association between pro-inflammatory cytokines, regional cerebral metabolism, and cognitive complaints following adjuvant chemotherapy for breast cancer. Brain Imaging and Behavior. 2013;7(4):511–523. doi:10.1007/s11682-013-9243-2
30. Ekert JO, Gould RL, Reynolds G, Howard RJ. TNF alpha inhibitors in Alzheimer’s disease: A systematic review. Int J Geriatr Psychiatry. 2018;33(5):688–694. doi:10.1002/gps.4871
31. Decourt B, Lahiri KD, Sabbagh MN. Targeting Tumor Necrosis Factor Alpha for Alzheimer’s Disease. Curr Alzheimer Res. 2017;14(4):412–425.
32. Ing NH, Berghman L, Abi-Ghanem D, et al. Marinobufagenin regulates permeability and gene expression of brain endothelial cells. Am J Physiol Regul Integr Comp Physiol. 2014;306(12):R918–R924. doi:10.1152/ajpregu.00499.2013
33. Oliver J, Abbas K, Lightfoot JT, et al. Comparison of Neurocognitive Testing and the Measurement of Marinobufagenin in Mild Traumatic Brain Injury: A Preliminary Report. J Exp Neurosci. 2015;27(9):67–72.
34. Ingebrigtsen T, Waterloo K, Jacobsen EA, Langbakk B, Romner B. Traumatic brain damage in minor head injury: relation of serum S-100 protein measurements to magnetic resonance imaging and neurobehavioral outcome. Neurosurgery. 1999;45(3):468–475.
35. Steiner J, Bogerts B, Schroeter ML, Bernstein HG. S100B protein in neurodegenerative disorders. Clin Chem Lab Med. 2011;49(3):409–424.
36. Mussack T, Hauser C, Klauss V, et al. Serum S-100B protein levels during and after successful carotid artery stenting or carotid endarterectomy. J Endovasc Ther. 2006;13:39–46.
37. Foerch C, Wunderlich MT, Dvorak F, et al. Elevated serum S100B levels indicate a higher risk of hemorrhagic transformation after thrombolytic therapy in acute stroke. Stroke. 2007;38:2491–2495.
38. Grubb NR, Simpson C, Sherwood RA, et al. Prediction of cognitive dysfunction after resuscitation from out-of-hospital cardiac arrest using serum neuron-specific enolase and protein S-100. Heart. 2007;93(10):1268–1273.
39. Rasmussen LS, Christiansen M, Hansen PB, Moller JT. Do blood levels of neuron-specific enolase and S-100 protein reflect cognitive dysfunction after coronary artery bypass? Acta Anaesthesiol Scand. 1999;43(5):495–500.
40. Anderson RE, Hansson LO, Nilsson O, Dijlai-Merzoug R, Settergren G. High serum S100B levels for trauma patients without head injuries. Neurosurgery. 2001;48(6):1255–1258.
41. Chabok SY, Moghadam AD, Saneei Z, Amlashi FG, Leili EK, Amiri ZM. Neuron-specific enolase and S100BB as outcome predictors in severe diffuse axonal injury. J Trauma Acute Care Surg. 2012;72(6):1654–1657.
42. Anand N, Lg S. Neuron-specific enolase as a marker for acute ischemic stroke: a systematic review. Cerebrovasc Dis. 2005;20(4):213–219.
43. Ramlawi B, Rudolph JL, Mieno S, et al. Serologic Markers of Brain Injury and Cognitive Function After Cardiopulmonary Bypass. Ann Surg. 2006;244(4):593–601.
44. Ramont L, Thoannes H, Volondat A, Chastang F, Millet MC, Maquart FX. Effects of hemolysis and storage condition on neuron-specific enolase (NSE) in cerebrospinal fluid and serum: implications in clinical practice. Clin Chem Lab Med. 2005;43(11):1215–1217.
45. Yang Z, Wang KKW. Glial fibrillary acidic protein: from intermediate filament assembly and gliosis to neurobiomarker. Trends Neurosci. 2015;38(6):364–374.
46. Vos PE, Jacobs B, Andriessen TM, et al. GFAP and S100B are biomarkers of traumatic brain injury: an observational cohort study. Neurology. 2010;75:1786–1793.
47. Oeckl P, Halbgebauer S, Anderl-Straub S, et al. Glial Fibrillary Acidic Protein in Serum is Increased in Alzheimer’s Disease and Correlates with Cognitive Impairment. J Alzheimers Dis. 2019;67(2):481–488.
48. Papa L, Lewis LM, Falk JL, et al. Elevated levels of serum glial fibrillary acidic protein breakdown products in mild and moderate traumatic brain injury are associated with intracranial lesions and neurosurgical intervention. Ann Emerg Med. 2012;59:471–483.
49. Metting Z, Wilczak N, Rodiger LA, Schaaf JM, van der Naalt J. GFAP and S100B in the acute phase of mild traumatic brain injury. Neurology. 2012;78:1428–1433.
50. Herrmann M, Vos P, Wunderlich MT, de Bruijn CH, Lamers KJ. Release of glial tissue-specific protein s after acute stroke. Stroke. 2000;31:2670.
51. Lin YS, Lee WJ, Wang SJ, Fuh JL. Levels of plasma neurofilament light chain and cognitive function in patients with Alzheimer or Parkinson disease. Sci Rep. 2018;8(1):17368.
52. Siman R, Toraskar N, Dang A, et al. A panel of neuron-enriched proteins as markers for traumatic brain injury in humans. J Neurotrauma. 2009;26:1867–1877.
53. Zurek J, Bartlova L, Fedora M. Hyperphosphorylated neurofilament NF-H as a predictor of mortality after brain injury in children. Brain Inj. 2012;25:221–226.
54. Natori A, Ogata T, Sumitani M, Kogure T, Yamauchi T, Yamauchi H. Potential role of pNF-H, a biomarker of axonal damage in the central nervous system, as a predictive marker of chemotherapy-induced cognitive impairment. Clin Cancer Res. 2015;21(6):1348–1352.
55. Inoue R, Sumitani M, Ogata T, Chikuda H, Matsubara T. Direct evidence of central nervous system axonal damage in patients with postoperative delirium: A preliminary study of pNF-H as a promising serum biomarker. Neurosci Lett. 2017;653:39–44.
56. Khalil M, Teunissen CE, Otto M, Piehl F, Sormani MP, Gattringer T. Neurofilaments as biomarkers in neurological disorders. Nat Rev Neurol. 2018;14(10):577–589.
57. de Wolf F, Mohsen Ghanbari M, Licher S, et al. Plasma tau, neurofilament light chain and amyloid-β levels and risk of dementia; a population-based cohort study. Brain. 2020;143(4):1220–1232.
58. Bradley-Whitman MA, Roberts KN, Abner EL, Scheff SW, Lynn B, Lovell MA. A novel method for the rapid detection of post-translationally modified visinin-like protein 1 in rat models of brain injury. Brain Inj. 2018;32(3):363–380.
59. Kester MI, Teunissen CE, Sutphen C, et al. Cerebrospinal fluid VILIP-1 and YKL-40, candidate biomarkers to diagnose, predict and monitor Alzheimer’s disease in a memory clinic cohort. Alzheimers Res Ther. 2015;7(1):59.
60. Wang L, Zhang M, Wang Q, Jiang X, Li K, Liu J. Alzheimer’s Disease Neuroimaging Initiative. APOE ε4 Allele Is Associated with Elevated Levels of CSF VILIP-1 in Preclinical Alzheimer’s Disease. Neuropsychiatr Dis Treat. 2020;8(16):923–931.
61. Groblewska M, Muszyński P, Wojtulewska-Supron A, Kulczynska-Przybik A, Mroczko B. The Role of Visinin-Like Protein-1 in the Pathophysiology of Alzheimer’s Disease. J Alzheimer’s Dis JAD. 2015;47(1):17–32.
62. Cata JP, Abdelmalak B, Farag E. Neurological biomarkers in the perioperative period. Br J Anaesth. 2011;107(6):844–858.
63. Josephs KA. Current Understanding of Neurodegenerative Diseases Associated With the Protein Tau. Mayo Clin Proc. 2017;92(8):1291–1303.
64. Wattmo C, Blennow K, Hansson O. Cerebro-spinal fluid biomarker levels: phosphorylated tau (T) and total tau (N) as markers for rate of progression in Alzheimer’s disease. BMC Neurol. 2020;20:10.
65. Chatfield DA, Zemlan FP, Day DJ, Menon DK. Discordant temporal patterns of S100beta and cleaved tau protein elevation after head injury: A pilot study. Br J Neurosurg. 2002;16:471–476.
66. Johnson VE, Stewart W, Smith DH. Traumatic brain injury and amyloid-β pathology: a link to Alzheimer’s disease? Nat Rev Neurosci. 2010;11(5):361–370.
67. Nakamura A, Kaneko N, Kato T, et al. High performance plasma amyloid-β biomarkers for Alzheimer’s disease. Nature. 2018;554(7691):249–254.
68. Wan H, Wang Y, Ai J, et al. Role of von Willebrand factor and ADAMTS-13 in early brain injury after experimental subarachnoid hemorrhage. J Thromb Haemost. 2018;16(7):1413–1422.
69. Hanson E, Jood K, Karlsson S, Nilsson S, Blomstrand C, Jern C. Plasma levels of von Willebrand factor in the etiologic subtypes of ischemic stroke. J Thromb Haemost. 2011;9(2):275–281.
70. Quinn TJ, Gallacher J, Deary IJ, Lowe GD, Fenton C, Stott DJ. Association between circulating hemostatic measures and dementia or cognitive impairment: systematic review and meta-analyzes. J Thromb Haemost. 2011;9(8):1475–1482.
71. Greisenegger S, Segal HC, Burgess AI, Poole DL, Mehta Z, Rothwell PM. Biomarkers and mortality after TIA and minor ischemic stroke: population-based study. Stroke. 2015;46(3):659–666.
72. Wannamethee SG, Whincup PH, Lennon L, Rumley A, Lowe GD. Fibrin D-dimer, tissue-type plasminogen activator, von Willebrand factor, and risk of incident stroke in older men. Stroke. 2012;43(5):1206–1211.
73. Weitz JI, Fredenburgh JC, Eikelboom JWA. Test in Context: D-Dimer. J Am Coll Cardiol. 2017;70(19):2411–2420.
74. Yepes M, Sandkvist M, Wong MK, et al. Neuroserpin reduces cerebral infarct volume and protects neurons from ischemia-induced apoptosis. Blood. 2000;96(2):569–576.
75. Wu W, Asakawa T, Yang Q, et al. Effects of neuroserpin on clinical outcomes and inflammatory markers in Chinese patients with acute ischemic stroke. Neurol Res. 2017;39(10):862–868.
76. Martin SJ, Grimwood PD, Morris RG. Synaptic plasticity and memory: an evaluation of the hypothesis. Annu Rev Neurosci. 2000;23:649–711.
77. Kernie SG, Liebl DJ, Parada LF. BDNF regulates behaviour and loco motor activity in mice. EMBO J. 2000;19(6):1290–1300.
78. Murer MG, Yan Q, Raisman-Vozari R. Brain-derived neurotrophic factor in the control human brain, and in Alzheimer’s disease and Parkinson’s disease. Prog Neurobiol. 2001;63(1):71–124.
79. Lu B, Nagappan G, Lu Y. BDNF and synaptic plasticity, cognitive function, and dysfunction. Handb Exp Pharmacol. 2014;220:223–250.
80. Shibazaki K, Kimura K, Okada Y, et al. Plasma brain natriuretic peptide as an independent predictor of in-hospital mortality after acute ischemic stroke. Intern Med. 2009;48(18):1601–1606.
81. Naveen V, Vengamma B, Mohan A, Vanajakshamma V. N-terminal pro-brain natriuretic peptide levels and short term prognosis in acute ischemic stroke. Ann Indian Acad Neurol. 2015;18(4):435–440.
82. Kara K, Mahabadi AA, Weimar C, et al. N-Terminal Pro-B Type Natriuretic Peptide is Associated with Mild Cognitive Impairment in the General Population. J Alzheimers Dis. 2017;55(1):359–369.
83. van Vliet P, Sabayan B, Wijsman LW, et al. NT-proBNP, blood pressure, and cognitive decline in the oldest old: the Leiden 85-plus Study. Neurology. 2014;83(13):1192–1199.
84. Zhang H, Ng KP, Therriault J, et al. Alzheimer’s Disease Neuroimaging Initiative. Cerebrospinal fluid phosphorylated tau, visinin-like protein-1, and chitinase-3-like protein 1 in mild cognitive impairment and Alzheimer’s disease. Transl Neurodegener. 2018;10(7):23.
85. Suárez-Calvet M, Kleinberger G, Caballero MAA, et al. sTREM2 cerebrospinal fluid levels are a potential biomarker for microglia activity in early-stage Alzheimer’s disease and associate with neuronal injury markers. EMBO Mol Med. 2016;8(5):466–476.
86. Willemse EAJ, Vos AD, Herries EM, Andreasson U, Engelborghs S. Neurogranin as Cerebrospinal Fluid Biomarker for Alzheimer Disease: an Assay Comparison Study. Clin Chem. 2018;64(6):927–937.
87. Portelius E, Zetterberg H, Skillbäck T, Törnqvist U. Alzheimer’s Disease Neuroimaging Initiative. Cerebrospinal fluid neurogranin: relation to cognition and neurodegeneration in Alzheimer’s disease. Brain. 2015;138(Pt 11):3373–3385.
88. Danborg PB, Simonsen AH, Waldemar G, Heegaard NHH. The potential of microRNAs as biofluid markers of neurodegenerative diseases-a systematic review. Biomarkers. 2014;19(4):259–268.
89. Frater J, Lie D, Bartlett P, McGrath JJ, Factor I-LG. (IGF-1) as a marker of cognitive decline in normal ageing: A review. Ageing Res Rev. 2018;42:14–27.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.