Back to Journals » International Medical Case Reports Journal » Volume 19
Bilateral Pulmonary Embolism Following Arthroscopic Anterior Cruciate Ligament Reconstruction: A Case Report
Authors Mohebi AS, Hakimi SR, Bek B ![]() , Mohebi S, Naibkhil N
, Mohebi S, Naibkhil N
Received 4 February 2026
Accepted for publication 27 June 2026
Published 8 July 2026 Volume 2026:19 601331
DOI https://doi.org/10.2147/IMCRJ.S601331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Ahmad Shakib Mohebi,1,2 Sayed Rahman Hakimi,2 Basira Bek,1 Sabawoon Mohebi,1,3 Nommanudien Naibkhil4,5
1Department of Orthopedic Surgery and Traumatology, Kabul Atlas Hospital, Kabul, Afghanistan; 2Department of Orthopedic Surgery and Traumatology, Wazir Mohammad Akbar Khan Hospital, Kabul, Afghanistan; 3Department of Medicine, Kateb University, Kabul, Afghanistan; 4Department of Biochemistry, Faculty of Pharmacy, Kabul University, Kabul, Afghanistan; 5Department of Research, Ariana Medical Complex, Kabul, Afghanistan
Correspondence: Basira Bek, Department of Orthopedic Surgery and Traumatology, Kabul Atlas Hospital, District 5, Karte Parwan, Kabul, 100202, Afghanistan, Email [email protected]
Abstract: Venous thromboembolism (VTE) is a serious complication associated with orthopedic surgery. It is well recognized in major procedures, such as total hip arthroplasty. However, there are few reports on the incidence of pulmonary embolism (PE) and its related risk factors following less invasive procedures, such as arthroscopic knee surgery. We present the case of a previously healthy young adult who developed bilateral PE following arthroscopic ACLR. The patient had no known predisposing risk factors for VTE. Early postoperative symptoms were nonspecific and resulted in delayed clinical diagnosis. Imaging studies confirmed the diagnosis bilateral PE. The patient was successfully managed with appropriate anticoagulation medication, leading to complete clinical recovery and resolution of symptoms. He was discharged in a stable condition and remained clinically stable during follow-up, with no further complications. Although VTE is a known complication of ACLR, this case highlights that VTE may occur even after routine arthroscopic procedures in patients without identifiable risk factors, underscoring the need for a high index of clinical suspicion and timely diagnostic assessment of postoperative symptoms to prevent delayed recognition of potentially life-threatening PE.
Keywords: knee arthroscopy, anterior cruciate ligament reconstruction, pulmonary embolism, deep venous thrombosis, case report
Introduction
Anterior cruciate ligament reconstruction (ACLR) is one of the most commonly performed orthopedic sports medicine procedures. Over 200,000 anterior cruciate ligament injuries occur annually in the United States alone.1 ACLR is the standard surgical treatment for anterior cruciate ligament tears, particularly in young and athletic populations.2 Although ACLR is generally considered a safe procedure, it may be associated with serious and potentially life-threatening complications, including venous thromboembolism (VTE), which encompasses deep vein thrombosis (DVT), and pulmonary embolism (PE). PE, in particularly, may lead to fatal outcomes.3,4 The incidence of VTE following ACLR has been reported to range from 0.16% to 0.53%.5, While PE remains uncommon but potentially life-threatening complication.6 Previous studies have reported an incidence of PE after ACLR ranging from 0.05% to 0.21%,7–9 with an estimated overall incidence of approximately 0.1%.10 Notably, PE may occur following any type of arthroscopic ACL reconstruction, regardless of graft choice or fixation method. Consequently, several authors have suggested that patients with identifiable risk factors for VTE should receive postoperative thromboprophylaxis following ACLR.10 While major orthopedic procedures, such as hip and knee arthroplasty follow well-established anticoagulation protocols, ACLR is not universally classified as a high-risk procedure. As a result, decisions regarding thromboprophylaxis are often based on individual patient risk assessment and clinical judgment. Current guidelines from the American College of Chest Physicians (ACCP) do not recommend routine thromboprophylaxis following arthroscopic procedures.2,11
This case demonstrates that clinically significant venous thromboembolism may occur even in patients without identifiable risk factors following arthroscopic surgery. Despite being a recognized complication, its presentation with nonspecific postoperative symptoms in low-risk patients may delay diagnosis. This underscores the importance of maintaining a high index of suspicion and prompt evaluation of postoperative symptoms to ensure early diagnosis and management of thromboembolism.
Presentation of the Case
A 28-year-old man presented with right knee pain and a giving-away sensation that developed after a twisting injury sustained while playing football. Physical examination demonstrated a positive anterior drawer and Lachman test. His body mass index was 22. He was previously healthy, with no known comorbidities or identifiable risk factors for VTE. There was no personal or family history of thromboembolic disorders or premature cardiovascular disease complications. Magnetic resonance imaging of the right knee confirmed a complete anterior cruciate ligament tear consistent with clinical findings.
The patient underwent arthroscopic ACLR under spinal anesthesia using a peroneus longus tendon graft. The total operative time was 60 min. A pneumatic tourniquet was applied at a pressure of 300 mmHg for 40 min. The procedure was uneventful, with minimal intraoperative blood loss, and the patient was subsequently transferred to the recovery room in stable condition. In accordance with existing guidelines, neither pharmacological nor mechanical thromboprophylaxis was administrated.
Postoperatively, the patient followed a standardized rehabilitation protocol, which included non–weight-bearing activities and isometric quadriceps exercises beginning on the first postoperative day. The knee was immobilized for approximately one week. From the second postoperative week onward, full weight-bearing was gradually allowed as tolerated. One week after surgery, the patient developed pain, erythema, and swelling of the right lower limb around the knee joint. On postoperative day 22, he presented to the emergency department with an acute onset of chest pain, dyspnea, and hemoptysis. On examination, his vital signs were as follows: heart rate 89 beats/min, respiratory rate 19 breaths/min, temperature 37 °C, blood pressure 100/75 mmHg, and oxygen saturation 92% on room air.
Laboratory investigations showed a normal complete blood count, normal electrocardiographic findings, and no elevation of cardiac biomarkers. However, the C-reactive protein level was markedly elevated at 105.87 mg/L (Table 1). Initial high-resolution computed tomography (HRCT) findings were suggestive of an acute infective inflammatory pulmonary process, while sputum microscopy revealed Gram-positive cocci. Collectively, these findings initially raised suspicion for a pulmonary infectious etiology, and empirical antibiotic therapy was initiated. However, the patient’s symptoms persisted and progressively worsened, prompting further diagnostic evaluation. Doppler ultrasonography of the lower limbs revealed deep vein thrombosis of the right leg extending from the tibioperoneal veins to the common femoral vein, accompanied by grade 1 soft tissue swelling. Computed tomography pulmonary angiography demonstrated extensive bilateral pulmonary emboli involving the main, lobar, and segmental pulmonary arteries as shown in Figure 1, with evidence of right heart strain and pulmonary arterial hypertension. Radiological features of pulmonary infarction were also noted in the upper and lower lobes.
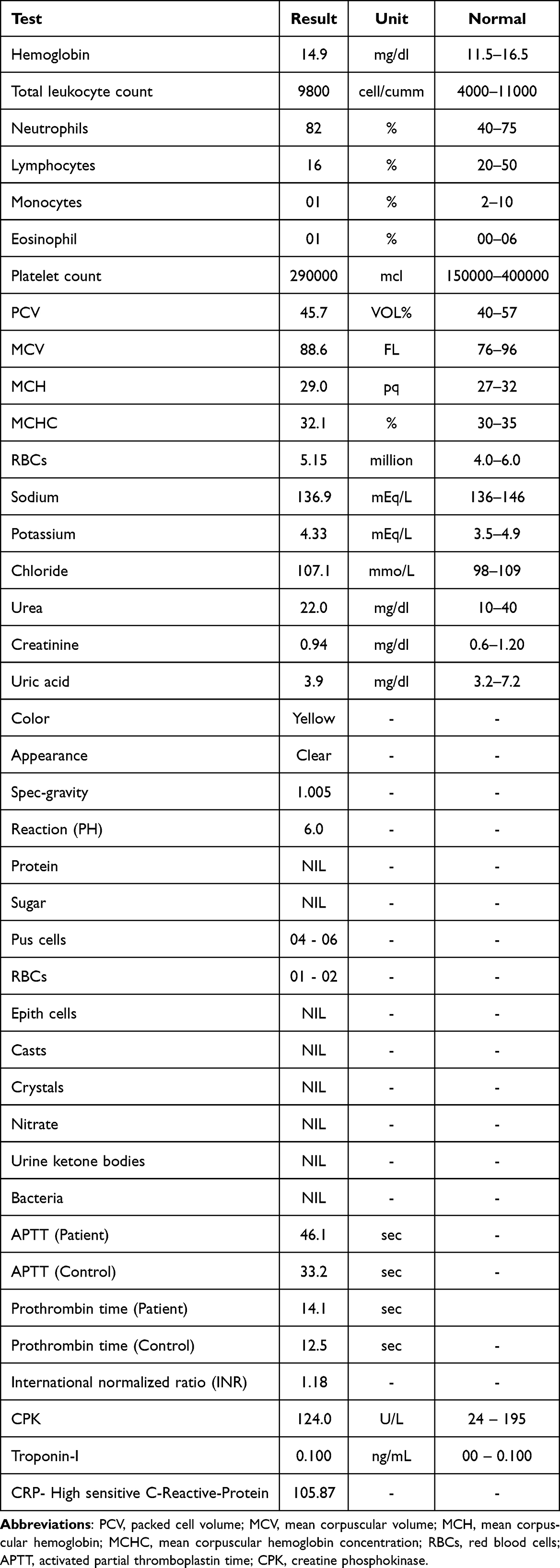 |
Table 1 Summary of the Patient’s Laboratory Investigations |
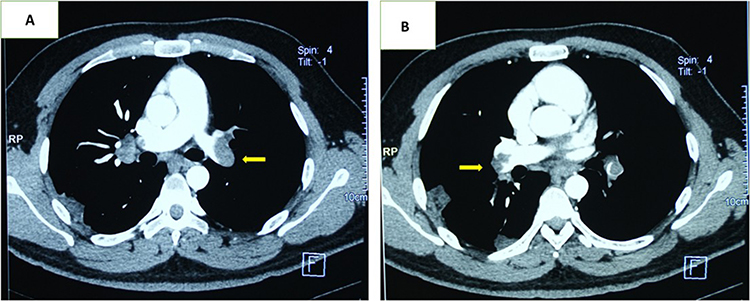 |
Figure 1 Axial contrast-enhanced CT images (A and B) reveal pulmonary embolism with filling defects in the left (A) and right (B) pulmonary artery branches (yellow arrows), consistent with acute pulmonary thromboembolism. |
Following the diagnosis of pulmonary embolism, the patient was admitted and treatment with low-molecular-weight heparin injection was initiated. After one week of hospitalization, he remained hemodynamically stable and was breathing comfortably on room air. He was discharged on oral rivaroxaban (15 mg twice daily) for 20 days and (20 mg once daily) for a planned duration of four months.
During five months’ follow-up, the patient reported no residual cardiopulmonary symptoms, was actively participating in physiotherapy, and demonstrated satisfactory recovery of knee function.
Discussion
The purpose of this case report is to describe a rare occurrence of symptomatic PE following routine ACLR in a previously healthy adult. Arthroscopic orthopedic procedures are commonly performed as same-day surgeries and are generally considered low risk. Nevertheless, as demonstrated in this case, serious and potentially life-threatening complications may occur, even in patients without identifiable perioperative risk factors. This highlights that PE can develop following ACLR irrespective of the patient’s baseline risk profile.
Several studies have examined the role of thromboprophylaxis following ACLR. One comparative study evaluated patients who underwent ACLR with and without chemical thromboprophylaxis; one group received low-molecular-weight heparin for 14 days, while the other received no prophylaxis. Notably, no symptomatic VTE events were reported in either group. These findings support previous evidence suggesting that symptomatic VTE is rare after ACLR and favor a selective, risk-based approach rather than routine thromboprophylaxis for all patients.2 In contrast, Nagashima et al reported a surprisingly high incidence of asymptomatic VTE in patients who did not receive pharmacological prophylaxis. Using contrast-enhanced computed tomography and ultrasonography, they identified asymptomatic DVT and PE in 16.4 and 7.3% of patients, respectively, following ACLR.4 Other studies have reported lower overall VTE rates; however, two investigations with high levels of scientific evidence (levels I and II) demonstrated that chemoprophylaxis significantly reduced VTE incidence and therefore recommended its use.12,13
The present case is comparable to that reported by Koaban et al, in which a healthy young adult without known risk factors developed bilateral PE after ACLR.3 Furthermore, a randomized controlled trial demonstrated that administration of enoxaparin for 20 days after ACLR significantly reduced the incidence of DVT compared with thromboprophylaxis limited to the in-hospital period (P < 0.001).12 Similarly, a meta-analysis concluded that LMWH significantly reduces the risk of VTE following ACLR compared with no prophylaxis.13
Several risk factors for PE following ACLR have been identified, including age over 40 years, female sex, operative duration exceeding 90 minutes, and a history of malignancy.14 The risk of postoperative symptomatic VTE is also increased in patients with previous thromboembolic events, vascular disorders, malignancies, prolonged anticoagulant use, hormone replacement therapy, or estrogen–progestin oral contraceptives. Additional factors such as obesity (BMI > 30 kg/m2), smoking, previous DVT, and advanced age further elevate the risk, particularly when multiple factors coexist.15,16 Notably, our patient had none of these risk factors, underscoring the rarity and clinical importance of this presentation.
Given the absence of clear risk factors in some patients, preoperative decision-making regarding thromboprophylaxis remains challenging. Current guidelines generally do not recommend routine thromboprophylaxis for knee arthroscopy in patients without a prior history of VTE or established risk factors.17 However, the present case emphasizes that PE may still occur in low-risk individuals, suggesting that existing recommendations may not fully capture the spectrum of postoperative thromboembolic risk.
This report emphasizes that, although international guidelines exist, recommendations for prophylactic anticoagulation following arthroscopic ACLR are largely based on individual risk stratification. The occurrence of PE in a young, healthy patient who adhered to postoperative rehabilitation underscores the need for further large-scale studies to better define thromboembolic risk and to develop clearer, evidence-based recommendations for thromboprophylaxis after knee arthroscopy.
It is noteworthy that VTE after ACLR may remain asymptomatic in the early postoperative period. Previous studies have reported an unexpectedly high rate of asymptomatic DVT and PE following ACLR. Consequently, the absence of severe symptoms does not rule out thromboembolic events. Patients, surgeons, physiotherapists, and nursing staff should be educated about warning signs such as pain, unilateral cramp, and swelling of the lower limb (especially the calf), dyspnea, pleuritic chest pain, tachycardia, tachypnea, cough, hemoptysis, and syncope. Immediate recognition and evaluation of these symptoms may facilitate faster diagnosis and treatment before progression to bilateral PE.
In the present case, diagnosis was initially challenging due to chest CT findings interpreted as an infectious or inflammatory pulmonary condition, together with elevated inflammatory markers and sputum microscopy demonstrating gram-positive cocci. This case illustrates that pulmonary embolism with pulmonary infarction may closely mimic pulmonary infection, which can lead to delayed consideration of thromboembolic disease.
Following this case, our postoperative management approach was adjusted in our institution. Prophylactic anticoagulant therapy was implemented for 14 days to all patients, particularly those with a higher body mass index (BMI) and those aged over 30 years. No further thromboembolic events were observed, and all patients achieved favorable clinical outcomes.
Limitations
As a single-patient case report, the findings are inherently limited in their generalizability to the broader population undergoing ACLR. Further large-scale studies are needed to better define thromboembolic risk factors and optimal thromboprophylaxis strategies following ACLR.
Conclusion
We report a case of DVT and bilateral PE following arthroscopic ACLR in a healthy 28-year-old adult without conventional risk factors. Prompt diagnosis and appropriate anticoagulant therapy resulted in a favorable outcome. Although PE after routine arthroscopic surgery is uncommon, this case emphasizes how crucial it is to keep a high level of suspicion throughout the recovery phase. Patient, nurses, physiotherapists, and all healthcare providers involved in postoperative care should be educated about the warning signs of VTE. In suspected cases, prompt clinical evaluation and appropriate investigations, such as Doppler ultrasound and D-dimer testing, which are both affordable and easily accessible, should be taken into consideration.
Ethics and Consent Statements
The patient provided written informed consent for publication of this report, including all relevant clinical data and images. Institutional approval was also obtained from the Institutional Review Board of Kabul Atlas Hospital (protocol code 03, date 20 January 2026).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Sherman SL, Calcei J, Ray T, et al. ACL study group presents the global trends in ACL reconstruction: biennial survey of the ACL study group. J ISAKOS. 2021;6(6):322–7. doi:10.1136/jisakos-2020-000567
2. Afana HB, Ashokan S, Nau T. Venous thromboembolism prophylaxis after anterior cruciate ligament reconstruction: retrospective case-control study. SICOT-J. 2025;11:38. doi:10.1051/sicotj/2025032
3. Koaban S, Alatassi R, Ahmed B, Alogayyel N. Bilateral pulmonary embolism after arthroscopic anterior cruciate ligament reconstruction: a case report. Int J Surg Case Reports. 2018;49:64–66. doi:10.1016/j.ijscr.2018.06.021
4. Nagashima M, Otani T, Takeshima K, et al. Unexpectedly high incidence of venous thromboembolism after arthroscopic anterior cruciate ligament reconstruction: prospective, observational study. J ISAKOS. 2020;5(2):80–82. doi:10.1136/jisakos-2019-000390
5. Bayle-Iniguez X, Cassard X, Vinciguerra B, Murgier J. Postoperative thromboprophylaxis does not reduce the incidence of thromboembolic events after ACL reconstruction. Orthopaed Traumatol. 2021;107(4):102904. doi:10.1016/j.otsr.2021.102904
6. Janssen RPA, Sala HAGM. Fatal pulmonary embolism after anterior cruciate ligament reconstruction. Am J Sports Med. 2007;35(6):1000–1002. doi:10.1177/0363546506298581
7. Nagashima M, Takeshima K, Origuchi N, et al. Not using a tourniquet may reduce the incidence of asymptomatic deep venous thrombosis after ACL reconstruction: an observational study. Orthopaed J Sports Med. 2021;9(12):23259671211056677. doi:10.1177/23259671211056677
8. Christian RA, Lander ST, Bonazza NA, et al. Venous thromboembolism prophylaxis and hormonal contraceptive management practice patterns in the perioperative period for anterior cruciate ligament reconstruction. Arthroscopy Sports Med Rehabil. 2022;4(2):e679–e685. doi:10.1016/j.asmr.2021.12.010
9. Montesinos-Berry E, Sanchis-Alfonso V, Monllau JC. Deep venous thrombosis and pulmonary embolism after acl reconstruction: what can we do to prevent it? In: Sanchis-Alfonso V, Monllau JC editors. The ACL-Deficient Knee. Springer London; 2013:391–399. doi:10.1007/978-1-4471-4270-6_33
10. Janssen RPA, Reijman M, Janssen DM, Van Mourik JBA. Arterial complications, venous thromboembolism and deep venous thrombosis prophylaxis after anterior cruciate ligament reconstruction: a systematic review. WJO. 2016;7(9):604. doi:10.5312/wjo.v7.i9.604
11. Gaskill T, Pullen M, Bryant B, Sicignano N, Evans AM, DeMaio M. The prevalence of symptomatic deep venous thrombosis and pulmonary embolism after anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43(11):2714–2719. doi:10.1177/0363546515601970
12. Marlovits S, Striessnig G, Schuster R, et al. Extended-duration thromboprophylaxis with enoxaparin after arthroscopic surgery of the anterior cruciate ligament: a prospective, randomized, placebo-controlled study. Arthroscopy. 2007;23(7):696–702. doi:10.1016/j.arthro.2007.02.001
13. Zhu J, Jiang H, Marshall B, Li J, Tang X. Low-molecular-weight heparin for the prevention of venous thromboembolism in patients undergoing knee arthroscopic surgery and anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trials. Am J Sports Med. 2019;47(8):1994–2002. doi:10.1177/0363546518782705
14. Hetsroni I, Lyman S, Do H, Mann G, Marx RG. Symptomatic pulmonary embolism after outpatient arthroscopic procedures of the knee: the incidence and risk factors in 418323 arthroscopies. J Bone Joint Surg British Volume. 2011;93-B(1):47–51. doi:10.1302/0301-620X.93B1.25498
15. Krych AJ, Sousa PL, Morgan JA, Levy BA, Stuart MJ, Dahm DL. Incidence and risk factor analysis of symptomatic venous thromboembolism after knee arthroscopy. Arthroscopy. 2015;31(11):2112–2118. doi:10.1016/j.arthro.2015.04.091
16. Delis KT, Hunt N, Strachan RK, Nicolaides AN. Incidence, natural history and risk factors of deep vein thrombosis in elective knee arthroscopy. Thromb Haemost. 2001;86(09):817–821. doi:10.1055/s-0037-1616137
17. Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients. Chest. 2012;141(2):e278S–e325S. doi:10.1378/chest.11-2404
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Triage of Massive Pulmonary Embolism Masked by Giant Bullous Disease: The Diagnostic Value of Silent Hypoxia and Physical Examination
Mousa MM, Ali AO, Jama AM, Muse SM, Ibrahim FE, Muse JM, Yey BE, Abdi MH
International Medical Case Reports Journal 2026, 19:598779
Published Date: 3 June 2026