Back to Journals » International Medical Case Reports Journal » Volume 18
Bilateral Oculomotor Nerve Palsy: A Rare Complication of Bridging Thrombolysis for Acute Basilar Artery Occlusion
Authors Lv S, Liu R, Sun J, Liu H, Guo X, Ding C
Received 7 April 2025
Accepted for publication 27 August 2025
Published 4 September 2025 Volume 2025:18 Pages 1141—1146
DOI https://doi.org/10.2147/IMCRJ.S532206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Shuangyun Lv,1 Ronghui Liu,1 Jiapeng Sun,1 Hongmei Liu,1 Xin Guo,2– 4 Changxia Ding1
1Department of Neurology, Huanghua Municipal People’s Hospital, Huanghua, Hebei, 061100, People’s Republic of China; 2Department of Neurology, the First Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China; 3Department of Neurology, Hebei Hospital, Xuanwu Hospital, Capital Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China; 4Neuromedical Technology Innovation Center of Hebei Province, Shijiazhuang, Hebei, 050000, People’s Republic of China
Correspondence: Changxia Ding, Department of Neurology, Huanghua Municipal People’s Hospital, Huanghua, Hebei, 061100, People’s Republic of China, Email [email protected] Xin Guo, Department of Neurology, the First Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China, Email [email protected]
Abstract: Acute vertebrobasilar artery occlusion (AVBAO) accounts for only 1– 2% of ischemic stroke, but it has high disability and mortality rates. Mechanical thrombectomy (MT) combined with intravenous thrombolysis can quickly achieve vascular recanalization and significantly improve patient prognosis. This report describes a 73-year-old male who was admitted to the hospital in a coma due to AVBAO. After MT, successful recanalization of the basilar artery was achieved; however, the patient subsequently developed the rare but serious complication of bilateral oculomotor nerve palsy. The report emphasizes the need for careful preoperative planning, including detailed assessment of vascular anatomy and thrombus characteristics, and the importance of operator expertise. Improved intraoperative technique and close postoperative monitoring may help prevent complications such as vessel injury or embolic recurrence. Additionally, clinicians should be aware of the limitations of early DWI (Diffusion-weighted imaging) in detecting brainstem infarcts and of the need for clinical vigilance in the postoperative period.
Keywords: acute ischemic stroke, acute vertebrobasilar artery occlusion, mechanical thrombectomy, bilateral oculomotor nerve palsy
Introduction
Acute vertebrobasilar artery occlusion (AVBAO) accounts for only 1–2% of all ischemic strokes but represents 5% of large-vessel occlusion strokes, with a sudden onset and with mortality rates of up to 68%-90%.1 Patients often present with dizziness, vomiting, diplopia, dysarthria, swallowing difficulties, and rapidly progressing coma or quadriplegia. If left untreated, the mortality rate can reach up to 90%. It has been confirmed that early recanalization of occluded arteries in acute stroke is associated with good functional prognosis. The recanalization treatment includes intravenous thrombolysis (IVT), mechanical thrombectomy (MT), or combination therapy. MT, as the core vascular recanalization technique for acute large-vessel occlusion cerebral infarction, can significantly improve prognosis. However, its benefits come with significant risks that cannot be ignored. According to reports, the prevalence of distal embolism caused by basilar artery occlusion is 30%-35%.2 Other complications include perforated artery injury, intracranial hemorrhage, vascular dissection, reocclusion, and hyperperfusion syndrome, all of which can exacerbate neurological deficits and even endanger life. At present, isolated and complete bilateral oculomotor nerve paralysis is an extremely rare complication after MT, with only sporadic case reports. The exact mechanism is still unclear, and most clinicians speculate that it is related to mechanical tearing or microembolic migration of the top perforating branch of the basilar artery (such as the basilar artery superior cerebellar artery perforating branch) causing ischemic damage to the oculomotor nucleus. This report introduces a 73-year-old male who was admitted to the hospital in a coma due to AVBAO. After IVT combined with MT, a rare complication of bilateral oculomotor nerve paralysis occurred. Over 6 months of follow-up, the symptoms of oculomotor nerve paralysis gradually improved. This article conducts an in-depth analysis of the possible pathogenesis of this case and proposes that optimizing thrombus resection equipment and improving surgical methods can effectively reduce the risk of complications, providing a reference for clinical decision-making.
Case Presentation
The patient, a 73-year-old male, was admitted to our hospital due to impaired consciousness for 2 hours. Prior to admission, family members found him unconscious and unable to move his limbs. He had no vomiting, limb convulsions, or incontinence. No special treatment was given prior to hospital arrival, an arrival prompted by an urgent call to our facility via the emergency number 120. Past medical history included hypertension and gout, with no history of coronary heart disease, atrial fibrillation, or type 2 diabetes. He had a 40-year history of smoking and alcohol consumption. On admission, physical examination revealed a blood pressure of 204/69 mmHg. He could not cooperate with the physical examination because of his reduced level of consciousness and aphasia. His limbs were immobile, and both pupils were equal and round, measuring 2 mm in diameter, with no deviation of the eyes. Extraocular movements were absent, and no nystagmus was observed. Tongue extension was uncooperative, and muscle strength of all limbs was grade 0. Muscle tone was reduced, and bilateral Babinski sign was positive. The NIHSS score was 26. The Glasgow Coma Scale score was 6. After admission, cranial MRI with MRA was performed. DWI showed no obvious new cerebral infarction (Figure 1A–C), while MRA revealed basilar artery occlusion. ECG indicated a sinus rhythm with a heart rate of 72 bmp Blood glucose, complete blood counts, liver and kidney function, and coagulation profiles were all within the normal range. The patient presented with an acute onset and severe symptoms. The DWI results did not show new cerebral infarctions. The examination was performed very early after symptom onset. However, based on clinical symptoms, a diagnosis should be considered: 1. cerebral infarction, 2. acute basilar artery occlusion. The preoperative examination was completed. With the consent of the family, contraindications were excluded. IVT with rt-PA was initiated immediately. The patient, weighing 78 kg, received a 7 mg rt-PA bolus intravenously over 1 minute, followed by the remaining 63 mg infused at 0.9 mg/kg over 1 hour via intravenous pump, while concurrent MT was performed. Cerebral angiography indicated basilar artery occlusion (Figure 2A). A Solitaire 4–20 thrombectomy stent was placed in the right posterior cerebral artery for thrombectomy once, and a large amount of thrombus was removed. Re-angiography revealed that the blood flow in the occluded basilar artery was smooth, and the operation went smoothly (Figure 2B). Physical examination under sedation after the operation revealed exotropia of both eyes, with unequal pupil sizes of 3 mm on the right side and 2–5 mm on the left side. The NIHSS score was 3. Postoperatively, tirofiban was administered at a rate of 6 mL/h via continuous infusion, along with medications for lipid reduction, plaque stabilization, and circulation improvement.
 |
Figure 1 Cranial DWI scan results. (A–C) DWI results before MT. (D–F) DWI results after MT. Red arrow indicates new cerebral infarctions. Abbreviation: MT, mechanical thrombectomy. |
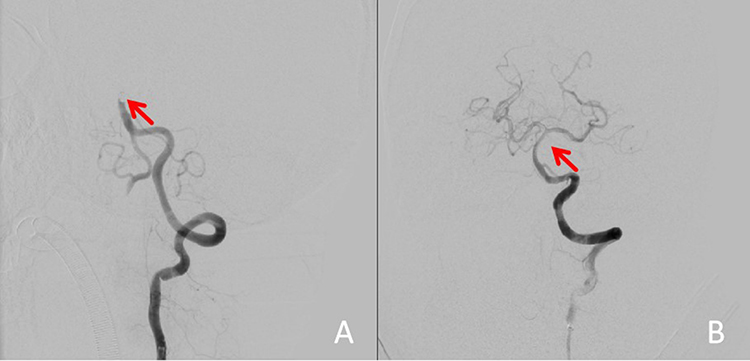 |
Figure 2 Cerebral angiography results. (A) Angiography results before MT. Red arrow indicates occlusion of basilar artery. (B) Angiography results after MT. Red arrow indicates complete recanalization of basilar artery. Abbreviation: MT, mechanical thrombectomy. |
On the second postoperative day, the patient was alert with clear speech and normal motor function in the limbs. However, he developed bilateral ptosis, an inability to open his eyes, and limited ocular movement with only abduction possible. Adduction, elevation, and depression were all compromised (Figure 3). Bilateral pupillary light reflexes were diminished, with the right pupil measuring 3.0 mm in diameter and the left pupil measuring 2.5 mm. Bilateral oculomotor nerve palsy may have been indicated. Aspirin enteric-coated tablets and clopidogrel were administered for antiplatelet aggregation treatment 48 h after tirofiban pumping. At the same time, neurotrophic drugs were administered. On the fourth day after admission, a follow-up cranial DWI indicated an acute cerebral infarction in the right pons and midbrain (Figure 1D–F). The patient was discharged after 10 days. At time of discharge, there was no significant improvement in the symptoms of bilateral oculomotor nerve palsy. At a 3-month follow-up, the symptoms of ptosis were alleviated. Both eyeballs could move inward, upward, and downward, but not completely. At 6-month follow-up, symptoms of ptosis and ocular motility disorders were not present.
 |
Figure 3 Symptoms of bilateral oculomotor nerve palsy after bridging therapy. (A and E) When looking up or down, the eyeballs exhibit no obvious change. (B and D) When looking left or right, neither eyeball shows adduction, elevation, or depression, but both retain abduction. (C) In a natural state, both eyelids droop.The red arrow indicates the patient’s gaze direction. |
Discussion
The patient in this case was admitted due to sudden unconsciousness for 2 hours. After admission, the head MRI DWI sequence showed no significantly high signal, and MRA indicated occlusion of the basilar artery. The patient successfully achieved recanalization of large blood vessels through bridging therapy and quickly regained consciousness. However, bilateral oculomotor nerve palsy occurred. The DWI sequence of the patient’s head before thrombectomy showed no significantly high signal, which may have been due to the following: a. In the early stage of acute basilar artery occlusion (within 6 hours of onset), there is no significant cellular edema or increase in intracellular water content in brain tissue, resulting in limited diffusion that cannot be detected by DWI;3 b. The blood-brain barrier is less damaged, and the diffusion of water in the extracellular space is not significantly restricted. DWI may not be able to display abnormalities;4 c. Some patients may maintain local brain tissue perfusion with the formation of cellular edema delayed through the mechanism of cerebral blood flow autoregulation;5 d. The resolution and imaging parameters of the equipment may also affect the accuracy of results.6
The patient’s bilateral oculomotor nerve damage manifested as bilateral ptosis of the upper eyelids, inability to open the eyes, eyeballs that could only be extended outward (with limited inward, upward, and downward movement), and uneven pupils on both sides with slow light reflex. These were all related to a midbrain infarction that appeared during subsequent follow-up MRI. Due to the widespread distribution of the oculomotor nucleus in the midbrain, it often manifests as incomplete oculomotor nerve paralysis. At the same time, the positions of the oculomotor nuclei on both sides were relatively close, so midbrain damage may have led to bilateral oculomotor nerve paralysis.7
The main blood supply artery of the oculomotor nucleus is the median artery adjacent to the midbrain, mainly originating from the posterior cerebral artery but also from the bifurcation of the basilar artery and the posterior communicating artery. Bridging therapy restored the patient’s basilar artery blood flow. But then there were infarctions in the thalamus, midbrain, and pons, which were considered to be caused by occlusion of the midbrain artery supplying the bilateral oculomotor nuclei.4 Possible reasons may be that there are many perforating arteries at the apex of the basilar artery, and release and pulling of thrombectomy equipment and long surgical time can all result in a perforated artery with traumatic tearing. The thrombus burden is high, the thrombus texture is hard or not firmly attached, and thrombus fragments move with the blood flow, finally leading to distal vascular embolism8 In addition, the selection, operation mode, and force of the thrombectomy device may affect the integrity of the thrombus, and a thrombus fragment embolism can result.9
To avoid the occurrence of the above complications, before surgery, the characteristics of the thrombus and the anatomical structure of the blood vessels should be evaluated, and appropriate thrombectomy devices and operating methods should be selected. Intraoperative procedures should be gentle and slow to avoid excessive pulling of blood clots. Methods such as suction assistance or direct suction can be used to reduce or even avoid vascular damage and the detachment of thrombus fragment.10 Even if the surgery is successful and the NIHSS score significantly improves, changes in condition should be closely monitored in a specialized stroke unit to reduce the likelihood of disability or mortality.
Conclusion
This case highlights the rare but serious risk of bilateral oculomotor nerve paralysis following MT in BAO. It emphasizes the need for careful preoperative planning, including detailed assessment of vascular anatomy and thrombus characteristics, and the importance of operator expertise. Improved intraoperative technique and close postoperative monitoring may help prevent complications such as vessel injury or embolic recurrence. Additionally, clinicians should be aware of the limitations of early DWI imaging in detecting brainstem infarcts, which reinforces the need for vigilance in the postoperative period. This case can raise awareness about the MT procedure, which will assist neurointerventionalists, the stroke community, and the general public.
Ethical Approval
This case report is exempt from ethical approval as determined by the ethical review board at our institution, given the nature of the article.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Acknowledgments
The authors would like to express their sincere gratitude to the patient and the patient’s guardian for providing consent to include the case details and photographs in this publication.
Funding
The medical science research project of Hebei Province (No. 20232154).
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Zi W, Qiu Z, Wu D, et al. Assessment of endovascular treatment for acute basilar artery occlusion via a nationwide prospective registry. JAMA Neurol. 2020;77:561–573. doi:10.1001/jamaneurol.2020.0156
2. Yeo LLL, Holmberg A, Mpotsaris A, et al. Posterior circulation occlusions may be associated with distal emboli during thrombectomy: factors for distal embolization and a review of the literature. Clin Neuroradiol. 2019;29:425–433. doi:10.1007/s00062-018-0679-z
3. Mokin M, Rojas H, Levy EI. Randomized trials of endovascular therapy for stroke--impact on stroke care. Nat Rev Neurol. 2016;12:86–94. doi:10.1038/nrneurol.2015.240
4. Launhardt N, Jesser J, Hasan D, et al. DWI reversibility in acute ischemic stroke due to basilar artery occlusion following successful recanalization. Clin Neuroradiol. 2025. doi:10.1007/s00062-025-01512-9
5. Lee YY, Yoon W, Kim SK, et al. Acute basilar artery occlusion: differences in characteristics and outcomes after endovascular therapy between patients with and without underlying severe atherosclerotic stenosis. AJNR Am J Neuroradiol. 2017;38:1600–1604. doi:10.3174/ajnr.A5233
6. Ortega-Gutierrez S, Rodriguez-Calienes A, Mierzwa AT, et al. Rescue stenting for failed mechanical thrombectomy in acute basilar artery occlusions: analysis of the PC-SEARCH registry. Stroke. 2025;56:401–412. doi:10.1161/STROKEAHA.124.047694
7. Redden LD, Gubitz GJ. A unique case of internuclear ophthalmoplegia and artery of percheron infarct. Cureus. 2024;16:e74744. doi:10.7759/cureus.74744
8. Ahmed RA, Dmytriw AA, Patel AB, et al. Basilar artery occlusion: a review of clinicoradiologic features, treatment selection, and endovascular techniques. Interv Neuroradiol. 2023;29:748–758. doi:10.1177/15910199221106049
9. Wakabayashi T, Miyata T, Ogura T, et al. Effectiveness of mechanical thrombectomy for acute unilateral vertebral artery occlusion with patent basilar artery: case series and literature review. Clin Neurol Neurosurg. 2025;250:108804. doi:10.1016/j.clineuro.2025.108804
10. Tanimura M, Ikeda H, Fujiwara T, et al. Basilar artery occlusion due to vertebral artery injury treated with thrombectomy and distal vertebral artery embolization through the unaffected side. Surg Neurol Int. 2024;15:12. doi:10.25259/SNI_948_2023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.