Back to Journals » International Medical Case Reports Journal » Volume 16
Bilateral Central Retinal Vein Occlusion Secondary to Leukostasis in the Setting of Diffuse Large-B Cell Lymphoma: Case Report
Authors Toohey TP, Corker A, Lee MB, Kidson-Gerber G ![]()
Received 13 February 2023
Accepted for publication 23 May 2023
Published 27 May 2023 Volume 2023:16 Pages 319—322
DOI https://doi.org/10.2147/IMCRJ.S408404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thomas P Toohey,1,2 Alma Corker,1,2 Mitchell B Lee,2,3 Giselle Kidson-Gerber1,2
1Department of Haematology, Prince of Wales Hospital, Sydney, Australia; 2Department of Medicine, the University of New South Wales, Sydney, Australia; 3Department of Ophthalmology, Prince of Wales Hospital, Sydney, Australia
Correspondence: Thomas P Toohey, Prince of Wales Hospital, 320-346 Barker St, Randwick, NSW, 2031, Australia, Tel +61 39727945, Email [email protected]
Abstract: A woman in her 50’s was diagnosed diffuse large B-cell lymphoma (DLBCL) after presenting to hospital in a critical condition, characterised by marked hyperleukocytosis (white cell count 290 x109/L). She subsequently developed painless blurred vision bilaterally, and was diagnosed with bilateral central retinal vein occlusion secondary to leukostasis. She was managed with non-Hodgkin lymphoma R-CHOEP14 (rituximab, cyclophosphamide, doxorubicin, vincristine, etoposide, prednisolone) immunochemotherapy, with her ocular signs and symptoms improving following treatment. Optical coherence tomography and funduscopic examination demonstrated no evidence of intraocular lymphoma. Visual acuity returned to 6/6 in each eye with subsequent resolution of her symptoms. Repeat examination demonstrated stable appearance of her ocular disease.
Keywords: hyperleukocytosis, diffuse large-b cell lymphoma, ophthalmology
Introduction
Diffuse large B-cell lymphoma (DLBCL) accounts for approximately 25% of non-Hodgkin lymphoma (NHL), making it the most common subtype of this disease.1,2 DLBCL is an aggressive and heterogenous lymphoma, further subdivided into morphological and molecular variants with distinct clinical presentations that have varying prognoses and treatment choices.3 The initial presentation of DLBCL is most commonly with an enlarging neck or abdominal nodal mass, and can feature ‘systemic B symptoms’ such as fever, unintentional weight loss, and night sweats.3 Ocular manifestations are a rare feature of diffuse large B-cell lymphoma, most commonly presenting as primary central nervous system (CNS) lymphoma.4 Central retinal vein occlusion (CRVO) is typically unilateral, although in rare cases it may present bilaterally. This can be linked to underlying conditions such as hyperviscosity, vasculopathy or other blood dyscrasias.5
The patient in this report demonstrated a case of bilateral non-ischaemic CRVO secondary to leukostasis. To our knowledge, no previous case report has documented this complication in the setting of DLBCL.
Case Presentation
A woman in her mid 50s presented to the emergency department of a large metropolitan teaching hospital in a critical condition. Initial investigations demonstrated hyperleukocytosis, severe anaemia and hypo-osmolar hyponatraemia (white cell count 290 x109/L, haemoglobin 39 g/L, sodium 108 mEq/L). She was transferred to the high-dependency unit for ongoing assessment and multidisciplinary management with haematology, renal and intensive care specialists.
She underwent computed tomography (CT) chest/abdomen/pelvis with contrast and positron emission tomography whole body fluorodeoxyglucose studies, which demonstrated extensive nodal disease above and below the diaphragm, with splenic and skeletal involvement. Blood film and diagnostic bone marrow aspirate and trephine was performed which confirmed a diagnosis of DLBCL (Figure 1). The tumour cells were large and show marked nuclear pleomorphism. On immunohistochemistry, they were positive for CD20, PAX5, CD5, BCL2, cMYC and MUM1, and negative for cyclin D1 and TdT. Weak-to-moderate Bcl-6 immunostaining was seen in around 30% of tumour cells. The Ki-67 proliferation index is approximately 25% by visual estimation. The immunophenotype based on flow cytometric assessment was CD45+/HLA-DR+/CD19+/CD20+/CD22+/CD23-/CD200+/CD5+/CD10-/CD38-/CD11c+/FMC7+/cyto-Kappa+ with absent surface light chain expression. MYC, BCL2 and BCL6 gene rearrangements were not detected by FISH. Cytogenetics analysis reveal an abnormal clone with [42–44, XX, add(1)(p32), add (4)(p14), add(12)(p11.2)]. TP53 variant was present at 92%VRF on NGS. CNS involvement was present with 19% lymphoma cells noted in the CSF at diagnosis. Non-contrast CT brain demonstrated no abnormality.
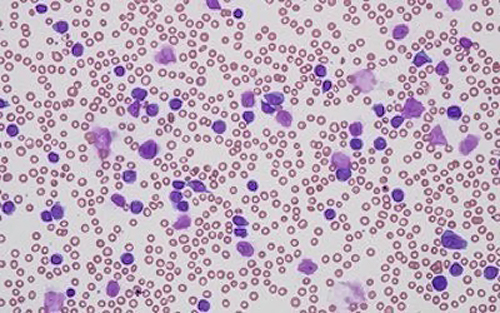 |
Figure 1 Blood film demonstrates normocytic anaemia, moderate thrombocytopenia hyperleukocytosis with large lymphoma cells. |
One week into her hospital admission, the patient reported bilateral, painless blurred vision and difficulty focusing on near objects. The onset of these symptoms was reported to have coincided with her presentation to the emergency department seven days prior. Aside from presbyopia, the patient had no previous ophthalmological history. Best corrected visual acuity (BCVA) was 6/9 in the right eye and 6/6 in the left, with no relative afferent pupillary defect. The intraocular pressures were normal in both eyes (15 OD and 12 OS). Ophthalmoscopy demonstrated bilateral venous dilation and tortuosity in the retinal vasculature, superficial retinal hemorrhages scattered throughout the posterior pole of the eye and cotton wool spots indicative of localized ischemia (Figure 2). Dynamic fundoscopy demonstrated raised retinal venous pressure, with ocular compression causing closure of the retinal arterioles prior to the retinal venules. However, there was no evidence of anterior or posterior uveitis, no keratic precipitates and no other features suggestive of intraocular lymphoma. Similarly, optical coherence tomography (OCT) imaging found no associated macular edema in either eye (Figure 3).
 |
Figure 2 Fundus photography of the right and left eyes demonstrates bilateral venous dilation retinal hemorrhages (labelled) and cotton wool spots (circled). |
 |
Figure 3 Optical coherence tomography of the right eye which demonstrates no associated macular edema, as shown by normal foveal thickness. |
The patient was diagnosed with bilateral CRVO, secondary to leukostasis. Given her concurrent systemic illness, the management centred around treating her underlying lymphoma, with ongoing ophthalmology follow-up. In the absence of cystoid macular oedema or retinal neovascularisation, no active ophthalmic intervention was indicated.
She was subsequently commenced on the first of eight planned cycles of non-Hodgkin lymphoma R-CHOEP14 (rituximab, cyclophosphamide, doxorubicin, vincristine, etoposide, prednisolone) immunochemotherapy. One week later she was reviewed again in ophthalmology clinic. Her BCVA had improved to 6/6 OD and was stable at 6/6 OS, whilst funduscopic and OCT examination showed no change in the patient’s ocular signs. After two weeks, she was discharged from hospital with a plan for ongoing ophthalmology follow-up.
Three weeks later she was re-admitted to hospital with chest pain in the context of DLBCL. She had a complicated admission with ongoing pain and cytopenias, which required multiple specialist medical team input. Whilst her ocular disease remained subjectively stable, the patient’s condition continued to deteriorate, as she developed febrile neutropenia, a gram negative (pseudomonas) bacteraemia, as well as COVID-19 infection. Despite ongoing active treatment of her infections, the patient sadly passed away less than two months after commencing chemotherapy.
Discussion
Ocular disease secondary to NHL is a rare phenomena, typically the result of a primary CNS lymphoma.4 Other ophthalmological complications secondary to lymphoma include systemic spread to the eye and hematologic complications, such as hypercoagulability.6,7 The patient in this report developed bilateral CRVO secondary to leukostasis.
The cause of CRVO is thought to be in keeping with Virchow’s Triad of venous stasis, vessel integrity damage and hypercoagulation. Early manifestation of this condition is characterised by dilated and tortuous retinal veins. Progression to complete CRVO is characterised by painless blurred vision and diplopia, with retinal hemorrhages and cotton wool-spots on funduscopic examination.8 All cases of retinal venous occlusion may be complicated by cystoid macular oedema and/or retinal neovascularisation. The treatment of cystoid macular oedema secondary to CRVO comprises of intravitreal anti- vascular endothelial growth factor (VEGF) injections.9 Neovascularisation in turn may lead to vision-threatening complications including vitreous haemorrhage, tractional retinal detachments, and neovascular glaucoma.8
Bilateral CRVO has been described in various hyperviscous or leukostatic states including mucosal-associated lymphoid tissue lymphoma, multiple myeloma, acute lymphoblastic leukaemia and Waldenström’s macroglobulinemia.5,7,10 Therefore, a diagnosis of certain B-cell lymphoproliferative disorders or other causes of hyperviscosity should be considered following observation of bilateral CRVO. To our knowledge, this is the first reported case of bilateral CRVO in the setting of DLBCL.
Our case represents a rare complication of NHL. In summary, cancer patients reporting bilateral visual changes warrant prompt evaluation for ophthalmic manifestations of metastatic, paraneoplastic and hyperviscosity-related disease.
Consent
The case report and its contents, including the results of investigations and images, was discussed with the patient, and informed consent for publication was obtained and documented in the hospital medical records system in June of 2022, prior to her death.
Institutional approval was not required.
Author Contributions
T.P.T and G.KG conceived the presented idea. T.P.T, A.C, M.B.L and G.KG carried out the patient examination and acquisition of data. A.C, M.B.L, G.KG contributed to the interpretation and analysis of the results. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors have no financial, commercial or competing interests to disclose.
References
1. Jakobsen LH, Øvlisen AK, Severinsen MT, et al. Patients in complete remission after R-CHOP(-like) therapy for diffuse large B-cell lymphoma have limited excess use of health care services in Denmark. Blood Cancer J. 2022;12(1):16. doi:10.1038/s41408-022-00614-8
2. Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood. 2006;107(1):265–276. doi:10.1182/blood-2005-06-2508
3. Hui D, Proctor B, Donaldson J, et al. Prognostic implications of extranodal involvement in patients with diffuse large B-cell lymphoma treated with rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone. Leuk Lymphoma. 2010;51(9):1–10. doi:10.3109/10428194.2010.504872
4. Fend F, Ferreri AJM, Coupland SE. How we diagnose and treat vitreoretinal lymphoma. Br J Haematol. 2016;173(5):680–692. doi:10.1111/bjh.14025
5. Uhr JH, Thau A, Chung C, Zhang XC. Rare Presentation of Bilateral Central Retinal Vein Occlusion and Leukemic Retinopathy in a Young Adult Diagnosed with T-cell Acute Lymphoblastic Leukemia. Cureus. 2020;12(1):e6666. doi:10.7759/cureus.6666
6. Mashayekhi A, Shields CL, Shields JA. Iris involvement by lymphoma: a review of 13 cases. Clin Exp Ophthalmol. 2013;41(1):19–26. doi:10.1111/j.1442-9071.2012.02811.x
7. Yoshida A, Watanabe M, Ohmine K, Kawashima H. Central retinal vein occlusion caused by hyperviscosity syndrome in a young patient with Sjögren’s syndrome and MALT lymphoma. Int Ophthalmol. 2015;35(3):429–432. doi:10.1007/s10792-015-0056-8
8. Rajagopal R, Apte RS. Seeing through thick and through thin: retinal manifestations of thrombophilic and hyperviscosity syndromes. Surv Ophthalmol. 2016;61(2):236–247. doi:10.1016/j.survophthal.2015.10.006
9. Brown DM, Campochiaro PA, Singh RP, et al. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a Phase III study. Ophthalmology. 2010;117(6):1124–1133. doi:10.1016/j.ophtha.2010.02.022
10. Alexander P, Flanagan D, Rege K, Foss A, Hingorani M. Bilateral simultaneous central retinal vein occlusion secondary to hyperviscosity in Waldenstrom’s macroglobulinaemia. Eye. 2008;22(8):1089–1092. doi:10.1038/eye.2008.193
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.