Back to Journals » International Medical Case Reports Journal » Volume 19
Bilateral Asymmetrical Presentation of Dead Bag Syndrome: A Case Report
Authors Alruwaili S ![]() , Alhaidari A, Alamoudi S
, Alhaidari A, Alamoudi S ![]() , Alamoudi R, Raheman SJ
, Alamoudi R, Raheman SJ
Received 13 February 2026
Accepted for publication 12 May 2026
Published 9 July 2026 Volume 2026:19 598625
DOI https://doi.org/10.2147/IMCRJ.S598625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Giuseppe Giannaccare
Shahad Alruwaili,1 Abdulmajeed Alhaidari,1 Saeed Alamoudi,1 Renad Alamoudi,2 Syed J Raheman1
1Fellowship and Residency Training Program, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia; 2College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Abdulmajeed Alhaidari, Fellowship and Residency Training Program, King Khaled Eye Specialist Hospital, Riyadh, 11462, Saudi Arabia, Email [email protected]
Background: Delayed complications after uneventful cataract surgeries may arise, including IOL (Intraocular Lens) dislocation. Among the rarest etiologies is Dead Bag Syndrome (DBS), a condition defined by the presence of a clear, transparent capsular bag accompanied by spontaneous posterior capsular rupture (PCR) occurring many years after cataract surgery. This late-onset PCR represents the most distinctive clinical feature of the syndrome.
Case Presentation: We report a case of healthy 69-year-old male presented to our Emergency Room (ER) complaining of sudden onset painless decreased vision in the left eye for 2 weeks. He has undergone uneventful cataract surgeries in both eyes. On examination, his uncorrected visual acuity (VA) in the right eye was 20/25 and in the left eye was 20/300. Slit-lamp Examination of the right eye showed vitreous prolapse in the anterior chamber, the IOL was in-situ, however, there was a central PCR. Fundus exam for the right eye was unremarkable. Examination of the left eye showed vitreous prolapse in anterior chamber, and the patient was aphakic with a central PCR. Fundus exam of the left eye showed healthy flat retina with a dislocated IOL. Patient underwent a successful Pars Plana Vitrectomy (PPV) + secondary IOL implantation with excellent visual outcome.
Conclusion: In conclusion, this case illustrates a rare bilateral manifestation of DBS and provides additional insight to this condition. It reinforces the importance of long-term postoperative monitoring and supports the recognition of DBS as a distinct pathological entity. With appropriate evaluation and tailored surgical intervention, satisfactory visual outcomes can be attained despite substantial capsular compromise.
Keywords: spontaneous PCR, IOL dislocation, dead bag syndrome, cataract
Introduction
Intraocular lens (IOL) implantation is the standard of care following cataract extraction, and in most cases provides stable and long-lasting visual rehabilitation. However, late complications such as IOL dislocation can occur, and among the rarest causes is dead bag syndrome (DBS). This entity is characterized by the presence of a transparent capsular bag many years after cataract surgery, which serves as its most distinguishing clinical hallmark.1
The long-term stability of the capsular bag IOL complex depends on the integrity of the zonular fibers. Several clinical conditions have been associated with progressive zonular weakening, including pseudoexfoliation, chronic uveitis, high myopia, systemic connective tissue disorders, previous pars plana vitrectomy, and ocular trauma.1 These risk factors highlight the importance of evaluating the underlying ocular and systemic milieu when assessing patients with unexplained late IOL subluxation.
Despite these associations, the exact cause of DBS remains uncertain. Competing hypotheses suggest that the initial pathology may reside within the capsule, triggering a cascade of lens epithelial cell (LEC) injury and capsular degeneration.2 Alternatively, degeneration may begin within the LECs themselves, with secondary weakening of the capsule. Another proposed mechanism involves late postoperative zonular failure caused by capsular splitting or delamination at the sites of zonular attachment.3 Importantly, DBS has not been linked to any particular IOL design or material, indicating that its pathogenesis is independent of lens type.
Histopathological studies have provided valuable insights. When DBS capsules were compared with those from 40 eyes with in-the-bag IOL dislocation, including 26 with confirmed Pseudoexfoliation, all specimens demonstrated the presence of LECs and Soemmerring’s ring formation, while capsulorhexis phimosis was also relatively frequent. By contrast, true capsular splitting or delamination was extremely rare, reported in only a single case.4,5
Diagnosis of DBS requires a high index of suspicion and relies on a careful, systematic evaluation. A comprehensive medical and surgical history, particularly relating to prior cataract surgery, should be obtained. Slit-lamp biomicroscopy is essential for assessing IOL centration and documenting the degree of subluxation. Other causes of IOL instability must also be excluded. For example, true exfoliation, typically associated with chronic exposure to heat or infrared radiation, may mimic the presentation.6 Similarly, pseudoexfoliation syndrome with its hallmark deposition of fibrillar material in the anterior segment, elevation of intraocular pressure, and progressive zonular instability remains a more common cause that should be differentiated from DBS.7
Management strategies depend on the extent of IOL subluxation. Patients with mild displacement may be observed with close follow-up, while those with severe subluxation generally require surgical intervention. In such cases, IOL exchange combined with anterior vitrectomy is recommended to restore stability and prevent secondary inflammatory complication.8
Dead bag syndrome remains a rare and under-recognized entity because of its uncertain pathogenesis and challenging diagnosis. Continued reporting of such cases is important to raise awareness, improve recognition, and guide management of this unusual cause of late IOL dislocation. Here, we describe a rare presentation of bilateral asymmetrical dead bag syndrome, with different management approach for each eye, contributing further insights into this uncommon condition.
Case Report
A healthy 69-year-old male, presented to our Emergency Room (ER) at King Khaled Eye Specialist Hospital (KKESH), Riyadh, Saudi Arabia. He was complaining of sudden onset painless decreased vision in the left eye for 2 weeks. There were no history of flashes or floaters or visual filed defects. He denied any history of trauma. He has undergone an uneventful phacoemulsification with posterior chamber IOL implantation in the right eye followed by the left eye in 2017 and 2019, respectively. Both surgeries were done at our hospital.
On examination, his uncorrected Visual Acuity (VA) in the right eye was 20/25 and in the left eye was 20/300. His Intraocular Pressure (IOP) in both eyes was 21 mmHg. Slit-lamp Examination (SLE) of the right eye showed normal lids with quiet conjunctiva, clear cornea, deep and quiet anterior chamber (AC) with vitreous prolapse in the AC, normal iris with normal pupil, no signs of pseudoexfoliation or trauma, the IOL was in place, however, there was a central posterior capsular rupture (PCR) (Figures 1–4). Dilated fundus exam showed flat retina with no breaks or retinal detachment (RD). SLE of the left eye showed similar findings anteriorly with vitreous prolapse in AC, normal iris and pupil, and no signs of pseudoexfoliation or trauma. The patient was aphakic with a central PCR similar to what was found in the right eye (Figure 5). Dilated fundus exam of the left eye showed healthy flat retina with a dislocated IOL that was also confirmed by B scan ultrasound (US) (Figure 6). Ultrasound Biomicroscopy (UBM) was also done, and it confirmed the status of aphakia in the left eye.
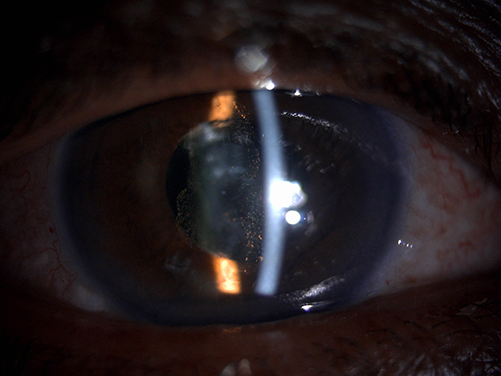 |
Figure 1 Slit-lamp photo of the right eye with slit-beam showing vitreous in anterior chamber. |
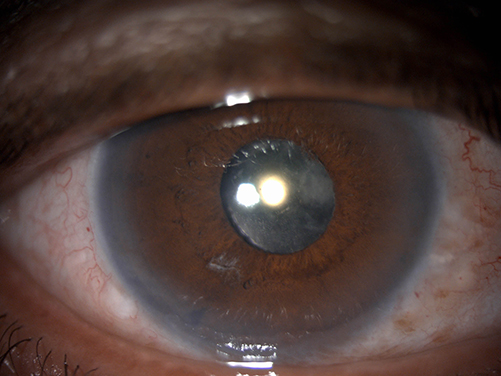 |
Figure 2 Slit-lamp photo of the right eye with diffuse illumination showing in-the-bag IOL reflection. |
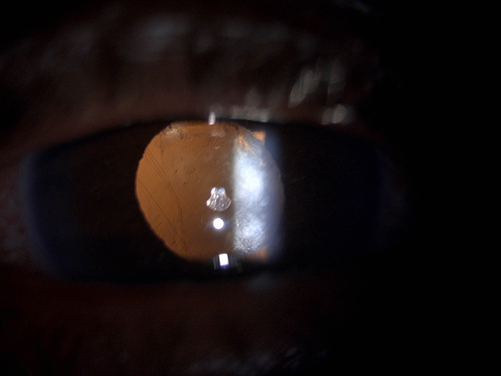 |
Figure 3 Slit-lamp photo of the right eye with retro-illumination showing posterior capsular rupture. |
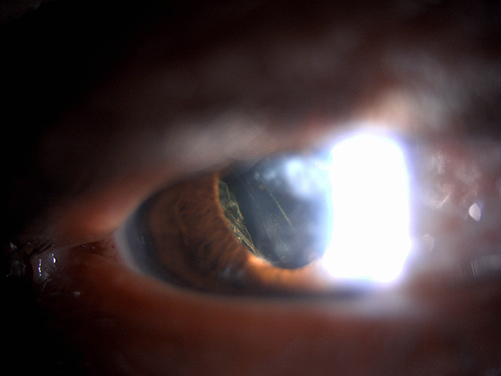 |
Figure 4 Slit-lamp photo of the right eye (right gaze) with direct-illumination showing posterior capsular rupture. |
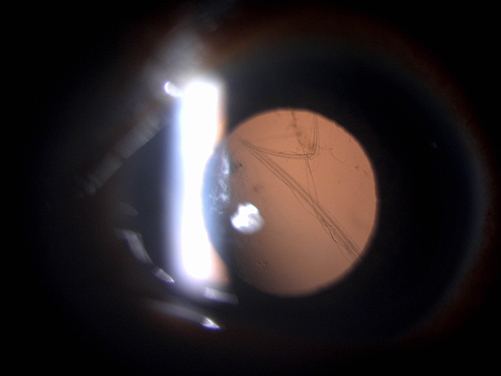 |
Figure 5 Slit-lamp photo of the left eye with retro-illumination showing posterior capsular rupture in aphakic eye. |
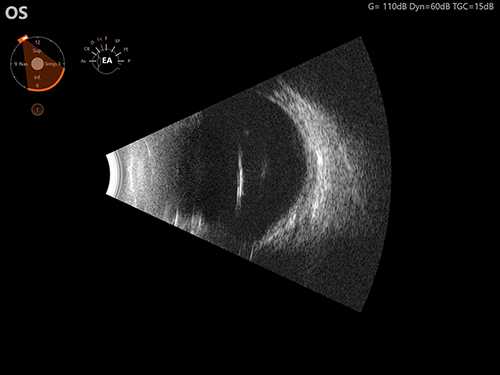 |
Figure 6 Ultrasound image of the left eye (transverse cut) showing inferotemporal highly reflective surface representing dislocated IOL. |
Patient has undergone an uneventful Pars Plana Vitrectomy (PPV) with secondary IOL implantation in the left eye. The dislocated IOL was cut and explanted through the main corneal wound. Yamane technique was implemented with an intrascleral fixation of a 3-Piece IOL. Two Scleral flaps were made 2 mm away from the limbus and 180 degrees apart, and scleral tunnels were made using MVR blade. Both haptics were externalized through the scleral tunnels, and the flaps were sutured with 10–0 nylon. One month later, his uncorrected VA in the left eye was found to be 20/20. SLE of the left eye showed a well-centered scleral-fixated IOL. SLE of the right eye showed the same clinical findings as previously mentioned with a stable in-situ IOL despite having the central PCR and prolapsed vitreous in the AC. As the patient is asymptomatic with 20/20 VA, the decision of observing the right eye with no intervention was made.
Spontaneous PCR in both eyes was consistent with what was described lately in literature as DBS.
Discussion
DBS is a rare late complication of cataract surgery characterized by progressive degeneration of the capsular bag.9 This degeneration results in the loss of LEC and the structural weakening and thinning of the posterior capsule. This creates a fragile intraocular environment that is vulnerable to IOL instability and spontaneous PCR, often years after an otherwise uneventful phacoemulsification procedure.4,9 Importantly, DBS does not directly cause PCR but predisposes the capsule to rupture under minimal mechanical stress or even spontaneously. In DBS, histopathological results reveal significant posterior capsule thinning and delamination as well as almost total LEC depletion, producing a “dead” capsular bag devoid of biomechanical resilience and regenerative potential.4 These characteristics distinguish DBS from other late-stage postoperative complications such as capsular contraction syndrome or pseudoexfoliation-related zonulopathy.
In our patient, Bilateral spontaneous PCR occurred several years after routine cataract surgery, with no known risk factors such eye trauma, pseudoexfoliation, uveitis, or systemic connective tissue disorders. This case’s idiopathic and bilateral characteristics are consistent with rare but documented DBS presentations, pointing to a possible individual predisposition or underlying systemic factors that are still poorly understood.4,9,10 Since bilateral involvement is still very uncommon, it is crucial to consider DBS as a potential cause, even in healthy eyes. Clinically, DBS often presents with sudden, painless visual decline due to posterior capsule rupture, anterior vitreous prolapse, and IOL dislocation. Diagnosis is based on slit-lamp examination revealing vitreous strands in the anterior chamber and a ruptured posterior capsule, often supported by B scan US and UBM to rule out retinal pathology and IOL position abnormalities, respectively. Our patient exhibited these findings bilaterally, consistent with the classic clinical picture of DBS.9
PPV with secondary IOL implantation is the usual surgical treatment; when done promptly, this procedure is linked to positive visual results. In our instance, scleral-fixated IOL implantation and PPV were performed on the left eye, yielding a 20/20 visual acuity. A similar approach was described by Thakur et al, who reported late-onset intra-bag IOL subluxation in the absence of risk factors, successfully managed with scleral fixation of IOL and achieving a favorable visual outcome.10 Despite having a central PCR, the right eye was observed and it maintained good visual acuity with an in-situ IOL, highlighting the significance of individualized clinical decision-making.10
While bilateral DBS has been documented previously,9,11 our case is unique in that the patient was fully systemically healthy, presented with spontaneous posterior capsule rupture in both eyes within a short period of time, and displayed asymmetrical symptoms. Furthermore, both eyes had excellent visual results, making this a novel and valuable addition to the restricted data on idiopathic bilateral DBS.9,11 This case highlights the value of long-term postoperative surveillance, even in cases of simple cataracts, and adds to the body of literature on DBS, particularly its bilateral manifestation. Early diagnosis and better surgical planning may be possible for patients with DBS, as it is recognized as a separate cause of late-onset IOL instability and PCR. Our case report has inherent limitation as it cannot establish causality or generalize the findings to a broader population. Additionally, diagnosis of DBS was made on clinical grounds, as histopathological confirmation of the capsular bag was not obtained.
Conclusion
Dead Bag Syndrome is a critical yet rare differential diagnosis for late spontaneous posterior capsule rupture, even in healthy patients with uncomplicated cataract surgery. The bilateral and idiopathic nature of this entity underscores the potential for an underlying individual predisposition that is not yet completely understood. Despite significant structural complications, excellent visual outcomes can be achieved through careful clinical assessment and tailored surgical intervention. This report emphasizes the importance of long-term postoperative follow-up and contributes to the growing body of knowledge on DBS as a distinct clinical entity.
Abbreviations
IOL, intraocular lens; DBS, dead bag syndrome; LEC, lens epithelial cells; ER, emergency room; KKESH, King Khaled Eye Specialist Hospital; VA, visual acuity; IOP, intraocular pressure; SLE, slit-lamp examination; AC, anterior chamber; PCR, posterior capsular rupture; RD, retinal detachment; US, ultrasound; UBM, ultrasound biomicroscopy; PPV, Pars Plana Vitrectomy.
Data Sharing Statement
All data supporting the findings of this case report are available within the manuscript.
Ethics Approval and Consent to Participate
This case report was performed in accordance with the Declaration of Helsinki. Institutional approval was required to publish the case details and was obtained from the Institutional Review Board at King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia (reference: RD/26001/IRB/0757-25). Written informed consent was obtained from the patient to participate in this report and clinical assessments as relevant to this publication.
Consent for Publication
Consent to publish this case report has been obtained from the patient.
Funding
This study was conducted without any funding or financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moshirfar M, Moin KA, Ronquillo Y. Dead bag syndrome. In: StatPearls. Treasure Island (FL):StatPearls Publishing;2025. http://www.ncbi.nlm.nih.gov/books/NBK606108/.
2. Shentu XC, Zhu YN, Gao YH, Zhao SJ, Tang YL. Electron microscopic investigation of anterior lens capsule in an individual with true exfoliation. Int J Ophthalmol. 2013;6(4):553–6. doi:10.3980/j.issn.2222-3959.2013.04.27
3. Danysh BP, Duncan MK. The lens capsule. Exp Eye Res. 2009;88(2):151–164. doi:10.1016/j.exer.2008.08.002
4. Culp C, Qu P, Jones J, et al. Clinical and histopathological findings in the dead bag syndrome. J Cataract Refract Surg. 2022;48(2):177–184. doi:10.1097/j.jcrs.0000000000000742
5. Liu E, Cole S, Werner L, Hengerer F, Mamalis N, Kohnen T. Pathologic evidence of pseudoexfoliation in cases of in-the-bag intraocular lens subluxation or dislocation. J Cataract Refract Surg. 2015;41(5):929–935. doi:10.1016/j.jcrs.2014.08.037
6. Senthilkumar V, Krishna M, Krishnadas R. True exfoliation with double delamination of the anterior lens capsule. Indian J Ophthalmol. 2020;68(5):919. doi:10.4103/ijo.IJO_1631_19
7. Olawoye OO, Pasquale LR, Ritch R. Exfoliation syndrome in Sub-Saharan Africa. Int Ophthalmol. 2014;34(5):1165–1173. doi:10.1007/s10792-014-9953-5
8. Darian-Smith E, Safran SG, Coroneo MT. Lens epithelial cell removal in routine phacoemulsification: is it worth the bother? Am J Ophthalmol. 2022;239:1–10. doi:10.1016/j.ajo.2022.01.013
9. Nayak R, Pai HV, S S. Bilateral dead bag syndrome. JCRS Online Case Rep. 2024;12(2):e00119. doi:10.1097/j.jcro.0000000000000119
10. Thakur A, Bansal M, Challa D, Malhotra C, Jain AK. Dead bag syndrome—in-the-capsular-bag subluxated intraocular lens centration and refixation: a new technique. Indian J Ophthalmol. 2023;71(10):3412–3414. doi:10.4103/IJO.IJO_1061_23
11. Banerjee P, Priya S, Khan S, Chowdhury M. Bilateral dead bag syndrome in skeletal dysplasia: a case report and review of literature. Taiwan J Ophthalmol. 2024. doi:10.4103/tjo.TJO-D-23-00088
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.