Back to Journals » International Medical Case Reports Journal » Volume 13
Big Bag IOL Implantation with Scleral Fixation Technique in IOL/Crystalline Lens Subluxation/Luxation Cases and High Myopia
Received 12 June 2020
Accepted for publication 24 July 2020
Published 26 August 2020 Volume 2020:13 Pages 383—389
DOI https://doi.org/10.2147/IMCRJ.S267180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Raffaele Nuzzi, Francesca Monteu
Department of Surgical Sciences, University Eye Clinic, Molinette Hospital, Torino, Italia
Correspondence: Francesca Monteu
Clinica Oculistica Universitaria, Dipartimento di Scienze Chirurgiche, Città della Salute e della Scienza, presidio Molinette, via Cherasco 23, Torino 10126, Italia
Tel +39 347 9949826
Fax +39 011 2485708
Email [email protected]
Purpose: The aim of this study is to report our experience in the surgical management of over 180° luxation/subluxation of the intraocular lens (IOL). Special cases are high myopic eyes, whose tissues are constitutionally more fragile, and consequently, surgery is more dangerous.
Patients and Methods: The authors propose the use of the Big Bag, three loops, IOL (Zeiss), to be implanted with the scleral fixation technique, with a double-armed needle. This technique seems to improve IOL stability and visual outcome of these patients.
Results: Big Bag IOL implantation with the scleral fixation technique in eyes with subluxation (over 180°) of the cataractous lens, high myopia and subluxation/dislocation of the IOL seems to suggest a possible and optimal management, with good long-term results and it is well tolerated by the patient.
Conclusion: This specific ocular surgical technique can be used/standardized in all surgical “converted” complicated cases and especially in high myopic eyes.
Keywords: Big Bag IOL, high myopia, scleral fixation, subluxation/luxation lens/IOL
Introduction
In eyes with high myopia it is easier to find cases of cataract subluxation/luxation or IOL (intraocular lens) subluxation/luxation. In these cases it is frequently decided to implant IOL using the scleral fixation technique. The authors propose the use of the Big Bag, three loops, IOL (Zeiss), to be implanted with the scleral fixation technique, with a double-armed needle, to improve IOL stability and visual outcome of these patients.
Case Report
A 92-year-old woman presented with a history of high myopia since childhood; at the age of 20 she had suffered a left eye trauma, which caused low vision.
In 1990 she was diagnosed with a senile maculopathy in both eyes; in 2004 she underwent phacoemulsification and IOL implantation in both eyes; then, in April 2014 she was hospitalized for subluxated IOL in the right eye, and we proceeded with the removal of the IOL.
In June 2015 the visual acuity for the right eye was hand motion, 20/500 with +10 sph, and the visual acuity for the left eye was 20/200, 20/100 with −4 cyl120. She was hospitalized for IOL and capsular bag subluxation/dislocation in toto in the left eye; the IOL and capsular bag were removed and Big Bag IOL implantation with the scleral fixation technique was performed in the left eye (optical biometry + ultrasonic biometry – Holladay).
In August 2015 she was hospitalized for Big Bag IOL implantation with the scleral fixation technique in surgical aphakia and high anisometropia in the right eye (Figures 1–5).
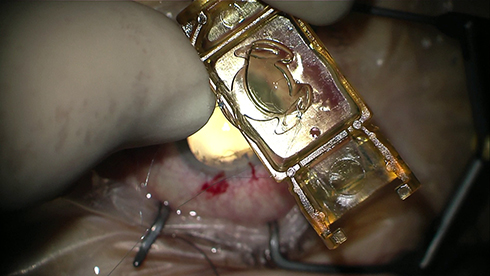 |
Figure 1 Big Bag IOL (Zeiss) and just anchored to the IOL loops prolene wires. |
 |
Figure 2 The insertion of the IOL. |
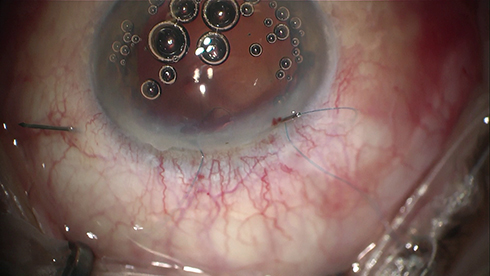 |
Figure 3 Scleral anchoring. |
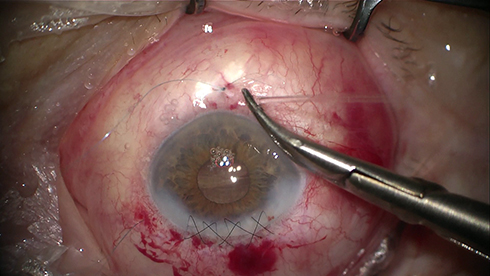 |
Figure 4 Prolene suture with double-armed needles, covered by conjunctiva. |
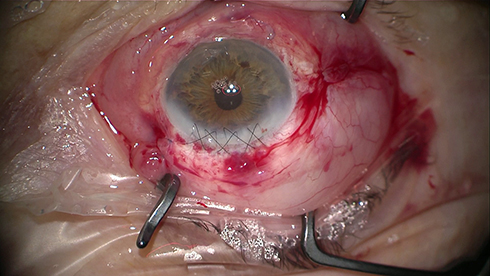 |
Figure 5 Final result. |
One month after surgery (September 2015) the right eye visual acuity was 20/320 with −0.75sph −3.50 cyl15, and the left eye visual acuity was 20/63 with −2.50 sph −6.50 cyl160. We did not observed iridodonesis or phacodonesis or displacement of the IOL.
The intraocular pressure was in range (10–18 mmHg with Goldmann tonometer) during all of the controls (1 day – 7 days – 1 month – 2 months – 6 months – 1 year after the surgery).
The visual acuity remained stable, the patient did not have retinal or surface complications and we did not observe phacodonesis of the IOL or displacement of the IOL during all the follow-up period (from 1 month to 1 year after the surgery) (Figures 6–10).
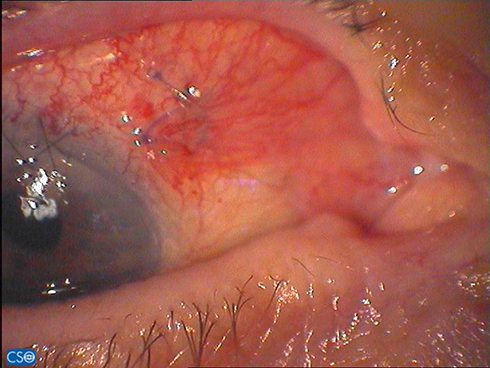 |
Figure 6 Right eye nasal scleral sutures, 15 days after surgery. |
 |
Figure 7 Left eye temporal scleral sutures, 15 days after surgery. |
 |
Figure 8 Left eye inferior scleral sutures, 15 days after surgery. |
 |
Figure 9 Left eye nasal scleral sutures, 15 days after surgery. |
 |
Figure 10 Anterior segment slit lamp photo, 30 days after surgery. |
We valued the IOL stability, studying the absence of iridodonesis, phacodonesis, verifying the IOL stability during the eye movements both in miosis then in mydriasis and taking photos of the anterior segment during all the follow-up times. Then, we valued the visual acuity stability during the follow up, the IOL centering both in miosis then in mydriasis, the pupil regularity also after dilatation with mydriatic drugs, the absence of metamorphopsias and the negative Amsler test as well as the absence of glare effect and optic aberrations.
A written informed consent letter has been signed by the patient to allow any case details and any accompanying images to be published. Based on our hospital policy, Institutional Review Board (IRB) approval was not required to publish the case details as it was a case report.
Discussion
High myopic eyes show some typical alterations due to thinning and degeneration of eye layers, chorioretinal atrophy and posterior staphyloma.
High-resolution magnetic resonance imaging studies demonstrated that myopic eyes are larger in the three dimensions (equatorial, anteroposterior and vertical axes). The results suggest that during myopic progression an overall enlargement or a radial volume expansion has occurred.1
Because of these characteristics, also the zonular fibers are longer and have to support greater stress than the ones in a normal axial-length eye.2
Abnormally loose zonules in highly myopic eyes, during phacoemulsification, cause the known “lens–iris diaphragm retropulsion syndrome”. This syndrome requires an infusion of fluid into the anterior chamber and it is characterized by posterior displacement of the lens–iris diaphragm, marked deepening of the anterior chamber, posterior iris bowing, pupil dilation and often significant patient discomfort.3
The spontaneous luxation of the lens is a rare ocular disease. There are three forms of this pathology: hereditary, great myopia correlated and senile cataract correlated.4
IOL subluxation means an incomplete intraocular lens displacement from its normal anatomical position. It may be due to an incorrect placement of the IOL during the implant, to the occurrence of an intraoperative complication, to a defect of the lens, such as a loop deformed by the injector, to a displacement of the IOL in the postoperative time, due to laxity of the zonules, trauma, failure of the zonules and retraction of the capsular bag. The subluxation can consist of a displacement along the anteroposterior axis, on a plane perpendicular to the anteroposterior axis (or decentralization), in a rotation of a meridian (or tilting) or in an association between these.
The optical function of an IOL is linked to its position in relation to the axis of vision, to the cornea and to the retina; a backward movement of the IOL causes a hyperopic refractive error, a forward movement causes a myopic refractive error.
Merlin5 has shown that the variation in the refraction caused by a dislocated IOL is linked to the power of the IOL; in case of an IOL of 26 D, a displacement of 0.1 mm results in a variation of the refraction about 0.15 D. This value is directly proportional to the dioptric power of the IOL, thus it increases for high power IOL and is reduced to a few hundredths of a diopter for lens power close to zero.
In the case of decentralization of the IOL the situation is different: the IOL optical function is carried out to the maximum if its main planes are perpendicular to the optical axis of the eye and its optical axis coincides with the optical axis of the eye, but if the IOL is decentralized it determines optical aberrations, coma, directly proportional to the power of the IOL and to the distance of the optical center to the axis of the vision. The consequence is represented by qualitative disorders of vision not correctable with lenses.
It is possible to classify subluxations in the bag (in the bag IOL dislocation) and out of the bag (out of the bag dislocation).
In the first case, possible causes are pseudoexfoliation, retinitis pigmentosa, vitrectomized eye, previous trauma and axial length greater than normal.
In the second case, possible causes are secondary IOL implants, surgical complications, mature cataracts and pseudoexfoliation (PEX).6
PEX is likely to produce zonular insufficiency by two mechanisms. First, PEX accumulations mechanically weaken the zonular lamella and impair zonular anchoring to the epithelial basal membrane at both its origin and insertion. Furthermore, patients with PEX also exhibit an increase in elastinolysis that weakens the zonula. Second, PEX has been shown to facilitate the anterior capsule contraction syndrome, that if left untreated usually leads to zonular failure.2
In the case of IOL decentralization the management can be:
In the case of complete dislocation of the IOL in the vitreous, surgery is instead considered, because of the visual decrease warned by the patient and the possible retinal complications (fluctuating IOL in the vitreous, vitreous hemorrhage/cystoid macular edema, IOL contact with the retina, tractions and retinal detachment).
If there are signs of inflammation or IOL instability with the risk of retinal detachment, surgery is the gold standard.
It will carry out the removal of the IOL and replanting in the bag if more than 6 hours of the lower portion of the bag are undamaged, otherwise the removal of the IOL and replanting with scleral fixation or anterior chamber implantation.7
According to Smiddy et al,8 the timing of intervention has no effect on the outcome of vision.
The scleral fixation technique was described for the first time by Malbran in 1986: this is an ab externo technique which consists of hooking IOL loops to the sclera by needles covered by two closed sclerotomies which have the purpose of protecting knot erosion and exposure.
Over the years, several authors have proposed variations of the original technique that differ primarily in the surgical approach (ab externo or ab interno), for the fixation technique of the loop, by the number of sutures performed (two to four) and for the method which should prevent the erosion of suture wires in time.
In 1991, James S. Lewis published in Ophthalmology a variation of the original technique in which sutures are covered only by conjunctiva, without scleral flaps. Nuzzi has changed it, maintaining a prolene suture with double-armed needles and then anti-lysis/anti-erosion with wire ends after knotting kept deliberately very long (Figure 4). This technique is to be related to the consistency of the scleral wall as well as to the number of interventions previously performed.
The scleral fixation implantation needs loop anchorage to the sclera with two scleral flaps at 3 and 9 o’clock (rarely it is preferable to anchorage at 6 and 12 o’clock) with 10/0 prolene suture (not absorbable polypropylene), single or doubl-armed with a long straight or curved needle. Scleral flap function is to allow the burial of the loop fixation node.
This technique's advantages are related to the IOL positioning in the posterior chamber, thus reducing the risk of complications related to an implant in the anterior chamber (endothelial cell progressive depletion, synechiae resulting in pupil deformation, elevation of intraocular pressure, chronic inflammatory states).
The scleral fixation implantation is subjected to different technique changes based on the choices of the surgeon and there are numerous variations in the international literature. Every technique begins with a conjunctival peritomy followed by the deployment of two scleral flaps at 3 and 9 o’clock.
Ab Externo Technique with Two Prolene Single Double-Armed Wires with Straight Needle
A sclerocorneal cut about 7 mm is made, and then the straight needle is passed from the flap, about 1.5 mm from the limbus, to the limbus at 12 o’clock; the procedure is repeated at 3 o’clock. Then, the 10/0 prolene wire is anchored to the IOL loop. The opening of the anterior chamber is performed, with eventual introduction of any air bubble to better assess the presence of vitreal fibrils. Making an anterior vitrectomy, the viscoelastic in the anterior chamber is introduced; then, the IOL is introduced and the scleral fixation is made. The viscoelastic substance from the anterior chamber is removed, and corneal and conjunctival sutures are made.
Ab Externo Technique with Single Prolene Double-Armed Wire with Straight Needle
Making a sclerocorneal cut, the straight needle is introduced to the flap and using as a guide an insulin needle from the controlateral flap the needle escape from the sulcus is facilitated. A paracentesis is created at the level of pre-cut, allowing to bring out a loop of prolene wire; the loop of prolene is cut and two heads are fixed to the loops of the IOL. Then, the paracentesis is widened throughout the whole incision; the IOL is introduced after filling the anterior chamber with viscoelastic substance and the scleral anchoring is done. Therefore, the viscoelastic substance is removed from the anterior chamber, and cornea and conjunctiva sutures are made.
Ab Interior Technique with Two Prolene Loop Wires with Curved Long Needle
At first, you have to affix one of the end of the 10/0 prolene wire to the loop of the IOL; then, you have to open the anterior chamber and to do an anterior vitrectomy and to introduce the viscoelastic. The ab interior introduction of the curved needle below the plane of the iris is done, making it come out from the flap, and the procedure is repeated contralaterally; therefore, you have to introduce the IOL. Then, you have to affix the scleral anchor point after cutting a head of the prolene loop. Thereby, after the removal of the viscoelastic substance from the anterior chamber, corneal and conjunctival sutures are made.
The erosion of sutures due to exposure has always been a topic of discussion about the IOL stability in the long term, with the possible risk of decentration, tilting and dislocation into the vitreous cavity.
According to Cavallini et al,9 in a study of 13 patients who underwent Lewis’s scleral fixation technique, with a follow up to 129 months there were no significant complications like dislocation into the vitreous cavity. The erosion of the sutures is not common, but the IOL remains stable over time for a fibrotic process of sutures and loops, which prevents IOL displacement.
The largest proportion of the complications related to the scleral fixation is related to malpositioning and wrong tension of the sutures and improper use of IOL that do not have eyelets in the loops.
You can identify three groups of complications:10
Many IOL models for scleral fixation techniques are commercially available. The peculiarity of these IOLs consists of the presence of eyelets at the ends of the two loops to enable the anchoring of the prolene wire to the IOL. They have been placed on the market as also folding scleral fixation IOL, allowing a corneal cut less wide than PMMA IOL. It is possible, however, to use capsular bag IOL with acrylic handles in specific cases.11
In our case, the need for an 8 D IOL for the right eye and a 7 D (K121) for the left eye in high myopia led us to choose the use of a Big Bag, one-piece foldable acrylic IOL (overall diameter 10.35 mm, meniscus optical diameter 6.5 mm, three closed-loop haptic IOL). This lens is used preferentially in high myopic eyes because the three haptic configuration seems to prevent lateral IOL dislocation while the larger optical diameter minimizes the risk of symptoms related to the edge of the IOL.
The particularity of this lens is its “Y “shape, three closed-loop haptic configuration. Then, the anchorage is through three haptics, unlike other two-haptic IOLs, with a marked improvement in stability and centering of the IOL. It was therefore tried to keep the lens more anteriorly to avoid a hypermetropization due to the concavity of the lens and to gain more stability.
Indeed, the stability improvement is obtained by both the 240° anchorage and the haptic ending wider contact with the pars plana. In this way, the IOL is more centered and it has a lower risk of dislocation than the traditional twohaptic surgery. In addition, traditional IOLs are always fixed by 10/0 prolene, without scleral tunnel or glue because of their instability risk.
In our specific case it was chosen to use a prolene 9/0, because it used a double-folded wire, to prevent/reduce the risks of lysis/erosion over time.
The advantages of our technique, compared to the traditional sclera fixation techniques, were that we used the same approach of a foldable IOL, with a corneal incision with a smaller diameter, with a lesser anterior vitreal protrusion and, theoretically, with a lower retinal detachment risk. Then, we obtained major stability during the correction of high myopias because of the wider 240° support obtained by the three windowed flat haptics, which offered a 240° contact, with an optic place diameter of 6.5 mm (while the optic place diameter of many scleral fixation foldable IOLs is 6 mm). The haptic had an inwards opened parenthesis shape, therefore they were less traumatizing.
The IOL posterior convexity held the vitreous and, if present, the posterior capsule in place and stabilized the capsular bag, if present, dehiscence.
Then, we had a hypothetically minor risk of increased intraocular pressure (and secondary glaucoma) during the postoperative time and during the follow up, and a minor risk of cystoid macular edema, because of a minor vitreal reactivity induction.
Conclusion
In conclusion, Big Bag IOL implantation with the scleral fixation technique in eyes with subluxation (over 180°) of the cataractous lens, high myopia and subluxation/dislocation of the IOL seems to suggest a possible and optimal management, with good long-term results and it is well tolerated by the patient. This specific ocular surgical technique can be used/standardized in all surgical “converted” complicated cases and especially in high myopic eyes.
Moreover, there is a need for further studies to evaluate limits and indications in a larger share of the population.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cheng HM, Singh OS, Kwong KK, Xiong J, Woods BT, Brady TJ. Shape of the myopic eye as seen with high-resolution magnetic resonance imaging. Optom Vis Sci. 1992;69:698–701. doi:10.1097/00006324-199209000-00005
2. Fernandez-Buenaga R, Alio JL, Perez-Ardoy AL, et al. Late in-the-bag intraocular lens dislocation requiring explantation; risk factors and outcomes. Eye (Lond). 2013;27:795–801. doi:10.1038/eye.2013.95
3. Cionni RJ, Barros MG, Osher RH. Management of lens-iris diaphragm retropulsion syndrome during phacoemulsification. J Cataract Refract Surg. 2004;30:953–956. doi:10.1016/j.jcrs.2004.01.030
4. Redor JY, Liber M, Huet JF, Henry J. [Spontaneous bilateral lens luxation]. Ophtalmologie. 1989;3:89–90. French.
5. Merlin U. [IOL dislocations]. In: Buratto L, editor. [Cataract Surgery in Complicated Cases]. Slack Incorporated; 1991:387–420. Italian.
6. Hayashi K, Hirata A, Hayashi H. Possible predisposing factors for in-the-bag and out-of-the-bag intraocular lens dislocation and outcomes of intraocular lens exchange surgery. Ophthalmology. 2007;114:969–975. doi:10.1016/j.ophtha.2006.09.017
7. Tassinari P, [Management of Luxated/Subluxated IOLs].
8. Smiddy WE, Ibanez GV, Alfonso E, Flynn HW. Surgical management of dislocated intraocular lenses. J Cataract Refract Surg. 1995;21:64–69. doi:10.1016/S0886-3350(13)80482-8
9. Cavallini GM, Volante V, De Maria M, et al. Long-term analysis of IOL stability of the Lewis technique for scleral fixation. Eur J Ophthalmol. 2015;25:525–528. doi:10.5301/ejo.5000652
10. Tassinari G. [Management of the complications]. La Voce Aiccer. 2014;4:54–57. Italian.
11. Agrawal S, Singh V, Gupta SK, Misra N, Srivastava RM. Transscleral fixation of closed loop haptic acrylic posterior chamber intraocular lens in aphakic nonvitrectomized eyes. Indian J Ophthalmol. 2015;63:649–653. doi:10.4103/0301-4738.169797
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.