Back to Journals » Patient Preference and Adherence » Volume 20
Bidirectional Longitudinal Associations Among Health-Related Quality of Life, Emotional Expressivity, and Readiness to Return to Work in Patients with Non–Muscle-Invasive Bladder Cancer Receiving Intravesical Therapy: A Three-Wave Cohort Study
Received 6 January 2026
Accepted for publication 26 March 2026
Published 9 April 2026 Volume 2026:20 594081
DOI https://doi.org/10.2147/PPA.S594081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mingming Zhang,1 Yi Zhou2
1Department of Nursing, Shanghai General Hospital, Shanghai, People’s Republic of China; 2Department of Urology, Shanghai General Hospital, Shanghai, People’s Republic of China
Correspondence: Mingming Zhang, Email [email protected] Yi Zhou, Email [email protected]
Purpose: We aimed to elucidate the temporal relationship among health-related quality of life(HRQoL), emotional expressivity, and readiness for return to work(RRTW) in patients with non–muscle-invasive bladder cancer receiving intravesical therapy.
Design: A three-wave cohort study.
Methods: In this prospective observational study, we recruited 425 patients from two tertiary hospitals between August 2022 and January 2024. Three waves of self-reported questionnaires were administered at the start of at the start of intravesical therapy (T1, N=412), at six months (T2, N=309), and at twelve months (T3, N=227). The main analysis was based on data from patients who completed all three waves of the assessment. We constructed cross-lagged panel models to examine the temporal associations among HRQoL, emotional expressivity, and RRTW.
Results: A total of 227 patients completed all three waves of assessment. Controlling for covariates such as intravesical therapy medication, age, gender, economic income, and marital status, the results indicated a longitudinal relationship between HRQoL at T1 and T2 and emotional expressivity and RRTW at T2 and T3. Emotional expressivity at T1 and T2 was positively associated with HRQoL and RRTW at T2 and T3. HRQoL and emotional expressivity were mutually reinforcing relationships. RRTW at T1 and T2 was positively associated with HRQoL at T2 and T3; however, this positive association disappeared after emotional expressivity was added. Mediation analyses revealed that HRQoL at T1 was positively associated with RRTW at T3 through emotional expressivity at T2 (standardized indirect effect=0.020, 95% bootstrap CI [0.005, 0.035]).
Conclusion: These results demonstrated that HRQoL and emotional expressivity mutually reinforced effect relationships, and both could facilitate RRTW among non–muscle-invasive bladder cancer receiving intravesical therapy. As an observational study, these findings identify potential targets for intervention but require confirmation in experimental designs.
Keywords: non-muscle-invasive bladder cancer, receiving intravesical therapy, readiness for return to work, health-related quality of life, emotional expressivity
Introduction
Bladder cancer is the most common malignant tumor of the urinary system, with 70–80% of cases of non-muscle-invasive bladder cancer (NMIBC). Notably, an increasing number of young people are being diagnosed.1 Receiving intravesical therapy is an important treatment for NMIBC, with a treatment cycle of 1–3 years.2 China’s socio-demographic aging, delayed retirement policy, and labor supply constraints have led to a growing problem of return to work (RTW) for people with illnesses after or during treatment, which is defined as returning to their previous or other job and undertaking the corresponding work tasks after recovery from the disease.3 For NMIBC patients who were in the workforce prior to treatment, returning to work not only signifies successful recovery from the disease and reintegration into the family and social environment but also reduces labor tensions to some extent, which is of great practical importance.
Franche et al4 proposed the concept of readiness for return to work(RRTW) and developed the “readiness for return to work scale(RRTWS)” to measure patients readiness to return to work, including their willingness and confidence in RTW Franche noted that RRTW occurs throughout the transition from illness to recovery and is divided into six stages, including the precontemplation stage, contemplation stage, action preparation stage, action stage, uncertain maintenance stage and maintenance stage, with different stages of behavioral change representing different levels of readiness. RRTW is the first and critical step that has a huge impact on a patient’s successful return to work. The RRTW level will influence how quickly and when return to work occurs, so clarifying the RRTW level will allow for accurate and optimal timing of the patient’s return to work. Currently, studies have shown that the level of RRTW in patients with cancer remains suboptimal, indicating a significant need for intervention. Ghasempour et al5 assessed 227 cancer patients and found that 68.47% of the patients were in the precontemplation stage; Petersen et al6 conducted qualitative interviews with 13 breast cancer patients and found that they could not prepare for action to return to work; Wang Liying et al7 assessed middle-aged cancer patients and showed that 30.7% of the 212 patients who did not return to work were in the precontemplation stage; Yang Lijun et al8 assessed 158 breast cancer patients and showed that 36.7% of the patients were in the precontemplation stage. In summary, it can be seen that RRTW is generally at a low level, therefore, identifying the factors that promote RRTW has important theoretical and practical significance.
Emotional expressivity refers to the tendency and intensity with which individuals outwardly display their emotional experiences through verbal and non-verbal channels.9 In the context of chronic illness and cancer care, emotional expressivity has been recognized as a key indicator of psychological adjustment, as it facilitates social communication and elicits supportive responses from others.10 For patients with non-muscle-invasive bladder cancer (NMIBC) undergoing intravesical therapy (eg., BCG or mitomycin C instillation), the treatment regimen typically spans 6 weeks to several months, involving repeated hospital visits and invasive procedures. This prolonged and repetitive treatment cycle can evoke significant emotional responses, including anxiety, embarrassment, fear of recurrence, and treatment-related discomfort. However, unlike patients with other cancer types who may have more opportunities for spontaneous emotional expression during clinical encounters, NMIBC patients often experience limited interaction with healthcare providers due to the brief and procedure-focused nature of intravesical therapy sessions.11 Consequently, their emotional concerns may remain unspoken, potentially affecting their health-related quality of life (HRQoL) and readiness to return to work. Despite the theoretical importance of emotional expressivity in oncology settings, its role in the specific context of intravesical therapy for NMIBC remains underexplored. Understanding how emotional expressivity interacts with HRQoL and return-to-work readiness over time may provide valuable insights for developing targeted psychosocial interventions for this unique patient population.
Prochaska et al12 proposed the dynamic theory “Readiness for Change Model” to describe the mental and behavioral processes of an individual or organization in the face of change. The model aims to address motivational factors that contribute to maintaining behavioral change, and its application to RTW emphasizes that the stages of behavioral change in a patient’s return to work are dynamic, with different influences at different stages, and that the influences do not end with a change in behavior. Our previous study based on the Readiness to Change Model showed that health-related quality of life (HRQoL) and emotional expressivity of non–muscle-invasive bladder cancer receiving intravesical therapy were influential factors in the process of returning to work.13 Meanwhile, there is ample evidence to support that emotional expressivity and health-related quality of life are key determinants of RRTW.5,14
However, The current research has several limitations. First, most studies, including our previous research, which mostly used cross-sectional or qualitative study designs, make it difficult to reveal the temporal relationship between HRQoL, emotional expressivity, and RRTW. Second, the Readiness for Change Model provides a conceptual framework that considers emotional expressivity as a key factor in RRTW, but in clinical practice, the consideration of emotional expressivity factors is often criticized for blaming the patient for the failure to return to work.15 Although ample evidence supports emotional expressivity as a key determinant of RRTW, there has been no systematic investigation into the changes in emotional expressivity during the treatment cycle. Therefore, these pieces of evidence have limited help in addressing patients’ psychological distress and RRTW. Third, most studies focus on patients’ postoperative recovery and on patients receiving regular outpatient receiving intravesical therapy, which may vary the correlation among factors.We used a longitudinal design to explore the temporal relationship between HRQoL, emotional expressivity, and RRTW in patients with receiving intravesical therapy. Cross-lagged panel modeling (CLPM) has been shown in many studies to have good utility in testing the interaction effects of variables in studies with longitudinal designs, as well as being an effective tool for testing possible bidirectional time correlations between different variables while also supporting mediation factor analysis.16 Given the repetitive, outpatient nature of intravesical therapy for NMIBC—which involves brief, procedure-focused visits that may limit spontaneous emotional interaction with healthcare providers—a patient’s RRTW may be even more pessimistic.we hypothesized that there is an interrelationship between HRQoL and RRTW, and emotional expressivity would play a critical role in maintaining psychosocial resources and facilitating readiness to return to work over the 12-month treatment cycle.
Methods
Participants
A prospective observational study design was used. Patients receiving outpatient receiving intravesical therapy who were treated in two tertiary hospitals from August 2022 to January 2024, Study protocol was approved by the Ethics Committee (2024394). Inclusion criteria: (1) histopathology of non-muscle invasive bladder cancer and in accordance with the risk categories and treatment guideline recommendations of the expert consensus on receiving intravesical therapy (2021edition); (2) 18 years≤age≤ 65years; at work prior to the procedure; (3) receiving intravesical therapy medication prescription of BCG or mitomycin C; (4) patients were voluntarily enrolled and family members or patients signed an informed consent form; and (5) ability to read, write, or articulate clearly. Exclusion criteria: (1) combined other malignant tumors; (2) pregnancy; and (3) post-urethral reconstruction or bladder mobility syndrome or severe urinary incontinence.425patients were initially enrolled, 412 completed the baseline assessment (T1), and 227 completed all three waves (T3).
Receiving Intravesical Therapy Procedure
The receiving intravesical therapy procedure was performed on an outpatient basis after long-term prescription by the medical team; an immediate receiving intravesical therapy procedure was performed in NMIBC patients within 24 hours after electrodesiccation, and the first induction receiving intravesical therapy procedure was performed on an outpatient basis after one month of discharge, once/week for a period of 8 weeks. The maintenance receiving intravesical therapy procedure was performed once per month for a period of 12–36 months. The bladder was emptied before receiving intravesical therapy, and the drug was solubilized and injected into the bladder through a disposable catheter, retained for 2 h, excreted, and subjected to uniform chemical treatment. Patients were rechecked for cystoscopy every 6 months to ensure that the treatment was effective and safe,and adverse events were recorded by the nursing staff using the Common Terminology Criteria for Adverse Events (CTCAE criteria).17 Disease health management counseling was provided at outpatient follow-up visits in addition to urology specialty counseling, which included postoperative home medication instruction and nursing care for NIBMIC patients as well as physical relaxation exercises and rehabilitation instruction during receiving intravesical therapy.
Tools
General Information Questionnaire
A questionnaire designed by our research team was collected, including gender, age, education, chronic diseases (hypertension, diabetes, COPD, cerebral blood disease, etc)., body mass index (BMI), tumor staging, economic income, irrigation medication, surgical method, resection of lymph nodes, and marital status.
The MOS Item Short from Health Survey
HRQoL was measured using The MOS item short form health survey (SF-36) compiled by the Boston Health Research Institute in the U.S,18 which has been widely used in studies on HRQoL evaluation in cancer populations. The SF-36 is a well-established instrument with demonstrated reliability and validity for assessing HRQoL in cancer patients internationally. It consists of 26 items measuring eight dimensions: physical functioning, bodily pain, general health, vitality, social functioning, role-physical, role-emotional, and mental health. Total scores range from 0–100, with higher scores reflecting better HRQoL. In the present study, the SF-36 exhibited excellent construct reliability and validity at all three time points (Table 1).
 |
Table 1 Self-Report Questionnaire Reliability and Validity Tests at Three Waves of Assessment |
The Berkeley Expressivity Questionnaire
Emotional expressivity was measured using the Berkeley Expressivity Questionnaire (BEQ) developed by Gross et al19 1995 and was used to assess the nature of the content and intensity of emotional expressivity. The BEQ has been translated and culturally adapted by the Chinese scholars Zhao Xin et al20 to form a Chinese version. It consists of 16 items in five dimensions: positive emotion expression, negative emotion expression, positive emotion expression intensity, negative emotion expression intensity, and negative emotion suppression. A 7-point Likert scale was used, with scores ranging from 1 to 7 from “not at all conforming” to “fully conforming”, and three items were reverse-scored. The total score was 16–112, with higher scores indicating a greater emotional expressivity. The scale in this study has excellent structural reliability and validity at all three time points (Table 1).
Readiness for Return to Work Scale
RRTW was measured using the Readiness for Return to Work Scale (RRTWS) designed by Franche et al4 which was used to assess the readiness of cancer patients before and after work and has been translated and culturally adapted by Chinese scholars by Cao Huili et al21 to form a Chinese version in 2018. The scale is divided into two parts: the not returned to work part including the pre-contemplation stage, contemplation stage, action preparation stage, and action stage, and returned to work part including uncertain maintenance stage and maintenance stage. It consists of 22 items across six dimensions. A 5-point Likert scale was used, in which items 7 and 21 were reverse scored, the mean scores of the items in each dimension were calculated, and the dimension with the highest mean score indicated the stage in which the patient was at in terms of readiness for return to work. The higher the stage, the better is the patient’s readiness for return to work. The scale in this study had excellent structural reliability and validity at all three time points (Table 1).
Procedures
A dedicated patient recruitment team was established to ensure consistent and accurate screening. The team comprised six members: a nurse manager, three charge nurses, an auxiliary nurse from the oncology clinic, and a volunteer who had achieved good symptom control following bladder cancer surgery. A nursing administrator provided overall guidance and quality control throughout the study.
The recruitment process proceeded as follows. First, a recruiter conducted a brief, structured conversation with each potential participant to assess initial eligibility. For those who met the preliminary criteria, the recruiter explained the study in detail, including its purpose, the informed consent process, and the voluntary nature of participation. Eligible patients were then asked to complete a short demographic questionnaire designed by the research team. Additionally, the recruiter assessed the patient’s functional status using the Karnofsky Performance Status (KPS) scale to document pre-enrollment performance scores.
Baseline clinical characteristics were subsequently extracted from the electronic medical record system. Health-related quality of life (HRQoL), readiness to return to work (RRTW), and emotional expressivity were assessed at three time points: at the start of intravesical therapy (T1), at six months (T2), and at twelve months (T3). All assessments were conducted in a private room in the outpatient clinic by a fixed, trained assessor. To ensure data accuracy, the assessor verified the patient’s treatment timeline before each questionnaire session. Patients were reminded at each visit that participation was voluntary and that they could withdraw at any time without consequence. All assessors received specialized training in oncology nursing and the study methodology.
Statistical Analysis
The issue of missing data was addressed in two stages. We examined the missing data mechanism using Little’s MCAR test.22 The result was not statistically significant (χ2=216.870, df=216, p=0.781), indicating that the data were missing completely at random. Although this supports the use of complete case analysis (CCA),23 the high attrition rate at T3 (45.01%) exceeded the 40% threshold recommended for longitudinal studies.24 Therefore, for our primary analysis, we included only the 227 participants with complete data across all three waves.To validate the stability of our model, we conducted supplementary analyses using maximum likelihood estimation (MLE) and full-information maximum likelihood (FIML) on the broader sample of 412 participants who completed at least one assessment. The consistency of results across these methods would support the robustness of our conclusions.
For the Readiness for Return to Work Scale (RRTWS), we followed the developers’ guidelinesby calculating dimension-specific mean scores and assigning the stage with the highest mean score as the patient’s current readiness stage. For longitudinal analysis, stages were coded 1 through 6 (1=precontemplation, 6=proactive maintenance). While these stages represent an ordinal progression, previous research has supported treating them as a continuous measure of readiness trajectory, assuming that movement through stages reflects increasing readiness. To test the robustness of this assumption, we conducted sensitivity analyses using ordinal logistic regression for key pathways, which yielded consistent results.All statistical analyses were performed using SPSS 26.0 and Mplus 8.3 software, with a two-tailed significance level of p<0.05.
Step 1: Preliminary Analyses and Covariate Selection
First, descriptive statistics were calculated for all main study variables. To identify potential covariates, we compared baseline characteristics between patients who completed all three assessments (follow-up group) and those who dropped out (dropout group). Statistically significant differences were observed for irrigation medication, gender, age, economic income, and marital status (p<0.05). These variables were therefore included as covariates in subsequent analyses. In contrast, no significant differences were found between groups for baseline HRQoL, RRTW, or emotional expressivity (p>0.05).
Step 2: Longitudinal Measurement Invariance and Cross-Lagged Panel Modeling
Prior to hypothesis testing, we assessed longitudinal measurement invariance for all main variables using confirmatory factor analysis (CFA) in Mplus 8.3. This step ensured that the constructs were measured consistently across the three time points. We then constructed a series of cross-lagged panel models (CLPM) to examine the temporal relationships among HRQoL, emotional expressivity, and RRTW. Model 1 tested the bidirectional associations between HRQoL and RRTW. Model 2 incorporated emotional expressivity to examine the full three-variable dynamic. Both models included autoregressive paths (to assess stability of each variable over time) and cross-lagged paths (to examine predictive associations between different variables across time points).
Step 3: Model Selection, Mediation Testing, and Model Fit
To identify the most parsimonious and well-fitting model, we compared four competing models for each analysis: (M1) an unconstrained baseline model; (M2) a model with constrained autoregressive paths (time-invariant stability); (M3) a model with constrained cross-lagged paths (time-invariant cross-lagged effects); and (M4) a fully constrained model with both autoregressive and cross-lagged paths constrained to be equal across time.After selecting the optimal model, we tested indirect effects using bootstrapping with 5,000 resamples. A mediating effect was considered statistically significant if the 95% bias-corrected bootstrap confidence interval for the indirect effect did not include zero.Model fit was evaluated using multiple indices: the chi-square statistic (χ2) and its degrees of freedom (df), the comparative fit index (CFI), the Tucker-Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR).25 Acceptable model fit was defined as CFI and TLI ≥0.90, RMSEA ≤0.08, and SRMR≤0.08.
Result
Baseline Characteristics and Comparison Between Follow-Up and Drop-Out Groups
A total of 425 patients were enrolled at baseline. Of these, 412 completed the initial assessment (T1), and 227 completed all three waves of data collection (T3), yielding a final analytic sample comprising 55.1% of the original cohort. As shown in Table 2, significant differences were observed between patients who completed all assessments (follow-up group) and those who dropped out (drop-out group) with respect to intravesical therapy medication, gender, age, economic income, and marital status (p<0.05). Accordingly, these variables were controlled for in all subsequent analyses.
 |
Table 2 Comparison of Baseline Characteristics Between the Follow-Up Group and the Drop-Out Group |
Descriptive Statistics and Partial Correlations for Main Study Variables
Descriptive statistics showed that the main observed variables gradually improved over time (p=0.024, 0.031, 0.090) (Table 3). After controlling for irrigation medication, age, gender, economic income, and marital status, partial correlation analyses were conducted. All correlations were significantly positive, except for the correlation between RRTW at T1 and emotional expressivity at T2 and T3, and the correlation between HRQoL at T1 and RRTW at T2 (Table 4).
 |
Table 3 Descriptive Statistics of Main Observed Variables |
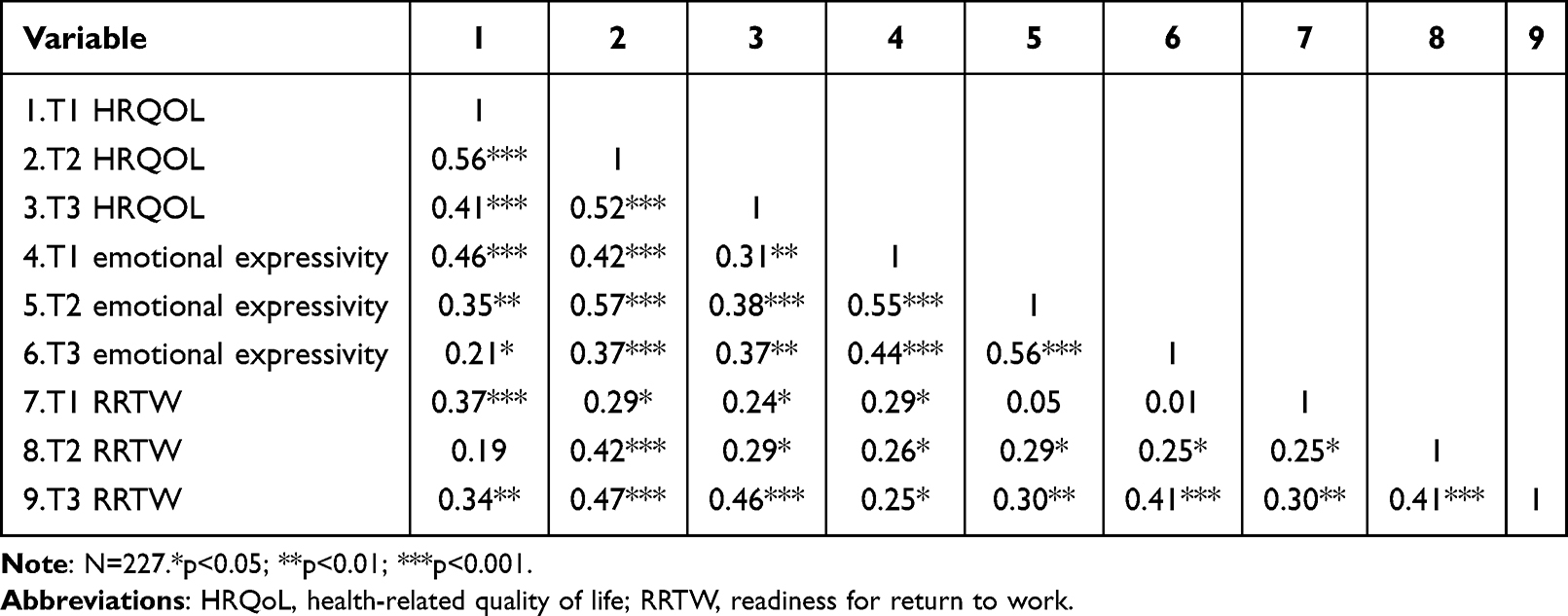 |
Table 4 Partial Correlation Among Main Observed Variables |
Longitudinal Measurement Invariance of Main Observed Variables
Confirmatory factor analysis (CFA) was conducted to test longitudinal measurement invariance for HRQoL, emotional expressivity, and RRTW across the three assessment waves. As shown in Table 5, all models demonstrated good fit to the data. Configural and metric invariance were established for all three measures, as indicated by changes in CFI (|ΔCFI|<0.02) and RMSEA (|ΔRMSEA|<0.02) that fell within acceptable thresholds. These results confirm that the factor structures and factor loadings remained stable over time, supporting the comparability of construct measurement across T1, T2, and T3.
 |
Table 5 Model Fit Statistics for Longitudinal Measurement Invariance |
Vertical Correlation Between HRQoL, RRTW and Emotional Expressivity
HRQoL and RRTW. A cross-lagged panel model examining bidirectional associations between HRQoL and RRTW was tested, controlling for intravesical therapy medication, age, gender, economic income, and marital status. Based on model fit comparisons, the fully constrained model (M4a) was selected as the most parsimonious (Table 6). As shown in Figure 1, significant bidirectional cross-lagged paths were observed: HRQoL at T1 and T2 positively predicted RRTW at T2 and T3, respectively, and RRTW at T1 and T2 positively predicted HRQoL at T2 and T3, respectively (all p<0.05).Full Model with Emotional Expressivity. When emotional expressivity was added to the model, the fully constrained model (M4b) again provided the best fit (Table 6). As illustrated in Figure 2, the bidirectional associations between HRQoL and RRTW remained significant. Furthermore, emotional expressivity at T1 and T2 showed significant positive associations with RRTW at T2 and T3, respectively (both p<0.05). According to standardized guidance estimates and 95% confidence intervals, a mediating effect of emotional expressivity at T2 exists between HRQoL at T1 and RRTW at T3 (β=0.020, 95% bootstrap CI[0.005, 0.035]).To assess the robustness of our findings to the continuous treatment of RRTW stages, we re-estimated the key mediation pathway using ordinal logistic regression with RRTW at T3 as an ordinal outcome. The pattern of results remained consistent, with a significant indirect effect of HRQoL at T1 through emotional expressivity at T2 on RRTW at T3 (OR=1.12, 95% CI [1.03, 1.22]), supporting the validity of our primary analysis.
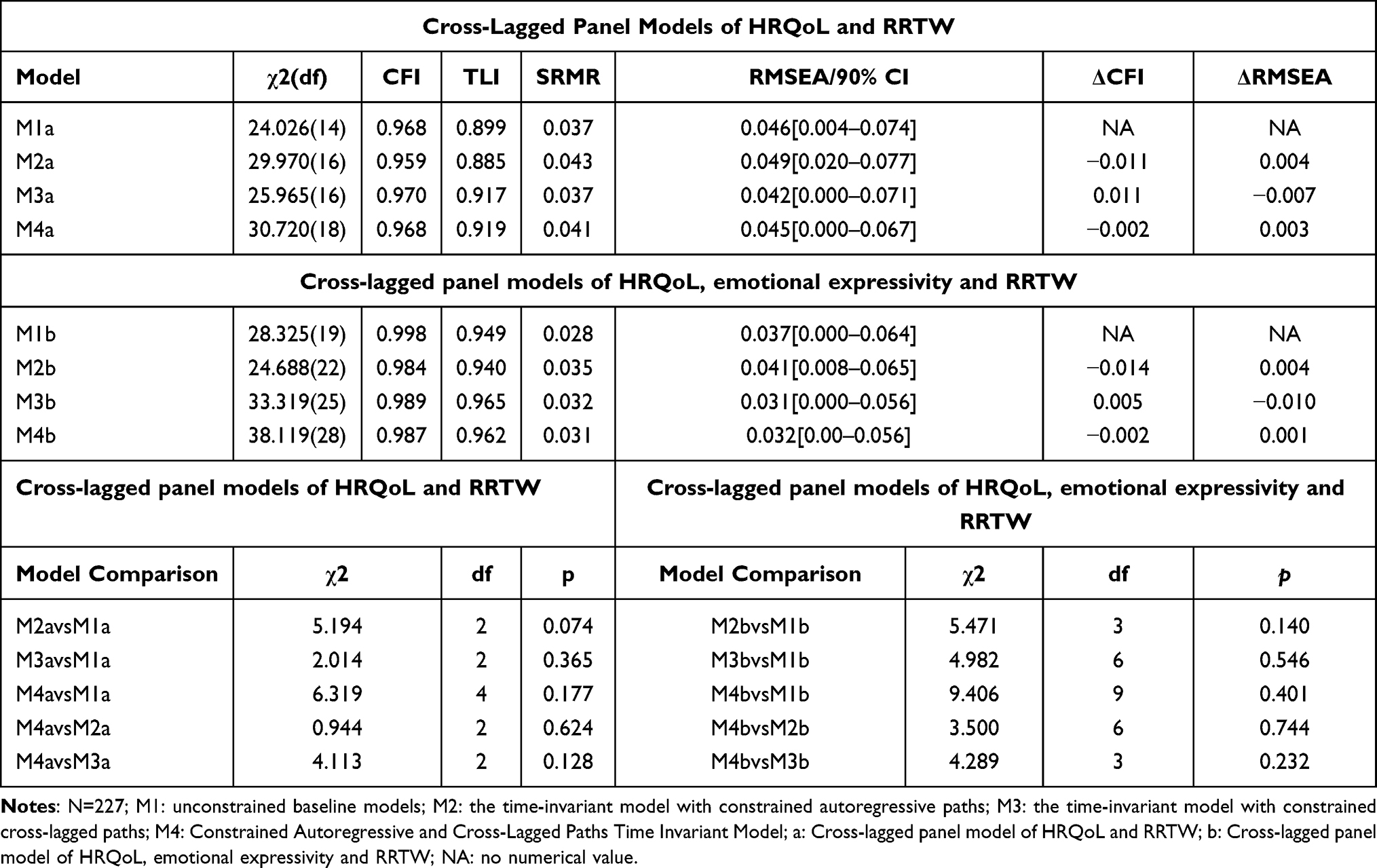 |
Table 6 Comparison of Different Cross-Lagged Panel Models Constructed with Main Observational Variables |
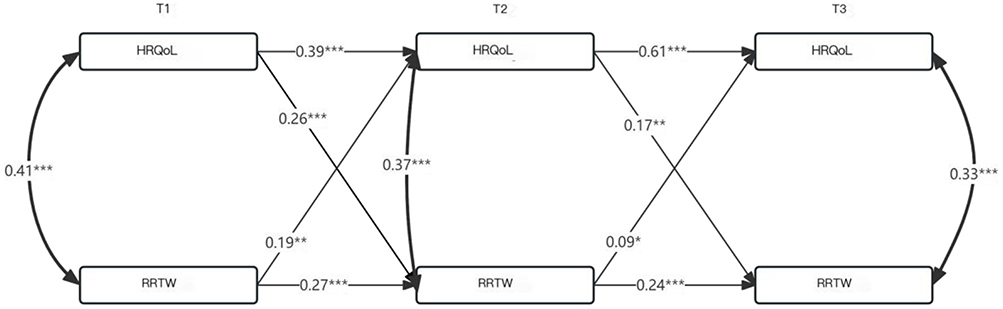 |
Figure 1 Model 4a: Cross-lagged panel model of HRQoL and RRTW: N=227;*p<0.05;**p<0.01;***p<0.001; the dashed line represents insignificant paths, whereas the solid line represents significant paths that are important. |
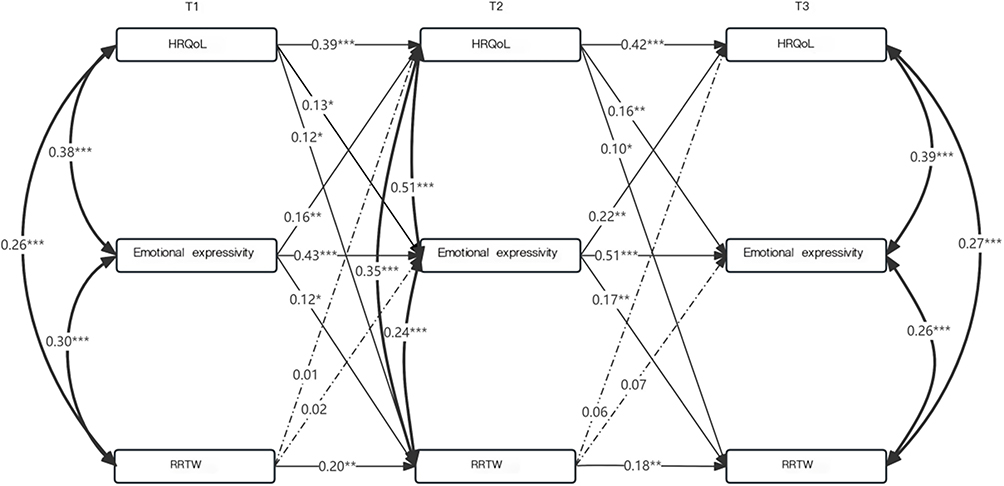 |
Figure 2 Model 4b: Cross-lagged panel model of HRQoL, emotional expressivity and RRTW: N=227;*p<0.05;**p<0.01;***p<0.001; the dashed line represents insignificant paths, whereas the solid line represents significant paths that are important. |
Validation of Cross-Lagged Panel Model for Main Observational Variables
A sensitivity analysis was conducted using the full sample (N=412) with maximum likelihood and full information maximum likelihood estimation to validate the robustness of our primary findings (N=227). As shown in Table 7 and Figure 3, the cross-lagged panel models demonstrated good fit. The mediating effect of T2 emotional expressivity on the relationship between T1 HRQoL and T3 RRTW was confirmed (standardized indirect effect=0.019, 95% CI [0.004, 0.033]). Additionally, the bidirectional associations between emotional expressivity and HRQoL observed in the primary analysis were replicated, supporting the stability of these findings.
 |
Table 7 Comparison of Different Cross-Lagged Panel Models Constructed with the Main Observational Variables Including All Patients |
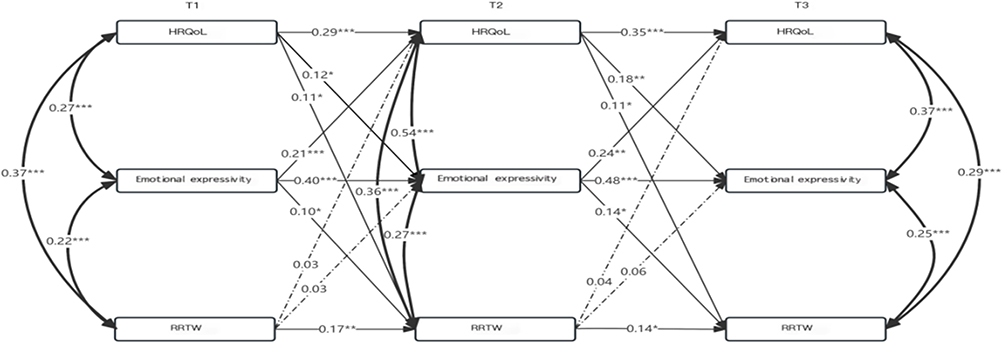 |
Figure 3 Model 4c: Cross-lagged panel model of HRQoL, emotional expressivity and RRTW: N=412;*p<0.05;**p<0.01;***p<0.001; the dashed line represents insignificant paths, whereas the solid line represents significant paths that are important. |
Discussion
This longitudinal study examined the temporal relationships among health-related quality of life (HRQoL), emotional expressivity, and readiness to return to work (RRTW) in patients receiving intravesical therapy for non‑muscle‑invasive bladder cancer. The main findings were fourfold: (1) HRQoL and RRTW showed significant longitudinal associations, with HRQoL indirectly linked to RRTW through the mediating role of emotional expressivity; (2) emotional expressivity demonstrated consistent positive associations with subsequent RRTW; (3) HRQoL and emotional expressivity exhibited bidirectional longitudinal associations, suggesting a mutually reinforcing dynamic; and (4) the positive association between RRTW and later HRQoL observed in the bivariate model was attenuated after accounting for emotional expressivity, indicating that emotional expressivity may play an important role in this relationship. Collectively, these findings suggest that HRQoL and emotional expressivity may jointly facilitate improvements in RRTW over time. The results extend our team’s prior cross-sectional and qualitative work by clarifying the temporal directionality of these associations, and may inform the development of both short‑term and long‑term supportive interventions aimed at enhancing RRTW in this population.It is important to emphasize that, despite the longitudinal design, this study remains observational. The associations identified, while temporally ordered, do not imply causality. The term “predict” is used in a statistical sense to refer to longitudinal associations, not to assert deterministic causal effects.
HRQoL Showed a Positive Longitudinal Association with Subsequent RRTW
Systematic assessment of health-related quality of life (HRQoL) using standardized self-report instruments has become a cornerstone of clinical oncology practice and a key indicator of treatment outcomes in cancer patients.26 According to the “Readiness for Change Model” in the field of health promotion, patients with RRTW may benefit from HRQoL; in this study, HRQoL at T1 and T2 was positively correlated with RRTW directly at T2 and T3, respectively (p<0.001,<0.01). Patients with higher HRQoL have a more objective and positive view of early recovery from illness and will be more willing to return to work in the later stage.A study on the burden of cancer symptoms in China showed that HRQoL is the main predictor of patients’ ability to withstand sudden stress, stress resistance and health outcomes.27 Therefore, further strengthening the recovery of daily activity ability in non–muscle-invasive bladder cancer receiving intravesical therapy and reducing the factors that affect HRQoL may be an effective choice to improve patients’ RRTW. It is necessary to fully recognize the positive effect of HRQoL on RRTW, develop targeted support programs to promote the improvement of HRQoL for non–muscle-invasive bladder cancer receiving intravesical therapy, such as increased education and policy advocacy, taking initiative, and increasing patient utilization of social support to maintain HRQoL in a more stable state as much as possible,guide patients in self-regulation and physical and mental management, and allow non–muscle-invasive bladder cancer receiving intravesical therapy to return to life and return to work in a gradual manner.
Emotional Expressivity Was Positively Associated with Subsequent RRTW Directly
Emotional expressivity, as measured by the BEQ, reflects the outward manifestation of emotional states. In the context of repeated, brief clinical encounters for intravesical instillation, the ability to visibly express emotions may serve as an important signal to healthcare providers and family members, facilitating timely supportive interventions and social connection. There is a great conflict between the high level of perfectionism in the appearance of non-muscle-invasive bladder cancer receiving intravesical therapy and the changes in physical and appearance images caused by the side effects of receiving intravesical therapy medications.28 Patients with a higher interest in emotional expressivity are more willing to participate in social activities, broaden the platform for external communication and promote patients to maintain a positive attitude towards life.In this study, emotional expressivity at T1 and T2 was positively correlated with RRTW at T2 and T3, respectively (p<0.05,<0.01). For NMIBC patients facing frequent clinic visits for intravesical instillations, the ability to express emotions during these brief encounters may be particularly crucial. Unlike patients with other cancer types who may have extended consultations, NMIBC patients often have limited time with providers, making the quality of emotional expression during these interactions potentially more impactful for maintaining social connections and facilitating RRTW.Especially in Chinese culture, emotional expressivity often implies seeking help from society; thus, it helps non-muscle-invasive bladder cancer receiving intravesical therapy establish emotional connections with others, enabling them to receive more encouragement and feedback. It is worth noting that some studies have shown that non–muscle-invasive bladder cancer receiving intravesical therapy may suffer from severe psychological stress due to passive disclosure of their emotions, such as feeling discriminated against, disrespected by others, and rejected by mainstream society.29 Therefore, it is important to provide necessary measures to help non-muscle-invasive bladder cancer receiving intravesical therapy reduce or eliminate shame, such as actively generating emotional empathy in communication with patients to reduce their sense of isolation and to induce patients to actively vent their negative emotions, so as to enable them to develop a new sense of self-identity and improve their RRTW.
Emotional Expressivity and HRQoL Demonstrated Bidirectional Longitudinal Associations, Suggesting a Mutually Reinforcing Relationship
Emotional expressivity and health are two major aspects of human existence that constantly interact.30 In this study, emotional expressivity was a direct positive predictor of HRQoL. Patients with NMIBC undergoing intravesical therapy face a range of socioeconomic challenges; the ability to express emotions outwardly may help alleviate psychological burden and facilitate adaptive coping.emotional expressivity intervention to improve patient HRQoL outcomes may have more important practical significance.Yang YL et al31 found that encouraging bladder cancer patients to write down their own lives how they are coping with cancer can promote positive responses to the symptomatic experience of cancer.It helps healthcare professionals to recognize patients’ specific concerns early, stimulates the expression of positive emotions, and helps patients to develop positive cognitions, which can lead to an increase in HRQoL.In this study, HRQoL also was a direct positive predictor of emotional expressivity, and the Readiness to Change Model in health promotion suggests that patients with better HRQoL are more willing to share their recovery experiences with others. In traditional Chinese thinking, people tend to “report the good news but not the bad news” to family and friends, when patients with good HRQoL are more willing to use active emotion regulation strategies, while patients with poor HRQoL tend to use deactivation strategies of emotion suppression, and are uncomfortable to actively talk about it.32 The 12-month treatment cycle involving repeated catheterizations and drug instillations can evoke significant embarrassment, anxiety, and physical discomfort. In this context, emotional expressivity may serve as a valuable coping mechanism, allowing patients to communicate their distress and receive empathetic responses from both providers and family members.Therefore, the mutually reinforcing correlation between emotional expressivity and HRQoL discovered in this study may serve as a theoretical guide for making preliminary predictions about patients’ health outcomes and emotional expressivity, especially since emotional expressivity interventions are increasingly proving to be simple and effective in fostering physical and mental development, and levels of emotional expressivity can be considered an indicator of the effectiveness of psychological interventions or mental health status, which may improve non–muscle-invasive bladder cancer receiving intravesical therapy’ HRQoL.
HRQoL Showed an Indirect Longitudinal Association with RRTW Through Emotional Expressivity, Consistent with a Mediating Pathway
HRQoL is a multidimensional concept that involves aspects such as an individual’s physiological, psychological, and social functioning. In our previous research, we reported a bidirectional predictive relationship between HRQoL and emotional expressivity.13 In the mediating pathway analysis, emotional expressivity at T2 had a mediating effect on HRQoL at T1 and RTW at T3. Although the standardized indirect effect of 0.020 is small in magnitude according to conventional guidelines, the narrow confidence interval [0.005, 0.035] indicates precision of the estimate. This finding suggests that even modest improvements in emotional expressivity may contribute meaningfully to readiness for return to work over time, particularly when considered in the context of a 12-month treatment cycle.One possible explanation is that patients’ better self-reported HRQoL had a motivating effect on their desire to express their emotions, and those with a good HRQoL report were more likely to believe that their emotions would be accepted and acknowledged by the listener. In addition, emotional expressivity can help alleviate the psychological distress caused by the illness, facilitate patients’ reassessment of the illness treatment experience, and complete the reconstruction of their self-perceptions, a virtuous cycle that can help improve patients’ RTW. It has been suggested that helping patients maintain a healthy psychological and physiological state can promote emotional expressivity, which can serve as a positive incentive to enhance patients’ confidence in returning to work.33 Notably, RRTW had a significant predictive effect on HRQoL in the first model, but the predictive effect of RRTW on HRQoL disappeared when the second model was constructed with the addition of emotional expressivity. One possible interpretation of the attenuated association between RRTW and subsequent HRQoL after including emotional expressivity is that these dynamics may be more complex than initially hypothesized. It is possible that patients with higher RRTW temporarily increase their emotional expression, but the sustainability of this pattern may depend on interpersonal responses. As a hypothesis for future research, it could be explored whether prolonged or intense emotional expression might, under some circumstances, lead to listener fatigue or reduced empathic engagement, potentially diminishing the benefits for the patient’s subsequent HRQoL.34 However, our data do not directly test interpersonal dynamics, and this interpretation remains speculative. Further studies incorporating dyadic data from patients and their support persons are needed to examine these potential mechanisms. In clinical practice, it is important to enhance patients’ awareness of HRQoL and develop their emotional expressivity skills. This can be achieved by improving patients’ knowledge of intravesical therapy and fostering a better understanding of the disease. Additionally, strengthening verbal communication skills may enable patients to more effectively express their feelings about the traumatic aspects of their illness. Guiding patients to positively articulate their mental activities and emotions throughout the intravesical therapy cycle may be critical for developing targeted interventions to improve RRTW.
Mechanistic Pathway Linking HRQoL, Emotional Expressivity, and RRTW
The mediating role of emotional expressivity between HRQoL and RRTW can be understood through a sequential mechanism grounded in cognitive adaptation theory and the readiness for change model.15,35 It is important to emphasize that this mechanistic pathway, while theoretically grounded, represents a conceptual model derived from observational data. Experimental or intervention studies are needed to test whether manipulating these variables indeed produces the hypothesized effects. First, adequate HRQoL provides the foundational psychological safety, physical energy, and social reserves necessary for emotional expression, enabling patients to move beyond survival mode toward active engagement with their emotional experiences. Second, when patients disclose their emotions, they engage in linguistic processing that reduces neurobiological threat responses, while simultaneously receiving empathic feedback that challenges maladaptive cognitions (eg., “I am a burden”, “I will never work again”)l.36 Third, this disclosure mobilizes social support networks, eliciting emotional reassurance, practical advice about workplace reintegration, and modeling of successful return-to-work experiences. Finally, these resources coalesce into enhanced self-efficacy, reduced stigma, and realistic expectations—the core components of readiness for return to workl.37 This mechanistic explanation transforms the statistical mediation finding into actionable clinical insights: interventions should not merely encourage disclosure in isolation, but rather create conditions where HRQoL is sufficient to support disclosure, and where listeners are trained to provide the specific responses that facilitate cognitive restructuring and self-efficacy development.
Theoretical and Practical Implications
This study emphasizes the importance of HRQoL and emotional expressivity in RRTW, further enriching our team’s previous research on the return to work of patients with receiving intravesical therapy. Theoretically, RRTW is a long-term functional outcome that can gradually improve over time during the receiving intravesical therapy cycle. In the long run, emotional expressivity may enhance the development of close, trust-based relationships with others, thereby supporting patients’ HRQoL and RRTW. From a practical standpoint, helping patients maintain good HRQoL and encouraging emotional expressivity may be mutually reinforcing, with both processes contributing to improved RRTW. Rather than relying on general encouragement, healthcare providers can implement the following specific, actionable strategies:①Peer support groups:Establish structured, professionally facilitated peer support programs where patients with similar experiences (eg., those undergoing receiving intravesical therapy) can share their feelings, concerns, and coping strategies. Such groups normalize emotional expression, reduce isolation, and provide real‑life models of successful work reintegration.38 Hospitals can collaborate with patient organizations to organize regular in‑person or online group sessions.②Expressive writing interventions:Introduce brief, evidence‑based expressive writing tasks (eg., 15–20 minutes, 3–4 sessions) during outpatient visits. Patients are guided to write about their deepest thoughts and feelings regarding their illness and treatment.39 This low‑cost, easily implemented technique has been shown to improve emotional processing, reduce distress, and enhance HRQoL.③Nurse‑led emotional expressivity conversations:Train oncology nurses to initiate brief, empathic conversations during each instillation visit. Using open-ended questions and active listening, nurses can create a safe space for patients to voice their worries (eg., fear of recurrence, treatment-related embarrassment, work-related concerns). A simple checklist or prompt card can help nurses systematically address emotional topics without prolonging consultation time. ④Psychoeducation and counseling:Offer individual or group psychoeducation sessions that explain the role of emotions in recovery and teach practical skills for self‑disclosure (eg., how to express feelings to family members, how to ask for support). For patients with high levels of distress, referral to a clinical psychologist or counselor for brief, focused therapy (eg., cognitive‑behavioral therapy, acceptance and commitment therapy)40 should be integrated into routine care. ⑤Workplace liaison and ergonomic support:Develop a partnership with occupational health services or vocational rehabilitation specialists. Patients who are ready to return to work can benefit from a workplace assessment to identify necessary adjustments (eg., flexible hours, modified duties, access to a restroom due to urinary symptoms). Providing a written summary of recommended accommodations to both the patient and their employer can facilitate a smoother transition.⑥Family caregiver training:Since emotional expressivity often occurs within the family, offering brief training sessions for spouses or adult children can enhance their ability to listen non‑judgmentally and respond with empathy.41 Simple communication guides or role‑playing exercises can help family members avoid common pitfalls such as giving premature advice or minimizing concerns.⑦Mobile health (mHealth) applications:Develop or recommend smartphone apps that include mood tracking, psychoeducational content, and secure messaging with healthcare providers.42 Apps can also provide reminders for expressive writing exercises and offer anonymous peer support forums, making emotional support accessible outside hospital settings.
These interventions should be tailored to the individual’s current HRQoL level and readiness to engage in emotional disclosure. For patients with very low HRQoL, initial efforts must focus on symptom control and basic supportive care before introducing more demanding emotional work. Conversely, patients with moderate to high HRQoL may benefit from direct encouragement to join peer groups or start expressive writing.Importantly, the effectiveness of these strategies depends on creating a supportive environment both within the healthcare system and in the patient’s social network. Therefore, we recommend that hospitals establish a multidisciplinary return‑to‑work team comprising urology nurses, psychologists, social workers, and vocational counselors to coordinate care and monitor progress over the 12‑month treatment cycle. Regular follow‑up assessments of HRQoL, emotional expressivity, and RRTW can guide the timely adjustment of interventions.By translating our mechanistic findings into these concrete actions, clinicians can move beyond general recommendations and offer patients a clear, evidence‑based pathway from improved well‑being and emotional expression to successful work reintegration.
Limitations
There are some limitations to this study.first, our study did not stratify the characteristics of the population (eg., education stratification, gender stratification, preoperative work type stratification, etc)., HRQoL and RRTW were strongly correlated across these stratification factors. Second, The patients in this study were all receiving outpatient intravesical therapy for NMIBC at two tertiary hospitals in Shanghai. The psychosocial experiences and return-to-work trajectories of these patients may differ from those with muscle-invasive bladder cancer or those receiving different treatment modalities. Therefore, generalizability of the findings to other cancer populations is limited. In the future, multicenter studies with large sample sizes can be considered to improve the generalizability of the findings. Third, although the more mature self-reported scale was used to assess patients in this study, only 227 patients completed all three waves of assessment.Although supplemental analyses were conducted to validate the data, the high attrition rate may have introduced bias. The protocol design should be improved in the future to minimize the patient dropout rates.Fourth, the Readiness for Return to Work Scale yields ordinal stage classifications. While we treated stages as continuous in our primary cross-lagged panel models following common practice in the literature, this approach assumes equal intervals between stages. Although sensitivity analyses using ordinal methods produced consistent findings, future studies with larger samples may benefit from employing latent growth curve modeling or ordinal logistic regression approaches that better respect the ordinal nature of the data.Fifth, while we have discussed potential mechanisms underlying the observed associations—such as listener fatigue or empathic responses—these interpretations extend beyond our data. The observational design precludes causal inference, and mechanisms proposed in the discussion should be regarded as hypotheses requiring direct testing in future studies. Research incorporating interpersonal or dyadic data, or experimental manipulation of emotional expressivity, would be necessary to validate these mechanistic explanations.
Conclusion
In this longitudinal study of patients with NMIBC undergoing intravesical therapy, we identified significant temporal associations among HRQoL, emotional expressivity, and RRTW. Our findings are consistent with a model where HRQoL and emotional expressivity mutually influence one another over time. Both factors demonstrated direct longitudinal associations with RRTW, and the relationship between HRQoL and RRTW was partially mediated by emotional expressivity. Given the observational nature of this study, these findings should be interpreted as identifying potential pathways and targets—specifically, improving HRQoL and promoting emotional expressivity—that warrant confirmation in future experimental or interventional research designed to enhance RRTW.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Mingming Zhang) upon reasonable request.
Ethical Approval
This study was approved by the Ethics Committee of the Shanghai General Hospital 2024394).Patients provided consent via an informed consent process that was reviewed by the Ethics Committee of Shanghai General Hospital, China, and certify that the study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki. This study was approved by IRB and registered in the Chinese Clinical Trial Registry (Registration number:ChiCTR2400091061; Date of trial registration: 20 October 2024).
Acknowledgments
The authors would like to express their sincere appreciation to the Urology Clinical Medical Center of Shanghai General Hospital for providing the essential platform and resources that enabled this research. We are profoundly grateful to each patient and caregiver who participated in this study; their willingness to share their experiences and time has been invaluable. We also wish to acknowledge the dedication and support of our nursing colleagues and medical staff, whose assistance throughout the research process was instrumental to its completion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in study design, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published, have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Science and Technology Research Project of the Songjiang District Science and Technology Committee, Shanghai 2024SJKJGG092. This study was conducted under the research program Clinical Research Innovation of Shanghai General Hospital CCTR-2023N04. This study was conducted under the 2025 Shanghai “Rising Stars in Medicine” Young Medical Talent Development Grant Program.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Li H, Zheng R, Du L, et al. Epidemic status and trend analysis of bladder cancer in China. Chinese J Cancer. 2021;43(3):293–17. doi:10.3760/cma.j.cn112152-20200421-00362
2. Zhou W, Liu J, Mao D, Hu C, Gao D, Rizzo A. The clinical efficacy and safety of equipment-assisted intravesical instillation of mitomycin C after transurethral resection of bladder tumour in patients with nonmuscular invasive bladder cancer: a meta-analysis. PLoS One. 2022;17(10:e0276453. doi:10.1371/journal.pone.0276453
3. Bilodeau K, Gouin MM, Fadhlaoui A, Porro B. Supporting the return to work of breast cancer survivors: perspectives from Canadian employer representatives. J Cancer Surviv. 2024;18(4):1384–1392. doi:10.1007/s11764-023-01382-5
4. Franche R-L, Corbière M, Lee H, Breslin FC, Hepburn CG. The readiness for return-to-work (RRTW) scale: development and validation of a self-report staging scale in lost-time claimants with musculoskeletal disorders. J Occupation Rehabil. 2007;17(3):450–472. doi:10.1007/s10926-007-9097-9
5. Ghasempour M, Shabanloei R, Rahmani A, Jafarabadi MA, Abri F, Khajehgoodari M. The relation of readiness for return to work and return to work among Iranian cancer survivors. J Cancer Educ. 2020;35(6):1237–1242. doi:10.1007/s13187-019-01588-1
6. Petersen KS, Madsen LS, Nielsen CV, Labriola M, Stapelfeldt CM. To have and then lose the safety net - female cancer survivors’ experiences of the process of becoming ready to return to work. Work. 2021;70(4):1121–1130. doi:10.3233/WOR-213623
7. Wang L. Analysis of the Current Status and Influencing Factors of Postoperative Readiness for Returning to Work in Middle-Aged and Young Colorectal Cancer Patients. Yan’an: Yan’an University; 2021.
8. Yang L, Lin Z, Wang Y, et al. The relationship between breast cancer patients’ readiness to return to work and family flexibility. Chinese J Modern Nurs. 2020;26(15):2055–2060.
9. Wu Y, Yang D, Jian B, et al. Can emotional expressivity and writing content predict beneficial effects of expressive writing among breast cancer patients receiving chemotherapy? A secondary analysis of randomized controlled trial data from China. Psychol Med. 2023;53(4):1527–1541. doi:10.1017/S0033291721003111
10. Pinks D, Warren-James M, Katsikitis M. Does a peer social support group intervention using the cares skills framework improve emotional expression and emotion-focused coping in paramedic students? Australasian Emergency Care. 2021;24(4):308–313. doi:10.1016/j.auec.2021.03.005
11. Gore JL, Wolff EM, Nash MG, et al. Twelve-month results from the CISTO study comparing radical cystectomy versus bladder-sparing therapy for recurrent high-grade non–muscle-invasive bladder cancer. J Clin Oncol. 2026;44(4):274–285. doi:10.1200/JCO-25-01324
12. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. doi:10.4278/0890-1171-12.1.38
13. Zhang MM. Analysis of factors and pathways influencing health related quality of life in patients undergoing bladder infusion chemotherapy. Chinese J Modern Nurs. 2025;31(7):897–904. doi:10.3760/cmaj.cn115682-20240315-01374
14. Liu Z, Li J, Liu F, et al. Exploring the status and associated factors of the readiness for return-to-work in young and middle-aged stroke patients. Sci Rep. 2024;14(1):2841. doi:10.1038/s41598-024-53262-2
15. Nilsson MI, Olsson M, Wennman-Larsen A, Petersson L-M, Alexanderson K. Women’s reflections and actions regarding working after breast cancer surgery – a focus group study. Psychooncology. 2013;22(7):1639–1644. doi:10.1002/pon.3192
16. Hamaker EL, Kuiper RM, Grasman RPPP. A critique of the cross-lagged panel model. Psychol Methods. 2015;20(1):102–116. doi:10.1037/a0038889
17. Basch E, Reeve BB, Mitchell SA, et al. Development of the national cancer institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106(9):dju244. doi:10.1093/jnci/dju244
18. Brazier JE, Harper R, Jones NM, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305(6846):160–164. doi:10.1136/bmj.305.6846.160
19. Gross JJ, John OP. Revealing feelings: facets of emotional expressivity in self-reports, peer ratings, and behavior. J Pers Soc Psychol. 1997;72(2):435–448. doi:10.1037/0022-3514.72.2.435
20. Zhao X, Zhang B, Zhou W, et al. Reliability and validity analysis of the Chinese version of the Berkeley emotional expression scale among Chinese college students. Chinese J Clin Psycholog. 2015;23(3):406–409. doi:10.16128/j.cnki.1005-3611.2015.03.006
21. Cao H, He K. Research progress on patient readiness for returning to work. Chinese J Nurs. 2017;52(6):749–753. doi:10.3761/j.issn.0254-1769.2017.06.022
22. Van Ness PH, Murphy TE, Araujo KLB, Pisani MA, Allore HG. The use of missingness screens in clinical epidemiologic research has implications for regression modeling. J Clin Epidemiol. 2007;60(12):1239–1245. doi:10.1016/j.jclinepi.2007.03.006
23. Xu T, Chen K, Li G. The more data, the better? Demystifying deletion-based methods in linear regression with missing data. Stat Interface. 2022;15(4):515–526. doi:10.4310/21-sii717
24. Pan Y, Zhan P. The impact of sample attrition on longitudinal learning diagnosis: a prolog. Front Psychol. 2020;11:1051. doi:10.3389/fpsyg.2020.01051
25. Peugh JL, Litson K, Feldon DF. Equivalence testing to judge model fit: a Monte Carlo simulation. Psychol Methods. 2023;10. doi:10.1037/met0000591
26. Weijuan T, Yixin W. Research progress on symptom burden of cancer patients abroad. Nurs Res. 2010;24(27):2447–2449. doi:10.3969/j.issn.1009-6493.2010.27.002
27. Dun Y, Liu C, Chen L, et al. Evaluation of health-related quality of life in prostate cancer patients after simple androgen removal therapy. Chinese J Urol. 2017;38(1):33–37. doi:10.3760/cma/j.issn.1000-6702.2017.01.008
28. Haifeng Z, Chaoqun D, Yan T, et al. A study on the relationship between early self disclosure and posttraumatic growth in individuals with accidental trauma. J Nurs. 2020;35(1):57–60. doi:10.3870/j.issn.1001-4152.20.01.057
29. Zhao C, Aiqiu C, Lingling W, et al. A study on the impact of written emotional expression on young and middle-aged stroke patients with first onset. Hebei Med J. 2021;43(20):3140–314231446. doi:10.3969/j.issn.1002-7386.2021.20.024
30. Yunmei X, Gengsheng Y, Yayan Lan, et al. The effect of self disclosure health education combined with sensory integration training on the psychological state, self-management behavior, and cognitive function of hospitalized schizophrenia patients. Chinese J Health Psycholog. 2025;33(4):543–548. doi:10.13342/j.cnki.cjhp.2025.04.013
31. Yang Y-L, Liu L, Li M-Y, Shi M, Wang L, Müller-Myhsok B. Psychological disorders and psychosocial resources of patients with newly diagnosed bladder and kidney cancer: a cross-sectional study. PLoS One. 2016;11(5:e0155607. doi:10.1371/journal.pone.0155607
32. Wu S. Seeking truth from facts, reporting good news, reporting worries: reading ‘integrated traditional Chinese and Western medicine for the treatment of skin diseases’. Chinese J Integrated Traditional Chinese Western Med Dermatolog Venereolog. 2015;14(4):218. doi:10.3969/j.issn.1672-0709.2015.04.003
33. Mengmeng Q, Lihua Z, Xiuhua H, et al. The current application status of written emotional expression in clinical nursing interventions. Nurs Res. 2019;33(10):1711–1714. doi:10.12102/j.issn.1009-6493.2019.10.015
34. Ferrara E, Yang Z, Bauch CT. Measuring emotional contagion in social media. PLoS One. 2015;10(11:e0142390. doi:10.1371/journal.pone.0142390
35. Taylor SE, Kemeny ME, Reed GM, Bower JE, Gruenewald TL. Psychological resources, positive illusions, and health. Am Psychol. 2000;55(1):99–109. doi:10.1037/0003-066X.55.1.99
36. Tamir DI, Mitchell JP. Disclosing information about the self is intrinsically rewarding. Proc Natl Acad Sci U S A. 2012;109(21):8038–8043. doi:10.1073/pnas.1202129109
37. Gremore TM, Brockstein B, Porter LS, et al. Couple-based communication intervention for head and neck cancer: a randomized pilot trial. Support Care Cancer. 2021;29(6):3267–3275. doi:10.1007/s00520-020-05848-5
38. Ross EE, Colbath RA, Yu J, Munabi N, Gillenwater TJ, Yenikomshian HA. Peer support groups: identifying disparities to improve participation. J Burn Care Res. 2022;43(5):1019–1023. doi:10.1093/jbcr/irac086
39. Lee Y, Kim D, Lim J-E. Do expressive writing interventions have positive effects on Koreans?: a meta-analysis. Front Psychiatry. 2023;14:1204053. doi:10.3389/fpsyt.2023.1204053
40. Sherman DW, Haber J, Hoskins CN, et al. The effects of psychoeducation and telephone counseling on the adjustment of women with early-stage breast cancer. Appl Nurs Res. 2012;25(1):3–16. doi:10.1016/j.apnr.2009.10.003
41. Fields B, Rodakowski J, Leighton C, Feiler C, Minnier T, James AE. Including and training family caregivers of older adults in hospital care: facilitators and barriers. J Nurs Care Qual. 2020;35(1):88–94. doi:10.1097/NCQ.0000000000000400
42. Lee J-A, Choi M, Lee SA, Jiang N. Effective behavioral intervention strategies using mobile health applications for chronic disease management: a systematic review. BMC Med Inform Decis Mak. 2018;18(1:12. doi:10.1186/s12911-018-0591-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.