Back to Journals » Patient Preference and Adherence » Volume 20
Beyond the Prescription: Hydroxycarbamide Utilization and Adherence Among Persons Living with Sickle Cell Disease in Rural Ghana
Authors Mensah KB ![]() , Osei-Owusu V, Boamah Mensah AB
, Osei-Owusu V, Boamah Mensah AB ![]() , Boachie-Ansah P
, Boachie-Ansah P ![]() , Appiah-Num Safo AA
, Appiah-Num Safo AA ![]() , Padayachee N
, Padayachee N
Received 15 September 2025
Accepted for publication 8 January 2026
Published 12 June 2026 Volume 2026:20 567619
DOI https://doi.org/10.2147/PPA.S567619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Kofi Boamah Mensah,1 Veronica Osei-Owusu,2 Adwoa Bemah Boamah Mensah,3 Pauline Boachie-Ansah,1 Akua Asantewaa Appiah-Num Safo,1 Neelaveni Padayachee4
1Department of Pharmacy, Kwame Nkrumah University of Science & Technology, Kumasi, Ghana; 2Pharmacy Department, Agogo Presbyterian Hospital, Agogo, Ghana; 3Department of General Nursing, Kwame Nkrumah University of Science & Technology, Kumasi, Ghana; 4Department of Pharmacy and Pharmacology, School of Therapeutic Sciences, University of the Witwatersrand, Johannesburg, South Africa
Correspondence: Kofi Boamah Mensah, Email [email protected]
Purpose: To assess the utilization and adherence to hydroxycarbamide therapy among sickle cell disease (SCD) patients in a rural Ghanaian setting, and predictors of adherence.
Patients and Methods: We conducted a cross-sectional study among 100 SCD patients receiving care at a rural health facility in Ghana. Data were collected using a structured questionnaire administered to adult patients and caregivers of paediatric patients. Descriptive statistics and multivariable logistic regression were used to assess hydroxyurea utilisation, adherence, and associated factors.
Results: The study population was predominantly paediatric, with caregivers completing questionnaires for most participants. More than half of the respondents (56%) had use hydroxyurea for over 2 years. While 80% reported always taking the drug, the majority admitted to missing at least one dose in the preceding month. The most reported barriers were forgetfulness (50%) and financial constraints (44.6%). Although gender and educational level were associated with adherence in unadjusted analyses, these factors were not independent predictors in the multivariable logistic regression model.
Conclusion: Hydroxyurea utilization in this rural setting is encouraging and reflects the positive impact of national policies such as the “Ahodwo Program”. However, adherence challenges persist. This is primarily driven by behavioral and financial barriers than demographic factors. Optimising hydroxyurea use will require targeted interventions, including patient and caregiver education and financial risk protection mechanisms that build on the existing national programs. From a policy perspective, these findings support strengthening caregiver-centred adherence interventions. Future studies should prioritise age-stratified, longitudinal designs to better characterise adherence patterns in adults and children.
Keywords: sickle cell disease, hydroxyurea, Agogo, Ghana
Introduction
Sickle-cell disease (SCD) is a genetic blood disorder characterised by chronic hemolytic anaemia, vaso-occlusion, and recurrent painful episodes, including sickling crises and other complications such as sickle cell organ syndrome, which can lead to a poor quality of life and early mortality.1 Internationally, SCD further exerts a substantial burden that is not amply addressed.2 Approximately twenty-five million people are affected worldwide, with most of them in sub–Saharan Africa (SSA).1 Also, 312,000 children are born with SCD annually globally.3 Disproportionately concentrated in Sub-Saharan Africa, the highest burden accounts for 75% of the global sickle cell disease burden.2,4 It is estimated that >90% of babies with sickle cell disease die by early adulthood, mainly in sub-Saharan Africa.5 It affects 1–3% of the population in many African countries and accounts for 7–16% of under-five deaths.5–7 Along with all other countries around the world, Nigeria, Ghana, and Tanzania are among the top ten in the number of children born with SCD, with more than 11,000 babies born annually in each country.8
Worldwide, hydroxyurea (HU) has been recognised as a significant advancement in SCD therapy, being one of the few currently approved medications capable of modifying the disease course.1,9 In 2014, the National Institute of Health (NIH) and in 2018, the British Society of Haematology recommended that all affected individuals receive HU therapy, and all sickle cell children should be started on the drug from age nine months upwards, irrespective of their clinical severity, to reduce SCD-related morbidity and mortality in end-stage organ failure.10,11
While treatment is present to enhance the outcome of this disease, different socioeconomic circumstances can affect utilization and adherence to the medication, resulting in a higher disease burden within different geographical areas.12,13 The available data on the use of hydroxyurea by the sickle cell health-care providers in Nigeria indicate underutilization.1 Other nationally representative administrative databases have demonstrated increased under-utilisation, resulting in more hospital admissions and Emergency Room (ER) visits, in both pediatric and adult patients with SCD.14,15 A cross-sectional study conducted in the Eastern province of Saudi Arabia, where the prevalence of SCD is higher than in other regions, also cited under-utilisation.16
The Sickle Cell Foundation of Ghana, in partnership with the Ghana Ministry of Health (MOH), Ghana Health Services and Novartis, launched a public-private partnership in 2019 to address major SCD management gaps.17 The initiative was holistic and included access to hydroxyurea (HU) scale-up, newborn screen implementation services, as well as broader health system strengthening activities.18 Biomedical data were derived from health records, combined with reported modifications in clinical outcomes and quality of life (QoL) ascertained via patient and/or caregiver interviews in the only published evaluation of this programme to date.17 These results have significantly enhanced our understanding of the clinical and patient-reported impact of this benefit.
Although Ghana has expanded access to HU, most evidence comes from urban or tertiary settings. Rural populations face unique barriers such as limited drug supply, inadequate laboratory monitoring, costs, and sociocultural beliefs that may hinder utilization and adherence. These factors may contribute to a rural–urban gap in utilization and adherence that remains unexamined. This study aimed to assess hydroxyurea utilisation and adherence, and to identify factors associated with adherence, among patients with sickle cell disease in a rural Ghanaian setting.
Methods
Study Area
The study was carried out at the Presbyterian Hospital in Agogo, Ashanti Akim North, Ghana. The hospital is a 350-bed referral facility offering diverse services, including specialized clinics. The hospital’s sickle cell clinic, operating weekly, manages about 130 patients, with roughly 110 on hydroxyurea therapy.
Study Design
This study was a hospital-based descriptive cross-sectional design, conducted to assess the utilization and adherence of HU among patients with sickle cell disease. Patients were recruited using a convenience sampling technique. The data were collected using a structured questionnaire administered as an online survey via Google Forms (sent and followed up via WhatsApp) or in hard copy for patients without internet access. Participation was voluntary, and anonymity was maintained. The cross-sectional design was selected to provide a snapshot of HU utilization and adherence, enabling the evaluation of associations between demographic, socioeconomic, and HU utilization.
Study Population
The study population comprised patients with sickle cell disease receiving hydroxyurea therapy at the Presbyterian Hospital, Agogo. Eligible participants were adults aged 18 years and above who could independently provide informed consent and complete the questionnaire. Also, patients below 18 years whose parents or caregivers provided consent were allowed to complete the questionnaire on their behalf. For paediatric participants, information on education level and monthly household income was provided by caregivers and reflects caregiver or household socioeconomic characteristics.
Exclusion criteria included individuals with sickle cell disease who are not on hydroxyurea, caregivers who refused to participate, and subjects with cognitive or other severe medical impairment that precluded them from providing valid responses. Questionnaires were completed by caregivers for paediatric participants. Adherence reflects caregiver-supervised medication use. Due to the small number of adult participants, analyses were conducted on the combined sample, with age group included as a covariate.
Data Collection Tool
The study questionnaire was developed based on a previously validated tool used in a similar study and adapted to the Ghanaian context.19 The original questionnaire demonstrated acceptable internal consistency reliability in the previous study, with a reported Cronbach’s alpha of α ≥ 0.70. The questionnaire used included sections on demographic information, hydroxyurea utilization patterns, adherence, perceived barriers, and clinical outcomes. The questionnaire was pretested in 10 participants to ensure consistency in responses. These participants were excluded from the final study. In the present study, the questionnaire demonstrated acceptable internal consistency, with a Cronbach’s alpha of α ≥ 0.71. Data collection was conducted from 4th September to 4th December 2024.
Ethical Concerns
Ethical clearance (REF.CHRPE/AP/953/24) was sought from the Kwame Nkrumah University of Science and Technology (KNUST) Committee on Human Research Publication and Ethics (CHRPE) and from the research committee of the Presbyterian hospital, Agogo (APH/ADM/RES-135/24) which was the only site for the data collection. Prior to data collection, the study purpose was explained to participants using a Patient Information Leaflet. Informed consent was obtained from each participant before they were granted access to the questionnaire. Participation in the study was entirely voluntary, and respondents were assured of anonymity and confidentiality. They were informed that they could withdraw from the study at any stage without providing any reason and without any consequences to their clinical care.
Data Analysis
Data were entered into Google Forms and exported to SPSS (Statistical Package for the Social Sciences, Version 27) for analysis. Caregivers completed the questionnaires for paediatric participants. Measures of hydroxyurea utilisation, adherence, and missed doses reflect caregiver-supervised medication use. Due to the small number of adult participants, analyses were conducted on the combined sample, with age group included as a covariate. The results were presented as percentages and frequencies. Descriptive statistics were used to present the demographic characteristics, hydroxyurea utilization, and adherence patterns, and results were presented as frequencies and percentages. Chi-square tests and independent t-tests were used to examine associations between adherence and selected demographic variables, as appropriate.
Furthermore, a multivariable binary logistic regression model was used to determine the predictors of hydroxyurea adherence. Adherence (adherent vs. non-adherent) was treated as the dependent variable. The independent variables were age, gender, educational status, and years since diagnosis. The adjusted odds ratios (AORs) with 95% confidence intervals were estimated. A p-value < 0.05 was considered statistically significant.
Variables that showed associations in bivariate analyses were further evaluated using multivariable binary logistic regression. This identifies independent predictors of hydroxyurea adherence, with adjusted odds ratios and 95% confidence intervals reported.
Results
Respondents’ Characteristics
From Table 1, a total of 100 respondents with sickle cell disease (SCD) who were receiving care at Presbyterian Hospital, Agogo, participated in the study. The age distribution revealed that 46% of participants were aged 11–20 years. At the same time, 42% were 2–10 years. Females constituted 51% of the sample (n=51), and 87% were students. The majority have primary-level education (66%) and come from households with monthly incomes below GH₵ 500 (49%).
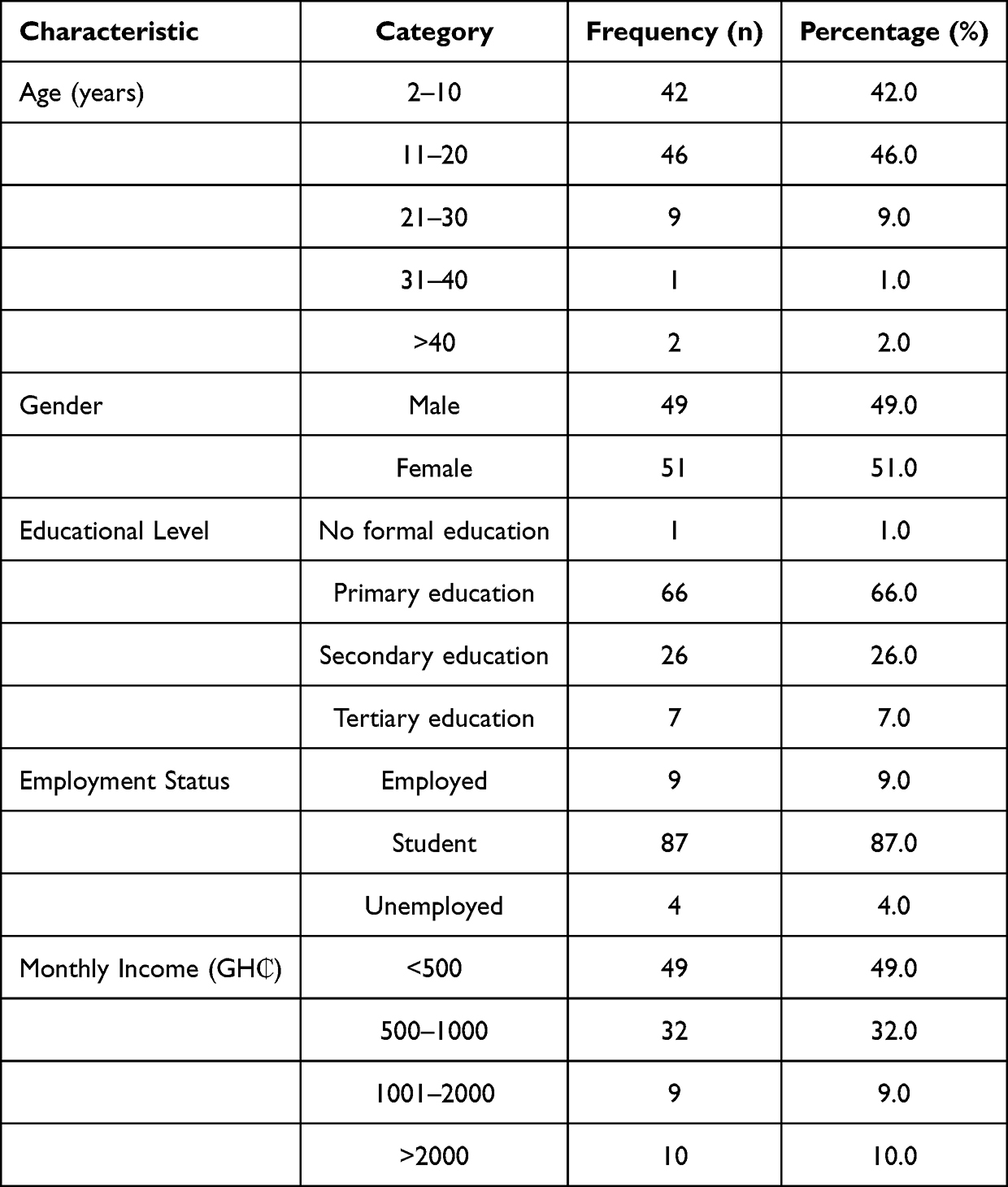 |
Table 1 Demographic Characteristics of SCD Patients at Presbyterian Hospital, Agogo (n=100) |
Hydroxyurea Utilization Patterns
Among the patients, 56% reported using hydroxyurea for more than two years. Regarding adherence, 80% reported “always” taking the medication as prescribed, while 10% used it “often”, 8% “sometimes, 2%” never. Despite these high reported adherence levels, 56% had missed not less than one dose in the previous month. Although 80% of respondents reported always taking hydroxyurea as prescribed, more than half reported missing at least one dose in the preceding month, indicating that adherence challenges in this setting are largely driven by behavioural and financial barriers rather than by a lack of prescription or utilisation. Details are presented in Table 2.
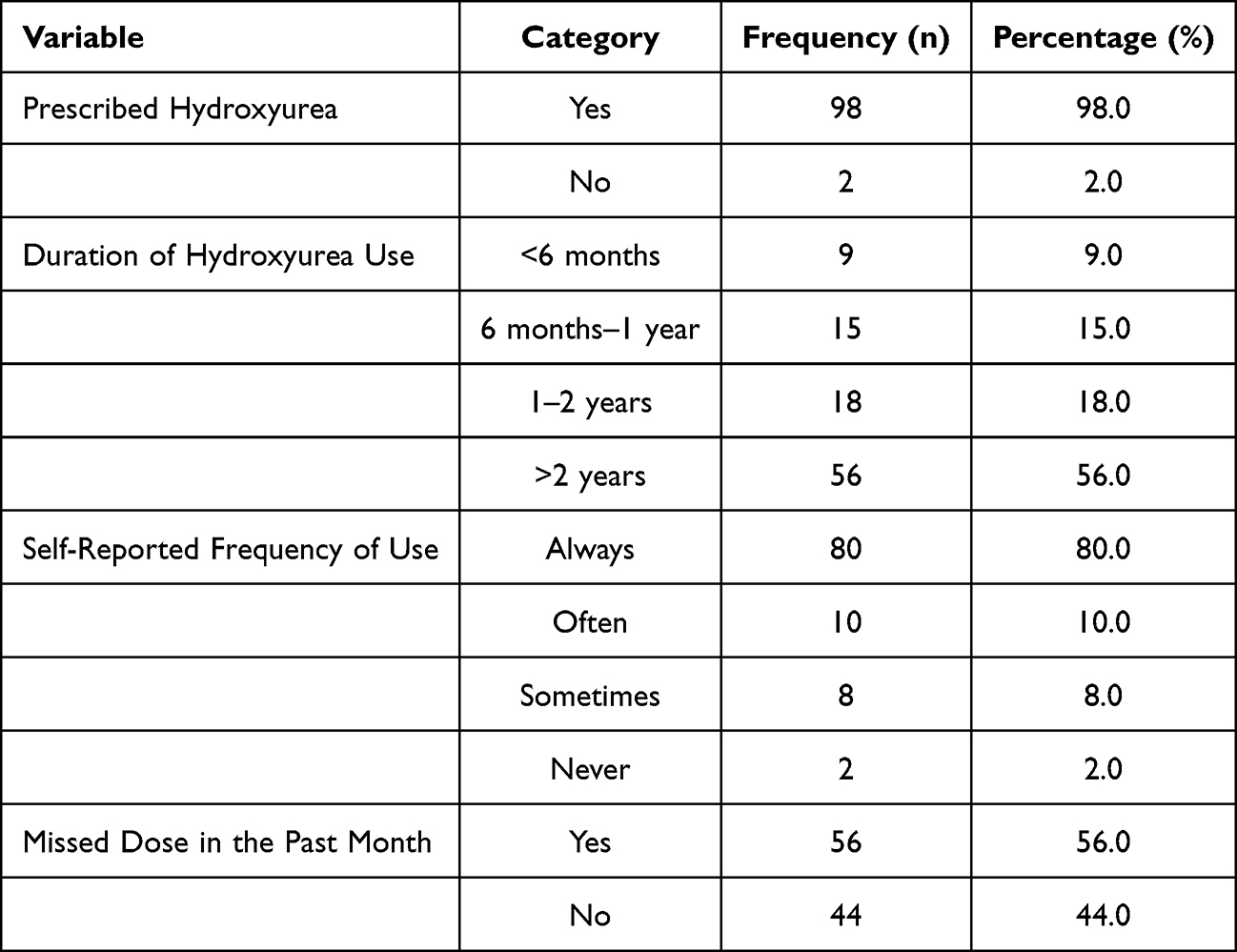 |
Table 2 Hydroxyurea Utilization Patterns Among SCD Patients (N = 100) |
Missed Doses and Frequency
Among those who missed doses (n=56), 49.1% missed 1–2 doses, 21.1% missed 3–5 doses, and 29.8% missed more than 5 doses within the last month. The primary reasons cited were forgetfulness (50%) and cost (44.6%). Followed by difficulty obtaining the drug (2%) and fear of long-term side effects (1.8%). This indicates a significant adherence gap in a considerable proportion of the study population. Details are presented in Table 3.
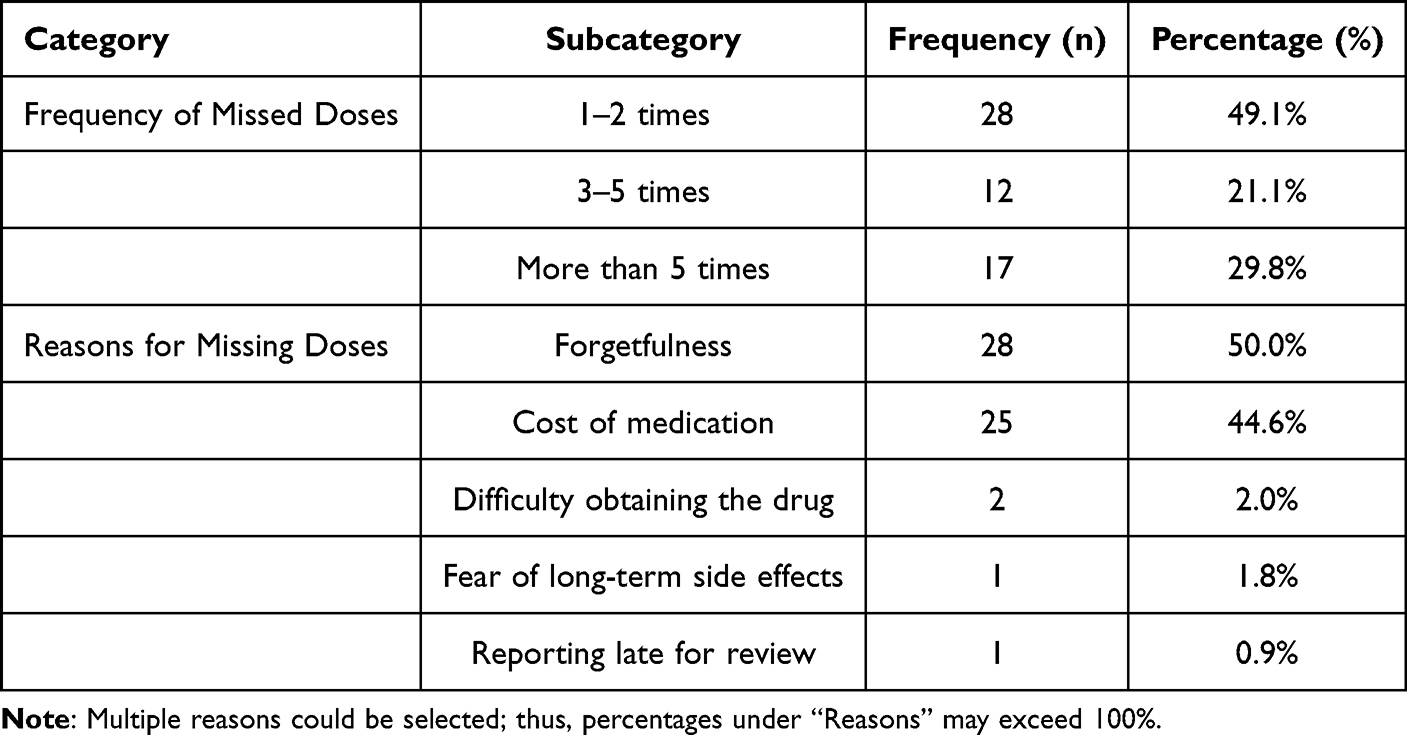 |
Table 3 Frequency and Reasons for Missed Hydroxyurea Doses in the Past Month |
Factors Associated with Hydroxyurea Adherence
Gender role and educational level significantly impacted adherence from the Chi-square analysis. Male patients were more likely to adhere than females (p=0.045). Similarly, participants with primary education had significantly higher adherence than those with secondary or tertiary education (p=0.021). No significant association was found between adherence and age group (p=0.444) or household income (p=0.571). However, these associations reflect unadjusted bivariate relationships and were not retained after adjustment in the multivariable regression analysis.Details are presented in Table 4.
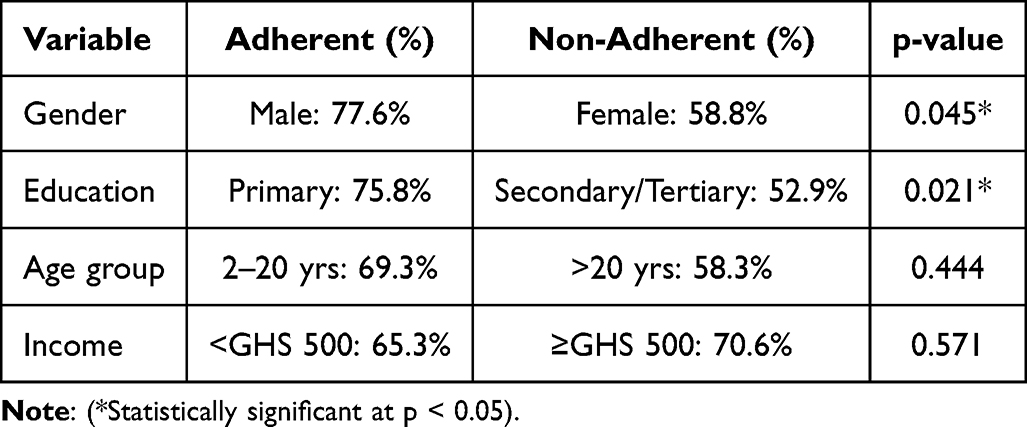 |
Table 4 Adherence to Hydroxyurea by Demographic Characteristics |
Logistic Regression Analysis of Predictors of Hydroxyurea Adherence
To further explore predictors of hydroxyurea adherence, binary logistic regression analysis was conducted using age, gender, education level, and years since diagnosis as predictor variables. Although gender and education level were significantly associated with adherence in bivariate (chi-square) analyses, these associations were not retained in the multivariable logistic regression model after adjustment for age group and years since diagnosis. Predictors of adherence showed that none of the variables were statistically significant.
Gender (B = −0.068, p = 0.882) and age category (B = −0.978, p = 0.265) were not associated with adherence. Level of education (B = −0.401, p = 0.483) and years since diagnosis (B = 0.172, p = 0.752) did not show any significant impact. Adjusted odds ratios (AOR) for all the variables fell within the range of 0.376 to 1.457 with wide confidence intervals crossing unity, indicating no significant relationships. The overall logistic regression model was not statistically significant (p > 0.05), suggesting that demographic and clinical factors considered in this study were not significant predictors of adherence. That would suggest hydroxyurea adherence in this rural Ghanaian setting is more likely to be influenced by unmeasured behavioural, psychosocial, or system-level factors such as patient beliefs, medication availability, reminder systems, or caregiver support. All the details are presented in Table 5.
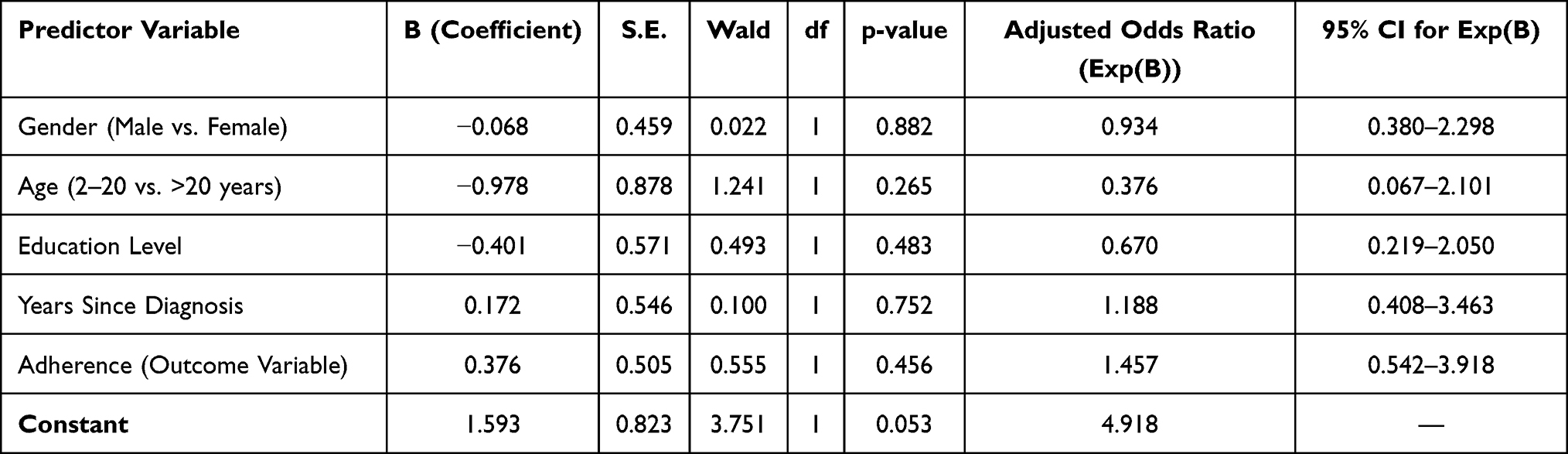 |
Table 5 Multivariable Binary Logistic Regression Analysis of Predictors of Hydroxyurea Adherence (N = 100) |
Discussion
The demographic characteristics of the study population at the Presbyterian Hospital, Agogo, indicate that most of the patients were adolescents (11–20 years) and children aged 2–10 years. This indicates the considerable burden of SCD within pediatric and adolescent groups. Findings of this study are consistent with global trends, where most SCD cases are detected early in life due to the genetic basis of the condition.19,20 Although evidence demonstrates that early diagnosis substantially reduces morbidity and mortality, neonatal sickle cell screening programs in Ghana are limited.21 As a result, many patients are only diagnosed following their first severe clinical crisis, which delays the timely initiation of disease-modifying interventions such as hydroxycarbamide therapy.22
In this study, almost all patients were prescribed hydroxyurea, with more than half reporting continuous use for over two years, and the majority self-reporting that they “always” take the medication. Given that the study population was predominantly paediatric, and adherence for children is largely caregiver-supervised, these utilisation and adherence patterns should be interpreted as reflecting caregiver- and household-level behaviours rather than autonomous patient behaviour. Accordingly, associations with education and socioeconomic status represent caregiver or household influences on adherence rather than child-level determinants.
These findings can be further contextualised using the World Health Organization’s multidimensional adherence framework. This conceptualises medication adherence as being influenced by five interacting domains: patient-related, therapy-related, condition-related, health system–related, and socioeconomic factors. With this study, financial barriers align with socioeconomic constraints, forgetfulness and caregiver supervision reflect patient- and caregiver-related factors. Difficulties in accessing hydroxyurea indicate health system–related factors. Concerns about long-term side effects relate to therapy-related influences. Placing these findings within the WHO framework highlights that multiple interacting determinants shape hydroxyurea adherence in this predominantly paediatric population. This reinforces the need for integrated, caregiver-focused, and system-level interventions.
The study’s rural setting further shapes these adherence dynamics. Caregivers and patients in rural areas often encounter challenges. Some of these include the distances that may need to be traveled to access medical facilities, as well as the shortage of specialized medicines and medical personnel. All of these can affect consistent access to hydroxyurea and routine follow-up. Inter-period medicine stock-outs, the time lag between lab testing and prescription refills, out-of-pocket costs, and loss of income for households with scarce financial resources are also factors that worsen adherence. Within this context, adherence behaviour reflects not only individual or caregiver motivation but also structural health-system barriers characteristic of rural, resource-limited settings.
The sustained utilization reported in this study is encouraging. Given that long-term adherence is essential for realising the full clinical benefits of hydroxyurea, including reductions in vaso-occlusive crises, hospitalisations, transfusion requirements, and mortality.23,24 Our study findings are in contrast to earlier reports from several sub-Saharan African countries, where uptake has historically been limited by high cost, irregular supply, and inadequate monitoring systems.25,26 The adherence observed in our cohort reflects recent policy advances on sickle disease in Ghana, such as national approval in 2018 and implementation of the “Ahodwo Program”.27 The program expanded access and improved affordability. The study findings suggest national investments in hydroxyurea are being translated into long-term patient use at the facility level. It also highlights the potential for reductions in sickle cell disease burden in Ghana.
Despite the encouraging levels of long-term use, many patients in our study acknowledged “missing doses” in the month before the study mainly due to forgetfulness and financial constraints. A smaller proportion attributed non-adherence to difficulty obtaining the drug and concerns about long-term side effects. Forgetfulness as a key factor has also been reported in Nigerian and Ugandan cohorts.28,29 Where patients often struggle to integrate hydroxyurea into their daily routines. Similarly, financial barriers have been widely documented. Studies done in Tanzania and the Democratic Republic of Congo reported that the out-of-pocket cost of hydroxyurea remains prohibitive for many families despite demonstrated clinical benefits.30,31
In contrast, studies conducted in high-income countries have reported much higher adherence rates, mainly attributable to subsidized drug costs, reliable supply chains, and structured follow-up systems.16 Although our study emphasizes that national initiatives such as the “Ahodwo Program” have widened access to hydroxyurea in Ghana, ancillary interventions are still required. They may be in the form of patient education, debunking of myths surrounding side effects, reminders to limit forgetfulness, and financial support mechanisms to avoid cost-related discontinuations. Such multipronged approaches are required to sustain adherence and ensure that the clinical effectiveness of hydroxyurea observed globally can be ideally realized in the Ghanaian context.
Adherence to hydroxyurea has clinical and public health implications. Reductions in vaso-occlusive crises, hospital admissions, transfusion requirements, and mortality among patients with sickle cell disease are associated with improved adherence. Improved adherence can also translate into reduced healthcare utilisation, lower treatment costs, and improved quality of life, particularly in high-burden, resource-limited settings. In this context, the adherence patterns observed in our predominantly paediatric cohort have implications not only for individual clinical outcomes but also for strengthening sickle cell disease control strategies within the health system.
Socio-demographic characteristics also appeared to influence adherence in our study. Given that the majority of participants were children and adolescents, educational level and income in this study reflect caregiver or household characteristics, and the observed associations should therefore be interpreted as caregiver-level influences on hydroxyurea adherence rather than child-level determinants.
Male patients and participants with primary education showed higher adherence in bivariate analyses; however, these factors were not independent predictors after multivariable adjustment. It is possible that the higher adherence reported among males reflects social desirability bias, as males have been shown in other self-reported health and quality-of-life studies to report more favourable outcomes, a pattern consistent with the lack of an independent gender effect in the multivariable regression analysis.
The observed gender difference is consistent with findings from other sub-Saharan African studies.25,29,32 Similar studies in the region reported that women often have additional caregiving responsibilities, limited autonomy in health decisions, and financial constraints that may reduce treatment consistency.28,33 By contrast, studies from high-income countries have found no significant gender-related differences in adherence.34,35 This pattern was likely attributable to more substantial health system support and fewer gender-based barriers. The association between lower educational level and higher adherence in our cohort may be explained by the fact that the majority of our patients were children and adolescents.
In this age group, caregivers, often parents or guardians, mostly supervise daily medication use, thereby promoting better adherence despite the patient’s limited formal education. However, patients with higher education, mainly older adolescents or young adults, may have competing school or work demands. This may interfere with consistent hydroxyurea use, leading to low adherence. It is also possible that, given the predominantly paediatric nature of the study population, parental or caregiver involvement in medication supervision may have contributed to the observed adherence patterns. However, caregiver involvement was not directly assessed in this study. Hence, the need for tailored adherence support strategies that will address the realities of different patient subgroups.
The logistic regression analysis did not identify any of the examined demographic, age, gender, educational level, or years since diagnosis as significant predictors of hydroxyurea adherence. In our rural Ghanaian setting, the absence of significant demographic predictors suggests that adherence may be influenced by factors beyond baseline characteristics. However, behavioural, psychosocial, and system-level influences, such as patient or caregiver beliefs, reminder practices, and family support, were not directly assessed in this study and should be explored in future research.
Similar findings have been reported in studies from Uganda and Nigeria, where demographic factors were poor predictors of adherence.28,32,36 Instead, health system barriers and patient-level factors, including perceptions of side effects, forgetfulness, and financial constraints, played a more prominent role.28,37 Conversely, studies from high-income countries have sometimes found associations between adherence and variables such as parental education, but these effects were often attenuated once psychosocial support and structured follow-up were taken into account.38,39 Our findings therefore reinforce the need to broaden adherence research beyond demographic predictors, to include qualitative and system-level assessments that can inform context-specific interventions aimed at sustaining hydroxyurea use.
Limitations
This study has some limitations that should be considered when interpreting the findings. First, adherence was assessed through self-report, which is open to recall and social desirability bias and may not fully reflect actual medication use. Secondly, the study was conducted in a single rural hospital, which may limit generalizability to other settings in Ghana with different health system resources or patient populations. The findings are most applicable to similar rural Ghanaian or West African contexts and may not be directly generalisable to urban settings or nationwide populations.
Thirdly, the cross-sectional design rules out causal inferences, as predictors of adherence could not be assessed longitudinally. In addition, the use of convenience sampling and electronic data collection via WhatsApp and Google Forms may have introduced selection bias by favouring respondents with greater access to digital technologies or higher technological literacy, potentially limiting the representativeness of the study population.
Fourthly, the predominance of children and adolescents limited the feasibility of age-stratified analyses; future studies with larger adult samples should examine age-specific determinants of adherence. Fifthly, the sample was predominantly paediatric; education and socioeconomic variables reflect caregiver or household characteristics, which limit direct comparison with adult-only adherence studies. Also, some potentially important factors such as psychosocial influences, caregiver dynamics, and health system barriers, were not measured, and these factors could have provided a more comprehensive understanding of adherence patterns. Age-stratified analyses were not feasible because adherence behaviour differs fundamentally between caregiver-mediated paediatric treatment and self-managed adult treatment. Also, the sample size for the adult group was small. Hence, the findings should be interpreted primarily within a predominantly paediatric, caregiver-supervised context. The regression approach was appropriate for the study objectives, the sample size may have limited the multivariable model’s statistical power to detect small effect sizes, and non-significant associations should therefore be interpreted with caution. In addition, the regression model included mainly demographic variables and did not capture other potentially important clinical and health system–related factors, such as disease severity, frequency of clinic visits, or intermittent drug availability, which may have confounded the observed associations.
Finally, the study did not assess supply chain challenges, promotional activities by the Ministry of Health or non-governmental organisations, or specific implementation strategies such as decentralised medicine pick-up points, which may influence hydroxyurea access and adherence following national approval. The extent to which supply chain reliability and promotional activities influence adherence requires further investigation.
Conclusion
This study demonstrates encouraging hydroxyurea utilisation and adherence among predominantly paediatric sickle cell disease patients receiving caregiver-supervised treatment in a rural Ghanaian setting. Notably, the multivariable regression analysis identified no demographic characteristics as independent predictors of adherence, suggesting that structural and contextual factors, rather than individual-level attributes, may play a more critical role in shaping hydroxyurea adherence in this setting.
This also reflects the positive impact of national policy initiatives such as the Ahodwo Program in Ghana. However, adherence challenges persist, with many patients reporting missed doses in the preceding month. This was primarily due to forgetfulness and financial barriers. Sociodemographic variables such as gender, age, and education did not significantly predict adherence in regression analysis. And this emphasizes the role of unmeasured behavioural, psychosocial, and system-level factors. These findings align with Ghana’s National Sickle Cell Disease Control Program and the WHO 2023–2030 Sickle Cell Disease Implementation Strategy, both of which prioritise equitable access to hydroxyurea and system-level support for adherence, particularly in resource-limited settings.
Again, these findings highlight that while policy-driven improvements in access are critical, sustained adherence will require targeted interventions to maximize the clinical benefits of hydroxyurea.
Recommendations
Improving understanding of hydroxyurea, correcting misconceptions, and educating patients and caregivers are important future intervention strategies. The introduction of adherence-support tools (example reminder systems) and regular follow-ups should be incorporated into routine practice. Strategies to reduce out-of-pocket expenses, which hinder continuous therapy, include financial protection mechanisms and subsidy programs. More mixed-methods and longitudinal studies are needed to focus on the behavioural, psychosocial, and health system factors that influence adherence, thereby developing context-relevant strategies. To ensure equitable and sustained access, expanding the Ahodwo Program and incorporating hydroxyurea monitoring into national sickle cell services are crucial for maintaining access across Ghana.
Abbreviations
SCD, sickle-cell disease; SSA, sub–Saharan Africa; HU, hydroxyurea; ER, emergency room; NIH, national institute of health; QoL, quality of life; MOH, ministry of health; KNUST, kwame nkrumah university of science and technology; CHEPE, committee on human research publication and ethics; AOR, adjusted odds ratios.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Ethics Statement
The study was approved by was sought from the Kwame Nkrumah University of Science and Technology (KNUST) Committee on Human Research Publication and Ethics (REF.CHRPE/AP/953/24) and the research committee of the Presbyterian hospital, Agogo (APH/ADM/RES-135/24).
Informed Consent
The procedures used in this study adhered to the principles of the Declaration of Helsinki.
Acknowledgments
The authors appreciate all the sickle cell patients, caregivers, and staff of Agogo Presbyterian Hospital for their support during this study period.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report there are no conflicts of interest in this work.
References
1. Ofakunrin AO, Okpe ES, Afolaranmi TO, et al. Level of utilization and provider-related barriers to the use of hydroxyurea in the treatment of sickle cell disease patients in Jos, North-Central Nigeria. Afr Health Sci. 2021;21(2):765–11. doi:10.4314/ahs.v21i2.36
2. Tusuubira SK, Nakayinga R, Mwambi B, Odda J, Kiconco S, Komuhangi A. Knowledge, perception and practices towards sickle cell disease: a community survey among adults in Lubaga division, Kampala Uganda. BMC Public Health. 2018;18(1):561. doi:10.1186/s12889-018-5496-4
3. Piel FB, Patil AP, Howes RE, et al. Global epidemiology of sickle haemoglobin in neonates: a contemporary geostatistical model-based map and population estimates. Lancet. 2013;381(9861):142–151. doi:10.1016/S0140-6736(12)61229-X
4. Piel FB, Hay SI, Gupta S, Weatherall DJ, Williams TN, Osrin D. Global burden of sickle cell anaemia in children under five, 2010–2050: modelling based on demographics, excess mortality, and interventions. PLoS Med. 2013;10(7):e1001484. doi:10.1371/journal.pmed.1001484
5. Murray CJL. Findings from the global burden of disease study 2021. Lancet. 2024;403(10440):2259–2262. doi:10.1016/S0140-6736(24)00769-4
6. Organization WH. Sickle cell disease in the African region: current situation and the way forward. Regional Office Africa. 2006;56:1–2.
7. Thomson AM, McHugh TA, Oron AP, et al. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Haematol. 2023;10(8):e585–e599. doi:10.1016/S2352-3026(23)00118-7
8. Amuzu EX, Urio F, Dogbe EE, et al. Clinical manifestations of sickle cell disease in Africa and its association with foetal haemoglobin parameters. Communicat Med. 2025;5(1):238. doi:10.1038/s43856-025-00954-z
9. Halsey C, Roberts IAG. The role of hydroxyurea in sickle cell disease. Br J Haematol. 2003;120(2):177–186. doi:10.1046/j.1365-2141.2003.03849.x
10. Qureshi A, Kaya B, Pancham S, et al. Guidelines for the use of hydroxycarbamide in children and adults with sickle cell disease a British society for haematology guideline. Br J Haematol. 2018;181(4):460–475. doi:10.1111/bjh.15235
11. UDoHaH S. National Heart, Lung, and Blood Institute. Evidence-Based Management of Sickle Cell Disease: Expert Panel Report. 2014. Available from: http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines.
12. Lee L, Smith-Whitley K, Banks S, Puckrein G. Reducing health care disparities in sickle cell disease: a review. Public Health Reports®. 2019;134(6):599–607. doi:10.1177/0033354919881438
13. Wastnedge E, Waters D, Patel S, et al. The global burden of sickle cell disease in children under five years of age: a systematic review and meta-analysis. J Global Health. 2018;8(2):021103. doi:10.7189/jogh.08.021103
14. Badawy SM, Thompson AA, Holl JL, Penedo FJ, Liem RI. Healthcare utilization and hydroxyurea adherence in youth with sickle cell disease. Pediatric Hematol Oncol. 2018;35(5–6):297–308. doi:10.1080/08880018.2018.1505988
15. Raphael JL, Mei M, Mueller BU, Giordano T. High resource hospitalizations among children with vaso-occlusive crises in sickle cell disease. Pediatr Blood Cancer. 2012;58(4):584–590. doi:10.1002/pbc.23181
16. Madkhali MA, Abusageah F, Hakami F, et al. Adherence to hydroxyurea and patients’ perceptions of sickle cell disease and hydroxyurea: a cross-sectional study. Medicina. 2024;60(1):124. doi:10.3390/medicina60010124
17. Dwomoh D, Abankwah DNY, Kuma AB-A, et al. Effectiveness of hydroxyurea in patients with sickle cell disease in Ghana: a population-level, healthcare facilities-based study. Blood. 2024;144(Supplement 1):2499. doi:10.1182/blood-2024-209483
18. Dwomoh D, Abankwah DNY, Benneh-Akwasi Kuma AA, et al. Effectiveness of hydroxyurea (hydroxycarbamide) in a national sickle cell disease programme in Ghana. Br J Haematol. 2025;207(5):2099–2108. doi:10.1111/bjh.70079
19. Grosse SD, Odame I, Atrash HK, Amendah DD, Piel FB, Williams TN. Sickle cell disease in Africa: a neglected cause of early childhood mortality. Am J Prev Med. 2011;41(Suppl 6):S398–405. doi:10.1016/j.amepre.2011.09.013
20. Newby GA, Yen JS, Woodard KJ, et al. Base editing of haematopoietic stem cells rescues sickle cell disease in mice. Nature. 2021;595(7866):295–302. doi:10.1038/s41586-021-03609-w
21. Segbefia CI, Goka B, Welbeck J, et al. Implementing newborn screening for sickle cell disease in Korle Bu Teaching Hospital, Accra: results and lessons learned. Pediatr Blood Cancer. 2021;68(7):e29068. doi:10.1002/pbc.29068
22. Sims AM, Bonsu KO, Urbonya R, et al. Diagnosis patterns of sickle cell disease in Ghana: a secondary analysis. BMC Public Health. 2021;21(1):1719. doi:10.1186/s12889-021-11794-6
23. Wang WC, Ware RE, Miller ST, et al. Hydroxycarbamide in very young children with sickle-cell anaemia: a multicentre, randomised, controlled trial (BABY HUG). Lancet. 2011;377(9778):1663–1672. doi:10.1016/S0140-6736(11)60355-3
24. Ware RE, Davis BR, Schultz WH, et al. Hydroxycarbamide versus chronic transfusion for maintenance of transcranial Doppler flow velocities in children with sickle cell anaemia—TCD with Transfusions Changing to Hydroxyurea (TWiTCH): a multicentre, open-label, Phase 3, non-inferiority trial. Lancet. 2016;387(10019):661–670. doi:10.1016/S0140-6736(15)01041-7
25. Tshilolo L, Tomlinson G, Williams TN, et al. Hydroxyurea for children with sickle cell Anemia in Sub-Saharan Africa. N Engl J Med. 2019;380(2):121–131. doi:10.1056/NEJMoa1813598
26. Ware RE, de Montalembert M, Tshilolo L, Abboud MR. Sickle cell disease. Lancet. 2017;390(10091):311–323. doi:10.1016/S0140-6736(17)30193-9
27. Ohene-Frempong K, Segbefia C, Spector J, et al. S129: IMPLEMENTATION OF HYDROXYUREA THERAPY FOR SICKLE CELL DISEASE ON A LARGE SCALE IN GHANA. HemaSphere. 2022;6:16. doi:10.1097/01.Hs9.0000821484.39112.40
28. Namaganda P, Nantume P, Mubiru KR, Twimukye A, Wiltshire CS. Understanding patient-related barriers to hydroxyurea use among adolescent and adult patients with sickle cell disease in Mulago and Kiruddu hospitals, Uganda, a qualitative study. BMC Health Serv Res. 2024;24(1):666. doi:10.1186/s12913-024-11125-6
29. Okocha EC, Gyamfi J, Ryan N, et al. Barriers to therapeutic use of hydroxyurea for sickle cell disease in Nigeria: a cross-sectional survey. Front Genetics. 2022;12:765958. doi:10.3389/fgene.2021.765958
30. Mukinayi BM, Cibeyibeyi GK, Tumba GD, Gulbis B. Sickle cell disease in the Democratic Republic of the Congo: what are the barriers to treatment using hydroxyurea. Pan Afr Med J. 2021;38:41. doi:10.11604/pamj.2021.38.41.18718
31. Ryan N, Dike L, Ojo T, et al. Implementation of the therapeutic use of hydroxyurea for sickle cell disease management in resource-constrained settings: a systematic review of adoption, cost and acceptability. BMJ Open. 2020;10(11):e038685. doi:10.1136/bmjopen-2020-038685
32. Adewoyin AS, Oghuvwu OS, Awodu OA. Hydroxyurea therapy in adult Nigerian sickle cell disease: a monocentric survey on pattern of use, clinical effects and patient’s compliance. Afr Health Sci. 2017;17(1):255–261. doi:10.4314/ahs.v17i1.31
33. Morrice J, Mupfururirwa W, Chianumba RI, et al. Sickle cell disease in Africa: sickleInAfrica Registry in Ghana, Nigeria and Tanzania. EJHaem. 2025;6(3):e70044. doi:10.1002/jha2.70044
34. Fogarty H, Gaul A, Syed S, et al. Adherence to hydroxyurea, health-related quality of life domains and attitudes towards a smartphone app among Irish adolescents and young adults with sickle cell disease. Ir J Med Sci. 2022;191(2):809–816. doi:10.1007/s11845-021-02588-1
35. Reddy PS, Cai SW, Barrera L, King K, Badawy SM. Higher hydroxyurea adherence among young adults with sickle cell disease compared to children and adolescents. Ann Med. 2022;54(1):683–693. doi:10.1080/07853890.2022.2044509
36. Isa HA, Nnebe-Agumadu U, Nwegbu MM, et al. Determinants of hydroxyurea use among doctors, nurses and sickle cell disease patients in Nigeria. PLoS One. 2022;17(11):e0276639. doi:10.1371/journal.pone.0276639
37. Ambrose EE, Kidenya BR, Charles M, et al. Outcomes of hydroxyurea accessed via various means and barriers affecting its usage among children with sickle cell anaemia in North-Western Tanzania. J Blood Med. 2023;Volume 14:37–47. doi:10.2147/JBM.S380901
38. Green NS, Manwani D, Aygun B, et al. Hydroxyurea Adherence for Personal Best in Sickle Cell Treatment (HABIT) efficacy trial: community health worker support may increase hydroxyurea adherence of youth with sickle cell disease. Pediatr Blood Cancer. 2024;71(4):e30878. doi:10.1002/pbc.30878
39. Walsh KE, Cutrona SL, Kavanagh PL, et al. Medication adherence among pediatric patients with sickle cell disease: a systematic review. Pediatrics. 2014;134(6):1175–1183. doi:10.1542/peds.2014-0177
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.