Back to Journals » Clinical Interventions in Aging » Volume 17
Bestform-F – Best Function of Range of Motion: A Feasibility Study of a Multimodal Exercise Training Program for Older Adults in Retirement Homes
Authors Schaller N ![]() , Krusemark H, Mende E, Weiß M, Spanier B, Zelger O, Bischof J, Haller B, Halle M, Siegrist M
, Krusemark H, Mende E, Weiß M, Spanier B, Zelger O, Bischof J, Haller B, Halle M, Siegrist M ![]()
Received 24 March 2022
Accepted for publication 14 June 2022
Published 11 July 2022 Volume 2022:17 Pages 1069—1080
DOI https://doi.org/10.2147/CIA.S367858
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Nina Schaller,1 Helge Krusemark,1 Esther Mende,1 Michael Weiß,1 Bianca Spanier,1 Otto Zelger,1 Jan Bischof,1 Bernhard Haller,2 Martin Halle,1,3,* Monika Siegrist1,*
1Department of Prevention and Sports Medicine, School of Medicine, University Hospital ‘rechts der Isar’, Technical University of Munich, Munich, Germany; 2Institute of AI and Informatics in Medicine, University Hospital ‘rechts der Isar’, Technical University of Munich, Munich, Germany; 3DZHK (German Center for Cardiovascular Research), Partner Site Munich Heart Alliance, Munich, Germany
*These authors contributed equally to this work
Correspondence: Nina Schaller, Department of Prevention and Sports Medicine, School of Medicine, University Hospital ‘rechts der Isar’, Technical University of Munich, Georg-Brauchle-Ring 56, Munich, 80992, Germany, Tel +49 89 289 24441, Fax +49 89 289 24451, Email [email protected]
Purpose: Mobility is a crucial factor for independence and quality of life in old age. Nevertheless, many old people in retirement homes do not meet the physical activity recommendations. The aim of the Bestform-F – Best Function of Range of Motion feasibility study (bestform-F) was to evaluate the feasibility of implementing a machine-based multimodal exercise training program in older residents in retirement homes.
Materials and Methods: The participants (n = 77) were recruited from two retirement homes and took part in a six-month multimodal exercise training program (2x/week, 45 minutes) on pneumatic strength training machines, a balance platform and bicycle ergometers. Feasibility criteria were recruitment number ≥ 35 participants within six months, dropout rate < 40% of participants within six months of exercise, and training adherence ≥ 50% of participants taking part in at least 50% of offered training sessions. Additionally, physical performance, fear of falling, cognitive function, and quality of life were assessed at baseline and after six months.
Results: For the bestform-F study, 77 (85.6 ± 6.6 years; 78% women) out of 215 eligible residents from two senior residences were recruited. The dropout rate over six months was 10% (8/77 participants). The training adherence rate for the finishing participants was 77% (53/69 participants). In addition to the achieved feasibility criteria, significant improvements were recorded in the Chair Stand Test, Six-Minute Walk Test, and fear of falling after six months.
Conclusion: All feasibility criteria have been fulfilled. The high number of recruited participants, the low dropout rate, and high adherence to the training program confirm the feasibility of a multimodal machine-based exercise training program offered to residents in retirement homes. The results provide a basis for a cluster-randomized controlled trial aimed at further investigating the efficacy of the bestform-F program.
Keywords: machine-based exercise, seniors, sarcopenia, mobility, resistance training, balance
Introduction
Aging is traditionally associated with functional and mental decline. Improved therapeutic strategies have increased average life expectancy in the Western world. However, this extra time does not necessarily expand the individuals’ healthy life span. Although the benefits of being mobile and active, including in old age (eg numerous health aspects, mental well-being and social interaction) are well known, most seniors do not meet common recommendations for physical activity.1
Inactivity leads to a decline in muscle mass and muscle function,2 promoting sarcopenia and frailty in old age. Both conditions are also associated with osteoporosis and an increased risk of fall-related injuries or death. In 2014, nearly 30% of older adults (≥ 65 years) in the United States reported at least one annual fall; approximately 27,000 older adults died as a result of falls; and 2.8 million seniors needed medical care in emergency departments.3 An important psychological aspect associated with falls is fear of falling, which can be observed in some 50% of older adults, and is often associated with the avoidance of activity4 and a decline in physical function. The consequences of limited or lost physical function have a major impact on the daily lives of seniors, who increasingly struggle with activities such as walking, climbing stairs, kneeling and carrying loads of five kilograms.5
Aging, in general, and all age-related conditions mentioned above, can be counteracted through physical activity, exercise and fall prevention programs.6,7 Regarding different training modalities, aerobic or strength training seems to have better effects than aqua fitness, at least in women over 60 years.8 Progressive resistance training also proofed to be effective in sarcopenic old men9 and oldest-old people.10 Most physical activity interventions in older adults are performed in the community-dwelling setting:11 structured exercise programs in retirements homes are rare occurrences. The heterogeneity of the settings, ranging from facilities of independent living to assisted living or care units, makes it more difficult to run and to compare interventions. When provided, they usually focus on fall prevention and are most commonly offered in nursing homes,12 hospitals and care facilities. Consequently, the overall effect on the rate of falls or risk of falling in these settings remain uncertain due to mixed results in the analyzed studies.13 We assume that the intensity of these programs is often too low (eg seated exercises), compared to evidence-based recommendations,14 in order to prevent a decline in muscle mass and muscle function. Age-adapted, structured and individually tailored machine-based resistance training therefore would appear to be a more effective option compared to a traditional fall prevention program. In contrast to gymnastic exercises, our approach, which involves training on pneumatic strength machines, offers several advantages: Movement pattern, range of motion, and exercise intensity can be defined individually and precisely. The resistance of each exercise can be adapted to enable each individual to progress on their own terms. Using technical and digital support (saved instrument settings), the machines enable largely independent and safe training for older adults. Further, playfully animated exercise games performed on a balance platform and ergometers suitably round off our multimodal training concept.
To our knowledge, there is a scarcity of data assessing the feasibility or impact of regular resistance training using sturdy, age-adapted strength training machines in retirement homes, like the ones customarily found in fitness clubs.13 Knowing this, we assessed as primary objective the feasibility of implementing a machine-based exercise training program for older (≥ 65 years) residents in retirement homes without any upper age limit by analyzing recruitment numbers, dropout rates, and adherence to the program. Secondary objectives were the assessment of physical function and physical performance, fear of falling, cognitive function and quality of life.
Materials and Methods
Study Design
The study “Bestform-F – Best Function of Range of Motion” (hereinafter referred to as “bestform-F”) was designed as a single-arm intervention feasibility study without a control group. To begin with, two senior retirement homes (a home with assisted living and a home with assisted living and care area) in Bavaria, southern Germany, were recruited. Various spatial options, including barrier-free access, age-adapted room design, furnishings, and training equipment, were pre-requested in order to set up a fitness gym for older adults. Figure 1 illustrates the study flow diagram.
 |
Figure 1 Participant flow diagram. |
The study was approved by the local ethics committee of the University Hospital “rechts der Isar”, Technical University of Munich, Germany (83/18S) in accordance with the Declaration of Helsinki. The trial registration number is DRKS00015051. The trial has been registered retrospectively. No changes have been made since commencement of the trial.
Recruitment of Participants
Potentially eligible residents (n=215, defined by staff members based on health status) and staff members of the two recruited retirement homes were informed about the feasibility study and exercise modalities through lectures and flyers. Interested residents were registered by the residential management. Screening appointments from June 2018 to December 2018, followed by baseline medical examinations, were organized by the residential management in consultation with the study coordinator.
Interested residents were included in the bestform-F study based on the following inclusion criteria: (1) permanent residence in one of the two participating retirement homes; (2) aged 65 or over; (3) ability to take part in a supervised group-based multimodal exercise training program without individual monitoring or support or medical supervision. Lastly, the participants’ written consent – after having been briefed on the requirements – was a mandatory requirement before they could take part in the study.
Exclusion criteria were as follows: (1) unstable cardiopulmonary diseases; (2) chronic inflammatory diseases; (3) acute illness; or (4) any other medical condition that, in the opinion of supervising physician, significantly limits exercise training. Orthopedic problems, walking aids, or non-permanent wheelchair assistance or frailty were not defined as exclusion criteria so as to cover a broad spectrum of older residents.
Intervention
All included participants took part in a supervised six-month multimodal exercise intervention program consisting of a combination of machine-based resistance, coordination and aerobic endurance training.
Exercise was offered on pneumatic strength training machines, a balance platform and bicycle ergometers (HUR® Deutschland GmbH, Freudenstadt, Germany, http://www.hur-deutschland.de). The training equipment also included easy-access machines for wheelchair users. All training devices were age-adapted and therefore offered high levels of safety, ease of operability, minimalism, and quality.
Resistance training focused on general strength training for the major muscle groups: elbow extensors/flexors, shoulders, chest, abdomen, upper/lower back, hip extensors, knee extensors/flexors. The training took place at least twice a week for 45 minutes at a time in fitness rooms established within the retirement homes prior to commencement of the study. The first eight weeks of the intervention served as an acclimation period, implementing progressive muscular endurance training (2 sets, 15–20 repetitions). This was followed by the introduction of progressive muscular hypertrophy training (2–3 sets, 12 repetitions). Coordination and balance training included standing balance, dynamic weight shifts, and stepping strategies, all performed on a balance platform, either before or after resistance training. Coordination and balancing exercises were conducted with an increasing level of difficulty and an increasing amount of variety. Aerobic endurance training was performed on a recumbent bicycle ergometer, a bicycle ergometer, or an upper-body ergometer. It was performed over a period of 5–15 minutes as general aerobic endurance training, either at the beginning or the end of the training session.
All training sessions were organized in small groups comprising 4–6 participants, which were instructed and supervised by sports scientists and supported by sports students or local physiotherapists. The trainers adjusted the individual device settings and increased the workloads according to the progressive training protocol from the beginning to the end of the training period, instructed the participants to correctly perform the exercises and provided support when changing the training machine, if necessary. By the end of the training period most participants were able to exercise mainly independently, but adherence to the training protocol was still supervised by the trainers. All contents of the training were carefully tailored to the individual needs of each participant based on their physical state and mental mood on the day of training or existing comorbidities. Participants were interviewed during each training session to assess their training-related side effects or exercise barriers. Adherence to the training was documented continuously, as were any side effects and dropouts.
Outcome Assessments and Measurements
Assessments were performed before the start of the study intervention (baseline examination t0 = −2 – 0 weeks before the beginning of the exercise intervention (t1); after three months intervention (t2); and at the end of the intervention after six months (t3) (Figure 1)). These included blood samples, medical history, a clinical examination, and an electrocardiogram (ECG). Following this, the participants’ physical and mental performance was assessed by sport scientists, and the questionnaires were completed together with the participants.
Primary Outcome: Feasibility of the Exercise Training Program
Feasibility was assessed by the number of recruited subjects, dropout rate, and adherence to the training. The recruitment rate was documented during the recruiting period from June 2018 until the end of 2018. The dropout rate was examined by the study coordinators from the beginning of the study until the end of the six-month exercise intervention period. The dropout rate was defined as the percentage of participants who dropped out of the study for any reason, eg death; withdrawal of consent and discontinuation of training due to severe injury; illness; or a general deterioration of physical/mental health status. The adherence of the participants to the training was documented during every training session over the six-month intervention period.
All of the three following feasibility criteria had to be fulfilled for the pilot study to be considered successful:
- Recruitment of at least 35 participants within six months
- Dropout rate < 40% within six months of exercise
- Adherence to the training program ≥ 50% of participants taking part in at least 50% of offered training sessions.
Side effects were documented by the trainers where these were related to the training and reported to the study coordinators. The participants were instructed to inform the trainer or the study coordinators whenever they experienced any unintended signs or symptoms connected with the training.
Secondary Outcomes
The following secondary outcomes were analyzed in an exploratory manner over six months:
- Changes in physical function and physical performance measured by the Timed Up and Go Test,15,16 by the Chair Stand Test,17 by a Static Balance Test,17 and by a Six-Minute Walk Test18
- Change in fear of falling measured by the Falls Efficacy Scale - International19
- Changes in cognitive function using the Clock Drawing Test using the Shulman system20
- Change in quality of life using the WHO-5 Well-Being Index.21
Secondary outcomes were measured at baseline, after three and six months. Data from the baseline and after six months are reported in this manuscript.
Physical Function, Fall Risk and Physical Performance
To determine physical function, risk of falling and physical performance, the following standardized examinations were applied: in the Timed Up and Go Test (TUG), which is an indicator for balance ability and mobility, the seniors were asked to stand up from a standard chair (seat height between 40 and 50 cm), walk a distance of three meters as quickly and as safely as possible, turn around, walk back to the chair, and sit down. The time was recorded from the start signal given by the investigator until the participant was sitting on the chair once again.15,16 The Chair Stand Test (CST) measures the time it takes to complete five rapid chair rise cycles (sit to stand to sit). Quick performances reflect a better functional strength of the lower extremity and a dynamic balance capability. Static balance capability was assessed using three different standing positions (side-by-side, semi-tandem, and tandem position of the feet) and the participants were asked to maintain each position for ten seconds. If the participants were able to stand in the side-by-side stand for ten seconds, the semi-tandem stand was tested. If participants were able to stand in the semi-tandem position for ten seconds, the tandem position was tested. The sum total of balance time (in seconds) was recorded.17
To determine cardiopulmonary performance, a Six-Minute Walk Test was performed.18,22 To do this, participants needed to walk at their own pace for six minutes, but do so back and forth as rapidly as possible across a 30-meter-long course. During the walk, participants were informed about the time and regularly asked about their well-being. The distance covered (in meters) was recorded after six minutes.
Fear of Falling
Fear of falling was assessed by the German version of the Falls Efficacy Scale - International, which was developed by the Prevention of Falls Network Europe (ProFaNE). It comprises 16 questions relating to everyday activities, each consisting of a choice of four responses (1 = not at all concerned; 4 = very concerned).19
Cognitive Function
The Clock Drawing Test by Shulman was used to assess cognitive function.20,23 The participants were asked to draw a clock face, complete with clock hands, in a pre-drawn circle for a specific time (10 after 11). A perfectly drawn clock, including the correct clock face and both hands showing the correct time, scores one point and indicates that the drawer’s cognitive function is unrestricted. No representation at all would score six points and indicate that the individual has impaired cognitive function.
Quality of Life
Quality of life was assessed using the WHO-5 Well-Being Index. This validated screening tool for depression and widely-used outcome measure in clinical trials consists of five statements, each offering six response options rated from “at no time” (0 points) to “all of the time” (5 points). The resulting score ranges from 0 (worst imaginable well-being) to 100 (best imaginable well-being).21
Adverse Events and Serious Adverse Events
Adverse events (AEs) were defined as all negative health events newly occurring in temporal relation to the training, and any events that could not be explained by the age or the health status of the participant and were not related to other everyday behaviors. Serious adverse events (SAEs) were recorded as follows: events related to the training and resulting in injuries, hospitalization, lasting physical damage, life-threatening events or death. In addition, before each training session, every participant was asked about the current health status and possible side effects. Whenever adverse events occurred, the next steps (adjustment of the training, temporary or complete interruption of the training) were coordinated with the sports scientists.
Statistics and Data Analysis
By way of determining the feasibility of the study, the number of residents recruited within a period of six months and the relative frequency of included residents out of all residents screened for eligibility are presented. The proportion of included residents dropping out of the study, their reasons for attrition as well as the proportion of included residents taking part in at least 50% of the offered training sessions are reported.
Data on physical function, physical performance, fear of falling, cognitive function, and quality of life, are summarized by means and standard deviations as well as medians and minimum/maximum values at baseline and at six months after initiation of the treatment. As all secondary endpoints were not normally distributed, Wilcoxon Signed-Rank Tests were performed to assess changes from baseline to six months. All statistical tests were performed two-sided on a significance level of 5% using IBM® SPSS® Statistics, Version 25.
Results
Participants
For the bestform-F study, 77 participants (mean age: 85.6 ± 6.6 years; 60 females) from two senior residences were enrolled over a recruitment period of six months. Nearly half of the participants (43%) had reported at least one fall during the last twelve months. The most common comorbidities were joint or back pain (73%), and hypertension (68%). The baseline characteristics of the participants are listed in Table 1.
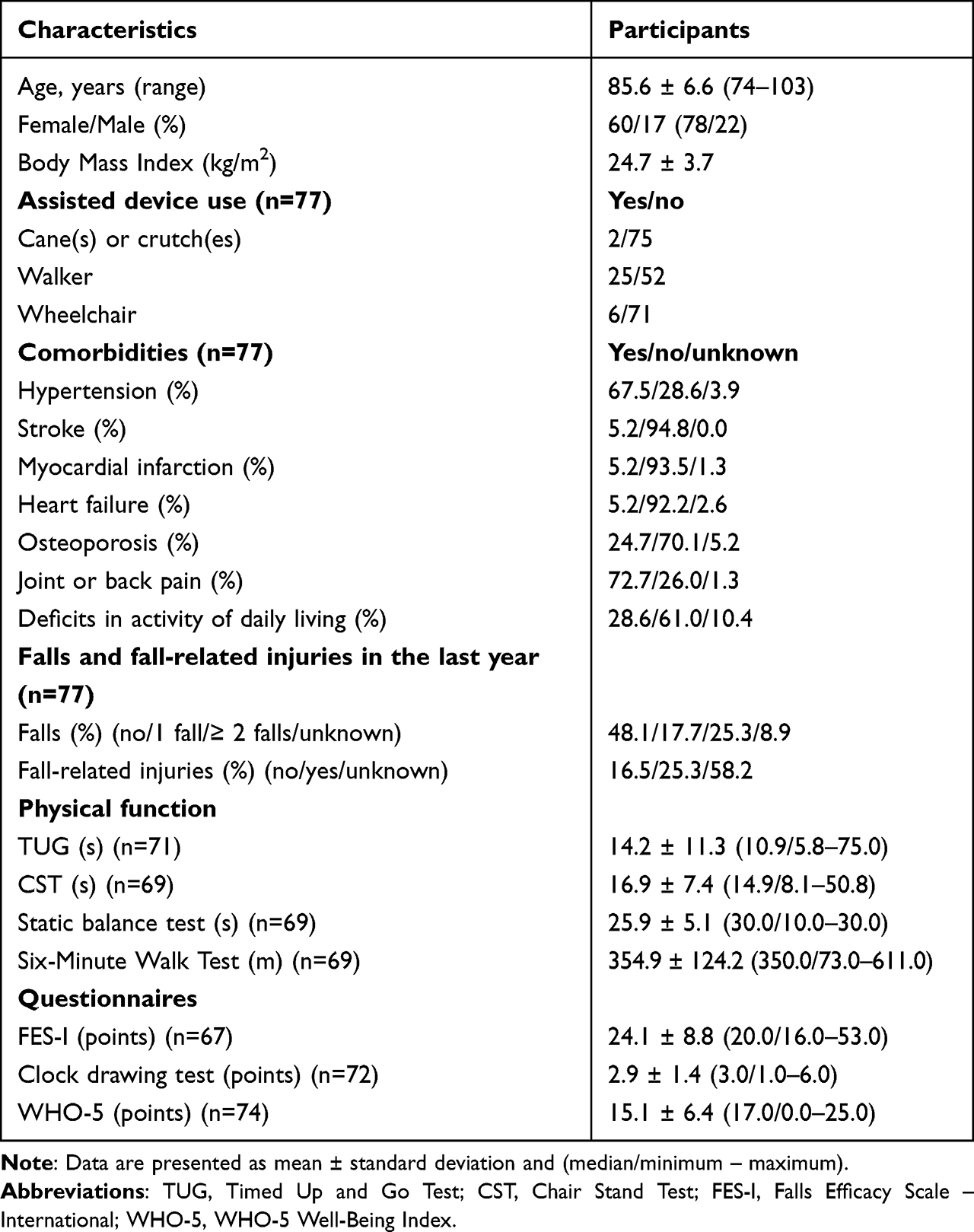 |
Table 1 Baseline Characteristics of the Participants |
Primary Outcome: Feasibility
The 77 participants were recruited from 215 eligible residents. This corresponds to a recruitment rate of 36%.
The dropout rate during the study period was 10% (8 of 77 participants). The reasons for dropping out were death (n = 4); severe falls (n = 2, not during training sessions); weakness in combination with blood pressure fluctuations (n = 1); and severe mobility restrictions (n = 1) (Figure 1).
Adherence to the exercise program (participation in at least 50% of the offered training sessions) was fulfilled in 77% of the finishing seniors (53/69 participants) over a six-month period (Table 2).
 |
Table 2 Feasibility Criteria for the Study |
No adverse or serious adverse events associated with the training had to be documented.
Secondary Outcomes
In addition, the following secondary endpoints were examined at baseline and after six months, and analyzed in an exploratory manner.
Physical Function, Fall Risk and Physical Performance
Physical function, fall risk and physical performance were measured using the TUG, the CST, the Static Balance Test, and the Six-Minute Walk Test. Participants showed significant improvements in the CST, and needed less time after six months (median baseline value: 14.4 seconds; median value after six months: 12.7 seconds, p = 0.022). The median walking distance in the Six-Minute Walk Test improved significantly from 394 m to 407 m (p = 0.037). No statistically significant changes were recorded in TUG or static balance over six months (Table 3).
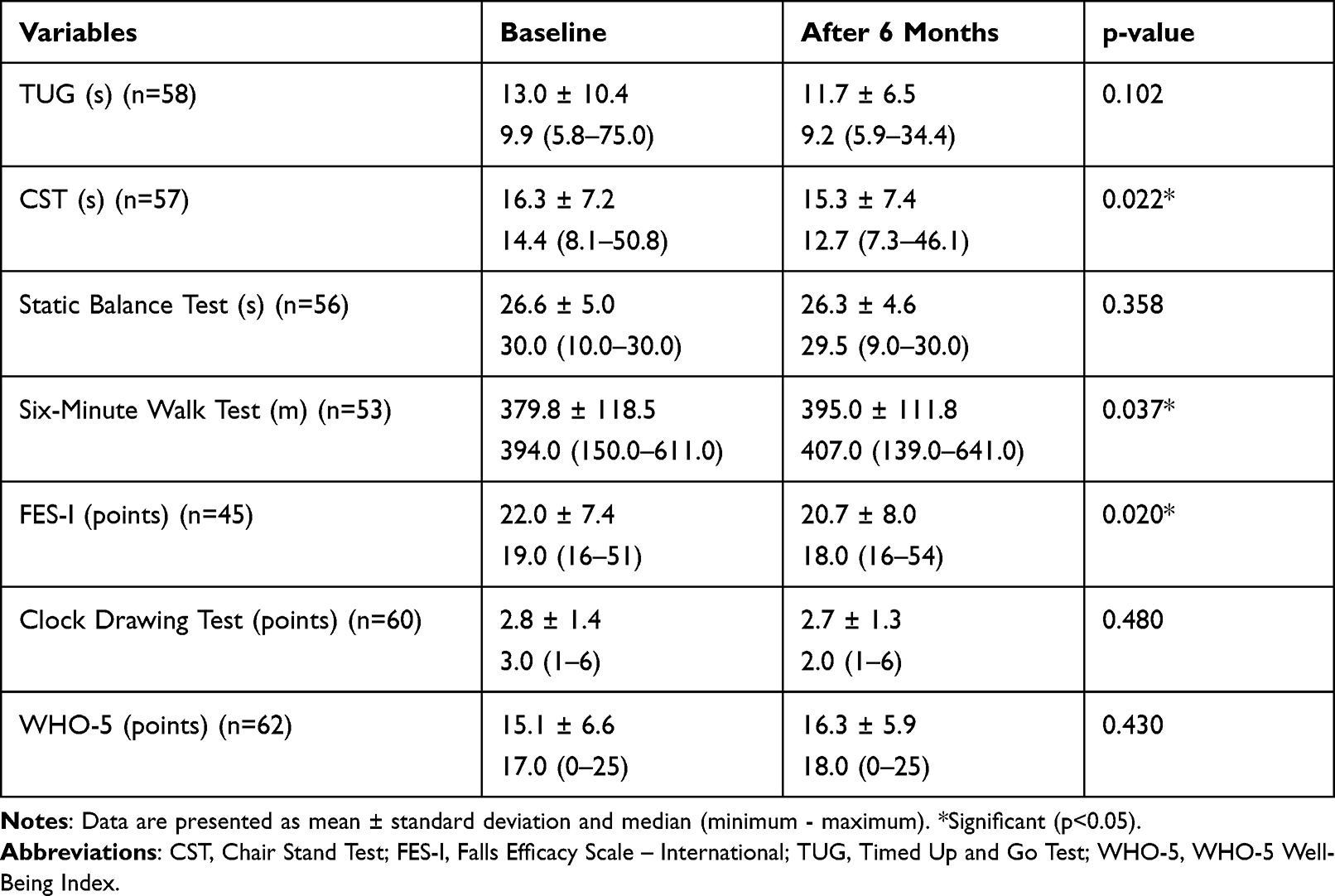 |
Table 3 Changes in Secondary Endpoints Over Six Months |
Fear of Falling
A significant reduction in fear of falling was observed, with the Falls Efficacy Scale – International measuring lower values, representing less fear of falling, after six months (baseline median value: 19.0 points; median value after six months: 18.0 points, p = 0.020; Table 3).
Cognitive Function
No statistically significant improvements in cognitive function, measured using the Clock Drawing Test, were recorded over six months (baseline median value: 3.0 points; median value after six months: 2.0 points, p = 0.480; Table 3).
Quality of Life
Participants reported a comparable quality of life after six months, as determined using the WHO-5 Well-Being Index, with 17.0 points (median value) at baseline and 18.0 points (median value) after six months (p = 0.430) (Table 3).
Discussion
Feasibility was confirmed for all feasibility criteria:
Firstly, the projected recruitment of 35 participants more than doubled, with 77 seniors out of 215 eligible residents starting the training. This reflects a high recruitment rate of 36%.
Secondly, the dropout rate was lower than expected. Only 10% of the participants dropped out over the six-month period, far less than a maximum assumed 40% dropout rate. The main reason for participants dropping out was death (n = 4), which was not unexpected as the participating persons were aged between 74 and 103 years. Other reasons for the dropout rate were severe fall-related injuries (n = 2), which led to these individuals needing long-time nursing care, severe mobility limitations (n = 1), and weakness in combination with blood pressure fluctuations (n = 1).
Thirdly, the adherence rate was higher than expected. When planning the feasibility study, it was assumed that at least 50% of the participants would take part in at least 50% of the offered training sessions. Due to age-related diseases, it was not anticipated that all participants would be able to take part in the training on a regular basis. Contrary to these expectations, 77% of the participants fulfilled the adherence criteria and, on average, the participants regularly took part in 67% of the offered training sessions (median value: 74%). The main reasons for low adherence were diseases or injuries (eg fall-related injuries, flue-like infections) and participants taking vacation.
Regarding the secondary outcomes, certain significant improvements were observed in physical function. After six months, the median time needed for the CST significantly decreased (p = 0.022) by more than one second, reflecting a slightly improved physical function of about 7%. This result is in line with some other studies: Gianoudis et al24 reported an 11% improvement among younger seniors (67 ± 6 years) in the 30-Second Sit to Stand Test after a six-month training intervention compared to no improvements in the control group. Lacroix et al25 also found significant increases in the CST in older adults (73 ± 4 years) after a three-month training intervention.
The median walking distance in the Six-Minute Walk Test improved by 3.3% after six months of training (p = 0.037). The results indicate slight improvements in physical performance and mobility. The participants’ average walking distance was above the discriminatory value of 350 m at baseline and after six months of training. Values below this threshold reflect an increasing risk of hospitalization and death.26 At baseline 56.6% of the seniors (n=30/53) and after six months of training 64.2% (n=34/53) were above this threshold.
Moreover, our participants reported a significantly decreased fear of falling, down by 1.7 points (p = 0.020). These improvements are important for health preservation, mobility, and independence among older adults.4 We found similar results in a cluster-randomized trial in a primary care setting. In this study, fear of falling was significantly reduced by 1.8 points, whereas a passive control group undergoing usual care recorded no improvements in fear of falling.27
No further improvements were observed (eg in cognitive function or in quality of life), or the improvements proved to be insignificant (eg in static balance and in TUG) after six months. In the absence of exercise, age-related decline can be expected, as shown in the above-mentioned passive control group in our former cluster-randomized trial involving 378 community-dwelling older adults.27 Consistent performances in TUG and Static Balance Tests after six months of training can therefore be taken as an indicator for the efficacy of the bestform-F program. Our working group recently published a systematic review and meta-analysis regarding the effects of progressive resistance training on physical performance in sarcopenic oldest old.10 Inter alia, significant improvements in CST and improvements in the TUG and the Six-Minute Walk test were shown, whereas the quality of evidence of the included trials was low to moderate. Studies that were carried out in retirement homes were also included. Three of these studies28–30 showed improvements in physical function and grip strength, while another review13 showed inconclusive results.
The unique aspect of our study is the location: the training intervention took place in retirement homes. The setting approach has great potential, as older people living in retirement homes only need to cover short distances in order to reach their training location and usually have enough time to exercise. Regular exercise sessions can easily be integrated into the daily routine. Moreover, there is potential for the fitness gym inside the residential home to become an “active meeting area”, resulting in improved social contacts between residents and reduced loneliness as additional benefits of group-based physical activity intervention programs.31
Finally, maintaining the mobility, independence and quality of life of the residents can decrease the physical workload and associated lower back pain of the staff members in residential homes,32 as fewer bed to chair transfers or mobility support are needed.
Conclusion
Multimodal machine-based exercise training is feasible among older adults who live in retirement homes. The high adherence rate and the low dropout rate confirm that even residents with a mean age of 85.6 years could be motivated to exercise regularly at least for six months, irrespective of any pre-existing minor physical or cognitive impairments.
There is evidence suggesting that this program improves physical function and fear of falling, thus grants a cluster-randomized trial within retirement homes to further investigate the clinical impact and efficacy.
Data Sharing Statement
In accordance with the data protection regulations of our clinic, the data set for the primary endpoint is available upon request from the corresponding author.
Acknowledgments
We would like to thank all collaborating partners who helped to realize the bestform-F project, especially the Beisheim Stiftung, Munich, Germany, for its funding. We further thank the management and the staff of the two participating retirement homes (KWA Stift Rupertihof and Diakoniewerk München-Maxvorstadt) who were involved in the recruitment process and the implementation of the training program. We are additionally grateful for the help provided by all trainers and students who assisted the training sessions and for the support given by all medical technical assistants. Finally, we would like to thank all participating seniors for taking part in our bestform-F feasibility study.
Author Contributions
NS, MS, and MH designed the study and obtained funding. NS, MS, EM, MW and MH designed and wrote the original proposal. BH and MS developed the statistical analysis plan. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, data analysis and interpretation, manuscript preparation or in all these areas, have read, critically reviewed and approved the final manuscript; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The work was funded by the Beisheim Stiftung, Munich, Germany. The study funder played no role in the development of the study design and had no influence on the collection, management or interpretation of the data.
Disclosure
The authors report no conflict of interests in this work.
References
1. Haskell WL, Lee I-M, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1081.
2. Larsson L, Degens H, Li M, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev. 2018;99(1):427–511. doi:10.1152/physrev.00061.2017
3. Bergen G. Falls and fall injuries among adults aged≥ 65 years—United States, 2014. Morb Mortal Wkly Rep. 2016;65(37):993–998. doi:10.15585/mmwr.mm6537a2
4. Zijlstra G, Van Haastregt J, Van Eijk JTM, van Rossum E, Stalenhoef PA, Kempen GI. Prevalence and correlates of fear of falling, and associated avoidance of activity in the general population of community-living older people. Age Ageing. 2007;36(3):304–309. doi:10.1093/ageing/afm021
5. Leiros-Rodriguez R, Ronno-Perez V, Garcia-Soidan JL, Soto-Rodriguez A. Prevalence and factors associated with functional limitations during aging in a representative sample of Spanish population. Phys Occup Ther Geri. 2018;36(2–3):156–167. doi:10.1080/02703181.2018.1449163
6. Gardner MM, Buchner DM, Robertson MC, Campbell AJ. Practical implementation of an exercise‐based falls prevention programme. Age Ageing. 2001;30(1):77–83. doi:10.1093/ageing/30.1.77
7. Hopewell S, Adedire O, Copsey BJ, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7:CD012221. doi:10.1002/14651858.CD012221.pub2
8. Leiros-Rodriguez R, Romo-Perez V, Perez-Ribao I, Garcia-Soidan JL. A comparison of three physical activity programs for health and fitness tested with older women: benefits of aerobic activity, aqua fitness, and strength training. J Women Aging. 2019;31(5):419–431. doi:10.1080/08952841.2018.1510242
9. Lichtenberg T, von Stengel S, Sieber C, Kemmler W. The favorable effects of a high-intensity resistance training on sarcopenia in older community-dwelling men with osteosarcopenia: the Randomized Controlled FrOST Study. Clin Interv Aging. 2019;14:2173–2186. doi:10.2147/CIA.S225618
10. Mende E, Moeinnia N, Schaller N, et al. Progressive machine-based resistance training for prevention and treatment of sarcopenia in the oldest old: a systematic review and meta-analysis. Exp Gerontol. 2022;163:111767. doi:10.1016/j.exger.2022.111767
11. Zubala A, MacGillivray S, Frost H, et al. Promotion of physical activity interventions for community dwelling older adults: a systematic review of reviews. PLoS One. 2017;12(7):1–36. doi:10.1371/journal.pone.0180902
12. Becker C, Rapp K. Fall prevention in nursing homes. Clin Geriatr Med. 2010;26(4):693–704. doi:10.1016/j.cger.2010.07.004
13. Cameron ID, Dyer SM, Panagoda CE, et al. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev. 2018;2018(9):1–385.
14. Fragala MS, Cadore EL, Dorgo S, et al. Resistance training for older adults: position statement from the National Strength and Conditioning Association. J Strength Cond Res. 2019;33(8):2019–2052. doi:10.1519/JSC.0000000000003230
15. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
16. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the timed Up & Go test. Phys Ther. 2000;80(9):896–903. doi:10.1093/ptj/80.9.896
17. Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A. 2000;55(4):M221–M231. doi:10.1093/gerona/55.4.M221
18. ATS. Committee on proficiency standards for clinical pulmonary function laboratories ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
19. Kempen GI, Todd CJ, Van Haastregt JC, et al. Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in older people: results from Germany, the Netherlands and the UK were satisfactory. Disabil Rehabil. 2007;29(2):155–162. doi:10.1080/09638280600747637
20. Shulman KI. Clock‐drawing: is it the ideal cognitive screening test? Int J Geriatr Psychiatry. 2000;15(6):548–561. doi:10.1002/1099-1166(200006)15:6<548::AID-GPS242>3.0.CO;2-U
21. Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. 2015;84(3):167–176. doi:10.1159/000376585
22. Enright PL. The six-minute walk test. Respir Care. 2003;48(8):783–785.
23. Aprahamian I, Martinelli JE, Neri AL, Yassuda MS. The Clock Drawing Test a review of its accuracy in screening for dementia. Dement Neuropsychol. 2009;3(2):74–80. doi:10.1590/S1980-57642009DN30200002
24. Gianoudis J, Bailey CA, Ebeling PR, et al. Effects of a targeted multimodal exercise program incorporating high-speed power training on falls and fracture risk factors in older adults: a community-based randomized controlled trial. J Bone Miner Res. 2014;29(1):182–191. doi:10.1002/jbmr.2014
25. Lacroix A, Kressig RW, Muehlbauer T, et al. Effects of a supervised versus an unsupervised combined balance and strength training program on balance and muscle power in healthy older adults: a randomized controlled trial. Gerontology. 2016;62(3):275–288. doi:10.1159/000442087
26. Agarwala P, Salzman SH. Six-minute walk test: clinical role, technique, coding, and reimbursement. Chest. 2020;157(3):603–611. doi:10.1016/j.chest.2019.10.014
27. Siegrist M, Freiberger E, Geilhof B, et al. Fall prevention in a primary care setting. Dtsch Arztebl Int. 2016;113(21):365–372. doi:10.3238/arztebl.2016.0365
28. Cadore EL, Casas-Herrero A, Zambom-Ferraresi F, et al. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age. 2014;36(2):773–785. doi:10.1007/s11357-013-9586-z
29. Hassan BH, Hewitt J, Keogh JW, Bermeo S, Duque G, Henwood TR. Impact of resistance training on sarcopenia in nursing care facilities: a pilot study. Geriatr Nurs. 2016;37(2):116–121. doi:10.1016/j.gerinurse.2015.11.001
30. Hewitt J, Goodall S, Clemson L, Henwood T, Refshauge K. Progressive resistance and balance training for falls prevention in long-term residential aged care: a cluster randomized trial of the sunbeam program. J Am Med Dir Assoc. 2018;19(4):361–369. doi:10.1016/j.jamda.2017.12.014
31. Franke T, Sims-Gould J, Nettlefold L, Ottoni C, McKay HA. “It makes me feel not so alone”: features of the Choose to Move physical activity intervention that reduce loneliness in older adults. BMC Public Health. 2021;21(1):ARTN312. doi:10.1186/s12889-021-10363-1
32. Otto AK, Pietschmann J, Appelles LM, et al. Physical activity and health promotion for nursing staff in elderly care: a study protocol for a randomised controlled trial. BMJ Open. 2020;10(10):e038202. doi:10.1136/bmjopen-2020-038202
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unveiling Seniors’ Perception of Mobility: Urbanization, Region, and Physical Activity
Maresova P, Komarkova L, Horak J, Krejcar O, Kukuliac P, Vitkova L, Joukl M, Truhlarova Z, Tomsone S
Patient Preference and Adherence 2023, 17:3015-3031
Published Date: 20 November 2023
Non-Pharmacological Strategies for Managing Sarcopenia in Chronic Diseases
Hu J, Wang Y, Ji X, Zhang Y, Li K, Huang F
Clinical Interventions in Aging 2024, 19:827-841
Published Date: 15 May 2024