Back to Journals » Clinical Ophthalmology » Volume 20
Bench Evaluation of Intraocular Pressure Control with Clinical Assessment of Anterior Chamber Stability of a Dual Peristaltic Phacoemulsification Device
Authors Berdahl J ![]() , Terveen D
, Terveen D ![]() , Aboughaida A, Dyk DW
, Aboughaida A, Dyk DW ![]() , Yalamanchili S, Makari S, Thompson V
, Yalamanchili S, Makari S, Thompson V
Received 15 October 2025
Accepted for publication 2 February 2026
Published 11 February 2026 Volume 2026:20 570189
DOI https://doi.org/10.2147/OPTH.S570189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
John Berdahl,1 Daniel Terveen,1 Ali Aboughaida,2 David William Dyk,2 Satish Yalamanchili,2 Sarah Makari,2 Vance Thompson1
1Vance Thompson Vision, Sioux Falls, SD, USA; 2Research & Development, Alcon Research LLC, Fort Worth, TX, USA
Correspondence: John Berdahl, Vance Thompson Vision, 3101 W 57th S.t, Sioux Falls, SD, 57108, USA, Email [email protected]
Purpose: To demonstrate intraocular pressure (IOP) control using the UNITY® Vitreoretinal Cataract System (UVCS) during cataract surgery based on bench testing and initial clinical experience.
Patients and Methods: Bench testing using an eye model and calibrated pressure sensor measured IOP control error by evaluating the pressure difference between the IOP setpoint and the measured IOP under continuous irrigation for approximately 10 seconds followed by aspiration for approximately 15 seconds. To examine the system at its limits, 30 phacoemulsification (phaco) handpieces were tested at 20 mmHg IOP and 60 cc/min aspiration flow rate, and 15 irrigation/aspiration (I/A) handpieces were tested at 20 mmHg IOP and 30 cc/min aspiration flow rate. In addition, a prospective, single-arm clinical study evaluated the safety and performance of UVCS in adults presenting for routine cataract surgery (clinicaltrials.gov, NCT06071104, Registered October 2, 2023).
Results: The expected IOP variation at an IOP setpoint of 20 mmHg was 2.36 ± 2.13 at an aspiration flow rate of 60 cc/min during phaco and 4.19 ± 1.97 mmHg at an aspiration flow rate of 30 cc/min during I/A. These results compare favorably to physiologic IOP diurnal variation in normal patients (5.0 ± 2.7 mmHg) and demonstrate that IOP would be expected to be maintained approximately within 18 to 22 mmHg when the IOP is set to 20 mmHg during the phacoemulsification step. This is supported by results from the clinical study where 68 subjects underwent cataract surgery using UVCS, with exceptional anterior chamber stability observed during all cases.
Conclusion: UNITY VCS/CS demonstrates excellent IOP control in bench testing and was reported to provide exceptional AC stability clinically. Maintaining IOP at the desired surgeon setpoint with minimal fluctuation throughout surgery may reduce intraoperative and postoperative complications, especially in more complex cases.
Keywords: cataract surgery, anterior chamber stability, irrigation, aspiration, UNITY Vitreoretinal Cataract System
Introduction
While cataract surgery has a high safety profile and success rate, significant fluctuations in IOP may be induced during key phases of the procedure, including phacoemulsification (phaco) and irrigation/aspiration (I/A).1,2 Intraocular pressure (IOP) plays an important role in anterior chamber (AC) stability, which is critical for ensuring safety throughout the procedure and achieving optimal postoperative outcomes.3 Maintaining AC stability is influenced by a phacoemulsification system’s fluidics, which can rapidly shift during surgery.4 Older gravity-based fluidic systems lack mechanisms for fluid loss compensation, and as such, are not able to actively maintain IOP at set values. Active-fluidics systems allow for improved detection and maintenance of IOP when aspiration flow is activated, which is essential for AC stability especially during occlusion break surge events.5,6 Reducing IOP variation during cataract surgery may provide several advantages and have been associated with reduced corneal damage and anterior chamber inflammation during the early postoperative period.1 To achieve successful surgical performance, modern phacoemulsification systems have been focused on innovations to provide excellent intraoperative IOP control accuracy at different steps of cataract surgery.
Earlier phaco systems, such as the CENTURION® Vision System (Alcon Vision LLC), employed peristaltic aspiration for fluid control and an active-fluidics mechanism to modulate infusion fluid source pressure to maintain desired surgical IOP. The UNITY® Vitreoretinal Cataract System/ Cataract System (UVCS/UCS; Alcon Vision LLC) was introduced in 2025 and features a dual peristaltic system that includes an infusion pump in addition to an aspiration pump to control pressure and flow both into and out of the eye. This system allows for real-time sensing, independent and precise control of irrigation and aspiration, enhanced dynamic leakage compensation, and pressure stability at the desired IOP.
To evaluate the effectiveness of the UVCS in maintaining intraoperative IOP, an experimental bench study was performed under controlled conditions using a mechanical model of the human eye.7 In addition, a prospective clinical study was conducted to assess the performance of UVCS in a clinical setting. This study aims to evaluate the IOP control using UVCS during cataract surgery based on bench testing and initial clinical experience.
Materials and Methods
Study Design and Ethics
The bench study did not involve human or animal subjects and therefore did not require ethical approval. The clinical investigation was conducted in compliance with Good Clinical Practice and with international and national regulations, laws, and guidelines such as ISO 14155:2020 where applicable; and in accordance with the ethical medical research principles outlined in the Declaration of Helsinki. The protocol and all amendments, the informed consent form, any other written information given to subjects, and any advertisements planned for subject recruitment were approved by an IRB/IEC before initiation of study-related procedures. Informed consent was obtained from all subjects and documented prior to the initiation of any study-specific procedures. The study was approved by Sterling Institutional Review Board (IRB), an Independent Review Board registered with the Office of Human Research Protections (OHRP) and US Food and Drug Administration (FDA) (IRB registration number: IRB00001790; parent organization number: IORG0001354). The protocol was approved under IRB ID: 11378-JPBerdahl. This study was registered on ClinicalTrials.gov (NCT06071104, Registered October 2, 2023).
Bench Testing
A mechanical spring eye model that represents average human eye compliance, as described in Dyk et al,7 a calibrated IOP sensor (CPC6000, Mensor LP), and an oscilloscope (WaveRunner 606Zi, LeCroy) were utilized to measure and determine IOP variation at different surgical steps using the UVCS with the experimental setup shown in Figure 1. IOP readings were measured with an oscilloscope under continuous irrigation for approximately 10 seconds followed by aspiration for approximately 15 seconds. IOP variation was determined as: IOP variation = [Average IOP with Flow (at steady state)] – [IOP Setpoint]. 30 phaco handpieces (UNITY Phaco Handpiece with 0.9 mm Balanced Tip; Alcon Vision LLC) were tested at an IOP setpoint of 20 mmHg and aspiration flow rate of 60 cc/min, and 15 I/A handpieces (Alcon Vision LLC) were tested at an IOP of 20 mmHg and aspiration flow rate of 30 cc/min as outlined in Table 1. The lowest, most physiological IOP and the highest aspiration flow rates were selected to test the system at its limits. In addition, the differences in accessory resistance made it necessary to select different flow rates based on the access to reach the flowrate within the test timespan. This study was designed to evaluate IOP variation during flow at steady state. The bench portion of this study was designed to characterize general IOP control performance as a singular performance metric by evaluating IOP consistency across varying user-initiated flow demands and targets.
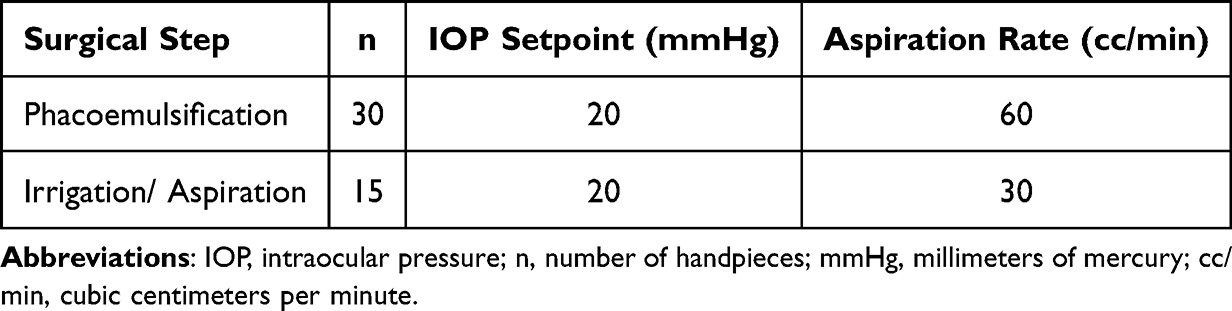 |
Table 1 Bench Testing: Intraoperative Parameters for IOP Maintenance Accuracy Testing at Flow vs Setpoint |
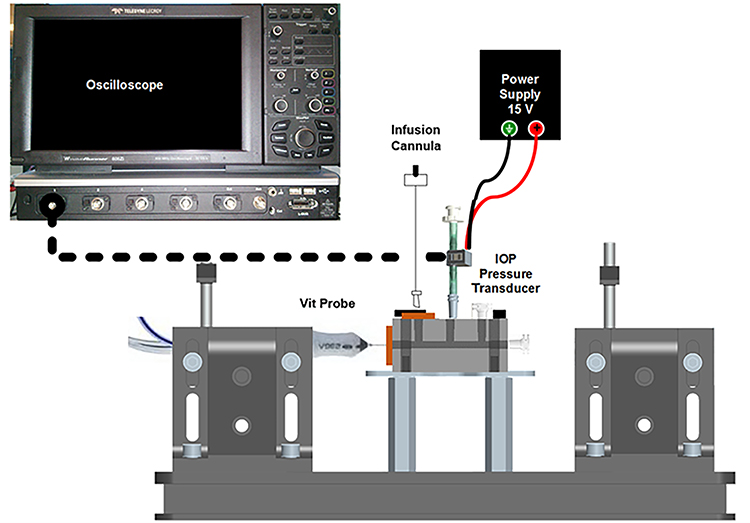 |
Figure 1 Experimental Bench Testing Setup. Abbreviations: IOP, intraocular pressure; V, volts. |
Data were analyzed using descriptive statistics only. No hypothesis testing was performed. Values measured are presented as means ± standard deviations. All analyses were conducted using the Microsoft 360 Excel® software Version 2408 (Microsoft Corp).
Clinical Study
The results of the bench study were corroborated with a prospective, interventional, open-label, single-arm, nonrandomized and multicenter clinical study conducted in the United States. This study represents the first clinical use of UVCS in cataract patients. Adults (>18 years of age) with a clinically documented diagnosis of age-related noncomplicated cataracts and eligible to undergo primary hydrophobic acrylic intraocular lens implantation into the capsular bag were included in this trial. Subjects underwent cataract removal with UVCS and followed prospectively for approximately 1 month to evaluate the safety and performance of the device. This study was designed to mirror the real world setting by allowing the site’s standard of care for surgery. After the last subject surgery, surgeons were asked if they “Strongly Disagree (1)”, “Disagree (2)”, “Neither Agree or Disagree (3)”, “Agree (4)”, or “Strongly Agree (5)” to the following statement: “Compared to your current system, UNITY VCS Fluidics provides more anterior chamber stability”. All surgeons’ current system was identified as the CENTURION Vision System with ACTIVE SENTRY® (CAS; Alcon Vision LLC). The present study discusses the results from one site, involving three surgeons. All surgeons at this site used the same phaco handpiece, tip, and sleeve for all surgeries (ACTIVE SENTRY Handpiece with 0.9 mm 45-degree Balanced Tip and Ultra Sleeve; Alcon Vision LLC). All surgeons reported the same settings for both UVCS and their current device, CAS. Vacuum limit and flow rate was set at 525 mmHg and 40 cc/min for all surgeons, respectively, and IOP setpoint was 40 mmHg for two surgeons and 50 mmHg for one surgeon.
Results
Bench Testing
As shown in Table 1, the IOP setpoint is at its lowest and aspiration flow rate is at its highest such that the IOP variations values presented in Table 2 are a worst-case scenario for the system. In other words, these results represent the highest expected IOP variation for each surgical step during cataract surgery. The IOP variation for UVCS at flow vs setpoint was 2.36 ± 2.13 mmHg and 4.19 ± 1.97 mmHg during phacoemulsification and irrigation/aspiration, respectively. Figure 2 illustrates the distribution and variation in IOP across both surgical steps. These results demonstrate that IOP would be expected to be maintained within 18 to 22 mmHg when the IOP is set to 20 mmHg during the phacoemulsification step. Similarly, with an IOP setpoint of 20 mmHg, IOP would be expected to be within 16 and 24 mmHg during I/A.
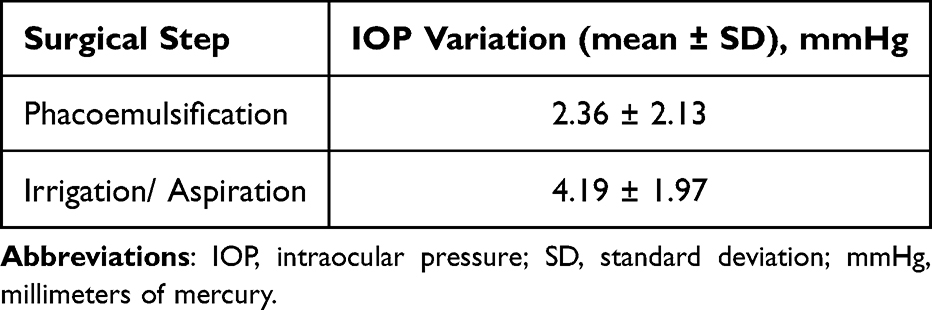 |
Table 2 Bench Testing: IOP Maintenance Accuracy for UNITY VCS at Flow vs Setpoint |
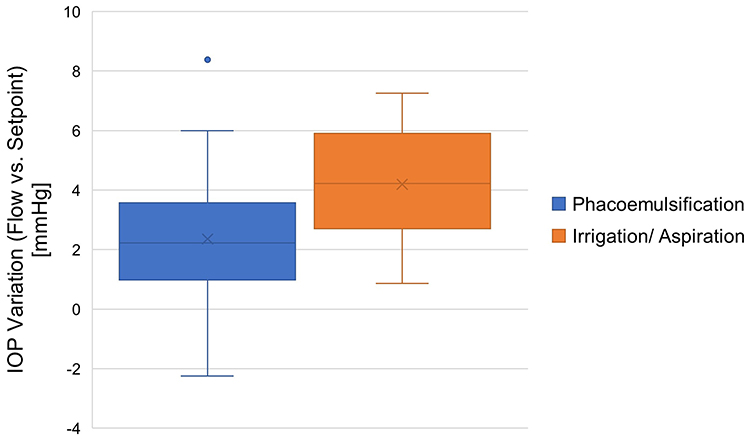 |
Figure 2 IOP Variation for UNITY VCS at Flow vs Setpoint. Abbreviations: UNITY VCS, UNITY Vitreoretinal Cataract System; IOP, intraocular pressure; mmHg, millimeters of mercury. |
Clinical Study
Sixty-eight (68) patients underwent cataract surgery using UVCS with exceptional AC stability observed in all cases. 100% (3/3) of the surgeons responded that they “Strongly Agree” that the UVCS fluidics provided better anterior chamber stability compared to CAS. Please refer to Video S1 demonstrating the anterior chamber stability using UVCS in a dense cataract. Additionally, there were no adverse device effects, posterior captures ruptures, or unplanned intraoperative surgical procedures reported.
Discussion
Advances in the fluidic capabilities of phacoemulsification systems have allowed for more consistent intraoperative IOP control during anterior segment surgery. The current study found that the UNITY VCS exhibited excellent IOP control during all surgical steps of cataract surgery. The results demonstrated that once the desired IOP was reached, IOP was maintained at the desired setpoint during flow such that the variation did not exceed a mean of 4.19 ± 1.97 mmHg regardless of the surgical step. In one of the larger studies examining diurnal IOP variations, David et al found a mean range of IOP fluctuations of 5.0 ± 2.7 mmHg in normal patients.8 UVCS was able to maintain the desired IOP as set by the surgeon during all cataract surgery steps where the average variation from the setpoint was similar to the typical IOP diurnal variation in normal patients. Maintaining IOP at the desired setpoint will likely increase surgeons’ confidence to operate more efficiently and at lower IOP.9,10 Operating at a lower, more physiological IOP has also been previously reported to be associated with more postoperative clear corneas and less anterior chamber inflammation 1 day postoperatively.1
Maintaining accurate IOP control during cataract surgery is also essential for intraoperative AC stability and surgical success, as fluctuations in IOP can cause the chamber to become unstable or collapse. Anterior chamber instability, which may be more common in patients with conditions such as pseudoexfoliation due to poor zonular stability, has been associated with poor corneal health.11
In an experimental study by Suzuki et al, UVCS demonstrated both a lower rate of IOP reduction and lower AC depth changes during occlusion break surge events compared with CAS, which suggests an association with intraoperative IOP changes and AC changes.12 Similarly, Araño-Ferrer et al’s clinical study compared AC stability during one-handed phacoemulsification with CENTURION OZil® and ACTIVE SENTRY handpieces. The study reported that use of the ACTIVE SENTRY handpiece, which includes an integrated pressure sensor at the level of the handpiece to allow for real-time detection and compensation of IOP fluctuations during surgery, was correlated with improved AC stability scores.13
Like CAS, UVCS/UCS is equipped with an aspiration sensor and pump, but now also includes the addition of an infusion sensor and pump that allows for dynamic leakage compensation. The out-of-phase peristaltic flow pulsation for both infusion and aspiration allows for smoother and faster fluidic response, thereby enhancing stability. This was observed in the present clinical study, where all surgeons reported that UVCS fluidics provided more AC stability compared to CAS at the same settings.13 In clinical practice, surgeons generally correlate lower IOP variations with better AC stability, which is often observed as less iris movement during surgery. UVCS’ IOP maintenance was also visually represented in Video S1, which illustrates less iris movement during the removal of a dense cataract lens.
This study has some limitations. The current bench study utilized a mechanical eye model with average human compliance, which allowed for repeatable testing in a controlled environment. However, this model may not accurately represent all human eyes under surgical conditions due to large variability in compliance. Eyes with higher compliance, such as larger, myopic eyes, for example, may experience more pronounced anterior chamber shallowing in response to IOP change, potentially limiting the clinical applicability of the findings. The clinical study provides valuable preliminary insights through a comparison of surgeons’ assessment of the AC stability with UVCS and CAS. The results, however, are based on surgeons’ retrospective self-reports comparing the UVCS with their current system, which may introduce recall bias affecting the findings. As both studies were also conducted as single-arm studies, additional comparative head-to-head clinical studies are needed to further corroborate these findings, directly assess intraoperative performance of UVCS compared to CAS, and evaluate its impact on postoperative clinical outcomes.
Conclusion
The UNITY VCS/CS demonstrated low IOP variation in bench testing and was perceived to have high AC stability by surgeons. Maintaining IOP at the desired surgeon setpoint with minimal variation throughout the duration of the surgery may reduce intraoperative and postoperative complications, especially in more complex cases.
Data Sharing Statement
The clinical data presented is a subset analysis from a larger, multi-center study registered on ClinicalTrials.gov (NCT06071104), focusing on questionnaire responses from surgeons from one study site. No patient-level data are reported in this manuscript. Study-related information for the larger study, including study registration, participation criteria, study plan summary, and summary result, is publicly available at: https://clinicaltrials.gov/study/NCT06071104?id=NCT06071104&rank=1
Acknowledgments
The authors thank Samantha Do, OD for her input to this manuscript and assistance with medical writing. The abstract of this paper was presented at the 2025 Annual Meeting of the American Society of Cataract and Refractive Surgery (ASCRS) as a paper presentation. The paper’s abstract is available online in the 2025 ASCRS Annual Meeting Program (https://ascrs.confex.com/ascrs/25am/meetingapp.cgi/Paper/107467). The abstract was also presented at the 2025 Congress of the European Society of Cataract and Refractive Surgeons (ESCRS) Congress as an e-poster presentation.
Funding
This study was supported by funds from Alcon Vision LLC.
Disclosure
J. Berdahl and V. Thompson are consultants to Alcon Vision LLC. J. Berdahl is also a consultant for AbbVie, Aerpio, ALJ Health, Aldeyra, Aquea Health, Aurion Biotech, Avelino, Balance Ophthalmics, Bausch And Lomb, Belkin, CorneaGen, Dakota Lions Eye Bank, Elios Vision INC, Expert Opinion, EyeX Solutions, Glaukos, Gore, Greenman, Harrow Health, Horizon Surgical, Iacta Pharmaceuticals, iRenix, IVERIC bio, Inc, JNJ, Kala, LayerBio, MELT Pharmaceuticals, MicroOptx, New World Medical, Ocular Surgical Data, Ocular Theraputix, Omega Ophthalmic, Orasis, Oyster Point, RxSight, Santen, Sight Sciences, Tarsus, TavoBio, Tear Clear, Tissue Gen, True North CRO, Vance Thompson Vision, Verana Health, Versea Biologics, Vertex Ventures, and ViaLase, outside the submitted work. D. Dyk, S. Yalamanchili, S. Makari, and A. Aboughaida are employees of Alcon Vision LLC. The authors report no other conflicts of interest for this work.
References
1. Vasavada V, Raj SM, Praveen MR, Vasavada AR, Henderson BA, Asnani PK. Real-time dynamic intraocular pressure fluctuations during microaxial phacoemulsification using different aspiration flow rates and their impact on early postoperative outcomes: a randomized clinical trial. J Cataract Refract Surg. 2014;44(7):884–7.
2. Hejsek L, Kadlecova J, Sin M, Velika V, Jiraskova N. Intraoperative intraocular pressure fluctuation during standard phacoemulsification in real human patients. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2019;163(1):75–79. doi:10.5507/bp.2018.065
3. Geng W, Lin W, Song P, et al. Effect of anterior chamber instability during phacoemulsification combined with intraocular lens implantation. J Ophthalmol. 2022;2022:2848565. doi:10.1155/2022/2848565
4. Miller KM, Dyk DW, Yalamanchili S. An experimental study of occlusion break surge volume in three different phacoemulsification systems. J Cataract Refract Surg. 2021;47(11):1466–1472. doi:10.1097/j.jcrs.0000000000000651
5. Nicoli CM, Dimalanta R, Miller KM. Experimental anterior chamber maintenance in active versus passive phacoemulsification fluidics systems. J Cataract Refract Surg. 2016;42(1):157–162. doi:10.1016/j.jcrs.2015.08.017
6. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol. 2014;14:96. doi:10.1186/1471-2415-14-96
7. Dyk DW, Miller KM. Mechanical model of human eye compliance for volumetric occlusion break surge measurements. J Cataract Refract Surg. 2018;44(2):231–236. doi:10.1016/j.jcrs.2017.10.052
8. David R, Zangwill L, Briscoe D, Dagan M, Yagev R, Yassur Y. Diurnal intraocular pressure variations: an analysis of 690 diurnal curves. Br J Ophthalmol. 1992;76(5):280–283. doi:10.1136/bjo.76.5.280
9. Brézin AP, Monnet D, Lignereux F, Rozot P, Jilet L, Abdoul H. Impact of a handpiece with a built-in fluidics pressure sensor on phacoemulsification: a multicentre prospective comparative study. BMJ Open Ophthalmol. 2023;8(1):e001431. doi:10.1136/bmjophth-2023-001431
10. Cyril D, Brahmani P, Prasad S, et al. Comparison of two phacoemulsification system handpieces: prospective randomized comparative study. J Cataract Refract Surg. 2022;48(3):328–333. doi:10.1097/j.jcrs.0000000000000769
11. Hayashi K, Manabe S, Yoshimura K, Kondo H. Corneal endothelial damage after cataract surgery in eyes with pseudoexfoliation syndrome. J Cataract and Refractive Surg. 2013;39(6):881–887. doi:10.1016/j.jcrs.2013.01.032
12. Suzuki H, Kurose M, Horie T, Makari S, Yalamanchili S. Anterior chamber stability of novel phacoemulsification machine via the slit side view method. J Cataract Refract Surg. 2025. doi:10.1097/j.jcrs.0000000000001859
13. Araño-Ferrer J, Medina-Perez AB, Solis-Hernandez C, Gulias-Cañizo R, Guerrero-Berger O. Comparison of intraoperative parameters between two handpieces in one-handed phacoemulsification with active fluidics. Diagnostics. 2024;14(19):2141. doi:10.3390/diagnostics14192141
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.