Back to Journals » Open Access Emergency Medicine » Volume 12
Basic Life Support Knowledge and Its Associated Factors Among a Non-Medical Population in Gondar Town, Ethiopia
Authors Mekonnen CK ![]() , Muhye AB
, Muhye AB
Received 29 July 2020
Accepted for publication 27 October 2020
Published 3 November 2020 Volume 2020:12 Pages 323—331
DOI https://doi.org/10.2147/OAEM.S274437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Chilot Kassa Mekonnen,1 Addis Bilale Muhye2
1Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Pediatric Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Chilot Kassa Mekonnen Tel +251 955220378
Email [email protected]
Background: Different life-threatening accidents can happen anywhere at any time in our daily livings. In this study, the knowledge about basic life support was below average among the non-medical population.
Objective: The aim of the study was to assess basic life support knowledge and its associated factors among non-medical population attending the outpatient department.
Methods: An institutional-based cross-sectional study was conducted from January 15/2020 to February 30/2020. Systematic random sampling was employed to get representative samples. Data were collected by using a structured interviewer-administered questionnaire. The data were analyzed by using a binary logistic regression model. Crude and adjusted odds ratios with the corresponding 95% confidence intervals were computed. Those variables with P-values of ≤ 0.05 were considered significantly associated with the outcome variable.
Results: A total of 412 participants took part in the study with a response rate of 97.4%. Among the participants, 183 (44.4%) [95% CI (39.8– 49.5)] were knowledgeable about basic life support. Age of 30– 40 years was 50% [AOR=1.50, 95% CI (1.15– 1.97)], the age of > 40 years was 2.45 [AOR=2.45, 95 CI (1.53– 3.91)], being male [AOR=2.22, 95% CI (1.41– 3.49)], lived in the urban [AOR=1.66, 95% CI (1.25– 3.56)], being trained [AOR=4.65, 95% CI (1.85– 11.67)], ever heard about BLS and having exposure with the person in need of BLS [AOR=3.02, 95% CI (2.05– 4.74)], and [AOR=2.59, 95% CI (1.69– 3.98)] times more to be knowledgeable as compared with their counterparts.
Conclusion: The finding of this study demonstrated that knowledge score of the participants was below average. Therefore, there has to be more to do so as to scale up the knowledge of the community for reducing preventable deaths from unexpected emergency situations.
Keywords: basic, life, first aid, support, knowledge, cardiac arrest, non-medical, population
Introduction
Background
Basic life support is the provision of initial care for an illness or injury, usually by any nearby (bystander) person, until medical treatment can be accessed.1 Early recognition and activation of Emergency medical service (EMS) and early bystander basic life support (BLS) are the most important factors determining the survival probabilities in patients. This in turn depends entirely on the knowledge and actions of the bystanders.2 Evidence showed that difficulties in performing bystander cardiopulmonary recitations (CPR) in developing countries are due to inadequate knowledge or training, absence of skill, lack of confidence, and fear of litigation.2–4 The World Health Organization estimated a homicidal rate of 8 per 100,000 populations in its 2014 Global Status Report on homicidal prevention (>7000 deaths annually).5 On top of theses and that reason provision of immediate basic life support to patients who require emergency care can make a big difference to the outcome.6 Basic life support as the first action, taken for the management of injuries and common illness reduce the future occurrence of the disease and its complication rates.7
In certain self-limiting illnesses or minor injuries, appropriate basic life support/first aid measures may be sufficient to avoid a medical consultation and the risk of life lost.8 Different unintentional and life-threatening accidents can happen anywhere at any time in our daily living. This needs immediate and appropriate life-saving care before the affected person gets further medical or surgical treatment options. This life-saving care or basic life support is an assessment and interventions that can be carried out by a person nearby immediately with minimal or without medical equipment.7,9 Patient’s chance of survival is not only a concern for health care professionals but also a concern for the general public, who have the opportunity to act when witnessing unintentional accidents or injuries.10
The ultimate goal of basic life support is to stop or to reverse the possible harm at a given time before reaching the appropriate health care Centre.11,12 BLS knowledge is a method and technique that used to perform practice related to prevention and immediate response to health emergencies. It can be given in all areas such as household, schools, workplace, and recreational areas. Beyond health matters, basic life support knowledge also increases the social responsibility of society and strengthens values.3,13 Therefore, this makes it important to have a basic knowledge of basic life support. The proportion of basic life support knowledge was reported 39.2% in Saudi Arabia, 43.7% in Iran, 74.3% in Egypt, and 44.0% in Jimma, respectively.14–16 Other similar studies, in Saudi Arabia and Addis Ababa also reported that basic life support knowledge was 50.0%, 45.8%, 40.0%, and 50.3%, respectively.4,9,14,17 Studies in India and Portugal showed that level of education, gender, and income was significantly associated with knowledge score towards basic life support.18,19 The study in Saudi Arabia revealed that higher income and level of education were significantly associated with higher knowledge score towards BLS.14 Another study in Saudi Arabia also showed that the age of the participants, higher education, and taking training courses significantly increased the knowledge about basic life support information.9
Studies conducted in India, Egypt, Republic of Slovenia, Saudi Arabia and Portugal revealed that having training about first aid was significantly associated with knowledge.2,3,9,19,20 The study conducted in Addis Ababa also revealed that those participants who had first aid training were nearly five times more to have adequate knowledge towards basic life support compared with those participants who did not have training.21 Knowledge of the Public about basic life support is especially as important as the care given in the Hospital. This is because many adverse consequences of unintentional accidents or injuries can be averted if the public knows what actions to take. Therefore, this study was aimed to assess knowledge towards basic life support and its associated factors among the non-medical population.
Methods
Study Design and Period
An institutional-based cross-sectional study was conducted among the non-medical population living in Gondar town from January 15/2020 to February 30/2020.
Study Area
The study was conducted at Gondar town Northwest Ethiopia. Gondar is found in Amhara National Region State which is 735 km far from Addis Ababa (the capital city of Ethiopia) and it is one of the ancient towns in the country. It has one Comprehensive specialized Hospital which serves around 7 million people both within and outside of the town. It has also eight health centers.
Source Population
All adult non-medical individuals attending Gondar town public health institution were the source population.
Study Population
All adult non-medical individuals attending the selected outpatient departments of Gondar town public health institutions during data collection.
Inclusion and Exclusion Criteria
All adult non-medical individuals attending outpatient department of Gondar town public health institutions and available during data collection were included in the study. Whereas, individuals who had a serious illness and had the difficulty of communication were excluded in the study.
Sample Size and Sampling Procedures
The sample size was determined by using a single population proportion formula with the assumptions of 95% level of confidence, 5% marginal error, taking 50% for basic life support proportion since no study in the study area and 5% non-response rate. Taking these assumptions, the initial sample size was 385. Considering the 10% non-response rate, the final sample size was 423. The public institutions found in the town were selected by a simple random method. Then after the average flow of patients at the outpatient department was identified at each selected health institutions and proportional allocation was done to get a representative sample. Finally, the study participants were selected using a systematic random sampling by using the lottery method in their sitting order during service waiting (See supplementary file 1: Figure S1).
Data Collection Tools and Procedures
A structured pre-tested interviewer-administered questionnaire modified from other related published studies were used to collect the data.9,10,14,16 The Cronbach’s Alpha after items deleted for the knowledge items was found 0.845. Before the actual data collection, five BSc nurse data collectors had a brief training about the aim of the study and the content of the questionnaire to collect uniform data. The questionnaire has 2 parts which include: socio-demographic and knowledge related items, respectively. Knowledge about basic life support was measured by thirty interviewer-administered questions (supplementary file 2) collected by four trained BSc degree nurses. The data collected in about 20–25 minutes were computed by coding the correct response as “1” and the incorrect responses as “0”. Then after the correct answers were added up and participants who scored the mean and above were labeled as having good knowledge, whereas with a score of below mean were classified as poor knowledge about basic life support.
Operational Definition
BLS Knowledge
Knowledge about component of basic life support/first Aid, sign and management of the respiratory problem, management of bleeding and immobilization of fracture, the position of the victim, communication and transportation of victim start from the scene.22
Knowledge
Sum of the knowledge correctly answered questions were normally distributed. So that it was measured by calculating the mean score and categorized as knowledgeable (if participants scored ≥ mean) of the correctly answered questions) or not knowledgeable [if participants scored < mean] of the correctly answered questions.21,22
Data Quality Control
The questionnaire was pre-tested among 5% non-medical population a week before the actual data collection. The questionnaire was prepared in English first and translated to Amharic for better understanding of the participants. Based on the findings of the pretest modifications on vague questions and flow of items was done. One day training was given for data collectors. The data were checked for its completeness during data collection, entry and analysis process.
Data Processing and Analysis
After data collection, a questionnaire was checked for completeness and consistency. The data template format was prepared and entered into Epi info version7. Then data were exported and analyzed using SPSS version 20. Descriptive statics was employed to describe the frequency, percentages, and distributions of the sample. The knowledge score was tested for normality using Shapiro–Wilk test and its distribution was compared between the pre-sated categories of socio-demographic variables. The model fitness was checked by Hosmer-Lemeshow goodness of fit with the p-values of >0.05. Binary logistic regression analysis was used to see the association between dependent and independent variables. Crude and adjusted odds ratios with the corresponding 95% confidence intervals were computed. In multivariable logistic regression, those independent variables with a P-values ≤ 0.05 were considered statistically significant in multivariable analysis.
Result
Socio-Demographic Characteristics
Among a total of 423 study participants, 412 were responding to the interview with the response rate of 97.4%. The mean age of the participants was (35.09±8.737 SD) with a range of 18–56 years. Majorities (67.0%, 68.0% and 71.8%) were male, married, and urban residents, respectively. The large proportion of 355 (91.5%) of the study participants did not take any training regarding basic life support. Among participants about (62.9%) had one occasion to be trained about basic life support (Table 1).
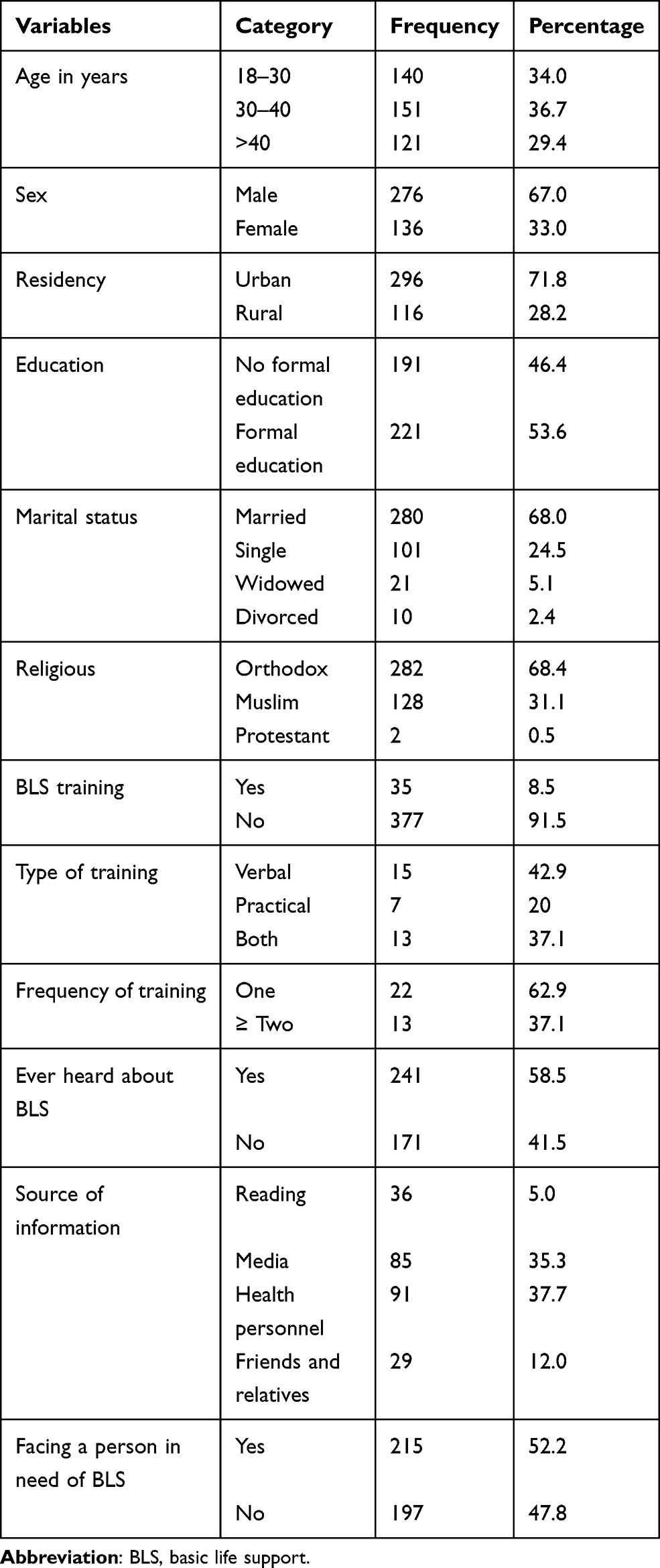 |
Table 1 Socio-Demographic Characteristics of Participants at Gondar Town Public Health Institutions Northwest, Ethiopia, 2020 |
Knowledge Towards Basic Life Support
Among 412 participants took part in the study183 (44.4%) [95% CI (39.8–49.5)] were knowledgeable towards basic life support.
Distribution of Basic Life Support Knowledge by Socio-Demographic Characteristics
Participants who had trained possessed higher basic life support mean knowledge score than had not trained (21.20±2.21 vs 18.84±4.22). Moreover, participants who dweller in Urban had a higher mean score of basic life support knowledge than rural (19.48± 4.14 vs 17.92 ± 4.02) (Table 2).
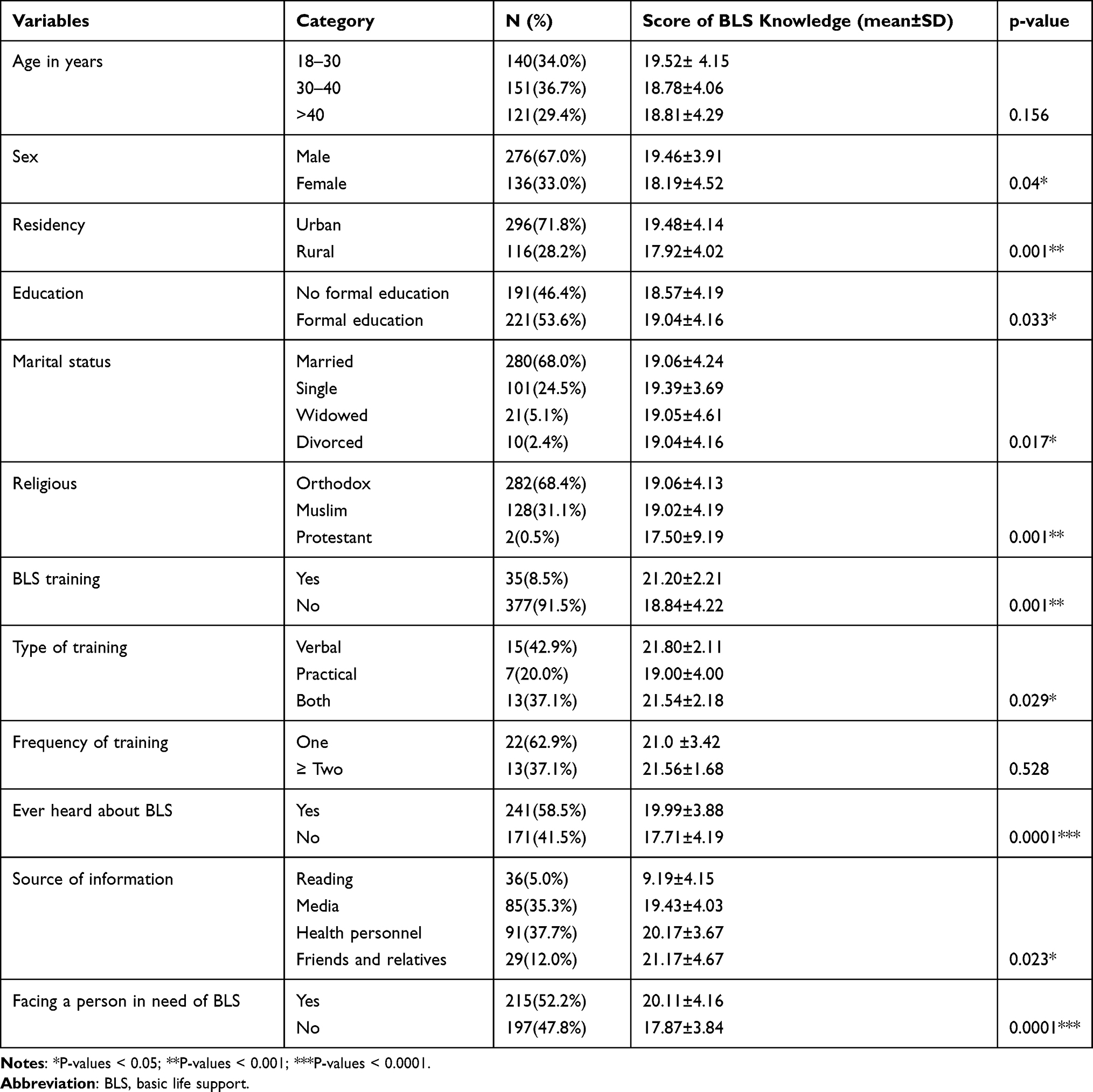 |
Table 2 Socio-Demographic Distribution of Participants’ Score of BLS Knowledge at Gondar Town Public Health Institutions Northwest, Ethiopia, 2020 |
Factors Associated with Knowledge of Participants About Basic Life Support
Among variables entered into multiple logistic regression analysis age, sex, residence, trained about basic life support, ever heard about basic life support, and exposure with the person in need of basic life support was significantly associated with the knowledge score. In this regard, being in the age of 30–40 years was 50% [AOR=1.50, 95% CI (1.15–1.97)] more to have good knowledge about basic life support. Whereas, being in the age of >40 years was 2.45[AOR=2.45, 95 CI (1.53–3.91)] times more knowledgeable as compared with its counterpart. Being male was found to be nearly two [AOR=2.22, 95% CI (1.41–3.49)] times knowledgeable as compared with being female. Those who lived in the urban were found 66% [AOR=1.66, 95% CI (1.25–3.56)] more knowledgeable compared with rural dwellers. Being trained was nearly five [AOR=4.65, 95% CI (1.85–11.67)] times more knowledgeable compared with its counterpart. Ever heard about BLS and having exposure with the person in need of BLS were found to be three [AOR=3.02, 95% CI (2.05–4.74)], and [AOR=2.59, 95% CI (1.69–3.98)] times more knowledgeable as compared with their counterparts (Table 3).
 |
Table 3 Bivariable and Multivariable Analysis of Factors Associated with Knowledge of Basic Life Support at Gondar Town Public Health Institutions, Northwest, Ethiopia, 2020 (n=412) |
Discussion
In this study, the level of good knowledge about basic life support was found to be 44.4% among non-medical participants. The result was in line with the study conducted in Addis Ababa,17 Saudi Arabia9 and Iran23 which was 40.0%, 40.3%, and 45.8%, respectively.
The current study result was lower than the studies conducted in Addis Ababa 50.3%, Saudi Arabia 50%, Egypt 74.3%, respectively.4,15,21 The possible explanations might be due to the fact that tool variation in using the cut points, socio-demographic variations, and the inclusion criteria variations. Majority of the study participants in the studies above were at least they had formal education and at most degree holders whereas in the current study majority did not have even formal education. Therefore, for this and that reason, the knowledge score might be decreased or increased. The finding of this study was higher than the study conducted in Saudi Arabia showed that 39.2% of the study participants were knowledgeable towards basic life support or first aid during an emergency.14 The possible variation might be due to the fact that there socio-demographic, variation, sample size, and cut point variations which brought the significant score difference. Being urban residency demonstrated a higher knowledge mean score as compared with rural (19.48 vs 17.92). The possible explanation might be due to the fact that 85% of the rural community is not educated as compared with 15% urban dweller. The urban community might have access for information about basic life support than the rural.
The higher knowledge mean score was demonstrated among ever trained than not yet (21.20 vs 18.84) (Table 2).
Among variables entered into multiple logistic regression analysis age, sex, residence, trained about basic life support, ever heard about basic life support, and exposure with the person in need of basic life support was significantly associated with the knowledge score.
In this regard, being in the age of 30–40 years was 50% more to have good knowledge about basic life support. Whereas, being in the age of >40 years was 2.45 times more knowledgeable as compared with its counterpart. The possible explanation might be due to the fact that as age increase the awareness and exposure also increase, this fact was supported by the study conducted in Saudi Arabia which revealed that those with older age were knowledgeable as compared with younger age.9
Being male was found to be nearly two times to be knowledgeable as compared with being female. The possible explanation might be due to the fact that being male could have many more exposures and contacts with people having knowledge about basic life support which is more practical in the community than females. The work environment of males and females has its own impact on shared information. This has been supported by the study conducted in Portugal.19
Those who lived in the urban were found to be 66% more knowledgeable compared with rural dwellers. The possible explanation might be due to the fact that things are different in the accessibility in the urban and the rural such as media, reading materials, and due to health professional education regarding basic life support.
Not only these but also the majority of the rural communities did not have an educational background which hinders them from getting information by reading. These findings were supported by the studies conducted in Saudi Arabia.14 In this study, only 35 (18.5%) of the participants had a chance to take training about basic life support, of this only 20.0% had had a practical type of training. In the multivariable analysis, being trained about basic life support was found to be nearly five times more to be knowledgeable compared with did not take the training.
The possible explanation might be due to the fact that trained participants had increased awareness about basic life support components which might bring good knowledge score compared to did not take the training. This has been supported by the studies conducted in Addis Ababa, Egypt, Slovenia, Saudi Arabia, and South Austral2,3,9,18,21 In this study, the main source of information about basic life support was found to be from health professionals followed by media 37.7% and 35.5%, respectively. In the multiple logistic regressions analysis, ever heard about basic life support was found to be significantly associated with knowledge score of the participants. In this regard, those with prior information about BLS were found to be three times more knowledgeable as compared with did not have any information.
The possible explanation might be due to the fact that those heard could have a chance to look through to know about it as compared to did not hear about BLS. Even who hear might have a chance to read if they can, and to ask others than those who did not know about basic life support. Having exposure to the person in need of BLS was also found to be nearly three times more knowledgeable as compared with their counterparts. The possible explanation might be due to the fact that they have the chance to know what about basic life support with practice compared to no exposure at all. As the study result depicted that the knowledge score of non-medical participants was not satisfactory since it was below average. Therefore, the respected health institutions need have to do a lot so as to scale up knowledge of the community regarding basic life support. Giving health education when they come for service might have a great impact on the scale up the knowledge of the patients and the community at large. This in turn might save lots of sudden life loss due to lack of knowledge about basic life support.
Strength and Limitation of the Study
The study was newly conducted in the study area with adequate sample size. It tried to assess the knowledge of non-medical population which could be important to set strategies to reduce the sudden cause of death. The limitation of the study did not address the attitude and practice of the participants.
Conclusion
The study revealed that the proportion of good knowledge about basic life support was found to below half which implies that there has to be more to do in the future. This is because scaling up of the communities awareness has a great impact on the individual as well as government level by decreasing sudden cause of death. This in turn prevents an individual’s, families’, and the government from budget drainage through saving life of the citizens. In this study being old, male, being urban dwellers, having training, ever heard about BLS, and having exposure of a person in need of basic life support were statically significant predictors of good knowledge score of non-medical participants’ about basic life support.
Recommendations
- To central Gondar health bureau better to set strategies so as to create awareness by going deep through the community. This has to be a very crucial strategy to reduce the sudden cause of death and in the way forward increasing productivity and development of the Zone, in particular, the region and the country at large.
- To health professionals to strengthen their information provision for the community while they give care.
- To the study participants better to look through different sources of information such as reading, watching or following media, ask other who are near to information, and ask the health professionals what is unclear for them.
- To researchers better to do large-scale studies by incorporating the attitude and practice of the community.
Abbreviations
AED, automated external defibrillator; AOR, adjusted odds ratio; BLS, basic life support; COR, adjusted odds ratio; CPR, cardiopulmonary resuscitation; EMS, emergency medical service; FA, first aid; OHCA, out of hospital arrest; SPSS, statical package for social science; SCD, sudden cause of death; WHO, World Health Organization.
Data Sharing Statement
The data could not be given in order to protect participants’ confidentiality by far for this study. The whole summary of the data is available in the manuscript document. It could also be given if it is necessary, but upon reasonable request.
The Ethical Approval and Consent of Participating
Ethical clearance and the approval of the study was done by the University of Gondar, college of medicine and health sciences, school of nursing research and ethical review committee so as to precede it. The letter of permission and support was gained from the clinical director of the Hospital. All the participants of the study were well informed about the overall rationales of the study. They had got written informed consents to secure their confidentiality. The study has been performed following the ethical standards laid down in the 1964 Declaration of Helsinki.
Consent to Publish
This is not applicable.
Acknowledgment
The authors would like to forward our deepest appreciation to the University of Gondar College of Medicine and health Sciences, school of nursing research and ethical review committee for approval of the ethical clearance. The authors also would give our great thank for data collectors and the supervisors for their devotion and the participants for their unlimited and valuable information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by the University of Gondar College of Medicine and Health sciences. But, the funder has no significant role to play in the study design, data collection, analysis, manuscript preparation, and finally on the decision on publication.
Disclosure
Both authors declared that they have no competing interest concerning this work.
References
1. Kleinman ME, Goldberger ZD, Rea T, et al. 2017 American Heart Association focused update on adult basic life support and cardiopulmonary resuscitation quality: an update to the American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2018;137(1):e7–e13. doi:10.1161/CIR.0000000000000539
2. Arbon P, Hayes J, Woodman R. First aid and harm minimization for victims of road trauma: a population study. Prehosp Disaster Med. 2011;26(4):276–282. doi:10.1017/S1049023X11006522
3. Rajapakse R, Noč M, Kersnik J. Public knowledge of cardiopulmonary resuscitation in Republic of Slovenia. Wien Klin Wochenschr. 2010;122(23–24):667–672. doi:10.1007/s00508-010-1489-8
4. Althubaiti AQA, Altowairqi RM, Alsulimani FA, Alnefaie BM. Awareness, knowledge, attitude and practices of first aid skills among medical and non-medical students at Taif University. Middle East J Fam Med. 2019;17(11).
5. FMOH. HSTP-Health Sector Transformation Plan. Addis Ababa: FMOH; 2015.
6. Tsegaye F, Abdella K, Ahmed E, Tadesse T, Bartolomeos K. Pattern of fatal injuries in Addis Ababa, Ethiopia: a one-year audit. East Central Afr J Surg. 2010;15(2):10–17.
7. Jarrah S, Judeh M, AbuRuz ME. Evaluation of public awareness, knowledge and attitudes towards basic life support: a cross-sectional study. BMC Emerg Med. 2018;18(1):37. doi:10.1186/s12873-018-0190-5
8. Woyessa AH, Dibaba BY, Hirko GF, Palanichamy T. Spectrum, pattern, and clinical outcomes of adult emergency department admissions in selected hospitals of western ethiopia: a hospital-based prospective study. Emerg Med Int. 2019;2019.
9. Midani O, Tillawi T, Saqer A, Hammami MB, Taifour H, Mohammad H. Knowledge and attitude toward first aid: a cross-sectional study in the United Arab Emirates. Avicenna J Med. 2019;9(1):1. doi:10.4103/ajm.AJM_140_18
10. Adib-Hajbaghery M, Kamrava Z. Iranian teachers’ knowledge about first aid in the school environment. Chin j Traumatol. 2019;22(4):240–245. doi:10.1016/j.cjtee.2019.02.003
11. Monsieurs KG, et al. European resuscitation council guidelines for resuscitation 2015 section 1. Executive summary. Resuscitation.-Limerick, 1972. Currents. 2015;95:1–80.
12. Association AH. Highlights of the 2015 American Heart Association Guidelines Update for CPR and ECC. 2015. 2018.
13. Athipathy V, Kumar PA, Tolstoy R, Jeyakrishnan P, Mohanasundaram P, Reddy A Basic life support through early clinical exposure: students’ perspective. Aust Med J. 2016;9(9):319.
14. Subki AH, Mortada HH, Alsallum MS, et al. Basic life support knowledge among a nonmedical population in Jeddah, Saudi Arabia: cross-sectional study. Interact J Med Res. 2018;7(2):e10428. doi:10.2196/10428
15. Eldosoky R. Home-Related Injuries Among Children: Knowledge, Attitudes and Practice About First Aid Among Rural Mothers. 2012.
16. Anmut W, Mesele M, Tekalign T. Knowledge, attitude and practice towards first aid among kindergarten teachers of Jimma Town, South West, Ethiopia, 2017. 2019. J Emerg Med Prim Care. 10008. RD-EMP.
17. Ganfure G, Ameya G, Tamirat A, Lencha B, Bikila D. First aid knowledge, attitude, practice, and associated factors among kindergarten teachers of Lideta sub-city Addis Ababa, Ethiopia. PLoS One. 2018;13(3).
18. Megahed MA, et al. Knowledge, attitude and practice of rural mothers towards home injuries among children under 5 years of age in Menouf District-Menoufia Governorate, Egypt. Menoufia Med J. 2016;29(4):1033.
19. Dixe MDACR, Gomes JCR. Knowledge of the Portuguese population on Basic Life Support and availability to attend training. Revista Da Escola De Enfermagem Da USP. 2015;49(4):0640–0649. doi:10.1590/S0080-623420150000400015
20. ElwardanyAly S, Khalaf S. Impact of training program regarding first aid knowledge and practices among preparatory schools’ teachers at Assiut City. J Nurs Educ Pract. 2017;7:12–89.
21. Teshale AA, Alemu ZA. Knowledge, Attitude and Practice of first aid and factors associated with practice among taxi drivers in Addis Ababa, Ethiopia. Ethiop J Health Develop. 2017;31(3):200–207.
22. Tafere T. Assessment of Knowledge, Attitude and Practice of First Aid Associated with Fighting Accidents Among Community Police Officers in Addis Abeba City, Ethiopia. Addis Ababa University; 2017.
23. Adib-Hajbaghery M, Kamrava Z. Iranian teachers’ knowledge about first aid in the school environment. Chin j Traumatol. 2019;22(4):240–245. doi:10.1016/j.cjtee.2019.02.003
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.