Back to Journals » International Journal of Women's Health » Volume 18
Basal Luteinizing Hormone Combined with Age and BMI as a Simplified Screening Model for Central Precocious Puberty in Girls
Authors Li J, Cui Y, Shuai J, Li W ![]() , Li Y, Yan Z
, Li Y, Yan Z ![]() , Yu T
, Yu T
Received 24 November 2025
Accepted for publication 2 February 2026
Published 16 February 2026 Volume 2026:18 583959
DOI https://doi.org/10.2147/IJWH.S583959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jiayu Li,1,2,* Yali Cui,3– 5,* Jiaji Shuai,6 Wei Li,1 Yingying Li,3 Ziyi Yan,3,7 Tao Yu1,6
1Department of Child Healthcare, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Department of Child Healthcare, Angel Women’s and Children’s Hospital, Chengdu, People’s Republic of China; 3Department of Laboratory Medicine, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China; 4Department of Laboratory Medicine, Sichuan Provincial Children’s Hospital (Sichuan Provincial Children’s Medical Center), Meishan, People’s Republic of China; 5Department of Laboratory Medicine, Meishan Women and Children’s Hospital, Meishan, People’s Republic of China; 6Department of Child Healthcare, Meishan Women and Children’s Hospital, Meishan, People’s Republic of China; 7Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ziyi Yan, Department of Laboratory Medicine, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, China, No. 20, Section 3, South Renmin Road, Chengdu, Sichuan, People’s Republic of China, Email [email protected] Tao Yu, Department of Child Healthcare, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, China, No. 1416, Section 1, Chenglong Road, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Purpose: The gonadotropin-releasing hormone (GnRH) stimulation test is regarded as the diagnostic gold standard for central precocious puberty (CPP); however, its invasiveness and limited accessibility restrict its routine use in clinical practice. Moreover, reported cutoff values for basal luteinizing hormone (LH) vary across studies, and simple screening models applicable to everyday clinical settings remain limited. This study aimed to evaluate routinely available clinical, biochemical, and imaging indicators and to develop a simplified screening model for early differentiation of CPP from premature thelarche (PT) in girls.
Patients and methods: This retrospective study included 429 girls aged 4– 8 years presenting with early breast development between January 2019 and January 2023. Basal sex hormone levels, anthropometric parameters, bone age, and pelvic ultrasound findings were collected. Univariable analysis, multivariable logistic regression, and receiver operating characteristic (ROC) curve analysis were performed to assess the screening performance of individual indicators and a combined model.
Results: Girls with CPP exhibited significantly higher age, BMI, bone age advancement, basal LH levels, and ovarian volumes than those with PT did (all p< 0.05). Multivariable analysis identified age, BMI, and basal LH concentration as independent factors associated with CPP. Among individual indicators, basal LH concentration showed the strongest discriminatory ability (AUC=0.842), with a cutoff value of 0.15 IU/L. A simplified combined model integrating basal LH concentration, age, and BMI further improved screening performance (AUC=0.880). Pelvic ultrasound parameters did not emerge as independent predictors in multivariable analyses.
Conclusion: A simplified screening model incorporating basal LH concentration, age, and BMI may serve as a practical initial screening tool to identify girls at higher risk of CPP and to reduce unnecessary GnRH stimulation testing. Prospective multicenter studies are required to validate the generalizability of this approach before broader clinical implementation.
Keywords: breast development, basal LH, body mass index, precocious puberty, ovarian volume
Introduction
Precocious puberty (PP) is a childhood endocrine disorder that is characterized by the premature appearance of secondary sexual characteristics. In accordance with the Expert Consensus on the Diagnosis and Treatment of Central Precocious Puberty (2022) issued by the Pediatric Endocrinology and Metabolism Group of the Chinese Medical Association, the following criteria are used to diagnose PP: breast development before 7.5 years or menarche before 10 years in girls and testicular enlargement before 9 years in boys.1 Epidemiological data indicate a continuous increase in the incidence of PP in recent years, with an overall prevalence of approximately 1 in 10,000–1 in 5,000 children. Additionally, the incidence in girls is 5–10 times greater than that in boys.2 Central precocious puberty (CPP) is the primary subtype of PP reported in girls and is caused by premature activation of the hypothalamic-pituitary-gonadal axis (HPGA). Among CPP cases, idiopathic central precocious puberty (ICPP) accounts for approximately 80–90% of cases.3 Other types include peripheral precocious puberty (PPP) and incomplete precocious puberty (IPP).4 The premature activation of the HPGA in CPP accelerates bone maturation and epiphyseal closure, thus leading to a compromised final adult height. It also results in early gonadal maturation and menarche and may cause a range of psychosocial issues.5,6
Currently, the exact pathophysiologic mechanism responsible for PP remains unknown.7 Epidemiological data indicate a direct correlation between early pubertal development and obesity.8,9 Studies in different regions reported that increased BMI is a predictor of early onset of puberty in girls.10–13 A higher BMI promotes earlier puberty timing through both central and peripheral biological mechanisms.
At the central level, obesity-induced hypothalamic inflammation may cause premature activation of gonadotropin-releasing hormone (GnRH) neurons, resulting in the development of precocious or early puberty.14 Concurrently, chronically elevated leptin secreted by adipocytes acts on the hypothalamus, disinhibiting the secretion of GnRH and thereby promoting the premature initiation of puberty.15 Peripherally, excess adipose tissue functions as an active endocrine organ; its abundant aromatase converts androgens into estrogens, directly elevating systemic sex hormone levels.16 The insulin resistance and hyperinsulinemia commonly associated with obesity increase the bioactivity of IGF-1, which synergistically stimulates gonadal development and contributes to precocious puberty.17
The clinical management of CPP involves long-acting gonadotropin-releasing hormone agonist (GnRHa) therapy.18 Management strategies markedly differ between CPP and non-CPP; specifically, PPP typically necessitates etiology-specific interventions, such as surgical removal of ovarian tumors or corticosteroid therapy for congenital adrenal hyperplasia, whereas partial precocious puberty (e.g., premature thelarche) is primarily managed with regular follow-up observation.19 Notably, partial precocious puberty carries a risk of progression to CPP, warranting ongoing monitoring. Therefore, the early and accurate diagnosis of CPP is essential for improving final adult height, normalizing menarche, and preventing psychological and social problems.
The diagnosis of CPP requires a comprehensive evaluation of multiple parameters, including secondary sexual characteristics, growth velocity, and the GnRH stimulation test, which remains the gold standard.1 However, this test is time-consuming, technically demanding, and costly, thus limiting its use in primary healthcare settings.20
Consequently, the identification of early, accurate, and cost-effective diagnostic tools for use in real-world practice remains a key clinical goal. Recently, accumulating evidence has highlighted the critical role of basal hormones (including LH, FSH and E2) and the LH/FSH ratio in achieving a timely diagnosis of CPP. Pelvic ultrasound, while lacking definitive diagnostic cut-offs and being operator-dependent, serves as an adjunct diagnostic tool for CPP. Its non-invasive, safe, and repeatable features enable direct evaluation of uterine/ovarian development to gauge HPGA activity. Integrating hormone detection with ultrasound enhances diagnostic accuracy and facilitates personalized interventions, highlighting its important clinical and research prospects. Therefore, this study aims to develop a simplified screening model based on routinely available clinical and laboratory variables to enable early differentiation between CPP and PT.
Materials and Methods
Materials
Study Subjects
This retrospective study included 429 girls aged 4–8 years who presented with early breast development at the Department of Pediatrics, West China Second University Hospital, Sichuan University (China National Regional Medical Center), between January 2019 and January 2023.
Inclusion Criteria
(1) Clinical confirmation of breast development ≥Tanner stage B2 by a pediatric endocrinologist; no history of exogenous hormone exposure; documentation of breast stage (B2/B3/B4).
(2) Completed pelvic ultrasonography and bone age X-ray assessment; measurements of uterine endometrial thickness, ovarian dimensions, ovarian volume, and maximum follicular diameter; and exclusion of uterine or adnexal tumors.
(3) Measurements of basal LH, FSH, E2, thyroid hormones (including TSH, FT3, and FT4), and tumor markers (including AFP and hCG) to exclude thyroid and gonadal neoplasms.
(4) Performance of the GnRH stimulation test via intravenous administration of gonadorelin (2.5 μg/kg, maximum of 100 μg), with blood samples collected at 0, 30, 60, 90, and 120 minutes for LH and FSH assays.
(5) Cranial MRI among CPP patients to exclude hypothalamic-pituitary organic lesions (such as pituitary adenomas and sellar masses).
The diagnosis of CPP was based on the Expert Consensus (2022) and involved the following criteria: onset of secondary sexual characteristics before 7.5 years of age, accelerated growth rate, bone age advancement ≥ 1 year, pelvic ultrasound showing an increased ovarian volume with multiple follicles ≥4 mm, and a positive GnRH stimulation test (LH peak >5.0 IU/L and LH/FSH ratio ≥0.6). A negative stimulation test with the exclusion of peripheral causes was defined as PT (Figure 1).
 |
Figure 1 Patient inclusion and exclusion process. |
Sample Collection
Venous blood was collected between 08:00 and 10:00 under sterile conditions for measurements of basal LH, FSH, E2, PRL, TSH, FT3, FT4, AFP, and hCG levels. Some indices were analyzed by using automated biochemical analyzers.
Instruments
Hormones and thyroid indices were analyzed by using a chemiluminescence immunoassay analyzer (Roche Cobas e601); biochemical parameters were analyzed with a Hitachi 7600 analyzer; pelvic ultrasound was performed with a GE LOGIQ E9; cranial MRI was performed with a Philips Achieva 1.5T; and bone age was assessed via digital X-ray by using the China-05 (RUS-CHN) method.
Reagents
All of the assays used the manufacturer’s supplied reagents. Chemiluminescent immunoassay kits were obtained from Roche. The GnRH stimulation test utilized gonadorelin injections (Ipsen, 0.1 mg/vial) at 2.5 μg/kg (maximum: 100 μg). Bone age was interpreted via the RUS-CHN (China-05) method by experienced radiologists.
Standardization Procedures and Strategies
All reports were generated by experienced, systematically trained physicians using structured templates. Bone age reports underwent a dual-reading process by two experienced physicians.
Methods
Principle of the Experiment
The GnRH stimulation test evaluates HPGA activation via exogenous GnRH administration. Prepubertal children exhibit a minimal LH/FSH response, whereas CPP patients demonstrate marked LH elevation and concomitant increases in FSH and E2 levels after stimulation. A peak LH level >5.0 IU/L and LH/FSH ratio ≥0.6 confirms CPP.
Procedures
The collected data included demographics (such as age, height, and weight), Tanner breast stage, bone age, ovarian dimensions (including length, width, and depth), endometrial thickness, maximum follicular diameter and count, and cranial MRI findings.
BMI was calculated as weight (kg)/height2 (m2); ovarian volume was defined as length × width × depth × 0.5233; and the bone age index (BAI) was defined as bone age/chronological age. Blood samples for LH and FSH were collected at 0, 30, 60, 90, and 120 minutes after the GnRH injections.
The diagnostic criteria for CPP included (1) onset of secondary sexual characteristics before 7.5 years, (2) accelerated growth rate, (3) bone age advancement ≥1 year, (4) ovarian enlargement with ≥4 mm follicles, and (5) a positive GnRH test. Patients not meeting these criteria were classified as PT.
Data Collection
Data including demographic details, Tanner staging, bone age, ovarian and uterine parameters, follicle data, hormone levels, GnRH test results, and MRI findings were retrieved from HIS, PACS, LIS, and electronic medical records. The data were entered into a unified template and analyzed in SPSS 26.0. The derived indices included the BMI, ovarian volume, and bone age index.
Statistical Analysis
A total of 429 subjects were included in this retrospective study. This sample size was considered sufficient to support multivariable logistic regression and ROC analyses, thereby ensuring adequate statistical power and model stability.
Statistical analyses were conducted by using SPSS 26.0. Continuous variables were tested for normality by using the Kolmogorov–Smirnov test. Nonnormally distributed data are expressed as medians (interquartile ranges) [M (QR)] and were compared between groups by using the Wilcoxon rank-sum test. ROC curves were generated to calculate AUC, sensitivity, specificity, and Youden index values for determining cutoff values. Two-tailed p values<0.05 were considered to indicate statistical significance.
Results
Univariable Comparisons of Clinical Characteristics Between the CPP and PT Groups
A total of 429 girls with precocious puberty were included in this study. The initial Tanner breast stages were B2, B3, and B4. According to the GnRH stimulation test, 157 girls (36.6%) were classified as having CPP, and 272 girls (63.4%) were classified as having PT. Univariable comparisons revealed that most of the parameters were significantly greater in the CPP group than in the PT group (Tables 1 and 2).
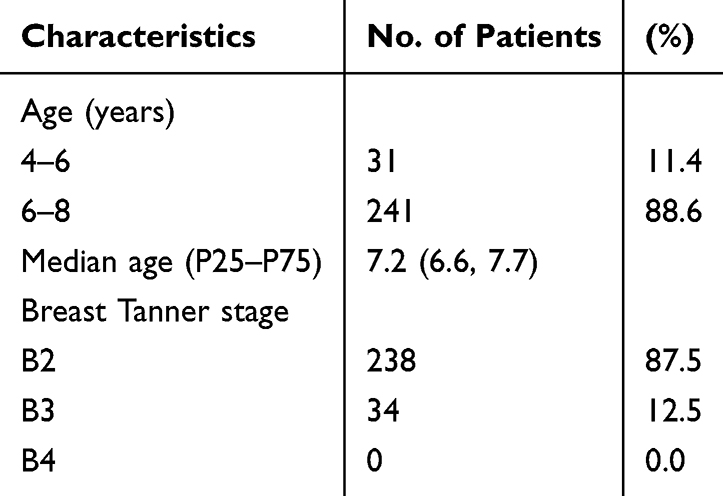 |
Table 1 Demographic and Clinical Characteristics of 272 Girls with PT |
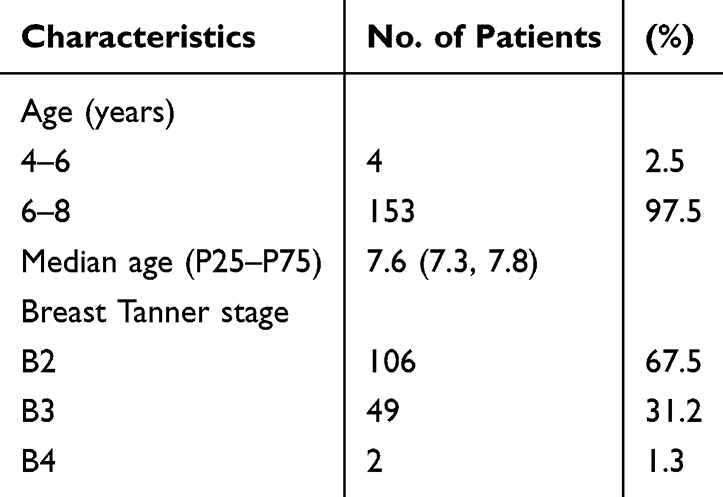 |
Table 2 Demographic and Clinical Characteristics of the 157 Girls with CPP |
In terms of developmental characteristics, age was greater in the CPP group (median: 7.7 vs 7.3 years; Z=−5.803, p<0.001), thus supporting age as a fundamental discriminator of the PP subtype. Height, weight, and BMI were also significantly greater in the CPP group (all p<0.001), which is consistent with more active linear growth due to earlier HPGA activation; additionally, the increase in BMI suggests the potential involvement of nutritional status/adiposity in CPP risk. Higher proportions of B3/B4 stages in the CPP group (B3+B4: 32.5% vs 12.5% in PT; p<0.001) indicate more advanced breast maturation, which aligns with older age and higher hormone levels. The basal LH, FSH, and E2 levels, as well as the LH/FSH ratio, were higher in the CPP group (all p<0.001) (Table 3).
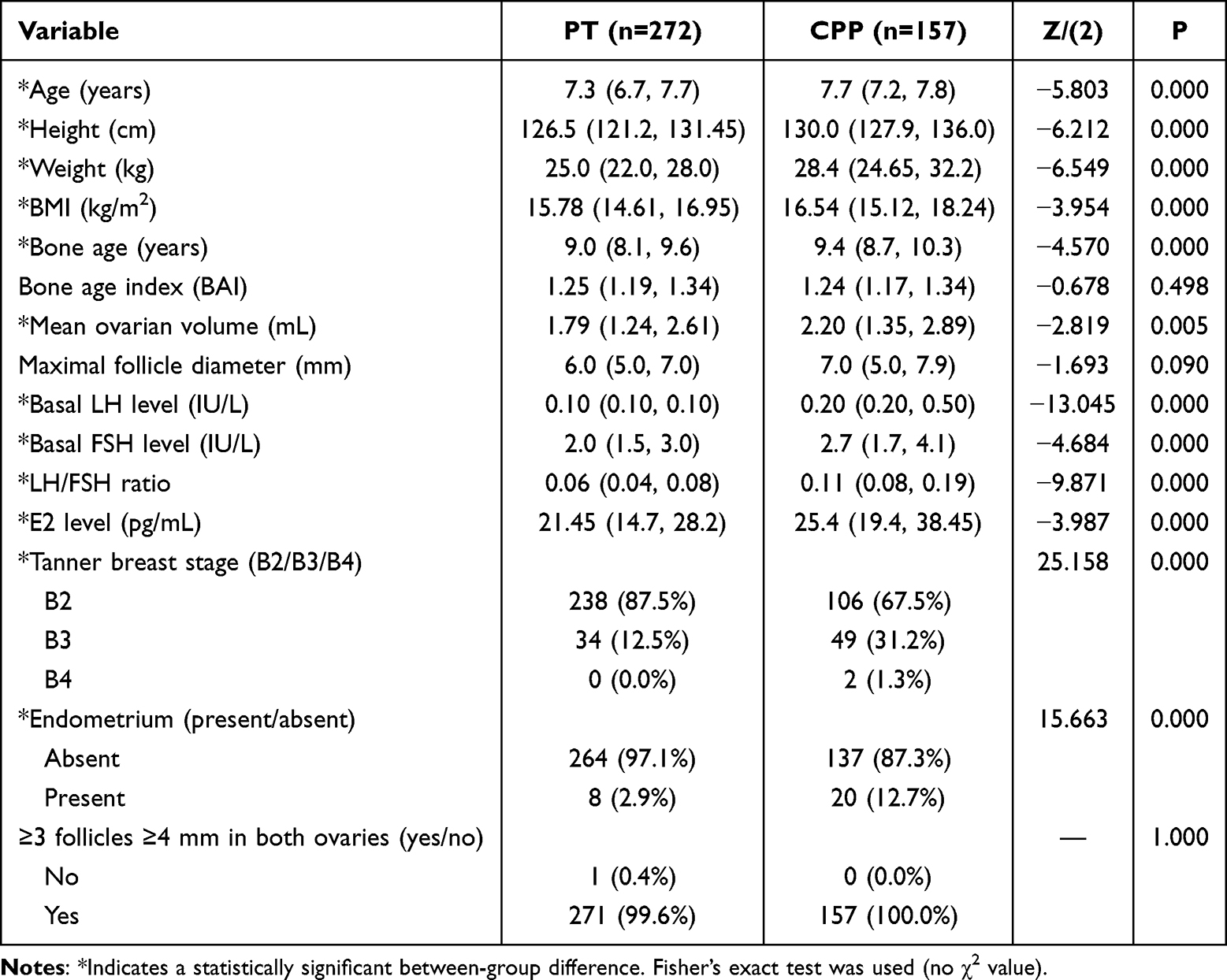 |
Table 3 Comparison of Clinical Characteristics Between the PT and CPP Groups |
On pelvic ultrasound, endometrial echo positivity was more frequent in patients with CPP (12.7% vs 2.9%; p<0.001), thus reflecting estrogen-driven endometrial responsiveness. The mean ovarian volume was greater in the CPP group (2.20 vs 1.79 mL; p=0.005). Bone age significantly differed (median: 9.4 vs 9.0 years; p<0.001), thus indicating accelerated skeletal maturation in CPP; however, the bone age index did not differ (p=0.498), thereby implying similar degrees of advancement relative to chronological age across the groups.
Binary Logistic Regression for Predictors of CPP
To evaluate independent predictors of CPP, seven variables with statistical or clinical relevance (age, Tanner stage, BMI, endometrial echo, mean ovarian volume, basal LH level, and E2 level) were entered into a binary logistic model. Age, BMI, and the basal LH level emerged as independent predictors (all p<0.05), whereas Tanner stage, endometrial echo, mean ovarian volume, and the E2 level did not demonstrate independent predictive value (Table 4).
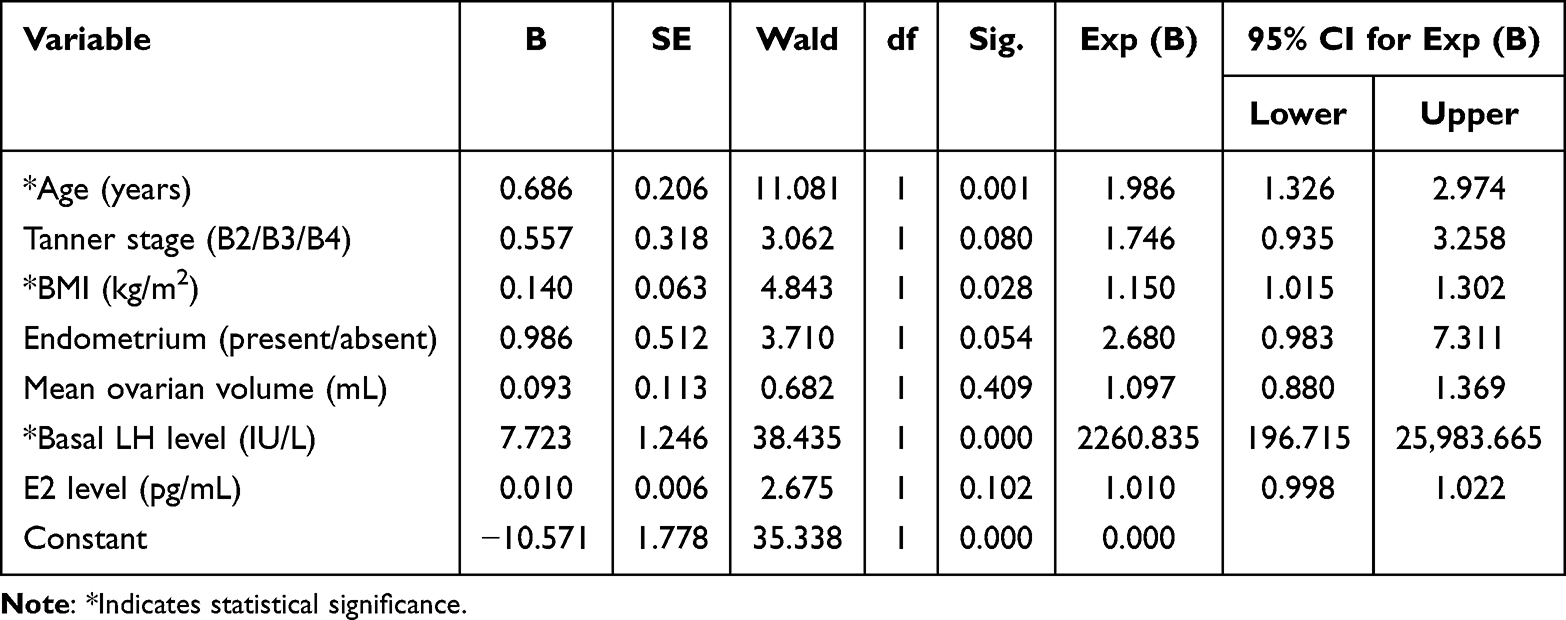 |
Table 4 Multivariable Analysis of Clinical Indicators Associated with CPP |
Each additional year of age nearly doubled the odds of CPP (OR=1.986, 95% CI: 1.326–2.974; p=0.001), thus reflecting an increased probability of HPGA activation with age. Each 1-kg/m2 increase in BMI increased the odds of having CPP by 15.0% (OR=1.150, 95% CI: 1.015–1.302; p=0.028), thereby suggesting a link between adiposity and earlier HPGA activation. The basal LH level was the strongest predictor (OR=2260.835, 95% CI: 196.715–25,983.665; p<0.001), thus indicating excellent discriminatory capacity as a single marker. Tanner stage (p=0.080), endometrial echo (p=0.054), and E2 level (p=0.102) tended to exhibit significance but were not independent predictors; moreover, mean ovarian volume was not predictive (p=0.409). In summary, chronological age, BMI, and basal LH level are independent risk factors for CPP, with the basal LH level contributing the greatest predictive value; therefore, these three variables are suitable for representing an early warning model.
ROC Analysis of Diagnostic Performance
ROC analyses were performed for age, BMI, and the basal LH level, and a combined model of the three variables was constructed. All of the variables demonstrated AUC values >0.6, thus indicating diagnostic utility. The basal LH level exhibited the largest single-parameter AUC (0.842), whereas the combined model demonstrated the highest AUC (0.880), thus indicating superior performance when the variables were integrated (Table 5).
 |
Table 5 ROC Curves of Different Variables and the Prediction Model |
Age alone (AUC: 0.668; p<0.001) and BMI alone (AUC: 0.615; p<0.001; optimal cutoff: 17.595 kg/m2) provided modest discrimination. The basal LH level demonstrated strong discrimination (AUC: 0.842; p<0.001; optimal cutoff: 0.15 IU/L). The combined model (age + BMI + basal LH level) demonstrated the best performance (AUC: 0.880; sensitivity: 82.2%; specificity: 80.9%; Youden index: 0.631), thereby offering a clinically practical balance between sensitivity and specificity for early CPP screening (Figure 2).
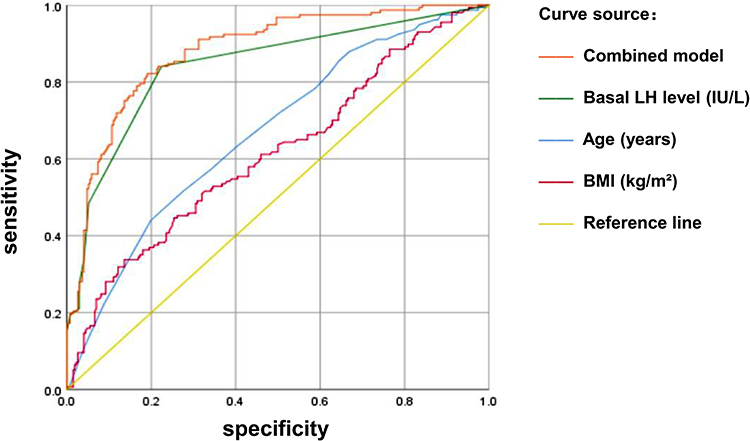 |
Figure 2 ROC curves of the prediction model. |
Sensitivity Analysis of Diagnostic Model
To assess the robustness of the proposed screening model, we conducted a sensitivity analysis by varying the cutoff used to dichotomize basal LH (0.15, 0.20, and 0.30 IU/L). For each threshold, diagnostic performance metrics were recalculated, and the multivariable model combining age, BMI, and dichotomized basal LH was refitted. Model discrimination was evaluated using the area under the ROC curve (AUC).
Small variations in the basal LH cutoff within the routine reporting precision of our dataset (0.15 vs 0.20 IU/L) produced identical classification results, and the discriminative performance of the combined model remained stable (AUC=0.87), comparable to the model using continuous basal LH (AUC=0.88).When a more stringent cutoff of 0.30 IU/L was applied, sensitivity decreased whereas specificity increased, accompanied by a moderate reduction in overall discrimination (AUC=0.81).
Discussion
This study systematically evaluated the diagnostic and screening value of age, BMI, Tanner stage, basal sex hormone levels, pelvic ultrasound parameters, and bone age in a cohort of 429 girls aged 4–8 years presenting with early pubertal development. By integrating routinely available clinical, biochemical, and imaging variables, we aimed to identify practical indicators for differentiating central precocious puberty (CPP) from premature thelarche (PT) in real-world clinical settings.
Comparative Value of the Basal LH Level, BMI, and Age for CPP Screening
Basal luteinizing hormone (LH) levels were significantly higher in the CPP group than in the PT group, confirming basal LH as the single indicator with the strongest discriminatory ability. Although multivariable analysis yielded an extremely large odds ratio for the basal LH level, this finding likely reflects the highly skewed distribution of LH values and near-complete separation between groups rather than a linear increase in clinical risk.
Additionally, we conducted sensitivity analyses, which demonstrated that the basal LH level maintained robust screening performance across a range of cutoff values, including the lower thresholds reported in recent studies—consistent with previous reports. This indicates that the diagnostic value of LH is not driven by a single, narrowly defined cutoff.
Moreover, the comparable discrimination between models using continuous and dichotomized the basal LH level indicates that the predictive ability of the model is preserved under simplified decision rules, which may facilitate real-world screening implementation. The basal LH level can serve as a useful first-line screening indicator for CPP, particularly in settings where GnRH stimulation testing is limited or impractical.21
In addition to the basal LH level, both BMI and chronological age were independently associated with CPP. Girls with CPP exhibited higher BMI values, supporting existing evidence that adiposity-related mechanisms—such as leptin signaling, insulin resistance, and inflammatory mediators—may facilitate activation of the hypothalamic–pituitary–gonadal axis and contribute to earlier pubertal onset.22 Epidemiological data from large pediatric cohorts further corroborate the association between overweight status/obesity and increased prevalence of precocious puberty.23
Age, a fundamental and readily available clinical variable, also contributed meaningfully to risk stratification. Although neither age nor BMI alone achieved high discriminatory power, their integration with the basal LH level substantially improved the overall screening performance. In our cohort, the combined model incorporating basal LH, age, and BMI clearly outperformed any single indicator, particularly in individuals with borderline basal LH concentrations. Accordingly, we propose a pragmatic screening approach that leverages these routinely obtainable variables to identify girls at higher risk of CPP who may benefit from confirmatory GnRH stimulation testing, while potentially reducing unnecessary testing in low-risk cases.
Clinical Implications of BMI and Hormonal Parameters
BMI remained an independent predictor of CPP in both the univariable and multivariable analyses, consistent with findings from previous large retrospective studies.24 Importantly, elevated BMI has been shown to influence gonadotropin dynamics, including blunted LH peak responses and reduced LH/FSH ratios during GnRH stimulation. As a result, reliance on stimulation testing alone in overweight or obese girls may increase the risk of underdiagnosis.25
These observations underscore the clinical value of integrating basal hormonal measurements with anthropometric parameters and overall clinical assessment. Combining the basal LH concentration with BMI may improve risk stratification and help clinicians interpret equivocal hormonal results more accurately. Emerging studies further suggest that multiparameter approaches incorporating additional serum markers may enhance diagnostic performance;26 however, such strategies may be less feasible in routine practice. In contrast, the present model prioritizes simplicity and accessibility, which are essential for effective screening in everyday clinical settings.
Role of Pelvic Ultrasonography in Screening and Phenotyping
Pelvic ultrasonography revealed larger ovarian volumes and more frequent endometrial echo positivity in girls with CPP, consistent with previous imaging studies, demonstrating the additive value of uterine and ovarian parameters in pubertal assessment.27 Nevertheless, in the multivariable analysis, ovarian volume did not emerge as an independent predictor, highlighting the substantial overlap in ultrasound findings between CPP and PT and the absence of universally accepted cutoff values.
Rather than diminishing the clinical relevance of ultrasonography, these findings emphasize its supportive role. Pelvic ultrasound remains a valuable adjunctive tool, particularly in cases with borderline basal LH levels or atypical clinical presentations, where morphological information may refine risk assessment and guide follow-up decisions.28 Ultrasound may also be especially informative in overweight or obese girls, in whom adiposity-related endocrine alterations complicate interpretation of hormonal thresholds.29
Taken together, our results suggest that pelvic ultrasonography should not be used in isolation for CPP screening but should instead be integrated with basal LH levels, age, and BMI to optimize diagnostic accuracy. The retrospective, single-center nature of this study, the lack of longitudinal follow-up, and the potential variability in ultrasound measurements represent important limitations. Future multicenter prospective studies incorporating standardized imaging protocols and external validation are warranted.
Conclusion
In this retrospective study of 429 girls aged 4–8 years presenting with early breast development, we identified chronological age, BMI, and basal LH concentration as independent factors associated with central precocious puberty. The basal LH concentration demonstrated the strongest individual discriminatory ability, and a cutoff value of 0.15 IU/L showed favorable screening performance in this cohort. A simplified multiparameter model integrating basal LH concentration, age, and BMI further improved the overall screening accuracy compared with that of any single indicator, particularly relevant for early screening of CPP.
Although pelvic ultrasound findings such as ovarian enlargement and endometrial echo positivity were more frequently observed in girls with CPP, these parameters were not independent predictors and should be interpreted as supportive rather than definitive indicators. Collectively, these findings suggest that a simple, low-cost screening strategy based on routinely available clinical and laboratory variables may help identify girls at higher risk of CPP and reduce unnecessary GnRH stimulation testing.
Given the single-center, retrospective design of the study and assay-dependent nature of basal LH measurements, external validation is required before broader clinical implementation. Future prospective, multicenter studies are needed to confirm the generalizability of this screening approach and to explore its integration into routine clinical decision-making pathways.
Ethics
The clinical experimental plan was approved by the Clinical Trial Ethics Committee of the West China Second University Hospital, Sichuan University (2025-540). The requirement for informed consent was waived by the Ethics Committee because of the retrospective nature of the study and the use of previously collected clinical data. The study involved no additional interventions or contact with the participants.
All data were anonymized and de-identified prior to analysis. Only the minimum necessary data were collected, and all personal identifiers were permanently removed. The privacy and confidentiality of the participants were strictly protected throughout the study. The work was carried out in accordance with the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Endocrine, Genetic and Metabolic Group of the Pediatrics Branch, Chinese Medical Association; Editorial Board of Chinese Journal of Pediatrics. Expert knowledge on diagnosis and treatment of central precocious puberty (2022). Chin J Pediatr. 2023;61(1):16–10.
2. Dai Y, Liang Z. Therapeutic effects of clomiphene on idiopathic central precocious puberty in girls and its impact on sex hormone levels and PCOS incidence. Pract Gynecol Endocrinol Electron J. 2019;6(17):132–133,191.
3. Brito VN, Canton APM, Seraphim CE, et al. The congenital and acquired mechanisms implicated in the etiology of central precocious puberty. Endocr Rev. 2023;44(2):193–221. doi:10.1210/endrev/bnac020
4. Chinese Preventive Medicine Association Women’s Health Branch Adolescent Health Group. Consensus on the diagnosis and treatment of precocious puberty in females. China Matern Child Health Res. 2018;29(2):135–138.
5. Zhu D, Zhu H. A survey and research on the current status of precocious puberty in urban children in China. Chin J Integr Tradit West Med Pediatr. 2016;8(1):100–102.
6. Knific T, Lazarevič M, Žibert J, et al. Final adult height in children with central precocious puberty: a retrospective study. Front Endocrinol. 2022;13:1008474. doi:10.3389/fendo.2022.1008474
7. Chirico V, Lacquaniti A, Salpietro V, et al. Central precocious puberty: from physiopathological mechanisms to treatment. J Biol Regul Homeost Agents. 2014;28(3):367–375.
8. Shearrer GE, Sadler JR, Papantoni A, et al. Earlier onset of menstruation is related to increased body mass index in adulthood and altered functional correlations between visual, task control and somatosensory brain networks. J. Neuroendocrino. 2020;32(12):e12891. doi:10.1111/jne.12891
9. Liu G, Guo J, Zhang X, et al. Obesity is a risk factor for central precocious puberty: a case-control study. BMC Pediatric. 2021;21(1):509. doi:10.1186/s12887-021-02936-1
10. Biro FM, Galvez MP, Greenspan LC, et al. Pubertal assessment method and baseline characteristics in a mixed longitudinal study of girls. Pediatrics. 2010;126(3):e583–e590. doi:10.1542/peds.2009-3079
11. Anyanwu OU, Ibekwe RC, Nwokocha ARC, et al. An assessment of sexual maturation among school girls in Abakaliki Metropolis, Ebonyi State, South-East Nigeria. Niger Postgraduate Med J. 2016;23(3):121–126. doi:10.4103/1117-1936.190348
12. Lian Q, Mao Y, Luo S, et al. Puberty timing associated with obesity and central obesity in Chinese Han girls. BMC Pediatric. 2019;19(1):1. doi:10.1186/s12887-018-1376-4
13. Khadgawat R, K MR, Mehan N, et al. Age of onset of puberty in apparently healthy school girls from Northern India. Indian pediatrics. 2016;53(5):383–387. doi:10.1007/s13312-016-0857-5
14. M TA, Stathori G, Paltoglou G, et al. Childhood obesity, hypothalamic inflammation, and the onset of puberty: a narrative review. Nutrients. 2024;16(11):1720. doi:10.3390/nu16111720
15. Calcaterra V, C MV, Hruby C, et al. Links between childhood obesity, high-fat diet, and central precocious puberty. Children. 2023;10(2):241. doi:10.3390/children10020241
16. Ahmed ML, Ong K, Dunger DB. Childhood obesity and the timing of puberty. Trends Endocrinol Metab. 2009;20(5):237–242. doi:10.1016/j.tem.2009.02.004
17. Ruonan LI, Xin S, Tenglin Z, Shuxun Y. Childhood obesity and central precocious puberty. J. Cent. South Univ. 2024;49(7):1034–1041.
18. Zevin EL, Eugster EA. Central precocious puberty: a review of diagnosis, treatment, and outcomes. Lancet Child Adolesc Health. 2023;7(12):886–896. doi:10.1016/S2352-4642(23)00237-7
19. Schoelwer M, Eugster EA. Treatment of peripheral precocious puberty. Endocr Dev. 2016;29:230–239.
20. Williams V, Soliman AM, Barrett AM, et al. Review and evaluation of patient-centered psychosocial assessments for children with central precocious puberty or early puberty. J Pediatr Endocrinol Metab. 2018;31(5):485–495. doi:10.1515/jpem-2017-0465
21. Francis K, Candler T, Pritchard C. Using basal LH to predict response on luteinising hormone releasing hormone stimulation test. Endocr Abstr. 2023;95.
22. Shi L, Jiang Z, Zhang L. Childhood obesity and central precocious puberty. Front Endocrinol. 2022;13:1056871. doi:10.3389/fendo.2022.1056871
23. Liu Y. Cross-sectional study on precocious puberty in children in Guangdong, China [dissertation]. Guangzhou. 2022.
24. Zhao M, Liu M, Cao B, et al. Associations between body mass index and pubertal development based on the outcomes of girls with early breast development. Front Endocrinol. 2022;13:991908. doi:10.3389/fendo.2022.991908
25. Gul SU, Karadag A, Ozsoy NS, et al. The effect of obesity on the GnRH stimulation test in girls with idiopathic central precocious puberty. Eur J Pediatr. 2025;184(4):254. doi:10.1007/s00431-025-06077-w
26. Song X, Zhou J, Han T, et al. Early warning value of multiple serum indicators combined with ultrasound detection in girls with central precocious puberty. Front Endocrinol. 2025;16:1518764. doi:10.3389/fendo.2025.1518764
27. Yu HK, Liu X, Chen JK, et al. Pelvic ultrasound in diagnosing and evaluating the efficacy of gonadotropin-releasing hormone agonist therapy in girls with idiopathic central precocious puberty. Front Pharmacol. 2019;10:104. doi:10.3389/fphar.2019.00104
28. You J, Cheng X, Li X, et al. Clinical risk score for central precocious puberty among girls with precocious pubertal development: a cross-sectional study. BMC Endocr Disord. 2021;21(1):75. doi:10.1186/s12902-021-00740-7
29. Huang RH, Yang L, Yang Y, et al. Development and application of a nomogram model for predicting the risk of central precocious puberty in obese girls. Front Pediatr. 2024;12:1421775.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.