Back to Journals » Risk Management and Healthcare Policy » Volume 19
Barriers to Lean & Safety Management Implementation in Primary Care Settings: Insights from an Unsuccessful Case
Authors Tiso A ![]() , Pozzan C, Pamich C, Verbano C
, Pozzan C, Pamich C, Verbano C ![]()
Received 25 April 2026
Accepted for publication 24 June 2026
Published 9 July 2026 Volume 2026:19 610926
DOI https://doi.org/10.2147/RMHP.S610926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Anna Tiso, Caterina Pozzan, Chiara Pamich, Chiara Verbano
Department of Management Engineering, University of Padua, Vicenza, Italy
*These authors contributed equally to this work
Correspondence: Chiara Verbano, Department of Management and Engineering, University of Padua, Vicenza, Italy, Email [email protected]
Background: Primary care is widely recognized as a cornerstone of universal health coverage, providing high-quality care in community-based settings. Structured managerial approaches such as Lean & Safety Management (L&SM) can support quality improvement in healthcare by reducing waste and risk and enhancing patient safety and satisfaction. However, evidence on the sustainable implementation of L&SM—defined as the ability to complete implementation and maintain improvements over time—remains limited in primary care. This study aims to identify key challenges affecting the sustainability of L&SM implementation in community healthcare centers.
Methods: An unsuccessful L&SM implementation was analyzed through an in-depth case study of an Integrated Family Medicine Centre in Italy. The project, based on the DMAIC framework, was discontinued after the Define phase. A structured three-step methodology was adopted: 1) selection of a failed implementation case using predefined suitability criteria; 2) identification of implementation barriers through a systematic assessment of Critical Success Factors for sustainable Lean and Safety implementation adapted from the literature; and 3) validation of findings and exploration of corrective actions through a stakeholders focus group.
Results: The analysis identified multiple barriers that contributed to implementation failure. These barriers were synthesized into three interrelated themes: organizational readiness, stakeholder ownership and engagement, and governance fragmentation. Together, these factors limited coordination, reduced commitment to improvement activities, and hindered the sustainability of the implementation process.
Conclusion: Sustainable L&SM implementation in primary care requires organizational readiness, committed leadership, stakeholder engagement, adequate training, and robust data infrastructure. Addressing these factors may improve the successful adoption and long-term sustainability of quality improvement initiatives in community-based settings.
Keywords: healthcare lean management, lean and safety management, territorial healthcare, sustainability, critical success factors
Introduction
Primary care is widely recognized as a cornerstone of high-performing health systems, ensuring accessibility, continuity, and coordination of care across prevention, treatment, and long-term management of chronic conditions.1 In recent years, OECD countries have increasingly emphasized the central role of primary care in ensuring accessibility, continuity, and quality of care, while promoting reforms aimed at strengthening community-based service delivery models.2 In Italy, this process is mainly driven by a series of initiatives outlined in Ministerial Decree 77/2022, aimed at pursuing the sustainability healthcare goals established by the Italian National Recovery and Resilience Plan (NRRP). However, these reforms face persistent implementation challenges, including limited interprofessional coordination, resource constraints, and increasing demand driven by population ageing and chronic disease burden. These pressures increase the complexity of delivering coordinated and efficient care in primary care settings.3–6
Within this context, primary care organizations must manage increasingly complex care pathways involving multiple professional groups, including general practitioners (GPs), nurses, and administrative staff, while ensuring quality, efficiency, and patient safety.7–9 To address these challenges, structured managerial approaches have been introduced to support healthcare quality improvement and enhance the performance of care delivery systems.
Lean management originated in the Toyota Production System and was initially developed in industrial manufacturing contexts, where it aimed to improve efficiency and quality through the systematic elimination of wastes and defects.10,11 Since the early 2000s, Lean principles have been progressively transferred to healthcare organizations, with the purpose of enhancing patient value through the reduction of non-value-adding activities, such as errors, task duplication, patient waiting times, and inefficient care processes.12–14 Lean healthcare has evolved from a set of operational tools to a broader management philosophy oriented toward value creation and quality improvement. In the healthcare context, quality is a multidimensional concept, encompassing efficiency, effectiveness, timeliness, safety, accessibility, integration and equity, as defined by the World Health Organization.15 In this perspective, recent contributions have integrated Lean Healthcare with clinical risk management into a Lean and Safety Management approach, enabling the simultaneous and proactive management of risks and wastes.16 As proposed in prior studies,17,18 L&SM extends traditional Lean approaches by explicitly incorporating structured risk identification, prevention, and mitigation mechanisms into process improvement initiatives. This integration enables healthcare organizations to address both efficiency and patient safety within a unified improvement framework.
Evidence from hospital-based settings suggests that Lean interventions can improve patient flow, operational efficiency, and quality of care.19 However, their effectiveness remains highly context-dependent and strongly influenced by organizational and implementation conditions. In particular, given the rise in chronic conditions and population ageing, L&SM can also support the integration of hospital-based services with territorial healthcare in managing patients more effectively, reducing acute events and exacerbations.15,20 In particular, a previous study17 developed an integrated L&SM methodology, identifying a set of activities, tools, and organizational practices aimed at proactively addressing both waste and risk across care processes. The methodology was empirically tested on a chronic obstructive pulmonary disease (COPD) care pathway requiring integration between hospital and community services, demonstrated measurable improvements in performance as well as learning-related outcomes.
Despite a growing body of literature on Lean healthcare, the implementation of L&SM remains challenging. Many initiatives fail, either due to premature abandonment or because the improvements achieved during implementation are not sustained over time.21–23 Previous literature shows that such failures are frequently associated with insufficient organizational, managerial, and cultural factors. Several barriers to successful and sustainable implementation have been identified, including limited leadership engagement, insufficient staff involvement, inadequate training, weak data infrastructure, and cultural resistance to change.24–27 The literature consistently identifies the involvement of healthcare professionals and management as critical for the sustainability of improvement initiatives. In particular, fostering a culture of continuous improvement, collaboration, and mutual trust among team members appears to support long-term success.28,29 Multidisciplinary teams are also considered beneficial, as they bring together diverse expertise and perspectives. Conversely, limited leadership engagement, inadequate availability of Lean expertise, and insufficient time and resources allocated to improvement activities have been frequently reported as barriers to implementation and sustainability.30–33 Furthermore, the lack of active managerial support may reduce employee motivation and involvement in Lean initiatives, hindering their integration into routine practice.34,35
However, most of this evidence originates from hospital settings, which are typically characterized by hierarchical governance structures and more standardized workflows. Less is known about Lean implementation in primary care environments,36,37 where decentralized governance, organizational fragmentation and high professional autonomy may significantly influence the transferability of findings from hospital-based studies.38,39
Moreover, most Lean healthcare studies focus on successful or partially successful implementations, while failed or discontinued initiatives remain underexplored.22,40,41 This creates a positive-outcome bias in the literature and limits understanding of the mechanisms underlying implementation failure.42 Analyzing unsuccessful implementations can generate insights that are often not observable in successful implementations alone and can guide future interventions. Failure cases are therefore critical for understanding how and why interventions do not work within a practical context.43,44
Hence, this study aims to identify barriers to the sustainable implementation of Lean & Safety Management in primary care by analyzing a case of unsuccessful implementation in an Integrated Family Medicine Centre (IFMC) in Italy. IFMCs are primary care centers that integrate the efforts of GPs, nurses, and administrative staff to deliver integrated community-based services. These centers rely on coordinated multidisciplinary teamwork and shared operational procedures, while allowing physicians to maintain high degree of professional autonomy, responsibility for clinical decision-making and patient management.45,46 This characteristic reflects the organization of primary care in Italy and several other OECD countries, where GPs typically operate as self-employed professionals working as independent contractors within publicly funded health systems rather than as salaried employees.47,48 While this model may promote professional accountability, continuity of care, and responsiveness to patients’ needs, it can also pose challenges for the implementation of organizational change initiatives. Healthcare organizations characterized by decentralized governance and strong professional autonomy may encounter greater difficulties in achieving consensus, standardizing work practices, and sustaining system-wide quality improvement interventions.49–51 Previous highlights that structural characteristics, professional culture, and readiness for change significantly influence the success of organizational interventions.52,53 Consequently, the implementation of approaches such as Lean & Safety Management may be particularly challenging in highly professionalized healthcare settings, where successful change relies heavily on voluntary engagement and alignment among autonomous professionals.54
By focusing on a failed implementation in this setting, this study contributes to the literature in two main ways: first, by extending knowledge on Lean implementation barriers beyond hospitals into decentralized primary care systems characterized by high GP autonomy, while identifying context-specific solutions for addressing these barriers; and second, by leveraging a failure-based case analysis to identify sustainability barriers that may remain hidden in success-oriented studies, thereby contributing to a more complete understanding of Lean implementation in healthcare systems.
Methods
A structured methodology was applied to achieve the main objective of the study (ie, identifying key barriers to L&SM implementation in IFMC in Italy). As shown in Figure 1, the methodology included (1) identifying a case study involving unsuccessful L&SM implementation, (2) identifying barriers to L&SM implementation by adapting critical success factors from previous studies, and (3) focus group discussion of the identified barriers to suggest possible solutions.
- Identifying a case study involving the unsuccessful implementation of L&SM:
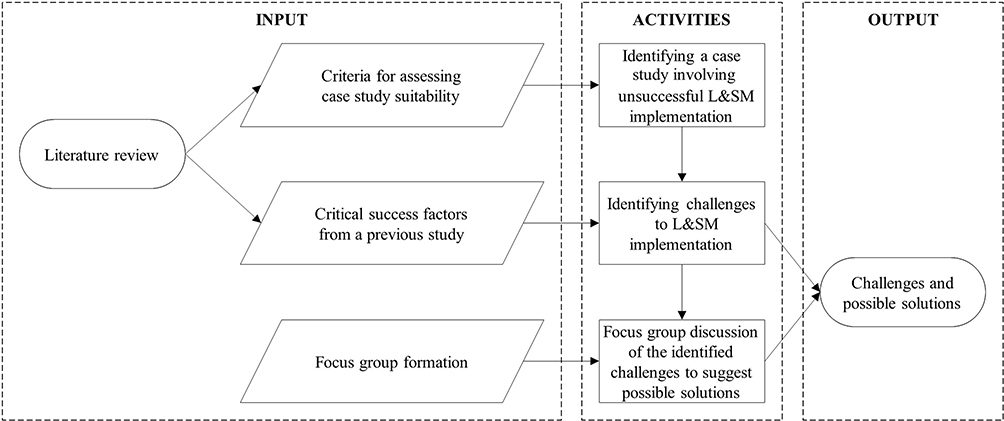 |
Figure 1 Structural flow of the methodology. Figure by authors. |
To identify a suitable case study, four criteria were considered according to the stated objective: (i) a primary care setting, similar to Italian IFMC; ii) L&SM application; (iii) an unsuccessful or incomplete L&SM project, and (iv) the availability of sufficient information to identify and investigate the barriers contributing to implementation failure.
- Identifying barriers to L&SM implementation:
The challenges to the project’s success were identified by adapting the framework proposed by Henrique et al21 that defines Critical Success Factors (CSFs) as aspects fostering the sustainability of L&SM implementations. This framework was selected because it closely aligns with the objective of this study and was developed through an extensive literature review and empirical analysis, including multiple case studies and cross-case analysis.
The adaptation process followed two steps:
- Step 1 - Coding framework: the CSFs were organized into a structured coding matrix, used both to assess implementation status in the case study and to guide the focus group discussion;
- Step 2 - Implementation status assessment: each CSF was evaluated against documented evidence from the case study, determining whether it was fully implemented, partially implemented, or not implemented. Factors that were not implemented because the project failed at an earlier stage were judged as “not applicable”. This assessment was conducted independently by two pairs of researchers and subsequently validated through the focus group discussion.
- Focus group discussion of the identified barriers and possible solutions:
A focus group was conducted to systematically discuss the identified challenges and explore potential solutions, bringing together key stakeholders with direct knowledge of the case.55 Participants were selected through purposive sampling, ensuring direct knowledge and experience relevant to the research question. The focus group involved six participants representing heterogeneous professional profiles: a Human Resources Director, a Manager, a Physician-Manager, a PhD researcher with direct field experience, and a Master’s student in Management Engineering. The session was moderated by an external senior researcher who also actively participated in the discussion, contributing a critically distant perspective on the case. This multi-profile composition ensured the capture of organizational, clinical, managerial, and research perspectives on the failure.55 Prior to the focus group, participants received an oral information statement outlining the study purpose, voluntary participation, and anonymous and aggregated data use. The session was conducted online via Zoom, lasted 90 minutes, and was guided by a semi-structured interview guide developed deductively from the CSF framework,21 ensuring systematic coverage of all barrier categories. The CSFs served as sensitizing concepts to ensure systematic coverage of the implementation factors previously identified during the case analysis while allowing participants to contextualize, challenge, refine, and expand the interpretation of these factors. Accordingly, the focus group was primarily not intended to generate barriers inductively, but rather to critically examine and interpret the implementation challenges identified through the literature-informed analytical framework. This approach is consistent with deductive qualitative analysis, in which existing theoretical constructs guide data collection and interpretation while remaining open to contextual refinement.56,57 The guide included open-ended questions structured around three thematic areas: (i) participants’ direct experience of the identified challenges, (ii) contextual factors that facilitated or hindered L&SM implementation, and (iii) potential solutions for future implementations.
The session was audio-recorded with participants’ informed consent and subsequently transcribed verbatim. The moderator facilitated the discussion while also actively contributing an external research perspective. The transcription was analyzed using deductive content analysis based on the CSF categories from Henrique et al21 as a priori coding framework.58,59 Four researchers with deliberately diverse backgrounds conducted the analysis: the external researcher, the PhD researcher with direct field experience, and two additional researchers external to both the field project and the focus group. After a shared preparation phase involving repeated reading of the transcription, researchers worked in two independent pairs to code the data. Each pair assigned meaningful units of text to predefined CSF categories. The two pairs then compared their coding schemes through a structured consensus-building process, systematically identifying and discussing discrepancies until full agreement was reached. The quality of the consensus was evaluated qualitatively in terms of depth of discussion, transparency of coding decisions, and inclusiveness of all researchers’ perspectives.60
This study focused exclusively on the organizational and administrative structure of an IFMC, including workflows such as appointment scheduling, prescription management, and telephone triage procedures. No patients, clinical decision-making processes, biological materials, patient–physician interactions, medical records, or health-related outcomes were involved or analyzed. The analysis was based on the experience and professional knowledge of physicians and nurses, who participated voluntarily in a non-interventional study. All information was collected and handled in an aggregated and fully anonymized form, and no identifiable personal data were gathered. According to institutional and national regulations, studies of this type do not require Ethics Committee approval. Procedures followed the ethical principles of the Declaration of Helsinki, as applicable.
Results and Discussion
Identifying a Case Study Involving the Unsuccessful Implementation of L&SM
The identified case study regards a L&SM implementation aiming to improve the quality of care delivered within an Italian IFMC. The DMAIC cycle was adopted as a high-level algorithm to guide the implementation process.61 However, the project was interrupted after completing only the initial “Define” phase, without advancing through the complete cycle and thus without implementing improvement actions and monitoring the outcomes. The target IFMC comprises eight family physicians, five nurses, and six administrative staff members. Family physicians operate as independent professionals collaborating with the Local Public Healthcare System. Patients affiliated with this system can choose their physician from this or other IFMCs in the area, depending on availability. Administrative and nursing staff are supplied and managed by a private service provider. The improvement project was strongly endorsed by the director of the private company and by one of the IFMC’s physicians, who served as designated coordinator. Before starting the “Define” phase, a core project team was created, comprising a Master’s thesis student in management engineering, a PhD student, a full professor expert in L&SM, the director, and the head of human resources from the private company. The primary aim of the core project team was to design, plan, and oversee the various activities throughout the project.
The “Define” phase comprehended three main activities: 1) context and resources analysis, 2) demand analysis, and 3) critical care pathways identification. The context analysis highlights the presence of 14,000 patients served by the IFMC, with extended weekday hours from 8:00 AM to 8:00 PM and additional walk-in emergency services on Saturday mornings. A comprehensive analysis of resources and activities revealed the dual nature of the services provided, addressing acute care interventions, follow-up, and prevention activities. Key findings outlined a lack of standardization in physicians’ activities, resulting in operational challenges for administrative staff. The demand analysis, supported by Electronic Health Record (EHR) data, outlined the significant workload associated with chronic patients stemming from ongoing follow-up, preventive care needs, and acute exacerbations. Hypertension, type 2 diabetes, and chronic kidney disease emerged as the most prevalent chronic conditions. Additional self-recorded measurements by personnel, EHR data analysis, and qualitative interviews with staff led to the identification of the diabetes care pathway as the primary target for improvement. This decision was based on the high resource consumption and frequency of patient visits, the need for proactive patient engagement, and the wide range of required care activities. The project concluded at this stage without completing the planned implementation, and no further developments are expected.
Identifying Challenges to L&SM Implementation
The assessment of the CSFs revealed that the unsuccessful L&SM implementation was not associated with a single missing factor, but rather with the simultaneous presence of multiple barriers. The identified barriers can be grouped into three implementation domains: organizational readiness, stakeholder ownership and engagement, and governance fragmentation.
The first area concerns organizational readiness. Several CSFs associated with implementation planning, process standardization, data availability, internal expertise, and long-term improvement capability were either absent or only partially implemented. No detailed implementation plan was developed, internal L&SM and IT expertise were lacking, and available data were fragmented and only partially reliable. Furthermore, the selected IFMC represented quite complex pilot context for a first implementation attempt. These findings suggest that the organization entered the implementation process without several of the structural and managerial preconditions required to support sustainable improvement initiatives.62
The second area concerns stakeholder ownership and engagement. Limited participation was observed among physicians, healthcare workers, and administrative staff throughout the project, as they provided minimal feedback and support for the implementation efforts. This limited participation was partly explained by the lack of a formally established project team, which hindered regular attendance at project meetings. Focus group participants repeatedly highlighted communication shortcomings as a key factor contributing to this limited engagement. Healthcare professionals were not always fully aware of the project objectives, expected benefits, or the specific activities required from them. As one participant noted, “Physicians were not equally informed about either the final purpose of the project or the activities they were expected to perform”.
In addition, staff members were not introduced to the philosophy and principles of L&SM through a structured training program. This gap can be considered particularly relevant, as the literature widely recognizes the development of continuous improvement capabilities and targeted training as critical success factors for both employees and management in ensuring the effective implementation of L&SM.63,64
These communication gaps reduced stakeholders’ understanding of the initiative and hindered the development of a shared commitment to the implementation process. The limited use of visual management tools and the absence of structured communication mechanisms further constrained opportunities to align expectations and maintain engagement over time.65
The third area concerns governance fragmentation. The IFMC operated as a network of autonomous professionals without a formal managerial hierarchy capable of coordinating collective action, establishing common priorities, allocating dedicated time to improvement activities, or promoting standardized work practices. As highlighted during the focus group:
Unlike hospitals, these settings do not have a real hierarchical structure because physicians are self-employed professionals who ultimately answer only to themselves.
This organizational arrangement was further compounded by the absence of clear leadership able to effectively engage, motivate, and align all professional groups around shared improvement goals. Communication challenges among project actors, together with the limited involvement of key stakeholders, further reduced opportunities for collective learning and collaborative decision-making.
Overall, the findings indicate that implementation failure emerged from the interaction among organizational, relational, and governance-related barriers rather than only from deficiencies in Lean tools or methodologies themselves. While many of the identified barriers have been previously reported in Lean healthcare studies, the present case highlights how their combined effect may be amplified in primary care settings characterized by professional autonomy and decentralized governance structures.
Table 1 summarizes the implementation status of each CSFs, the barriers identified during the case analysis, and the suggested solutions proposed during the focus group discussion.
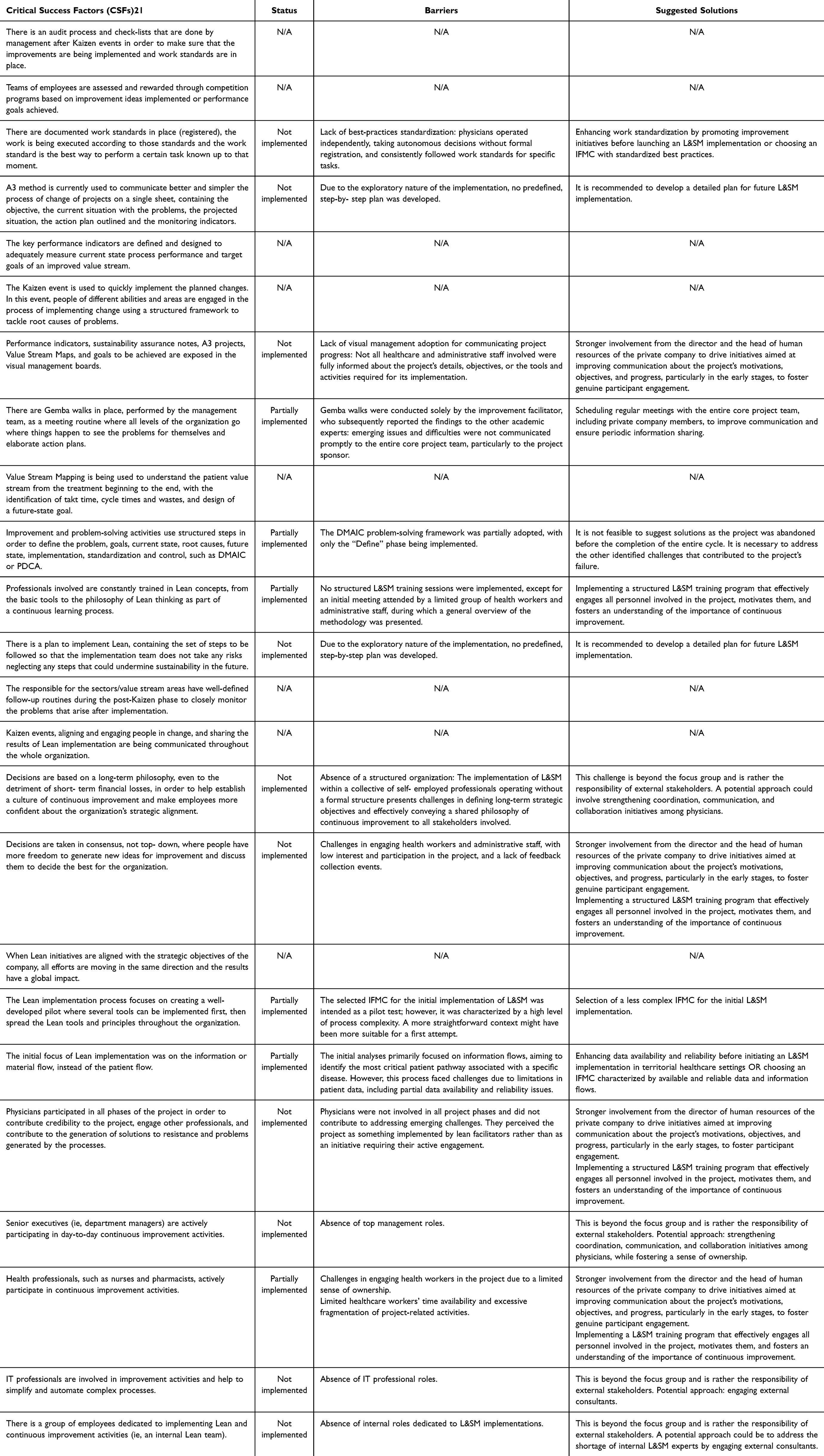 |
Table 1 Implementation Status of Each CSFs, the Barriers Identified During the Case Analysis, and the Suggested Solutions, Table by Authors |
Focus Group Discussion
The focus group discussion provided an opportunity to better understand how the barriers identified through the CSF assessment manifested within the specific organizational context of the IFMC and also to identify potential solutions to overcome the challenges emerged.
A first important insight concerns organizational readiness. The solutions proposed during the focus group pointed towards the need to strengthen the organizational conditions required to support implementation before improvement activities begin. These recommendations included clearer implementation planning, greater process standardization, improved data infrastructures, and the development of internal competencies.
Importantly, the present case extends this literature by illustrating the consequences of initiating an improvement project in the absence of these preconditions. While readiness is often discussed as an enabling factor in successful Lean implementations,23,66 the failure case examined here highlights how insufficient readiness can prevent implementation from progressing beyond its initial stages. In this respect, the findings support the view that readiness should not be considered merely a contextual factor, but rather a foundational condition for lean improvement sustainability.
A second insight relates to stakeholder ownership and engagement. Existing literature consistently identifies staff involvement, empowerment, and training as critical success factors for Lean sustainability.67–69 However, the present findings underline that ownership is not solely determined by participation opportunities but also by stakeholders’ understanding of the initiative and their perceived role within it.
Several participants reported that healthcare professionals perceived the initiative primarily as a university-led project rather than as a shared organizational improvement effort. As one participant explained:
Physicians perceived the project as something that had to be carried out mainly by the university side.
Similarly, another participant noted:Healthcare professionals did not fully understand that a project of this scale would require them to invest some of their own time and effort.
The proposed solutions therefore emphasized communication and training not simply as knowledge-transfer mechanisms, but as tools for fostering shared responsibility and active engagement in the improvement process. This observation appears particularly relevant in primary care settings, where professionals often operate with considerable autonomy and where participation in improvement initiatives depends on voluntary commitment rather than formal managerial authority. In such contexts, ownership appears to develop through continuous communication, role clarification, and meaningful involvement in decision-making processes.
A third insight concerns governance fragmentation. The solutions discussed during the focus group emphasized the need for stronger coordination mechanisms, clearer governance arrangements, and more effective leadership processes capable of aligning stakeholders around shared improvement goals. Participants highlighted that, although the IFMC lacked a formal managerial hierarchy, a stronger leadership role could have been assumed by the private company’s management, not only through the direct oversight of nursing and administrative staff but also by facilitating consensus-building among physicians. The focus group further emphasized that leadership should not be interpreted as a formal authority function, but as a mechanism for fostering engagement, communication, and collective commitment to improvement initiatives. As highlighted in the literature,70–72 leadership plays a critical role in guiding improvement initiatives, empowering and training employees, fostering open communication, and sustaining continuous improvement efforts.30,32 Consequently, a more integrated governance approach, combining stronger leadership support from the director and the head of human resources with proactive engagement strategies, may have strengthened alignment among participants, promoted a shared improvement culture, and enhanced the implementation feasibility.
Beyond the three implementation domains, the focus group highlighted several cross-cutting issues that were present across all implementation stages and domains, helping explain how the identified barriers translated into implementation failure.
First, the discussion revealed challenges related to the perceived legitimacy of the intervention. Legitimacy refers to the extent to which stakeholders perceived the initiative as meaningful, relevant, and shared rather than externally imposed. This mechanism influenced engagement across all professional groups and affected the willingness to participate in implementation activities. Although the project had been formally accepted, professionals were not always fully aware of its objectives, expected benefits, and required contributions. As one participant observed:
We should have organized another meeting with all physicians involved, clearly explaining the objectives, the work required, and letting them decide whether to commit or not.
This suggests that formal agreement to participate did not necessarily translate into genuine commitment to implementation activities. Indeed, the project was not always perceived as a shared organizational priority, but rather as an externally promoted initiative requiring additional effort without clear benefits for everyday practice. This perception reduced motivation to actively participate in implementation activities and further weakened commitment among professional groups.
Second, participants highlighted the difficulty of integrating improvement activities into routine clinical practice. Improvement tasks were frequently perceived as additional responsibilities competing with patient care demands and everyday operational priorities. As one participant explained: “If I have to choose between solving problems in the clinic and attending the project, I will stay in the clinic”. Similarly, another participant noted: “Physicians’ time is spent inside the consultation room”. These observations suggest that many professionals did not develop a strong sense of ownership over the project, as implementation activities were often viewed as separate from routine clinical work rather than as an integral part of professional practice.
Taken together, these findings suggest that implementation failure cannot be fully explained by examining individual barriers in isolation. Rather, failure emerged from the interaction among insufficient organizational readiness, weak stakeholder ownership, and governance fragmentation. Although the individual barriers identified in this study are largely consistent with those reported in previous Lean healthcare literature, the findings contribute to current knowledge by illustrating how these barriers reinforce one another within decentralized primary care organizations.
Conclusion
This study investigated the challenges of implementing L&SM in primary care, focusing on an unsuccessful case conducted within an IFMC in Italy. This research addresses three main gaps identified in the literature on lean healthcare implementation.
First, existing evidence is predominantly based on successful or partially successful implementations,73 resulting in a positive-outcome bias and a limited understanding of the barriers that hinder the lean transition from theory to practice.
Second, most studies are conducted in hospital settings, whereas primary care environments, characterized by decentralized governance, professional autonomy, and fragmented coordination, remain underexplored.
Third, current literature largely emphasizes technical and methodological determinants of success (eg, lean tools), while offering less insight into the organizational and relational conditions that shape whether implementation can progress beyond initial phases.
The findings suggest that implementation failure was primarily driven by insufficient organizational readiness, limited stakeholders’ ownership and engagement, and governance fragmentation. The focus group analysis showed that these barriers were emphasized by reduced perceived legitimacy of the intervention, and limited integration of improvement activities into routine clinical workflows. Although technical competencies and internal L&SM expertise were not fully developed, the findings indicate that organizational and contextual barriers played a more prominent role in constraining implementation progress. In particular, the IFMC setting highlighted how decentralized governance structures, high professional autonomy among GPs, and fragmented coordination mechanisms limited the development of shared and collective commitment to the initiative. In addition, the involvement of multiple stakeholders with differing priorities, expectations, and levels of expertise generated misalignment and competing interests from the earliest stages of implementation.74
Overall, this study contributes to the literature by: i) extending L&SM research beyond hospital settings through evidence from a primary care IFMC characterized by high professional autonomy and decentralized governance; ii) advancing understanding of L&SM implementation failure by analyzing an unsuccessful case; iii) shifting the focus from technical determinants to organizational readiness, interprofessional alignment, and perceived legitimacy as critical conditions for implementation success.
From a practical perspective, the findings suggest that Lean & Safety implementation in primary care should be approached as a comprehensive organizational transformation requiring managerial commitment, workforce engagement, and structural readiness, rather than a mere technical intervention. Several managerial recommendations emerged from the analyzed case:
- Ensure perceived legitimacy of the initiative, through early stakeholders’ involvement, clear communication of objectives, and explicit clarification of expected contributions;
- Foster shared ownership across stakeholders, through structured training, active participation in decision-making, and shared responsibility for implementation activities;
- Integrate improvement activities into routine clinical practice, by allocating dedicated time, embedding improvement tasks into existing workflows, and reducing the perception of Lean as an additional burden;
- Strengthen process readiness and organizational conditions before improvement intervention through implementation planning, process standardization, competency development, and reliable information systems;
- Establish governance and leadership mechanisms capable of coordinating autonomous professionals and aligning stakeholders around shared improvement goals.
The study is based on a single-case design and on an implementation that was discontinued in its early phase. Therefore, the findings cannot be statistically generalized. However, they offer analytical insights that may be transferable to primary care contexts characterized by similar governance structures, professional autonomy, and organizational fragmentation.
Future research could further examine how organizational readiness for L&SM can be systematically assessed and strengthened prior to implementation in primary care settings. Additional longitudinal studies are needed to explore how to sustain L&SM practices in primary care over time, as well as the role of information systems and infrastructure in supporting coordination and shared decision-making in decentralized healthcare systems.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT 5.3 in order to improve the readability and language of the manuscripts. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethics Statement
This study focused exclusively on the organizational and administrative structure of an IFMC, including workflows such as appointment scheduling, prescription management, and telephone triage procedures. No patients, clinical decision-making processes, biological materials, patient–physician interactions, medical records, or health-related outcomes were involved or analyzed. The analysis was based on the experience and professional knowledge of physicians and nurses, who participated voluntarily in a non-interventional study. All information was collected and handled in an aggregated and fully anonymized form, and no identifiable personal data were gathered. According to institutional and national regulations, studies of this type do not require Ethics Committee approval. Procedures followed the ethical principles of the Declaration of Helsinki, as applicable.
Acknowledgments
Anna Tiso, Caterina Pozzan, Chiara Pamich, and Chiara Verbano gratefully acknowledge funding from Next Generation EU, in the context of the National Recovery and Resilience Plan, Investment Partenariato Esteso PE8 “Conseguenze e sfide dell’invecchiamento”, Project Age-It (Ageing Well in an Ageing Society) - CUP C93C22005240007. The views and opinions expressed are only those of the authors and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. World Health Organization. Primary health care. World Health Organization; 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/primary-health-care.
2. World Health Organization. Primary health care: making our commitments happen. Realizing the potential of primary health care: lessons learned from the COVID-19 pandemic and implications for future directions in the WHO European Region. 2022.
3. Mauro M, Giancotti M. The 2022 primary care reform in Italy: improving continuity and reducing regional disparities? Health Policy. 2023;135:104862. doi:10.1016/j.healthpol.2023.104862
4. Tiso A, Pozzan C, Verbano C. Health lean management implementation in local health networks: a systematic literature review. Oper Res Perspect. 2022;9:100256. doi:10.1016/j.orp.2022.100256
5. World Health Organization. Long-Term Care for Older People: Package for Universal Health Coverage. World Health Organization; 2024.
6. World Health Organization, UNICEF. Global Report on Assistive Technology. World Health Organization; 2022.
7. Gress S, Baan CA, Calnan M, et al. Co-ordination and management of chronic conditions in Europe: the role of primary care–position paper of the European Forum for Primary Care. Qual Prim Care. 2009;17(1):75–15.
8. Van Houdt S, Heyrman J, Vanhaecht K, Sermeus W, De Lepeleire J. Care pathways across the primary-hospital care continuum: using the multi-level framework in explaining care coordination. BMC Health Serv Res. 2013;13(1):296. doi:10.1186/1472-6963-13-296
9. Contandriopoulos D, Perroux M, Cockenpot A, Duhoux A, Jean E. Analytical typology of multiprofessional primary care models. BMC Fam Pract. 2018;19(1):44. doi:10.1186/s12875-018-0731-8
10. Womack JP, Jones DT. The Machine That Changed the World: The Story of Lean Production-- Toyota’s Secret Weapon in the Global Car Wars That Is Now Revolutionizing World Industry … World Industry).
11. Ohno T. Toyota Production System: Beyond Large-Scale Production. Productivity Press; 1988.
12. Talero-Sarmiento L, Escobar L, Avila F, Parra-Sánchez D. A literature review on Lean healthcare: implementation strategies, challenges, and future research directions. Cogent Eng. 2024;11. doi:10.1080/23311916.2024.2411857
13. Alkaabi M, Simsekler MCE, Jayaraman R, et al. Evaluation of system modelling techniques for waste identification in lean healthcare applications. Risk Manag Healthc Policy. 2021;13:3235–3243. doi:10.2147/RMHP.S283189
14. de Carvalho JC, Ramos M, Paixão C. A lean case study in an oncological hospital: implementation of a telephone triage system in the emergency service. Risk Manag Healthc Policy. 2013;7:1–10. doi:10.2147/RMHP.S49535
15. World Health Organization. Quality health services: a planning guide. 2020. Available from: https://www.who.int/publications-detail-redirect/9789240011632.
16. Crema M, Verbano C. Investigating the connections between health lean management and clinical risk management: insights from a systematic literature review. Int J Health Care Qual Assur. 2015;28:791–811. doi:10.1108/IJHCQA-03-2015-0029
17. Tiso A, Pozzan C, Crema M, Verbano C. Bridging organizational boundaries in complex care pathways: lessons from a Lean and Safety Management approach. BMC Health Serv Res. 2026;26. doi:10.1186/s12913-026-14415-3
18. Mendes L, França G. Lean thinking and risk management in healthcare organizations: a systematic literature review and research agenda. Int J Qual Reliab Manage. 2024;42(3):851–892. doi:10.1108/IJQRM-06-2023-0210
19. Antony J, Sunder MV, Sreedharan R, Chakraborty A, Gunasekaran A. A systematic review of Lean in healthcare: a global prospective. Int J Qual Reliab Manage. 2019;36(8):1370–1391. doi:10.1108/IJQRM-12-2018-0346
20. Tiso A, Verbano C. Lean and safety management in primary care: guidelines to improve the continuity of care for chronic pathways. In:
21. Henrique DB, Filho MG, Marodin G, Jabbour ABLDS, Jabbour CJC. A framework to assess sustaining continuous improvement in lean healthcare. Int J P Res. 2021;59(10):2885–2904. doi:10.1080/00207543.2020.1743892
22. Kunnen YS, Roemeling OP, Smailhodzic E. What are barriers and facilitators in sustaining lean management in healthcare? A qualitative literature review. BMC Health Serv Res. 2023;23(1):958. doi:10.1186/s12913-023-09978-4
23. Narayanamurthy G, Gurumurthy A, Subramanian N, Moser R. Assessing the readiness to implement lean in healthcare institutions – a case study. Int J Prod Econ. 2018;197:123–142. doi:10.1016/j.ijpe.2017.12.028
24. Vaishnavi V, Suresh M. Assessment of readiness level for implementing lean six sigma in healthcare organization using fuzzy logic approach. Int J Lean Six Sigma. 2020;12(2):175–209. doi:10.1108/IJLSS-07-2019-0081
25. Vaishnavi V, Suresh M, Dutta P. A study on the influence of factors associated with organizational readiness for change in healthcare organizations using TISM. Benchmarking. 2019;26(4):1290–1313. doi:10.1108/BIJ-06-2018-0161
26. LaGanga LR. Lean service operations: reflections and new directions for capacity expansion in outpatient clinics. J Oper Manage. 2011;29(5):422–433. doi:10.1016/j.jom.2010.12.005
27. Fournier PL, Jobin MH, Lapointe L, Bahl L. Lean implementation in healthcare: offsetting Physicians’ resistance to change. Prod Plann Control. 2023;34(6):493–505. doi:10.1080/09537287.2021.1938730
28. Leal Codognotto E, Lizarelli FL, Godinho Filho M, Ganga GMD. From barriers to breakthroughs: organizational learning as a catalyst for Lean Healthcare excellence. Int J Lean Six Sigma. 2025;1–41. doi:10.1108/IJLSS-05-2025-0141
29. Erthal A, Frangeskou M, Marques L. Cultural tensions in lean healthcare implementation: a paradox theory lens. Int J Prod Econ. 2021;233:107968. doi:10.1016/j.ijpe.2020.107968
30. McDermott AM, Kidd P, Gately M, et al. Restructuring of the Diabetes Day Centre: a pilot lean project in a tertiary referral centre in the West of Ireland. BMJ Qual Saf. 2013;22(8):681–688. doi:10.1136/bmjqs-2012-001676
31. Hung DY, Gray CP, Truong QA, Harrison MI. Sustainment of lean redesigns for primary care teams. Qual Manag Health Care. 2019;28(1):15–24. doi:10.1097/QMH.0000000000000200
32. Tlapa D, Zepeda-Lugo CA, Tortorella GL, et al. Effects of lean healthcare on patient flow: a systematic review. Value Health. 2020;23(2):260–273. doi:10.1016/j.jval.2019.11.002
33. Morell-Santandreu O, Santandreu-Mascarell C, Garcia-Sabater JJ. A model for the implementation of lean improvements in healthcare environments as applied in a primary care center. Int J Environ Res Public Health. 2021;18(6):6. doi:10.3390/ijerph18062876
34. Bhat S, Gijo EV, Antony J, Cross J. Strategies for successful deployment and sustainment of Lean Six Sigma in healthcare sector in India: a multi-level perspective. TQM J. 2022;35(2):414–445. doi:10.1108/TQM-10-2021-0302
35. Leite H, Williams S, Radnor Z, Bateman N. Emergent barriers to the lean healthcare journey: baronies, tribalism and scepticism. Prod Plann Control. 2024;35(2):115–132. doi:10.1080/09537287.2022.2054386
36. Pozzan C, Tiso A, Pamich C, Verbano C. Sustainable care quality improvement: a scoping literature review of performance measurement in lean healthcare implementations. BMC Health Serv Res. 2025;25(1):1452. doi:10.1186/s12913-025-13598-5
37. Misra R, Fernando S. Organisational barriers to the lean management approach in healthcare. Sage Open. 2026;16(1):21582440251413494. doi:10.1177/21582440251413494
38. Taglione MS, Brown JB. Primary care engagement in health system change: a scoping review of common barriers and effective strategies. BMC Prim Care. 2023;24(1):157. doi:10.1186/s12875-023-02117-2
39. Kringos DS, Boerma WGW, Hutchinson A, Saltman RB, eds. Building Primary Care in a Changing Europe. European Observatory on Health Systems and Policies; 2015.
40. Moraros J, Lemstra M, Nwankwo C. Lean interventions in healthcare: do they actually work? A systematic literature review. Int J Qual Health Care. 2016;28(2):150–165. doi:10.1093/intqhc/mzv123
41. Costa LBM, Godinho Filho M. Lean healthcare: review, classification and analysis of literature. Prod Plann Control. 2016;27(10):823–836. doi:10.1080/09537287.2016.1143131
42. Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ. Publication and related biases: a review. Health Technol Assess. 2000;4(10):1–115. doi:10.3310/hta4100
43. Sibbald SL, Van Asseldonk R, Cao PL, Law B. Lessons learned from inadequate implementation planning of team-based chronic disease management: implementation evaluation. BMC Health Serv Res. 2021;21(1):134. doi:10.1186/s12913-021-06100-4
44. Green J, Hanckel B, Petticrew M, Paparini S, Shaw S. Case study research and causal inference. BMC Med Res Methodol. 2022;22:307. doi:10.1186/s12874-022-01790-8
45. Ghiotto MC, Rizzolo Y, Gandolfo E, Zuliani E, Mantoan D. Strengthening primary care: the Veneto Region’s model of the Integrated Medical Group. Health Policy. 2018;122(11):1149–1154. doi:10.1016/j.healthpol.2018.08.008
46. Tousijn W. Integrating health and social care: interprofessional relations of multidisciplinary teams in Italy. Curr Sociol. 2012;60(4):522–537. doi:10.1177/0011392112438335
47. OECD. Health at a Glance 2025: OECD Indicators. OECD Publishing; 2025.
48. European Observatory on Health Systems and Policies. Italy: Health System Review 2022. World Health Organization; 2022.
49. Scott WR. Managing professional work: three models of control for health organizations. Health Serv Res. 1982;17(3):213–240.
50. Freidson E. Professionalism, the Third Logic: On the Practice of Knowledge. Bibliovault OAI Repository, the University of Chicago Press; 2001.
51. Mintzberg H. The Structuring of Organizations. In: Asch D, Bowman C, editors. Readings in Strategic Management. Macmillan Education UK; 1989:322–352. doi:10.1007/978-1-349-20317-8_23
52. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581–629. doi:10.1111/j.0887-378X.2004.00325.x
53. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implementation Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
54. Lindsay C, Kumar M, Juleff L. Operationalising lean in healthcare: the impact of professionalism. Prod Plann Control. 2019;31:1–15. doi:10.1080/09537287.2019.1668577
55. Morgan DL. Focus Groups as Qualitative Research. SAGE Publications, Inc.; 1997. doi:10.4135/9781412984287
56. Bryant A, Charmaz K, Gilgun JF. Deductive qualitative analysis and grounded theory: sensitizing concepts and hypothesis-testing. In: The SAGE Handbook of Current Developments in Grounded Theory. SAGE Publications Ltd; 2019:107–122. doi:10.4135/9781526485656
57. Fife ST, Gossner JD. Deductive qualitative analysis: evaluating, expanding, and refining theory. Int J Qual Methods. 2024;23:16094069241244856. doi:10.1177/16094069241244856
58. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
59. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
60. Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory Into Pract. 2000;39(3):124–130. doi:10.1207/s15430421tip3903_2
61. Pyzdek T, Keller P. The Six Sigma Handbook, 5E.
62. Al-Balushi S, Sohal AS, Singh PJ, Al Hajri A, Al Farsi YM, Al Abri R. Readiness factors for lean implementation in healthcare settings–a literature review. J Health Organ Manag. 2014;28(2):135–153. doi:10.1108/JHOM-04-2013-0083
63. Poksinska B. The current state of lean implementation in health care: literature review. Qual Manag Health Care. 2010;19(4):319–329. doi:10.1097/QMH.0b013e3181fa07bb
64. van Elp B, Roemeling O, Aij KH. Lean leadership: towards continuous improvement capability in healthcare. Health Serv Manage Res. 2022;35(1):7–15. doi:10.1177/09514848211001688
65. Radnor ZJ, Holweg M, Waring J. Lean in healthcare: the unfilled promise? Soc Sci Med. 2012;74(3):364–371. doi:10.1016/j.socscimed.2011.02.011
66. Costa F, Portioli-Staudacher A, Alemsan N, Tortorella GL. Readiness level assessment for lean Six Sigma implementation in the healthcare sector. Int J Lean Six Sigma. 2023;15(1):131–152. doi:10.1108/IJLSS-02-2023-0031
67. Drotz E, Poksinska B. Lean in healthcare from employees’ perspectives. J Health Organ Manag. 2014;28(2):177–195. doi:10.1108/JHOM-03-2013-0066
68. Tiso A, Pozzan C, Contreras MFM, Verbano C. Enhancing chronic care pathways with Health Lean Management: a case study in a Spanish hospital. Int J Lean Six Sigma. 2025;16(8):1–36. doi:10.1108/IJLSS-04-2024-0070
69. Abdallah AA. Healthcare engineering: a lean management approach. J Healthc Eng. 2020;2020(1):8875902. doi:10.1155/2020/8875902
70. Mierzwa A, Syrkiewicz-świtała M, Kuraszewska B, et al. Competencies of a healthcare manager in the context of hospital and ambulateral diagnostic imaging centers. Logistics. 2024;8(4):133. doi:10.3390/logistics8040133
71. Poksinska B, Swartling D, Drotz E. The daily work of Lean leaders–lessons from manufacturing and healthcare. Total Qual Manag Bus. 2013;24(7–8):886–898. doi:10.1080/14783363.2013.791098
72. Aij KH, Teunissen M. Lean leadership attributes: a systematic review of the literature. J Health Organ Manag. 2017;31(7–8):713–729. doi:10.1108/JHOM-12-2016-0245
73. Mazzocato P, Savage C, Brommels M, Aronsson H, Thor J. Lean thinking in healthcare: a realist review of the literature. Qual Saf Health Care. 2010;19(5):376–382. doi:10.1136/qshc.2009.037986
74. Madine M, Simsekler MCE, Salah K, Ellahham S. Applying quality improvement science to patient safety: strategies, frameworks, and sustainable solutions. Risk Manag Healthc Policy. 2025;18:3781–3791. doi:10.2147/RMHP.S564459
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.