Back to Journals » International Medical Case Reports Journal » Volume 18
Balanitis Circumscripta Plasmacellularis in a Young Circumcised Male: A Case Report
Authors Alsulaiman OA ![]() , Alsaati AA
, Alsaati AA ![]() , Alsaif NM
, Alsaif NM ![]() , Al-Husain KM
, Al-Husain KM ![]() , Al-Jindan FA, Algamdi BN
, Al-Jindan FA, Algamdi BN ![]()
Received 12 June 2025
Accepted for publication 4 September 2025
Published 8 September 2025 Volume 2025:18 Pages 1167—1173
DOI https://doi.org/10.2147/IMCRJ.S546576
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Omer A Alsulaiman,1 Ahmed A Alsaati,2 Nasser Mohammed Alsaif,1 Khalid M Al-Husain,1 Fatma A Al-Jindan,3 Bader N Algamdi1
1Department of Dermatology, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 2Internal Medicine Department, Jubail General Hospital, Jubail, Saudi Arabia; 3Department of Pathology and Laboratory Medicine, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia
Correspondence: Omer A Alsulaiman, Department of Dermatology, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, 34222, Saudi Arabia, Email [email protected]
Abstract: A 22-year-old incarcerated Saudi man presented with a 2-day history of painful vesicles on the shaft of his circumcised penis that were unrelated to drug use, trauma, exposure to ill persons, or sexual intercourse. Initial laboratory tests were normal, and the patient was initially diagnosed with herpes simplex infection. Due to nonadherence to the initial antiviral treatment, the lesions progressed, leading to a revised diagnosis of chancroid. Subsequent testing ruled out sexually transmitted infections and revealed methicillin-resistant Staphylococcus aureus in the culture of the purulent exudate. Histopathology confirmed balanitis circumscripta plasmacellularis (BCP, zoon’s balanitis). The lesion responded well to topical betamethasone, with marked clinical improvement over 2 months. This case highlights that although rare, BCP should be considered in circumcised patients with non-venereal genital lesions. Additionally, it underscores that early histopathological confirmation is essential to avoid misdiagnosis and inappropriate treatment.
Keywords: balanitis circumscripta plasmacellularis, Zoon’s balanitis, plasma cell balanitis, circumcision, non-venereal genital dermatosis
Introduction
The non-venereal anogenital skin disorders are a spectrum of non-sexually transmitted diseases characterized by pain, pruritus, erythema, swelling, discharges, erosions, ulcerations, plaques, nodules, pigmentary changes, fissures, or lichenification. Compared to diseases at other cutaneous sites, the diagnosis of anogenital skin disorders is challenging due to the sensitive and private nature of the area, delayed decision to biopsy such an area, and the occasional lack of typical lesion appearance.1 In addition, the lack of diagnostic criteria and treatment guidelines for these diseases make them complex and burdensome. Moreover, patients’ fears of sexually transmitted diseases or malignancy often cause anxiety, complicating diagnosis and management.2
Non-venereal anogenital diseases include a variety of conditions such as lichen sclerosus, anogenital lichen planus, contact dermatitis, psoriasis, Zoon’s balanitis, infections, as well as premalignant and malignant lesions.1 Zoon’s balanitis, one of the benign non-venereal dermatoses, was primarily described by Zoon in 1952.3 Clinically, BCP typically presents as a solitary, persistent, well-demarcated, bright erythematous to orange-red patch often with a glossy surface and occasional focal erosions most often on the glans penis or prepuce, but can sometimes present with multiple pinpoint, brighter red spots that may be speckled on the background of an orange to red plaque which is called as “cayenne pepper spots” that are related to microhemorrhages and hemosiderin deposition. Histologically, it is characterized by epidermal atrophy, spongiosis, lichenoid interface dermatitis and a dense band-like plasma cell–rich infiltrate in the upper dermis, along with dilated capillaries and hemosiderin deposition. BCP accounts for approximately 10% of all cases of balanitis, with most patients being uncircumcised middle-aged and older men. The prevalence in circumcised individuals is extremely low, and also exceptionally rare in young adults.2 Its etiology remains idiopathic but may be related to chronic irritation or poor penile hygiene.4 The conventional treatment for Zoon’s balanitis was considered to be circumcision, but in circumcised individuals or few rare cases, other options have also been shown efficacious, such as potent topical corticosteroids, topical mupirocin or topical calcineurin inhibitors.5,6
Case Presentation
A 22-year-old incarcerated Saudi male presented to our clinic complaining of painful vesicles over the shaft of his penis for 2 days prior to his visit. The lesions were not preceded by any history of drug use, trauma, contact with sick people, or sexual intercourse. In addition, this was the first time the patient had such a complaint, and he was medically free of any dermatoses or other chronic diseases. At the time of presentation, the patient was afebrile, and vital signs were stable There were no constitutional or systemic symptoms related to his chief complaint.
On examination, multiple coalescing vesiculopustular lesions with scalloped margins were seen over the glans of his adequately circumcised penis. The lesions were painful and tended to rupture, inevitably resulting in ulcerated lesions. General examination revealed no rash involving other parts of the body and no palpable lymph nodes or organomegaly.
Laboratory tests, including complete blood count and C-reactive protein levels, were normal. In addition, swab cultures and sexually transmitted infection workups, including hepatitis B surface antigen, hepatitis B surface antibody, hepatitis B core antibody, hepatitis C virus, human immunodeficiency virus, and syphilis immunoglobulin G, were ordered. However, polymerase chain reaction and herpes simplex virus serology were not performed due to limited availability within the healthcare setting at the time of presentation.
The preliminary diagnosis at that time was herpes simplex infection, and the patient was prescribed oral valacyclovir 1g in addition to topical fusidic acid cream, both twice daily for 7 days. Unfortunately, at follow-up, the patient was nonadherent to his medications, which were not readily available during his incarceration, and his lesions progressed to a solitary, eroded, erythematous, and tender plaque over the glans (Figure 1).
 |
Figure 1 Solitary well-circumscribed eroded ulceration with scattered deep follicular lesions and crusts on them. |
The preliminary impression was then changed to chancroid. Therefore, gram stain and culture swabs were obtained, and the patient received a single dose of azithromycin 1 g orally in addition to a course of oral doxycycline 100 mg once daily for 10 days. Laboratory tests were subsequently negative for human immunodeficiency virus, hepatitis B virus, hepatitis C virus, and syphilis. In addition, the aerobic culture was positive for methicillin-resistant Staphylococcus aureus (MRSA), while the anaerobic culture was negative. The Haemophilus ducreyi swab did not show any signs of the disease.
The differential diagnosis was expanded to include primary syphilis, fixed drug eruption, balanitis circumscripta plasmacellularis (BCP), erythroplasia of Queyrat, and pemphigus disease. Meanwhile, the patient was instructed to continue taking oral doxycycline 100 mg once daily for 2 weeks and apply topical mupirocin twice daily. At follow-up a few weeks later, another syphilis immunoglobulin G screening test was performed, which again showed nonreactivity with no change in the lesion.
Therefore, a punch biopsy was taken from the margin of the lesion. The histology report showed focal skin ulceration with granulation tissue formation (Figure 2). The epidermis showed acanthosis, mild spongiosis, and exocytosis (Figure 3), while the upper dermis had an extensive band-like infiltrate with plasma cells, lymphocytes, histocytes, scattered eosinophils, and hemosiderin-laden macrophages with numerous capillaries. Special stains for microorganisms, including Warthin-Starry and Grocott-Gömöri’s methenamine silver stains, were negative. All of the above features were consistent with BCP.7 Therefore, topical betamethasone ointment was prescribed once daily for 2 weeks, followed by every other day for another 2 weeks, and finally once a week for 1 month. After 2 months, the patient presented with significant improvement as the lesion had decreased in size and became asymptomatic (Figure 4). Future follow-up should show a complete resolution of the lesion. The sequence of clinical events from presentation to resolution was illustrated in Table 1. The patient provided written informed consent for the publication of this case report.
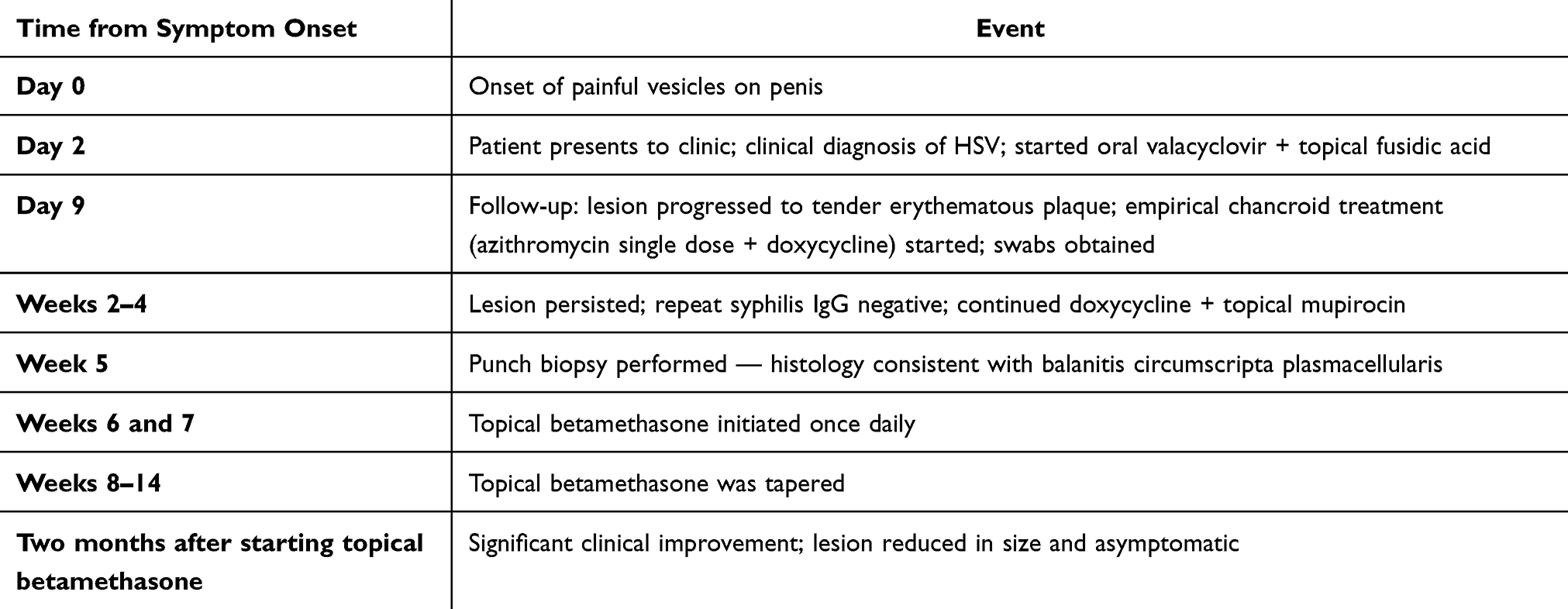 |
Table 1 Timeline of Clinical Events from Presentation to Resolution |
 |
Figure 2 (A) Low-power view of the skin biopsy showing surface ulceration and granulation tissue formation. (B) High-power view of the area of ulceration showing focal loss of the epidermis and necrotic debris. |
 |
Figure 3 (A) Low-power view showing epidermal acanthosis and spongiosis with a band-like infiltrate of the upper dermis. (B) High-power view showing a band-like infiltrate of plasma cells with lymphocytes, histocytes, and scattered eosinophils. Hemosiderin-laden macrophages are also seen. Red arrows in (B) indicate plasma cells. |
 |
Figure 4 Improved solitary well-circumscribed eroded ulceration with fewer scattered deep follicular lesions and few crusts on them. |
Discussion
Zoon’s balanitis, also known as BCP or plasma cell balanitis, is a benign inflammatory dermatosis that affects uncircumcised men.1 Although it usually occurs in older men, the age of onset ranges from 20 to 91 years.6,8 Its counterpart in women, vulvitis circumscripta plasmacellularis, has similar features.9 Clinically, Zoon’s balanitis presents as an asymptomatic erythematous plaque involving the glans, prepuce, or both; however, although generally asymptomatic, the condition may present with tenderness or pruritus.6,10 The histopathologic hallmarks of Zoon’s balanitis include a dense lichenoid infiltrate in the upper and middle dermis with a predominance of band-like plasma cells in the submucosa.1,4,6 Loss of rete ridges, mucosal atrophy, spongiosis, dilated vessels, “lozenge-shaped” keratinocytes, and hemosiderin deposition have also been reported. Special stains are negative for microorganisms, which helps to exclude infectious etiologies. The combination of these clinical and histological features confirms the diagnosis.1,4,6,11,12 However, a report indicates that dermoscopic evaluation of suspected cases often reveals characteristic findings, such as a reddish-orange structureless area and curved and serpentine vessels. Thus, dermoscopy can aid in diagnosis and potentially obviate the need for invasive procedures.13
The differential diagnosis of chronic erythematous or ulcerative lesions of the glans includes infectious, inflammatory, and neoplastic causes. Infectious etiologies such as herpes simplex virus, chancroid, syphilis, and Staphylococcus aureus balanitis were initially suspected in this patient due to the initial onset of vesiculopustular and ulceration. These were excluded by negative serologies for syphilis, negative Haemophilus ducreyi culture, lack of viral confirmation, and lesion persistence despite antiviral and antibacterial therapy. Inflammatory, premalignant and autoimmune conditions such as fixed drug eruption, lichen planus, erythroplasia of Queyrat, and pemphigus vulgaris were considered. The absence of recent medication exposure, characteristic clinical patterns, dysplastic changes, or histologic features of acantholysis allowed their exclusion. In this case, the biopsy findings including epidermal acanthosis, mild spongiosis, and a dense plasma cell–rich infiltrate in the upper dermis, with negative special stains were diagnostic for BCP. Table 2 demonstrating the differential diagnosis of balanitis circumscripta plasmacellularis with a comparison between it and both erythroplasia of Queyrat, and fixed drug eruption according to Chipollini et al14
 |
Table 2 Differential Diagnosis Comparison Table of Balanitis Circumscripta Plasmacellularis, Erythroplasia of Queyrat, and Fixed Drug Eruption |
Circumcision has been the treatment of choice for BCP because the absence of the foreskin would inevitably eliminate the chronic inflammation.2,12–17 However, since the condition develops in a highly sensitive area, many patients do not opt for surgical intervention. In our patient, the penis was adequately circumcised. As a result, several alternative non-surgical treatments have also been reported. These include topical corticosteroids,18,19 topical calcineurin inhibitors such as tacrolimus and pimecrolimus,5,15,20–22 topical imiquimod,21,22 and topical mupirocin.6 Photodynamic therapies such as topical porphyrin precursors (5-aminolaevulinic acid) or methyl aminolevulinate have also been proposed.23,24 Other modalities, such as carbon dioxide7,25 and Erbium YAG laser,26,27 have yielded promising responses. In our patient, topical high-potency corticosteroid (betamethasone ointment) was started after histological confirmation of BCP, with a tapering regimen over approximately 6 weeks. The lesion showed marked reduction in size and complete symptomatic resolution by two months. Longer-term monitoring was advised to detect any recurrence or late complications. If this happened, maintenance betamethasone therapy can be extended.
Our case highlights the fact that although BCP is most commonly seen in middle-aged to older men, it can also develop in young adolescents. Furthermore, the development of non-venereal skin lesions on a circumcised penis does not exclude the possibility of BCP as one of the differential diagnoses.28 The case also emphasizes the need for early biopsy in atypical or non-resolving anogenital lesions and the importance of considering a broad differential diagnoses to avoid delayed treatment.
A similar case was reported by Toker et al29 in which they reported a 59-year-old man with a circumcised penis who developed a persistent ulcerative lesion with a necrotic base over the glans and sulcus coronarius of the penis, which was later found to be consistent with BCP after pathologic examination. Their case suggested the possibility of developing BCP in an inadequately circumcised penis, whereas our case highlights that even an adequately circumcised patient can develop BCP after being confirmed by lesional biopsy. Another case has been reported in a 43-year-old human immune deficiency-positive man who was circumcised since birth.30
Conclusion
This case report highlights the importance for dermatologists and venereologists to consider BCP as a differential diagnosis for non-venereal genital lesions, even in young circumcised patients. BCP should be suspected in cases of chronic, well-demarcated erythematous or erosive lesions of the glans, particularly when they are asymptomatic or mildly symptomatic, while infectious causes have been excluded. As early recognition and appropriate treatment can lead to significant improvement and resolution of the condition.
Ethical Statement
The study was approved by the Imam Abdulrahman Bin Faisal University Institutional Review Board on May 5, 2024 (IRB-PGS-2024-01-412), and we confirm that institutional approval was required for publication of the case details. The patient’s informed consent to publish the case details included publication of the images.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bolognia JL, Schaffer JV, Cerroni L, editors. Dermatology.
2. Dayal S, Sahu P. Zoon balanitis: a comprehensive review. Indian J Sex Transm Dis AIDS. 2016;37(2):129–138. doi:10.4103/0253-7184.192128
3. Zoon JJ. Chronic benign circumscript plasmocytic balanoposthitis. Dermatologica. 1952;105(1):1–7. doi:10.1159/000256880
4. Pastar Z, Rados J, Lipozencić J, Skerlev M, Loncarić D. Zoon plasma cell balanitis: an overview and role of histopathology. Acta Dermatovenerol Croat. 2004;12(4):268–273.
5. Bardazzi F, Antonucci A, Savoia F, Balestri R. Two cases of Zoon’s balanitis treated with pimecrolimus 1% cream. Int J Dermatol. 2008;47(2):198–201. doi:10.1111/j.1365-4632.2008.03392.x
6. Bari O, Cohen PR. Successful management of Zoon’s balanitis with topical mupirocin ointment: a case report and literature review of mupirocin-responsive balanitis circumscripta plasmacelluaris. Dermatol Ther. 2017;7(2):203–210. doi:10.1007/s13555-017-0178-1
7. Retamar RA, Kien MC, Chouela EN. Zoon’s balanitis: presentation of 15 patients, five treated with a carbon dioxide laser. Int J Dermatol. 2003;42(4):305–307. doi:10.1046/j.1365-4362.2003.01304.x
8. Temelkova I, Broshtilova V, Bezhanova S, et al. Zoon’s balanitis (balanitis circumscripta plasmacellularis)-a case report with a review of literature. Clin Dermatol. 2023;6(2):14–17. doi:10.11648/j.ijcd.20230602.11
9. Goldstein AT, Christopher K, Burrows LJ. Plasma cell vulvitis: a rare cause of intractable vulvar pruritus. Arch Dermatol. 2005;141(6):789–790. doi:10.1001/archderm.141.6.789
10. Davis DA, Cohen PR. Balanitis circumscripta plasmacellularis. J Urol. 1995;153(2):424–426. doi:10.1097/00005392-199502000-00043
11. Alessi E, Coggi A, Gianotti R. Review of 120 biopsies performed on the balanopreputial sac from Zoon’s balanitis to the concept of a wider spectrum of inflammatory non-cicatricial balanoposthitis. Dermatology. 2004;208(2):120–124. doi:10.1159/000076484
12. Kumar B, Sharma R, Rajagopalan M, Radotra BD. Plasma cell balanitis: clinical and histopathological features—response to circumcision. Genitourin Med. 1995;71(1):32–34. doi:10.1136/sti.71.1.32
13. Ramar S, Ramamoorthy L, Somasundaram A. Dermoscopy of Zoon’s balanitis. CosmoDerma. 2023;3:158. doi:10.25259/CSDM.195-2023
14. Chipollini J, De la Rosa AH, Azizi M, Shayegan B, Zorn KC, Spiess PE. Patient presentation, differential diagnosis, and management of penile lesions. Can Urol Assoc J. 2019;13(2 Suppl 1):S2–S8. doi:10.5489/cuaj.5712
15. Daga SO, Wagaskar VG, Jumnake SF, Patwardhan SK. Zoon’s balanitis treated with topical tacrolimus. Urol Ann. 2017;9(2):211–213. doi:10.4103/UA.UA_10_16
16. Sonnex TS, Dawber RP, Ryan TJ, Ralfs IG. Zoon’s (plasma‐cell) balanitis: treatment by circumcision. Br J Dermatol. 1982;106(5):585–588. doi:10.1111/j.1365-2133.1982.tb04563.x
17. Ferrándiz C, Ribera M. Zoon’s balanitis treated by circumcision. J Dermatol Surg Oncol. 1984;10(8):622–625. doi:10.1111/j.1524-4725.1984.tb01266.x
18. Yoganathan S, Bohl TG, Mason G. Plasma cell balanitis and vulvitis (of Zoon). A study of 10 cases. J Reprod Med. 1994;39(12):939–944.
19. Tang A, David N, Horton LW. Plasma cell balanitis of Zoon: response to Trimovate cream. Int J STD AIDS. 2001;12(2):75–78. doi:10.1258/0956462011916811
20. Santos-Juanes J, Sánchez Del Río JS, Galache C, Soto J. Topical tacrolimus: an effective therapy for Zoon balanitis. Arch Dermatol. 2004;140(12):1538–1539. doi:10.1001/archderm.140.12.1538
21. Hague J, Ilchyshyn A. Successful treatment of Zoon’s balanitis with topical tacrolimus. Int J Dermatol. 2006;45(10):1251–1252. doi:10.1111/j.1365-4632.2006.02934.x
22. Chander R, Garg T, Kakkar S, Mittal S. Treatment of balanitis of Zoon’s with tacrolimus 0.03% ointment. Indian J Sex Transm Dis AIDS. 2009;30(1):56–57. doi:10.4103/0253-7184.55482
23. Pinto-Almeida T, Vilaça S, Amorim I, Costa V, Alves R, Selores M. Complete resolution of Zoon balanitis with photodynamic therapy–a new therapeutic option? Eur J Dermatol. 2012;22(4):540–541. doi:10.1684/ejd.2012.1779
24. Torchia D, Cappugi P. Photodynamic therapy for Zoon balanitis. Eur J Dermatol. 2014;24(6):707. doi:10.1684/ejd.2014.2439
25. Baldwin HE, Geronemus RG. The treatment of Zoon’s balanitis with the carbon dioxide laser. J Dermatol Surg Oncol. 1989;15(5):491–494. doi:10.1111/j.1524-4725.1989.tb03407.x
26. Albertini JG, Holck DE, Farley MF. Zoon’s balanitis treated with erbium: YAG laser ablation. Lasers Surg Med. 2002;30(2):123–126. doi:10.1002/lsm.10037
27. Wollina U. Ablative erbium: YAG laser treatment of idiopathic chronic inflammatory non-cicatricial balanoposthitis (Zoon’s disease)–A series of 20 patients with long-term outcome. J Cosmet Laser Ther. 2010;12(3):120–123. doi:10.3109/14764171003706125
28. Morris B, Krieger JN. Balanitis and related inflammatory conditions affecting the penis. 2018.
29. Toker SC, Baskan EB, Tunali S, Yilmaz M, Karadogan SK. Zoon’s balanitis in a circumcised man. J Am Acad Dermatol. 2007;57(2):S6–S7. doi:10.1016/j.jaad.2006.02.071
30. Adégbidi H, Atadokpèdé F, Dégboé B, et al. Balanite de Zoon chez un homme circoncis et infecté par le VIH, à Cotonou (Bénin) [Zoon’s balanitis in circumcised and HIV infected man, at Cotonou (Benin)]. Bull Soc Pathol Exot. 2014;107(3):139–141. French. doi:10.1007/s13149-014-0359-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.