Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Bacterial profile of urinary tract infection and antimicrobial susceptibility pattern among pregnant women attending at Antenatal Clinic in Dil Chora Referral Hospital, Dire Dawa, Eastern Ethiopia
Authors Derese B, Kedir H, Teklemariam Z, Weldegebreal F ![]() , Balakrishnan S
, Balakrishnan S ![]()
Received 4 November 2015
Accepted for publication 17 December 2015
Published 18 February 2016 Volume 2016:12 Pages 251—260
DOI https://doi.org/10.2147/TCRM.S99831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Behailu Derese,1 Haji Kedir,2 Zelalem Teklemariam,3 Fitsum Weldegebreal,3 Senthilkumar Balakrishnan4
1Department of Medical Laboratory, Dil Chora Referral Hospital, Dire Dawa, 2Department of Public Health, 3Department of Medical Laboratory Sciences, 4Department of Medical Microbiology, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Purpose: The aim of this study was to determine the bacterial profile of urinary tract infection (UTI) and antimicrobial susceptibility pattern among pregnant women attending at antenatal clinic in Dil Chora Referral Hospital, Dire Dawa, Eastern Ethiopia.
Patients and methods: An institutional-based cross-sectional study was conducted from February 18, 2015 to March 25, 2015. Clean-catch midstream urine specimens were collected from 186 pregnant women using sterile containers. Then, culture and antimicrobial susceptibility tests were performed by standard disk diffusion method. Patient information was obtained using pretested structured questionnaire. Data were entered and cleaned using EpiData Version 3 and then exported to Statistical Package for Social Science (Version 16) for further analysis.
Results: The prevalence of significant bacteriuria was 14%. Gram-negative bacteria were more prevalent (73%). Escherichia coli (34.6%), coagulase-negative staphylococci (19.2%), Pseudomonas aeruginosa (15.4%), and Klebsiella spp. (11.5%) were common bacterial isolates, where most of them were resistant against ampicillin, amoxicillin, tetracycline, trimethoprim–sulfamethoxazole, and chloramphenicol. Multidrug resistance (resistance in ≥2 drugs) was seen in 100% of the isolated bacteria. A majority of the bacterial isolates were sensitive to ciprofloxacin, ceftriaxone, erythromycin, and gentamicin.
Conclusion: This study found a number of bacterial isolates with very high resistance to the commonly prescribed drugs from pregnant women with and without symptoms of UTI. Therefore, the early routine detection of causative agents of UTI and determining their drug susceptibility pattern are important for pregnant women to avoid complications in mother and fetus. Ciprofloxacin, ceftriaxone, gentamicin, and erythromycin can be used with great care for the empirical treatment of UTI.
Keywords: pregnant, urinary tract infections, multidrug resistant, antenatal, Dil Chora, Dire Dawa
Introduction
Urinary tract infection (UTI) is the most common infection in women worldwide.1 It can range from presence of bacteria in urine without symptoms (asymptomatic bacteriuria) to infections producing chiefly bladder symptoms (symptomatic UTIs).2 It is a major health problem reported among 20% of the pregnant women and a common cause of admission in obstetrical wards.3 It results in low birth weight fetus, intrauterine growth retardation, preterm labor and premature babies, intrauterine fetal death, and increased prenatal mortality and morbidity. Maternal complications include anemia, preeclampsia, renal failure, septicemia, and adult respiratory syndrome.4–9
The prevalence of UTI during pregnancy that was reported varied. An overall prevalence of 20% from Saudi Arabia,10 7.7% from India,11 30% from Libya,12 15.5% from Tanzania,13 14% from Khartoum, Sudan,14 and 75% from Niger15 was reported, whereas in Ethiopia, the prevalence of 11.6% from Addis Ababa,16 12% from Gondar,17 and 9.5% from Bahir Dar18 was reported.
Different factors were identified likely to increase risk of UTI during pregnancy, including the history of UTI, sexual activity, history of catheterization, lower socioeconomic status, and multiparity.9,17,19
Antibiotics were given for the treatment of UTI. However, the antibiotic susceptibility patterns of UTI vary according to regional and geographical locations10,20–23 and also change through time.24 The emergence of antibiotic resistance of UTIs is a serious public health issue, particularly in the developing world where apart from high level of poverty, ignorance, and poor hygienic practices, there is also a high prevalence of fake and spurious drugs of questionable quality in circulation.25 Because of rapid increase and spread of mutant strains that are insusceptible to medical treatment, there is also a serious medical problem.23
In many parts of Ethiopia, antibiotics have been widely used to empirically treat the clinically examined individuals with UTI. Thus, there might be an increasing incidence of microbial resistance to commonly used antibiotics for the treatment of UTI.16–18,26 Thus, knowing the magnitude of drug resistance is of critical importance as the changing rate of antibiotic resistance has a large impact on the empirical therapy of UTIs.27
In Dil Chora Referral Hospital, Dire Dawa, routine culture and antibiotic susceptibility testing are not performed and the treatment is on empirical basis. This may lead to the overuse of antibiotics and development of resistant microbial species. However, there is no published information on the prevalence of bacterial profile of UTI and antimicrobial susceptibility pattern in Dire Dawa, Eastern Ethiopia. Therefore, this study tried to determine the bacterial profile of UTI and antimicrobial susceptibility pattern among pregnant women attending at antenatal clinic in Dil Chora Referral Hospital, Dire Dawa, Eastern Ethiopia.
Materials and methods
Study area, design, and period
Dire Dawa city administration is located 520 km away from East Addis Ababa, which is the capital city of Ethiopia. It has a total population of 342,827, of whom 171,930 are males. Approximately 67.9% of inhabitants are urban dwellers. It has 34 health posts, 31 private clinics, 16 health centers, and six hospitals (three private hospitals: one belongs to Ethio-Djibouti railway and two belong to the City Administration Health Bureau). The primary health coverage of the town is 100%.28 A cross-sectional study was conducted at antenatal clinic of Dil Chora Referral Hospital, Dire Dawa, Eastern Ethiopia, from February 18, 2015 to March 25, 2015.
Sample size determination and sampling technique
A single population formula was used to calculate the sample size among pregnant women in the Gondar University Hospital, Ethiopia, by using the following parameters: 12% prevalence rate of UTI,26 margin of error (d) of 0.05, (Zα/2) of 95% confidence interval (CI) level, and 15% nonresponse rate. The final sample size was 186. A convenient sampling technique was used to enroll consecutive pregnant women attending antinatal care in the hospital during the study period.
Method of data collection
All pregnant women were interviewed face to face by trained physician using a pretested questionnaire adapted from the Tazebew et al19 to collect the information about sociodemographic and clinical data related to UTI. After the completion of interview, each pregnant woman was sent to hospital laboratory with her request form. In the laboratory, instruction was given to them by trained medical laboratory professional about how to collect a clean-catch midstream urine specimen. From all the pregnant women, ~10–20 mL of urine specimen was collected by using sterile screw-capped, wide-mouth container.29 The bottles were labeled with unique sample number, date, and time of collection, then immediately they were sent to bacteriology department for testing the culture and antimicrobial susceptibility.
Culture
The well-mixed and noncentrifuged urine samples were inoculated by a wire loop that can deliver 0.001 mL of urine specimen into 5% sheep blood agar, cysteine-lactose-electrolyte-deficient agar, and MacConkey agar plates (Oxoid Ltd, Basingstoke, UK) by using streak plate method following the standard microbiological procedures.29,30 Then, the plates were aerobically incubated at 37°C for 24 hours and examined for the presence or absence of the bacterial growth. Colonies were counted and checked for significant bacteriuria on blood agar. A culture that grew >105 colony-forming unit (CFU/mL) was considered significant bacteriuria. For cultures growing more than one bacterium, subculturing of individual distinct colonies was performed using a sterile wire loop to ensure pure cultures.31 Asymptomatic bacteriuria was defined as the presence of >105 CFU/mL of urine, without the symptoms of an acute UTI.29
All positive urine cultures showing significant bacteriuria were further tested for their physical characteristics such as colony morphology, odor, swarming, and the presence of hemolysis on their respective media. Then, it was confirmed by the pattern of biochemical reactions using the standard procedures.29,30 Thus, Gram-negative rods were identified with the help of a series of biochemical tests such as triple sugar iron agar, indole, simmons citrate agar, oxidase, urease, and motility.29 Morphologically identical colonies of the suspected strains were taken from the agar plates and were suspended in nutrient broth and vortexed. Then, the suspensions were inoculated into the butt and slant of the biochemical testing media. The inoculated media were aerobically incubated at 37°C and after overnight incubation bacteria were identified following the standard flow chart. Gram-positive cocci were identified based on their Gram reaction in catalase and coagulase tests.29,30
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed for the bacterial isolates identified from urine cultures with significant bacteriuria using Kirby-Bauer disk diffusion method32 on Mueller-Hinton agar (Oxoid Ltd) according to the criteria set by the Clinical and Laboratory Standards Institute formerly known as the National Committee for Clinical Laboratory Standards33–35 to determine the susceptibility patterns of the commonly used antibiotics. The antibiotics disks were obtained from Oxoid Ltd in the following concentrations: ampicillin (AMP; 10 μg), ceftriaxone (CRO; 30 μg), chloramphenicol (C; 30 μg), amoxicillin (AMO; 20/10 μg), erythromycin (ERY; 15 μg), gentamicin (GEN; 10 μg), nalidixic acid (NA; 30 μg), nitrofurantoin (F; 300 μg), trimethoprim–sulfamethoxazole (SXT; 25/125 μg), ciprofloxacin (CIP; 5 g), and tetracycline (TTC; 30 μg). Of these, NA can be used only for Gram-negative bacteria, whereas ERY can be used only for Gram-positive bacteria; however, the rest of the antibiotics were used for both isolates. The procedure for antimicrobial susceptibility testing is as follows: Briefly 4–6 morphologically identical colonies of bacteria from pure cultures were collected with an inoculating loop and transferred into a tube containing 5 mL of nutrient broth, then mixed gently until a homogenous suspension was formed, and incubated at 37°C for 3–5 hours until the turbidity of the suspension becomes adjusted to the density of 0.5 McFarland standards, which yield a uniform suspension containing 105–106 cells/mL.31
Using a sterile nontoxic dry cotton swab, sample of the standardized inoculums (turbidity was adjusted to obtain confluent growth) was taken and streaked on the entire surface of the dried Mueller–Hinton agar plate three times, turning the plate at 60° angle between each streaking to ensure even distribution. The inoculums were allowed to dry for 5–15 minutes with the lid in place. Using sterile forceps, the selected antibiotics disks were applied to the plates at a distance of 15 mm away from the edge and 24 mm apart from each other. After incubating the plates at 37°C for 24 hours, diameters of the zone of bacterial growth inhibition around the disks were measured to the nearest millimeter. The susceptibility or resistance to the agent in each disk was determined, and the isolates were classified as sensitive, intermediate, or resistant according to the standardized table.34,35
Data quality assurance
Detailed quality assurance procedures were used to keep the quality of data. Training was given to data collector. The collected data were checked for completeness at the end of each day of data collection. For culturing and biochemical tests, standard operating procedures and manufacturer’s instruction manual were strictly followed. The American Type Culture Collection (ATCC) reference strains such as Escherichia coli (ATCC-25922), Staphylococcus aureus (ATCC-25923), and Pseudomonas aeruginosa (ATCC-27853) were used as quality control parameters throughout the study for testing the culture and biochemical and antimicrobial susceptibility. All the standard strains were obtained from the Ethiopian Public Health Institute.
Data analysis
Data were first entered and cleaned using EpiData Version 3 and exported to Statistical Package for Social Science (Version 16) for further analysis. The proportion of bacterial causes of UTI was calculated by dividing the frequency of positive samples by the total number of samples examined. The proportion of bacterial resistant to a specific drug was calculated by dividing the frequency of resistant bacteria by the total number of bacterial isolates tested to a specific drug. Bivariate and multivariate analyses were performed to evaluate whether individual predictors of interest are associated with UTI. Only variables with P<0.05 at 95% CI in the bivariate analysis were considered for inclusion in the multivariate analysis. Variables with P<0.05 at 95% CI in the multivariate analysis were considered significantly associated with UTI.
Ethical consideration
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee, College of Health and Medical Science, Haramaya University. The objectives of the study were explained well to the head of the hospital and each pregnant woman. Signed consent was also obtained from the head of the hospital and all study participants. Information obtained during this study was kept confidential and used only for this study.
Results
Sociodemographic, obstetrics, and clinical characteristics
A total of 186 pregnant women were included in this study. The majority of the study participants were in the age range of 25–34 years (44.4%) and they mentioned married (92.5%) in their marital status, high school (9–12; 40.3%) in their educational status, and urban dwellers (90.9%) in their residence. Based on their parity, the majority (42.5%) of the study participants were multiparous. Approximately 44.6% of the study participants were in the third trimester of pregnancy. Approximately 26.9% and 29% of the study participants had the history of UTI and antibiotics use, respectively (Table 1).
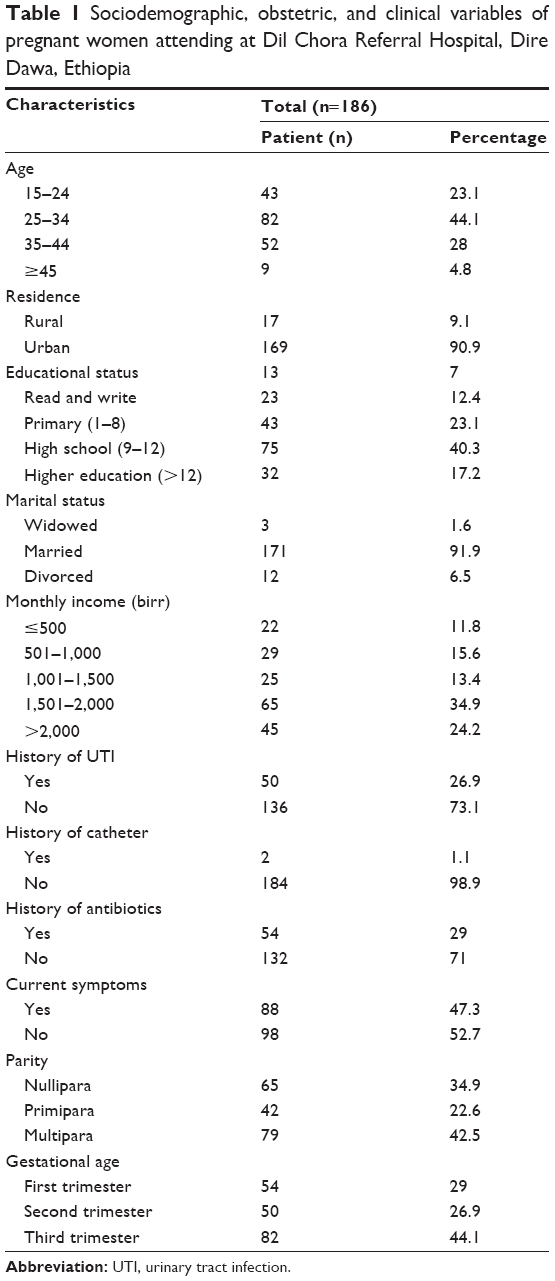 | Table 1 Sociodemographic, obstetric, and clinical variables of pregnant women attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia |
Prevalence of UTI and types of bacterial isolates
In this study, 26 (14%) of the study participants have significant bacteriuria. The prevalence of bacteriuria among symptomatic and asymptomatic pregnant women was 15 (17%) and eleven (11.0%), respectively.
Seven different bacteria were isolated in this study. The majority of the isolates 19 (73.1%) were Gram-negative organisms. E. coli was found to be the most frequent isolate (34.6%), followed by coagulase-negative staphylococci (CONS) (19.2%), P. aeruginosa (15.4%), and Klebsiella spp. (11.5%; Table 2).
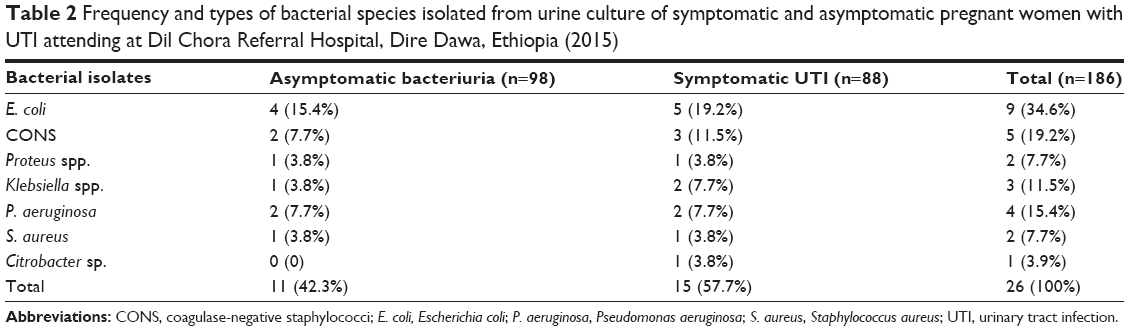 | Table 2 Frequency and types of bacterial species isolated from urine culture of symptomatic and asymptomatic pregnant women with UTI attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia (2015) |
Associated risk factors of UTI
Higher prevalence of UTI was found in the age group of 25–34 years, the education status of read and write, history of UTI, family monthly income level ≤500 birr and income level 501–1,000 birr. Percentages of the bacterial isolates were 73.1%, 38.5%, 80.8%, 34.6%, and 50%, respectively. In multivariate analysis, the prevalence of UTI was significantly associated with those participants with the history of UTI (adjusted odds ratio [AOR] =10.8, 95% CI: 2.008–50.027), family monthly income ≤500 birr (AOR =11.50; 95% CI: 1.789–19.397) and 501–1,000 birr (AOR =15.454; 95% CI: 3.948–26.414), in the age groups of 25–34 years (AOR =5.57; 95% CI: 2.167–19.255), and with the read and write educational level (AOR =2.07; 95% CI: 1.008–9.187; Table 3).
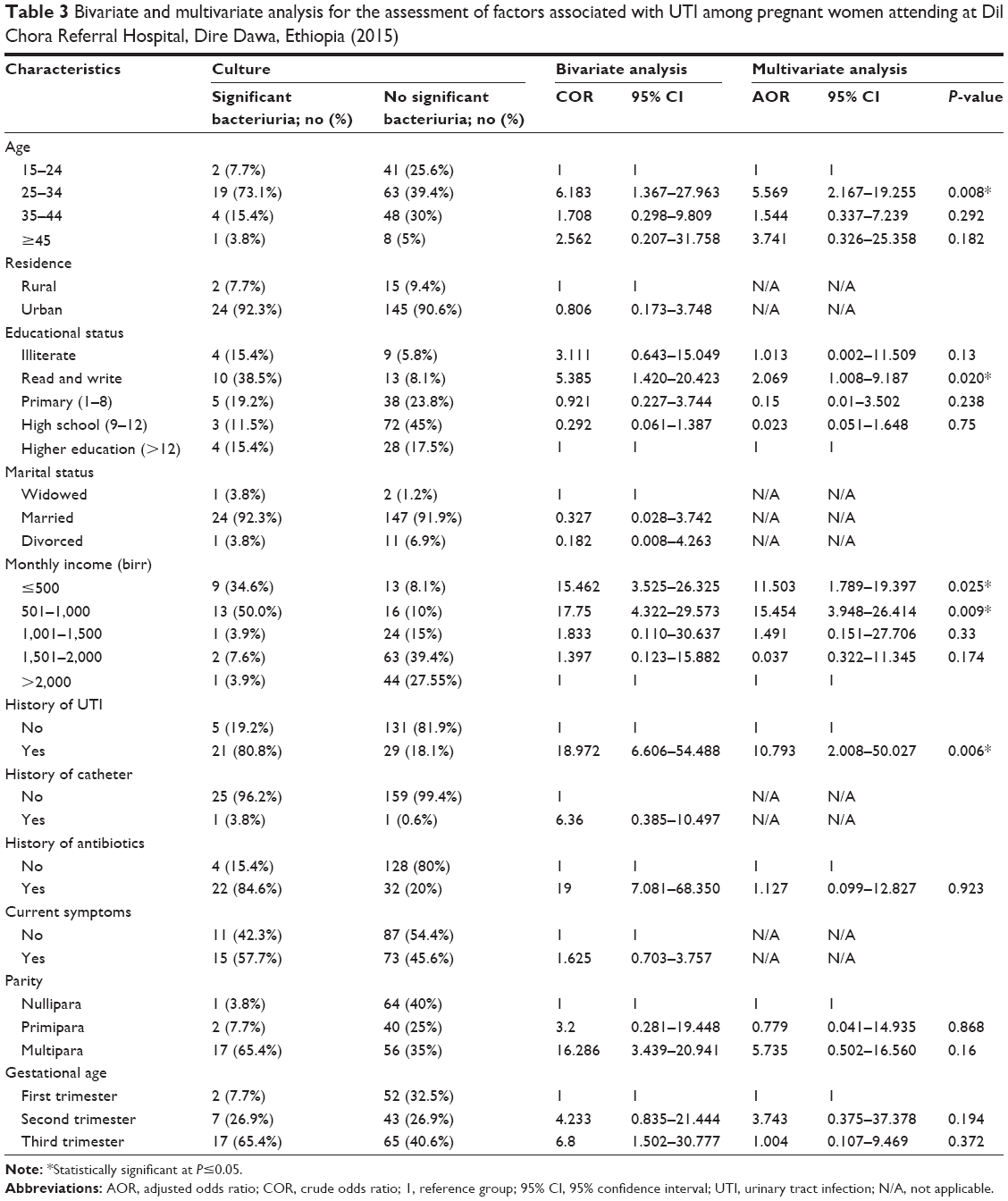 | Table 3 Bivariate and multivariate analysis for the assessment of factors associated with UTI among pregnant women attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia (2015) |
Antimicrobial susceptibility pattern
Gram-negative isolates showed a high level of sensitivity to CRO (94.7%), GEN (89.5%), and CIP (84.2%). Of these, E. coli in most clinical samples was highly sensitive to CRO (100%), GEN (100%), CIP (88.9%), SXT (88.9%), and C (77.8%). P. aeruginosa was sensitive to CRO (75%) and CIP (75%). But Gram-negative isolates showed a high-level resistance against AMP (89.5%), NA (52.6%), AMO (73.3%), and TTC (73.7%). However, it was relatively low resistant to SXT (36.8%), C (31.6%), and F (31.6%). E. coli was resistant to AMP (77.7%) and AMO (77.7%). P. aeruginosa was highly and fully resistant to AMP, SXT, C (75%), TTC (75%), F (75%), and NA (75%). Klebsiella species were fully (100%) resistant to AMP, AMO, and F, but they were 66.7% resistant to TTC, SXT, and C (Table 4).
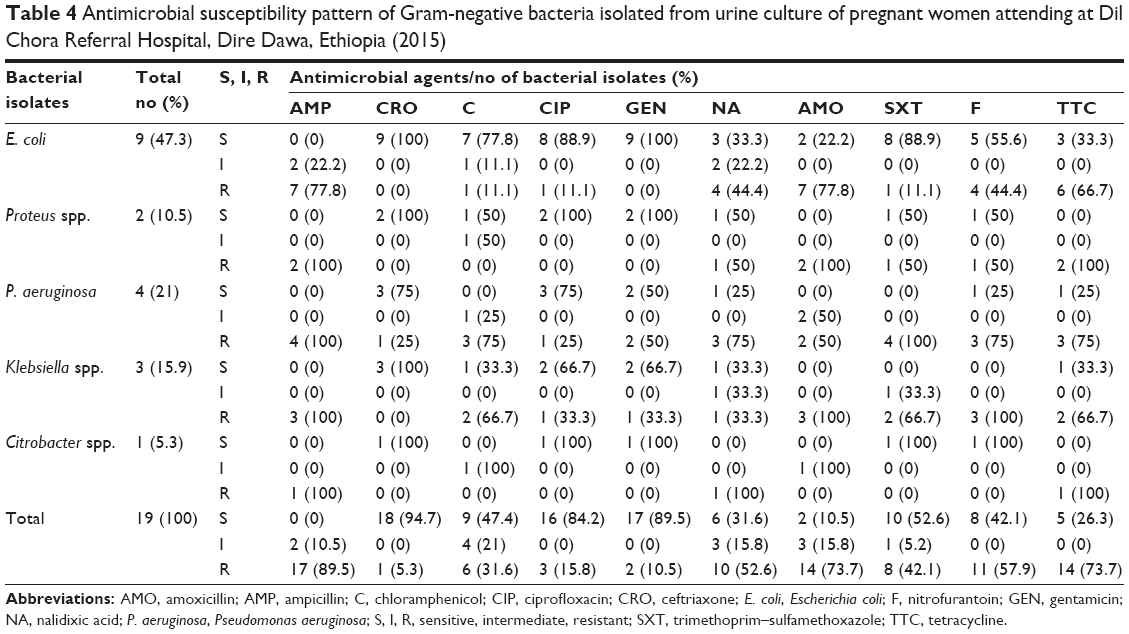 | Table 4 Antimicrobial susceptibility pattern of Gram-negative bacteria isolated from urine culture of pregnant women attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia (2015) |
Gram-positive isolates were highly susceptible to GEN (100%), ERY (85.7%), CRO (71.4%), CIP (71.4%), and F (71.4%) and resistant to AMP (87.5%), TTC (57.1%), and SXT (71.4%), while the low level of resistance (<30%) was observed in the remainder of the antimicrobials tested (ERY, CRO, CIP, and F). CONS, which were the predominant isolates, were highly resistant to AMP (80%) and SXT (80%; Table 5).
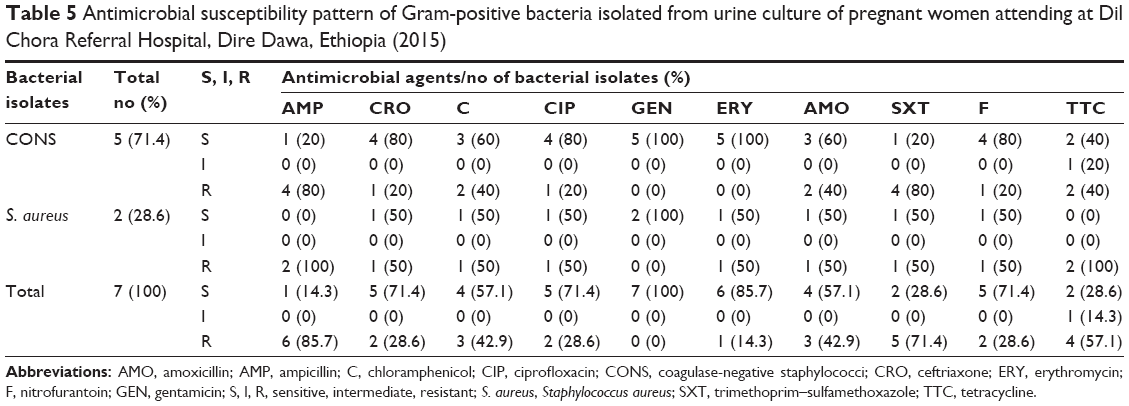 | Table 5 Antimicrobial susceptibility pattern of Gram-positive bacteria isolated from urine culture of pregnant women attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia (2015) |
Multidrug resistance (MDR = resistance in ≥2 drugs) was seen in 100% of the isolated bacterial uropathogens. MDR to two or more drugs was observed in all Gram-negative isolates (Table 6) and in Gram-positive bacteria isolates (Table 7). Three bacterial isolates Klebsiella spp., P. aeruginosa, and S. aureus were highly resistant to most of the antibiotics tested.
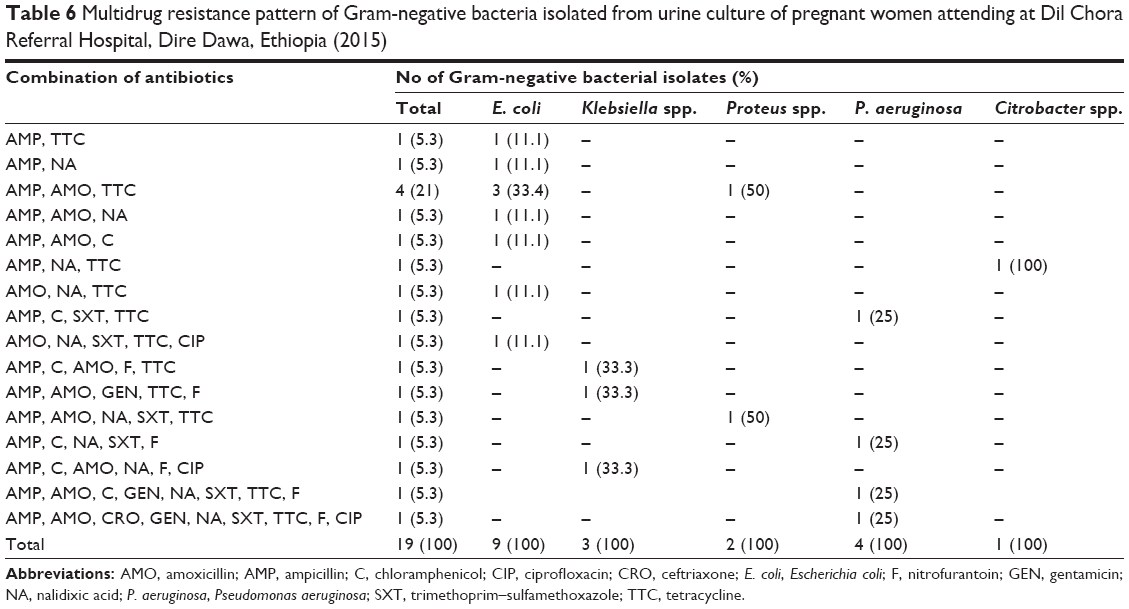 | Table 6 Multidrug resistance pattern of Gram-negative bacteria isolated from urine culture of pregnant women attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia (2015) |
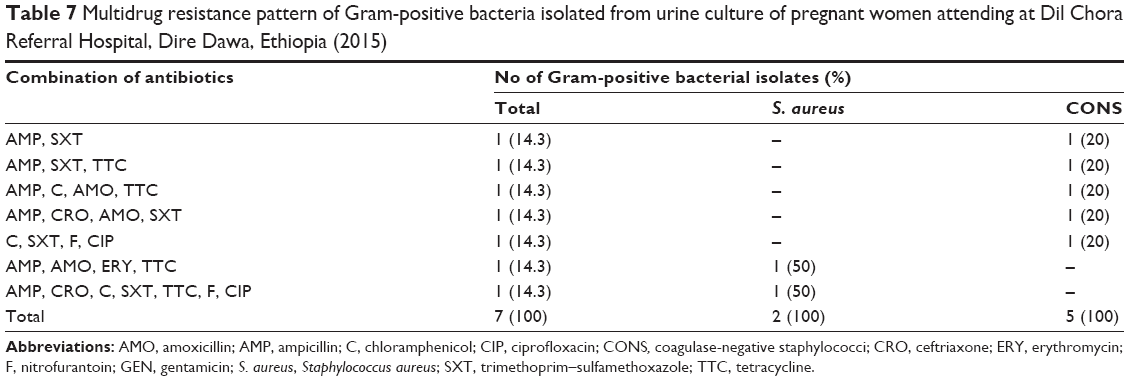 | Table 7 Multidrug resistance pattern of Gram-positive bacteria isolated from urine culture of pregnant women attending at Dil Chora Referral Hospital, Dire Dawa, Ethiopia (2015) |
Discussion
The overall prevalence of UTI was 14% in this study. This was similar to the prevalence of UTI reported from Sudan14 and Tanzania,13 but it was lower than reported from Niger,15 Libya,12 and Saudi Arabia.10 This finding was also relatively higher than the findings of a study performed in many parts of Ethiopia such as Addis Ababa,16 Gondar,17 and Bahir Dar.18 This variation in prevalence might be due to the difference in sample size and geographical location.
The prevalence of UTI was 17% among pregnant women with the symptoms of UTIs. This was comparable with the previous studies conducted in Addis Ababa (20%)16 and Tanzania (17.9%).13 It was relatively higher than the study performed in Gondar, Ethiopia (10.2%),17 Bahir Dar, Ethiopia (8.5%),18 Khartoum, Sudan (12.1%),14 and Makkah, Saudi Arabia (12%).10 The difference might be due to the small number of symptomatic pregnant women included in the later studies.10,14,17,18 However, the prevalence of UTIs was 11% among pregnant women without the symptoms of UTIs. This was similar to the findings reported from Addis Ababa (10.6%)16 and Tanzania (13%).13 This was lower than the study findings from Gondar, Ethiopia (15.9%),17 Bahir Dar, Ethiopia (18.9%),18 and Khartoum, Sudan (14.7%).14 The difference might be due to the large number of asymptomatic pregnant women included in the later studies.14,17,18
The majority of ethological agents of UTIs in this study were Gram-negative bacteria. A similar finding was found from other studies in Ethiopia and abroad.11,14,16–18 This could be due to the presence of unique structure in Gram-negative bacteria that help with the attachment to the uroepithelial cells and to prevent bacteria from urinary lavage, allowing for multiplication and tissue invasion resulting in invasive infection and pyelonephritis during pregnancy.36
E. coli (34.6%) was found to be the most frequent bacterial isolate in this study, which is inline with other reports from different areas.10,14,16,26 However, it was lower than reported in the previous studies conducted in different countries, which was 47.5% in Gondar,17 64.4% in Libya,12 50% in Afikpo, Ebonyi State,37 and 57.1% in Italy.24 E. coli is the most common microorganism in the vaginal and rectal area. Anatomical and functional changes and difficulty of maintaining personal hygiene during pregnancy might increase the risk of acquiring UTI by E. coli.38 The second most common isolate was CONS (19.2%), and the findings were also comparable with other studies conducted in Ethiopia, which was 16% in Addis Ababa,16 22.5% in Gondar,17 and 17.1% in Bahir Dar.18
In this study, the prevalence of UTI was higher in the age groups of 25–34 years. Similar findings have been reported in different studies.22,37 This might be due to women in this age group being more sexually active which might predispose them to UTI. Low-income status was another factor that was related with high prevalence of UTI among pregnant women. A similar finding was reported in other studies on pregnant women.9,18 This could be due to the relation of low socioeconomic status with nutrition and immunity especially in pregnant women. In addition, those pregnant women with the past history of UTI were highly affected by UTIs. This was similar to other studies.10,17,19 This might be due to the presence of resistance strains from those who had the previous history of UTI. However, gestational age, marital status, parity, and residence were not significantly associated with the prevalence of UTI in pregnant women. This was in agreement with studies conducted in Ethiopia,17,19 Sudan,14 and Tanzania,13 but it was not in agreement with a study conducted in Kenya and Nigeria, where the gestational age was significantly associated with the prevalence of UTI in pregnant women.22,39
Knowledge on antimicrobial susceptibility pattern of UTI pathogens was very important for clinician to select and use the best effective antimicrobial agent for the treatment of patient with UTI.16,40 In this study, CRO showed 94.7% sensitivity to Gram-negative bacteria isolates. The finding of this study was similar to the previous findings in Ethiopia, which was 96.3% in Gondar. The high sensitivity pattern for CRO might be due to the drug being less likely to be purchased without prescription in the study area. In this study, GEN had a sensitivity of 89.5%. This is in-line with the report of 87.7% in Gondar26 and in Addis Ababa it was slightly lower than reported, that is, 93.3%.16 Ciprofloxacin had a sensitivity of 84.2% in this study. This was lower than 96.3% sensitivity report from Gondar.17 On the other hand, Gram-negative isolates showed resistance against commonly prescribed drugs: AMP (89.5%), amoxicillin (73.7%), TTC (73.7%), NA (52.6%), and nitrofurantoin (57.9%). Similar findings have been reported from previous studies in Ethiopia17,18,26 and Iran.38 There was a high prevalence of UTIs reported among pregnant women who previously used antibiotics. This observed resistance to the abovementioned common antibiotics might be due to the earlier exposure of the isolates to these drugs. The abovementioned drugs are with low cost and often can be purchased without prescription in different areas. An irrational and unnecessary use of antibiotics can result in the emergence of bacterial strains that exhibit MDR.41 Among the Gram-negatives, the predominant isolate was E. coli, which is resistant to AMP and AMO (77.8%); NA and F (44.4%); and TTC(66.7%). With the exception of F this was consistent with findings in other studies.13,17,18,42
Gram-positive bacteria were relatively susceptible to GEN (100%), CRO (71.4%), CIP (71.4%), and ERY (85.7%), which was also in agreement with the findings of other studies.16–18 However, it is in contrast to the previous study that reported from India.11
In this study, MDR was seen in 100% of the isolated bacteria. This was higher than the 95% MDR reported in the University of Gondar teaching hospital study18 and higher than the 74% MDR reported in the study from Tikur Anbessa Specialized Hospital Addis Ababa, Ethiopia.16 This indicates that MDR was found to be very high in this study. Antibiotic resistance has been recognized as the consequence of repeated antibiotic use and abuse.43 The reasons for this alarming phenomenon might be due to inappropriate and incorrect administration of antimicrobial agents in empiric therapies.
Conclusion
The overall prevalence of UTI was 14% among pregnant women. It was higher among pregnant women with symptoms than those without symptoms. E. coli (34.6%), CONS (19.2%), P. aeruginosa (15.4%), and Klebsiella spp. (11.5%) were common bacterial isolates. Low-income level, past history of UTI, educational status, and age of pregnant women with 25–34 years were highly likely to be affected by UTI. Gram-negative isolates showed a high level of sensitivity to CRO, GEN, and CIP. However, Gram-positive isolates were highly sensitive to GEN, ERY, CRO, CIP, and F. Most of the bacterial isolates are resistant against the available commonly used antibiotics such as AMP, AMO, TTC, SXT, and C. MDR was seen in 100% of the isolated bacteria. The majority of bacterial isolates were sensitive to CIP, CRO, ERY, and GEN. Therefore, the empirical antibiotic selection should be based on the knowledge of the local prevalence of bacterial organisms and antibiotic sensitivities rather than on universal guidelines. This study recommends that the early detection of causative agent of UTI and determining their drug susceptibility pattern in pregnant women will help to ensure adequate treatment of UTI and to prevent its further complication in mother and fetus. Health information dissemination about causes of UTI and drug use should be given to pregnant women. CIP, CRO, GEN, and ERY can be used for the empirical treatment of UTI when there is no facility of taking culture and drug susceptibility tests in their areas. However, it should be used with great care to reduce further emergence of drug resistance.
Acknowledgments
We are grateful to the study participants. The study was financially supported by the College of Health and Medical Sciences, Haramaya University, and Dire Dawa City Administration Health Bureau.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Dielubanza EJ, Schaeffer AJ. Urinary tract infections in women. Med Clin North Am. 2011;95(1):27–41. | ||
Park K. Infectious disease. In: Park K, Bhankot B, editors. Park’s Test Book of Preventive and Social Medicine. 18th ed. Jabalpur: Banarsidas Bhanot Publications; 2005:311–315. | ||
Bacak SJ, Callaghan WM, Dietz PM, Crouse C. Pregnancy-associated hospitalizations in the United States. Am J Obstet Gynecol. 2005;192(2):592–597. | ||
Njoku CO, Ezissi NH, Amandi AN. Observations on bacterial infection of urinary tract patients. Int J Environ Health Hum Dev. 1998;13(2):785–791. | ||
Colgan R, Nicolle LE, Mcglone A. Asymptomatic bacteriuria in adults. Am Fam Physician. 2006;74:985–990. | ||
Ullah MA, Barman A, Siddique MA. Prevalence of asymptomatic bacteriuria and its consequences in pregnancy in a rural community of Bangladesh. Bangladesh Med Res Counc Bull. 2007;33:60–64. | ||
Nandy P, Thakur AR, Ray CS. Characterization of bacterial strains isolated through microbial profiling of urine samples. On Line J Biol Sci. 2007;7:44–51. | ||
Mazor DE, Levy A, Schlaeffer F, Scheiner E. Maternal urinary tract infection, it is independently associated with adverse pregnancy out come. J Matern Fetal Neonatal Med. 2009;22(2):124–128. | ||
Haider G, Zehra N, Afroze Munir A, Haider A. Risk factors of urinary tract infection in pregnancy. J Pak Med Assoc. 2010;60:213–216. | ||
Hani SF, Ahmed MA, Ghada AAE, Ahmad KA, Amr MM. Urinary tract infections among pregnant women in Makkah, Saudi Arabia. Biomed Pharma J. 2013;6(1):01–07. | ||
Shazia PS, Sharada VR, Rama RMV, Janardhan RR. Uropathogens and their drug susceptibility patterns among pregnant women in a teaching hospital. Ann Biol Res. 2011;2(5):516–521. | ||
Tamalli M, Bioprabhu S, Alghazal MA. Urinary tract infection during pregnancy at Al-khoms, Libya. Int J Med Med Sci. 2013;3(5):455–459. | ||
Masinde A, Gumodoka B, Kilonzo A, Mshana SE. Prevalence of urinary tract infection among pregnant women at Bugando medical center Mwanza. Tanzan J Health Res. 2009;11(3):154–161. | ||
Hamdan ZH, Abdel HMZ, Salah KA, Ishag A. Epidemiology of urinary tract infections and antibiotics sensitivity among pregnant women at Khartoum North Hospital. Ann Clin Microbiol Antimicrob. 2011;10:2. | ||
Adabara NU, Momoh JA, Bala JD, Abdurrahman AA, Abu-Bakr MB. The prevalence of bacterial urinary tract infections (UTI) among women attending antenatal clinic in the general hospital, Minna in Niger state. Int J Biomed Res. 2012;3(03):171–173. | ||
Assefa A, Asrat D, Woldeamanuel Y, G/Hiwot Y, Abdella A, Melese T. Bacterial profile and drug susceptibility pattern of urinary tract Infection in pregnant women at Tikur Anbessa hospital. Ethiop Med J. 2008;46(3):227–235. | ||
Alemu A, Moges F, Shiferaw Y, et al. Bacterial profile and drug susceptibility pattern of urinary tract infection in pregnant women at University of Gondar teaching hospital, in Northwest Ethiopia. BMC Res Notes. 2012;5:197. | ||
Tazebew D, Getenet B, Selabat M, Wondewsen T. Urinary bacterial profile and antibiotic susceptibility pattern among pregnant women in Northwest Ethiopia. Ethiop J Health Sci. 2012;22(2):121–128. | ||
Tazebew E, Getenet B, Wondewosen T, Silabat M. Associated risk factors of urinary tract infection among pregnant women at Felege Hiwot referral hospital, Bahir Dar, Northwest Ethiopia. BMC Res Notes. 2013;6:292. | ||
Kibret M, Abera B. Prevalence and antibiogram of bacterial isolates from urinary tract infection at Dessie Health Research Laboratory, Ethiopia. Asian Pac J Trop Biomed. 2014;4(2):164–168. | ||
Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183(1):S1–S4. | ||
Ade-Ojo I, Oluyege A, Adegun PT, Akintayo A, Aduloju O, Olofinbiyi B. Prevalence and antimicrobial susceptibility of asymptomatic significant bacteriuria among new antenatal enrollees in Southwest Nigeria. Int Res J Microbiol. 2013;4(8):197–203. | ||
El-Astal Z. Bacterial pathogens and their antimicrobial susceptibility in Gaza Strip, Palestine. Pak J Med. 2005;20(4):365–370. | ||
de Francesco MA, Guiseppe R, Laura P, Ricardo N, Nino M. Urinary tract infection in Brescia, Italy: etiology of uropathogens and antimicrobial resistance of common uropathogens. Med Sci Monit. 2007;13:136–144. | ||
Abubakar EM. Antimicrobial susceptibility pattern of pathogenic bacteria causing urinary tract infections at the specialist hospital, Yola, Adamawa State, Nigeria. J Clin Med Res. 2009;1(1):001–008. | ||
Ferede G, Yismaw G, Wondimeneh Y, Sisay Z. Prevalence of antimicrobial susceptibility pattern of bacterial UTI isolates from pregnant women. Eur J Exp Biol. 2012;2(5):1497–1505. | ||
Taneja N, Rao P, Arora J, Dogra A. Occurrence of ESBL and Amp-C beta-lactamases susceptibility to newer antimicrobial agents in complicated UTI. Ind J Med Res. 2008;127(1):85–88. | ||
Dire Dawa City Administration Annual Report of 2013/2014. | ||
Cheesebrough M. District Laboratory Practice in Tropical Countries Part II. 2nd ed. London: Cambridge University Press; 2006:105–114. | ||
Baron EJ, Peterson LR, Finegold SM. Bailey and Scott’s Diagnostic Microbiology. 9th ed. St Louis: Mosby; 1994:249–257. | ||
Forbes BA, Sahm DF, Weissfeld AS, editors. Infections of the Urinary Tract. In Bailey and Scott’s Diagnostic Microbiology. 11th ed. Philadelphia, PA: Mosby; 2002:927–938. | ||
Bauer AW, Kirby WMM, Sherris JC, Turk M. Antibiotic susceptibility testing by a standardized single disc method. Am J Clin Pathol. 1966;45:493–496. | ||
National Committee for Clinical Laboratory Standards (NCCLS). Performance Standards of Antimicrobial Susceptibility. NCCLS Approved Standard M100-59. Wayne, PA: National Committee for Clinical Laboratory Standard; 2002. | ||
Clinical Laboratory Standard Institute (CLSI). Performance Standard for Antimicrobial Susceptibility Testing; Twentieth Informational Supplement. CLSI Document M100-S20. Vol. 30. Wayne, PA: Clinical and Laboratory Standards Institute; 2010:48–51. | ||
Clinical Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Fourth Informational Supplement. CLSI Document M100-S24. Vol. 34. Wayne, PA: Clinical and Laboratory Standards Institute; 2014:50–57. | ||
Amiri FN, Rooshan MH, Ahmady MH, Soliamani MJ. Hygiene practices and sexual activity associated with urinary tract infection in pregnant women. East Mediterr Health J. 2009;15:105–108. | ||
Onuoha SC, Fatokun K. Prevalence and antimicrobial susceptibility pattern of urinary tract infection (UTI) among pregnant women in Afikpo, Ebonyi State, Nigeria. Am J Life Sci. 2014;2(2):46–52. | ||
Ali JM, Gholamreza I. Asymptomatic urinary tract infection in pregnant women. Iran J Pathol. 2009;4(3):105–108. | ||
Wamalwa P, Omolo J, Makokha A. Prevalence and risk factors for urinary tract infections among pregnant women. Prime J Soc Sci. 2013;2(12):524–531. | ||
Mohammad M, Mahdy ZA, Omar J, Maan N, Jamil MA. Laboratory aspects of asymptomatic bacteriuria in pregnancy. Southeast Asian J Trop Med Public Health. 2002;33:575–580. | ||
Wolday D, Erge W. Increased incidence of resistance to antimicrobials by urinary pathogens isolated at Tikur Anbessa Hospital. Ethiop Med J. 1997;35:127–135. | ||
Okonko IO, Ijandipe LA, Ilusanya OA. Incidence of urinary tract infection (UTI) among pregnant women in Ibadan, South-Western Nigeria. Afr J Biotechnol. 2009;8:6649–6657. | ||
Albrich WC, Monnet DL, Harbarth S. Antibiotic selection pressure and resistance in Streptococcus pneumoniae and Streptococcus pyogenes. Emerg Infect Dis. 2004;38:363–371. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.