Back to Journals » Clinical Optometry » Volume 17
Availability of Eye Care Services and Management Strategies for Ocular Conditions in the uMgungundlovu District, KwaZulu-Natal
Authors Mosololi R ![]() , Sukati V, Nkoana P
, Sukati V, Nkoana P ![]()
Received 29 May 2025
Accepted for publication 11 September 2025
Published 28 November 2025 Volume 2025:17 Pages 383—397
DOI https://doi.org/10.2147/OPTO.S543461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Rorisang Mosololi, Velibanti Sukati, Pheagane Nkoana
Department of Optometry, University of Limpopo, Polokwane, South Africa
Correspondence: Rorisang Mosololi, University of Limpopo, C/O R71 Tzaneen Road and University Street, Mankweng Township, Polokwane, Limpopo, 0727, South Africa, Tel +27781126388, Email [email protected]
Purpose: Many ocular conditions that lead to blindness or visual impairment are preventable or treatable with early diagnosis and timely access to eye care. However, individuals in low-income areas often encounter significant barriers. This study assessed eye care management strategies and facility availability for patients in the uMgungundlovu district.
Methods: A cross-sectional, descriptive, quantitative, and retrospective study was conducted using an online questionnaire and record card reviews to assess management strategies in selected public eye care facilities in uMgungundlovu from January to December 2022. Cluster sampling across 27 facilities was employed. Data were analyzed with the Statistical Package for the Social Sciences (SPSS), with descriptive statistics presented in graphs and tables. Significant differences in optometrist prescribing patterns were identified, with a p-value of less than 0.05 considered statistically significant.
Results: A total of 1397 record cards were reviewed from seven facilities. Most patients received spectacles (n = 741, 53%), but 12.5% (n = 174) took six months or longer to receive them, and 12% (n = 167) did not receive them at all. Primary facilities occasionally supplied eye drops, requiring referrals to secondary hospitals for ongoing treatment. Statistically significant differences in optometrist prescribing patterns were found for spectacles (p = 0.039) and pharmaceutical treatments (p < 0.001) between primary and secondary care levels. Six out of seven representatives (85.7%) indicated that facilities lacked adequate ophthalmic equipment and qualified professionals. None of the facilities conducted data analysis, resulting in insufficient evidence-based information for planning.
Conclusion: The district faces healthcare access and management gaps. With 84% of the population relying on public services, a comprehensive eye care model (CEC) is essential for equitable access.
Keywords: accessibility, level of care, human resources, optometrists
Introduction
Eye care is a vital aspect of universal health coverage and is crucial for delivering Integrated People-Centered Eye Care (IPEC) services. These services should be coordinated across various levels of care, focus on individuals throughout their life course, and offer a comprehensive range of treatments.1 To ensure accessibility to eye care, it is essential to implement multiple strategies that consider the complexities of different settings.2 The Comprehensive Eye Care Model (CEC) aims to provide accessible and affordable eye care services, focusing on prevention, treatment, and rehabilitation for various conditions.3 It entails eye health promotion, disease diagnosis, and equitable service provision across diverse populations, regardless of complexity or cost.3
Globally, only about 36% and 17% of individuals with distance vision impairment due to refractive errors (RE) and cataracts, respectively, have access to the appropriate interventions.4 Over 90% of those with visual impairment suffer from preventable or treatable conditions, despite the availability of highly cost-effective interventions such as cataract surgery and corrective spectacles in many countries,4 highlighting the need for early detection and effective treatments to prevent avoidable blindness. Blindness and visual impairment (VI) in low- and middle-income countries, particularly in sub-Saharan Africa, are often attributed to low optometry-to-patient ratios. Over 90% of optometrists work in the private sector, serving only 16% of the population, which leaves the public sector struggling to meet demand. Factors such as uncorrected refractive errors, limited resources, inadequate facilities, and restricted access to eye care contribute to high rates of VI.5 In low-income areas, distance vision impairment is four times more common, and more than 80% of near vision issues remain unaddressed6 Rural regions are especially impacted by the shortage of eye care practitioners, resulting in increased preventable vision loss.
In South Africa, 0.9% of the population experiences vision impairment and blindness, with 84% relying on the public health sector. However, inadequate access to affordable services remains a significant barrier to comprehensive eye care for all.7 Furthermore, accessibility and affordability significantly impact the use of ophthalmic services, particularly in low-income countries.8 The effects of these factors are evident in South Africa, where indigenous populations face barriers to accessing eye care services due to limited facilities in rural areas, long waiting times, and a general ignorance about eye health.9 Gordon et al10 found that individuals with greater financial means are more likely to live within 10 kilometres of eye care facilities, whereas poorer communities often reside much farther away. This distance, coupled with travel costs and time constraints, reduces health service utilization among disadvantaged groups. These findings underscore the urgent need for cost-effective outreach eye care models to ensure equitable access to eye care services, particularly in underserved communities where a larger number of individuals are likely to report visual impairment (VI) disabilities.11
The province of KwaZulu-Natal is reported to have the highest prevalence of vision loss in South Africa at 17.6%, yet it faces significant challenges in resource allocation for comprehensive eye care. Eye care facilities struggle to provide spectacles and essential medications, resulting in treatment delays that can worsen the prognosis of eye diseases.12 The uneven distribution of eye health professionals, particularly in the public sector, insufficient program evaluations, and long waiting times for cataract surgeries exacerbate the situation. Furthermore, the public health sector is experiencing a notable exodus of eye health practitioners due to inadequate resources that hinder the provision of comprehensive care while managing large patient populations.13 The uMgungundlovu district, mainly rural, has a limited number of optometrists who are concentrated in urban areas, leading to long waiting periods of over a month for patients seeking eye health services. Additionally, the limited number of optometrists employed in the district, who are expected to provide outreach services to improve access for a significant population dependent on public eye health services, complicates the ability to conduct thorough and consistent program evaluations for future planning. Anecdotal evidence suggests that there is a lack of optical devices and medications, inadequate infrastructure, and a significant lack of data on commonly prevalent ocular conditions, along with supply chain delays, negatively impacting patient outcomes. To address these challenges, it is essential to align the eye health workforce planning with the epidemiology of eye diseases and assess the availability of resources, such as equipment necessary for the examination, diagnosis, and management of prevalent conditions within the uMgungundlovu district for effective patient care in the uMgungundlovu district.14 Consequently, this study seeks to identify the availability of eye care facilities and services as well as the strategies, practices, and methods employed in managing ocular conditions in the uMgungundlovu district of KwaZulu-Natal Province, South Africa.
Methods
Study Design
Study design is illustrated in Figure 1.
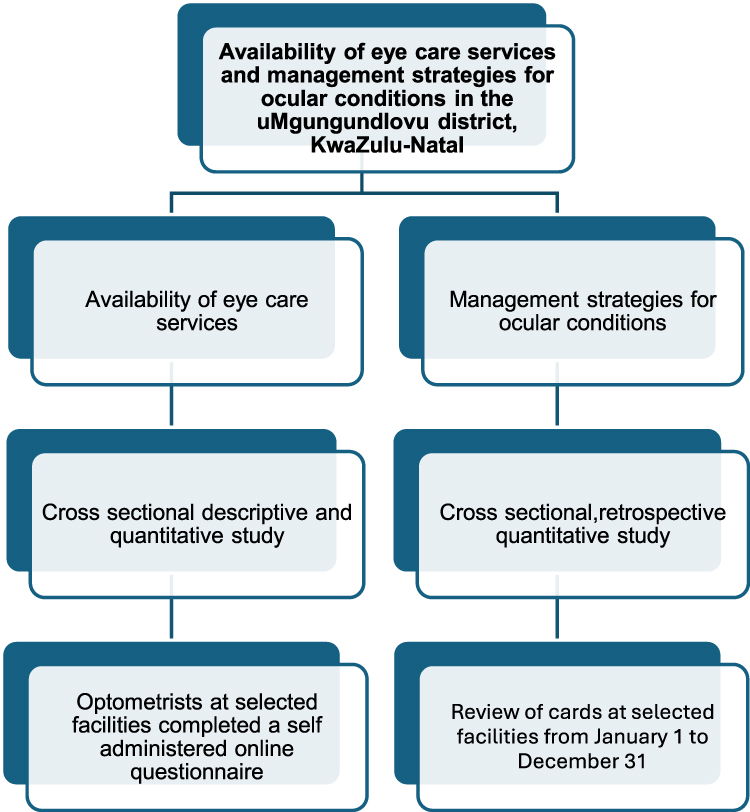 |
Figure 1 The flow diagram illustrating the study design. |
Setting
The study was conducted at seven selected public facilities providing eye care services within the uMgungundlovu health district. This district is one of eleven in KwaZulu-Natal, situated in the Midlands, and caters to approximately 10% of the population in the province.15 The district encompasses seven municipalities: Msunduzi, Mpofana, Mshwati, Impendle, Mkhambathini, Umgeni, and Richmond, with Msunduzi being the only municipality characterized by an urban profile. Figure 2 shows the map of the uMgungundlovu district, the distribution of optometrists, and the population in each municipality.
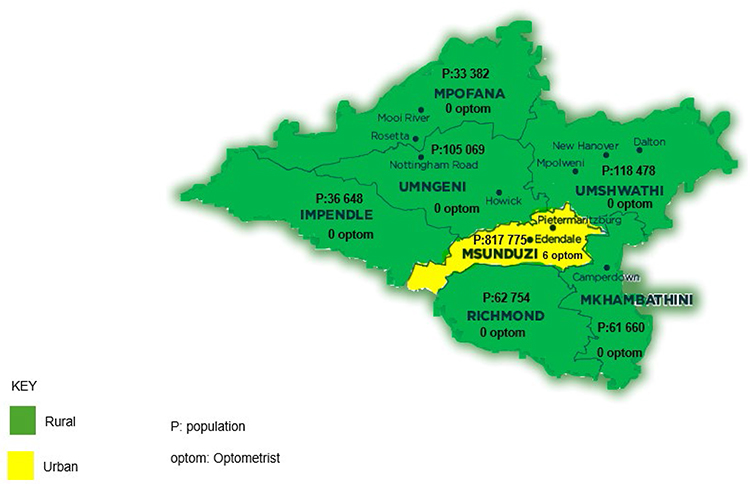 |
Figure 2 The map of the uMgungundlovu district. |
Study Population
A total of six optometrists in the uMgungundlovu district provide eye care services in hospitals and visit Community Health Care Centers (CHCs) and clinics. In line with the availability of eye care services, the study population included all eye clinic managers who were optometrists, or all optometrists nominated as representatives in each selected facility for completing clinical facility assessment questionnaire. All representatives (7) from selected facilities completed the questionnaire.
For management strategies, the population consisted of medical records from patients at selected eye clinics (7) in public sector facilities within the uMgungundlovu district, covering the period from January 1, 2022, to December 31, 2022. Cluster sampling was performed across 27 eye care facilities, followed by random sampling of medical records. The population was categorized into four clusters, with one facility sampled from each of the first three clusters: regional and tertiary hospitals, district hospitals, and community health clinics. One clinic per municipality was selected from a total of 20, resulting in four clinics (PHC). The sample size was calculated using Slovin’s formula [n = N / (1 + Ne2)], where n represents the samples, N indicates the total population, and e denotes the error tolerance (0.05). The estimated sample size was 1394 medical records. Well-completed records were chosen through a randomized systematic sampling method, formulated as k = N/n, where k is the systematic interval, N is the population size, and n is the sample size. Sample sizes varied by category: for tertiary hospitals, every 9th record was selected; for district hospitals, every 4th record was chosen; and all completed cards were included for the primary level. In total, 1397 cards were reviewed.
Data Collection
An online piloted questionnaire was distributed by Email and WhatsApp only to selected participants to collect the requisite data on the availability of eye care services within the public sector in the district. The questionnaire used closed-ended questions and was adapted from existing literature,16,17 contextualised and verified by two supervisors. It had 11 sections: general Information, available human resources for eye health, facility structure, general daily duties, statistics, available services, clinical duties, equipment, administrative procedures, utilities, and challenges encountered by optometrists at the workplace. It was then piloted on three participants in KZN working outside the uMgungundlovu health district to ensure the clarity and relevance of the questions and was adjusted accordingly. The questionnaire was password-protected, and participants were requested to give consent before participating and not to share any details of the study. Medical records of patients were used to gather data on the management strategies used in the district. The researcher reviewed the patient records of all individuals who presented at the selected public eye care facilities from January to December 2022. The medical records of patients were screened for completeness, and only qualifying medical files were included in the selection criteria. The information was entered into the data sheet created based on previous studies14,18,19 and confirmed by two expert supervisors.
Data Analysis
Data was captured in Microsoft Excel 365 and exported to the Statistical Package for the Social Sciences (SPSS), version 29, for analysis. Descriptive statistics, including frequencies, percentages, and average values, were calculated. Data is presented in the form of graphs and tables. Significant differences in optometrist prescribing patterns were determined using an independent samples t-test, and the p-value < 0.05 was considered significant.
Ethical Considerations
Ethical clearance to conduct the study was obtained from the School of Health Care Sciences Research Committee (SREC) and then from the Faculty of Health Sciences for postgraduate standards and ethical guidance (PROPOSAL NO: FHDC2023/52), and Turfloop Research Ethics Committee (TREC) (TREC/1745/2023:PG) at the University of Limpopo. Permission to conduct the study was requested from the KZN Department of Health, under the Directorate of Health Research and Knowledge Management (NHRD Ref: KZ_202402_008), uMgungundlovu Health District, and facility managers.
Results
A 100% response rate from all the selected public eye care facility managers or representative personnel was achieved. Table 1 shows the population served, geographic location of the selected eye care public facilities, and their level of care. Out of the seven eye care facilities, five were rural-based, including four primary eye care clinics and one district hospital. The average population served by the selected facilities is 698,903 (65.5%) of the population in the uMgungundlovu district (Stats SA 2022).
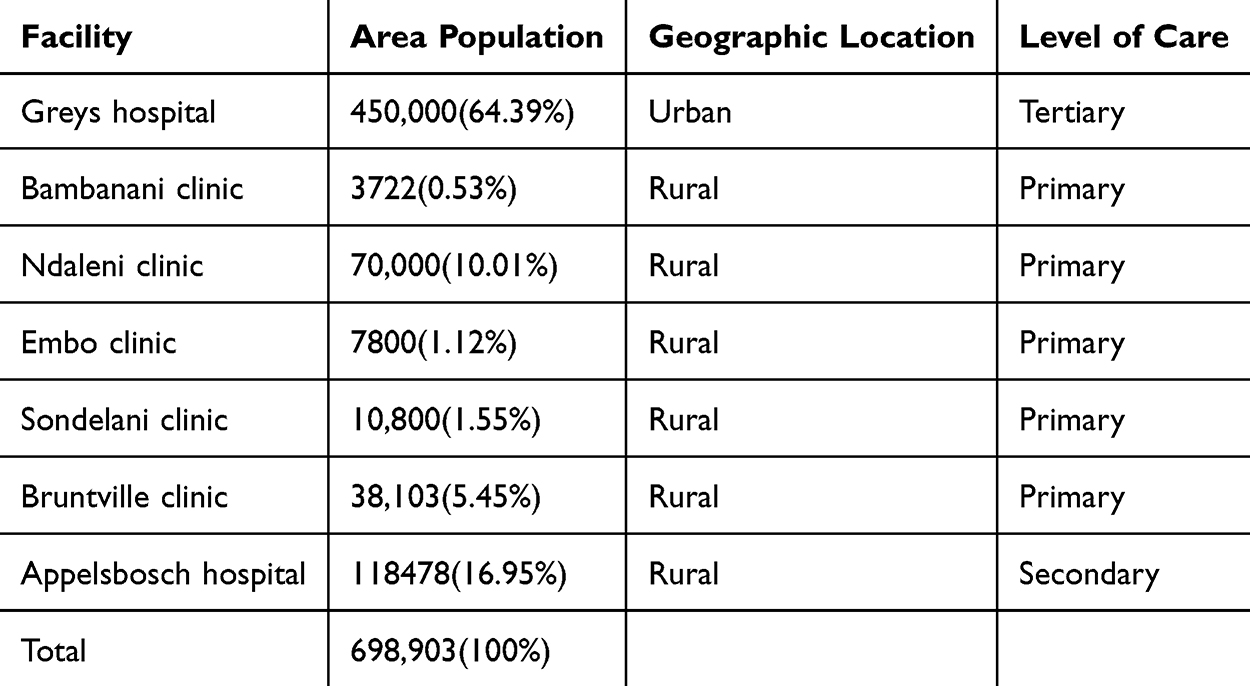 |
Table 1 Population Served, Geographic Location of Selected Facilities, and Their Level of Care |
Five facilities (71.4%), all at the primary level of care, had no stationed eye care professionals and received eye care services from a visiting optometrist who provided services twice a month. At the secondary level, one (14.3%) selected hospital had only one stationed ophthalmic nurse and a visiting optometrist who visited the hospital four times a month. At the tertiary level of care (14.3%), there were four stationed ophthalmologists, two ophthalmic medical officers, one optometrist, and four ophthalmic nurses.
Table 2 shows the required, available, and gaps in HReH categories in relation to WHO’s VISION 2020 minimum staff requirements for the 698,903-population served by the seven selected facilities. The rates for optometrists and ophthalmic nurses are 1.43 and 8.58, respectively, showing a shortage of 2 (66.67%) optometrists and (n=2) and 1 (14.29%) ophthalmic nurse.
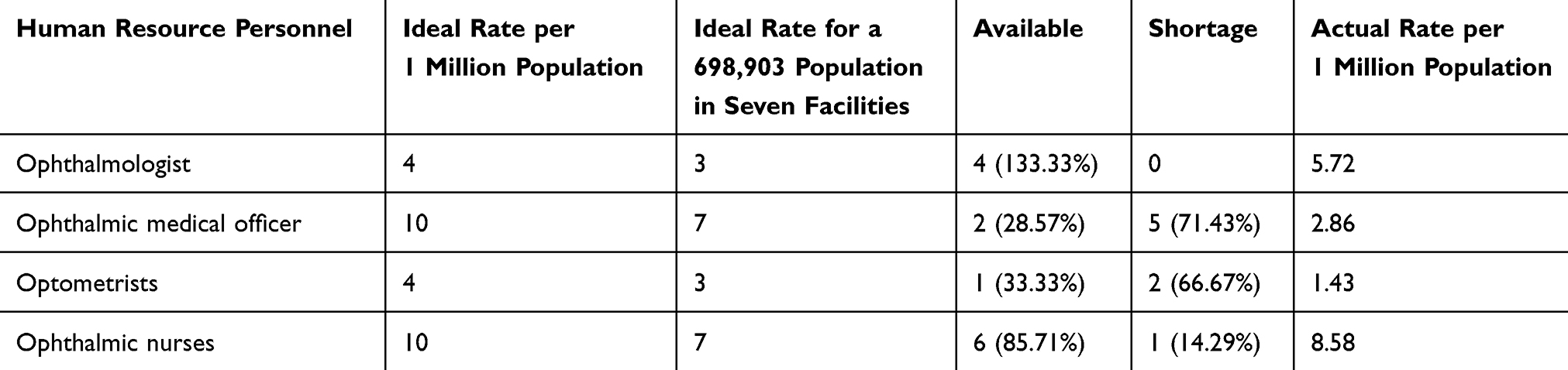 |
Table 2 HReH Ideal Rates for Low and High-Income Regions in Relation to the WHO, VISION 2020 |
Table 3 provides an overview of the availability and functionality of equipment at each selected facility, in accordance with the minimum requirements and additional recommendations set by the HPCSA. Six (85.7%) of the facilities did not have refraction equipment and no ophthalmic equipment audits were conducted. Four facilities (57.1%) did not have specific consultation rooms for eye care services. Two clinics, Bambanani and Embo, had non-functioning equipment and an absence of equipment, respectively.
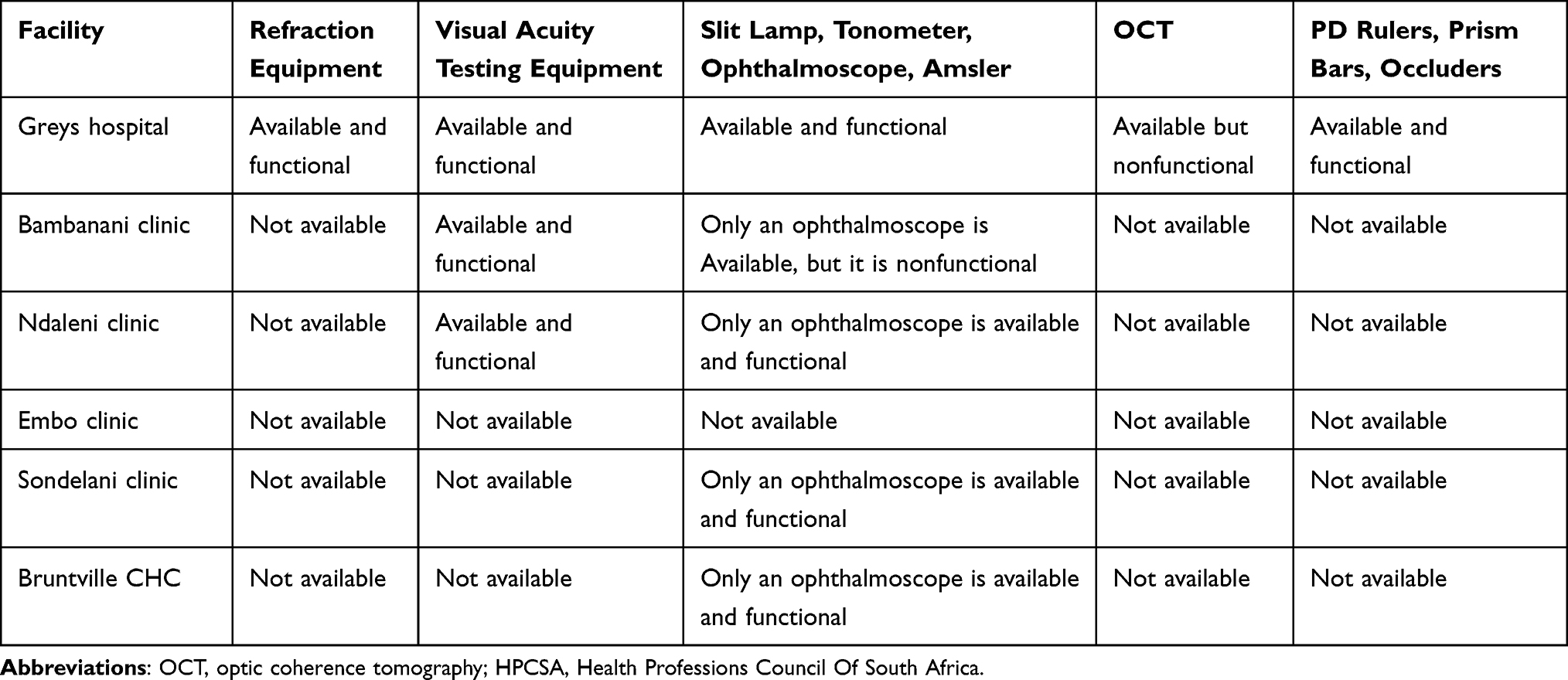 |
Table 3 Equipment Availability and Functionality for Eye Care Services as Guided by the HPCSA |
Representatives from all the facilities indicated that there were no equipment audits or maintenance. All facilities lacked a dispensing room specifically for eye care services. The gathered information in all the selected eye care facilities has not been analyzed despite the availability of registers. Ophthalmic nurses are responsible for filling registers in district (Appelsbosch) and tertiary (Greys) hospitals, while general nurses are tasked with this responsibility at primary level eye care facilities. Out of the seven facilities, only Grey’s Hospital is reported to be receiving reports from management for planning eye care services and stores eye clinic headcount statistics, as shown in Table 4. Table 4 provides an overview of record keeping and the utilization of information at each facility, in accordance with the policies set by the district health management information system (DHMIS).
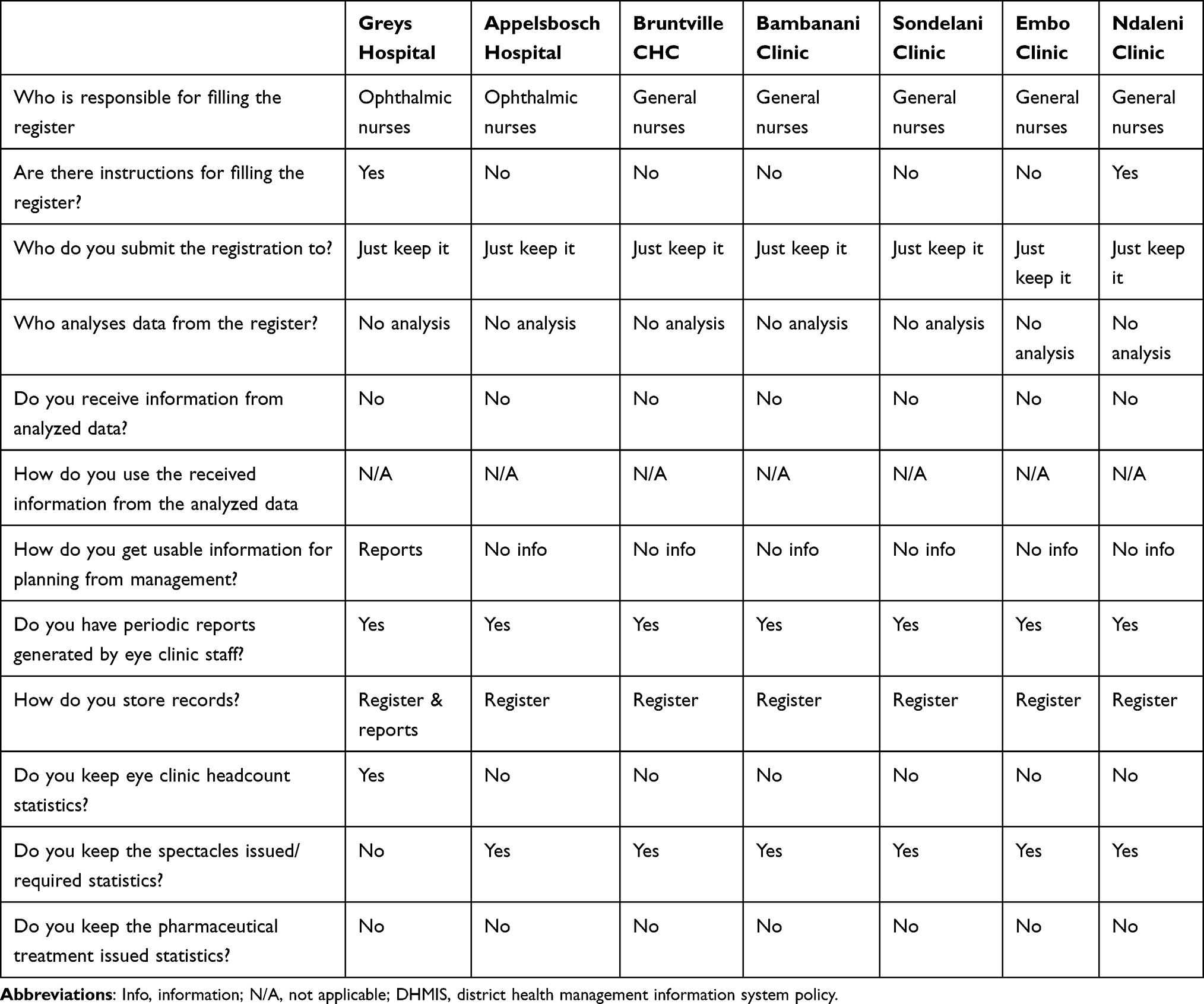 |
Table 4 Record Keeping and Information Use at Eye Care Facilities per DHMIS |
Participants indicated that diabetes and hypertension screening, pediatric vision screening, and routine eye tests for patients with chronic conditions were provided at all levels of care. Contact lens fitting services were only available at the tertiary level of care (Grey’s Hospital, 14.3%), while low vision services were not offered at any of the selected levels of facilities.
In a review of 1397 patient records from selected facilities in 2022, a notable 57% (801 patients) were seeking care for their initial eye examination. Conversely, 43% (596 patients) had previously undergone eye tests. Among those returning for follow-up examinations, more than half, specifically 375 patients, received care at the tertiary level, while the remaining 221 patients were treated at both primary and secondary care levels.
Among the patients undergoing their first eye exam, the majority were adults aged 40 years and older, making up 39% of the total, which equates to 538 individuals. This was followed by younger adults aged 19 to 39 years, who represented 10%, totaling 135 individuals. Children aged 6 to 18 years accounted for 8% of the patients, with 116 participants, while the smallest segment was the age group of 0 to 5 years, which constituted just 0.9% of the total, equating to 12 children. The time interval between the current and previous eye tests is illustrated in Figure 3, with 154 (11%) patients presenting in 0–6 months, and a few in 37 months or more.
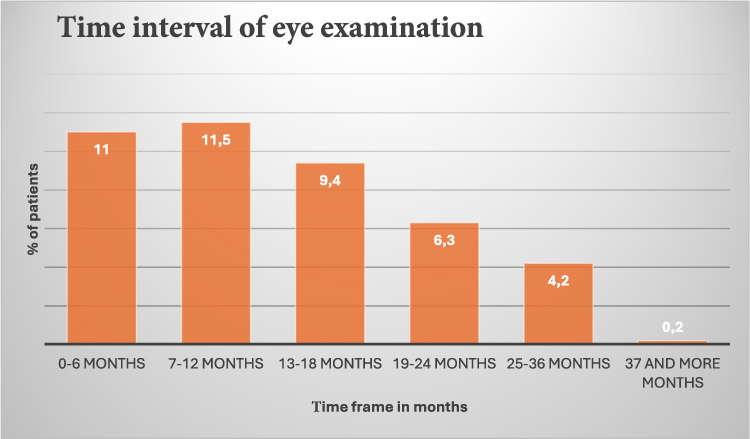 |
Figure 3 The time interval between the current and previous eye test. |
Refractive errors and cataracts were reported as the most prevalent conditions among patients at all selected facilities. Chart reviews indicated that 786 patients (55%) were diagnosed with refractive errors, while 279 patients (20%) had cataracts. Conjunctival disorders were also frequently observed, particularly in six facilities—five at the primary level and one at the secondary level of care—where 251 patients (18%) were diagnosed with this condition. Additionally, glaucoma was a common presenting condition at one tertiary care facility, with chart reviews showing that 84 patients (6%) were diagnosed with it. To manage these conditions, spectacles and pharmaceutical treatment were the most used (n=741, 53%) and (n=508, 38%) management strategies, respectively for refractive error and conjunctival disorders. Nine hundred and seventy-eight (70%) received the recommended management, while 167 (12%) did not. One hundred and seventy-four (12.5%) had to wait up to six months or more to receive their recommended spectacles. The study found significant differences in the prescribing practices of optometrists between primary and secondary levels of care. In primary care settings, the prescription of spectacles differed significantly, with a p-value of 0.039. In contrast, the prescribing of pharmaceutical treatments showed an even greater significance, with a p-value of less than 0.001. Tables 5 and 6 present additional findings on the ocular conditions, management strategies employed in the district, and funding allocation for spectacles, as well as strategies for accessing eye medication during stockouts in selected facilities, respectively.
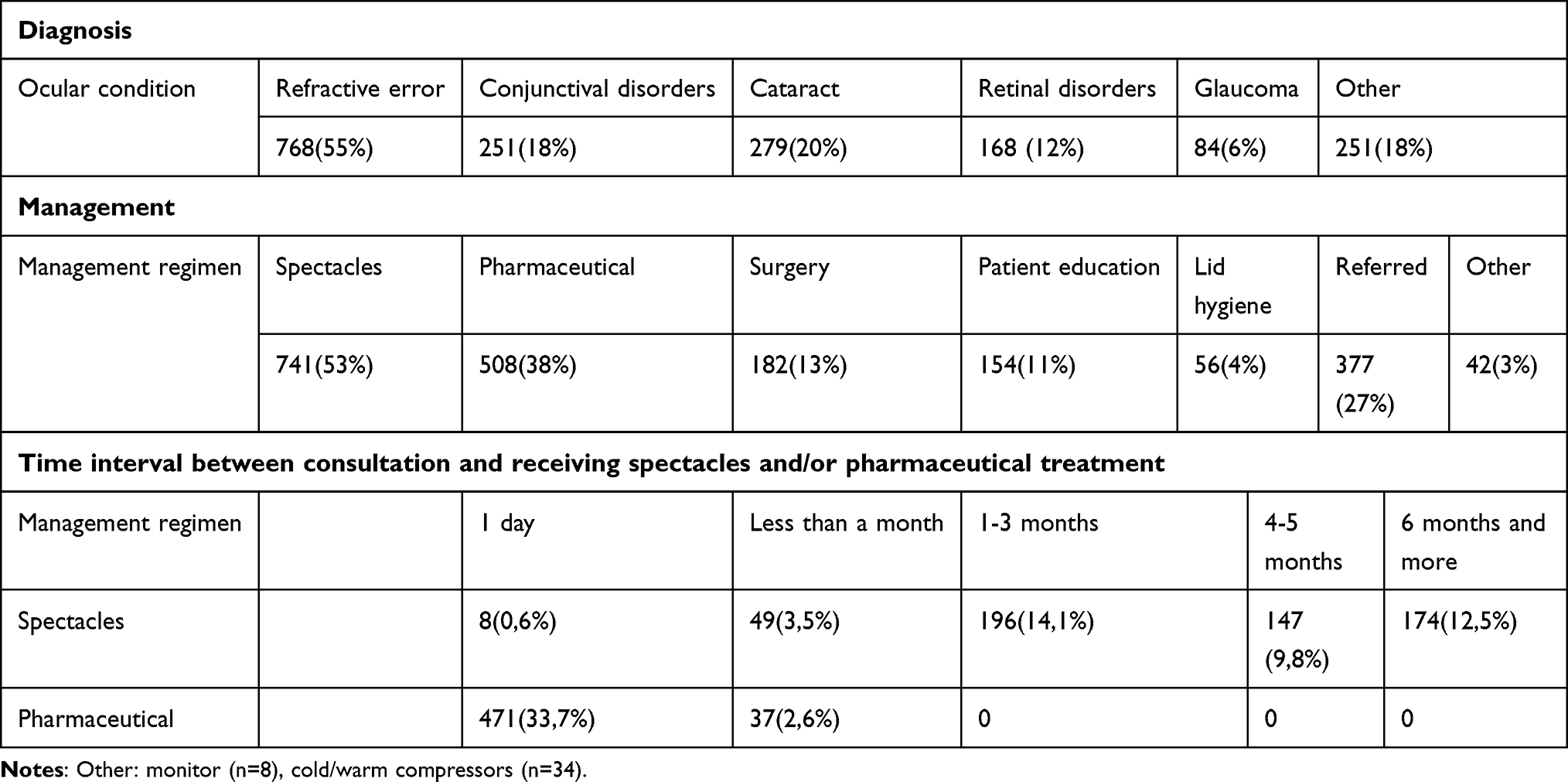 |
Table 5 Diagnosis and Management Strategies Utilised in the Selected Eye Care Facilities |
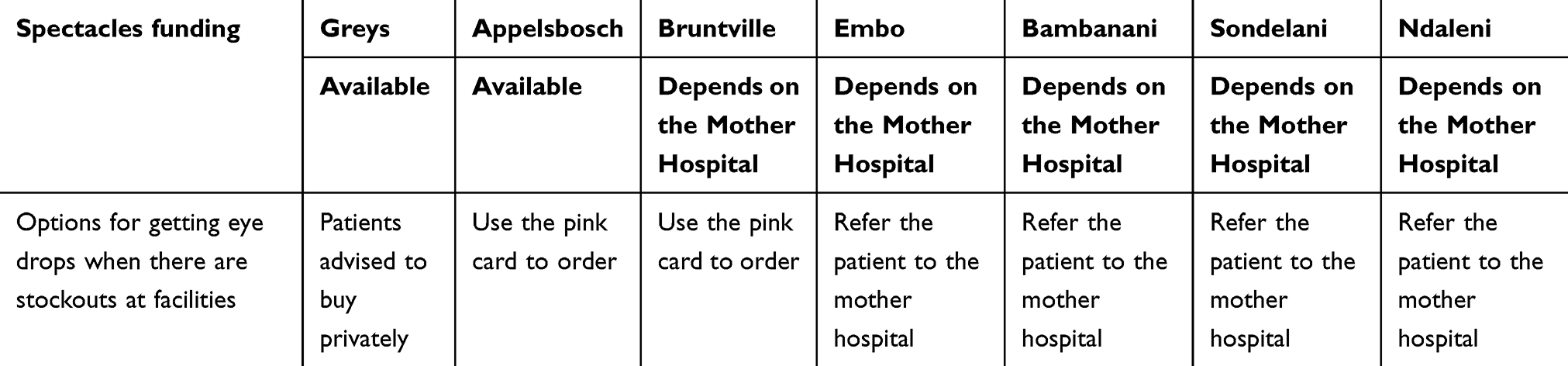 |
Table 6 Funding Allocation for Spectacles and Strategies for Accessing Eye Medication During Stockouts |
Figure 4 shows referral strategies for patients presenting to selected eye care facilities. Of the 377 referrals, referring to an ophthalmologist (n=240) and to a secondary hospital for pharmaceutical treatment (n=78) were the most common referrals.
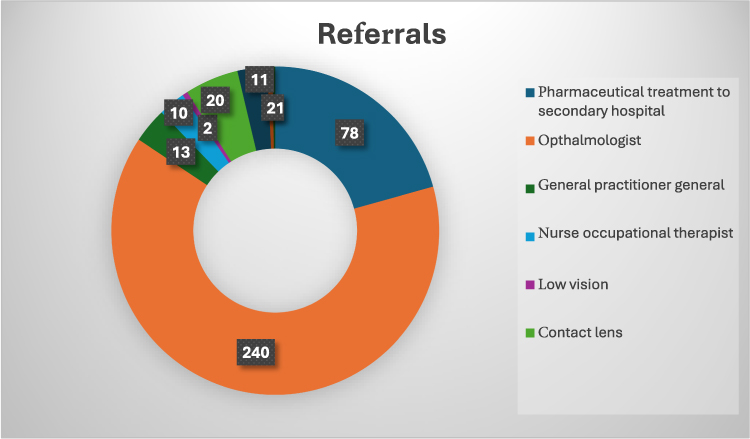 |
Figure 4 Referral strategies for patients presenting to selected eye care facilities. |
Participants from Greys Hospital, Appelsbosch Hospital, and Bruntville Clinic (42.86%) indicated staff shortages and increased workload. Only 4 (57.14%) primary eye care facilities reported experiencing a shortage of medication or no medication and having difficulties dispensing medication due to pharmacists refusing to dispense prescriptions, even though prescriptions are within the scope of optometry practice, as shown in Table 7.
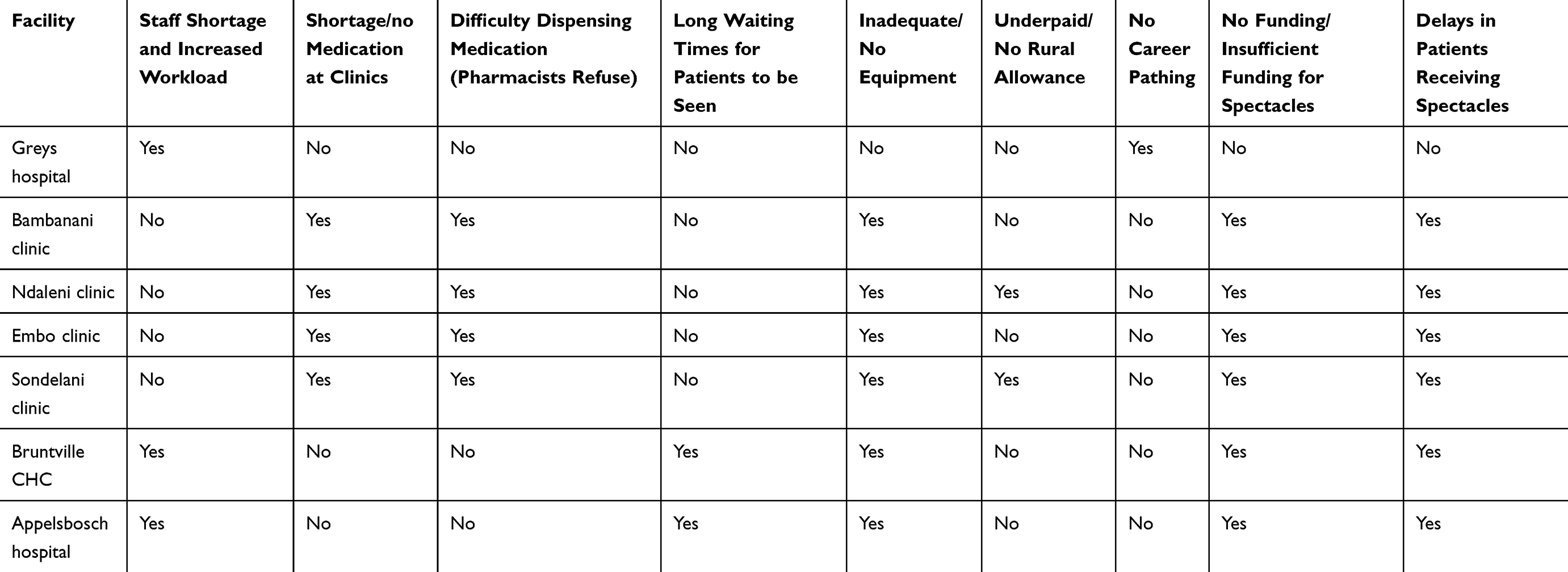 |
Table 7 Reported Difficulties Experienced by Optometrists at Selected Eye Care Facilities |
Discussion
The selected eye care facilities represent 5 of the 7 municipalities in the uMgungundlovu district, highlighting the availability and services offered, including the management strategies utilized for patients. The findings from selected facilities reveal gaps in the availability of eye care services in the different levels of care and different geographic locations in the district. This has a negative impact as it limits access to basic eye care services for the communities served. Literature20,21 indicated that despite having eye care facilities distributed in different geographic locations, accessibility remains a concern, especially in rural areas due to poor road infrastructure and limited transportation, which hinders access to clinics and limits mobility, particularly for older patients residing in rural communities. With the uMgungundlovu district being primarily rural, the experiences of patients accessing eye care services may be similar in the current study. Although eye care services are seldom provided on weekly basis as outreach to rural-based facilities, there is a need to improve service provision by availing human and working resources. This may be regarded as an improvement as the focus is on rural based clinics. This is in contrast to findings by Maake and Moodley18 who found that most optometrists in the public sector primarily catered to urban and semi-urban communities. The difference may be due to the geographic distribution of eye care facilities in KwaZulu-Natal.
Availability does not translate to automatic access as other factors may contribute to the inadequate use of eye care facilities such as lack of workforce and equipment. Only a tertiary facility situated in an urban area is adequately equipped in terms of working and human resources. This shows the continued disparity in eye care service provision at different levels of care and geographic distribution, attributable to the skewness of deployment of eye health care facilities. These findings align with reports from other low and middle-income countries21,22 Similar to the current study findings, Elam et al2 emphasized that the lack of stationed optometrists and ophthalmologists in under-resourced areas delays appropriate interventions, ultimately leading to poor prognosis. Furthermore, the reliance of optometry services in the district at primary and secondary levels of care while these are provided on a limited schedule, is also a cause for concern. Thompson et al23 cite that when eye services are provided on a limited schedule, it leads to delayed care, particularly for patients requiring more consistent management or follow-up, resulting in inconsistent and unreliable eye care for the population. These findings highlight the need for the uMgungundlovu district, supported by the Department of Health in the province, to invest in stationed eye care professionals, working resources, and improvement of infrastructure across various geographic locations to ensure accessible and available eye health for all. Furthermore, the district needs to accelerate the frequency of visits beyond twice a month to ensure timely and adequate care.
Based on the WHO recommended human resources rates for ophthalmic medical officers, ophthalmic nurses and optometrists, the district has not met these targets to serve the district population and characterized by skewness in distribution. Similarly, Hansraj et al,24 indicated that the expansion of the scope of practice for optometrists to include therapeutics is a significant development in eye care, particularly in South Africa, where the ratio of ophthalmologists to optometrists and ophthalmic nurses is 1:4:3, respectively, indicating a greater reliance on optometrists as primary eye care providers. This expansion is beneficial in eye care as it will ensure more comprehensive eye care services, reducing referrals to ophthalmologists and patients receiving timely care at their local clinics.24 Other reports by Xulu-Kasaba13 and Buthelezi and Van Staden12 in South Africa highlighted the lack of human resources as a common inhibitor of providing effective and efficient eye care services in KZN. The vulnerability in staff shortages, particularly in rural-based eye care clinics, results in patients not receiving timely care, furthermore highlighting the limited or absence of outreach programmes to communities for visual screening that is helpful for early detection and treatment of ocular conditions12 According to WHO (2019), it is recommended that PEC be included in PHC for improved accessibility. Other authors have raised concerns that there seems to be no alignment in the placement of optometrists as they are regarded as primary health professionals.13 Their deployment in the district is only at the tertiary level, while the secondary and primary levels remain without any, which prevents early detection and appropriate intervention. Mzyece et al25 in Zimbabwe reported similar challenges as those indicated in the current study for the district, whereby the push outweighs the pull risk factors. These included staff shortages leading to being overburdened with work, and the lack of career advancement opportunities, as well as satisfactory compensation. These also affect the referral protocols that patients should follow in seeking intervention. The recruitment of eye care professionals can be achieved by availing incentives such as rural allowance. It is also important for the district to invest in training existing health care staff at clinics and CHCs to equip them with basic eye care knowledge that will help in managing minor eye conditions and ensuring timely referrals.
Buthelezi and Van Staden in KZN12 Sukati et al,16 in Swaziland, and Nkoana et al17 in Limpopo, have highlighted that the lack of resources, such as space and equipment, negatively affects the quality of eye care services provided in support of the current study findings. In addition, where equipment is available, there is a lack of maintenance plans for the longevity of equipment and the provision of quality eye care service to the population. These findings on the lack of equipment at primary and secondary levels in the district are not peculiar to rural-based eye care facilities, as reported by previous reports, particularly in the African continent with similar resource allocation.26 In such circumstances, patients are denied early diagnosis of ocular conditions, resulting in unnecessary referrals to higher levels of care. Other patients may be misdiagnosed or underdiagnosed from the lack of equipment in the district eye care facilities which is consistent with a report by Nkoana et al.17 The investment on the basic equipment required for patient assessment and maintenance is paramount in improving eye care service provision in the district.
Despite the availability of statistics in all the eye care facilities, reports generated at tertiary level, this crucial information is barely analysed and utilized for planning purposes in the district. It is also worth noting that where analysis is reported to be taking place, it is for spectacles only. This highlights that the focus is on refractive services, while not prioritising other ocular conditions for planning purposes. In addition, the tool used for documenting stats is not comprehensive enough to provide a true reflection. Some other challenges are brought by the poor planning and budgetary constraints, common in low and middle-income countries. The non-comprehensive reporting tool used for eye care services does not give a true reflection of the services offered by ophthalmic staff in the district. This needs to be harmonised to improve data management by including indicators for reporting, analysis of data, and having online interactive storage that will ensure patients do not get duplicate management, especially with optical devices, as they sometimes consult at different facilities in the district.17 Nalebe et al27 suggest that progress capacity planning at the governance level is hindered by the inaccurate or incomplete information captured in eye health facilities. Comprehensive health information regarding eye care services is vital for planning, epidemiological monitoring, and evaluating health plans aimed at reducing preventable blindness and for evidence-based policy development.
Of concern, is the lack of provision of low vision and contact lens services, while the province where the district is located, has a reported VI prevalence of 17.6%. The main possible attributing factors are the lack of equipment and human resources to cater for these services in the current study, consistent with reports by Sukati et al.16 With 90% of visually impaired individuals living in low to middle-income countries and a significant number of patients presenting to the public sector with keratoconus, the lack of these services results in late diagnosis and management of the conditions, resulting in preventable blindness28,29 Managing these conditions involves referrals to tertiary facilities, which increases backlog and waiting times at these institutions.30 Furthermore, despite healthcare services being free in the public sector31 there are still costs related to transportation and lost opportunities, as some of these patients must pay transport fees to access these facilities and wait for services, resulting in lost productivity and income for those who are working.
There is a notable distinction between individuals seeking eye care for the first time and those who are returning for follow-up appointments. Jolley et al32 highlight that past limitations in access to or awareness of eye care services have resulted in an increase in first-time visits, which aligns with the findings of the current study.
Furthermore, a notable decline in the age of first-time patients has been observed at these facilities. Supporting these observations, Barman et al33 noted that older adults are more likely to attend eye examinations due to an increase in age-related visual impairments, which may drive their motivation to seek care. Conversely, a concerning finding32 highlighted a low presentation rate among children, attributed to their inability to articulate vision problems and the failure of those around them such as teachers and parents to recognize these issues34 This situation hampers early detection and prevention in this age group, underscoring the urgent need for improved health education among both children and their parents regarding the importance of regular eye examinations, even in the absence of visible symptoms. Such education is crucial to encourage more individuals to seek preventive care and ensure equitable attendance among both adults and children.
The majority of returning patients were seen at the tertiary level, indicating that those attending follow-up tests predominantly had more complex conditions that required the specialized services available at this level. In contrast, the lower rate of returning patients at primary and secondary care levels may suggest that these facilities are inadequate for managing a comprehensive range of eye conditions. Furthermore, Jolley et al33 highlight that past limitations in access to or awareness of eye care services have resulted in an increase in first-time visits, which aligns with the findings of the current study.
According to Lam et al the severity of the ocular conditions significantly impacts the duration between the most recent eye examination and the preceding one.35 In this study, most patients returned for follow-up visits within 0–12 months, highlighting the complexity inherent in their conditions. However, some patients demonstrated poor adherence to follow-up appointments, returning for their visits after 25 months or more. This timeframe is significantly longer than the standard schedule for routine eye examinations, a finding that aligns with the results reported by Zeng et al.36
The current study highlights that most patients were diagnosed with refractive errors (RE) and cataracts, aligning with previous research that identifies these conditions as leading causes of global visual impairment. While these conditions were managed through spectacles and surgical interventions, inconsistencies and delays in the provision of spectacles stemmed from budget constraints and limited funding for eye care services. Some patients received their spectacles within a timeframe of 3 to 12 months, while a noteworthy proportion did not receive spectacles at all. This indicates that patients, while waiting, endure difficulties negatively affecting their quality of life, which aligns with previous studies.12,37 In 2018, the Department of Health issued a circular that ceased payment for spectacles and optical devices in public facilities in KZN, and these were classified as medical devices. This move aligned with the global initiative to promote universal eye health coverage, ensuring accessible and affordable eye care services, however, this has not been achieved due to inadequate budget allocation for eye health in the district for spectacles and medication. This highlights the need for advocacy to increase funding, address delays in spectacle procurement, and invest in basic ophthalmic equipment in the district to ensure quality care.
In contrast to the findings presented in the WHO’s report, conjunctival disorders emerge as the third most prevalent ocular condition in the uMgungundlovu district. This observation aligns with research conducted in various African countries, which similarly underscores the significance of conjunctival disorders within the broader context of eye health in these populations.38 The preferred management strategies for these conditions were pharmaceutical treatment; however, the medication stockouts led to unwarranted referrals for pharmaceutical management, which were attributed to the lack of eye medications in the primary level clinics, highlighting the challenges in providing accessible and affordable eye care services, especially in rural areas. This is consistent with previous reports that raised concerns about the importance of addressing medication shortages in facilities to improve eye care services.39,40 Besides lack of funding, Lee et al41 cited ineffective communication also leading to medication stock outs in eye care clinics, suggesting the inclusion of this aspect in addressing unwarranted shortages. This is usually a costly exercise and places a financial burden on low-income individuals, as some were expected to purchase medication in the private sector. Enforcing adherence and periodic reviews of standard operating procedures for the procurement and availing of medications as per the standard guidelines for the different levels of care is crucial for the improvement of eye care services in the district. This also needs to be prioritised to enable full scope of practice for optometrists with therapeutic privileges.
Conclusion
A majority of selected facilities (85.7%) did not have enough stationed human resources or adequate equipment to diagnose ocular diseases. These facilities relied on visiting optometrists for the provision of eye care services; however, working space in some facilities posed an issue. Despite the availability of data for planning in the form of registers and reports, this information was not analyzed, and there was no management information providing a baseline for planning eye care service provision. Furthermore, spectacles and pharmaceutical treatments were the most commonly used management strategies in the district; however, some patients experienced delays in receiving recommended management, or sometimes they did not receive management at all due to budget constraints and drug stockouts, resulting in unnecessary referrals. Investment in proper planning, informed by evidence-based reports, is essential for the appropriate implementation of comprehensive eye care in the district. This will require proper governance, political will, and the involvement of relevant stakeholders in eye care, along with adequate budget allocations for success.
The primary limitation of this study was its brief timeframe. The authors suggest that future research should extend over multiple years to more effectively identify long-term patterns, monitor changes in ocular conditions, and assess treatment outcomes. Moreover, this broader approach would facilitate a more accurate evaluation of the availability of eye care services over time, including instances when essential equipment was either unavailable or present but non-functional.
Acknowledgments
The authors would like to acknowledge the optometrists who participated in the study, especially those in the uMgungundlovu district.
Disclosure
The authors have declared that no financial or personal competing interests in this work.
References
1. Khatri R, Endalamaw A, Erku D, et al. Continuity and care coordination of primary health care: a scoping review. BMC Health Serv Res. 2023;23(1). doi:10.1186/s12913-023-09718-8
2. Elam AR, Tseng VL, Rodriguez TM, et al. disparities in vision health and eye care. Ophthalmology. 2022;129(10):e89–e113. doi:10.1016/j.ophtha.2022.07.010
3. Cicinelli M, Marmamula S, Khanna R. Comprehensive eye care-issues, challenges, and way forward. Ind J Ophthalmol. 2020;68(2):316–323. doi:10.4103/ijo.IJO_17_19
4. Bourne RR, Cicinelli MV, Sedighi T, et al. Effective refractive error coverage in adults aged 50 years and older: estimates from population-based surveys in 61 countries. Lancet Glob Health. 2022;10(12):e1754–e1763. doi:10.1016/S2214-109X(22)00433-8
5. Willie MM. Eye care services and benefits paid by medical schemes in South Africa. Afr Vision Eye Health. 2023;82(1):1–9. doi:10.4102/AVEH.V82I1.756
6. World Health Organisation (WHO). Core competencies for the eye health workforce in the WHO African Region. World Health Organization, Regional Office for Africa; 2019; 62 Available from: https://www.afro.who.int/publications/core-competencies-eye-health-workforce-who-african-region.
7. Winnie M, Busisiwe B. CUR-42-1901. Challenges of Quality Improvement in the Healthcare of South Africa Post-Apartheid: a Critical Review. 2019
8. Frempong EA, Van Staden DW, Frempong E. Child health promotion during the COVID-19 pandemic: A health and welfare sector collaboration. African J Primary Health Care Family Med. 2024. doi:10.4102/phcfm
9. Sengo DB, Marraca NA, Muaprato AM, García-Sanjuan S, Caballero P, López-Izquierdo I. Barriers to accessing eye health services in Suburban communities in Nampula, Mozambique. Int J Environ Res Public Health. 2022;19(7). doi:10.3390/ijerph19073916
10. Gordon T, Booysen F, Mbonigaba J. Socio-economic inequalities in the multiple dimensions of access to healthcare: the case of South Africa. BMC Public Health. 2020;20(1). doi:10.1186/s12889-020-8368-7
11. Burn H, Puri L, Roshan A, Singh SK, Burton MJ. Primary eye care in Eastern Nepal. Ophthalmic Epidemiol. 2020;27(3):165–176. doi:10.1080/09286586.2019.1702217
12. Buthelezi LM, Van Staden D. Integrating eye health into policy: evidence for health systems strengthening in KwaZulu-Natal. Afr Vision Eye Health. 2020;79(1):1–10. doi:10.4102/AVEH.V79I1.549
13. Xulu-Kasaba ZN, Mashige KP, Naidoo KS. An assessment of human resource distribution for public eye health services in KwaZulu-Natal, South Africa. Afr Vision Eye Health. 2021;80(1):1–8. doi:10.4102/AVEH.V80I1.583
14. Verwey VF, Mahomed S. Burden of eye conditions at a specialised eye hospital in KwaZulu-Natal, South Africa. Afr Vision Eye Health. 2020;79(1):1–5. doi:10.4102/AVEH.V79I1.518
15. KwaZulu-Natal Department of Health. (2020). uMgungundlovu Health District, Growing KwaZulu-Natal Together. Available from: https://www.kznhealth.gov.za/umgungundlovu.htm.
16. Sukati VN, Moodley VR, Mashige KP. Barriers to Eye Health Care Among School Going Children in Swaziland: Towards the Development of a Framework for Access to Child Eye Health Care. 2018.
17. Nkoana PMW, Mashige KP, Moodley VR. Strengthening keratoconus management systems in South African public sector facilities. Afr Vision Eye Health. 2024;83(1). doi:10.4102/aveh.v83i1.832
18. Maake ME, Moodley VR. An evaluation of the public sector optometric service provided within the health districts in KwaZulu-Natal, South Africa. Afr Vision Eye Health. 2018;77(1):1–9.
19. Sewunet A, Afework E. Pattern of ocular diseases among patients attending ophthalmic outpatient department: a cross-sectional study. Int J Clin Exp Ophthalmol. 2020;4(2):049–053. doi:10.29328/journal.ijceo.1001033
20. Krasniuk S, Crizzle AM. Impact of health and transportation on accessing healthcare in older adults living in rural regions. Transp Res Interdiscip Perspect. 2023;21. doi:10.1016/j.trip.2023.100882
21. Evans MV, Andréambeloson T, Randriamihaja M, et al. Geographic barriers to care persist at the community healthcare level: evidence from rural Madagascar. PLOS Global Public Health. 2022;2(12):e0001028.
22. Solomon SD, Shoge RY, Ervin AM, et al. Improving access to eye care: a systematic review of the literature. Ophthalmology. 2022;129(10):e114–e126. doi:10.1016/j.ophtha.2022.07.012
23. Thompson AC, Thompson MO, Young DL, et al. Barriers to follow-up and strategies to improve adherence to appointments for care of chronic eye diseases. Invest Ophthalmol Vis Sci. 2015;56(8):4324–4331. doi:10.1167/iovs.15-16444
24. Hansraj R, Dlamini N, Khan S, et al. Ocular therapeutics and the profession of optometry in South Africa. Afr J Prim Health Care Fam Med. 2023;16(1). doi:10.4102/PHCFM.V16I1.4140
25. Mzyece B, Malemane O, Chimatira A, Macheka B. Patterns of eye diseases among children visiting two tertiary-level facilities in zimbabwe: a retrospective records review (2018-2020) at Sekuru Kaguvi and Richard Morris Eye Hospitals in Harare and Bulawayo. Open J Ophthalmol. 2022;12(03):218–232. doi:10.4236/ojoph.2022.123021
26. Aghaji A, Burchett HE, Mathenge W, et al. Technical capacities needed to implement the WHO’s primary eye care package for Africa: results of a Delphi process. BMJ Open. 2021;11(3). doi:10.1136/bmjopen-2020-042979
27. Nalebe RM, Odhiambo-Otieno GW, Kyalo CK. Towards a digital health information framework for management of essential medicine supply chain in public healthcare facilities in Kenya, Robert Mugubi Nalebe, a thesis submitted in partial fulfillment of the requirements for the conferment of the degree of Doctor of Philosophy in Health Systems Management in the School of Medicine and Health Sciences of Kenya Methodist University; 2024.
28. Naipal S, Rampersad N. A review of visual impairment. Afr Vision Eye Health. 2018;77(1). doi:10.4102/aveh.v77i1.393
29. Gcabashe NM, Moodley VR, Hansraj R. Prevalence and clinical profile of keratoconus in patients presenting at a provincial hospital in KwaZulu, Natal, South Africa: a case study. J Public Health Afr. 2023;14(9). doi:10.4081/jphia.2023.2356
30. Nkoana PMW, Moodley VR, Mashige KP. Keratoconic patient profile and management at public sector facilities in South Africa. Afr Vision Eye Health. 2023;82(1). doi:10.4102/aveh.v82i1.780
31. Malakoane B, Heunis JC, Chikobvu P, Kigozi NG, Kruger WH. Public health system challenges in the Free State, South Africa: a situation appraisal to inform health system strengthening. BMC Health Serv Res. 2020;20(1). doi:10.1186/s12913-019-4862-y
32. Jolley E, Mafwiri M, Hunter J, Schmidt E. Integration of eye health into primary care services in Tanzania: a qualitative investigation of experiences in two districts. BMC Health Serv Res. 2017;17(1). doi:10.1186/s12913-017-2787-x
33. Barman D, Mishra M. How does eye care seeking behaviour change with increasing age and visual impairment? Intersectional analysis of older adults in the Indian Sundarbans. BMC Geriatr. 2020;20(1). doi:10.1186/s12877-020-1438-y
34. Alrasheed SH. A systemic review of barriers to accessing paediatric eye care services in African countries. Afr Health Sci. 2021;21(4):1887–1897. doi:10.4314/ahs.v21i4.47
35. Lam D, Chong K, Shih K, Wan KH, Cheng A. Optimizing diagnosis and management of dry eye disease: a practical framework for Hong Kong. Ophthalmol Ther. 2025;14(5):815–833. doi:10.1007/s40123-025-01129-8
36. Zeng R, LaMattina KC. Follow-up adherence after community health vision screening programs: a review of the literature. J Acad Ophthalmol. 2023;15(02):e223–e231. doi:10.1055/s-0043-1771354
37. Maseko SN, van Staden D, Mhlongo EM. The rising burden of diabetes-related blindness: a case for integration of primary eye care into primary health care in Eswatini. Healthcare. 2021;9(7). doi:10.3390/healthcare9070835
38. Bukhari S, Ahsan S, Azam S, et al. Five years’ retrospective analysis of childhood ocular morbidities: a priority setting guidelines for pediatric eye clinic. Pak J Med Sci. 2022;38(6):1501–1507. doi:10.12669/pjms.38.6.5441
39. Aghaji A, Burchett HED, Oguego N, Hameed S, Gilbert C. Primary health care facility readiness to implement primary eye care in Nigeria: equipment, infrastructure, service delivery and health management information systems. BMC Health Serv Res. 2021;21(1). doi:10.1186/s12913-021-07359-3
40. Khanal S, Veerman L, Ewen M, Nissen L, Hollingworth S. Availability, price, and affordability of essential medicines to manage noncommunicable diseases: a national survey from Nepal. Inquiry. 2019;56. doi:10.1177/0046958019887572
41. Lee KM, Page A, Kim S, et al. Perceptions and expectations of health professionals regarding hospital pharmacy services and the roles of hospital pharmacists: a qualitative systematic review and meta-synthesis. Explor Res Clin Soc Pharm. 2023;10. doi:10.1016/j.rcsop.2023.100264
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.