Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Atypical Nevus Sebaceus at an Unusual Location Treated with Carbon Dioxide Laser: A Case Report
Authors Sutedja EK ![]() , Mareta S
, Mareta S ![]() , Sutedja E
, Sutedja E ![]() , Ruchiatan K
, Ruchiatan K
Received 7 September 2022
Accepted for publication 8 December 2022
Published 15 December 2022 Volume 2022:15 Pages 2745—2749
DOI https://doi.org/10.2147/CCID.S389050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Eva Krishna Sutedja, Shela Mareta, Endang Sutedja, Kartika Ruchiatan
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Eva Krishna Sutedja, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +62 812 201 4300, Email [email protected]
Abstract: Nevus sebaceus (NS) or organoid nevus is an epidermal nevus comprising predominantly sebaceous glands with a prevalence of approximately 0.3% of the newborns. The initial clinical manifestations of NS are single or less commonly multiple yellowish patches with overlying alopecia, usually confined to the scalp. However, it can also appear on the face, preauricular area, and the neck. During puberty, skin lesions will turn into round or linear verrucous plaques accompanied with an increase in number due to the influence of androgens. As they progress, about 20% of the NS cases might turn into secondary tumors which can be benign or malignant (in 2.5% cases). NS can manifest as atypical lesions and may also arise on areas other than its predilection sites. A case of a lesion presented on an atypical location of an 18-year-old male patient treated with carbon dioxide (CO2) laser was reported. Physical examination revealed skin-colored and blackish-brown papules arranged in groups on the left side of the patient’s chest. Histopathological examination on a sample taken from one of the skin lesions on the chest showed hyperkeratosis, acanthosis, papillomatosis, and sebaceous hyperplasia, confirming the diagnosis of NS. The patient was treated with CO2 laser, and clinical improvements were observed. Histopathological examination of NS is not routinely performed; however, it should be carried out when the lesion is atypical and presented at an unusual location, or there is a suspicion of malignancy.
Keywords: atypical lesion, nevus sebaceus, unusual location, carbon dioxide laser
Introduction
Nevus sebaceus (NS) or organoid nevus, also known as the NS of Jadassohn, was first described by Jadassohn in 1895.1,2 NS presents as well-demarcated hamartomatous lesions consisting of mainly sebaceous glands, epidermis, defective hair follicles, and apocrine glands.2,3 About two-thirds of NS cases are diagnosed at birth, while the rest are usually diagnosed in early childhood.4 This condition is most commonly found on the hairy scalp, face, and neck, but rarely presents on the chest and oral mucosa.5,6 The typical clinical manifestation of NS consists of three stages.7 At initial stage, the lesion is round, oval, or linear, flat, slightly yellowish, and hairless.4 At puberty, they turn into round or linear verrucous plaques with increased numbers of lesions, due to the influence of androgens.4,7 At a later stage, about 20% of NS might develop into secondary tumors which can be either benign or malignant.8,9 The most common benign tumors arising from NS are trichoblastoma and syringocystadenoma papilliferum,3 while the most common malignant tumors being basal cell carcinoma, squamous cell carcinoma, and sebaceous carcinoma.10 Histopathological examination of NS is not routinely performed; however, it should be carried out when there is a suspicion of malignancy. Various therapeutic modalities can be used to remove NS, including surgical excision, electrosurgery, cryosurgery, CO2 laser, and dermabrasion.3,11 The recommended treatment for NS is surgical excision,10,11 although surgery may leave a linear scar tissue. Therefore, other methods, such as CO2 laser therapy, is preferred.11
Based on the medical records from the Department of Dermatovenereology of Hasan Sadikin Hospital, Bandung, Indonesia, from January 1, 2016 to December 31, 2021, 22 NS cases were reported. This case report aims to describe a case of atypical nevus sebaceus at an unusual location on the left chest treated with CO2 laser.
Case
An 18-year-old male patient presented with intermittently itchy, skin-colored, and brown-black papules on the left side of his chest. These papules had increased in number and size over the last 2 months. Initially, the lesions appeared when he was aged 12 and they consisted of five small, pinhead-sized, yellowish papules with no hair on the left chest. He did not seek treatment for these lesions as there was no itching or pain. Three years later, the lesions darkened and turned into a brownish color. After a couple of years, the lesions increased in number and size as they turned into a cluster of corn kernel-sized lesions. There were no similar lesions on other body parts. He denied any history of rapidly growing mass or ulceration on the lesions. There was no history of seizures, eye problems, or bone abnormalities that may suggest Schimmelpenning syndrome. The patient underwent breast tissue reduction surgery 4 years ago for gynecomastia on his right chest. There was no family history of similar dermatological disorders.
Clinical examination revealed multiple, confluent, skin-colored and brownish black papules on the left chest (Figure 1). These lesions were mostly round with the size of 0.2 ×0.2×0.2 cm to 1×0.5 ×0.2 cm, clearly demarcated, raised, dry, and skin-colored or brownish black. Histopathological examination showed hyperplastic squamous epithelium with hyperkeratosis, mild papillomatosis, and acanthosis with no nuclear abnormalities. In the subdermal area, there were fibrocollagenous connective tissue with lymphocytic infiltration and vasodilation, along with hyperplasia of the sebaceous glands, hair follicles, and sudoriferous glands. There were no signs of malignancy. These histopathological findings supported the diagnosis of NS (Figure 2). CO2 laser was utilized to treat the lesions using the Ultrapulse® laser device with continuous pulsing at a frequency of 100 Hz and 200 μs pulse duration. There were no postprocedural complications. He was then prescribed 0.1% gentamicin cream to be applied twice daily after each session as a prophylactic antibiotic towards secondary infection that may arise following the laser treatment. We also prescribed 500 mg mefenamic acid to be taken as needed for pain. On a follow-up visit, 63 days after the initial laser therapy, the treatment site had mostly healed, with some hypertrophic and atrophic scarring(Figure 3).
 |
Figure 1 Pre-treatment feature in case. Brown blackish papules and skin colored papules on the chest (A and B) before treatment. |
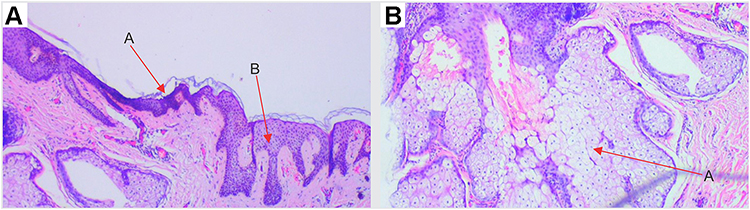 |
Figure 2 Histopathological feature of skin lesion: (A) A – epidermal hyperplasia and hyperkeratosis (red arrow), B – slightly papillomatosis and infiltration of lymphocytes in the upper dermis (red arrow). Hematoxylin–eosin stain, 40×. (B) A – Hyperplasia of the sebaceous glands (red arrow). Hematoxylin–eosin stain, 100×. |
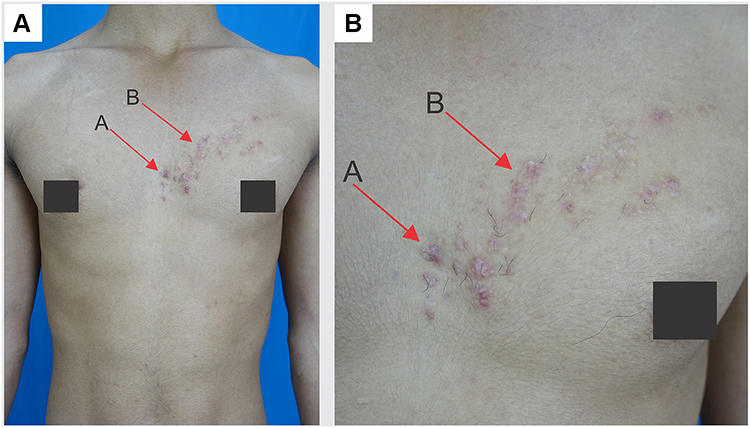 |
Figure 3 The patient was treated with CO2 laser. On a follow-up visit, 63 days after the initial laser therapy, most of the skin lesions on the chest flattened with some hypertrophic and atrophic scarring (red arrow) (A and B). |
Discussion
Nevus sebaceus (NS) is a form of well-demarcated epidermal nevus consisting mostly of sebaceous glands.3,7 The incidence is 3 out of 1000 live births,1,3 with males and females being equally affected.7,12 NS is commonly present at birth but can also develop during infancy or childhood.4 In this case report, the initial skin lesions appeared when the patient was 12 years old. NS is most commonly found on the scalp (66.8%), face (26.7%), and the neck (5.5%). However, they can occasionally appear at the preauricular area, oral mucosa, chest, and other areas of the body.5,12 Gu et al12 reported a case of NS with a rare predilection on the left chest of a 38-year-old woman which had been present for 20 years.12 Similarly, in our case, we found the NS lesion on the patient’s left chest. NS is typically solitary,13 round, oval, or linear in shape following the Blaschko’s lines,3 and varying in size from a few millimeters to a centimeter.6 NS lesions are also a hallmark of Schimmelpenning syndrome.14 The characteristics of this syndrome are the presence of a linear form of NS lesions with extracutaneous abnormalities of bone, eye, and especially neurologic findings.
Clinically, NS can be divided into three stages.7,15 The first stage usually appears at birth up to childhood in the form of pink plaques or solitary, slightly raised, yellowish, hairless, round, oval or linear plaque with a smooth surface.6 There are no morphological changes associated with these early lesions, and the yellowish coloration is caused by sebaceous gland secretions.16 The second stage usually occurs at early puberty, where the skin lesions may transform into brittle verrucous plaques and are usually accompanied by pruritus.6,12 At this stage, the lesions grow rapidly due to the development of the sebaceous glands triggered by androgen hormones.1 In 10–20% of the cases, the lesions may progress into the third stage,8 manifesting as secondary benign or malignant skin tumors (in 2.5% of the NS cases).9 Tumors usually appear in the fourth to seventh decades of life and are rare during childhood, since the risk of malignancy increases with age.17 In this case report, the lesions were also atypical, as they presented in the form of yellowish macules that appeared at the age of 12, which then developed into a cluster of confluent skin-colored and blackish brown papules on the left chest in 3 years. Therefore, further examination was required in order to establish the diagnosis.
The etiology of NS has not yet been elucidated.6 In a study by Levinsohn et al on 27 cases of NS, HRAS gene mutation was identified in 25 cases and KRAS gene mutation was found in two cases.18 Androgens may also increase the risk of NS, as reflected by the increased rate of lesions’ growth during puberty and the appearance of secondary tumors in adulthood.15 According to a study by Hamilton et al, the increase of androgen receptors in sebocytes and other epithelial components of the NS might reflect an increased sensitivity to androgen.4 Skin appendages tumors are commonly found in NS cases, including benign tumors such as trichoblastoma, syringocystadenoma papilliferum, syringoma, leiomyoma, keratoacanthoma, and hidradenoma.1,3 Furthermore, malignant tumors can also arise from NS lesions although the occurrence is rare. They include basal cell carcinoma, sebaceous carcinoma, squamous cell carcinoma, porocarcinoma, apocrine carcinoma, trichilemmal carcinoma, and malignant melanoma.1,17
The diagnosis of NS is established based on medical history, physical examination, and histopathologic features to identify secondary tumors.17 Histopathological examination is indicated in NS cases if there is a suspicion of malignancy.17 In our patient, histopathological examination showed hyperkeratosis, acanthosis, and mild papillomatosis, with fibrocollagenous connective tissue, lymphocytic infiltration, and vasodilation, along with hyperplasia of the sebaceous and sudoriferous glands. Although these lesions were not identified in typical predilection sites, the clinical findings and investigation results supported the diagnosis of NS with no signs of malignancy.
Treatment for NS aims to restore cosmesis, improve psychosocial issues,3 and prevent the occurrence of secondary tumors.17 Full thickness skin excision is the definitive treatment for NS of skin appendages within the subcutaneous tissue.6,19 However, excision of NS may cause a linear scar2; therefore, other less invasive modalities may be considered in specific cases, including CO2 laser treatment,20 dermabrasion, cryosurgery, and electrosurgery.3 Although CO2 laser therapy has excellent cosmetic results with low risk of scarring,20 this treatment only removes lesions partially up to the dermal papillae layer, and it is unable to prevent the occurrence of secondary tumors.1 Our patient was treated with CO2 laser since he refused the skin excision method due to the risk of large scarring. As a part of informed consent, the patient was explained about the risk of recurrence, postprocedural atrophic scarring, and the risk of secondary tumors.
The risk of malignant secondary tumors in adult NS cases is relatively low (0.8–3.5%).17 The majority of NS have excellent prognosis.3 In cases of linear or extensive NS, disorders of other systems known as Schimmelpenning syndrome may occur. This condition affects the central nervous system, ocular, skeletal, and cardiovascular.13 Based on our patient’s medical history, physical examination, and histopathological examination, there were no signs of secondary tumors or involvement of other organs. Therefore, the overall prognosis was good. NS lesions may be distressing esthetically or psychologically,3,6 and even superficial treatment such as CO2 laser treatment may still cause postinflammatory hyperpigmentation and scarring.20,21 Furthermore, NS lesions treated with CO2 laser may carry a risk of recurrence.1,20 Although the rate of recurrence of NS is unclear, the study by Alonso-Castro et al21 showed the risk of recurrence of 20% 10 months after CO2 laser treatment and 30% 18 months after treatment.21 We advised our patient to attend a follow-up appointment after 6 months post-laser treatment, but he failed to attend.
Conclusions
Nevus sebaceus (NS) is a relatively common skin disorder, mainly developed during the neonatal period and childhood. Although the incidence, predilection sites, and clinical manifestations should be considered in establishing the diagnosis of NS, their presentations may vary, especially regarding predilection sites. NS can occur on the chest, which is considered as an atypical site. It can also appear in adolescence. Surgical excision of the skin lesions is the definitive treatment for NS, although the risk of scarring may justify other treatment modalities, including CO2 laser treatment. Overall, NS has a good prognosis, although their functional and cosmetic results may be affected by treatment choice and the risk of recurrence.
Ethical Statement
This publication of images was included in the patient’s consent for publication of the case. The case report has been approved by the institutional ethics committee of Dr. Hasan Sadikin General Hospital, Bandung, Indonesia (Ethical Clearance No. LB.02.01/x.6.5/247/2022).
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of the case details and images.
Acknowledgments
The authors would like to thank the staff of the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patel P, Malik K, Khachemoune A. Sebaceus and Becker’s nevus: overview of their presentation, pathogenesis, associations, and treatment. Am J Clin Dermatol. 2015;16(3):197–204. doi:10.1007/s40257-015-0123-y
2. Garcias-Ladaria J, Cuadrado Rosón M, Pascual-López M. Epidermal nevi and related syndromes - part 2: nevi derived from adnexal structures. Actas Dermosifiliogr. 2018;109(8):687–698. doi:10.1016/j.ad.2018.05.004
3. Wali GN, Felton SJ, McPherson T. Management of nevus sebaceus: a national survey of UK dermatologists and plastic surgeons. Clin Exp Dermatol. 2018;43(5):589–591. doi:10.1111/ced.13422
4. Hamilton KS, Johnson S, Smoller BR. The role of androgen receptors in the clinical course of nevus sebaceus of Jadassohn. Mod Pathol. 2001;14(6):539–542. doi:10.1038/modpathol.3880346
5. Chi SG, Kim JY, Kim HY, et al. Multiple nevus sebaceous occurring on the scalp and on the contralateral side of the face. Ann Dermatol. 2011;23(3):389–391. doi:10.5021/ad.2011.23.3.389
6. Moody MN, Landau JM, Goldberg LH. Nevus sebaceous revisited. Pediatr Dermatol. 2012;29(1):15–23. doi:10.1111/j.1525-1470.2011.01562.x
7. Kazakov DV, Bhat Y, Hassan I, et al. Cutaneous type adnexal tumors outside the skin. Am J Dermatopathol. 2011;33(3):303–315. doi:10.1097/DAD.0b013e3181db1da3
8. Galvis KH, Frattini SC, Fernandes KA. Jadassohn’s sebaceous nevus. RBM Dermatol Cosmiat. 2015;71(2):23–25.
9. Idriss MH, Elston DM. Secondary neoplasms associated with nevus sebaceus of Jadassohn: a study of 707 cases. JAAD. 2014;70(2):332–337. doi:10.1016/j.jaad.2013.10.004
10. Alvarenga HR, Funez NI, Benitez YS. Nevus sebaceous of jadassohn in a 13 years old patient: case report. J Dermatol Res. 2020;2(1):1–3.
11. Goel P, Wolfswinkel EM, Fahradyan A, et al. Sebaceous nevus of the scalp. J Craniofac Surg. 2020;31(1):257–260. doi:10.1097/SCS.0000000000006007
12. Gu AK, Zhang X-J, Zhang L-T, et al. Nevus sebaceous at an unusual location: a rare presentation. Chin Med J. 2017;130(23):2897–2898. doi:10.4103/0366-6999.219147
13. El Ezzi O, de Buys Roessingh AS, Bigorre M, et al. Syndromic sebaceous nevus: current findings. Int J Dermatol. 2018;57(5):599–604. doi:10.1111/ijd.13942
14. Wang SM, Hsieh Y-J, Chang K-M, et al. Schimmelpenning syndrome: a case report and literature review. Pediatr Neonatol. 2014;55(6):487–490. doi:10.1016/j.pedneo.2012.12.017
15. Hsu MC, Liau J-Y, Hong J-L, et al. Secondary neoplasms arising from nevus sebaceus: a retrospective study of 450 cases in Taiwan. J Dermatol. 2016;43(2):175–180. doi:10.1111/1346-8138.13070
16. Liu Y, Valdebran M, Chen J, Elbendary A, Wu F, Xu M. Nevus sebaceous of jadassohn with eight secondary tumors of follicular, sebaceous, and sweat gland differentiation. Am J Dermatopathol. 2016;38(11):861–866. doi:10.1097/DAD.0000000000000603
17. Kamyab-Hesari K, Seirafi H, Jahan S, et al. Nevus sebaceus: a clinicopathological study of 168 cases and review of the literature. Int J Dermatol. 2016;55(2):193–200. doi:10.1111/ijd.12845
18. Levinsohn JL, Tian LC, Boyden LM, et al. Whole-exome sequencing reveals somatic mutations in HRAS and KRAS, which cause nevus sebaceus. J Invest Dermatol. 2013;133(3):827–830. doi:10.1038/jid.2012.379
19. Fathi R, Behan JW, Julapalli M. Special Dermatologic Surgery. J Pediatric Dermatol Surg. 2019;2019:171–187.
20. Bhat YJ, Hassan I, Sajad P, et al. Evaluation of carbon dioxide laser in the treatment of epidermal nevi. J Cutan Aesthet Surg. 2016;9(3):183–187. doi:10.4103/0974-2077.191646
21. Alonso-Castro L, Boixeda P, Reig I, De daniel-rodríguez C, Fleta-Asín B, Jaén-Olasolo P. Carbon dioxide laser treatment of epidermal nevi: response and long-term follow-up. Actas Dermosifiliogr. 2012;103(10):910–918. doi:10.1016/j.ad.2012.04.004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.