Back to Journals » International Medical Case Reports Journal » Volume 17
Atypical Clinical Manifestations of Herpes Simplex Virus-1 Infection
Authors Wicaksono IK ![]() , Ridho F
, Ridho F ![]() , Zakiawati D
, Zakiawati D
Received 26 July 2024
Accepted for publication 21 October 2024
Published 7 November 2024 Volume 2024:17 Pages 933—937
DOI https://doi.org/10.2147/IMCRJ.S475249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Imme Kris Wicaksono,* Faiznur Ridho,* Dewi Zakiawati*
Oral Medicine Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
*These authors contributed equally to this work
Correspondence: Imme Kris Wicaksono, Oral Medicine Residency, Faculty of Dentistry, Universitas Padjadjaran, Jl. Sekeloa Selatan No. 1, Bandung, West Java, 40132, Indonesia, Email [email protected]
Introduction: The Herpes Simplex Virus-1 (HSV-1) infection of the oral cavity is a disease that initiates with prodromal symptoms such as fever and malaise, followed by the emergence of oral and perioral lesions. The common clinical manifestations of HSV-1 infection involve the development of vesicles on the face, oral mucosa and lips, which eventually progress to ulceration. This case report aims to present an atypical clinical manifestation of HSV-1 infection.
History and Clinical Findings: A 62-year-old woman presented with complaints of a lump at the corner of her left lip, which had disappeared but reappeared. Six weeks ago, the lump started as a white spot, then gradually enlarging, becoming painful, and ruptured. The patient went to the clinic for treatment and was given gentamicin ointment, but there was no improvement. Extraoral examination showed a nodule in the corner of the left lip measuring 1 × 2 cm, filled with purulent exudate. Serological examination revealed reactive anti-HSV-1 IgG results, leading to a diagnosis of Herpes Labialis.
Case Management: Pharmacological therapy comprised antivirals and multivitamins. The lesion resolved after 10 days of treatment with no reported recurrence during the three-month evaluation.
Conclusions and Recommendations: HSV-1 infection presents with a variety of clinical features, including typical signs of vesicles, ulceration, and also other atypical forms of lesions. A comprehensive history accompanied with supporting examinations is crucial to identifying the diverse clinical manifestations of herpes simplex virus-1 infection.
Keywords: Herpes simplex virus-1 (HSV-1), herpes labialis, lumps, nodules
Introduction
Recurrent intraoral herpes simplex virus 1 infection (RIH) is a recurrent HSV-1 infection characterized by painful and itchy blisters and vesicles on the oral mucosa.1 The prevalence of HSV-1 infection in humans worldwide is 40–80%. According to the WHO, in 2016 an estimated 3.75 billion people in the world tested positive for HSV-1 and the prevalence in those under 50 years of age was 67%. There is no significant difference in incidence between women and men. A person can be infected with HSV-1 through sexual or non-sexual partners and the presentation of recurrence reaches 30–40%.2 HSV infection can be latent or reactivated. Predisposing factors that cause remission are sunlight, emotional stress, immunosuppression, hormonal dysfunction, or nerve injury. Bandung Indonesia shows data for the incidence of outpatients including RIH 85.71% and labial herpes (LH) 14.29%. Serologic examination of patients infected with primary HSV-1 usually shows a reaction to the anti-HSV-1 IgG and IgM tests, but patients with reactivation are only reactive to the anti-HSV-1 IgG test.3
There are three clinical manifestations of HSV-1 infection, namely herpes labialis infection, herpetiform stomatitis and recurrent intra oral ulceration herpes, which are generally asymptomatic.1 According to the World Health Organization (WHO), HSV-1 infection is mostly asymptomatic but can also be symptomatic. Symptoms can be very generalized such as fever and malaise with sores on the lips or commonly referred to as canker sores.3 Prodromal symptoms such as itching, tingling, or burning are followed by the appearance of papules, vesicles, ulcers, crusting, and then resolution of the lesions. Pain is generally present only 2 days in beginning.4
This case report aims to describe the unusual clinical features of herpes labialis in a female patient. A thorough history and supporting examinations help to establish the diagnosis. An accurate diagnosis can help in faster healing and improve the patient’s quality of life.
Case Presentation
The 62-year-old female patient came to Unpad Dental Hospital with complaints of a lump on the corner of the left lip and pain. Anamnesis showed that the patient had a fever and was somewhat weak at the beginning before the complaint of the lump. Initially in the form of a white spot since 6 weeks ago then getting bigger, painful and broken. When it broke, the patient squeezed the lump until a pus-like liquid came out. The lump had shrunk but never completely disappeared. The patient went to the clinic and was given gentamicin ointment, but there was no change. The patient’s occupation. The patient denied a history of recurrent thrush and food or drug allergies. Smoking and alcohol consumption were not present.
On extraoral examination, a lump was found on the left corner of the lip, there was a 1 × 2 cm lump, filled with purulent exudate, and sore. The lip also looked dry and flaky. Intraoral found white plaque on the entire dorsum of the tongue can be scraped without leaving reddish areas, and on the teeth, there are cervical caries in several teeth. Showed on Figure 1.
 |
Figure 1 (A) and (B) Showed nodul on left corner of the lip. (C) Coated tongue scala 2 Miyazaki on dorsum of the tongue. |
First visit, the patient was given pharmacological therapy in the form of chlorhexidine gluconate mouthwash 0.2%, which was swished twice a day 10 mL and then discarded, and given a vaseline album to be applied to the upper and lower lips twice a day. Non-pharmacological therapy is given in the form of advice to get enough rest, maintain diet and oral hygiene and not use lipstick alternately. The patient was asked to do an anti-HSV-1 IgG serology test.
The following day the patient’s serology test results came out and was found to be HSV-1 reactive with a result of 122 (Positive > 25) The patient was then prescribed acyclovir 400 mg five times a day for 7 days and added a multivitamin to be taken once a day. Mouthwash and vaseline albums were continued to be used, additional education was given to the patient to avoid triggering factors such as emotional stress, fatigue, spicy food and sun exposure.
The next follow-up, 10 days after taking acyclovir, was carried out via text conversation using the Whatsapp application because the patient still did not have time to return for control. Acyclovir and multivitamins are taken regularly and now that the lump is no longer painful and sore and has started to shrink but has not disappeared completely, the patient is advised to stop taking acyclovir and chlorhexidine gluconate mouthwash 0.2% and continue taking multivitamins and using vaseline albums.
Follow-up 3 months later, the lesions seemed to have disappeared, the pain and soreness had completely disappeared. The patient has not taken any medication, and in the past 3 months, the lesions have not reappeared. Showed on Figure 2.
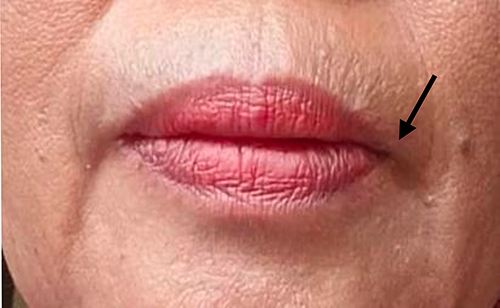 |
Figure 2 Follow up patient on three months lesion completely disappeared. |
Discussion
Herpes labialis is an HSV-1 infection that first manifests as tiny blisters or sores on the skin close to the infection site, either asymptomatic or symptomatic. Following the resolution of the original infection, the virus travels to sensory nerve cells where it remains dormant until it reactivates. The most common causes of HSV labial recurrence are stress, surgical trauma, menstruation or hormonal changes in women, infectious febrile disorders or hyperthermia, sunshine or UV light, and specific drugs like corticosteroids.5 The patient’s potential triggering variables included stress that led to exhaustion.
Recurrence of HSV-1 infection often appears on the lips and keratinized mucosa but it is possible to appear on other oral mucosa such as the tongue.6 The prognosis of labial herpes disease is characterized by variable frequency recurrences, ranging from sporadic episodes to monthly or even more frequent outbreaks per year.7 Recurrent infections can present as LH or RIH, LH is a major recurrent disease that often occurs in otherwise healthy individuals, whereas RIH generally has few, if any, systemic symptoms. LH is often preceded by symptoms of pruritus, tingling, burning or swelling, suggesting sensory in terminal viral replication localized to the future area of the new overflow.8 In this patient, a nodule appears in the corner of the left lip. The clinical presentation of HSV-1 infection has been previously reported in immunocompromised patients, while these patient also do not have other systemic diseases or can be said to be healthy individuals.
Tzanck smear, serology, viral culture, and polymerase chain reaction (PCR) are frequently employed supportive investigations to confirm the diagnosis of herpes infection. After undergoing a serologic examination, the patient’s anti-HSV-1 IgG result was 122 U/mL, which is higher than the usual limit of 25 U/mL. ELISA is a popular serological method that uses entire antigens to identify antibodies in the patient’s blood. When compared to Western blot testing, ELISA is easier to use and produces results faster. To differentiate between the two HSV types, these tests have a sensitivity range of 92–100% and a specificity range of 61–85%.9 Results with values four times the typical value suggest a continuing infection. Antibodies develop about 4–7 days of infection and peak within 2–4 weeks. Anti-HSV IgG antibody titers typically rise 1–2 weeks after first infection, peaking at 6–8 weeks.10
The therapy after the serology test results came out and the patient was found to be reactive to anti-HSV IgG with result of 122 U/mL out of the normal limit of 25 U/mL, its four times from normal limit so the patient was added to acyclovir 400 mg taken five times a day for 7 days as the main therapy aimed at controlling the spread of the virus. Acute episodes may be shorter, resulting in less pain. Nowadays, the most widely used medication to treat HSV-1 and HSV-2 is acyclovir (ACV), an acyclic guanosine analog that is present in the sponge Cryptotethya crypta. This is mostly because of its affordability, safety, and tolerability (Hassan et al, 2015). Crucially, for acyclovir to have antiviral effect, it must be phosphorylated to acyclovir triphosphate within the cell. The viral thymidine kinase (TK, gene UL23) is responsible for this activity. It catalyzes the conversion of acyclovir to acyclovir monophosphate, which increases the concentration of acyclovir inside the infected cell by decreasing its egress from the cell (Reusser, the thymidine kinase enzyme of HSV can phosphorylate acyclovir and acyclovir mono-phosphate (ACV-MP) which is trapped in infected cells, then cell kinases convert it into acyclovir diphosphate (ACV-DP) and acyclovir triphosphate (ACV-TP). ACV-TP is the active part of acyclovir that can inhibit HSV DNA replication.11
Patient was also given chlorhexidine gluconate 0.2% mouthwash, which is used to gargle 10 mL twice a day which aims as an antiseptic to prevent coated tongue and bad oral hygiene.12 Antiseptic administration is given to patients to create an oral environment that supports the speed of healing, one of which is by minimizing the number of oral microbes.3 Vaseline album is also given to patients to be used on the upper and lower lips because it has a function as a covering material that can protect the outer skin, protect the skin from the effects of weather and sun exposure and maintain the inner skin by preventing natural water loss so that the skin remains moist on the patient’s lips.13
Multivitamins are given to patients to increase the patient’s immune system.3 With the increase in body resistance and multivitamins are expected to help the nutritional adequacy needed by patients to fight the virus.14 The patients are recommended to take multivitamins once a day in the morning.
Follow-up for patient after 10 days after taking acyclovir was carried out via text conversation using the Whatsapp application because the patient still did not have time to return for control. Acyclovir and multivitamins are taken regularly for 7 days we follow up in 10 days because patient taking acyclovir on day three after first visit and now that the lump is no longer painful and sore and has started to shrink but has not disappeared completely, the patient is advised to stop taking acyclovir and chlorhexidine gluconate mouthwash 0.2% and continue taking multivitamins and using vaseline albums.
Follow-up 3 months later, the lesions seemed to have disappeared, the pain and soreness had completely disappeared. The patient has not taken any medication and in the past 3 months the lesions have not reappeared.
Conclusion
Complete examination of the herpes labialis patient is very important to establish accurate diagnosis. All this can improve the healing process and quality of life of the patient.
Consent Statements
The patient has approved and written informed consent for the publication of this case report, including the images. The institution has also approved the publication of this article.
Acknowledgments
The authors would like to thank the patient who generously participated in this study and also thank Padjadjaran University; Department of Oral Medicine, Faculty of Dentistry, Padjadjaran University; and the staff of Dental Hospital Padjadjaran University.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Suniti S, Setiadhi R. Infeksi herpes simpleks virus 1 rekuren dengan faktor predisposisi stres emosional Recurrent herpes simplex virus 1 infection with predisposing factors of emotional stress. J Kedokteran Gigi Univ Padjadjaran. 2018;30(3):207. doi:10.24198/jkg.v30i3.17964
2. Megawati A, Hidayat W. Lifestyle potential against recurrent intraoral herpes recurrence rate: a case series. Makassar Dent J. 2022;11(1):25–28. doi:10.35856/mdj.v11i1.503
3. Mahfaza H, Sufiawati I, Satari MH. Prevalensi dan pola penyakit infeksi virus rongga mulut di RSUP Dr. Hasan Sadikin Bandung tahun 2013-2017. Padjadjaran J Dent Res Stud. 2019;3(1):50–56. doi:10.24198/pjdrs.v3i1.22180
4. Glick M. Burket’s Oral Medicine 13th. USA: Wiley Blackwell; 2021:32.
5. Zakiawati D, Farisyi MA, Wahyuni IS. Clinical variability of recurrent oral HSV-1 infection with a high level of serum IgG antibody: three case reports. Clin Case Rep. 2021;9(9):3–9. doi:10.35856/mdj.v11i1.503
6. Gopinath D, Koe KH, Maharajan MK, Panda S. A Comprehensive Overview of Epidemiology, Pathogenesis and the Management of Herpes Labialis. Viruses. 2023;15(1):1–17. doi:10.3390/v15010225
7. Dwiarie TA, Zakiawati D, Hidayat W. Clinical Response Difference between Acyclovir and Valacyclovir in Recurrent Intraoral Herpes: adaptation Treatment in Pandemic Situation. e-Gigi. 2022;10(1):149. doi:10.35790/eg.v10i1.39267
8. Lin HS, Lin PT, Tsai YS, Chi CC. Interventions for treatment of herpes labialis (cold sores on the lips). Cochrane Database Syst Rev. 2022;2022(12). doi:10.1002/14651858.CD015216
9. Fatahzadeh M, Schwartz RA. Human herpes simplex labialis. Clin Exp Dermatol. 2007;32(6):625–630. doi:10.1111/j.1365-2230.2007.02473.x
10. Nath P, Kabir MA, Doust SK, Ray A. Diagnosis of herpes simplex virus: laboratory and point-of-care techniques. Infect Dis Rep. 2021;13(2):518–539. doi:10.3390/idr13020049
11. Hasanah NT, Hidayat W. Stress as Trigger Factor of HSV-1 Reactivation Causing Recurrent Intraoral Herpes Mimicking HAEM: a Case Report. Int Med Case Rep J. 2022;15(December):699–706. doi:10.2147/IMCRJ.S388708
12. Hakiman FA, Suharti N, Bahar E. Kajian Literatur: efektivitas Antiseptik Yang Mengandung Chlorhexidine Gluconate Terhadap Bakteri MRSA. J Ilmu Kesehat Indones. 2022;2(2):95–105. doi:10.25077/jikesi.v2i2.553
13. Scan_buku_compresed_Obat_Topikal_Untuk_Lesi_Mulut.
14. Álvarez DM, Castillo E, Duarte LF, et al. Current Antivirals and Novel Botanical Molecules Interfering With Herpes Simplex Virus Infection. Front Microbiol. 2020;11(February):1–19. doi:10.3389/fmicb.2020.00139
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.