Back to Journals » International Medical Case Reports Journal » Volume 19
Atypical Bilateral Iris Transillumination without Pigment Dispersion: A Case Report Suggestive of BAIT
Authors Mancini M ![]() , Brancato C
, Brancato C ![]() , Meduri A
, Meduri A ![]() , Lo Giudice G
, Lo Giudice G
Received 22 April 2026
Accepted for publication 30 June 2026
Published 9 July 2026 Volume 2026:19 619028
DOI https://doi.org/10.2147/IMCRJ.S619028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Maura Mancini,1 Claudio Brancato,2 Alessandro Meduri,1 Gregorio Lo Giudice2
1Department of Biomedical Sciences, Ophthalmology Clinic, University of Messina, Messina, Italy; 2Department of Ophthalmology, ARNAS Civico Hospital, Palermo, Italy
Correspondence: Maura Mancini, Email [email protected]
Introduction: Bilateral Acute Iris Transillumination (BAIT) is a rare ocular condition characterized by acute iris depigmentation, pigment dispersion in the anterior chamber, sphincter paralysis, and frequently elevated intraocular pressure. However, atypical presentations may occur, complicating diagnosis and expanding the clinical spectrum of the disease.
Case Presentation: A 25-year-old woman presented with acute onset of severe photophobia associated with migraine and visual aura. Slit-lamp examination revealed bilateral diffuse 360° iris transillumination and nearly fixed atonic mydriasis, in the absence of pigment dispersion, anterior chamber inflammation, or intraocular pressure elevation. Systemic evaluation revealed recent respiratory illness and associated dermatologic manifestations. No ocular treatment was initiated due to the absence of inflammatory signs or ocular hypertension. Photophobia resolved spontaneously, while iris abnormalities persisted.
Conclusion: This case suggests a possible pigment-negative or incomplete variant of BAIT, characterized by the absence of pigment dispersion and normal intraocular pressure. Recognition of such atypical presentations is essential to avoid misdiagnosis and unnecessary treatment, and may contribute to a broader understanding of the clinical spectrum and pathophysiology of BAIT.
Keywords: bilateral acute iris transillumination, BAIT, iris transillumination, mydriasis, photophobia
Introduction
Bilateral Acute Iris Transillumination (BAIT) is an uncommon ocular syndrome characterized by acute and severe iris transillumination, pigment dispersion in the anterior chamber, sphincter paralysis with mydriatic pupils, and, in many cases, transient elevation of intraocular pressure.1–4
It has been increasingly recognized over the last decade as a distinct clinical entity, although its pathogenesis remains incompletely understood.1,4 Cases have frequently been reported after upper respiratory tract infections and, in some patients, after systemic exposure to fluoroquinolones, particularly moxifloxacin, suggesting either a post-infectious or drug-related mechanism in susceptible individuals.1,3–5
From a clinical perspective, BAIT may represent a considerable diagnostic challenge because it can mimic other causes of iris depigmentation or pupillary abnormalities, including bilateral acute depigmentation of the iris (BADI), pigment dispersion syndrome, herpetic iridocyclitis, Adie tonic pupil, and pharmacologic mydriasis.1,2,4 Nevertheless, incomplete or atypical presentations may occur and risk being underrecognized, particularly when hallmark features such as pigment dispersion or intraocular pressure elevation are absent.4
Here, we report the case of a young woman presenting with bilateral diffuse iris transillumination and nearly fixed atonic mydriasis, but without anterior chamber pigment dispersion or ocular hypertension, in the setting of a recent respiratory illness and associated dermatologic manifestations. This presentation appears to be consistent with an atypical or incomplete form of BAIT and may further expand the currently recognized clinical spectrum of the disease.
Case Presentation
A 25-year-old woman presented to the ophthalmic emergency department with acute onset of severe photophobia associated with migraine and occasional visual aura. She denied any prior history of migraine or similar visual symptoms.
Her past ocular history was unremarkable, although previous ophthalmologic records were not available. She reported occasional use of cannabis and hashish, as well as a single lifetime exposure to intranasal cocaine. No recent use of topical or systemic medications, including antibiotics, was reported.
At presentation, best-corrected visual acuity (BCVA) was 20/20 in both eyes. Slit-lamp examination revealed bilateral, nearly fixed atonic mydriasis with poor or absent light response. Diffuse 360° iris transillumination was observed in both eyes (Figures 1 and 2). The cornea was clear in both eyes. Slit-lamp examination with specular illumination revealed no evidence of a Krukenberg spindle or pigment deposition on the corneal endothelium. The anterior chamber was deep and quiet, with no evidence of pigment dispersion, cells, or flare. Intraocular pressure was within normal limits in both eyes. Gonioscopic examination using a Goldmann three-mirror lens revealed open iridocorneal angles for 360° in both eyes, without evidence of Sampaolesi line, pseudoexfoliative material, iris neovascularization, or pathological trabecular pigmentation. These findings further supported the exclusion of pigment dispersion syndrome, pseudoexfoliation syndrome, and other anterior segment disorders. Fundus examination was unremarkable.
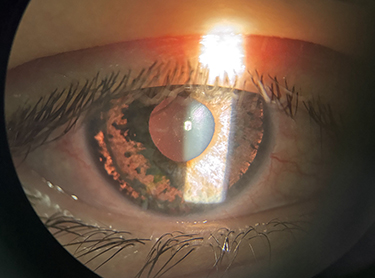 |
Figure 1 Slit-lamp photograph of the right eye showing diffuse 360° iris transillumination associated with nearly fixed atonic mydriasis. No pigment dispersion or anterior chamber inflammation is evident. |
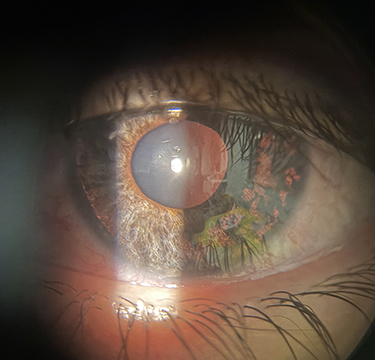 |
Figure 2 Slit-lamp photograph of the left eye demonstrating symmetric bilateral iris transillumination and atonic mydriasis. The absence of pigment release and inflammatory signs supports an atypical presentation compatible with a pigment-negative variant of Bilateral Acute Iris Transillumination (BAIT). |
Optic nerve head evaluation revealed a normal appearance in both eyes, without glaucomatous cupping or other suspicious findings. Spectral-domain OCT (Heidelberg Engineering) of the retinal nerve fiber layer and ganglion cell layer showed values within normal limits bilaterally. Visual field testing was not performed, as there was no evidence suggestive of glaucomatous optic neuropathy based on the patient’s age, normal gonioscopic findings, and the absence of structural optic nerve abnormalities.
Systemic evaluation revealed associated dermatologic findings, including progressive pruritus, diffuse skin desquamation, dermographism, and dry lips. The patient reported an episode of acute bronchitis occurring approximately 10–15 days prior, possibly associated with fever, although no antibiotic therapy was confirmed. The patient had no known history of drug, food, or environmental allergies. Laboratory testing showed mild leukocytosis.
Given the absence of anterior chamber inflammation, pigment dispersion, or intraocular pressure elevation, a conservative management approach was adopted, and no ocular therapy was initiated. Differential diagnoses requiring urgent treatment, including uveitis and acute angle-closure glaucoma, were considered unlikely based on the absence of intraocular inflammation, normal intraocular pressure, open iridocorneal angles on gonioscopy, and normal structural optic nerve findings. The patient was closely monitored.
Over the following days, photophobia gradually resolved spontaneously, while slit-lamp findings—including iris transillumination and atonic mydriasis—remained stable and unchanged.
Discussion
This case represents a diagnostic challenge characterized by bilateral diffuse iris transillumination and atonic mydriasis in the absence of anterior chamber pigment dispersion or intraocular pressure elevation. Bilateral Acute Iris Transillumination (BAIT) is a relatively recently described clinical entity, first reported by Tugal-Tutkun et al, typically characterized by acute pigment dispersion, diffuse iris transillumination, sphincter paralysis, and frequently elevated intraocular pressure.1–4 In most reported cases, pigment release into the anterior chamber represents a key diagnostic feature and is often associated with early ocular hypertension due to trabecular meshwork obstruction.1,3,4,6 In contrast, our patient showed no evidence of pigment dispersion at any stage of the disease and maintained normal intraocular pressure throughout the clinical course. This finding is highly unusual and suggests a possible incomplete or variant form of BAIT, in which iris epithelial damage occurs without significant pigment liberation into the anterior chamber. Recent reports and reviews suggest that BAIT may represent a spectrum disorder, with variability in clinical presentation and severity.4,6,7 The temporal association with a recent respiratory illness is consistent with previous reports supporting a post-infectious mechanism.1,4,7 In addition, exposure to fluoroquinolones, particularly moxifloxacin, has been implicated in several cases, raising the possibility of a toxic or immune-mediated pathogenesis.3,5,8 However, in our patient, no antibiotic exposure was documented, further supporting a non-drug-related trigger.
Interestingly, the presence of dermatologic manifestations, including pruritus, desquamation, and dermographism, has not been previously described in association with BAIT. These findings may suggest a broader systemic inflammatory or hypersensitivity response, potentially supporting an immune-mediated mechanism. However, this association remains speculative and warrants further investigation.
Differential diagnosis was carefully considered. Pigment dispersion syndrome was unlikely due to the absence of trabecular pigmentation and intraocular pressure elevation.6 Bilateral acute depigmentation of the iris (BADI) represents the main differential diagnosis of BAIT, as both conditions predominantly affect young adults and may occur following upper respiratory tract infections. However, several clinical features help distinguish these two entities. BADI is characterized by diffuse or patchy stromal depigmentation without iris transillumination defects, preservation of pupillary function, and the absence of significant pigment dispersion or intraocular pressure elevation. In contrast, BAIT typically presents with diffuse iris transillumination, marked pigment release into the anterior chamber, sphincter paralysis resulting in atonic or poorly reactive mydriasis, and transient ocular hypertension in a substantial proportion of cases. These observations are consistent with previous reports highlighting the overlap and potential diagnostic challenges between BAIT and BADI, as described by Kawali et al9 In our patient, the presence of bilateral diffuse iris transillumination and nearly fixed atonic mydriasis strongly favored a diagnosis within the BAIT spectrum, despite the unusual absence of pigment dispersion and elevated intraocular pressure, supporting the hypothesis of a pigment-negative or incomplete variant of BAIT.2,7 Herpetic iridocyclitis may present with iris atrophy and pupillary abnormalities, but is usually unilateral and associated with inflammation.10 Adie tonic pupil typically presents unilaterally and is not associated with diffuse iris transillumination. Pharmacologic mydriasis was excluded based on clinical history and persistence of pupillary abnormalities. The clinical course was self-limiting, with spontaneous resolution of photophobia and no need for therapeutic intervention. This benign evolution is in line with previously reported BAIT cases, although structural iris changes and pupillary dysfunction may persist over time.1,4
Overall, this case may represent a pigment-negative or incomplete variant of BAIT, expanding the currently recognized clinical spectrum of the disease. Awareness of such atypical presentations is essential to avoid misdiagnosis and unnecessary treatment, particularly in the absence of intraocular inflammation or intraocular pressure elevation.
This report has several limitations. Although extensive clinical evaluation, including gonioscopy and structural optic nerve assessment, supported the exclusion of several alternative diagnoses, pigment dispersion syndrome cannot be completely ruled out. Furthermore, this case does not fully meet the established diagnostic criteria for BAIT, as neither pigment dispersion nor intraocular pressure elevation was observed. Therefore, our findings should be interpreted cautiously and considered suggestive of an atypical, pigment-negative, or incomplete presentation rather than a definitive form of BAIT. Additional studies and further case reports are needed to better characterize the full clinical spectrum and underlying pathophysiology of this condition.
Conclusion
This case highlights an atypical presentation of Bilateral Acute Iris Transillumination (BAIT) characterized by diffuse iris transillumination and atonic mydriasis in the absence of pigment dispersion and intraocular pressure elevation. Such findings support the existence of a pigment-negative or incomplete variant of BAIT, expanding its currently recognized clinical spectrum. Awareness of these atypical presentations is essential to avoid misdiagnosis and unnecessary treatment, particularly when inflammatory signs and ocular hypertension are absent. Further studies are needed to better clarify the underlying pathophysiology and potential systemic associations of this condition.
Ethics Approval and Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. Institutional approval was not required for this case report in accordance with local regulations.
Consent for Publication
The patient provided written informed consent for publication of clinical details and images.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tugal-Tutkun I, Onal S, Garip A, et al. Bilateral acute iris transillumination. Arch Ophthalmol. 2011;129(10):1312–5. doi:10.1001/archophthalmol.2011.310
2. Tranos PG, Wickremasinghe SS, Stangos NT, et al. Bilateral acute depigmentation of the iris. Eye. 2006;20(12):1479–1481. doi:10.1038/sj.eye.6702369
3. Morshedi RG, Singh K, Sacher BA, Boldt HC. Bilateral acute iris transillumination syndrome associated with moxifloxacin use. JAMA Ophthalmol. 2015;133(1):109–111. doi:10.1001/jamaophthalmol.2014.3931
4. Perone JM, Chaum E. Bilateral acute iris transillumination: review of the literature. Curr Opin Ophthalmol. 2019;30(6):492–497.
5. Eadie BD, Etminan M, Maberley DAL. Oral fluoroquinolones and the risk of uveitis. JAMA Ophthalmol. 2015;133(1):38–43.
6. M WB-R, Brouwers K, van Langenhove L, et al. Uveitis-like syndrome after oral moxifloxacin. Ophthalmology. 2009;116(10):1848–1855.
7. Papasavvas I, et al. Bilateral acute iris transillumination and depigmentation syndromes: a review. Surv Ophthalmol. 2021;66(4):592–606.
8. Chang DF, Braga-Mele R, Mamalis N, et al. Clinical experience with pigment dispersion and iris abnormalities. Ophthalmology. 2012;119(7):1230–1235.
9. Kawali A, Mahendradas P, Shetty R. Acute depigmentation of the iris: a retrospective analysis of 22 cases. Can J Ophthalmol. 2019;54(1):33–39. doi:10.1016/j.jcjo.2018.03.020
10. Miserocchi E, Fogliato G, Bianchi I, Bandello F, Modorati G. Clinical features of ocular herpetic infection. Ocul Immunol Inflamm. 2013;21(3):210–218.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship of Atropine in Controlling Myopia Progression Among Pediatric Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Almusib RBA, Awad AH, Ghandorah AM, AnbarSerry AOM, Aljumah HK, Albarak AI, Alghanmi RM, Alshami FME, Alhejaili BFR, Alboqami AFF, Mohayya EMH, Almatrafi AM, Alzuwayr MA
Clinical Ophthalmology 2026, 20:590501
Published Date: 21 April 2026