Back to Journals » Patient Preference and Adherence » Volume 16
Attributes Characterizing Colorectal Cancer Screening Tests That Influence Preferences of Individuals Eligible for Screening in Germany: A Qualitative Study
Authors Brinkmann M ![]() , von Holt I, Diedrich L, Krauth C
, von Holt I, Diedrich L, Krauth C ![]() , Seidel G, Dreier M
, Seidel G, Dreier M
Received 7 March 2022
Accepted for publication 24 June 2022
Published 10 August 2022 Volume 2022:16 Pages 2051—2066
DOI https://doi.org/10.2147/PPA.S365429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Melanie Brinkmann, Isabell von Holt, Leonie Diedrich, Christian Krauth, Gabriele Seidel, Maren Dreier
Institute for Epidemiology, Social Medicine and Health Systems Research, Hannover Medical School, Hannover, Germany
Correspondence: Melanie Brinkmann, Institute for Epidemiology, Social Medicine and Health Systems Research, Hannover Medical School, Hannover, Germany, Email [email protected]
Purpose: This qualitative study is part of the SIGMO study, which evaluates general populations’ preferences for colorectal cancer (CRC) screening in Germany using a discrete choice experiment. Attribute identification and selection are essential in the construction of choice tasks and should be evidence-based ensuring that attributes are relevant to potential beneficiaries and contribute to overall utility. Therefore, this qualitative study aims to identify relevant attributes characterizing CRC screening tests from the perspective of those eligible for screening in Germany.
Patients and Methods: Individuals aged 50 to 60 were purposively selected. A questioning route was developed and piloted. Four focus groups (FG) (n=20) were conducted (November 2019) with two moderators and one observer each. FGs were audio recorded, transcribed, and analyzed using qualitative content analysis. Attributes were deductively assigned based on a priori identified attribute categories, and inductively derived.
Results: Across FGs, 24 attributes (n=293 codes) were discussed, five of which (sedation, inability to work, transportation home, predictive values, waiting time for screening colonoscopy) were inductively derived (n=76 codes). Four attributes identified a priori were not addressed in any FG. The most frequently discussed attribute category was procedural characteristics, followed by measures of screening test validity, benefits, harms, and structural characteristics of health care. The most commonly addressed attributes were preprocedural bowel cleansing, kind of procedure, and predictive values.
Conclusion: Newly identified attributes characterizing CRC screening tests from an individual’s perspective, and a priori identified attributes not addressed by any FG stress the added value of qualitative research and thereby the importance of applying a mix of methods in identifying and selecting attributes for the construction of choice tasks. This study meets the requirements for a transparent and detailed presentation of the qualitative methods used in this process, which has rarely been the case before.
Keywords: focus groups, qualitative study, colorectal cancer screening, attribute identification, discrete choice experiment
Introduction
In Germany, the general population aged 50 and older can decide between immunochemical fecal occult blood testing and colonoscopy within an organized colorectal cancer (CRC) screening program.1 However, participation rates are low. In 2018, 23% and 7.4% of 50- to 54-year-old women and men, respectively, considered a stool-based test.2 One-year colonoscopy uptake was 2.6% and 2.5% among 55 to 64 year old women and men, respectively.2 Evidence-based sigmoidoscopy, proven to reduce CRC incidence as well as mortality and recommended for individuals who reject a colonoscopy, is currently not part of the program.1,3–5
The SIGMO (Sigmoidoscopy as an evidence based colorectal cancer screening test – a possible option?) study evaluates whether sigmoidoscopy should be additionally offered for CRC screening in Germany.6 Part of the study is a discrete choice experiment (DCE) to determine general populations’ preferences for CRC screening. A DCE is a stated preference elicitation method that originates from (health) economics.7 Individuals are presented with several choice tasks, each of which consists of at least two, contrasting alternatives.8 The alternatives are defined by several attributes, each with different levels, representing the (hypothetical) health-related products or services of interest. For each choice task, individuals are asked to choose the alternative they most prefer.8–10 Attributes finally included in a DCE should be relevant to the target population and have an impact on the overall utility associated with the respective alternatives.9 Therefore, the identification and selection of the attributes is essential and should be supported by evidence based on, eg, systematic reviews as well as qualitative research.9,11
Qualitative research reflects the perspectives and needs of potential beneficiaries with respect to a particular health-related service or good, enabling the participation of those who are directly affected by regulatory decisions on health care, for example.12 Though recommended, the use of qualitative methods in the process of identifying and selecting attributes has often only been stated in previous DCE publications, but without reporting the methodological approaches and results in detail.13,14 To address this gap, and to consider the potential target populations’ perspectives in the process of identifying and selecting attributes for the DCE in the SIGMO study, the objective of this qualitative study was to identify attributes characterizing CRC screening tests that are relevant for individuals eligible for screening in Germany.
Materials and Methods
Focus groups (FG) were conducted as this method encourages participants to communicate with each other, revealing individuals’ experiences, attitudes, and needs.15 The reporting of this qualitative study was based on the COREQ (Consolidated criteria for reporting qualitative research) checklist.16 The SIGMO study is registered at the German Clinical Trials Register (DRKS00019010), and a study protocol was published.6
Theoretical Framework
A priori identified attributes based on systematic reviews, eg,17,18 and international primary studies eliciting average-risk populations’ stated preferences for CRC screening, eg,19–22 including an own systematic review currently submitted (Appendix 1), provided the theoretical framework for the data collection and analysis of this qualitative study (Table 1). The extracted attributes had been grouped into the six categories: procedure-related characteristics, test characteristics, benefits, harms, structural characteristics of health care, and level of evidence.
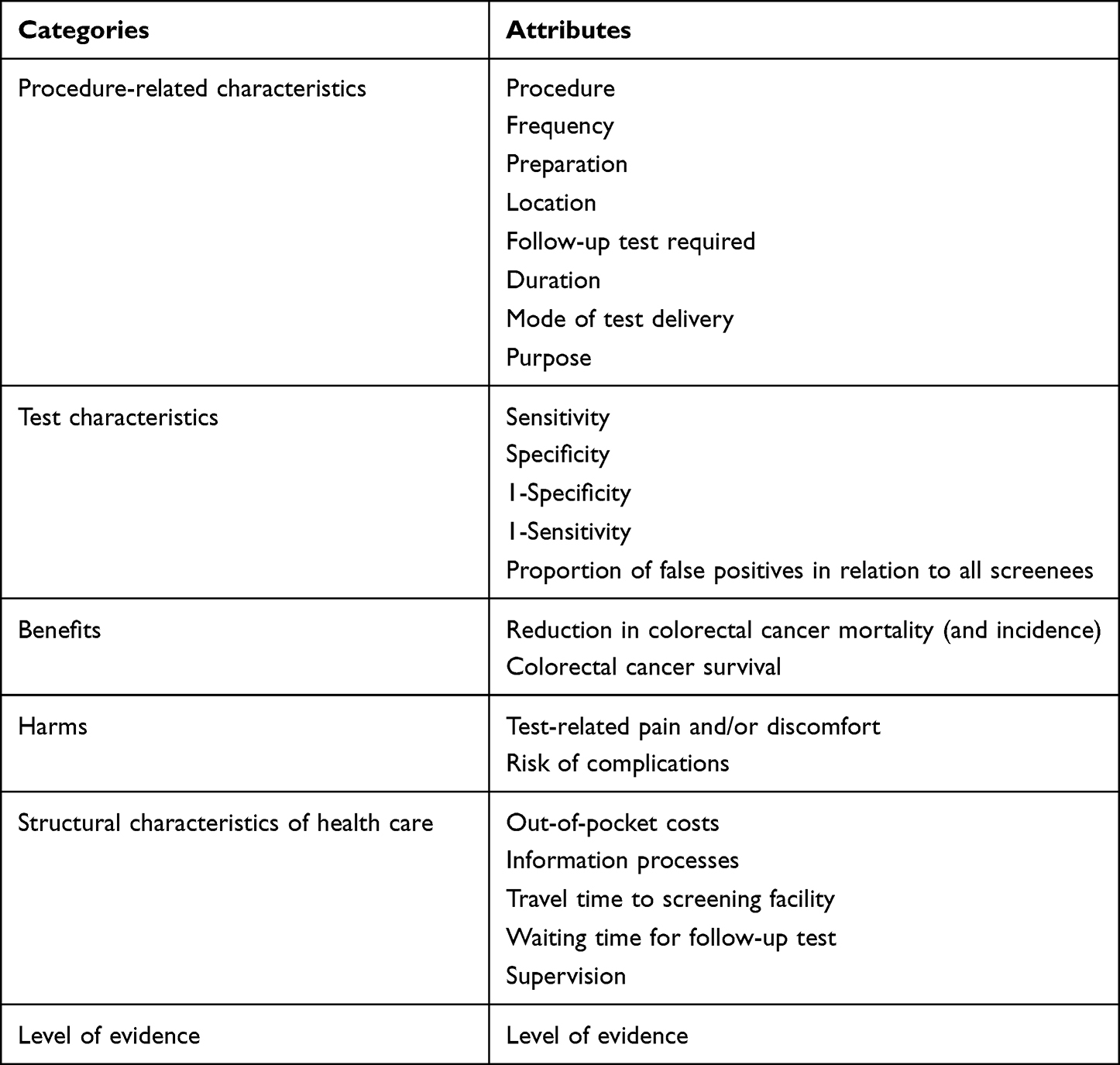 |
Table 1 A Priori Identified Attributes Characterizing Colorectal Cancer Screening Tests by Categories |
Participant Selection
Individuals aged 50 to 60 who had never been diagnosed with CRC or an inflammatory bowel disease, such as ulcerative colitis or Crohn’s disease, were eligible. Participants were selected purposefully based on the demographic characteristics of sex and prior colonoscopy experience.23,24 In October and November 2019, they were approached face-to-face at events of the Hannover Medical School’s Patient University,25 via flyers displayed at facilities of the Hannover Medical School and posted in letter boxes of a nearby residential area, and via an announcement on the intranet of the Hannover Medical School. To assess eligibility of potential participants and to obtain relevant information for group assignment, a short questionnaire was used during the first contact. Four FGs with a total of 20 participants were realized in November 2019.
Setting
All FGs took place in a conference room at the Hannover Medical School. To maximize different perspectives within each group situation,15 the four FGs were heterogeneously composed as follows: FG 1) women and men with previous colonoscopy experience (n=6), FG 2) women and men without previous colonoscopy experience (n=5), FG 3) men with and without previous colonoscopy experience (n=5), and FG 4) women with and without previous colonoscopy experience (n=4). For FG 4, 7 participants were originally recruited, 3 of which dropped out at short notice due to illness. See Table 2 for a description of the sample.
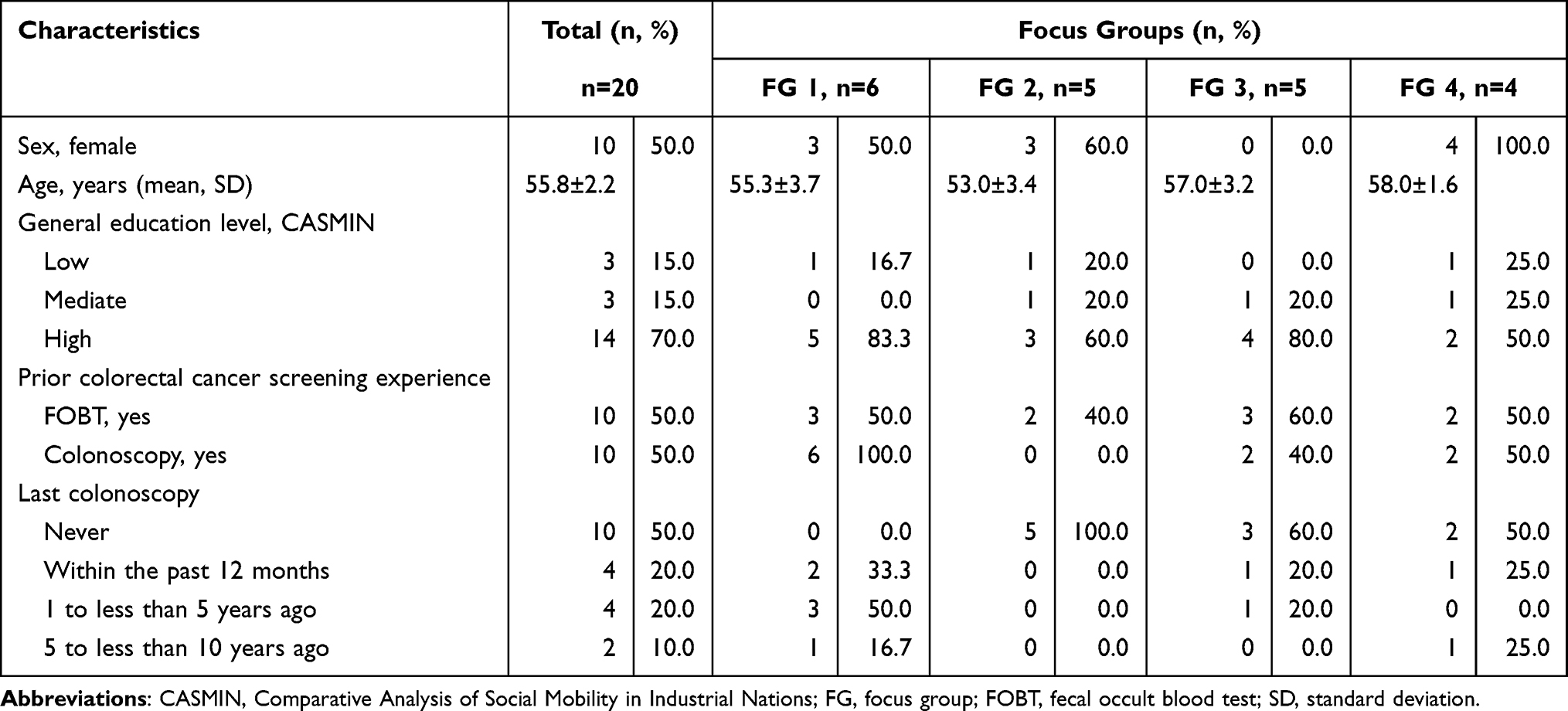 |
Table 2 Self-Reported Characteristics of Focus Group Participants (n=20) |
Data Collection
To ensure consistency of questions and information provided across all four FGs, a questioning route was developed based on the attributes identified a priori and on discussions within the research team.26 Prior to conducting the first FG, the questioning route was pilot tested in a group situation in early November 2019 with 5 individuals representing potential participants and researchers who were unfamiliar with the study. Each FG started with a short introduction by the moderator (MB) on study background, tape recording, voluntariness of participation, and discussion guidelines.26 The questions that followed could be assigned to five categories: 1) opening, 2) introductory phase on initial thoughts about CRC screening, 3) transition phase on attributes in which CRC screening tests differ from each other and which are perceived as reasons for or against participation, 4) key phase on the importance of the identified attributes for decision-making, and 5) ending.26 At the end of the transition phase, participants received background information on fecal testing and colonoscopy from the moderator (MB), which was based on the content of the information material provided for the general population as part of the organized screening program for CRC in Germany.27,28 See Table 3 for the introductory, transition, and key questions used. Attributes described or mentioned by participants were summarized and grouped thematically on a whiteboard by the assistant moderator (LD) during the FGs. In addition, an observer (LMF) was present who took field notes and photographically documented the overview of collected attributes per FG. At the end of each FG, participants completed an anonymous short questionnaire on socio-demographics.
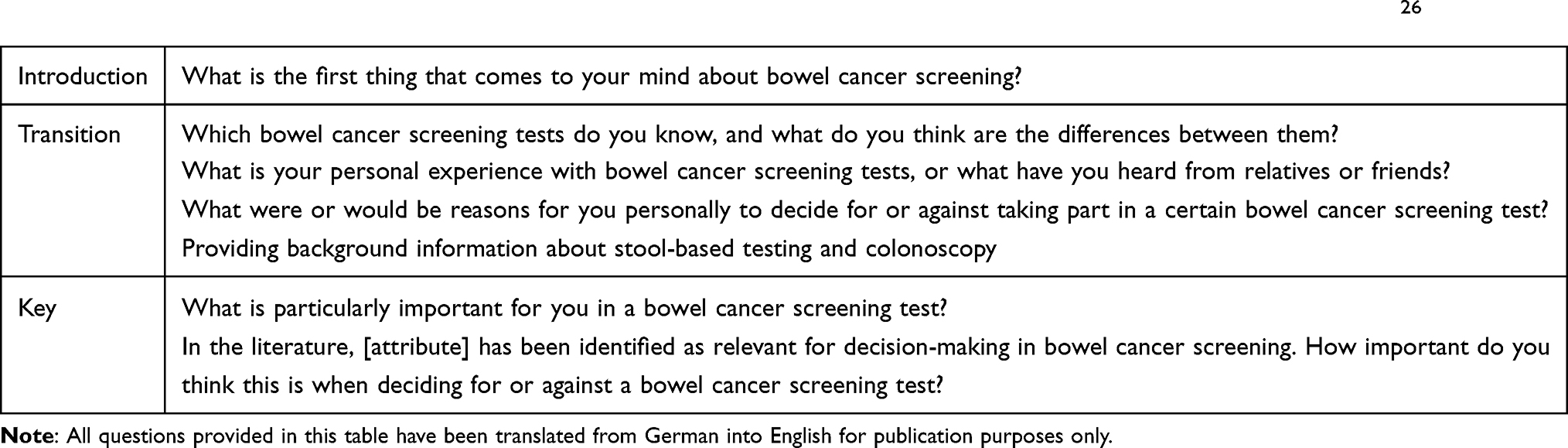 |
Table 3 Introductory, Transition, and Key Questions Used in the Focus Groups, Based on Morgan and Krueger 199826 |
All participants gave written informed consent at the beginning of each FG. The FGs lasted between 90 and 150 minutes and were audio recorded. Each participant received an expense allowance of € 50.
Data Analysis
The audio recorded FGs were transcribed. Data were analyzed using qualitative content analysis with categories derived deductively and inductively.29 For deductive category assignment, a coding guideline with definitions of the attribute categories identified a priori and coding rules for allocating text passages to categories were developed.30 Two data coders (MB, IVH) independently went through the transcripts line by line for category assignment. After the coding process of the transcripts of FG 1, FG 2, and FG 4 was completed, the codes were checked for inter-coder agreement and the coding guideline was adjusted and revised where necessary. For inductive category derivation, the two data coders worked through the transcripts independently, line by line, generating new categories by paraphrasing, generalizing, and reducing the text material.30 Inter-coder agreement was checked after the paraphrasing process was completed for the transcripts of FG 1, FG 2, and FG 4. Generalization of paraphrases was done jointly by both data coders. First and second reductions were performed by one data coder (MB). A second one (IVH) checked them independently and made changes where necessary. Disagreements in both deductive category assignment and inductive category derivation were resolved by discussion. Where no agreement was reached, a third person (MD) was included. Data analysis was conducted using MAXQDA (VERBI Software, Berlin, Germany; 2020, Version 20.4.0). Answers to the opening question were not included in the analysis.
Results
The analysis of all four FGs yielded 293 coded text passages and a total of 24 attributes related to CRC screening tests, 19 of which were deductively assigned (n=217 codes) and 5 inductively derived (n=76) (Tables 4 and 5). Compared to the others, significantly fewer relevant text passages were identified in FG 4.
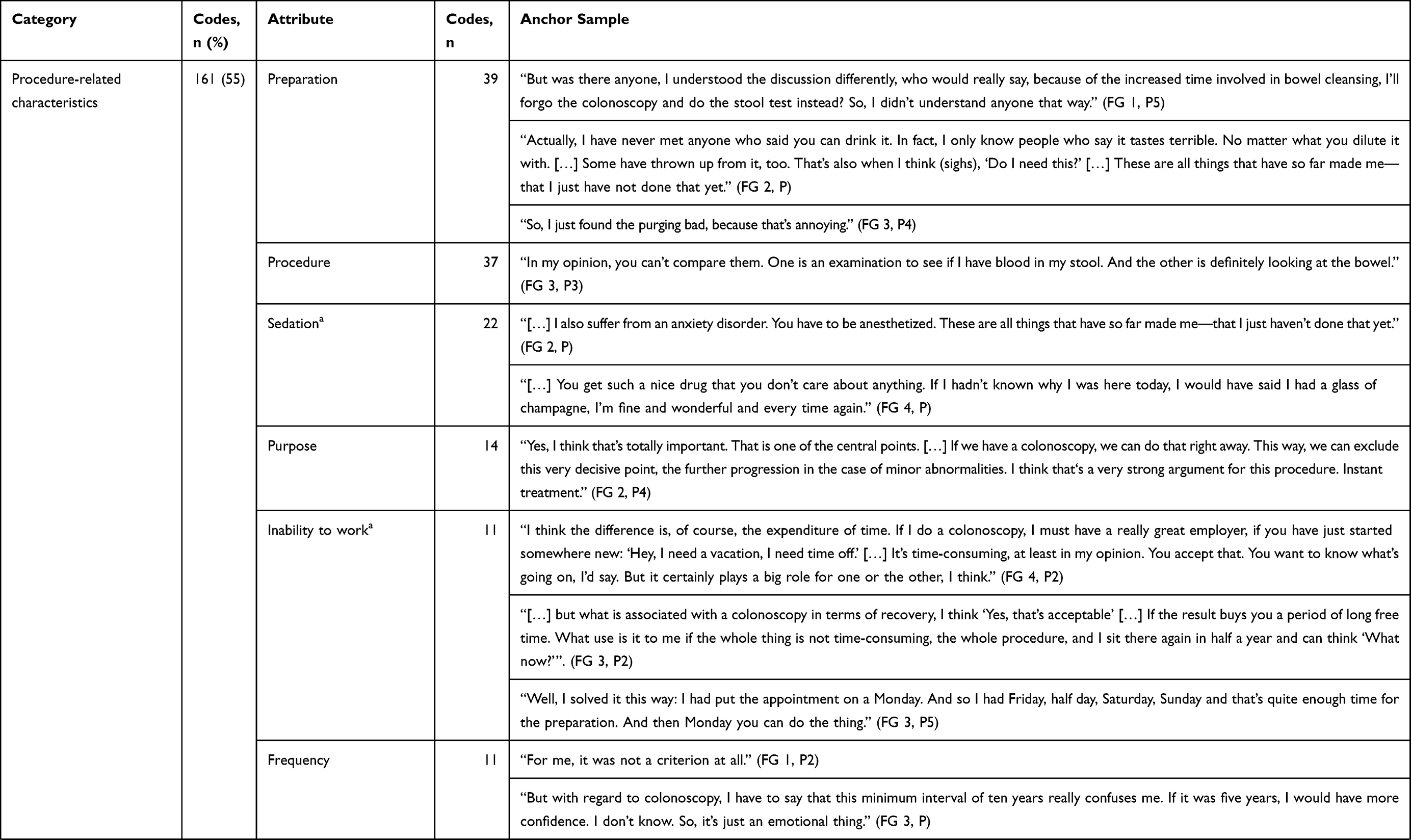 | 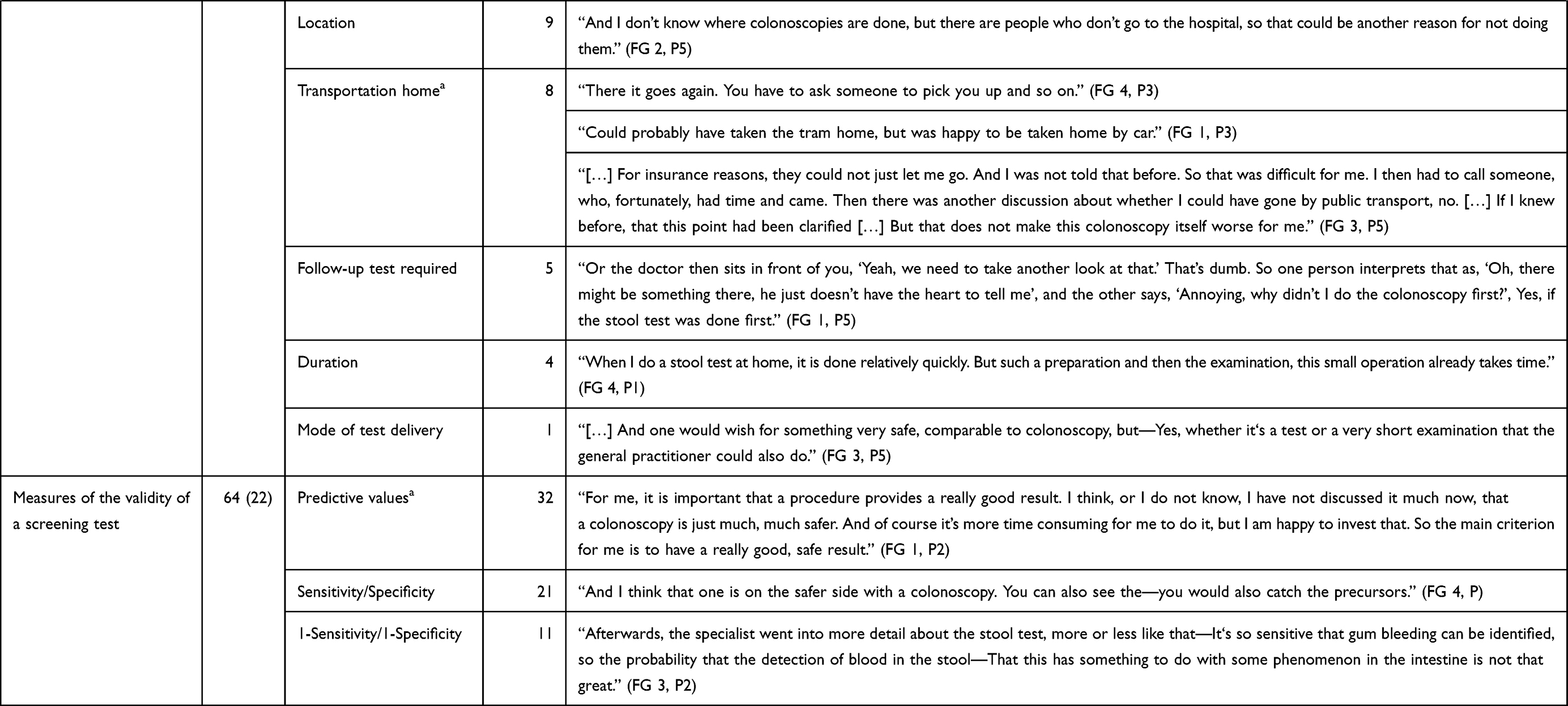 | 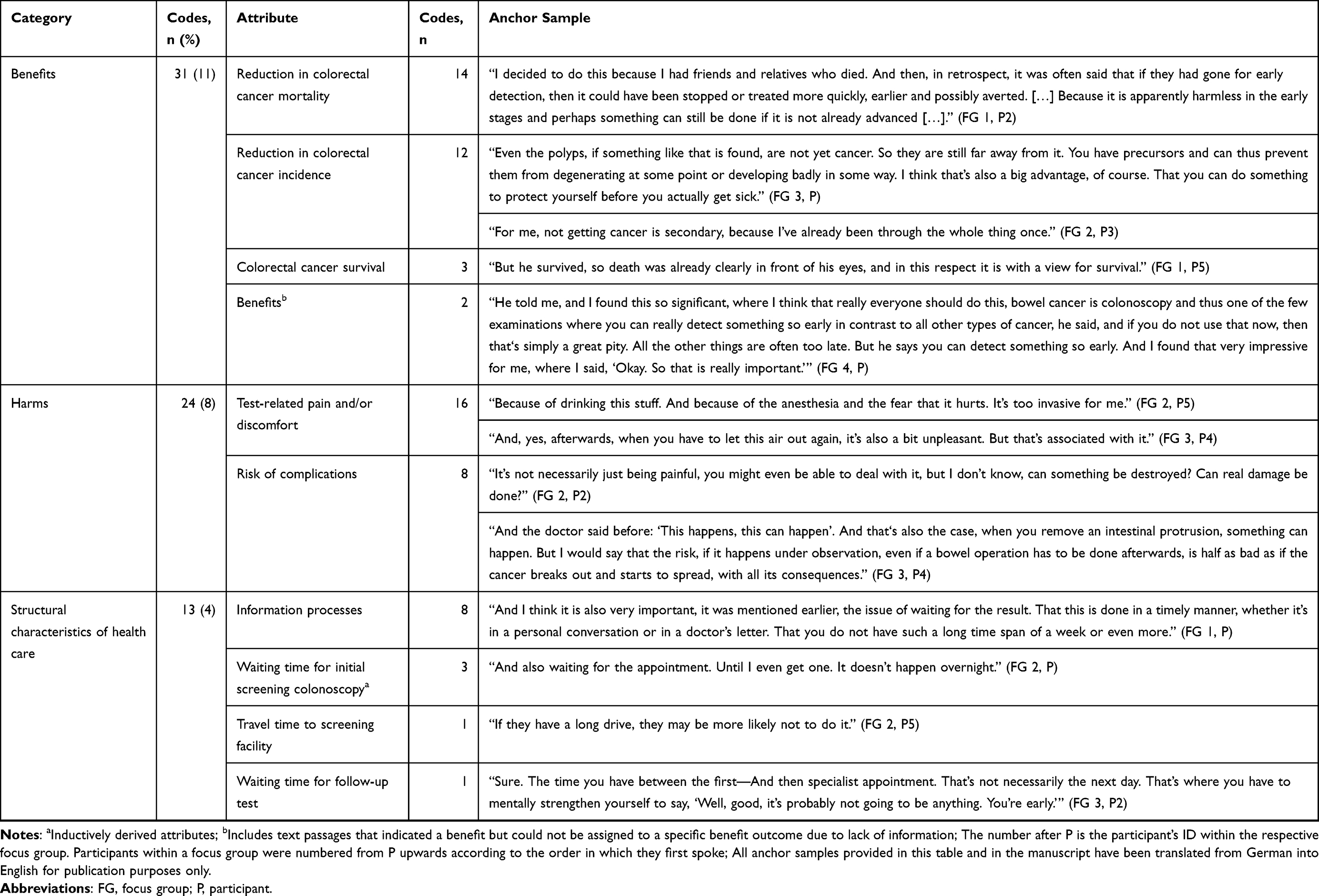 |
Table 4 Deductively Assigned (n=19; n=217 Codes) and Inductively Derived (n=5; n=76 Codes) Attributes Related to Colorectal Cancer Screening Tests, Their Relevance for Decision-Making, and Anchor Samples Across All Four Focus Groups |
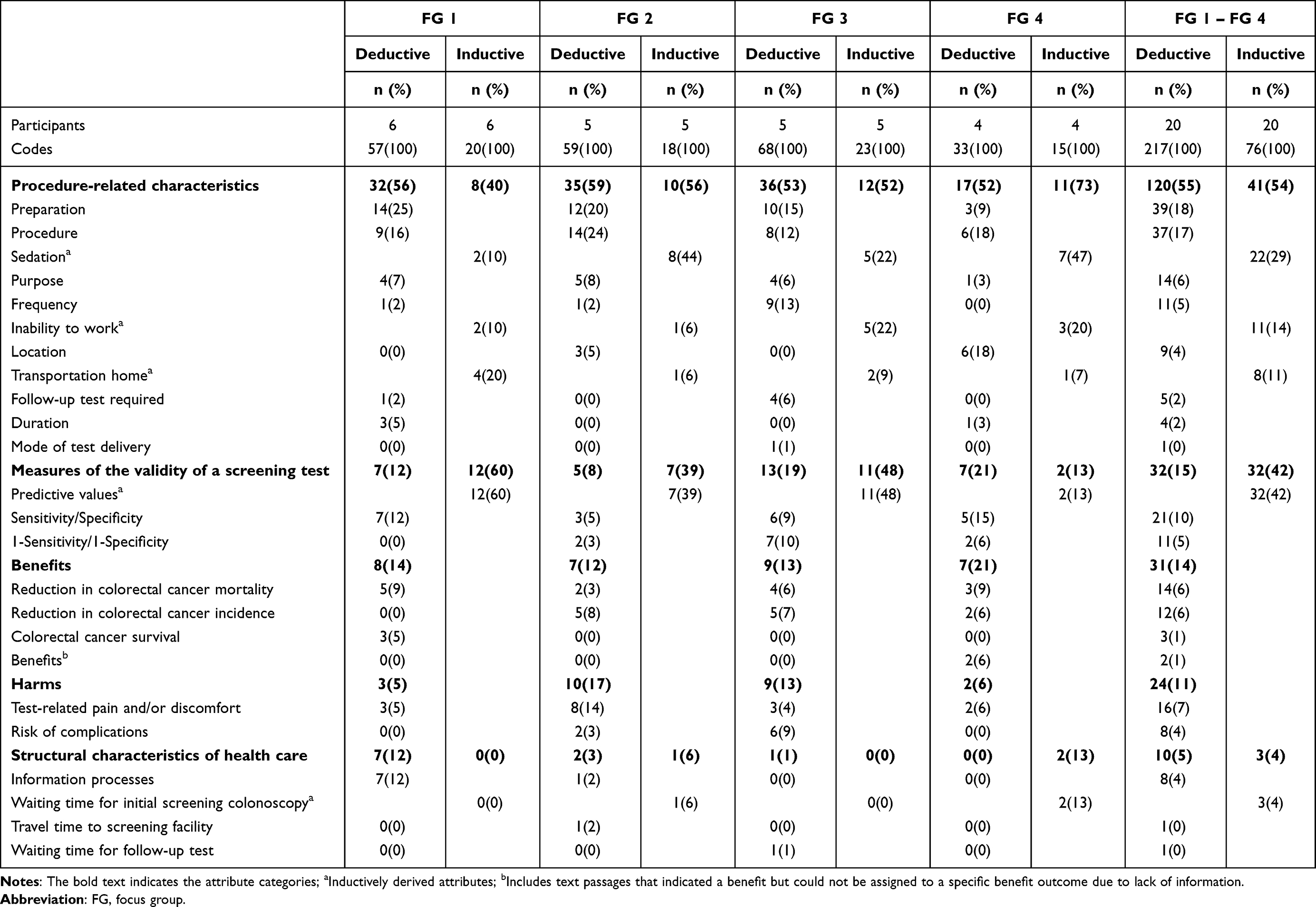 |
Table 5 Identified Attributes (n, %): Deductively Assigned (n=19; n=217 Codes) and Inductively Derived (n=5; n=76 Codes) Attributes Related to Colorectal Cancer Screening Tests Within and Across All Four Focus Groups |
Deductively Assigned Attributes
Of the attributes identified a priori, all but four (proportion of false positives in relation to all screenees, out-of-pocket costs, supervision, level of evidence) were discussed in at least one FG. Half of all codes (n=120) addressed attributes on procedure-related characteristics, followed by attributes on test characteristics (n=32 codes), benefits (n=31), harms (n=24), and structural characteristics of health care (n=19). While colonoscopy-naïve participants did not discuss duration, mode of test delivery, and colorectal cancer survival, individuals with previous colonoscopy experience did not address travel time to the screening facility and waiting time for follow-up (Appendices 2 and 3). No text passages on follow-up, mode of test delivery, and waiting time for follow-up were coded from women.
Category: Procedure-Related Characteristics
Bowel preparation (n=16 participants; Appendix 4), kind of procedure (n=17), and purpose (n=10) were discussed in all FGs. While some stated that preprocedural bowel cleansing was not decision-relevant, although it was perceived as time-consuming, disgusting, or unpleasant, the aspect of preparation was interpreted as being relevant for others. On CRC screening procedures, opposing opinions were expressed, suggesting that this attribute could have a positive or negative impact on decision-making, depending on its specification. Stool-based testing, for example, was described as unhygienic, disgusting, or difficult due to sanitary conditions
I don’t find this test very pleasant, I must say. Because I don’t find it very hygienic. It’s difficult for me, for example, this deep toilet bowl, where you don’t know how to handle the whole thing properly. [FG 1, P6]
but also as simple and unproblematic (“Well, I know the stool test […]. This is relatively simple.” FG 2, P3). Comparably, a colonoscopy was perceived as more extensive because the whole colon can be examined, but also as invasive, complicated, or time-consuming (“Much cheaper than an invasive colonoscopy, which is completely uncomfortable and everyone is afraid of.” FG 2, P5). In addition, some participants mentioned the wish for alternative screening tests: “I would like to have something, I go there, they take blood from me. I don’t think that’s so great either, but that would be the lesser evil for me.” (FG 2, P). A screening test’s ability to remove polyps or collect tissue samples was described as a benefit, an important property, a strong argument for participating in a colonoscopy, and an advantage of a colonoscopy over stool testing: “And what I also find good in a colonoscopy, if there are polyps that represent nothing malignant, they can be removed immediately” (FG 1, P4).
Test frequency was addressed differently in three FGs (FG 1, FG 2, FG 3; n=7 participants). Some perceived a higher interval as reassuring, or preferred a test that, besides having high accuracy, needs to be done as infrequently as possible:
So if you’re really worried about your health, then of course a shorter time interval is better. Sure, it makes a difference to wait ten years, oh God, what happens until next time? No, then I’ll just do a stool test, I can do it again next year. If you’re really worried about your health, that’s actually very important. [FG 2, P2]
Others preferred a colonoscopy regardless of the recommended frequency because preventing CRC was valued the most (“If that means doing it every year, then so be it. If it means I can prevent cancer.” FG 3, B3), or clearly stated that frequency was not important to them at all. Location (FG 2, FG 4; n=6 participants), follow-up (FG 1, FG 3; n=2), and duration (FG 1, FG 4; n=4) were each discussed in two FGs, and mode of test delivery was addressed in FG 3: A participant described the wish for an alternative screening modality that has comparable accuracy to a colonoscopy but can be performed by a primary care physician.
Category: Test Characteristics
Participants (n=15) in all FGs discussed a screening test’s sensitivity and specificity. A colonoscopy was described as more precise, more accurate, or more reliable than stool-based tests, whereas for fecal testing it was suggested that it can detect abnormalities only by chance or, if at all, late: “Only what it should detect, it shows relatively late or when it is already very advanced.” (FG 3, P). Others expressed a wish for alternative screening tests with an accuracy comparable to a colonoscopy but less time-consuming, or stated that they would accept higher expenditure for a more reliable test.
Three FGs (FG 2, FG 3, FG 4; n=9 participants) addressed the probability of misclassifying true positives or negatives (1-sensitivity and 1-specificity). Participants discussed, for example, that a positive stool test result may be due to polyps, CRC, or hemorrhoids, and therefore no conclusion can be made about the true cause: “Is it even possible to determine that this may be due to cancerous intestinal villi?” (FG 2, P4). They also considered, eg, whether fecal testing can miss abnormalities, and therefore a colonoscopy would be more reliable.
Category: Benefits
Reduction in CRC mortality was indirectly addressed in all four FGs (n=10 participants). Some explained that the death of relatives or acquaintances due to CRC was pivotal for them in deciding to participate in screening, or that the screening-induced early detection of CRC allows for better treatment:
Yes, that in case of doubt, the cancer is detected very early and can be treated accordingly. And since we know that bowel cancer is treatable if it is detected early enough, I can say: ‘What’s wrong with the examination?’. [FG 3, P3]
The respective attribute identified a priori was defined as a reduction in CRC mortality (and incidence) because the reduction in cancer-specific incidence was, if at all, described only in combination with mortality reduction.19,31 In three FGs (FG 2, FG 3, FG 4), however, participants (n=7) addressed incidence reduction as an independent attribute by stating, eg, that the prevention of CRC is perceived as an advantage of a colonoscopy, or that the ability to prevent CRC was decisive for them to participate in a colonoscopy: “In principle, of course, the most important thing is to remove the cancer so that it does not develop in the first place.” (FG 2, P4). As a consequence, reduction in CRC incidence was deductively assigned as a separate attribute.
CRC survival was raised as a relevant attribute in FG 1 (n=2 participants) by stating that CRC can be survived if diagnosed early through screening, or that the decision to participate in screening was influenced by relatives having survived CRC.
Category: Harms
In all FGs, participants (n=13) discussed test-related pain or discomfort. Some described that they felt mild pain after a colonoscopy, for example, or that a colonoscopy without sedation was not possible due to pain. Others indicated that pain or fear of pain were reasons for deciding against participating in a colonoscopy, suggesting that a corresponding attribute would be considered in their respective decision-making processes.
Risk of complications was addressed in two FGs (FG 2, FG 3; n=7 participants). In one, complications were described as more important compared to test-related pain or discomfort. In the other, opposing opinions were expressed: On the one hand, complications were described as important (“And for me, side effects, complications are always incredibly important”, FG 3, P) and must be appropriate compared to the benefit of a screening test
If my doctor told me, ‘I am going to do a colonoscopy, and in every second colonoscopy I’m going to perforate the bowel, and then you’re going to have to stay in the hospital for three weeks’, I probably wouldn’t do that as a screening examination. [FG 3, P3]
while on the other hand, complications were weighed against, eg, the risk of traffic accidents, and were considered secondary to the possibility of developing CRC.
Category: Structural Characteristics of Health Care
Two FGs (FG 1, FG 2; n=10 participants) addressed information processes such as information about test results and the waiting time required for communication of test results. In both cases, some indicated that it was important from their point of view, eg, to communicate test results, to come out of a medical examination with a result, or to not wait too long for information about test results. Others pointed out that test result communication is too infrequent: “And that educational talk before and also afterwards. That’s not done enough” (FG 2, P3).
Participants (n=2) in FG 2 assumed that long(er) travel times to the screening facility might be a reason, eg, for the elderly or rural population to decide against participating in a colonoscopy. Waiting time for a follow-up was described as challenging by one participant in FG 3 due to concerns about whether or not the positive result of the initial screening test actually means CRC.
Inductively Derived Attributes
Five attributes related to CRC screening tests (sedation, inability to work, transportation home, predictive values, waiting time for initial screening colonoscopy) were inductively derived. Half of the coded text passages (n=41) accounted for the three procedure-related characteristics sedation, inability to work, and transportation home, 32 codes for predictive values, and 3 for waiting time for initial screening colonoscopy. The latter was not discussed by both individuals with previous colonoscopy experience and men (Appendices 2 and 3).
Category: Procedure-Related Characteristics
Sedation (n=16 participants; Appendix 4), inability to work (n=14), and transportation home (n=10) were addressed in all FGs. Sedation was accepted by some as part of the examination. For others, sedation caused anxiety, was valued negatively, and was stated as a reason to decide against participation in a colonoscopy: “I’m not one of them myself, but I know a lot of people who wouldn’t have something like that done, just because of the anesthesia” (FG 2, P3). In contrast, others felt that sedation might be helpful in cases of anxiety about an examination, and some indicated that they would only participate in a colonoscopy if sedation was provided:
Because I had asked my gastroenterologist if it would be possible for me to be admitted as an inpatient for a day and I could get it under general anesthesia so that I see and hear absolutely nothing. [FG 4, P3]
An inability to work due to preprocedural bowel cleansing or the examination itself was also associated with varying and sometimes opposing expressions. Some suggested, for example, that this attribute might be considered depending on the particular professional activity:
It’s not an issue for me, but I could imagine that there are many who think about it and say: ‘Wait a minute, you might be away for two days, do you take holiday for that? Do you get a certificate of incapacity?’ […] Where they might think, why should I do that now? [FG 1, P]
This was confirmed by a participant in FG 4 who stated that inability to work is perceived as time-consuming and problematic because employers’ kindness is required. While some participants made it clear that this attribute is considered in decision-making (“I can only think of one more argument when deciding for or against a procedure. Of course, a sick day also plays a role.” FG 2, P5), others indicated that inability to work can be minimized if planned appropriately, that the additional organizational burden is not a reason to decide against a colonoscopy (“This doesn’t mean that I wouldn’t have the examination, but of course it has an impact: when, how, where?” FG 3, P3), or that this attribute is accepted and valued secondary to the perceived benefits.
Transportation home by an adult due to sedation was valued as desirable, relieving, and reassuring by some participants: “Having a familiar person around was reassuring for me” (FG 1, P6). In addition, it was noted that it is also possible to be picked up by a cab. Others felt that transportation home was time-consuming
Then I have to get a lift for the way back because I’m sedated. […] It’s all an effort, the total package. Any influence on my life, the effect on that I find relevant. [FG 2, P4]
annoying, and problematic. The additional organizational effort due to transportation home was specified by a participant as having to be compatible with the accompanying person’s daily routine.
Category: Measures of the Validity of a Screening Test
Text passages addressing the accuracy of screening test results were coded as predictive values, defined as the probability of having (or not having) a condition of interest given a positive (or negative) test result.32 Predictive values are measures of the validity of a screening test.33 This also applies to the deductively assigned attributes sensitivity, specificity, 1-sensitivity, and 1-specificity, which is why the test characteristics category has been renamed accordingly.33
Participants (n=17) in all FGs discussed predictive values, stating that they considered the results of a colonoscopy to be more conclusive and reliable than those of stool-based testing, allowing for a more certain and detailed diagnosis:
But […] for me personally: this test—I don’t know, it would have, no matter what the result would have been—I don’t really have confidence in it, I have to say. I have much more confidence in a colonoscopy—just as a definitive diagnosis. [FG 3, P]
Some indicated that they would accept a higher level of effort or testing frequency for a more reliable test result, or that their expectations of the accuracy of a test result were related to the effort of the particular screening modality. Others associated reliability or benefit with the fact that CRC can be ruled out in the case of a negative colonoscopy result, or that an appropriate treatment can be derived if a colonoscopy tests positive:
Yes, a confirmation that cancer is actually there, or a relief. Yes, and relief, okay, then you look for something else. And if there is something, then therapy. [FG 2, P5]
Contrarily, some participants stated that a stool test result is sufficiently informative for the purpose of early detection, which is perceived as reassuring (“Yes, but for my inner feeling, I have to say: Well, if nothing is found with the stool test, then I go home feeling good.” FG 3, P2), even though it is not as accurate as that of a colonoscopy.
Category: Structural Characteristics of Health Care
Participants (n=2) in two FGs (FG 2, FG 4) described waiting time for a screening colonoscopy as time-consuming, negative, and as one of the reasons for deciding not to have a colonoscopy:
If I hadn’t heard so many negative things, I would be willing to undergo a colonoscopy. […] And also that the time it takes to get an appointment is pretty long, as it is with any specialist. [FG 4, P2]
Discussion
The objective of this qualitative study was to identify relevant attributes characterizing CRC screening tests from the perspective of individuals eligible for screening in Germany. Based on four FGs with a total sample size of 20 participants, 24 attributes were identified. All attributes identified a priori, except four (proportion of false positives in relation to all screenees, out-of-pocket costs, supervision, level of evidence), were discussed in at least one FG. Five new attributes were inductively derived and implemented into the a priori category system: sedation, inability to work, transportation home (procedure-related characteristics), predictive values (measures of screening tests’ validity), and waiting time for a screening colonoscopy (structural characteristics of health care). With the exception of the latter, all newly identified attributes were addressed in all FGs, regardless of previous colonoscopy experience and sex. Across FGs, procedural characteristics was the most frequently addressed attribute category, followed by measures of the validity of a screening test, benefits, harms, and structural characteristics of health care. The most common attributes were preprocedural bowel cleansing, kind of procedure, and predictive values.
A major strength of this qualitative study is the extraction of five attributes that, to the best of our knowledge, have not been included as separate attributes in previous DCE surveys eliciting general populations’ preferences for CRC screening tests, eg.17,18 Besides needing further research for theoretical validation, this finding stresses the importance of applying a mixed-methods design in identifying and selecting attributes for a DCE to ensure that the final attributes used to characterize the alternatives available for choice are relevant to the target population and have an impact on overall utility.9,11,14
Sedation is an attribute in which screening tests differ from each other: While sedation is not required for fecal testing, data from England show that a diagnostic colonoscopy is almost always performed under conscious sedation.34 Similar results are also available from Germany, where sedation is given in 86.6% of screening colonoscopies.35 In contrast, a sigmoidoscopy is rarely performed under sedation. In a study of 7713 individuals undergoing routine flexible sigmoidoscopy in NHS Greater Glasgow and Clyde, sedation was used in only 23% of cases, and in a survey of German physicians, about 65% reported performing sedation in a maximum of 10% of all sigmoidoscopies.36,37 In addition, sedation can be associated with side effects: A multicenter randomized trial of CRC screening in Italy found that dizziness after discharge was more common in participants who had a colonoscopy with sedation than in those who had undergone this examination unsedated.38
Inability to work due to preprocedural bowel cleansing or the examination itself and transportation home due to sedation are two attributes that reflect the impact of screening on daily life.38 Although related to sedation, they were coded as independent attributes considering different subject focuses in participants’ expressions.38 In a study assessing the patient-rated importance of key information on a screening colonoscopy among 370 insured persons in Germany, information about whether one can go home alone after the procedure and whether one will be able to work on the day of the procedure were valued as important by 63% and 50% of respondents, respectively.39 However, there were significant differences by sex (going home alone after the procedure) and education level.39 While the results of this qualitative study do not enable comparable conclusions, they do, however, suggest different and sometimes opposing perspectives on these procedural characteristics. Corresponding attributes included in a DCE may contribute differently to overall utility depending on sociodemographic characteristics or previous screening experience. This potential preference heterogeneity should be considered when analyzing choice data through, eg, further subgroup analyses or latent-class models.8,40
Information on predictive values is considered much more appropriate for individual decision-making in (cancer) screening than reporting test characteristics such as sensitivity or specificity that may lead to overestimating the benefits of a test.41,42 The relevance of predictive values at an individual level was confirmed by the results of this qualitative study, in which predictive values are among the most frequently discussed attributes. Remarkably, a comparable attribute was not identified in any of the previous stated preference elicitation studies that most frequently included sensitivity to describe the test characteristics, eg.17,18 This indicates that profound knowledge of evidence-based information strategies is essential in the construction of choice tasks for the general population.
Another discovery of this qualitative study was that participants in three FGs addressed a screening test’s ability to reduce cancer-specific incidence as an independent attribute. A comparable attribute was included in only two studies eliciting stated preferences of the general population for CRC screening modalities, and in both cases combined with the reduction of cancer-specific mortality.19,31 However, especially the reduction of CRC incidence represents an important benefit outcome in which common CRC screening tests differ from each other: While stool-based testing only affects CRC mortality through early detection, endoscopic procedures can also reduce CRC incidence by removing precancerous lesions.4,43,44 This makes sigmoidoscopy and colonoscopy, along with cervical smear testing, the only common cancer screening procedures that are effective in terms of cancer prevention.42,43 Consequently, attributes on incidence and mortality reduction describe important different benefit outcomes and should be implemented as separate attributes.
Attributes identified a priori but not addressed in any of the FGs included proportion of false positives in relation to all screenees,45–48 supervision,46 and level of evidence for a screening test’s validity and benefit,49,50 each of which were considered in very few other studies eliciting general populations’ preferences for CRC screening tests. In contrast, out-of-pocket costs have been used as an attribute in many internationally conducted DCE surveys, eg.18,20,22 A possible explanation for why a comparable attribute was not discussed in any of the FGs could be that participation in CRC screening is completely covered by statutory health insurance for eligible individuals in Germany.
This qualitative study has limitations, and our results and interpretations do not claim to be exhaustive or generalizable. First, individuals with a low or mediate general education level were underrepresented, indicating selection bias. In addition, participants of the Hannover Medical School’s Patient University were recruited, among others, who may represent a group particularly interested in learning about health-related topics. Second, in FG 4, a group dynamic developed from strong requests for information by the two colonoscopy-naïve participants. Although the moderator (MB) actively tried to stimulate discussion, eg, by repeating questions or encouraging everyone to speak, significantly fewer relevant text passages could be extracted from this group for analysis. One reason could be the heterogeneous group composition. Possibly, in a more homogeneous FG, the colonoscopy-naïve women would have been more inclined to discuss their reasons for or against participation in CRC screening or the relevance of different attributes related to screening tests for their decision-making. Another reason could be the group size: Due to 3 women dropping out at short notice, only 4 people in total participated in this FG. However, 4 to 8 participants are discussed as an ideal group size for FGs.15 Third, although no new attributes were obtained in FG 4, indicating theoretical saturation, it cannot be excluded that further FGs with a different composition might have yielded new results.16 Last, the results and interpretations were not returned to the participants for feedback and thus could not be validated.16
Conclusions
This qualitative study contributed significantly to the identification of new attributes characterizing CRC screening tests from an individual’s perspective, which requires further research for theoretical validation. Inductively derived attributes, and a priori identified attributes that were not addressed by any FG stress the added value of qualitative research and the importance of using a mix of methods in attribute identification and selection, ensuring that the final attributes used to describe the alternatives available for choice in a DCE are evidence-based, relevant, and contribute to overall utility. This study meets the requirements of transparently reporting the use of qualitative methods in this process in detail, which has rarely been the case before.
Abbreviations
COREQ, Consolidated criteria for reporting qualitative research; CRC, colorectal cancer; DCE, discrete choice experiment; FG, focus group; SIGMO, “Sigmoidoscopy as an evidence based colorectal cancer screening test – a possible option?” study.
Ethics Approval and Informed Consent
This study complied with the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Hannover Medical School (reference number 8671_BO_K_2019). Participation in focus groups was voluntary and based on written informed consent including the right to refuse or withdraw at any time without any disadvantages, and the analysis of anonymized data in accordance with the purpose of the study, which also comprises publication.
Acknowledgments
We thank Lara Marleen Fricke for her assistance with data collection.
Author Contributions
Funding acquisition: Maren Dreier, Christian Krauth. Project administration: Maren Dreier, Christian Krauth. Supervision: Maren Dreier, Christian Krauth, Gabriele Seidel. Methodology: Melanie Brinkmann, Maren Dreier, Christian Krauth, Gabriele Seidel. Investigation: Melanie Brinkmann, Leonie Diedrich. Formal analysis: Melanie Brinkmann, Isabell von Holt. Visualization: Melanie Brinkmann. Writing-original draft: Melanie Brinkmann. Writing-review and editing: Melanie Brinkmann, Isabell von Holt, Leonie Diedrich, Christian Krauth, Gabriele Seidel, Maren Dreier. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the German Federal Joint Committee’s Innovation Fund (grant number 01VSF18007). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Melanie Brinkmann, Isabell von Holt, Leonie Diedrich, Christian Krauth, and Maren Dreier declare that they have received research grants from the German Federal Joint Committee’s Innovation Fund (grant number 01VSF18007). Gabriele Seidel has no competing interests to declare that are relevant to the content of this article.
References
1. Federal Joint Committee. Germany: Richtlinie für organisierte Krebsfrüherkennungsprogramme [Directive on organized cancer screening programs]; 2022. Available from: https://www.g-ba.de/richtlinien/104/.
2. Steffen A, Holstiege J, Hagen B, Akmatov MK, Bätzing J. Germany: Inanspruchnahme der Darmkrebsfrüherkennung in den Jahren 2009 bis 2018: Eine Bestandsaufnahme auf Basis bundesweiter vertragsärztlicher Abrechnungsdaten [Participation in colorectal cancer screening in Germany: results from nationwide claims data (2009–2018)]; 2020. Available from: https://www.versorgungsatlas.de/fileadmin/ziva_docs/108/VA_Abstract_en_20-02_Darmkrebsfr%C3%BCherkennung_2020-05-14.pdf.
3. German Guideline Program in Oncology (German Cancer Society, German Cancer Aid, AWMF). S3-guideline colorectal cancer, long version 2.1, 2019, AWMF registration number: 021-007OL; 2019. Available from: https://www.leitlinienprogramm-onkologie.de/leitlinien/kolorektales-karzinom/.
4. Jodal HC, Helsingen LM, Anderson JC, Lytvyn L, Vandvik PO, Emilsson L. Colorectal cancer screening with faecal testing, sigmoidoscopy or colonoscopy: a systematic review and network meta-analysis. BMJ Open. 2019;9(10):e032773. doi:10.1136/bmjopen-2019-032773
5. Brenner H, Stock C, Hoffmeister M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ. 2014;348:g2467. doi:10.1136/bmj.g2467
6. Brinkmann M, Diedrich L, Krauth C, Robra B-P, Stahmeyer JT, Dreier M. General populations’ preferences for colorectal cancer screening: rationale and protocol for the discrete choice experiment in the SIGMO study. BMJ Open. 2021;11(1):e042399. doi:10.1136/bmjopen-2020-042399
7. Mühlbacher A, Johnson FR. Choice experiments to quantify preferences for health and healthcare: state of the practice. Appl Health Econ Health Policy. 2016;14(3):253–266. doi:10.1007/s40258-016-0232-7
8. Ryan M, Gerard K, Amaya-Amaya M. Using Discrete Choice Experiments to Value Health and Health Care. Dordrecht: Springer; 2008.
9. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health- a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
10. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making. A user´s guide. Pharmacoeconomics. 2008;26(8):661–677. doi:10.2165/00019053-200826080-00004
11. Coast J, Al-Janabi H, Sutton EJ, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21(6):730–741. doi:10.1002/hec.1739
12. Pope C, Mays N. Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research. BMJ. 1995;311(6996):42–45. doi:10.1136/bmj.311.6996.42
13. Vass C, Rigby D, Payne K. The role of qualitative research methods in discrete choice experiments. Med Decis Making. 2017;37(3):298–313. doi:10.1177/0272989X16683934
14. Hall R, Medina-Lara A, Hamilton W, Spencer AE. Attributes used for cancer screening discrete choice experiments: a systematic review. Patient. 2021;15:269–285. doi:10.1007/s40271-021-00559-3
15. Kitzinger J. Introducing focus groups. BMJ. 1995;311(7000):299–302. doi:10.1136/bmj.311.7000.299
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Marshall D, McGregor SE, Currie G. Measuring preferences for colorectal cancer screening. Patient. 2010;3(2):79–89. doi:10.2165/11532250-000000000-00000
18. Wortley S, Wong G, Kieu A, Howard K. Assessing stated preferences for colorectal cancer screening: a critical systematic review of discrete choice experiments. Patient. 2014;7(3):271–282. doi:10.1007/s40271-014-0054-3
19. Pignone MP, Brenner AT, Hawley S, et al. Conjoint analysis versus rating and ranking for values elicitation and clarification in colorectal cancer screening. J Gen Intern Med. 2012;27(1):45–50. doi:10.1007/s11606-011-1837-z
20. Ramezani Doroh V, Delavari A, Yaseri M, Sefiddashti SE, Akbarisari A. Preferences of Iranian average risk population for colorectal cancer screening tests. Int J Health Care Qual Assur. 2019;32(4):677–687. doi:10.1108/IJHCQA-08-2017-0151
21. de Bekker-Grob EW, Swait JD, Kassahun HT, et al. Are healthcare choices predictable? The impact of discrete choice experiment designs and models. Value Health. 2019;22(9):1050–1062. doi:10.1016/j.jval.2019.04.1924
22. Phisalprapa P, Ngorsuraches S, Wanishayakorn T, Kositamongkol C, Supakankunti S, Chaiyakunapruk N. Estimating the preferences and willingness-to-pay for colorectal cancer screening: an opportunity to incorporate the perspective of population at risk into policy development in Thailand. J Med Econ. 2021;24(1):226–233. doi:10.1080/13696998.2021.1877145
23. Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18:179–183. doi:10.1002/nur.4770180211
24. Marshall MN. Sampling for qualitative research. Fam Pract. 1996;13(6):522–525. doi:10.1093/fampra/13.6.522
25. Seidel G, Kaiser B, Lander J, Dierks M-L. The Hannover Patient University: advanced mini-med school concept and evaluation results. Health Educ J. 2017;76(1):38–51. doi:10.1177/0017896916647751
26. Morgan DL, Krueger RA. The Focus Group Kit: Volumes 1–6. Thousand Oaks: SAGE Publications; 1998.
27. Institute for Quality and Efficiency in Health Care. Colonoscopy: information for women; 2021. Available from: https://www.informedhealth.org/colonoscopy-information-for-women.html.
28. Institute for Quality and Efficiency in Health Care. Stool test: information for men; 2021. Available from: https://www.informedhealth.org/stool-test-information-for-men.html.
29. Mayring P. Qualitative Content Analysis. Qual Soc Res. 2000;1(2). doi:10.17169/fqs-1.2.1089
30. Mayring P. Qualitative content analysis: theoretical foundation, basic procedures and software solution; 2014. Available from: https://www.ssoar.info/ssoar/bitstream/handle/document/39517/ssoar-2014-mayring-Qualitative_content_analysis_theoretical_foundation.pdf.
31. Brenner A, Howard K, Lewis C, et al. Comparing 3 values clarification methods for colorectal cancer screening decision-making: a randomized trial in the US and Australia. J Gen Intern Med. 2014;29(3):507–513. doi:10.1007/s11606-013-2701-0
32. Trevethan R. Sensitivity, specificity, and predictive values: foundations, pliabilities, and pitfalls in research and practice. Front Public Health. 2017;5:307. doi:10.3389/fpubh.2017.00307
33. Rothman RL, Montori VM, Cherrington A, Pignone MP. Perspective: the role of numeracy in health care. J Health Commun. 2008;13(6):583–595. doi:10.1080/10810730802281791
34. Ball AJ, Rees CJ, Corfe BM, Riley SA. Sedation practice and comfort during colonoscopy: lessons learnt from a national screening programme. Eur J Gastroenterol Hepatol. 2015;27(6):741–746. doi:10.1097/MEG.0000000000000360
35. Pox CP, Altenhofen L, Brenner H, Theilmeier A, von Stillfried D, Schmiegel W. Efficacy of a nationwide screening colonoscopy program for colorectal cancer. Gastroenterology. 2012;142(7):1460–7.e2. doi:10.1053/j.gastro.2012.03.022
36. Maliampurakal AJ, McMillan DC, Anderson JH, Horgan PG, Mansouri D. Factors associated with the efficacy of polyp detection during routine flexible sigmoidoscopy. Frontline Gastroenterol. 2018;9(2):135–142. doi:10.1136/flgastro-2017-100849
37. Cespedes I, Seidler U, Walter U, Dreier M. Physicians’ view on sigmoidoscopy as an additionally offered method for colorectal cancer screening. Z Gastroenterol. 2019;57(9):1059–1066. doi:10.1055/a-0963-0433
38. Senore C, Ederle A, Fantin A, et al. Acceptability and side-effects of colonoscopy and sigmoidoscopy in a screening setting. J Med Screen. 2011;18(3):128–134. doi:10.1258/jms.2011.010135
39. Dreier M, Krueger K, Walter U. Patient-rated importance of key information on screening colonoscopy in Germany: a survey of statutory health insurance members. BMJ Open. 2018;8(7):e019127. doi:10.1136/bmjopen-2017-019127
40. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR Conjoint Analysis Good Research Practices Task Force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.04.004
41. Bramwell R, West H, Salmon P. Health professionals’ and service users’ interpretation of screening test results: experimental study. BMJ. 2006;333(7562):284. doi:10.1136/bmj.38884.663102.AE
42. Pinsky PF. Principles of Cancer Screening. Surg Clin North Am. 2015;95(5):953–966. doi:10.1016/j.suc.2015.05.009
43. Bretthauer M, Kalager M. Principles, effectiveness and caveats in screening for cancer. Br J Surg. 2013;100(1):55–65. doi:10.1002/bjs.8995
44. Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for colorectal cancer: updated evidence report and systematic review for the US preventive services task force. JAMA. 2021;325(19):1978–1997. doi:10.1001/jama.2021.4417
45. Gyrd-Hansen D, Søgaard J. Analysing public preferences for cancer screening programmes. Health Econ. 2001;10(7):617–634. doi:10.1002/hec.622
46. Salkeld G, Ryan M, Short L. The veil of experience: do consumers prefer what they know best? Health Econ. 2000;9(3):267–270. doi:10.1002/(sici)1099-1050(200004)9:3<267:aid-hec511>3.0.co;2-h
47. Salkeld G, Solomon M, Short L, Ryan M, Ward JE. Evidence-based consumer choice: a case study in colorectal cancer screening. Aust N Z J Public Health. 2003;27(4):449–455. doi:10.1111/j.1467-842X.2003.tb00425.x
48. Nayaradou M, Berchi C, Dejardin O, Launoy G. Eliciting population preferences for mass colorectal cancer screening organization. Med Decis Making. 2010;30(2):224–233. doi:10.1177/0272989X09342747
49. Benning TM, Dellaert BGC, Dirksen CD, Severens JL. Preferences for potential innovations in non-invasive colorectal cancer screening: a labeled discrete choice experiment for a Dutch screening campaign. Acta Oncol. 2014;53(7):898–908. doi:10.3109/0284186X.2013.877159
50. Benning TM, Dellaert BGC, Severens JL, Dirksen CD. The effect of presenting information about invasive follow-up testing on individuals’ noninvasive colorectal cancer screening participation decision: results from a discrete choice experiment. Value Health. 2014;17(5):578–587. doi:10.1016/j.jval.2014.04.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.