Back to Journals » Clinical Optometry » Volume 18
Attitudes Towards the Use of Silicone Hydrogel Daily Disposable Contact Lenses (Verofilcon A) Among Neophyte Wearers: Results of a Short-Term Evaluation
Authors Zeri F ![]() , Tavazzi S
, Tavazzi S ![]() , Rizzo GC
, Rizzo GC ![]()
Received 22 November 2025
Accepted for publication 12 February 2026
Published 27 March 2026 Volume 2026:18 583712
DOI https://doi.org/10.2147/OPTO.S583712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
Fabrizio Zeri,1– 3 Silvia Tavazzi,1,2 Giulia Carlotta Rizzo1,2
1Department of Materials Science, University of Milano-Bicocca, Milan, Italy; 2Research Centre in Optics and Optometry (COMiB), University of Milano-Bicocca, Milan, Italy; 3College of Health and Life Sciences, Aston University, Birmingham, UK
Correspondence: Giulia Carlotta Rizzo, Department of Materials Science, University of Milano-Bicocca, Via Roberto Cozzi 55, Milan, I-20125, Italy, Tel +39 02 6448 5035, Email [email protected]
Purpose: To evaluate the intention to continue wearing silicone hydrogel daily disposable contact lenses (CLs) in verofilcon A (PRECISION1®, Alcon Laboratories, USA) among neophyte wearers after a short period of use and to identify potential factors influencing this intention.
Methods: A prospective, single-masked, single-arm clinical trial, was conducted at the University of Milano-Bicocca on ninety-five ametropic non-contact lens wearers (52 females and 43 males; mean age ± SD: 25.4 ± 5.3 years; range: 18– 40). Participants were fitted in verofilcon A daily disposable CLs, and after receiving training on lens application and removal, were instructed to wear them for 14 days (at least 5 days a week, minimum 5 hours a day). At the follow-up visit, participants completed a series of subjective evaluations (0– 100 visual analogue scales; VAS) referring to their experience over the 14-day with lens insertion and removal, comfort at insertion, end of day comfort, quality of vision, and overall satisfaction. They also rated their intention to continue CLs wear (0– 100 VAS scale) and indicated their main reasons for doing so.
Results: The mean (± SD) CL power prescribed was − 1.90± 1.42 D (range +2.00 to − 6.00) for the right eye and − 1.86± 1.43 D (range +1.50 to − 6.00) for the left eye. At the follow-up visit, monocular visual acuity with CLs was − 0.15± 0.08 logMAR in both eyes and − 0.20± 0.07 logMAR binocularly. Hierarchical regression analysis incorporating motivation-to-continue wear variables accounted for 57% of the variance. Three motivational factors (aesthetic, convenience, and sport) were significant predictors of the intention to continue CL wear.
Conclusion: Providing ametropic non-CL wearers with a structured, evidence-based CL fitting experience can be an effective strategy to promote long-term CL adoption. Behavioral intention to continue daily disposable CL wear was mainly influenced by motivational factors related to aesthetics, convenience and sport activities.
Keywords: daily disposable contact lenses, silicone hydrogels, attitudes
Introduction
Contact lens (CL) is a relatively common device for the correction of refractive errors, with an estimated 140 and 175 million wearers worldwide.1,2 Approximately 90% of CL wearers use soft lenses,3 and about 47% of fitting involve daily disposable lenses.4 In terms of materials, about 70% of CLs prescribed for daily wear are made of silicone hydrogels.5
Although the global number of CL wearers worldwide might appear large, it represents only a relatively small penetration into the potential market,6 and has remained fairly stable over the past decade.7 Understanding the diffusion of CLs among ametropic individuals requires the study of the mechanisms that drive the entry of new wearers on the one hand and the mechanisms that lead to discontinuation (a phenomenon known as dropout) on the other.
Important factors influencing the decision to wear CLs include the perceptions (benefits and barriers) and attitudes of ametropic individuals towards this corrective device, which has been extensively studied.6,8–16 Understanding these aspects provides valuable insights into key areas of the CL field, such as meeting patients’ needs, expanding market penetration among individuals requiring vision correction, and reducing dropout rates among existing wearers.
While aesthetics often drive initial interest, long-term use is typically motivated by convenience.8 Several studies have reported interesting effects of age, refractive errors, and sport participation on attitudes towards CL use.11–13 For young wearers, parental attitudes can act either as a barrier or a facilitating factor, and the perspectives of parents and children are not always aligned. For example, although strong evidence supports CLs as an effective, safe, and convenient correction modality for refractive errors also in children and adolescents,15,17 contributing significantly to enhance quality of life compared with glasses,9 parents often perceive CLs as less safe for adolescents than for adults.11
The attitudes and behavior of eye care professionals (ECPs) also play a crucial role in CL adoption.16 For instance, a proactive approach to CL fitting increases the likelihood of CL wear among ametropes.18 However, the tendency among ECPs to proactively prescribe CLs remains limited.2
Therefore, when a new CL is launched on the market, its eventual uptake depends not only on the technological characteristics (eg, material, replacement schedules, design) but also on the attitudes and perceptions of both ametropes and ECPs. Moreover, today, the age at first CL fitting has decreased considerably and typically occurs during adolescence.8,11 It is therefore of interest to evaluate whether adult, non-presbyopic individuals (over 18 years of age) who are given the opportunity to try contact lenses show an interest in continuing to use them. Verofilcon A (PRECISION1®) is a daily disposable CL recently introduced to the market, made of a silicone hydrogel “water surface” material.19,20 Scarce information is currently available regarding the willingness to continue wearing this CL after a short period,21 or the factors influencing such a decision. Therefore, the present study aims to evaluate the intention to continue using verofilcon A among neophyte adult wearers after a brief use and to identify potential factors influencing this intention.
Method
Study Design
A prospective, single-masked, single-arm clinical trial was conducted at the University of Milano-Bicocca. The protocol is summarized in the study flow chart shown in Figure 1.
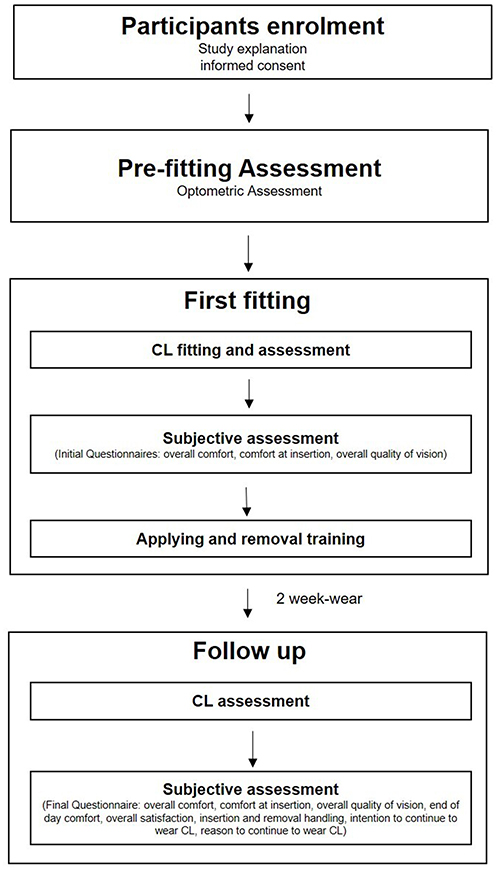 |
Figure 1 Flow chart of study design. |
Participants
This was a single-arm descriptive study where the primary endpoint is the proportion of spectacle wearers interested in becoming CL wearers. Based on the study of Atkins et al,18 we assumed that approximately 38% of participants of spectacle wearers would be interested in CL wear, as 38% of participants in that study proceed to purchase CLs after a trial. To ensure that the 95% confidence interval for the estimate proportion of spectacle wearers interested in becoming CL wearers is within ±10% of the true proportion, a minimum sample size of 91 subjects was required.
Ninety-five ametropic, non-contact lens wearers (52 females and 43 males; mean age ± SD: 25.4 ± 5.3 years; range: 18–40) were voluntarily enrolled according to the inclusion and exclusion criteria reported in Table 1 and completed the study. Six additional individuals (not included in the above sample), though eligible, did not complete the study: four due to difficulties in handling the CLs (mainly with insertion), and two because of discomfort experienced during the initial trial, which led them to withdraw from participation.
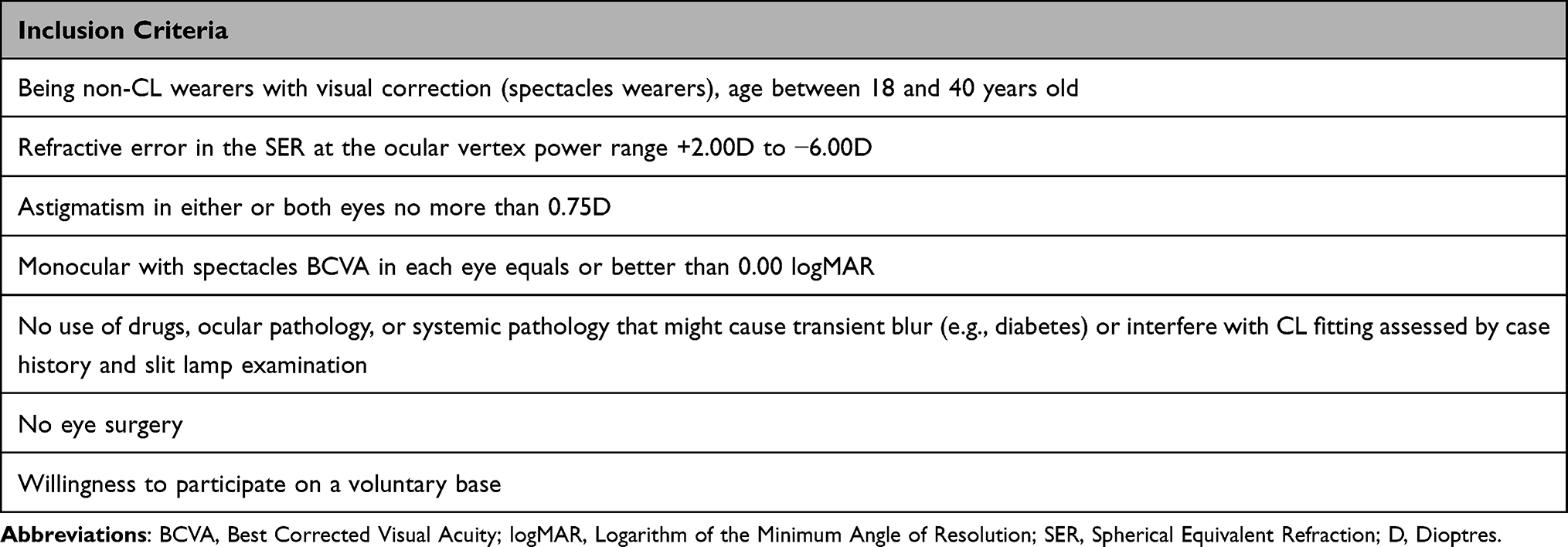 |
Table 1 Inclusion Criteria for Subjects Enrolled in the Study |
Ethical approval was granted by the Ethics committee of University of Milano-Bicocca (n.0122754; approved on February 1st 2024, issued on February 29th, 2024). The study adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants after they received a full explanation of the study’s nature and possible consequences.
Materials
The CL used in this study was verofilcon A (Alcon Laboratories, Fort Worth, TX, USA) a daily disposable silicone hydrogel lens featuring a “water surface” technology. It is a class IIa medical device with a back optic zone radius of 8.3 mm, a total diameter of 14.2 mm, a core water content of 51%, and a Dk/t of 100 Fatt units (at −3.00 DS).19,20 Lenses for the study were provided by Alcon.
Procedure
Participants were recruited via advertisements distributed throughout the University of Milano-Bicocca campus, including students, academic staff, and administrative personnel. Interested individuals attended a preliminary session in which the study protocol was explained, eligibility criteria were verified, and written informed consent was obtained. A baseline assessment was then scheduled for those meeting inclusion criteria.
Baseline Assessment
At baseline, participants completed the VF-14 QOL Questionnaire to evaluate vision-related quality of life.22 Following an anamnesis and a preliminary slit-lamp examination to identify any ocular condition contraindicating CL wear, a subjective refraction was performed to determine the starting power for CL fitting. Monocular and binocular high-contrast (about 95%) best corrected visual acuity was then measured at a distance of 4 meters under mesopic conditions, using a computerized chart (VisionChart, CSO, Florence, Italy). Optotypes consisted of rows of five Sloan letters presented in descending 0.10 logMAR steps, randomly generated from validated readability sets.23 A letter-by-letter scoring was applied to precisely determine the visual acuity threshold.
Following baseline assessments, participants were fitted with verofilcon A lenses by the ECP. After a short settling period, lens fit was evaluated in slit lamp. To minimize potential bias, participants were masked to the CL brand. Participants for whom an acceptable fit could not be achieved24,25 were excluded from further participation.
After successful fitting, monocular, and binocular high-contrast visual acuity with CLs was measured using the same setup.
Participants subsequently completed four subjective evaluations based on 0–100 visual analogue scales (VAS):26 comfort at insertion (recorded for each eye separately), overall comfort (average of both eyes), and overall quality of vision. The latter two assessments were performed after 1 hour of wear.27,28 For the comfort VAS, 0 represented “Extremely uncomfortable Causes pain. Cannot be tolerated”, while 100 indicated “Excellent. Cannot be felt”. For the quality of vision VAS, 0 corresponded to “Extremely poor”, and 100 to “Excellent. Unaware of any visual loss”.
Participants were then instructed on proper CL application and removal following the most common approach described by Vianya-Estopa et al29 They also received guidance on safe lens handling and hygiene, as well as on emergency procedures in case of adverse events. An instructional leaflet and emergency contact information were also provided. Once participants were deemed competent in lens handling (typically after one or 2 sessions), they were supplied with masked CLs for 14-day wearing period. Participants were instructed to wear the lenses at least 5 days per week, for a minimum of 5 hours a day. If participants were unable to meet this requirement (due to dry eye sensation, extremely high discomfort, poor vision, etc), they were withdrawn from the study and replaced. An adverse event reporting system was adopted.
Follow-Up Visit
After 14 days, participants attended a follow-up visit, having worn their CLs for at least 1 hour prior to examination. At the beginning of the visit, they completed a series of subjective evaluations (0–100 VAS) referring to their average experience over the 14-day period for both eyes. These included ease of insertion and removal, comfort at insertion, end of day comfort, quality of vision, and overall satisfaction. Moreover, participants rated their intention to continue wearing CLs on a 0–10 VAS scale (ranging from very unlikely to very likely) and their reasons for continuing CL wear by rating the importance (0–10) of the following potential factors: aesthetic, vision, convenience, sport, and other reasons. The scores for the intention and reasons-to-continue variables were subsequently transformed to a 1–100 scale to ensure consistency across all the subjective variables collected. Finally, monocular, and binocular high-contrast visual acuity with CLs were measured.
Statistical Analyses
As normality was not confirmed for all variables based on the Shapiro–Wilk test, non-parametric statistical methods were applied for data analysis. To describe the strength and direction of the relationship between two variables, Spearman’s rank correlation coefficient was calculated. For paired comparison, the Wilcoxon signed-rank test was applied to evaluate differences between conditions.
To predict the behavioral intention to continue wearing CLs after the trial, several hierarchical regression analyses (HRA) were performed, entering progressively different groups of variables into the model.
The first model (Model 1) included four predictors (from hereafter “background variables”): gender, age, spherical equivalent refraction (SER) of the right eye (only the right eye was considered due to high correlation with the left eye) and binocular BCVA achieved with CL at the follow-up visit.
The second model (Model 2) included all variables from Model 1 plus five subjective outcome ratings collected after 14 days of wear (from hereafter “subjective outcomes variables”): ease of insertion and removal, comfort at insertion, end of day comfort, quality of vision, and overall satisfaction.
The final model (Model 3) included all variables from Model 2 plus the four motivational factors for continue CL wear (from hereafter “motivation-to-continue variables”): aesthetic, vision, convenience, sport.
The overall significance of each model was assessed using the F-test statistic (F), and explanatory power was expressed as the coefficient of determination (R2), Probability values ≤.05 were considered statistically significant. Multicollinearity among independent variables was assessed using tolerance and variance inflation factor (VIF) values. All statistical analyses were conducted using SPSS Statistics 29.0.1.0 (IBM, 2023).
Results
Optometric data obtained during the preliminary assessment, and the final power of CLs prescribed are presented in Table 2. No serious adverse events occurred. One participant reported mild discomfort and slight vision reduction in one eye after two days of wear; after examination and a one-day break, lens wear was safely resumed and the study completed. All 95 participants who completed the two-week trial were able to meet the predefined inclusion criteria, which required wearing the lenses for more than 5 hours per day on at least 5 days per week. The overall age distribution (Figure 2A), and distributions by genders (Figure 2B and C) are shown, while the distribution of CL powers prescribed is illustrated in Figure 3. Visual Acuity with CLs at the first and follow-up visit is reported in Figure 4. At the first CLs fitting, monocular visual acuity (mean ± standard deviation) with CLs was −0.16±0.08 logMAR (range: 0.02 to −0.30) for the right eye, −0.16±0.07 logMAR (range: 0.02 to −0.30) for the left eye, and −0.20±0.07 logMAR (range: −0.00 to −0.30) binocularly. At the follow-up visit (after 14 days), monocular visual acuity with CLs was −0.15±0.08 logMAR (range: 0.08 to −0.28) for the right eye, −0.15±0.08 logMAR (range: 0.06 to −0.30) for the left eye, and −0.20±0.07 logMAR (range: −0.02 to −0.30) binocularly.
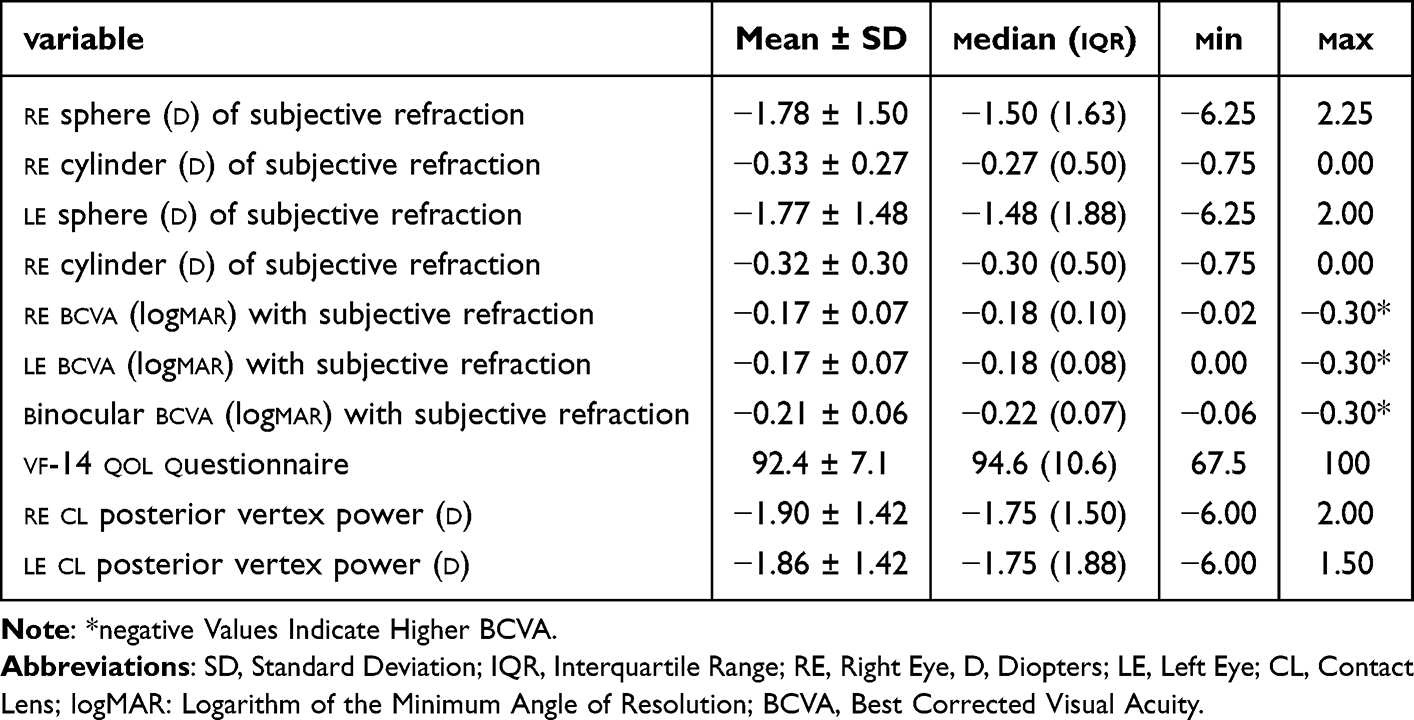 |
Table 2 Main Optometric Characteristics of Participants and CL Prescribed |
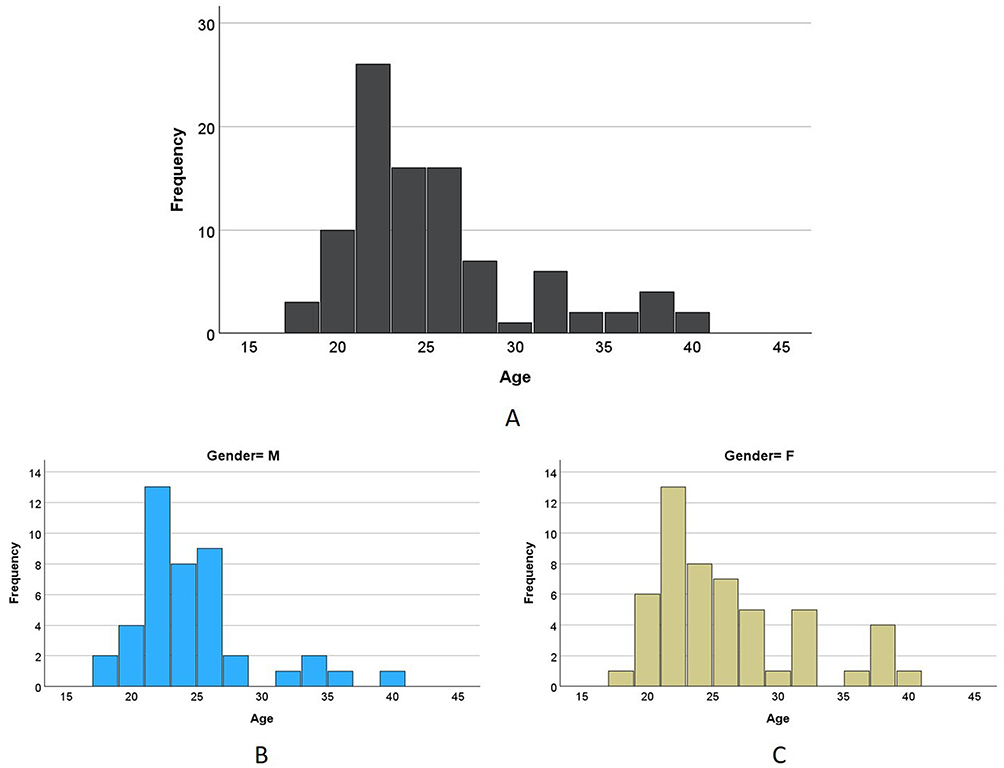 |
Figure 2 Distribution of participants by age: (A) total sample. (B) male subgroup (C) female subgroup. |
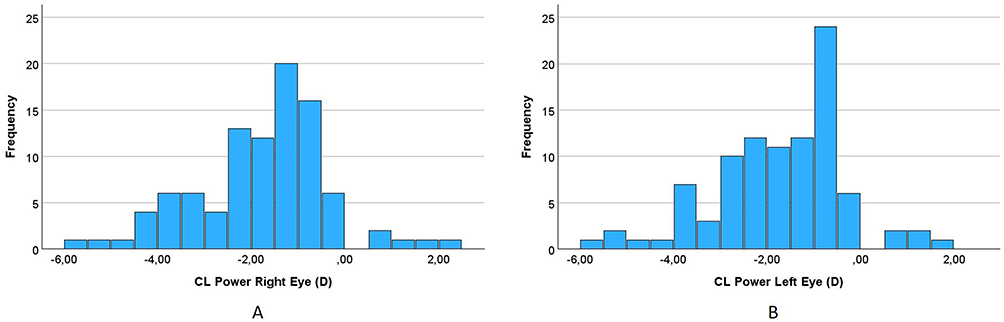 |
Figure 3 Distribution of participants by CL power: (A) Right eye. (B) Left eye. |
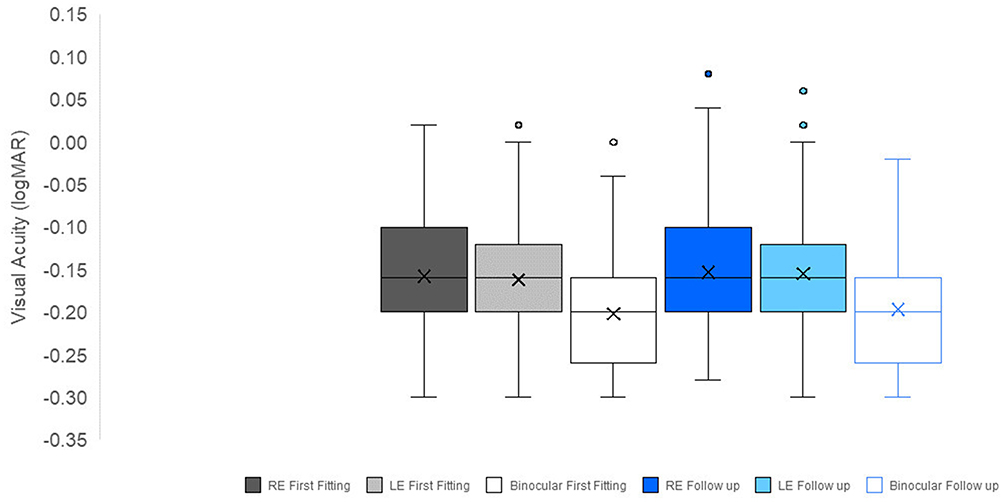 |
Figure 4 Visual Acuity achieved with CL during the initial fitting and at the follow-up visit. The X marks the mean, the horizontal line indicates the median, and the dots represent outliers. Abbreviations: RE, right eye; LE, left eye. |
BCVA with subjective refraction (values reported in Table 2) was significantly correlated with visual acuity with CLs at the first visit, for the right eye (Sperman Rho=0.70; p<0.001), left eye (Sperman Rho=0.75; p<0.001), and binocularly (Sperman Rho=0.76; p<0.001). No significant difference was found between the BCVA with subjective refraction and CL visual acuity for any comparison: right eye (Wilcoxon; p=0.08), left eye (Wilcoxon; p=0.33), and binocularly (Wilcoxon; p=0.16). Similarly, visual acuity with CL did not change between the first and the follow up visits: right eye (Wilcoxon; p=0.38), left eye (Wilcoxon; p=0.07), and binocularly (Wilcoxon; p=0.32).
Violin plots are graphical representation that combines a box plot with a kernel density plot, allowing visualization of both the distribution and variability of the data; wider sections indicate higher data density, while the central markers summarize median and interquartile range. Figure 5, illustrate the distribution of participants’ subjective outcome scores at the first visit, while Figure 6 shows the corresponding distributions after the 14-day wearing period. Analytic values (mean ± SD, median, IQ range, and the percentage of participants with a subjective score >50, ie, the neutral point) for the subjective outcomes collected at first fitting and during the follow-up visit are reported in Table 3.
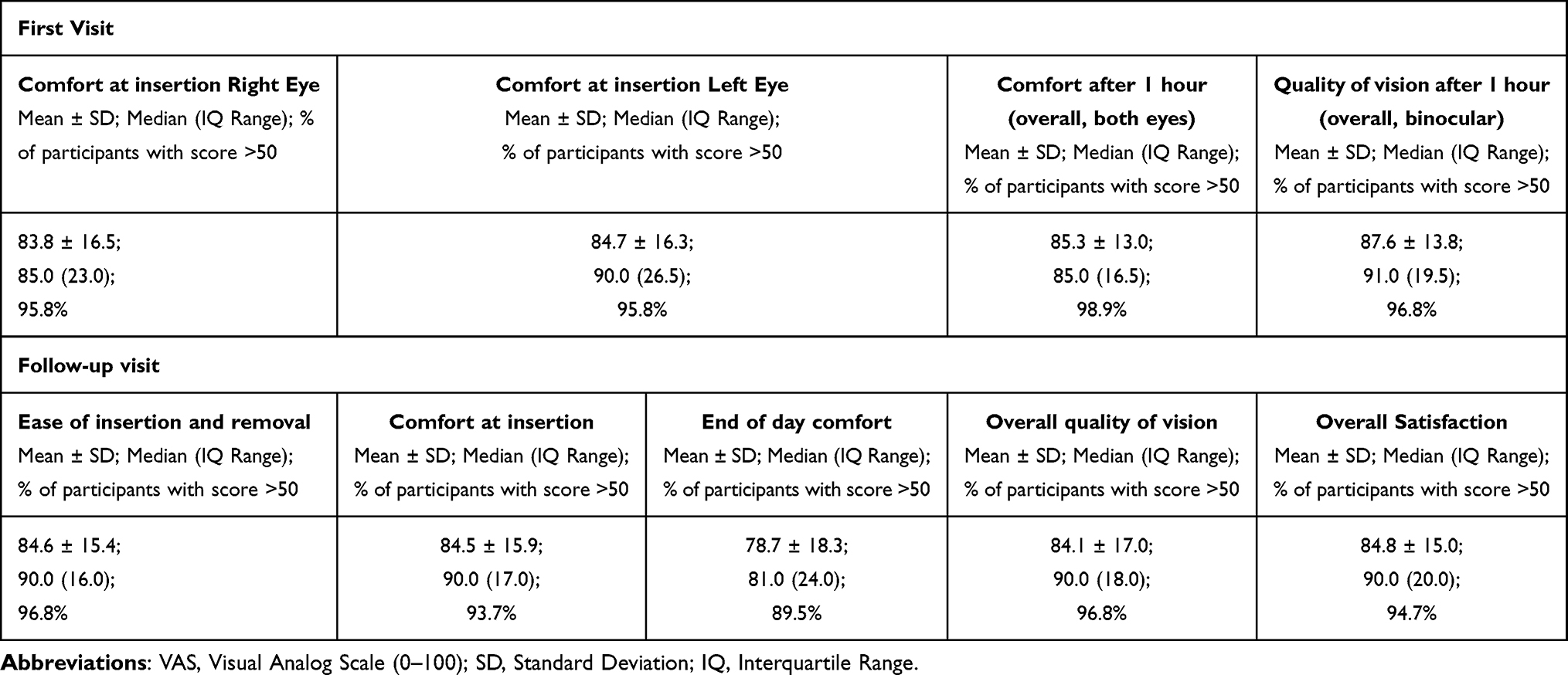 |
Table 3 Subjective Outcomes at First Fitting and During the 14-Day of Wear Collected at Follow-Up Visit |
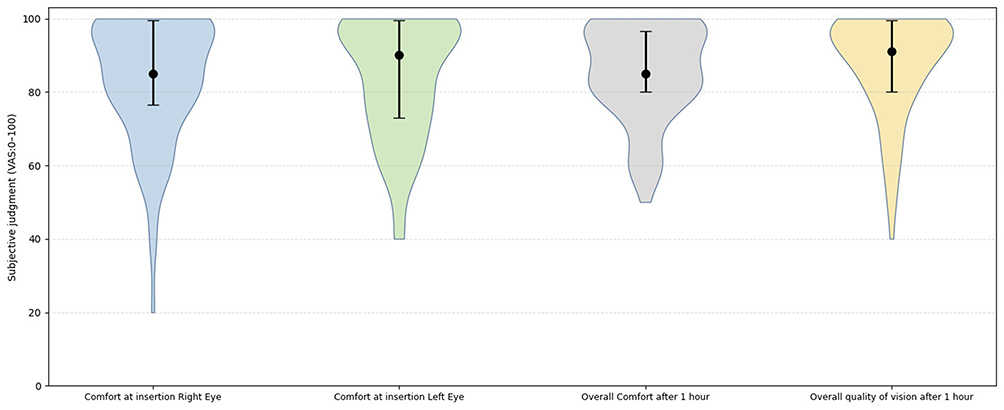 |
Figure 5 Violin plots of subjective judgments scores for the four questions: comfort at insertion for the right and left eye, overall comfort after 1 hour of wear, and overall quality of vision after 1 hour of wear as reported by participants at the first visit. The y-axis represents the VAS used for data collection. The grey area shows the probability density of the data across the range of subjective scores for each dimension. For each distribution, the black markers and error bars display the median with interquartile range (IQR). |
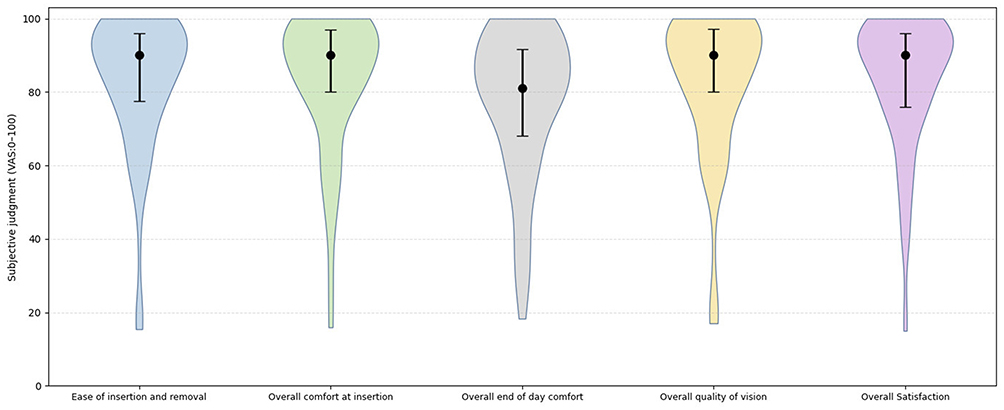 |
Figure 6 Violin plots of subjective judgments scores for the five questions (ease of insertion and removal, comfort at insertion, end of day comfort, overall quality of vision, and overall satisfaction) provided by participant at the follow-up visit referring to their 14-day wearing experience on a VAS scale. The y-axis represents the VAS scale used for data collection while grey rea shows the probability density of the data across different subjective score values for each dimension. For each distribution, the black markers and error bars display the median with interquartile range (IQR). |
The propensity to continue CL use after the follow-up, and the relative strength of the motivations to continue wearing CLs (aesthetic, vision, convenience, and sport) are summarized in Table 4. In this case, the percentage of participants with a subjective score >50 (ie, the neutral point) is reported only for the intention variable, since for the reasons-to-continue score, a value of 50 does not represent a neutral point but rather the midpoint of a continuum of increasing motivation ranging from 0 to 100. A further analysis of the proportion of participants as a function of the level of intention is reported in Figure 7.
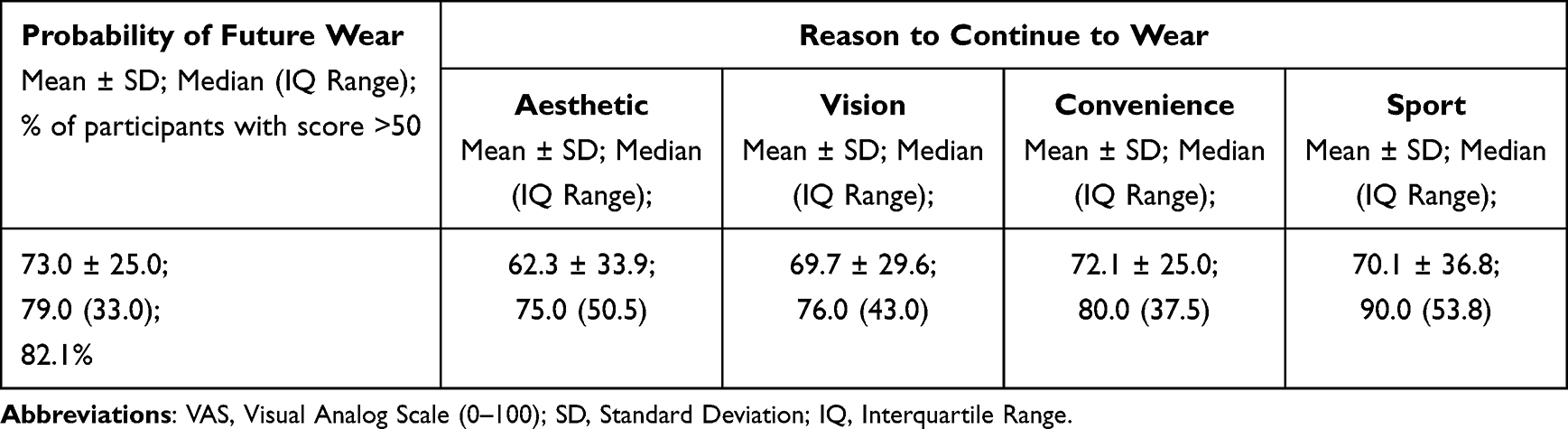 |
Table 4 Subjective Outcomes in Terms of Intention of Future Wear and the Strength of Different Reasons to Continue to Wear CL |
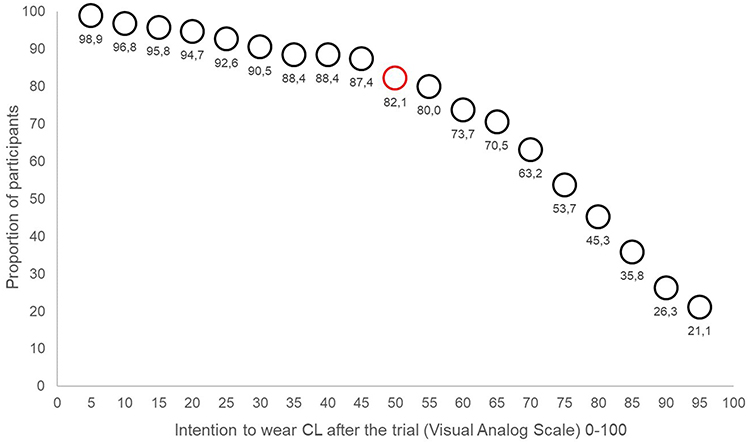 |
Figure 7 Proportion of participants as a function of the intention score (x). Values represent the proportion of participants with an intention score greater than x. The proportion corresponding to values greater than 50 (the midpoint of the scale) is highlighted in red. |
During the 14-day CL trial, a statistically significant difference was observed between comfort at insertion and at end-of-day comfort (Wilcoxon test; p < 0.001). End-of-day comfort showed a moderate significant positive correlation with subjectively perceived quality of vision (Spearman Rho 0.51; p<0.001), whereas no significant correlations were found between end-of-day comfort and monocular or binocular visual acuity (Spearman Rho, n.s). Similarly, subjective quality of vision was not correlated with psychophysical measures of visual acuity either monocular or binocular (Spearman Rho, n.s).
Predicting the Intention to Continue CL Wear
The results of the HRA assessing the intention to continue wearing CLs are reported in Table 5. Model 1 (background variables) was not statistically significant (p=0.46) and explained only 4% of the variance in the dependent variable. Model 2 (subjective outcome variables) was statistically significant (p < 0.001) and explained 38% of the variance. Within this model, overall satisfaction showed a significant positive association (Beta=0.59; p = 0.003) with the intention to continue wearing CLs. Model 3 (motivation-to-continue variables) was also significant (p < 0.001) and accounted for 57% of the variance. Three motivational factors, aesthetic, convenience, and sport, were significant predictors of the intention to continue CL wear, with standardized beta coefficients of β=0.20 (p = 0.02), β=0.35 (p < 0.001), and β=0.21 (p = 0.01) respectively.
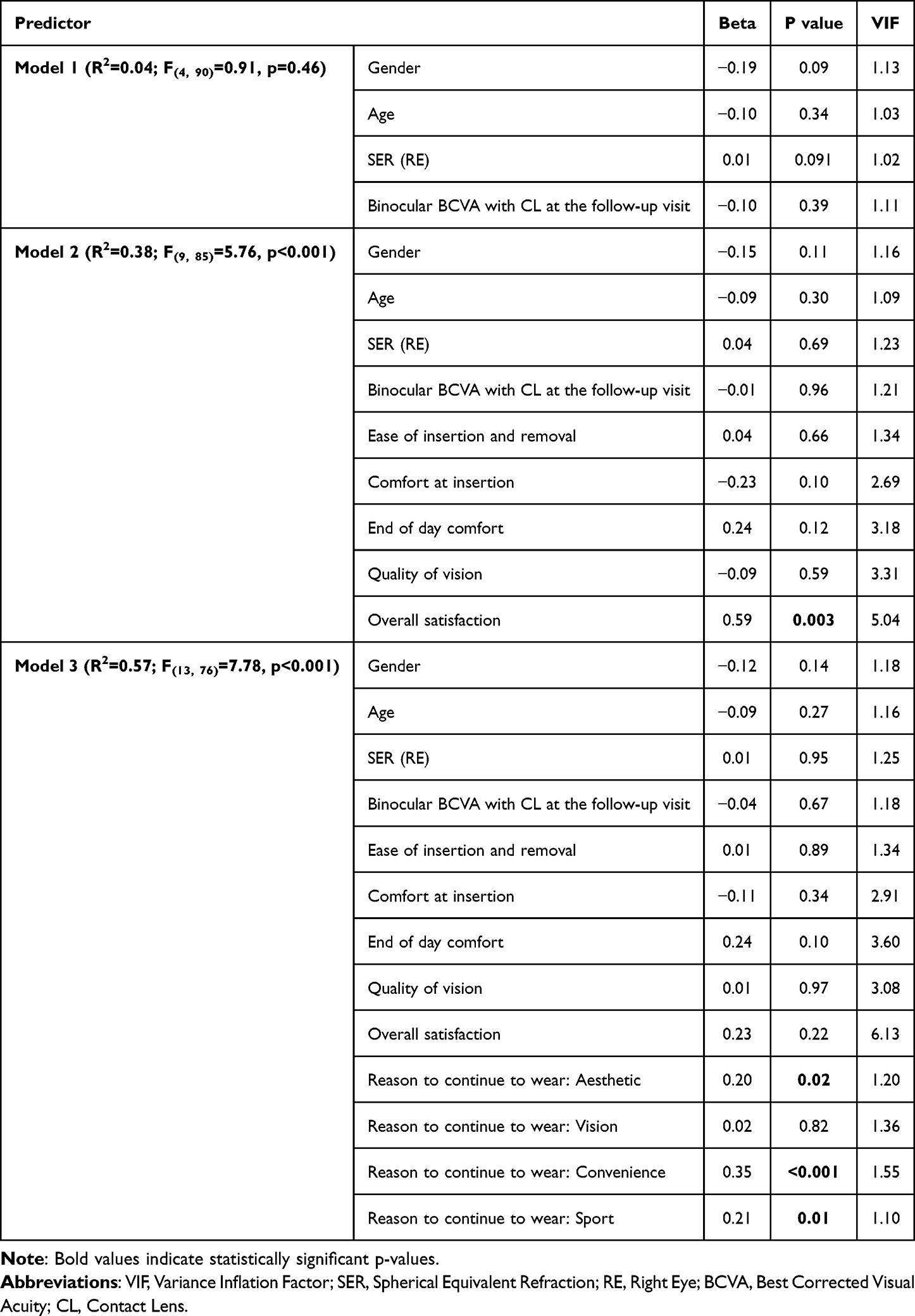 |
Table 5 Hierarchical Regression Analysis (HRA) for the Intention to Continue Wearing CLs |
Discussion
This present study evaluated the propensity (intention) to continue wearing a new daily disposal CL (verofilcon A) in a group of volunteer adult individuals with no prior CL experience (spectacle wearers only). This daily disposable CL, which offers clear advantages in terms of hygiene and convenience,5 is made of a silicone hydrogel “water surface” material.19,20 This material has the potential to enhance comfort.21 Therefore, this CL was selected to allow the study of participants’ intentions under the condition of appropriate CL fitting.
The demographic characteristics of the sample (55% females; mean age 25.4 ± 5.3 years) differ somewhat from the typical population of CL wearers, and this should be considered when interpreting the results. Indeed, the worldwide female-to-male ratio among CL wearers is approximately 65%,3 and the age of first fitting is generally younger, with about 36% of the wearers under 19 years of age8 and the highest prevalence between 15 and 25 years.30 The older age range of this study was specifically targeted to evaluate whether adult, non-presbyopic individuals (over 18 years of age) who are given the opportunity to try CL show an interest in continuing to use them.
The results obtained with the lenses used in this study were good in terms of vision: monocular and binocular visual acuity achieved with CL at the first visit (baseline) did not differ from the BCVA achieved with subjective refraction. In addition, also comfort and satisfaction resulted of high level, confirming the good clinical performance previously reported for this CL.19
Notably, no participants withdrew from the study due to an inability to meet wear-time criteria.
Visual acuity and subjective perceived quality of vision were both high at baseline and after the 14-day trial period. However, these two measures were not significantly correlated, confirming that high contrast visual acuity is not necessary a good predictor of subjective quality of vision.31
The violin plots (Figures 5 and 6) suggest a certain degree of multimodality in the subjective ratings. Although smoothing inherent to the density representation partly softens these features, the presence of multiple rounded peaks in the upper range of the scale (corresponding to high performance) nonetheless reveals an underlying tendency to provide near round-number scores (100%, 90%, 80%, etc). This pattern may reflect a cognitive bias toward scalar or rounded judgments.32 Such multimodal trends were less pronounced in data referring to the 14-day wear-period (Figure 6).
Regarding comfort, results were also good both in the first visit and after 14 days of wear. A statistically significant difference was observed between comfort at insertion and end-of-day comfort over the two-week wear period (means decrease: 5.8 ± 13.4 points on the VAS scale; Wilcoxon; p<0.001). However, this reduction, widely reported in literature,33,34 remains below the minimal clinical important difference for ocular subjective responses.26 Moreover, the significant correlation between the end-of-day comfort and perceived quality of vision during the 14-day period suggests that the overall subjective dimension of comfort incorporates a visual comfort component. The violin plots for comfort showed a similar multimodal response trend, again less evident in the scores referring to the14-day wear period (Figure 6).
The intention to continue wearing CLs among the participants, measured as the self-reported probability of future wear, was encouraging. After participants had the opportunity to experience lens wear, the declared probability of continued use was relatively high (mean ± SD 73.0 ± 25.0, median = 79.0, on the 0–100 VAS scale). Given that these individuals, who had no prior experience with contact lenses, were exclusively spectacle wearers reporting satisfactory vision-related quality of life, as indicated by their VF-14 results, this finding suggests that even among those satisfied with their habitual vision correction, direct exposure to contact lens wear can positively influence attitudes and acceptance. This outcome is consistent with the findings of the EASE study in which trying CLs induced a positive experience that encourage continued wear.18
More specifically, Atkins and co-authors18 used a questionnaire including two items exploring intention to continue wearing CL, rated on a five-point Likert scale: “I will try contact lenses in the future” and “Planning to wear contact lenses”. The proportion of participants who agreed or strongly agreed (ie. above the midpoint of the five-point Likert scale) with these statements was 70% and 33%, respectively. These percentages are lower than the proportion of participants scoring above the midpoint of the intention scale (50 out of 100) in the present study, which was 82.1% (see Figure 7). However, it should be noted that the two study protocols were substantially different. In the study by Atkins et al,18 participants experienced only a brief CL trial while choosing a spectacle frame, whereas in the present study participants wore CLs for two weeks, with a minimum of 5 hours per day. In addition, the wording of the questions differed slightly. The longer trial period in the present study may have acted as a factor increasing participants’ intention to wear CLs.
Another study, investigated the intention to continue CL wear in adult participants new to CL use, specifically assessing intention to continue wearing verofilcon A.21 The results showed that 70% of respondents agreed with the statement that the lens “is the one I will continue to wear in the future”. Again, this proportion is lower than that observed in the present study; however, the comparison should be interpreted with caution, as participants in that study were asked about a specific lens type, whereas the intention assessed in the present study was more general and not related to a particular CL.
The HRA revealed that significative predictors of intention to continue wearing CLs did not lie within the “background variables” (gender, age, and refractive error) or “subjective outcomes variables” (quality of vision, comfort or satisfaction). Instead, the model that best explained the variance (Model 3) included motivational factors (aesthetic, convenience, and sport) which were positively associated with the behavioral intention to continue CL wear.
This pattern is partially consistent with the findings of Bowden and Harknett,8 who found that aesthetic considerations were the predominant initial drivers for initiating CL wear, whereas convenience and sport-related factors gained greater importance with sustained use. The slight differences between the two studies may be attributed to the statistical approaches employed (HRA in the present study vs frequency analysis in Bowden and Harkenett’s study), and to the different characteristics of the sample (older than the average age of new CL wearer, non-spontaneously seeking CL fitting candidates in the present study vs younger and self-motivated wearers in the Bowden and Harknet’s).
Several limitations should be acknowledged in the present study. The intention measured in this study should be regarded as a proxy for actual behavior (ie willingness to continue wearing CLs), not a direct measure of the behavior itself. Furthermore, the follow-up period was relatively short (14 days), and subjective judgments were collected as cumulative experience at the end of the trial rather than as real-time assessments during the wearing period. Additionally, although participants were screened through medical history and preliminary evaluations to exclude contraindications to contact lens use (including dry eye), a specific dry eye assessment was not performed. A history of binocular vision problems was recorded; however, no specific binocular vision tests were conducted at the initial screening. These factors may contribute to contact lens discomfort or dissatisfaction with them.
In conclusion, the findings indicate that offering ametropic non–CL wearers a structured CL fitting experience, based on clinical guidelines, objective and subjective outcome measures, can be an effective strategy to foster long-term CL adoption. Behavioral intention to continue CL wear was chiefly influenced by motivational factors associated with aesthetics, convenience and sport activities.
Data Sharing Statement
Anonymized individual participant data that support the findings of this study will be made available by the corresponding author ([email protected]) upon reasonable request. The data will be available for one year following publication.
Funding
This study, titled “Attitudes Towards the use of Precision1® (ATP study)”, was supported by Alcon (IIT #90203571) through monetary support and provision of the study product.
Disclosure
The authors report no proprietary interest in any materials mentioned in this article. FZ reports funding to his institution from Hoya Vision Care and Johnson & Johnson Vision Care, and personal fees from Bausch + Lomb and Essilor Luxottica. ST reports funding to her institution from Yung Sheng Optical Co. Ltd, Johnson & Johnson Medical S.p.A., Hoya Holdings N.V., Horizons Optical SLU, Nikon Europe B.V., and Bausch & Lomb – IOM S.p.A., all outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Stapleton F, Keay L, Jalbert I, Cole N. The epidemiology of contact lens related infiltrates. Optometry Vision Sci. 2007;84(4):257–14. doi:10.1097/OPX.0b013e3180485d5f
2. Akerman D. Our greatest opportunity. Contact Lens Anterior Eye. 2018;41:319–320. doi:10.1016/j.clae.2018.05.007
3. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2021. Contact Lens Spectr. 2022;37(January):32–38.
4. Morgan P, Efron N, Woods C, Jones D, Jones L, Nichols J. International trends in daily disposable contact lens prescribing (2000-2023): an update. Contact Lens Anterior Eye. 2024;47(6):102259. doi:10.1016/j.clae.2024.102259
5. Efron N, Morgan P, Woods C, Jones D, Jones L, Nichols J. International trends in prescribing silicone hydrogel contact lenses for daily wear (2000-2023): an update. Contact Lens Anterior Eye. 2024;47(6):102310. doi:10.1016/j.clae.2024.102310
6. Thite N, Desiato A, Shinde L, et al. Opportunities and threats to contact lens practice: a global survey perspective. Contact Lens Anterior Eye. 2021;44(6):101496. doi:10.1016/j.clae.2021.101496
7. Markoulli M, Kolanu S. Contact lens wear and dry eyes: challenges and solutions. Clin Optom. 2017;9:41–48. doi:10.2147/OPTO.S111130
8. Bowden T, Harknett A. What the patient wore, and why. Contact Lens Anterior Eye. 2006;29(1):5–15. doi:10.1016/j.clae.2005.12.002
9. Walline JJ, Gaume A, Jones LA, et al. Benefits of contact lens wear for children and teens. Eye Contact Lens Sci Clin Pract. 2007;33(6):317–321. doi:10.1097/ICL.0b013e31804f80fb
10. Walline JJ, Jones LA, Sinnott L, et al. Randomized trial of the effect of contact lens wear on self-perception in children. Optom Vis Sci. 2009;86(3):222–232. doi:10.1097/OPX.0b013e3181971985
11. Zeri F, Durban JJ, Hidalgo F, Gispets J. Attitudes towards contact lenses: a comparative study of teenagers and their parents. Contact Lens Anterior Eye. 2010;33(3):119–123. doi:10.1016/j.clae.2009.12.009
12. Zeri F, Livi S, Maffioletti S. Attitudes towards visual correction in sport: what coaches, physical education teachers and sports physicians think. Contact Lens Anterior Eye. 2011;34(2):71–76. doi:10.1016/j.clae.2010.08.006
13. Zeri F, Livi S, Cesari M, Gheller P, Magni R, Holden BA. Benefits and barriers towards the use of contact lenses. how ametropes perceive them and how practitioners inform about them: an Italian survey. Contact Lens Anterior Eye. 2015;39(1):38. doi:10.1016/j.clae.2015.07.005
14. Zeri F, Di Censi M, Livi S, Ercoli A, Naroo SA. Factors that influence the success of contact lens fitting in presbyopes: a multicentric survey. Eye Contact Lens. 2019;45(6):382–389. doi:10.1097/ICL.0000000000000606
15. Walline JJ, Long S, Zadnik K. Daily disposable contact lens wear in myopic children. Optom Vis Sci. 2004;81(4):317–321. doi:10.1097/00006324-200404000-00011
16. Thite N, Desiato A, Shinde L, et al. Differences in practitioner experience, practice type, and profession in attitudes toward growing contact lens practice. Eye Contact Lens. 2022;48(9):369–376. doi:10.1097/ICL.0000000000000920
17. Li L, Moody K, Tan DTH, Yew KC, Ming PY, Long QB. Contact lenses in pediatrics study in Singapore. Eye Contact Lens. 2009;35(4):188–195. doi:10.1097/ICL.0b013e3181abb5bb
18. Atkins NP, Morgan SL, Morgan PB. Enhancing the approach to selecting eyewear (EASE): a multi-centre, practice-based study into the effect of applying contact lenses prior to spectacle dispensing. Contact Lens Anterior Eye. 2009;32(3):103–107. doi:10.1016/j.clae.2009.02.004
19. Miller J, Giedd B, Subbaraman LN. Clinical comparison of a silicone hydrogel and a conventional hydrogel daily disposable contact lens. Clin Ophthalmol. 2021;15:4339–45.
20. Ponzini E, Recchioni A, Cheloni R, Zeri F, Tavazzi S. Physical properties and interaction with the ocular surface of water-gradient contact lenses. Eye and Contact Lens. 2023;49:152–159. doi:10.1097/ICL.0000000000000974
21. Grant T, Tang A. A survey of contact lens wearers and eye care professionals on satisfaction with a new smart-surface silicone hydrogel daily disposable contact lens. Clin Optom. 2020;12:9–15. doi:10.2147/OPTO.S233328
22. Massof RW, Ahmadian L. What do different visual function questionnaires measure? Ophthal Epidemiol. 2007;14(4):198–204. doi:10.1080/09286580701487883
23. Ferris FL, Kassoff A, Bresnick GH, Bailey I. New visual acuity charts for clinical research. Am J Ophthalmol. 1982;94(1):91–96. doi:10.1016/0002-9394(82)90197-0
24. Gasson A, Morris J. The Contact Lens Manual a Practical Guide to Fitting.
25. Wolffsohn JS, Hunt OA, Basra AK. Simplified recording of soft contact lens fit. Contact Lens Anterior Eye. 2009;32(1):37–42. doi:10.1016/j.clae.2008.12.004
26. Navascues-Cornago M, Guthrie S, Morgan PB, Woods J. Minimal Clinically Important Difference (MCID) for ocular subjective responses. Transl Vis Sci Technol. 2024;13(8):28. doi:10.1167/tvst.13.8.28
27. Dumbleton KA, Woods CA, Jones LW, Fonn D. Comfort and adaptation to silicone hydrogel lenses for daily wear. Eye Contact Lens. 2008;34(4):215–223. doi:10.1097/ICL.0b013e31816499dc
28. Tavazzi S, Galli A, Maspero F, Rizzo G, Zeri F, Ponzini E. Dehydration kinetics of soft contact lenses: the hidden impact of early wear. Cont Lens Anterior Eye. 2025;13:102512.
29. Vianya-Estopa M, Ghorbani-Mojarrad N, Huntjens B, et al. Current approaches to soft contact lens handling training – global perspectives. Contact Lens Anterior Eye. 2023;46(6):102068. doi:10.1016/j.clae.2023.102068
30. Swanson MW. A cross-sectional analysis of U.S. contact lens user demographics. Optom Vis Sci. 2012;89(6):839–848. doi:10.1097/OPX.0b013e318255da45
31. Martelli M, Zeri F. Dall’immagine retinica all’elaborazione dell’informazione visiva. In: Zeri F, Rossetti A, Fossetti A, Calossi A, editors. Ottica Visuale. Rome: SEU; 2012.
32. Honda H, Kagawa R, Shirasuna M. On the round number bias and wisdom of crowds in different response formats for numerical estimation. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-11900-7
33. Santodomingo-Rubido J, Barrado-Navascués E, Rubido-Crespo MJ. Ocular surface comfort during the day assessed by instant reporting in different types of contact and non-contact lens wearers. Eye Contact Lens. 2010;36(2):96–100. doi:10.1097/ICL.0b013e3181d1d5a5
34. Stahl U, Keir NJ, Landers A, Jones LW. Effect of short recovery periods on ocular comfort during daily lens wear. Optom Vis Sci. 2016;93(8):861–871. doi:10.1097/OPX.0000000000000912
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.