Back to Journals » International Journal of Women's Health » Volume 17
Attitudes, Perceptions and Determinants of Non-Medically Indicated Caesarean Section Preference Among Pregnant Women in Thailand: A Three-Phase Mixed-Methods Study
Authors Chawanpaiboon S ![]() , Anuwutnavin S, Titapant V, Kanjanapongporn A, Pooliam J, Srichai R
, Anuwutnavin S, Titapant V, Kanjanapongporn A, Pooliam J, Srichai R
Received 26 September 2025
Accepted for publication 16 December 2025
Published 23 December 2025 Volume 2025:17 Pages 5577—5596
DOI https://doi.org/10.2147/IJWH.S570370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Saifon Chawanpaiboon,1 Sanitra Anuwutnavin,1 Vitaya Titapant,1 Attapol Kanjanapongporn,2 Julaporn Pooliam,3 Rangsima Srichai4
1Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynaecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 2Department of Social Sciences, Faculty of Social Sciences and Humanities Mahidol University, Nakhon Pathom, 73170, Thailand; 3Clinical Epidemiological Unit, Office for Research and Development, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 4Department of Research, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand
Correspondence: Saifon Chawanpaiboon, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynaecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand, Tel +66 2 419 7000 ext. 4777– 4888, Fax +66 2 418 2662, Email [email protected]
Background: Non-medically indicated caesarean section (CS) is a growing contributor to rising CS rates globally and in Thailand, influenced by maternal preference, socio-cultural factors and clinical decision-making. Understanding women’s perspectives is essential to guide counselling strategies and inform policy targeted at reducing unnecessary CS.
Objective: To explore pregnant women’s attitudes, perceptions and determinants of preference for non-medically indicated CS and identify factors associated with CS preference.
Methods: This prospective, descriptive, three-phase mixed-methods study was conducted from May 1 to July 30, 2024. The study was conducted at an antenatal clinic. The study comprised three phases: in-depth interviews with 40 pregnant women, questionnaire development and validation, and a survey of 400 participants. Descriptive statistics summarised had demographic data, while univariable chi-squared tests and multivariable logistic regression analysed factors associated with non-medically indicated CSs. Odds ratios and 95% confidence intervals (CIs) were reported, with statistical significance set at P < 0.05. The main outcomes and measures were the attitudes, perceptions, policy, implementation science, counselling frameworks, and clinician–patient power dynamics of pregnant women towards non-medically indicated caesarean sections.
Results: Among the 400 women surveyed, 75% preferred vaginal delivery as a more natural and less risky option. However, 60% 60% reported they would still agree to a CS if recommended by a doctor, indicating high reliance on physician guidance even in situations without clear medical indication. Key factors affecting delivery preferences included prior caesarean delivery (adjusted odds ratio 2.5, 95% CI 1.5‒4.0) and maternal age over 35 years (adjusted odds ratio 1.8, 95% CI 1.1‒2.9). Comprehensive counselling was deemed essential by 80% of participants, who reported greater confidence in choosing vaginal delivery after thorough discussions of risks and benefits. Auspicious timing influenced 39.5%, while 37.3% were swayed by pain perception. Higher education levels, assisted conception methods and concerns about safety, such as blood loss, also shaped CS preferences.
Conclusion: Pregnant women in Thailand generally prefer vaginal birth but are highly influenced by physician recommendations. Strengthening counselling, addressing misconceptions and incorporating shared decision-making into routine antenatal care may reduce non-indicated CS demand. Findings support future development of counselling frameworks and policy interventions to promote safe, evidence-based delivery choices.
Thai Clinical Trials Registry Reference: TCTR 20230913007: Date of registration 13 September 2023.
Plain Language Summary: Non-medically indicated caesarean section (CS) rates continue to rise in Thailand, despite the procedure carrying increased risk compared with vaginal birth when not clinically required. Understanding how women make decisions regarding delivery methods is therefore an important public health priority.
This mixed-methods study examined pregnant women’s attitudes, perceptions and factors influencing CS preference. Data were collected in three phases, including qualitative interviews, questionnaire development and a survey of 400 participants. Although most women initially preferred vaginal birth, many indicated they would consent to CS if advised by their doctor. Determining factors included previous CS, advanced maternal age, medical comorbidities, labour pain concerns and cultural practices such as selecting an auspicious birth date. Clear counselling from healthcare providers strengthened women’s confidence in choosing vaginal delivery. These findings can inform counselling approaches and policy aimed at reducing unnecessary CS and promoting informed decision-making.
What is already known on this topic?
Non-medically indicated caesarean sections (CS) have been increasing globally, influenced by factors such as physician recommendations, maternal age, and safety concerns. However, little is known about the perspectives of pregnant women in Thailand regarding CS and the cultural or socio-demographic factors shaping their preferences.
What this study adds?
This study reveals that Thai pregnant women’s preferences for CS are shaped by prior CS experience, advanced maternal age, and assisted conception methods. Factors such as pain perception, cultural considerations like auspicious timing, and the influence of comprehensive medical counselling significantly impact their decision-making.
How this study might affect research, practice or policy?
The findings emphasize the importance of tailored medical counselling to address misconceptions and provide balanced information, potentially reducing unnecessary CS rates. Insights from this study could inform patient education strategies and support evidence-based policymaking to promote safer delivery practices.
Keywords: attitudes, caesarean sections, decision-making, mixed-methods study, non-medically indicated, opinions, perceptions, perspective, pregnant women
Introduction
The global rate of caesarean sections (CSs) has been steadily increasing worldwide. A 2018 report from The Lancet1 revealed a sharp rise in the global CS rate. It climbed from 12.1% in 2000 to 22.1% in 2015, with Latin America exhibiting the highest rate at 44.3%. In China, the CS rate escalated to 39% in 2002,2 while in Thailand, it surged from 7.06% in 1990 to 44.46% in 2010.3,4 Despite such increases, the rates of most maternal and neonatal complications did not decrease.5–7 High CS rates in regions such as Latin America and Asia have been linked to increased preterm births, infant mortality and higher maternal morbidity. In contrast, African countries with a stable CS rate of 8.8% report lower neonatal mortality.6
The World Health Organization initially recommended that the CS rate not exceed 15% to 20% per country.8 However, recent research suggests that a rate of approximately 19% is associated with improved maternal and neonatal outcomes, indicating that 20% may be the optimal rate for CS.9 Childbirth is a natural process that most women can undergo safely.10 In contrast, CS is a life-saving procedure that should be performed only when medically necessary,11 such as in cases of foetal malposition, an abnormal foetal heart rate, or maternal complications.
However, CSs carry inherent risks, especially in hospitals with inadequate equipment or inexperienced surgeons. Complications include abnormal placental adhesion in future pregnancies, abdominal adhesions and newborn respiratory issues. Moreover, infants born via CS may miss exposure to beneficial bacteria acquired during vaginal delivery, which can affect their immune system and increase the risk of allergies.12 Conversely, CS can prevent maternal issues such as diaphragmatic prolapse and urinary incontinence.13
Despite awareness of these risks, both obstetricians and pregnant women continue to opt for CS without medical indications, thereby contributing to rising rates. In Thailand, several medical factors influence this trend, including the sensitivity of foetal monitoring tools, fear of malpractice lawsuits, and scheduling convenience for obstetricians. Additional factors are greater expertise in performing CS, the prolonged nature of natural childbirth, greater compensation for CS in private hospitals and the cultural practice of choosing CS timing based on astrological factors.
Although previous Thai studies have explored women’s delivery preferences, most were conducted more than 10 years ago and may not reflect current clinical practice, cultural attitudes, or the rapidly increasing CS rate in Thailand. Updated evidence is needed to understand contemporary factors influencing decision-making, particularly in the context of evolving maternal expectations, accessibility of information, and ongoing national efforts to reduce non-indicated CS. However, there remains limited research integrating qualitative perspectives with large-scale quantitative data to identify determinants of CS preference in Thailand. This study addresses this gap by applying a three-phase mixed-methods approach to examine attitudes, perceptions and factors influencing non-medically indicated CS decisions among pregnant women.
This research aimed to examine the attitudes, perceptions and opinions of pregnant women regarding non-medically indicated CSs. The findings will guide the development of an intervention model to address and manage the rising CS rate in Thailand.
Methods
Study Approval and Registration
This study was approved by the Siriraj Ethics Committee of the Faculty of Medicine Siriraj Hospital (approval number Si-802/2023) and was registered with the Thai Clinical Trials Registry (TCTR20230913007).
Study Design and Objective
We conducted a prospective descriptive implementation study to explore the attitudes, perceptions and opinions of pregnant women towards non-medically indicated CSs. This survey-based research aimed to inform the development of an intervention model to address and manage rising CS rates.
Patient and Public Involvement
Patients and the public were not involved in the design, conduct, reporting, or dissemination plans of this study. The study focused on collecting data through structured interviews and surveys with pregnant women as participants. While direct involvement of patients or the public was not included, the research aims to address maternal health concerns and inform clinical and public health practices to better meet their needs. Future research may incorporate patient and public involvement to refine study designs and enhance relevance to target populations.
Sample Size Calculation
To ensure sufficient statistical power and reliable data, we calculated the required sample size on the basis of an anticipated proportion of 50% (P = 0.5). The calculation assumed a 95% confidence level (type I error of 0.05, two-sided) and a maximum allowable estimation error of 5%. This calculation revealed that at least 385 pregnant women were needed for the study. We therefore planned to recruit 400 participants to account for potential non-response or incomplete data.
Study Phases
The research comprised three phases.
Phase I: In-Depth Interviews
Between May 1 and May 30, 2024, during the first phase, we conducted in-depth interviews to gather comprehensive information in four areas: general participant information, and attitudes, perceptions and opinions regarding non-medically indicated CSs. We recruited approximately 10% of the total required sample, resulting in 40 pregnant women participating in this phase.
Interested participants were invited to a private counselling room at antenatal clinic, where the research project was thoroughly explained. They were given time to ask questions and decide on their participation. The women’s involvement in the study was voluntary, and they could decline to take part or could withdraw at any time. Those who agreed to participate signed informed consent forms before the interviews commenced.
The semi-structured interview guide was organised into the following domains:
1. Sociodemographic and obstetric background;
2. Previous pregnancy and childbirth experiences;
3. Attitudes towards vaginal birth and CS;
4. Perceptions of risks and benefits of non-medically indicated CS;
5. Cultural and social influences (eg family opinions, auspicious birth date, social norms); and
6. Decision-making processes and expectations of counselling from healthcare professionals.
Basic demographic and clinical data were recorded using a short structured form. All interviews were conducted in Thai, audio-recorded with participant consent and lasted approximately 30–45 minutes. Recordings were transcribed verbatim and anonymised prior to analysis.
Qualitative data were analysed using thematic analysis. Two researchers first familiarised themselves with the transcripts and independently coded an initial subset of interviews to identify meaningful units related to the research questions. Codes were compared and discussed to develop a shared codebook, and discrepancies were resolved through discussion to enhance reliability. The remaining transcripts were coded using this codebook, and codes were iteratively grouped into broader themes through constant comparison. Themes from Phase I informed the development of the structured questionnaire used in Phases II and III.
Phase II: Questionnaire Development and Validation
Between 1 June and 30 June 2024, findings from Phase I and relevant literature were used to develop a structured questionnaire. The draft instrument comprised four main sections:
1. Demographic and clinical characteristics;
2. Attitudes towards non-medically indicated CSs;
3. Opinions and preferences regarding mode of delivery; and
4. Perceptions of risks and complications associated with CS.
The draft questionnaire underwent expert review by a multidisciplinary panel including obstetricians, an epidemiologist and a social scientist to assess face and content validity, particularly item clarity, relevance and comprehensiveness. Their feedback was used to refine item wording and response options.
The revised questionnaire was then pilot-tested in a convenience sample of pregnant women attending the antenatal clinic to evaluate comprehensibility, length and layout. Minor modifications were made to improve clarity and flow. Internal consistency of the main attitude and perception scales was assessed using Cronbach’s alpha, which indicated acceptable reliability for all key subscales.
Phase III: Survey Administration
In the final phase, from July 1 to July 30, the validated questionnaire was administered to 400 pregnant women attending the antenatal clinic.
Eligible participants were pregnant women aged 18 years or older who could read and understand Thai and were receiving antenatal care at the study site. We excluded women with severe medical or psychiatric conditions that precluded participation and those who were unable to complete the questionnaire in Thai. Questionnaires that were substantially incomplete (eg with a high proportion of missing responses in key sections) were excluded from the analysis.
The questionnaire was administered as a self-administered paper form in Thai and completed in the waiting area before or after the antenatal visit. Trained research nurses were available to clarify any questions about the items but did not influence participants’ responses. Completed forms were checked for completeness at the time of collection; questionnaires with minor missing data were retained, and missing values were handled as described in the Statistical analysis section.
This phase aimed to gather detailed quantitative information on participants’ attitudes, perceptions and opinions regarding non-medically indicated CSs and to identify factors associated with preference for CS.
Part 4 of the questionnaire clearly stated that the scenario was hypothetical and specifically referred to non-medically indicated CS, and item 1 (“If your doctor recommends a caesarean section, you will follow his/her advice”) was intended to measure willingness to accept CS based on physician recommendation even when no clinical indication is present.
Reporting of this study follows the STROBE cohort reporting guideline, with checklist providedin Supplementary File 1. Details of the complete questionnaire structure, including Parts I–V, are available in Supplementary File 2.
Statistical Analysis
Demographic and clinical data were summarised using descriptive statistics. Categorical variables are presented as counts and percentages, whereas continuous variables are reported as means and standard deviations. Attitudes, perceptions and opinions towards non-medically indicated CSs are also presented as counts, percentages, means and standard deviations, as appropriate.
For the main outcome, we compared women who preferred natural delivery with those who preferred CS. We used univariable chi-squared tests (or Fisher’s exact test when expected cell counts were small) to analyse factors associated with preference for CS. Variables with a P-value <0.10 in the univariable analysis were then included in a multivariable logistic regression model. The strength of associations is reported as odds ratios (ORs) with 95% confidence intervals (CIs). A two-sided P-value <0.05 was considered statistically significant.
Before fitting the multivariable model, we assessed multicollinearity among independent variables using variance inflation factors, which were all below commonly accepted thresholds, indicating no serious multicollinearity. The number of events per variable satisfied recommended criteria for logistic regression. Model fit was evaluated using the Hosmer–Lemeshow goodness-of-fit test and Nagelkerke R2 to assess calibration and explanatory power. All the statistical analyses were performed using IBM SPSS Statistics, version 29 (IBM Corp, Armonk, NY, USA).
Results
Participant Demographics
The 400 participants had a mean (± standard deviation [SD]) age of 32.1 years and a mean body mass index of 26.2 kg/m2. The large majority were Buddhist (95.5%) and married (94.4%). Educational attainment was predominantly at the bachelor’s degree level (51.7%), and the most common occupation was company employee (33.3%). Medical coverage through Thailand’s Social Security Scheme was reported by 46.3% of the participants. Most pregnancies (94.2%) were conceived naturally, and 52.3% of the participants were primiparous. Previous miscarriages were reported by 19.8% of the participants (Table 1).
 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Decision-Making Factors for CS
For 84.7% (n = 339) of the participants, consulting a doctor was crucial in CS decision-making. Advanced maternal age significantly influenced CS choices, with 79.9% (n = 320) considering it important. Health conditions such as diabetes and hypertension were influential for 76.5% (n = 306) of the participants. Predictability in scheduling CSs was valued by 75% (n = 300) of the participants for work and childcare planning.
In contrast, concerns over pelvic health (11.5%, n = 46), differences in pain between delivery methods (34.5%, n = 138) and social media influence (44.3%, n = 177) had lower impacts on decision-making. Family presence during delivery influenced 59.2% (n = 237) of the participants. Cost was a barrier for 50.7% (n = 203), while cultural timing preferences mattered for 39.5% (n = 158; Table 2).
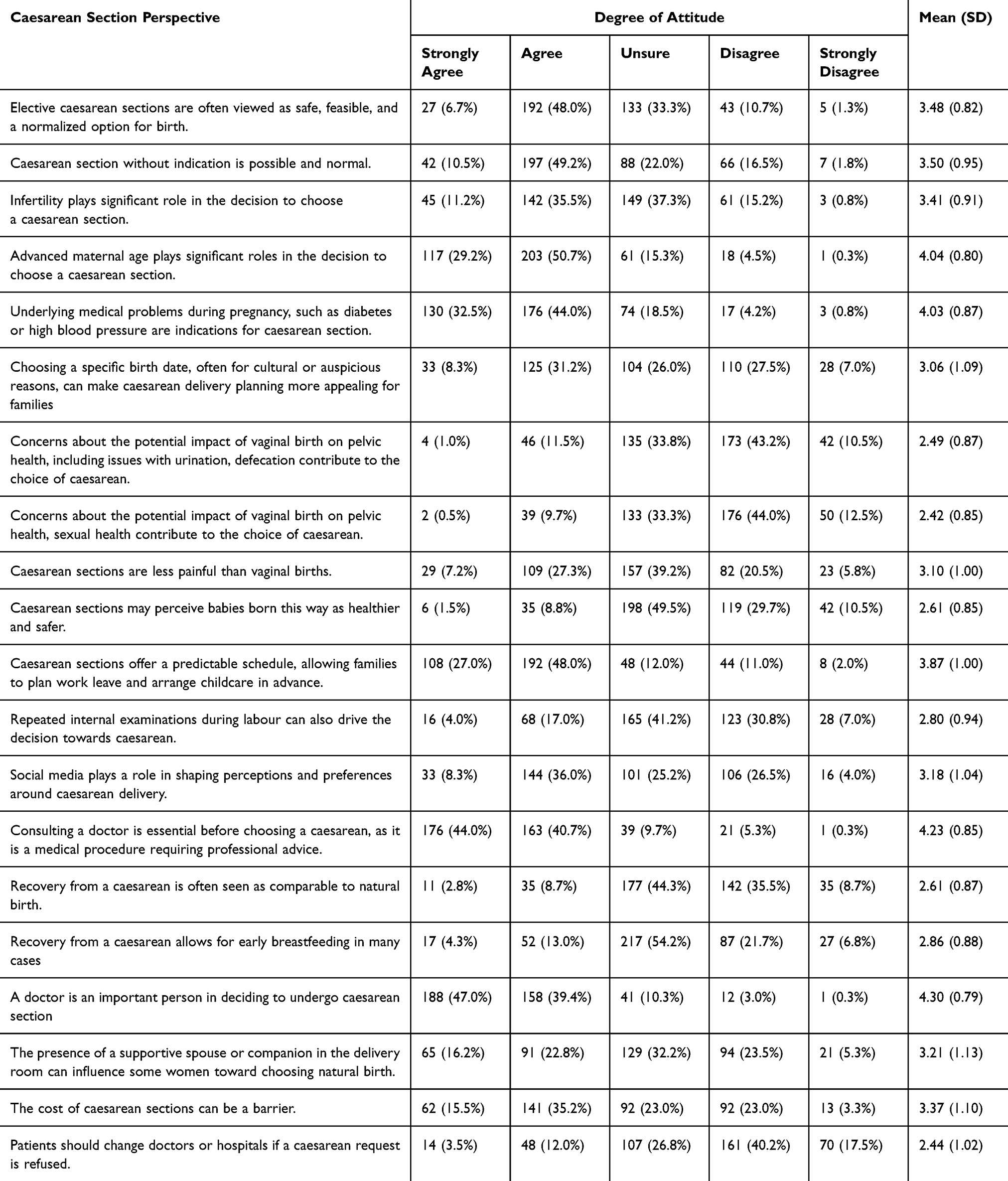 |
Table 2 Attitudes Towards Non-Medically Indicated Caesarean Sections |
Awareness and Preferences Regarding CS
Of the participants, 59.5% reported awareness of rising CS rates both globally and in Thailand. Prior to delivery, 69.2% expressed a preference for vaginal delivery. When presented with a hypothetical doctor’s recommendation for CS, 77.0% indicated that they would accept the procedure. Doctor recommendation was cited as the most influential factor in delivery method decision-making (93.5%).
The participants who declined a CS (n = 33) cited high costs (63.6%) and fear of surgical pain (45.5%) as primary reasons. Awareness of CS complications was high: 84.8% recognised a slower recovery, and 44.3% acknowledged greater risks of blood loss than with natural birth. Additionally, 52.5% rated the birth date as a “moderate” factor in delivery timing decisions (Table 3 and Figure 1).
 |
Table 3 Knowledge of Non-Medically Indicated Caesarean Sections |
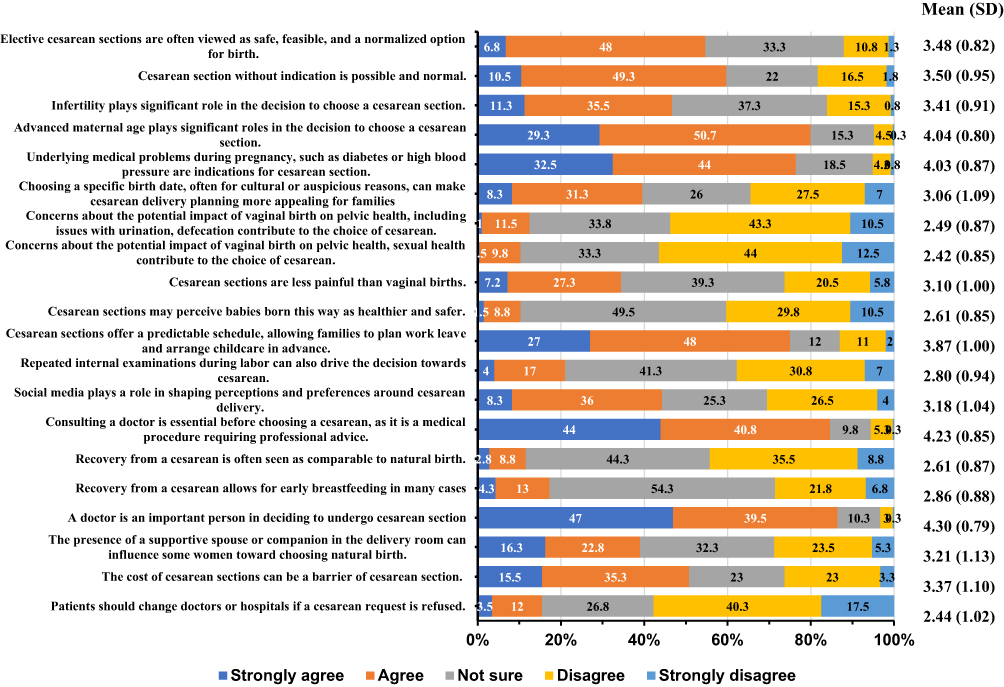 |
Figure 1 Attitudes towards non-medically indicated caesarean sections. |
Opinions on Non-Medically Indicated CSs
The participants’ opinions on CSs without medical indications varied across several factors. Most respondents indicated that they would follow a doctor’s recommendation for a CS (79.3%), and 93% expressed trust in their doctor’s guidance. Scheduling benefits were influential, with 62.7% favouring CSs for planning; however, only 17.8% valued auspicious timing.
While the majority acknowledged higher costs associated with CSs (92.5%), opinions on affordability were mixed, with 50.5% feeling comfortable with the expense. Safety perceptions varied: 54% were uncertain if a CS was safer than a natural birth, whereas 28.5% chose a CS because of concerns over birth canal injury. Pain considerations influenced 37.3% of the participants to choose CS, although 31.3% considered natural birth with epidural anaesthesia.
Social media had minimal influence on decision-making (3.3%), but 32% noted that spousal presence during delivery could encourage opting for a natural birth (Table 4 and Figure 2).
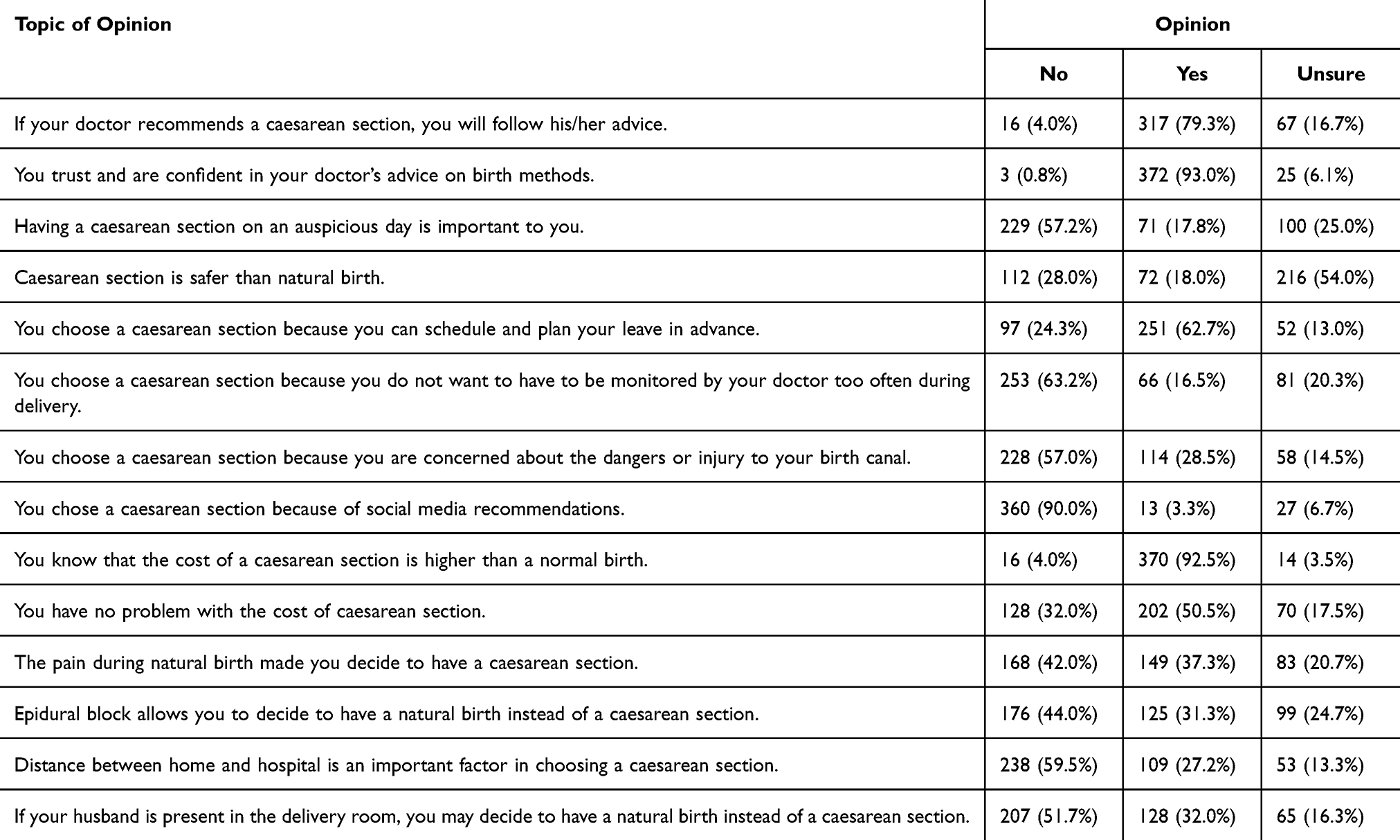 |
Table 4 Opinions on Non-Medically Indicated Caesarean Sections |
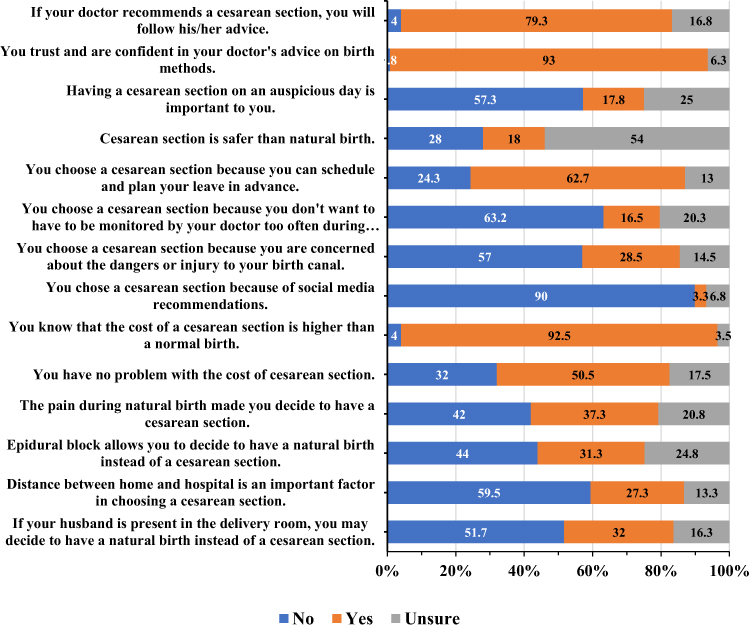 |
Figure 2 Opinions on non-medically indicated caesarean sections. |
Perceptions of Risks and Complications
The participants expressed varying perspectives on CSs without medical indications, with notable awareness of associated risks and complications. A significant majority (59.4%) acknowledged that CSs could involve more complications than a natural birth, reflected in a mean score of 3.68 (SD 0.73). Most respondents recognised that CSs may deprive infants of beneficial bacteria acquired during vaginal delivery (49.3%, mean 3.61, SD 0.80) and lead to greater blood loss (63.5%, mean 3.74, SD 0.68).
With respect to non-medical factors, only 17.8% of the participants considered auspicious timing to be important for delivery (mean 2.54, SD 1.00). Similarly, family influence on CS decisions was low, with only 14.8% agreeing that their decision was influenced by family preferences (mean 2.37, SD 0.93) and 26.5% feeling pressured by family members (mean 2.01, SD 0.81). Confidence in independent decision-making was relatively high, as shown by a mean score of 3.88 (SD 0.97).
The belief that CSs should be performed only when they are medically indicated received strong support, with a mean score of 4.04 (SD 0.89). Overall, the data highlighted a strong reliance on medical advice, with 79.3% stating that they would follow their doctor’s recommendations and a mean score of 4.31 (SD 0.75) for the influence of doctors in CS decisions (Table 5 and Figure 3).
 |
Table 5 Perceptions of Risks and Complications Associated with Caesarean Sections |
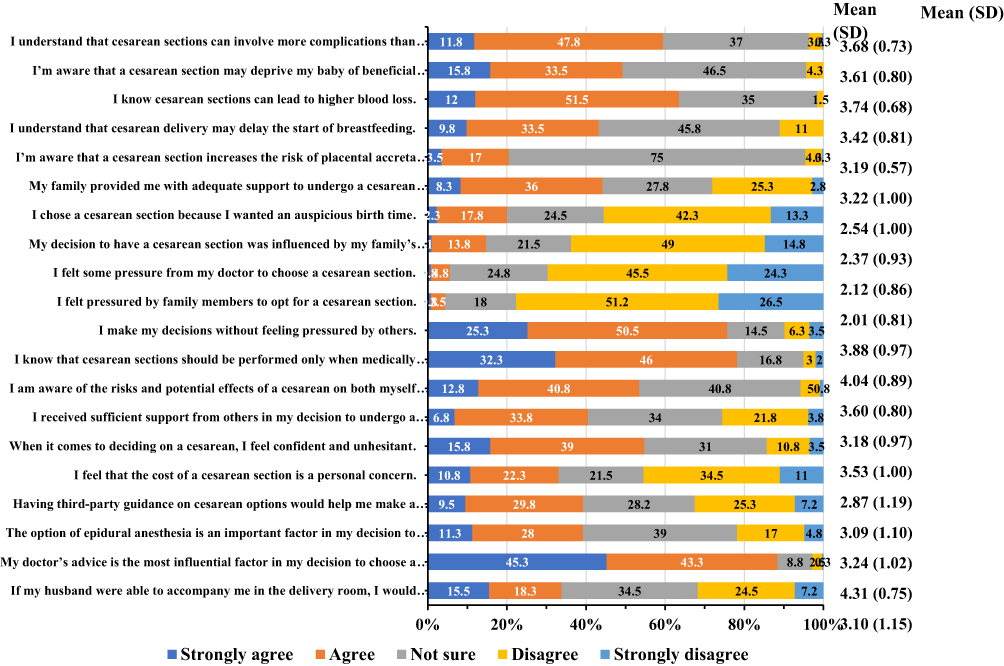 |
Figure 3 Perceptions of caesarean sections: risks, benefits and influences. |
Factors Influencing the Desire for CS (Univariable Analysis)
Table 6 presents the unadjusted ORs comparing various demographic factors between women who desired natural deliveries and those considering CSs. Key findings indicate that non-private cases were more likely to result in a desire for CS (OR 1.663, P = 0.052). Women with a history of CS had significantly greater odds of desiring repeat CSs (OR 3.396, P < 0.001). Maternal age also played a role, with women aged 35 years and older being more likely to prefer a CS (OR 2.378, P < 0.001).
 |
Table 6 Comparison of Demographic Data Between Women Opting for Natural Delivery and Caesarean Section |
Participants with at least a bachelor’s degree had higher odds of opting for CS (OR 1.917, P = 0.024), as did women with an income over 30,000 baht per month (OR 1.796, P = 0.023). Assisted conception methods were associated with increased odds of preferring CS (OR 4.262, P < 0.001), and women with underlying diseases were also more likely to consider CS (OR 2.558, P = 0.001). Additionally, a history of miscarriage (OR 2.137, P = 0.014) and concerns regarding infertility (OR 2.502, P = 0.007) were associated with a greater likelihood of preferring CS. These results indicate that demographic and medical history factors significantly influence the desire for CS among pregnant women (Table 6).
Multivariable Analysis of Factors Associated with CS
Multivariable analysis revealed three factors significantly associated with CS preference. They were previous CS (adjusted OR 3.990, 95% CI 1.021‒15.59, P = 0.047), maternal age > 35 years (adjusted OR 1.892, 95% CI 1.029‒3.479, P = 0.040) and the presence of underlying diseases (adjusted OR 2.193, 95% CI 1.131‒4.254, P = 0.020). These findings underscore the importance of previous delivery experiences, maternal age and health conditions in determining the likelihood of opting for a CS (Table 7).
 |
Table 7 Factors Associated with Caesarean Section: Univariable and Multivariable Analysis |
Discussion
This study explored pregnant women’s attitudes towards, acceptance of, and perceptions regarding CSs without medical indications. The findings revealed significant associations between various factors and the likelihood of opting for CS. Notably, maternal age over 35 years, a history of previous CS and underlying medical conditions were linked to increased odds of choosing CS. Additionally, preferences for assisted conception methods significantly influenced delivery method decisions. These insights illuminate how maternal characteristics and perceptions impact delivery choices, providing a foundation for discussing implications for maternal health and clinical practice.
The escalating rate of non-medically indicated CS raises critical questions about patients’ attitudes towards and perceptions of this surgical intervention. Research indicates that while many women prefer vaginal delivery, a significant number opt for CS, often influenced by fear of labour pain and prior birth experiences. For example, Yaqoub et al 14 highlighted that antenatal and postnatal women in Jeddah displayed limited awareness of CS complications, suggesting a knowledge gap shaping their preferences. Similarly, Souza et al 15 reported that non-medically indicated CS is associated with increased risks of adverse maternal outcomes, reinforcing the need for informed decision-making among patients.
Many participants in our study perceived CS as a safer and more controlled delivery option, particularly with respect to pain management and predictability. A study involving 410 pregnant women in Kermanshah, Iran, revealed that most participants held a positive attitude towards normal delivery, especially those with prior experience. However, 21.5% preferred CS, emphasising the necessity for targeted educational interventions.16 Furthermore, some respondents exhibited limited awareness of the risks associated with CS, such as longer recovery times and higher maternal morbidity. The limited understanding of CS risks mirrors global trends, where convenience and fear of labour pain drive preferences for CS even without medical indications.
Promoting comprehensive and balanced counselling on delivery options is essential. By increasing awareness of the potential benefits of vaginal delivery—such as shorter recovery times, reduced surgical risks and fewer complications in subsequent pregnancies—healthcare providers can address misconceptions leading to elective CS. Structured prenatal education and open dialogue with healthcare professionals are crucial for fostering informed, safe and satisfying birth experiences.
A study in Thailand by Yamasmit and Chaithongwongwatthana 17 reported that 87.5% of pregnant women preferred vaginal delivery, motivated by a desire for a natural process. In contrast, concerns about pain led some to favour CS. This finding indicates that while women may have preferences, external influences significantly shape their final decisions regarding delivery methods. Cultural beliefs, individual experiences and family support often affect these decisions, as observed in a Ghanaian study.18
Educational interventions are critical, as demonstrated by Maitanmi et al’s 19 findings in Nigeria, which revealed a high level of awareness and positive attitudes towards CS but persistent knowledge gaps. Enhancing education on the risks and benefits of both CS and vaginal deliveries empowers women to make informed choices aligned with their preferences and health needs.
The ethical implications surrounding CS without medical indications continue to generate discussions among healthcare professionals. Eide and Bærøe 20 emphasised the importance of trust, shared decision-making and a balanced approach to patient autonomy. This approach acknowledges the inherent power dynamics between patients and healthcare providers and advocates for transparent information exchange and collaborative decision-making.
In Thailand, healthcare professionals, particularly obstetricians, significantly influence pregnant women’s attitudes and decisions regarding delivery methods. Research consistently shows that expectant mothers trust their doctors’ and midwives’ advice, often viewing them as authoritative figures in maternal and infant health.21,22 This reliance on medical guidance means that the recommendations and counselling provided by healthcare professionals can profoundly impact delivery choices, especially concerning CS. In our study, physician recommendation was an influential factor even in situations without a definitive medical indication, reflecting decision-making in grey-zone or preference-driven scenarios where clinical judgement and counselling can shape maternal choice.
When doctors recommend a CS—either directly or indirectly—many pregnant women are likely to comply, believing that the advice is based on medical necessity and best practices. This dynamic underscores the importance of effective communication and counselling during prenatal care. Healthcare professionals must engage in comprehensive discussions with patients, providing clear information about the risks and benefits of various delivery methods. A collaborative environment where patients feel comfortable expressing their preferences and concerns enables women to make informed decisions aligned with their values and health needs.
In Saudi Arabia, while most pregnant women possess adequate knowledge about elective CS, the majority hold negative attitudes towards it, highlighting the necessity for healthcare providers to offer comprehensive education on potential consequences to reduce unnecessary procedures.14 Similarly, in rural Nigeria, although most pregnant women are aware of CS and would accept it if necessary, overall knowledge about the procedure remains limited.23 A study at the University of Benin Teaching Hospital in Nigeria revealed that while women had good knowledge of CS, only 6.1% would choose it as a delivery method, with 81% willing to accept it only in life-saving situations. Cultural misconceptions and low education levels contributed to their reluctance, emphasising the need for community programmes to improve perceptions of CS.24
Education and preparation for delivery are essential components of prenatal care that can significantly influence outcomes. Expectant mothers who are well informed about the birthing process, including the implications of choosing a CS, are more likely to actively participate in decision-making, potentially reducing the overall rate of unnecessary CS. Implementing structured educational programmes during antenatal visits can equip women with the knowledge to make informed choices, ultimately decreasing CS rates.
Our study contrasts women’s perceptions of CS as a safer option with clinicians’ concerns about associated health risks, revealing differing attitudes towards maternally requested CS.25 While women expect support for their CS choice, clinicians feel a responsibility to encourage vaginal births, underscoring the need for respectful and balanced dialogue.25
In the United States, nearly one-third of deliveries are CSs, which pose greater maternal and neonatal risks than does vaginal delivery. Following a previous CS, women must choose between attempting vaginal birth or undergoing a repeat CS. Approximately 75% of vaginal births attempted after having had a previous CS are successful. General practitioners can be key in providing comprehensive maternity care.22
Overall, healthcare professionals are responsible for ensuring that patients receive appropriate counselling that reflects current medical guidelines and practices. The counselling process should include transparency about the implications of non-medically indicated CS and discussions of the factors that may warrant such a decision based on the individual patient’s health status. By addressing these issues openly and empathetically, doctors can build stronger rapport with their patients and encourage a more informed and shared decision-making process.
The ethical implications surrounding CS without medical indications continue to generate discussion among healthcare professionals. Brown and Mulligan 26 argue for routinely offering planned CS to all pregnant women, regardless of clinical need. This perspective emphasises that healthcare practitioners have a duty to inform women about planned CS as a viable option rather than assuming that vaginal delivery is the default choice. Advocating for planned CS to be discussed alongside vaginal delivery enables informed choice and supports women’s preferences regarding their mode of delivery. This approach aligns with the need for comprehensive counselling, allowing expectant mothers to make decisions that reflect their values and health needs.
In summary, understanding how pregnant women feel about and perceive non-medically indicated CS is vital for developing strategies that help them make informed decisions and improve their health outcomes. Doctors and obstetricians play a crucial role in this process, as their guidance significantly influences outcomes for both mothers and babies. Ongoing research and education are necessary to fill knowledge gaps and ensure that care is centred on patients’ needs. By emphasising patient education and fostering a supportive environment for open discussions, healthcare providers can help lower the rates of unnecessary CS while prioritising maternal health. With proper counselling and education, pregnant women can better understand their options, leading to safer and more positive delivery experiences.
Strengths and Limitations of the Study
This study has several important strengths. The three-phase mixed-methods design, comprising qualitative interviews, questionnaire development and validation, and a large-scale quantitative survey, allowed for an in-depth understanding of women’s perceptions and ensured methodological rigor. The relatively large sample size (n=400) provided adequate statistical power to examine determinants of non-medically indicated caesarean section preferences. Furthermore, the integration of qualitative findings into the questionnaire enhanced cultural relevance and ensured that survey items reflected real maternal perspectives. Importantly, the research offers updated, Thailand-specific evidence in a field where recent data are scarce.
Some limitations should also be noted. Although the study was conducted at a single institution, Siriraj Hospital serves as a super-tertiary referral center that receives patients from multiple regions across Thailand, including both government and private sector antenatal services, which supports the diversity of the sample. Nevertheless, the findings may still primarily reflect women who have access to tertiary-level care, and results may differ in smaller provincial or community-based settings. Certain subgroups were relatively small, leading to wider confidence intervals for specific variables. In addition, data were self-reported and may be subject to social desirability or recall bias. While participants expressed improved confidence in decision-making when counselling was provided, counselling itself was not evaluated as an intervention; therefore, implications for practice should be interpreted cautiously. Finally, the cross-sectional study design limits causal inference, and future longitudinal or implementation-based studies could clarify how counselling influences delivery decisions over time.
Conclusions
This study identified significant factors associated with the likelihood of non-medically indicated caesarean section among pregnant women who initially preferred natural birth. Women aged over 35 years, those with a previous caesarean delivery, underlying medical conditions, and assisted conception were more likely to prefer or accept CS. These findings emphasise the complex interaction of maternal characteristics, cultural beliefs, and clinical considerations in shaping delivery decisions. Although this study did not evaluate counselling interventions directly, the strong influence of physician recommendations suggests that structured antenatal counselling may have the potential to reduce unnecessary CS. The findings contribute contemporary evidence relevant to Thai maternity care and may inform clinical communication strategies and policy development aimed at promoting informed, safe birth choices.
Data Sharing Statement
The data supporting the findings of this study are available from the Faculty of Medicine Siriraj Hospital, Mahidol University. However, restrictions apply to the availability of these data, which were used under licence for the current study and are not publicly available. Data are available from the authors upon reasonable request and with permission from the Faculty of Medicine Siriraj Hospital, Mahidol University.
Ethics Approval and Consent to Participate
This research was approved by the Ethics Committee of the Siriraj Institutional Review Board (approval number Si-802/2023). All procedures performed in this study involving human participants were conducted in accordance with institutional guidelines and the Declaration of Helsinki. Written informed consent was obtained from all participants included in the study.
Acknowledgments
We thank the Royal College of Obstetricians and Gynaecologists of Thailand and the Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand, for their funding support. Finally, we are grateful to Mr. David Park for his assistance with English-language editing of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received financial support from the “Pol Gen Dr Jongjate Aojanepong Fund” of the Royal College of Obstetricians and Gynaecologists of Thailand (grant number: RTCOG2401) and the Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand. The opinions expressed in this article are those of the authors and are not necessarily endorsed by the Royal College of Obstetricians and Gynaecologists of Thailand. Editorial assistance in the preparation of this article was provided by Mr David Park. Support for this assistance was funded by the Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boerma T, Ronsmans C, Melesse DY, et al. Global epidemiology of use of and disparities in caesarean sections. Lancet. 2018;392(10155):1341–1348. doi:10.1016/S0140-6736(18)31928-7
2. Tang S, Li X, Wu Z. Rising cesarean delivery rate in primiparous women in urban China: evidence from three nationwide household health surveys. Am J Obstet Gynecol. 2006;195(6):1527–1532. doi:10.1016/j.ajog.2006.03.044
3. Chawanpaiboon S, Sutantawibul A. Mode of delivery at siriraj hospital: a ten-year review (2001-2010). Thai J Obstet Gynaecol. 2011;19:181–192.
4. Titapant V, Phithakwatchara N. Trends in modes of delivery in Siriraj Hospital. Siriaj Med J. 2007;59:271–273.
5. Lumbiganon P, Laopaiboon M, Gülmezoglu AM, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007-08. Lancet. 2010;375(9713):490–499. doi:10.1016/S0140-6736(09)61870-5
6. Shah A, Fawole B, M’Imunya JM, et al. Cesarean delivery outcomes from the WHO global survey on maternal and perinatal health in Africa. Int J Gynaecol Obstet. 2009;107(3):191–197. doi:10.1016/j.ijgo.2009.08.013
7. Villar J, Valladares E, Wojdyla D, et al. Caesarean delivery rates and pregnancy outcomes: the 2005 WHO global survey on maternal and perinatal health in Latin America. Lancet. 2006;367(9525):1819–1829. doi:10.1016/S0140-6736(06)68704-7
8. World Health Organization. Appropriate technology for birth. Lancet. 1985;2(8452):436–437.
9. Molina G, Weiser TG, Lipsitz SR, et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015;314(21):2263–2270. doi:10.1001/jama.2015.15553
10. Smith R. Parturition. N Engl J Med. 2007;356(3):271–283. doi:10.1056/NEJMra061360
11. Villar J, Carroli G, Zavaleta N, et al. Maternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective study. BMJ. 2007;335(7628):1025. doi:10.1136/bmj.39363.706956.55
12. Signore C, Klebanoff M. Neonatal morbidity and mortality after elective cesarean delivery. Clin Perinatol. 2008;35(2):361–371. (). doi:10.1016/j.clp.2008.03.009
13. Mylonas I, Friese K. Indications for and risks of elective cesarean section. Dtsch Arztebl Int. 2015;112(29–30):489–495. doi:10.3238/arztebl.2015.0489
14. Yaqoub RM, Khouj MA, Alsaif AA, Eissa GA, Alhemdi JA, Albasri S. Awareness and knowledge of caesarean section complications among women in Jeddah, Saudi Arabia. Cureus. 2022;14(12):e32152. doi:10.7759/cureus.32152
15. Souza JP, Gülmezoglu A, Lumbiganon P, et al. Caesarean section without medical indications is associated with an increased risk of adverse short-term maternal outcomes: the 2004-2008 WHO global survey on maternal and perinatal health. BMC Med. 2010;8:71. doi:10.1186/1741-7015-8-71
16. Siabani S, Jamshidi K, Mohammadi MM. Attitude of pregnant women towards Normal delivery and factors driving use of caesarian section in Iran (2016). Biopsychosoc Med. 2019;13:8. doi:10.1186/s13030-019-0149-0
17. Yamasmit W, Chaithongwongwatthana S. Attitude and preference of Thai pregnant women towards mode of delivery. J Med Assoc Thai. 2012;95(5):619–624.
18. Bam V, Lomotey AY, Kusi-Amponsah Diji A, Budu HI, Bamfo-Ennin D, Mireku G. Factors influencing decision-making to accept elective caesarean section: a descriptive cross-sectional study. Heliyon. 2021;7(8):e07755. doi:10.1016/j.heliyon.2021.e07755
19. Maitanmi BT, Oluyomi OV, Aderemi IO, et al. Knowledge, attitude and perception of cesarean section among pregnant women attending antenatal clinic at Babcock University Teaching Hospital, Ilishan-Remo, Ogun State. J Matern Fetal Neonatal Med. 2023;36(2):2278019. doi:10.1080/14767058.2023.2278019
20. Eide KT, Bærøe K. How to reach trustworthy decisions for caesarean sections on maternal request: a call for beneficial power. J Med Ethics. 2020;47(12):e45. doi:10.1136/medethics-2020-106071
21. Panda S, Daly D, Begley C, et al. Factors influencing decision-making for caesarean section in Sweden - a qualitative study. BMC Pregnancy Childbirth. 2018;18(1):377. doi:10.1186/s12884-018-2007-7
22. Quinlan JD, Murphy NJ. Cesarean delivery: counseling issues and complication management. Am Fam Physician. 2015;91(3):178–184.
23. Ashimi A, Amole T, Aliyu L. Knowledge and attitude of pregnant women to caesarean section in a semi-urban community in northwest Nigeria. J West Afr Coll Surg. 2013;3(2):46–61.
24. Aziken M, Omo-Aghoja L, Okonofua F. Perceptions and attitudes of pregnant women towards caesarean section in urban Nigeria. Acta Obstet Gynecol Scand. 2007;86(1):42–47. doi:10.1080/00016340600994950
25. Johansson M, Alvan J, Pettersson A, Hildingsson I. Conflicting attitudes between clinicians and women regarding maternal requested caesarean section: a qualitative evidence synthesis. BMC Pregnancy Childbirth. 2023;23(1):210. doi:10.1186/s12884-023-05471-2
26. Brown RC, Mulligan A. ‘Maternal request’ caesarean sections and medical necessity. Clin Ethics. 2023;18(3):312–320. doi:10.1177/14777509231183365
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Perceptions of Chronic Patients in Saudi Arabia Regarding the Use of Artificial Intelligence to Improve Medication Adherence
Alsanosi SM, Aldajani AQ, Gheliwi HA, Alotibi MM, Bokhari GS, Almatrafi OA, Alqawlaq AK, Abujamai JZ, Shaikhomer M, Alhindi YZ, Alshanberi AM
Patient Preference and Adherence 2025, 19:1781-1792
Published Date: 19 June 2025
Knowledge, Attitude and Practice Regarding Thyroid Disorders in Pregnant Women: A Cross-Sectional Study in Guangdong, China
Han L, Jin J, Xu J, Wang H, Qin A, Chen J
International Journal of Women's Health 2025, 17:2001-2013
Published Date: 10 July 2025