Back to Journals » Open Access Emergency Medicine » Volume 12
Attention Deficit Hyperactivity Disorder (ADHD) in Patients with and without Head Trauma
Authors Amiri S ![]() , Esmaeili E, Salehpour F
, Esmaeili E, Salehpour F ![]() , Mirzaei F
, Mirzaei F ![]() , Barzegar H, Mohammad Namdar A, Sadeghi-Bazargani H
, Barzegar H, Mohammad Namdar A, Sadeghi-Bazargani H
Received 9 June 2020
Accepted for publication 8 October 2020
Published 17 November 2020 Volume 2020:12 Pages 405—410
DOI https://doi.org/10.2147/OAEM.S265883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Shahrokh Amiri,1 Elham Esmaeili,2 Firooz Salehpour,3 Farhad Mirzaei,4 Habibeh Barzegar,5 Aysan Mohammad Namdar,6 Homayoun Sadeghi-Bazargani7
1Child and Adolescent Psychiatry, Research Center of Psychiatry and Behavioral Sciences, Tabriz University of Medical Sciences, Tabriz, Iran; 2Psychiatry, Research Center of Psychiatry and Behavioral Sciences, Tabriz University of Medical Sciences, Tabriz, Iran; 3Department of Neurosurgery, School of Medicine, Imam Reza Medical Research & Training Hospital, Tabriz University of Medical Science, Tabriz, Iran; 4Neurosurgery, Tabriz University of Medical Sciences, Tabriz, Iran; 5Health Psychology, Research Center of Psychiatry and Behavioral Sciences, Tabriz University of Medical Sciences, Tabriz, Iran; 6Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 7Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Homayoun Sadeghi-Bazargani
Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Golgasht Ave, Tabriz, Iran
Tel +989144027218
Email [email protected]
Purpose: Attention deficit hyperactivity disorder (ADHD) in adults is one of the psychological problems that can increase the risk of accidents and trauma, especially head trauma. Recent studies have reported the frequency of adult attention deficit hyperactivity disorder (ADHD) among trauma patients. Adult AD0HD has been reported in trauma patients. In the present study, we hypothesized that adult ADHD was more common among head trauma patients following an accident compared to a group without trauma.
Materials and Methods: In this case-control study, 230 patients with head injuries and 460 non-trauma patients were selected. The adult Connors self-report screening scale (CAARS-SV) was used to screen for ADHD. Three subscales as subscale A (attention deficit index), subscale B (hyperactivity index) and subscale D (ADHD index) were evaluated between the two groups. Using linear multiple regression analysis, the effect of group, age, gender, and socioeconomic variables on ADHD scores was evaluated.
Results: The total frequency of adult ADHD was 9.5%, which was equal to 1.6% in the trauma group and 9.5% in the non-trauma group. The experimental group had more drivers as the job (11.7% vs 3.7%, P< 0.001) compared to the control group. Of the Connors subscales, only the D subscale was significantly lower in the case group than in the control group (6.35 6 5.11 vs 51.72 4 72.4, P=0.003). The prevalence of ADHD in patients with head trauma and non-trauma head injury was 6.1% and 5.9%, respectively, which did not show a statistically significant difference (P=0.9). Linear regression analysis showed that the subscale D only had a significant relationship with group and age. However, by entering variables in logistic regression analysis, it was observed that only the age variable was significant in the presence of other variables.
Conclusion: According to the results of the present study, the frequency of adult ADHD in trauma patients, as a screening diagnosis, was not found to be higher than non-traumatic patients.
Keywords: attention deficit hyperactivity disorder, ADHD, adults, head trauma, traumatic brain injury
Introduction
Injuries and traumas to the head are among the most common health problems being an important factor causing disability and death in young people.1 Traumatic brain injury (TBI) is mostly presented in its mild form or cerebral concussion comprising 70–90% of all TBI cases.
The leading cause of TBI among youths aged 15 years and older is traffic accidents, while among children aged less than 5 years it is falls. Based on findings of a comprehensive review, the median estimates of the annual incidence of childhood brain injuries have been reported to be 691 per 100,000 population treated in emergency departments, 74 per 100,000 treated in hospital, and 9 per 100,000 resulting in death.2
Psychological factors have always been the field of research interest in traumatology. While it is known that people are more likely to develop psychiatric sickness after traumatic brain injury, it is less clarified whether those who sustain a traumatic brain injury are more likely to have had a psychiatric illness before their injury.3,4
Many studies have been published on association of ADHD and accidents, the majority of which have shown that there is an increased likelihood of accidents and trauma among those suffering from ADHD both at childhood and adult age.5–11 Various types of trauma and accidents have been investigated in this regard including burn injuries, fall injuries, motorcycle injuries, traffic injuries, and injuries as a whole.
Although the association between ADHD and occurrence of various accidents is nearly unanimously accepted by the researchers, there is a need for investigating the association between ADHD and traumatic brain injuries. It has been reported that those with bodily injuries may have higher prevalence of ADHD, especially reported in case of children.12–14
In a large-scale, retrospective survey study, boys and girls with ADHD were significantly more likely to report a history of concussion.15 However, in another large case control study using a health maintenance organization database, no significant association between preexisting ADHD and mild traumatic brain injury was observed.4 Research is limited in the field of adult ADHD and risk of traumatic brain injury.
The aim of the current study was to determine the relative frequency of ADHD in adults with head trauma and investigate its relationship with head trauma through a comparative study design.
Materials and Methods
This was a case-control study with the statistical population of the study including all patients with acute head trauma during sampling who were referred to the neurosurgery department of Imam Reza Medical Training Center affiliated to Tabriz University of Medical Sciences. Moreover, the statistical population of the control group was selected from among the internal medicine department patients of the same center according to their age, gender, and level of education. Sampling was available to patients with acute head trauma in the neurosurgery department and included all patients who met the criteria for admission to the study. At the same time, the control group was matched among patients admitted to the internal medicine department, taking into account the characteristics of age, gender, and level of education. To calculate the sample size, the matched case-control (MCC) function was used in STATA software package (StataCorpLLC. Texas) version 14.1. Assuming a prevalence of 8.5% and odds ratio equal to 1.96, a confidence level of 95%, a statistical power of 80%, and, in terms of lack of access to the sample during the sampling, 230 cases and 460 controls were calculated.
Criteria for entering the study:
• Age 18–45 years
• Acute head trauma
• Glasgow Coma Scale/Score (GCS) equal to or greater than 13
• Having informed written consent to participate in the study
The exclusion criteria were as follows:
• Having debilitating physical illnesses
• History of any major psychiatric illness such as major depression or psychosis in the last six months
• Taking psychiatric medication
Disruptive variables included substance abuse and alcohol use, and any chronic underlying disease associated with impaired consciousness (uremic, liver, infectious, etc.).
Closed and open questions were used to identify the distorting variables. During the research, sufficient attention was paid to identifying the confounding variables and it was controlled by adopting the appropriate research and statistical method.
Ethical Considerations
All patients were asked to provide written informed consent before entering the study. No intervention was performed on patients, and only questions were asked in the form of a questionnaire.
The study was compiled according to the Helsinki Declaration. It was approved by the ethics committee of Tabriz University of Medical sciences (ID number: 59,017). The Regional Ethical code is IR.TBZMED.REC.1397.629.
Instrument
In this study, in addition to the demographic questionnaire, which asked questions about age, gender, marital status, level of education, economic status, etc., a number of open-ended questions had been developed to control for confounding variables.
Connors Adult Self-Reporting Scale (CAAS-S: SV):
The Adult Self-Reporting Scale (Connors et al, 1998)16 is a tool for screening attention deficit hyperactivity disorder in adults, which is based on DSM-IV indicators and has three distinct key subscales: Attention deficit index (subscale A), hyperactivity-impulsivity index (subscale B), and ADHD index (subscale D). The overall score of the scale assesses the individual’s ADHD screening score.
Procedure
All patients in the case and control group were evaluated to identify and also diagnose ADHD using the Adult Self-Reporting Scale (CAAS-S: SV), the reliability and validity of which have been previously evaluated by researchers in Iran. Thus, the prevalence of ADHD in both head trauma and non-head trauma patients was assessed using this instrument.17
In this study, the ADHD index scale with a cut-off point of 16 and above was used to screen adult ADHD for screening. Back translation has been prepared. Based on unpublished preliminary studies in Tehran and Tabriz conducted on the general population and clinical clients, the cut-off point of 70 and above has been determined for the screening based diagnosis of adult ADHD. In Sadeghi-Bazargani et al’s17 study, Cronbach’s alpha coefficient for this scale was reported to be between 0.83 and 0.97 for its various subscales, and its validity was reported to be 0.88 using the ROC curve. In this study, the Adult Self-Reporting Scale was used to diagnose ADHD in patients with headaches.
Variables examined:
• Age
• Gender
• Level of Education
• Marital status
• Having ADHD based on CAAS-S: SV screening scores
Statistical Analysis
All data were analyzed using Stata 15 statistical software package. Descriptive statistical methods (frequency, percentage, mean, standard deviation) were used for statistical studies. Using the Kolmogorov-Smirnov test, the normal distribution of data was evaluated. For subscales A, B, and D, the Mann–Whitney U nonparametric test was used due to the lack of normal distribution, and the independent t-test statistical test was used to compare other quantitative findings with normal distribution. The chi-square test was also used to examine categorical variable associations. Linear regression and logistic regression analyses were used to determine the relationship between ADHD score and potential regressors. In this study, a P-value of less than 0.05 was considered significant.
Results
In this study, 230 patients with head injuries and 460 non-traumatized individuals were evaluated. The mean time between head injury and ADHD investigation was 3 days with a range of 1–14 days. All the patients with head trauma had mild severity with a GCS≥13.
With cut-off points above 16 for subscale D of the Connor’s scale, people with potential ADHD were identified. This value was equivalent to a t-score of 66.4 and the percentile 95 on subscale D within the sample population. A total of 41 people (5.9%) had ADHD based on screening results. Of these, 14 in the case group (6.1%) and 27 (5.9%) in the control group had ADHD, but there was no statistically significant difference between the two groups in terms of disease (P=0.9).
As can be seen in Table 1, the case group had a significantly lower average mean and higher male proportion. Comparing the mean Conner’s ADHD screening scores, as can be seen in Table 2, there was no statistically significant difference between the two groups, with respect to the total Conner’s ADHD screening score and the two subscale A and subscale B scores. However, the case group clearly had a lower D subscale score.
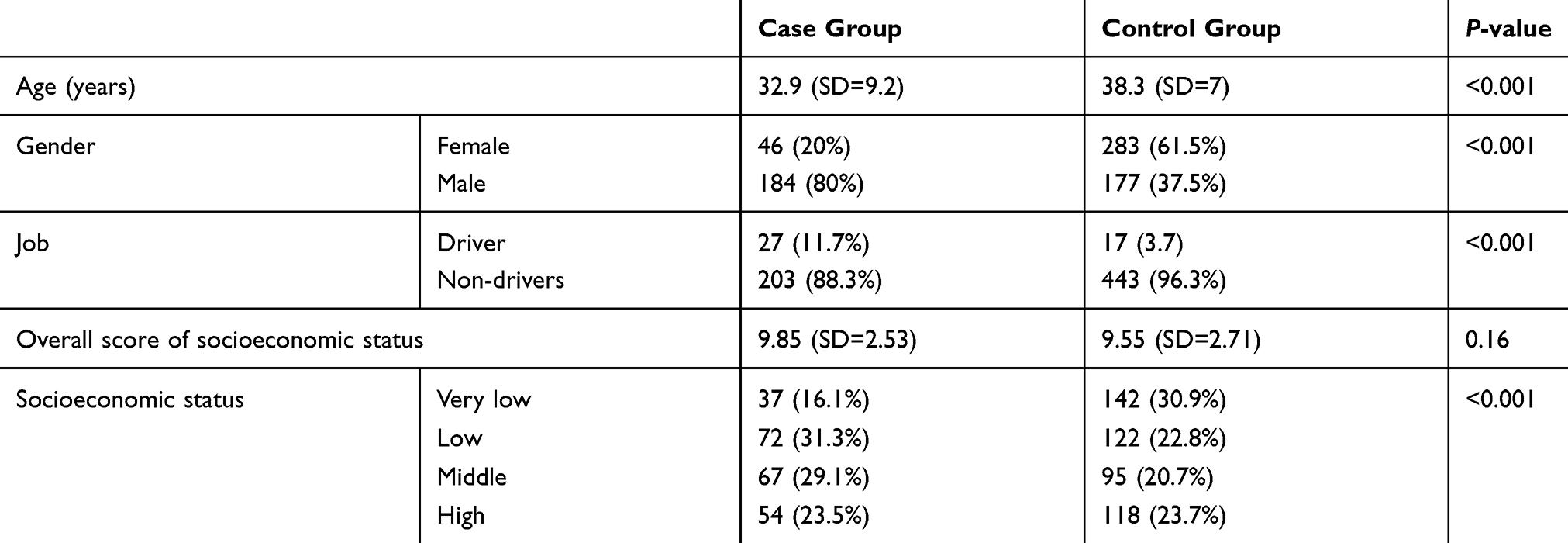 |
Table 1 Demographic Findings Compared Between the Patients with and without Head Trauma |
 |
Table 2 Conner’s Adult ADHD Screening Scale Scores Compared Between the Patients with and without Head Trauma |
In order to determine the distribution of ADHD score in three separate subscales based on demographic variables, linear regression analysis with group, age, sex, and general socioeconomic score variables were used (Table 3).
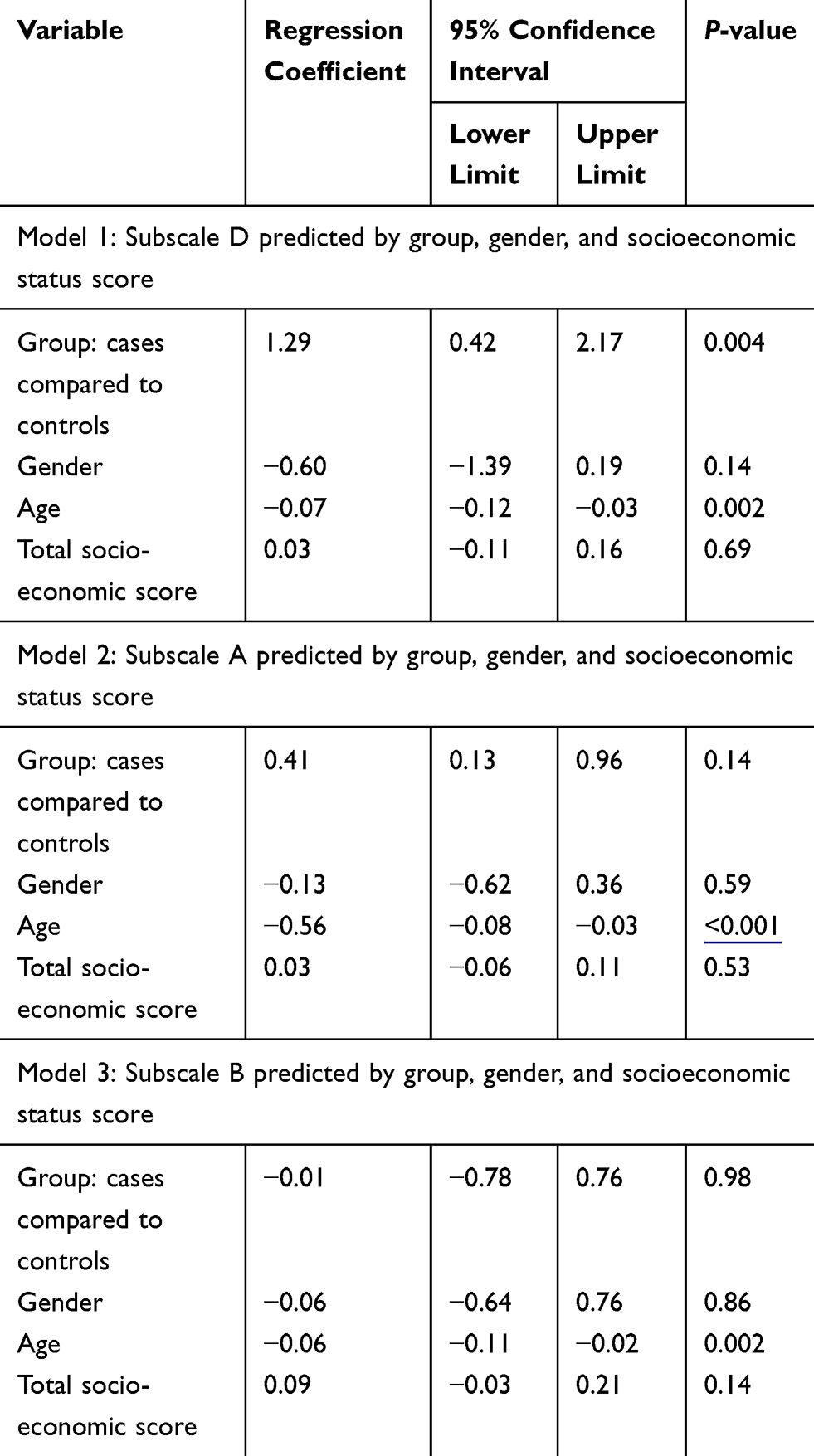 |
Table 3 Linear Regression Analysis of ADHD Screening Scores for the Three Subscales for Given Regressor Variables |
Discussion
In the present study, the researchers hypothesized that ADHD was more common in patients with head trauma following an accident compared to a group without trauma. The results showed that the overall frequency of adult ADHD was 5.9%, which was 6.1% in the trauma group and 5.9% in the non-trauma group. No such association was confirmed in the present study. In recent years, it has been repeatedly reported that ADHD in childhood, adolescence, and adulthood is associated with an increased risk of unintentional injuries and related accidents. A recent meta-analysis study concluded that the risk of injury in people with ADHD was higher than in people without it.18 Similarly, Amiri et al,5 in their review study, stated that ADHD patients are about twice as likely as non-ADHD people to have injuries and accidents. Dalsgaard et al,19 observed an increased mortality rate in ADHD patients, mainly due to accidents. In addition, there is evidence that ADHD patients are also at risk for multiple traumas and multiple accidents.20 Therefore, it can be assumed that the number of victims of accidents among ADHD people is higher than in the general population. In a similar study, Kittel-Schneider et al21 reported the prevalence of ADHD in adults to be 6.1% among trauma patients. Statistics from previous studies were lower than those, in the range of 3.4–4.7%. However, in studies conducted inside Iran, the percentages obtained were higher. In a 2011 study, Amiri et al22 found that the incidence of ADHD in trauma patients was 4.3%. Previous studies have reported different results on the frequency of ADHD among trauma patients compared to non-traumatic patients. The present study found that there was no statistically significant difference in the rate of adult ADHD among traumatic and non-traumatic patients. Similarly, Amiri et al22 reported that traumatic and non-traumatic patients accounted for an equal percentage of adult ADHD. Contrary to the above findings, Biederman et al23 reported that the patients with mild cerebral palsy had significantly higher levels of ADHD than the control group and, in all cases, the age at onset of ADHD was pre-existing to the trauma. Safiri et al24 also observed that the prevalence of ADHD was significantly higher among trauma patients. On the other hand, Shem-Tov et al25 stated that traumatic injuries were significantly higher in children with ADHD. Merrill et al26 also reported that the prevalence of accidental injuries in the ADHD group was 3.07-times higher than in non-traumatic individuals. The associated symptoms and compliance with the law and safety issues are related as both studies from Tabriz, unlike other studies in this regard, have not reported any difference between patients with and without head trauma in terms of ADHD.
Previous studies have identified a number of factors that contribute to the incidence of ADHD. One of these cases is a history of previous accidents that has been higher in most studies in ADHD patients.21,22 In the study in Tabriz, it was observed that high-risk behaviors were more prevalent among motorcyclists with ADHD, and these people were more careless than others in using helmets and having a driving license.27 Other studies have shown that high-risk behaviors, drunk driving, lack of certification,28 lack of helmet use on motorcyclists,24,27 and overconfidence21,29 were present among these individuals. Unfortunately, in the present study, we did not investigate the related causes and risk factors among the case and control groups.
With respect to our current knowledge of the association between ADHD and incidence of various injuries as well as specific findings in present study several issues should be considered:
- The association between the ADHD and head traumas could have a dual direction and the reverse causality should be addressed. Considering the very short time interval between the head trauma and ADHD symptom investigation in the current study, reverse causality is not considered a major concern in this regard.
- Although Conner’s screening scale has been shown to have high sensitivity and specificity, its results cannot fully replace the clinical diagnosis made by a psychiatrist, and this should be considered in interpretation of the results. However, recent studies have shown that even having higher rates of symptoms assessed through screening process may affect the risk of injuries irrespective of having a DSM-based clinical ADHD diagnosis.
- It is a general rule in case control studies that the recall bias and selection bias should always be considered in interpreting the results. The selection bias is considered as an important concern here, however, in the current study the use of hospital controls versus population controls helps to diminish the recall bias. Nevertheless, it should be considered that those with head trauma may to some extent under-report the symptoms of ADHD which if approved may affect the effect size. To diminish such an effect, the enrollment was restricted to those with a GCS≥13.
Conclusion
According to the results of the present study, the frequency of adult ADHD in trauma patients is not higher than non-traumatic patients. However, given the high percentage of undiagnosed adult ADHD in trauma patients, it seems that proper screening in this group and appropriate treatment can prevent further adverse events.
Acknowledgments
The authors are indebted to all subjects participating in this study.
Funding
This study was funded by Research Centre of Psychiatry and Behavioral Sciences of Tabriz University of medical science.
Disclosure
All authors confirm that they had no competing interest with respect to this manuscript.
References
1. Kennedy E, Cohen M, Munafò M. Childhood traumatic brain injury and the associations with risk behavior in adolescence and young adulthood: a systematic review. J Head Trauma Rehabil. 2017;32(6):425–432. doi:10.1097/HTR.0000000000000289
2. Thurman DJ. The epidemiology of traumatic brain injury in children and youths: a review of research since 1990. J Child Neurol. 2016;31(1):20–27. doi:10.1177/0883073814544363
3. Fann JR. Traumatic brain injury and psychiatry. J Psychosom Res. 1997;43:335–343. doi:10.1016/S0022-3999(97)00130-X
4. Fann JR, Leonetti A, Jaffe K, Katon WJ, Cummings P, Thompson RS. Psychiatric illness and subsequent traumatic brain injury: a case control study. J Neurol Neurosurg Psychiatry. 2002;72(5):615–620. doi:10.1136/jnnp.72.5.615
5. Amiri S, Sadeghi-Bazargani H, Nazari S, Ranjbar F, Abdi S. Attention deficit/hyperactivity disorder and risk of injuries: a systematic review and meta-analysis. J Inj Violence Res. 2017;(2):95.
6. Conversano E, Tassinari A, Monasta L, et al. Emergency department attendance for injury and behaviours suggestive of attention deficit hyperactivity disorder (ADHD): a cross-sectional study. BMC Pediatr. 2020;20(1):1–6. doi:10.1186/s12887-020-02166-x
7. Akbary A, Heydari ST, Sarikhani Y, et al. Association between adult attention-deficit/hyperactivity disorder and driving behaviors among Iranian motorcyclists. Bull Emerg Trauma. 2020;8(3):163.
8. Chang Z, Lichtenstein P, D’Onofrio BM, Sjolander A, Larsson H. Serious transport accidents in adults with attention-deficit/hyperactivity disorder and the effect of medication: a population-based study. JAMA Psychiatr. 2014;71(3):319–325. doi:10.1001/jamapsychiatry.2013.4174
9. Sadeghpour A, Sadeghi-Bazargani H, Ghaffari-Fam S, et al. Adult ADHD screening scores and hospitalization due to pedestrian injuries: a case-control study. BMC Psychiatry. 2020;20(1):1–2. doi:10.1186/s12888-020-02848-x
10. Maxson RT, Lawson KA, Pop R, Yuma-Guerrero P, Johnson KM. Screening for attention-deficit/hyperactivity disorder in a select sample of injured and uninjured pediatric patients. J Pediatr Surg. 2009;44(4):743–748. doi:10.1016/j.jpedsurg.2008.08.003
11. Sadeghi-Bazargani H, Mohammadi R, Amiri S, et al. Individual-level predictors of inpatient childhood burn injuries: a case–control study. BMC Public Health. 2016;16(1):209. doi:10.1186/s12889-016-2799-1
12. Max JE, Dunisch DL. Traumatic brain injury in a child psychiatry outpatient clinic: a controlled study. J Am Acad Child Adolesc Psychiatry. 1997;36:404–411. doi:10.1097/00004583-199703000-00020
13. Max JE, Lansing AE, Koele SL, et al. Attention deficit hyperactivity disorder in children and adolescents following traumatic brain injury. Dev Neuropsychol. 2004;25:159–177.
14. Bijur PE, Haslum M, Golding J. Cognitive and behavioral sequelae of mild head injury in children. Pediatrics. 1990;86:337–344.
15. Iverson GL, Atkins JE, Zafonte R, Berkner PD. Concussion history in adolescent athletes with attention-deficit hyperactivity disorder. J Neurotrauma. 2016;33(23):2077–2080. doi:10.1089/neu.2014.3424
16. Conners C, Erhardt D, &Sparrow E. The Conners Adult ADHD Rating Scale (CAARS). Toronto7 Multi-Health Systems Inc. 1998.
17. Sadeghi-Bazargani H, Amiri S, Hamraz S, Malek A, Abdi S, Shahrokhi H. Validity and reliability of the persian version of conner’s adult ADHD rating scales: observer and self-report screening versions. J Clin Res Govern. 2014;3:42–47.
18. Ruiz-Goikoetxea M, Cortese S, Aznarez-Sanado M, et al. Risk of unintentional injuries in children and adolescents with ADHD and the impact of ADHD medications: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2018;84:63–71.
19. Dalsgaard S, Østergaard SD, Leckman JF, Mortensen PB, Pedersen MG. Mortality in children, adolescents, and adults with attention deficit hyperactivity disorder: a nationwide cohort study. Lancet. 2015;385:2190–2196. doi:10.1016/S0140-6736(14)61684-6
20. Liou YJ, Wei HT, Chen MH, et al. Risk of traumatic brain injury among children, adolescents, and young adults with attention-deficit hyperactivity disorder in Taiwan. J Adolesc Health. 2018;63(2):233–238. doi:10.1016/j.jadohealth.2018.02.012
21. Kittel-Schneider S, Wolff S, Queiser K, et al. Prevalence of ADHD in accident victims: results of the PRADA study. J Clin Med. 2019;8(10):1643. doi:10.3390/jcm8101643
22. Amiri S, Ranjbar F, Sadeghi-Bazargani H, JodeiriEslami A, Navali AM, Saedi F. Association of adult attention deficit/hyperactivity disorder and traffic injuries in Tabriz - Iran. Iran J Psychiatry. 2011;6(2):61–65.
23. Biederman J, Feinberg L, Chan J, et al. Mild traumatic brain injury and attention-deficit hyperactivity disorder in young student athletes. J Nerv Ment Dis. 2015;203(11):813–819. doi:10.1097/NMD.0000000000000375
24. Safiri S, Sadeghi-Bazargani H, Amiri S, et al. Association between adult attention deficit-hyperactivity disorder and motorcycle traffic injuries in Kerman, Iran: a case-control study. J Clin Res Gov. 2013;2(1):17–21.
25. Shem-Tov S, Chodick G, Weitzman D, Koren G. The association between attention-deficit hyperactivity disorder, injuries, and methylphenidate. Glob Pediatr Health. 2019;6.
26. Merrill RM, Lyon JL, Baker RK, Gren LH. Attention deficit hyperactivity disorder and increased risk of injury. Adv Med Sci. 2009;54(1):20–26. doi:10.2478/v10039-009-0022-7
27. Sadeghi-Bazargani H, Abedi L, Mahini M, Amiri S, Khorasani-Zavareh D. Adult attention-deficit hyperactivity disorder, risky behaviors, and motorcycle injuries: a case-control study. Neuropsychiatr Dis Treat. 2015;11:2049–2054. doi:10.2147/NDT.S87614
28. Koisaari T, Michelsson K, Holopainen JM, et al. Traffic and criminal behavior of adults with attention deficit-hyperactivity with a prospective follow-up from birth to the age of 40 years. Traffic Inj Prev. 2015;16(8):824–830. doi:10.1080/15389588.2015.1029068
29. Wolff S, Queiser K, Wessendorf L, et al. Accident patterns in trauma surgery patients with and without self-reported ADHD. J Neural Transm (Vienna). 2019;126(9):1163–1173. doi:10.1007/s00702-019-02011-1
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.