Back to Journals » Journal of Blood Medicine » Volume 17
ATG Plus Post-Transplantation Cyclophosphamide Improves EBV-DNA Clearance and GVHD in Patients of Adult Chronic Active Epstein-Barr Virus Disease Undergoing Allogeneic HSCT
Authors Liu M ![]() , Yu Q, Cao Y, Ma Y, Hong Z, Yin Q, Feng Y, Li T, Zhang Y, Zheng M
, Yu Q, Cao Y, Ma Y, Hong Z, Yin Q, Feng Y, Li T, Zhang Y, Zheng M
Received 1 January 2026
Accepted for publication 7 May 2026
Published 3 June 2026 Volume 2026:17 593133
DOI https://doi.org/10.2147/JBM.S593133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Min Liu,1,2,* Qiuxia Yu,1,* Yang Cao,1 Yaxian Ma,1 Zetong Hong,1 Qing Yin,1 Yan Feng,1 Tongjuan Li,1 Yicheng Zhang,1 Miao Zheng1
1Department of Hematology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Hematology, Jingzhou Hospital, Affiliated to Yangtze University, Jingzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Miao Zheng, Department of Hematology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1095 Jiefang Avenue, Wuhan, 430022, People’s Republic of China, Tel +86 27 83665547, Email [email protected]
Background: Chronic active Epstein-Barr virus disease (CAEBVD) faces a challenging prognosis due to its inflammatory and tumorigenic nature and lack of standard treatment. The outcomes of adults are more disheartening. We aim to elucidate the efficacy of allogeneic hematopoietic stem cell transplantation (allo-HSCT) in adult CAEBVD, while clarifying whether the combination of antithymocyte globulin (ATG) and post-transplant cyclophosphamide (PTCy) can improve survival and reduce transplant-related complications.
Methods: We conducted a retrospective study analyzing adult CAEBVD patients who underwent allo-HSCT sequentially in the Department of Hematology at Tongji Hospital, Huazhong University of Science and Technology, from June 2015 to January 2022.
Results: Of 20 patients included. The median age at diagnosis was 30.5 years, and the median follow-up time post-transplantation was 26.9 months. The 5-year overall survival (OS), progression-free survival (PFS), GVHD-free and relapse-free survival (GRFS), and non-relapse mortality (NRM) rates were 54.5%, 39.4%, 44.4%, and 37.4%, respectively. These data were similar in ATG alone (50.0%, 33.3%, 33.3%, and 40.0%) and ATG+PTCy (56.3%, 41.7%, 49.0%, and 37.5%). On multivariable Cox regression, pre-transplant hemophagocytic syndrome (25.0% vs. 75.0%, P=0.029) and higher EBV copies (25% vs. 61.9%, P=0.048) reduced the OS. On multivariable logistic regression, ATG+PTCy showed a lower incidence of grade II–IV acute GVHD (14.3% vs. 66.7%, P=0.037) and chronic GVHD (14.3% vs. 66.7%, P=0.037). Additionally, faster EBV clearance (P=0.002) and lower EBV reactivation (P=0.018) were observed in ATG+PTCy.
Conclusion: Allo-HSCT can facilitate long-term survival in approximately half of adult CAEBVD. ATG+PTCy regimen did not improve survival but demonstrated advantages over ATG alone in reducing GVHD, eliminating EBV, and decreasing EBV reactivation.
Keywords: chronic active Epstein-Barr virus disease, hematopoietic stem cell transplantation, post-transplant cyclophosphamide, anti-thymocyte globulin, graft-versus-host disease
Introduction
Chronic active Epstein-Barr virus disease (CAEBVD) is a rare lymphoproliferative disorder caused by an EBV infection of T lymphocytes (T) or natural killer (NK) cells, and is predominantly observed in Asian populations.1–3 It is characterized by significantly increased EBV-DNA levels in the peripheral bloodstream, persistent fever, liver failure, enlarged lymph nodes, hepatosplenomegaly, and other infectious mononucleosis (IM)-like symptoms. CAEBVD can be potentially fatal because it exhibits both inflammatory and neoplastic characteristics. While some patients (13–17%) may achieve a transient self-limiting remission with minimal therapeutic measures (eg, corticosteroids, etoposide), others can progress to life-threatening complications, including hemophagocytic lymphohistiocytosis (HLH), disseminated intravascular coagulation (DIC), and multiple organ failure progressing into lymphoma, ultimately resulting in death.4–6 Prompt diagnostic and therapeutic interventions are essential. Currently, allo-HSCT remains the only method for EBV clearance and CAEBVD treatment.7 Children and adolescents with CAEBVD have a good prognosis, with most achieving long-term survival post-transplantation. Studies report 3-year overall survival (OS) rates of 60–87% in these populations.8,9 However, increasing evidence indicates that adult CAEBVD experience rising disease incidence and worse transplantation outcomes, with faster progression and more aggressive disease.10–14 In the transplant group, the 3-year OS of adults was 31%, which was much lower than that for children (100%) and adolescents (57%).13 In a study by Kimura et al focusing on the statistical analysis of CAEBVD transplantation data by age, 8-year overall survival rates were 59.7% for transplantations in patients with age < 15 years and only 4% for those in patients with age > 27 years.10 However, most existing literature is outdated, while allo-HSCT theory and technology have advanced significantly over the past decade. It is crucial to determine if these advancements have improved survival and transplantation outcomes for CAEBVD in adult hematology units. There is also limited research on how different graft versus host disease (GVHD) prophylaxis strategies, such as post-transplant cyclophosphamide (PTCy), anti-thymocyte globulin (ATG), or their combination, affect post-transplant complications and prognosis in adult CAEBVD. This study aims to examine survival rates of adult CAEBVD patients in the current transplantation network through a single-center retrospective analysis and compare the effects of ATG alone versus a combination of ATG and PTCy on post-transplant complications and prognosis.
Materials and Methods
Patients
Adult CAEBV patients who received allo-HSCT at Tongji Hospital’s Department of Hematology, Huazhong University of Science and Technology, between June 2015 and January 2022 were included in this retrospective analysis. Inclusion criteria (all conditions must be met): 1) Adults over 18 years old with a confirmed diagnosis of chronic active Epstein–Barr virus disease (CAEBVD); 2) Candidates willing to undergo transplantation and with a suitable donor available; 3) Eastern Cooperative Oncology Group (ECOG) performance status < 3; 4) Absence of severe organ dysfunction and ability to tolerate conditioning chemotherapy for transplantation. Diagnostic criteria for CAEBVD were derived from literature, WHO classification, and updated Japanese Health Ministry guidelines15,16 (all conditions must be met): 1) Persistent or recurrent infectious mononucleosis-like symptoms for more than three months; 2) Increased EBV-DNA load (≥102.5 copies/mL) in the peripheral blood and/or infected tissues; 3) EBV-infected T- or NK-cells in peripheral blood and/or infected tissues; and 4) A chronic condition that cannot be explained by other illnesses at diagnosis. IM-like symptoms included fever, enlarged lymph nodes, hepatosplenomegaly, and hematologic, digestive, pulmonary, skin, and other related disorders. Matched sibling or matched unrelated donors were prioritized, followed by haploidentical donors. The age of donors did not exceed 55 years.
Distinction of Cells Infected by EBV
Identify the cell types infected by EBV using flow cytometry. Cells were classified as B lymphocytes, T lymphocytes, and NK cells by measuring surface antigen expression on leukocytes, such as CD3, CD19, and CD56. A significantly higher EBV copy number in a specific cell subset compared with other cell types indicated that this cell type was predominantly infected with EBV.
Pre-Transplantation Treatment
Patients with CAEBVD received pre-transplant therapy to lower EBV-DNA levels and alleviate IM-like symptoms before allo-HSCT. The regimen included steroids (dexamethasone or methylprednisone), etoposide, ruxolitinib, and cyclosporine, either alone or in combination. Some underwent multiple chemotherapy courses, such as CHOP±E or P-GemOx. Patients with hemophagocytic syndrome (HPS) received HLH1994, HLH2004, or DEP regimens. Those with persistent IM-like or phagocytic symptoms after treatment but before transplantation were classified as activated.
HSCT Procedures and GVHD Prophylaxis
Patients in the ATG group were given busulfan at 3.2 mg/kg from day −10 to −7, cyclophosphamide at 1.8 g/m2 on days −6 to −5, and rabbit ATG at 2 mg/kg on days −4 to −1. Patients in the ATG+PTCy group received rabbit ATG 2 mg/kg on days −10 to −8, fludarabine 30 mg/m2 on days −7 to −3, and busulfan 3.2 mg/kg on days −5 to −2. Cyclophosphamide at 50 mg/kg was administered from days +3 to +4. From day −1, cyclosporine or tacrolimus was given with methotrexate and mycophenolate mofetil (MMF). MMF started at 0.5 mg twice daily from day +7, tapered from day +30, and stopped by day +60, with adjustments for clinical conditions. Four doses of methotrexate were given: 15 mg/m2 on day +1 and 10 mg/m2 on days +3, +6, and +11. Both groups followed the same post-transplant immunosuppressant tapering strategy.
Post-Transplant Evaluation
Post-transplant evaluation metrics included hematopoietic engraftment, acute and chronic GVHD, chimerism, EBV-DNA changes, cytomegalovirus and EBV reactivation, overall survival (OS), progression-free survival (PFS), GVHD-free and relapse-free survival (GRFS), and non-relapse mortality (NRM). Neutrophil recovery was marked by an absolute neutrophil count > 500/mL for three consecutive days, and platelet recovery was a count > 20×109/L for seven consecutive days without transfusions.17,18 OS was defined as the time span from transplantation to either death or the last follow-up, PFS was the interval from transplantation to disease progression, relapse, or death, and GRFS was characterized by the absence of death, relapse, severe acute GVHD, or systemic therapy for chronic GVHD.
Monitoring of EBV Copy Number Post-Transplantation
Post-transplant monitoring of EBV copy number was conducted weekly during the first 3 months and every two weeks for the subsequent 3–6 months. A viral load exceeding 1000 copies was considered a sign of reactivation. No prophylactic measures were taken.
Ethical Considerations
Ethical approval for the study (Number TJ-IRB202402025) was obtained from the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, and the research followed the principles outlined in the Helsinki Declaration and Good Clinical Practice Guidelines. Informed consent was duly obtained from all patients.
Statistical Analysis
GraphPad Prism 9 and SPSS 26.0 were used for statistical analyses. Categorical variables were analyzed using Fisher’s exact test, while continuous variables were examined with the Wilcoxon rank-sum test. Survival was evaluated using Kaplan-Meier Curves, and the Log rank test was used for comparisons. Analyses were conducted using Cox regression for survival and logistic regression for GVHD, incorporating both univariate and multivariate approaches. X-Tile software determined a survival-related cut-off value. All tests were two-sided with significance set at P<0.05.
Results
Patients
As shown in Table 1, A total of 20 patients were included in this study. The median age was 30.5 years (range, 18–56). Most patients exhibited IM-like symptoms such as fever (85%), hepatosplenomegaly (70%), and hepatic impairment (70%). The median time from disease onset to diagnosis was 4.2 months (range, 3.13–30.0). Before transplantation, 55% underwent chemotherapy, and 65% developed phagocytic syndrome with a median onset of 4.3 months (range, 3.13–28.6). The median interval from diagnosis to transplantation was 4.02 months (range, 0.83–30.3). 14 (75%) had active disease, including 8 with HLH. 35% had an HCT-CI score above 3, and 55% received haploidentical grafts. Peripheral blood stem cells were used as the graft source in 70% of patients. 6 (33.3%) received ATG as a GVHD prophylaxis strategy, and 14 (66.7%) received ATG+PTCy.
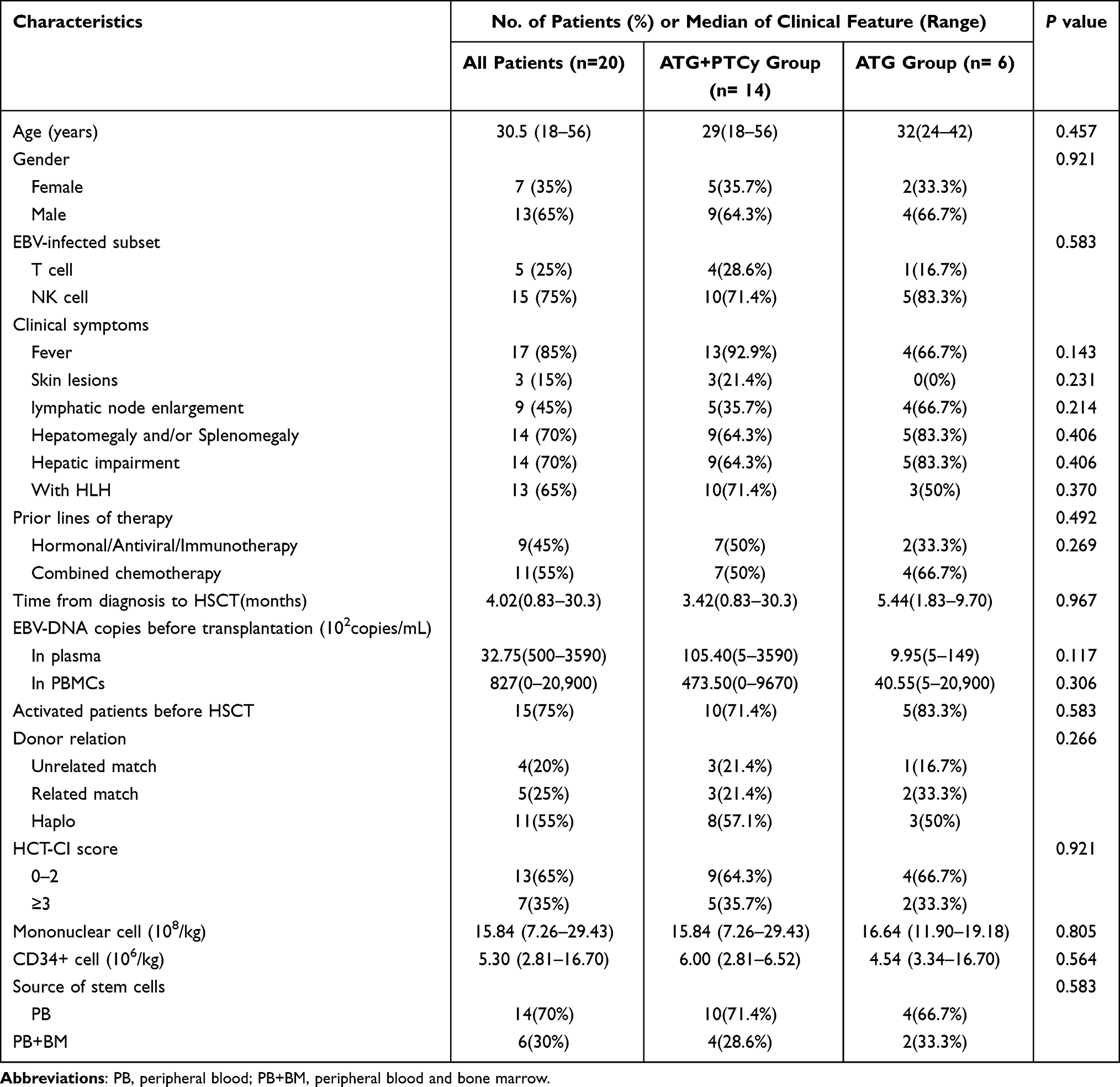 |
Table 1 Characteristics of Patients |
The Influence of the ATG + PTCy Combination on the Development of GVHD
Neutrophil engraftment rate by day 30 was 90.0% (95% CI, 76.9–100) and platelet engraftment rate by day 100 was 85.0% (95% CI, 69.4–100) for all patients. The ATG and ATG+PTCy groups had similar 30-day neutrophil (83.3% vs 92.9%, P=0.998) and 100-day platelet (83.3% vs 81.0%, P=0.798) engraftment rates (Figure 1). Additionally, there was no significant difference in the median time to neutrophil engraftment (14 vs. 14, P=0.526) and platelet engraftment (15 vs. 14, P=0.894) between the ATG and ATG+PTCy groups.
 |
Figure 1 Engraftment of patients in two groups. (a) Neutrophils. (b) Platelets. |
Within 100 days, the overall occurrence of grade II–IV aGVHD was 34.4% (95% CI, 17.0–61.5), while grade III–IV aGVHD was 22.3% (95% CI, 8.9–49.4). The cumulative incidence of cGVHD at one year was 40.0% (95% CI, 20.4–68.2), with extensive cGVHD being 20.0% (95% CI, 7.0–50.0). The ATG+PTCy group showed a lower occurrence in grade II–IV aGVHD (17.5% vs. 75.0%, P=0.004) and cGVHD (14.3% vs. 66.7%, P=0.037), but no significant benefit was noted for grade III–IV aGVHD (9.1% vs. 16.7%, P=0.515) or extensive cGVHD (9.1% vs. 50.0%, P=0.080).
We chose age, sex, infected cell type, donor type, graft origin, HLH occurrence, HCT-CI score, and transplantation regimen for univariate analysis. Significant factors for multivariate analysis included HLH occurrence, HCT-CI score, and transplantation regimen. The analysis showed that ATG+PTCy independently reduced the incidence of GVHD (OR 0.08, 95% CI, 0.01–0.80, P=0.031) (Table 2).
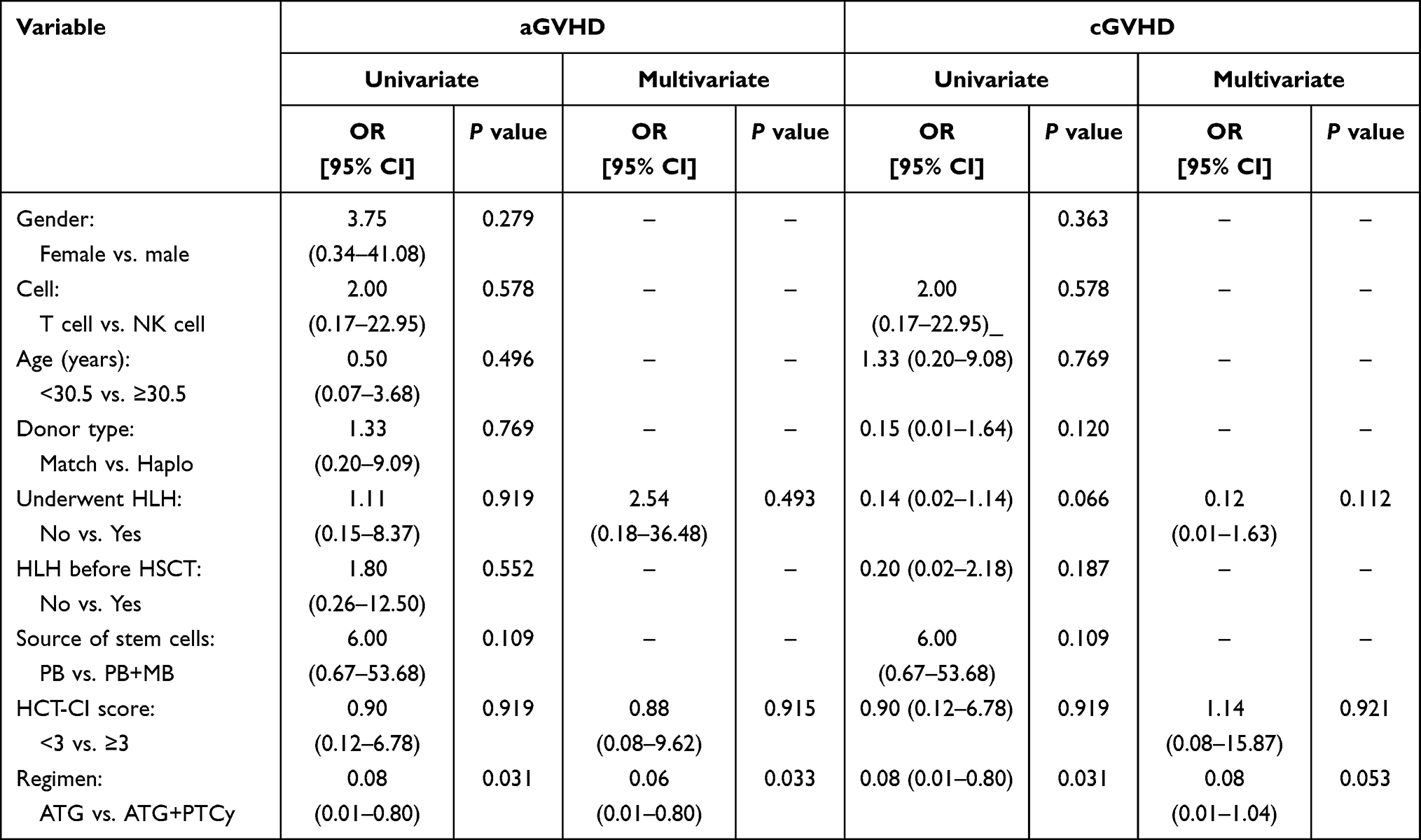 |
Table 2 Univariate and Multivariate Analyses of the Occurrence of GVHD in All Patients |
The Impact of Pre-Transplant Hemophagocytic Syndrome and Elevated EBV Copy Numbers on Overall Survival
The median follow-up after transplantation was 26.9 months (range: 0.3–95.0 months). The OS, PFS, and GRFS at 5 years in overall patients were 54.5% (95% CI, 30.7–73.2), 39.4% (95% CI, 18.6–59.7) and 44.4% (95% CI, 22.5–64.4), respectively (Figure 2a). In the ATG group, the OS, PFS, and GRFS at 5 years were 50.0%, 33.3%, and 33.3%, respectively, which were lower than 56.3% (P=0.738), 41.7% (P=0.593), and 49.0% (P=0.232) in the ATG+PTCy group, with no statistically significant differences (Figure 2c–e). The 5-year non-recurrent mortality NRM was 37.4% (95% CI, 19.8–63.2) overall (Figure 2b), 40.0% in the ATG group, and 37.5% in the ATG+PTCy group (P=0.990) (Figure 2f). OS, PFS, and GRFS stabilized after 2 years, suggesting that patients who survived for 2 years after transplantation may be cured.
 |
Figure 2 Survival figures based on overall patients and GVHD prophylaxis type. The overall patient survival and NRM (a and b), the comparison of OS, PFS, GRFS, and NRM between the ATG and ATG+PTCy groups (c–f), the worse OS of patients who were in HLH before transplantation (g), the OS of patients with pretransplant EBV copies over 25000/mL is worse (h). |
All patients were reclassified based on HLH status prior to transplantation. Patients with pre-transplant HLH exhibited a significantly worse 5-year OS (25.0% vs. 75.0%, HR 4.01, 95% CI, 1.00–16.06, P=0.029) (Figure 2g) but no significant difference in 5-year PFS (25% vs. 50%, P=0.470). To evaluate the impact of pre-transplant EBV copies on survival, plasma EBV copies, which reflect disease status more accurately compared to PBMCs, were analyzed.19 All patients were regrouped using 25,000 copies/mL as the cut-off value. Patients with pre-transplant plasma EBV copies above the cut-off value had a worse 5-year OS and PFS (25% vs. 61.9%, P=0.048; 0% vs. 50%, P=0.008) (Figure 2h). Subgroup analyses based on age, sex, and infected cell type showed no significant impact on survival, as results showed no significant differences (Table 3).
 |
Table 3 Unifactorial and Multifactorial Analyses of Survival |
ATG+PTCy Was More Effective in Clearing EBV-DNA
Seven days before transplantation, the median plasma EBV-DNA copies were 995 (range, 500–14900) and 10540 (range, 500–359000) in the ATG and ATG+PTCy groups, respectively (P=0.117). Median EBV-DNA copies in PBMCs in both groups were 405500 (range, 500–2090000) and 47350 (range, 0–967,000), respectively (P=0.306). At 28 days post-transplantation, median plasma EBV DNA copies were 1084.5 (range, 500–7500) and 0 (range, 0–1010) (P=0. 002) in the ATG and ATG+PTCy groups, respectively, while median EBV DNA copies in PBMCs were 15775 (range, 815–64600) and 0 (range, 0–23,000) (P=0.002), respectively. The rate of EBV clearance was significantly higher in the ATG+PTCy group than in the ATG group (Figure 3).
 |
Figure 3 EBV-DNA copy changes pre- and post-transplantation in the ATG and ATG+PTCy groups. 7 days before transplantation (a) 28 days post-transplantation (b). |
The Impact of the ATG + PTCy Combination on the Incidence of Infections
The 100-day cumulative EBV reactivation rate was 83.3% (5/6) in the ATG group, which was significantly higher than 21.4% (3/14) in the ATG+PTCy group (P=0.018). The 100-day cumulative reactivation rate of CMV was 16.7% (1/6) in the ATG group and 35.7% (5/14) in the ATG+PTCy group (P=0.613). In terms of early bacterial and fungal infections, the rates were 50.0% (3/6) and 16.7% (1/6) in the ATG group and 28.6% (4/14, P=0.613) and 7.1% (1/14, P=0.521) in the ATG+PTCy group, respectively. Although the ATG+PTCy group showed a trend of higher CMV reactivation rate but lower bacterial and fungal infection rates than the ATG group, the differences were not statistically significant (Table 4).
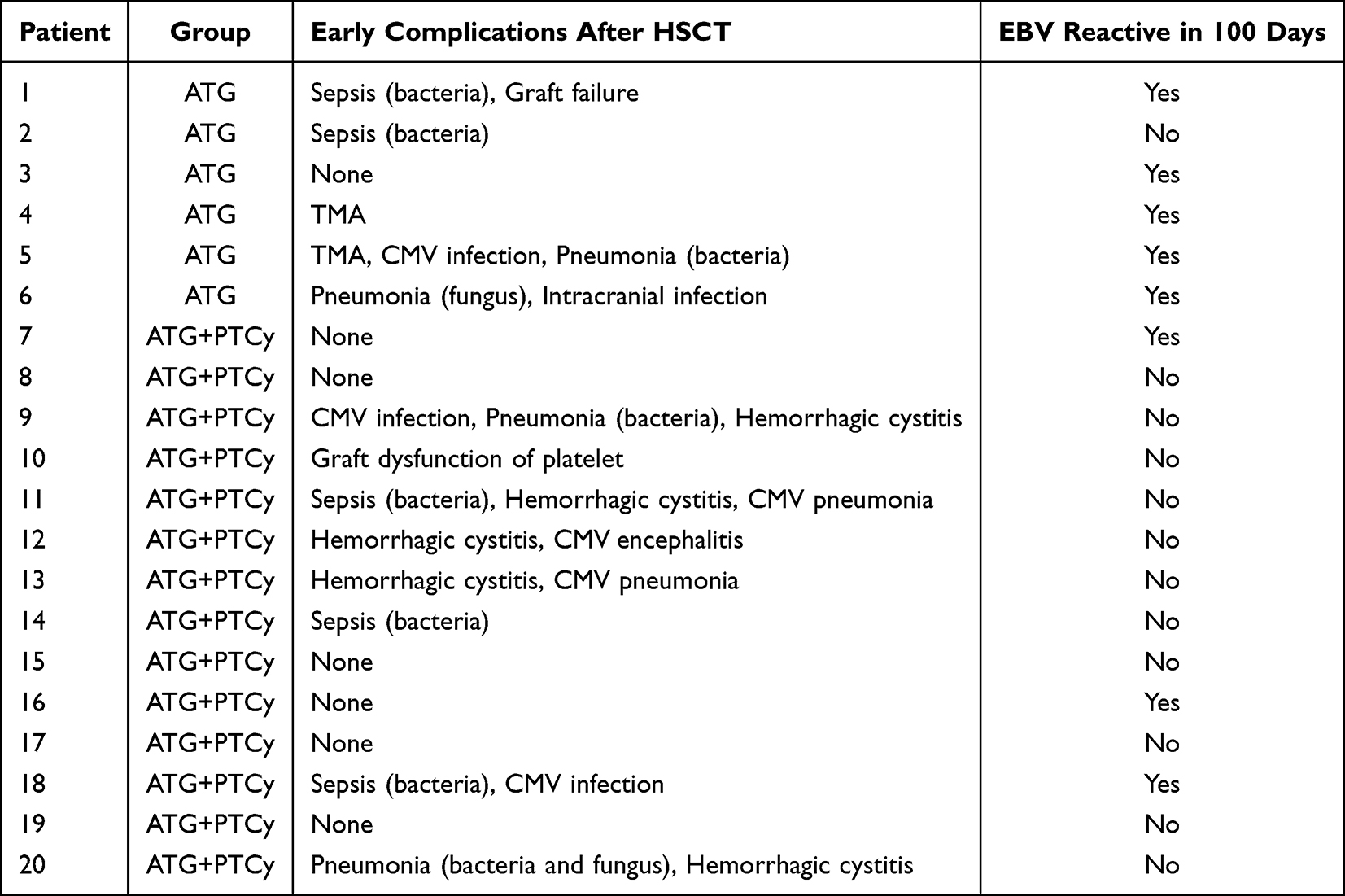 |
Table 4 The Early Complications of 20 Patients After Transplantation |
Discussion
This study examined the outcomes of CAEBVD patients admitted to an adult hematology unit and treated with hematopoietic stem cell transplantation. The incidence of acute and chronic GVHD, viral activation, early complications, and survival was compared between the two transplantation regimens. The ATG+PTCy regimen demonstrated significant advantages in controlling GVHD incidence, EBV clearance rate, and EBV reactivation post-transplantation. Despite the lack of significant differences in OS, PFS, and NRM between the two groups, the survival curve suggested a trend favoring the ATG+PTCy group, with a higher 5-year survival rate and lower non-relapse mortality rate compared to the ATG group. Additionally, our regrouping of transplanted patients revealed that patients with pre-transplant hemophagocytic syndrome and those with pre-transplant EBV-DNA copies exceeding 25,000 copies/mL had worse overall OS. These findings suggest the importance of avoiding phagocytic syndrome pre-transplantation and securing the eradication of plasma EBV-DNA copies for improved survival post-transplantation. Despite slightly higher pre-transplant median plasma EBV-DNA copies in the PTCy group compared to the ATG group, there was no significant difference in overall survival between the two groups post-transplant, suggesting that PTCy could partially mitigate the adverse effects on survival associated with high plasma EBV-DNA copies.
Chronic active Epstein-Barr virus disease (CAEBVD) is a rare T/NK-cell lymphoproliferative disorder that primarily affects individuals in Asia and Latin America, presenting significant treatment challenges. Lacking a specific, definitive therapy, CAEBVD has a poor overall prognosis. In a study by Kimura et al, 44% of 108 patients ultimately died from severe organ dysfunction caused by the disease.10 Japanese researchers have proposed a “three-step strategy” for treating CAEBVD, comprising immunosuppression, combination chemotherapy, and hematopoietic reconstitution. However, the success rates after the first two steps are only 13% to 17%,20,21 requiring allogeneic hematopoietic stem cell transplantation (allo-HSCT) for most patients to achieve long-term survival and better outcomes. Additionally, CAEBVD presents with both inflammatory and neoplastic features. Once T or NK cells are infected with Epstein- Barr virus (EBV), standard treatments such as antiviral drugs, chemotherapy, or immunotherapy often fail to completely eliminate the infected cells. This suggests that allo-HSCT might be the only curative option for CAEBVD. Recent advances, including single-cell sequencing, have shown that EBV can infect hematopoietic stem cells and lymphoid progenitors, thereby driving the development and progression of CAEBVD. This underscores the critical role of allo-HSCT in treatment. In a study by Yonese et al involving 100 CAEBVD patients, mostly children and adolescents, those who underwent HSCT achieved a 3-year overall survival (OS) rate of up to 82%, compared to 65% for patients who received chemotherapy followed by transplantation, and 0% for those treated with chemotherapy alone.13 Another study by Masahide Yamamoto et al, which included 102 CAEBVD patients with a median age of 21 years (more than 30% under 18), reported a 3-year OS of 72. 5%.22 Although transplantation significantly improves the prognosis for CAEBVD patients, the high rates of GVHD and non-relapse mortality remain major concerns.13,21,22
In the current landscape of GVHD prophylaxis strategies for allogeneic transplantation, two major systems stand out: the ATG-based “Beijing Protocol” and the PTCy-based “Baltimore Protocol”. ATG is an immunosuppressive drug used widely in allogeneic hematopoietic stem cell transplantation. It reduces the risk of grade II–IV aGVHD by 32% and the risk of overall cGVHD by 47%.23 However, its use is associated with an increased EBV activation rate, which is positively correlated with the dosage and is a significant risk factor for post-transplant lymphoproliferative disease (PTLD).24–27 For diseases closely related to EBV infection, such as CAEBVD, it is crucial to explore strategies to reduce post-transplant EBV reactivation and disease recurrence. As a novel prophylactic strategy for GVHD, PTCy can induce immune tolerance, eliminate donor and host-derived alloreactive T cell clones early after transplantation, and relatively retain Treg cells.28–30 Studies have shown that PTCy is effective in preventing both GVHD and PTLD.31–33 Masaya Maegaki et al reported a successful case of a 60-year-old CAEBVD patient who underwent haploidentical transplantation with PTCy prevention.34 However, PTCy carries a higher risk of engraftment failure, which can be mitigated by the use of ATG.35,36 In a prospective study involving 239 transplant patients, the ATG+PTCy group demonstrated significantly lower cumulative incidence rates of grade III–IV aGVHD and NRM within 100 days compared to the ATG group. Moreover, the ATG+PTCy group showed a significant improvement in GRFS (63% vs. 48%; P=0.039).37 Combining PTCy with a reduced ATG dose could theoretically reduce EBV reactivation. This combined strategy has been tested on numerous other diseases, including acute leukemia and myelodysplastic syndrome.38 The EBV activation rate after transplantation is around 15–21%.37,39,40 However, there is no existing literature specifically addressing CAEBVD. Our study was the first to compare the ATG regimen with the ATG+PTCy regimen in CAEBVD and confirmed that the ATG+PTCy transplantation regimen provides greater benefit to adult CAEBVD patients, particularly in reducing the occurrence of GVHD and the reactivation of EBV.
Our study combined the classical ATG transplantation system, which has been used for almost ten years, with the PTCy regimen. We found that under this combined system, the 5-year overall survival rate for adults with CAEBVD post-transplantation reached 54.5%, while the GRFS reached 49%. These outcomes are better than those reported in historical literature.
Our study also showed that the EBV clearance rate was faster in the ATG + PTCy system, and the occurrence of bacterial and fungal infections was lower compared to the ATG group. However, the cytomegalovirus (CMV) reactivation rate seemed to be higher in the ATG + PTCy system. This finding is consistent with observations in other studies. Wang Yu et al compared the ATG and ATG+PTCy cohorts in acute leukemia and found that the cumulative CMV activation rate at 100 days in the ATG+PTCy group was 70%, which was significantly higher than that in the ATG group.37 Similarly, Yang et al reported a CMV reactivation rate of 37.5% in the ATG+PTCy group in haploidentical peripheral blood HSCT.41 CMV reactivation under the ATG+PTCy system is a concern, possibly because of delayed T cell reconstitution in the combined system.
In this study, allo-HSCT facilitated long-term survival in approximately half of adult CAEBVD patients, although pre-transplant hemophagocytic syndrome and high EBV copy numbers diminished this effect. Furthermore, the ATG+PTCy regimen offered significant advantages over ATG alone in reducing GVHD, eliminating EBV, and decreasing EBV reactivation, but did not improve survival.
Although this study provides valuable insights, it has some limitations. First, it is a retrospective investigation, which inevitably involves selection bias and confounding factors. Second, due to the rarity of CAEBVD and the exclusion of pediatric and adolescent cases, the sample size is limited. Third, although both groups received myeloablative conditioning regimens, the specific drugs used differed, which could be a confounding factor. This is a preliminary study aimed at offering insights for future research. Future studies should involve a larger sample size and an appropriately adjusted ATG dose.
Data Sharing Statement
The data supporting this study’s findings are available on request from the corresponding author.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
This work was supported by the National Natural Science Foundation of China (Grant number 81974005), the Beijing Xisike Clinical Oncology Research Foundation (Grant number Y-SYBLD2022MS-0055), the Chen Xiao-ping Foundation for the Development of Science and Technology of Hubei Province (Grant number CXPJJH12000009-204), and the Open Fund of Key Laboratory of Biotherapy, Ministry of Education (Grant number 2024SWBS007).
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Cohen JI, Kimura H, Nakamura S, Ko YH, Jaffe ES. Epstein–Barr virus-associated lymphoproliferative disease in non-immunocompromised hosts: a status report and summary of an international meeting, 8–9 September 2008. Ann Oncol. 2009;20(9):1472–12. doi:10.1093/annonc/mdp064
2. Kimura H. EBV in T-/NK-Cell Tumorigenesis. In: Kawaguchi Y, Mori Y, Kimura H, editors. Human Herpesviruses. Vol. 1045. Advances in Experimental Medicine and Biology. Springer Singapore; 2018: 459–475. doi: 10.1007/978-981-10-7230-7_21
3. Campo E, Jaffe ES, Cook JR, et al. The international consensus classification of mature lymphoid neoplasms: a report from the clinical advisory committee. Blood. 2022;140(11):1229–1253. doi:10.1182/blood.2022015851
4. Arai A. Advances in the study of chronic active Epstein-Barr virus infection: clinical features under the 2016 WHO classification and mechanisms of development. Front Pediatr. 2019;7:14. doi:10.3389/fped.2019.00014
5. Kim HJ, Ko YH, Kim JE, et al. Epstein-barr Virus–Associated lymphoproliferative disorders: review and update on 2016 WHO classification. J Pathol Transl Med. 2017;51(4):352–358. doi:10.4132/jptm.2017.03.15
6. Fujiwara S, Nakamura H. Chronic active Epstein–Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers. 2020;12(11):3202. doi:10.3390/cancers12113202
7. Wang J, Su M, Wei N, et al. Chronic active Epstein-Barr virus disease originates from infected hematopoietic stem cells. Blood. 2024;143(1):32–41. doi:10.1182/blood.2023021074
8. Sawada A, Inoue M, Kawa K. How we treat chronic active Epstein-Barr virus infection. Int J Hematol. 2017;105(4):406–418. doi:10.1007/s12185-017-2192-6
9. Cohen JI, Jaffe ES, Dale JK, et al. Characterization and treatment of chronic active Epstein-Barr virus disease: a 28-year experience in the United States. Blood. 2011;117(22):5835–5849. doi:10.1182/blood-2010-11-316745
10. Kimura H, Ito Y, Kawabe S, et al. EBV-associated T/NK–cell lymphoproliferative diseases in nonimmunocompromised hosts: prospective analysis of 108 cases. Blood. 2012;119(3):673–686. doi:10.1182/blood-2011-10-381921
11. Arai A, Imadome KI, Watanabe Y, et al. Clinical features of adult-onset chronic active Epstein–Barr virus infection: a retrospective analysis. Int J Hematol. 2011;93(5):602–609. doi:10.1007/s12185-011-0831-x
12. Kawamoto K, Miyoshi H, Suzuki T, et al. A distinct subtype of Epstein-Barr virus-positive T/NK-cell lymphoproliferative disorder: adult patients with chronic active Epstein-Barr virus infection-like features. Haematologica. 2018;103(6):1018–1028. doi:10.3324/haematol.2017.174177
13. Yonese I, Sakashita C, Imadome KI, et al. Nationwide survey of systemic chronic active EBV infection in Japan in accordance with the new WHO classification. Blood Adv. 2020;4(13):2918–2926. doi:10.1182/bloodadvances.2020001451
14. Lin J, Wu H, Gu L, et al. Clinicopathologic findings of chronic active Epstein–Barr virus infection in adults: a single-center retrospective study in China. Clin Exp Med. 2021;21(3):369–377. doi:10.1007/s10238-021-00689-w
15. Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the world health organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375–2390. doi:10.1182/blood-2016-01-643569
16. Kawada J-I, Ito Y, Ohshima K, et al. Updated guidelines for chronic active Epstein–Barr virus disease. Int J Hematol. 2023;118(5):568–576. doi:10.1007/s12185-023-03660-5
17. Rowlings PA, Przepiorka D, Klein JP, et al. IBMTR severity index for grading acute Graft-Versus-Host disease: retrospective comparison with glucksberg grade. Br J Haematol. 1997;97(4):855–864. doi:10.1046/j.1365-2141.1997.1112925.x
18. Lee SJ, Wolff D, Kitko C, et al. Measuring Therapeutic response in chronic graft-versus-host disease. national institutes of health consensus development project on criteria for clinical trials in chronic Graft-Versus-Host disease: IV. The 2014 response criteria working group report. Biol Blood Marrow Transplant. 2015;21(6):984–999. doi:10.1016/j.bbmt.2015.02.025
19. Zheng M, Bao Y, Wang J, et al. The superiority of Epstein-Barr virus DNA in plasma over in peripheral blood mononuclear cells for monitoring EBV-positive NK-cell lymphoproliferative diseases. Hematological Oncol. 2022;40(3):381–389. doi:10.1002/hon.2998
20. Sawada A, Inoue M. Hematopoietic stem cell transplantation for the treatment of Epstein-Barr Virus-Associated T- or NK-Cell lymphoproliferative diseases and associated disorders. Front Pediatr. 2018;6:334. doi:10.3389/fped.2018.00334
21. Kawa K, Sawada A, Sato M, et al. Excellent outcome of allogeneic hematopoietic SCT with reduced-intensity conditioning for the treatment of chronic active EBV infection. Bone Marrow Transplant. 2011;46(1):77–83. doi:10.1038/bmt.2010.122
22. Yamamoto M, Sato M, Onishi Y, et al. Registry data analysis of hematopoietic stem cell transplantation on systemic chronic active Epstein–Barr virus infection patients in Japan. American J Hematol. 2022;97(6):780–790. doi:10.1002/ajh.26544
23. Chakupurakal G, Freudenberger P, Skoetz N, Ahr H, Theurich S; Cochrane Haematology Group, ed. Polyclonal anti-thymocyte globulins for the prophylaxis of graft-versus-host disease after allogeneic stem cell or bone marrow transplantation in adults. Cochrane Database Syst Rev. 2023;2023(6). doi:10.1002/14651858.CD009159.pub3
24. Enok Bonong PR, Zahreddine M, Buteau C, et al. Factors associated with post-transplant active Epstein-Barr virus infection and lymphoproliferative disease in hematopoietic stem cell transplant recipients: a systematic review and Meta-Analysis. Vaccines. 2021;9(3):288. doi:10.3390/vaccines9030288
25. Walker I, Panzarella T, Couban S, et al. Pretreatment with anti-thymocyte globulin versus no anti-thymocyte globulin in patients with haematological malignancies undergoing haemopoietic cell transplantation from unrelated donors: a randomised, controlled, open-label, Phase 3, multicentre trial. Lancet Oncol. 2016;17(2):164–173. doi:10.1016/S1470-2045(15)00462-3
26. Wei N, Wang Y, Wang J, Wu L, Wang Z. Characteristics of Epstein–Barr virus reactivation after allogeneic haematopoietic stem cell transplantation in patients with chronic active Epstein–Barr virus disease: favorable responses to rituximab. Bone Marrow Transplant. 2021;56(6):1449–1451. doi:10.1038/s41409-020-01193-7
27. Podgorny PJ, Ugarte-Torres A, Liu Y, Williamson TS, Russell JA, Storek J. High Rabbit-Antihuman thymocyte globulin levels are associated with low likelihood of Graft-vs-Host disease and high likelihood of posttransplant lymphoproliferative disorder. Biol Blood Marrow Transplant. 2010;16(7):915–926. doi:10.1016/j.bbmt.2010.02.027
28. Mussetti A, Greco R, Peccatori J, Corradini P. Post-transplant cyclophosphamide, a promising anti-graft versus host disease prophylaxis: where do we stand? Exp Rev Hematol. 2017;10(5):479–492. doi:10.1080/17474086.2017.1318054
29. Cieri N, Peccatori J, Oliveira G, et al. Tracking T cell dynamics in the first month after Haplo-HSCT with post-transplant cyclophosphamide reveals a predominant contribution of memory stem T cells to the early phase of immune reconstitution. Blood. 2013;122(21):4615. doi:10.1182/blood.V122.21.4615.4615
30. Ganguly S, Ross DB, Panoskaltsis-Mortari A, et al. Donor CD4+ Foxp3+ regulatory T cells are necessary for posttransplantation cyclophosphamide-mediated protection against GVHD in mice. Blood. 2014;124(13):2131–2141. doi:10.1182/blood-2013-10-525873
31. Solomon SR, Sizemore CA, Sanacore M, et al. Haploidentical transplantation using T cell replete peripheral blood stem cells and myeloablative conditioning in patients with High-Risk hematologic malignancies who lack conventional donors is well tolerated and produces excellent relapse-free survival: results of a prospective Phase II trial. Biol Blood Marrow Transplant. 2012;18(12):1859–1866. doi:10.1016/j.bbmt.2012.06.019
32. Munchel A, Kesserwan C, Symons H, et al. Nonmyeloablative, HLA-Haploidentical bone marrow transplantation with high dose, Post-Transplantation cyclophosphamide. Pediatr Rep. 2011;3(12):e15. doi:10.4081/pr.2011.s2.e15
33. Kanakry JA, Kasamon YL, Bolaños-Meade J, et al. Absence of post-transplantation lymphoproliferative disorder after allogeneic blood or marrow transplantation using post-transplantation cyclophosphamide as Graft-Versus-Host disease prophylaxis. Biol Blood Marrow Transplant. 2013;19(10):1514–1517. doi:10.1016/j.bbmt.2013.07.013
34. Maegaki M, Kawamura K, Hara K, et al. Successful HLA-haploidentical stem cell transplantation with post-transplant cyclophosphamide in an older patient with chronic active Epstein–Barr virus infection. Int J Hematol. 2022;116(4):630–634. doi:10.1007/s12185-022-03345-5
35. Bolaños-Meade J, Fuchs EJ, Luznik L, et al. HLA-haploidentical bone marrow transplantation with posttransplant cyclophosphamide expands the donor pool for patients with sickle cell disease. Blood. 2012;120(22):4285–4291. doi:10.1182/blood-2012-07-438408
36. Colson YL, Li H, Boggs SS, Patrene KD, Johnson PC, Ildstad ST. Durable mixed allogeneic chimerism and tolerance by a nonlethal radiation-based cytoreductive approach. J Immunol. 1996;157(7):2820–2829. doi:10.4049/jimmunol.157.7.2820
37. Wang Y, Wu DP, Liu QF, et al. Low-dose post-transplant cyclophosphamide and anti-thymocyte globulin as an effective strategy for GVHD prevention in haploidentical patients. J Hematol Oncol. 2019;12(1):88. doi:10.1186/s13045-019-0781-y
38. Li Y, Wang N, Zhang X, et al. Post-transplantation cyclophosphamide as GVHD prophylaxis in allogenic hematopoietic stem cell transplantation: recent advances and modification. Blood Rev. 2023;62:101078. doi:10.1016/j.blre.2023.101078
39. Lu J, Zhuang Y, Hong X, et al. Combining low-dose post-transplant cyclophosphamide(PTCY) with anti-thymocyte globulin (ATG) for prophylaxis of graft-versus-host disease in alternative-donor hematopoietic stem cell transplantation for β-thalassemia major. Blood. 2023;142(Supplement 1):3568. doi:10.1182/blood-2023-186196
40. Zu Y, Li Z, Gui R, et al. Low-dose post-transplant cyclophosphamide with low-dose antithymocyte globulin for prevention of graft-versus-host disease in first complete remission undergoing 10/10 HLA-matched unrelated donor peripheral blood stem cell transplants: a multicentre, randomized controlled trial. Bone Marrow Transplant. 2022;57(10):1573–1580. doi:10.1038/s41409-022-01754-y
41. Yang J, Jiang J, Cai Y, et al. Low-dose anti-thymocyte globulin plus low-dose posttransplant cyclophosphamide as graft-versus-host disease prophylaxis in haploidentical peripheral blood stem cell transplantation combined with unrelated cord blood for patients with hematologic malignancies: a prospective, phase II study. Bone Marrow Transplant. 2019;54(7):1049–1057. doi:10.1038/s41409-018-0382-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.