Back to Journals » International Medical Case Reports Journal » Volume 19
Asymptomatic Bilateral Giant Choroidal Osteoma Involving the Macula in a Child
Received 22 August 2025
Accepted for publication 19 May 2026
Published 24 June 2026 Volume 2026:19 557180
DOI https://doi.org/10.2147/IMCRJ.S557180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Linna Hao, Chaoyi Qu, Yanchun Zhang
Department of Ophthalmology, Xi’an People’s Hospital (Xi’an Fourth Hospital), Xi’an, 710016, People’s Republic of China
Correspondence: Linna Hao, Email [email protected]
Abstract: Choroidal osteoma is a rare benign tumor with an incidence of approximately 1 per 100,000 people, predominantly affecting young women aged 20– 30 years and mostly occurring unilaterally (72%-75%), but it is rare in children. We reported a case of asymptomatic bilateral giant choroidal osteoma involving the macula in a child. We have completed the relevant examinations for the patient. Choroidal osteoma can also occur in children, and when the lesion is in the early stage, even if it is located in the macular area, the children may be asymptomatic.
Keywords: choroidal osteoma, binocular, children, asymptomatic
Introduction
Choroidal osteoma is a rare benign ossifying tumor of the choroid, first described by Gass et al in 1978.1 Most cases are located at the posterior pole near the optic disc and often involve the macula. Early-stage choroidal osteomas exhibit an orange-red color, while the later stage shows a yellowish tinge due to RPE depigmentation. The majority of cases are unilateral and typically occur in women in their second to third decades of life but are rare in children. Patients usually present with symptoms such as blurred vision, metamorphopsia, photophobia, or visual field defects; however, some remain asymptomatic.2,3 We reported a case of asymptomatic bilateral giant choroidal osteoma involving the macula in a child, which enriches the clinical spectrum of this disease.
Case Report
In January 2023, an 11-year-old Chinese girl was referred to the Department of Ophthalmology at Xi’an People’s Hospital (Xi’an Fourth Hospital) with no history of systemic or ocular disease. Her best corrected visual acuity (BCVA) was 20/20 in both eyes. The anterior segment examination was unremarkable. Fundus examination revealed an orange, depigmented, granular subretinal macular lesion with well-defined geographic boundaries, measuring approximately 7 disc areas in the right eye and 6 disc areas in the left eye (Figure 1).
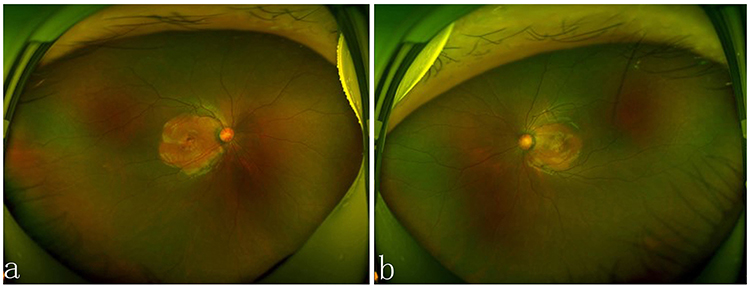 |
Figure 1 Fundus photograph showing a typical Orange-yellowish lesion in the right eye (a) and left eye (b). |
Spectral-domain optical coherence tomography (SD-OCT) showed irregular and uneven IS/OS layers in the macula of both eyes. Enhanced depth imaging SD-OCT (EDI-OCT) demonstrated a bony plate structure consistent with choroidal osteoma within the choroidal layer (Figure 2). Fundus autofluorescence (FAF) revealed mild spontaneous fluorescence corresponding to the lesions in both eyes (Figure 3).
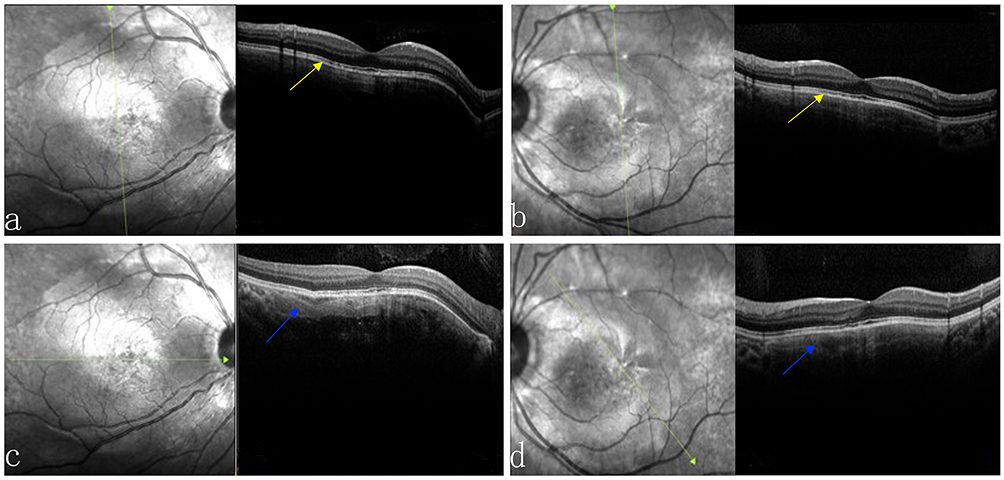 |
Figure 2 The green arrow indicates the OCT scan line.OCT (a and b) scan showing irregular and uneven IS/OS layers (yellow arrow) in the macula of both eyes. SD-OCT (EDI-OCT) (c and d) scan showing a bony plate structure (blue arrow) consistent with choroidal osteoma within the choroidal layer. |
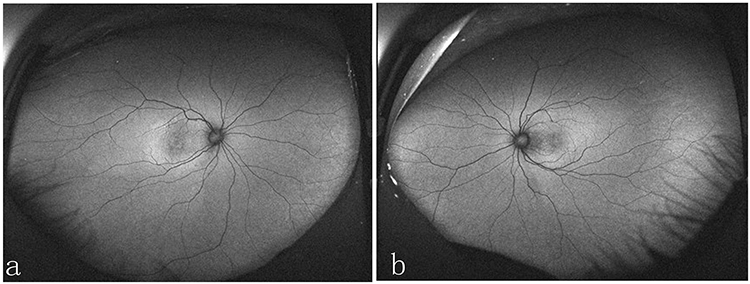 |
Figure 3 Autofluorescence showing mild spontaneous fluorescence corresponding to the lesions in the right eye (a) and left eye (b). |
Early-phase fluorescein angiography (FFA) showed weak fluorescence in the macular area bilaterally, with mottled transparent fluorescence observed in the mid and late phases. Indocyanine green angiography (ICGA) showed larger areas of persistent choroidal hypofluorescence (Figure 4). B-scan ultrasonography revealed highly reflective choroidal lesions in both eyes (3.52 mm diameter and 0.9 mm thickness in the right eye; 3.0 mm diameter and 0.9 mm thickness in the left eye) with an acoustic shadow consistent with tumor calcification (Figure 5). Computed tomography (CT) scans identified two arcuate high-density shadows approximately 5 mm in length on the posterior wall near the optic nerve head of both eyes (Figure 6).
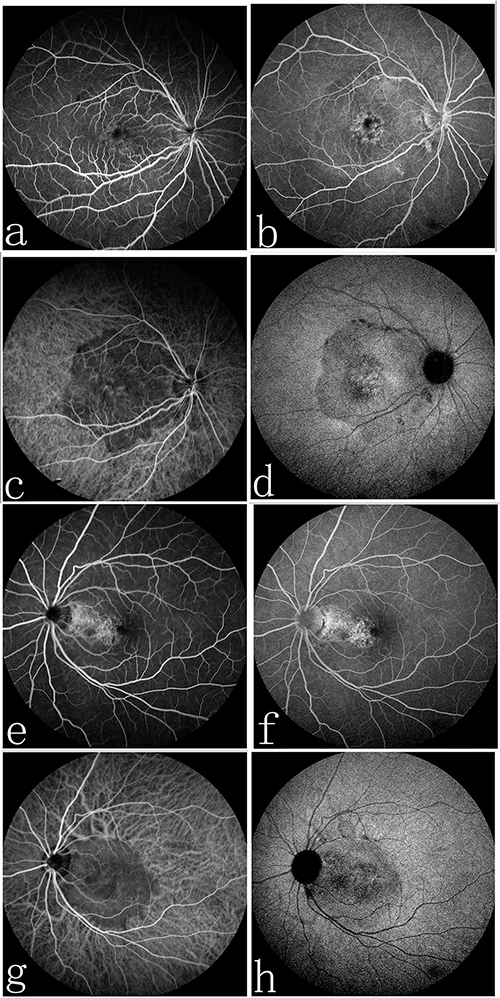 |
Figure 4 FFA showing weak fluorescence in the early phase (a) and mottled transparent fluorescence in the late phases (b) in the right eye; ICGA showing larger areas of persistent choroidal hypofluorescence (c and d) in the right eye. FFA showing mottled transparent fluorescence in the mid and late phases (e and f) in the left eye; ICGA showing larger areas of persistent choroidal hypofluorescence (g and h) in the left eye. |
 |
Figure 5 B-scan ultrasound showing hyperechogenic choroidal plaques (yellow arrow) with acoustic shadowing in the right eye (a) and left eye (b). |
 |
Figure 6 CT showing two arcuate high-density shadows (yellow arrow) approximately 6 mm in length on the posterior wall near the optic nerve head of both eyes. |
Due to various practical constraints, the patient was unable to return for an in-person follow-up evaluation. Nevertheless, we conducted a telephone follow-up assessment for two years and confirmed that the patient’s visual acuity remained stable without deterioration. The patient’s guardians have been thoroughly instructed to seek immediate medical consultation should any changes in visual acuity be observed.
Discussion
Choroidal osteoma (CO) is a rare condition, and existing studies3,4 have shown that it mostly occurs unilaterally in women aged 20–30 years. In contrast, this case involves an 11-year-old child with bilateral giant CO involving the macula—pediatric CO is extremely rare, and bilateral giant lesions in the macular area are even rarer. This unusual presentation enriches the clinical spectrum of CO and reminds clinicians to pay attention to the possibility of CO in pediatric patients, avoiding missed diagnosis due to its low incidence in children. The initial diagnosis is missed in up to 90% of cases;4 however, diagnosis becomes apparent with ultrasound and CT.
Due to calcified components, CO exhibits high acoustic reflectivity and shadowing on ultrasound, with high-intensity echo peaks on A-scan imaging. On B-scan, the osteoma appears as a slightly elevated choroidal mass showing calcifications at the lesion site. Ultrasound also helps differentiate CO from amelanotic choroidal melanoma and choroidal hemangioma. On CT, a hyperdense choroidal plaque with bone-equivalent density typically corresponds to the tumor.
Shields et al5 used time-domain OCT (model 3000 Stratus) to propose that the white fundus lesion areas in CO represent decalcified regions, while orange areas represent calcified regions. They also found that calcified CO lesions preserve the inner, outer, and photoreceptor retinal layers, whereas decalcified lesions have intact inner retina but significant thinning of the outer retina, with most patients losing the photoreceptor layer. In our case, the large choroidal osteoma involved the superior, inferior temporal, and infratemporal vascular arcs, reaching the optic disc nasally. Despite this, the patient’s visual acuity remained good, likely due to the lesion’s calcified stage and preserved outer retinal structure.
OCT alone cannot definitively diagnose osteoma. EDI-OCT can reveal characteristic features of CO: transient dense horizontal reflective lines (junction lines) representing bone lamellae, mottled (spongy, reticular) tissue, and horizontally or vertically oriented tubular channels corresponding to Haversian, Wacner, or cavernous vascular spaces. In our case, EDI-OCT clearly showed the horizontal reflective lamellae indicative of bone plates.
Studies have shown that CO can increase in size in 51% of cases, undergo decalcification in 46%, cause a loss of three or more lines of visual acuity in 45%, and result in visual acuity of 20/200 or worse in 56% of cases.3 Our patient had good vision at initial presentation; however, visual acuity may be at risk in the future due to decalcification. At the two-year telephone follow-up, no visual impairment was noted, but regular follow-up was recommended.
No standard treatment exists for uncomplicated osteomas; therapies target complications from choroidal neovascularization (CNV), which is common in CO. Overall, CNV occurs in 31–47% of cases.6,7 Treatment options include transpupillary thermotherapy (TTT), photodynamic therapy (PDT), and intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections.
The differential diagnosis of choroidal osteoma mainly includes choroidal hemangioma and choroidal hamartoma. Choroidal osteoma typically presents as a well-circumscribed, calcified, hyperechoic lesion on B-scan ultrasonography, with high reflectivity consistent with osseous tissue. Choroidal hemangioma is a vascular lesion characterized by homogeneous, moderate hyper-reflectivity without calcification, and shows characteristic early hyperfluorescence on fluorescein angiography. Choroidal hamartoma usually demonstrates variable internal reflectivity and lacks the typical calcified features of osteoma; it is often associated with systemic syndromes and shows no acoustic characteristics of bone. In the present case, the marked calcification and intense hyperechoic pattern on B-mode ultrasound strongly support the diagnosis of choroidal osteoma and effectively exclude choroidal hemangioma and choroidal hamartoma.
In our case, we recommended regular follow-up with funduscopy, SD-OCT, and EDI-SD-OCT. Fluorescein angiography or OCT angiography will be performed if CNV is suspected.
Systemic evaluation and further examinations of the patient’s parents and siblings were not performed in the present study. The diagnosis was established mainly on the basis of clinical characteristics and B-scan ultrasound findings, which revealed typical calcified and hyperechoic features consistent with choroidal osteoma.
Ethics and Consent Statements
This study is a retrospective single case report. According to the institutional ethical guidelines, formal institutional review board approval was not required for publishing de-identified clinical case details. Written informed consent was obtained from the patient’s guardians for the publication of this case. No identifiable personal information has been included in this report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gass JD, Guerry RK, Jack RL, Harris G. Choroidal Osteoma. Arch Ophthalmol. 1978;96(3):428–6. doi:10.1001/archopht.1978.03910050204002
2. Williams AT. Osseous choristoma of the choroid simulating a choroidal melanoma. Association with a positive 32P test. Arch Ophthalmol. 1978;96(10):1874–1877. doi:10.1001/archopht.1978.03910060378017
3. Shields CL. Factors predictive of tumor growth, tumor decalcification, choroidal neovascularization, and visual outcome in 74 eyes with choroidal osteoma. Arch Ophthalmol. 2005;123(12):1658–1666. doi:10.1001/archopht.123.12.1658
4. Browning DJ. Choroidal osteoma: observations from a community setting. Ophthalmology. 2003;110(7):1327–1334. doi:10.1016/S0161-6420(03)00458-5
5. Shields CL, Perez B, Materin MA, Mehta S, Shields JA. Optical coherence tomography of choroidal osteoma in 22 cases: evidence for photoreceptor atrophy over the decalcified portion of the tumor. Ophthalmology. 2007;114(12):e53–e58. doi:10.1016/j.ophtha.2007.07.037
6. Xu H, Zeng F, Shi D, Sun X, Chen X, Bai Y. Focal choroidal excavation complicated by choroidal neovascularization. Ophthalmology. 2014;121(1):246–250. doi:10.1016/j.ophtha.2013.08.014
7. Alameddine RM, Mansour AM, Kahtani E. Review of choroidal osteomas. Middle East Afr J Ophthalmol. 2014;21(3):244–250. doi:10.4103/0974-9233.134686
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.