Back to Journals » Clinical Ophthalmology » Volume 14
Asymmetric Thickness Intracorneal Ring Segments for Keratoconus
Authors Baptista PM ![]() , Marques JH
, Marques JH ![]() , Neves MM
, Neves MM ![]() , Gomes M
, Gomes M ![]() , Oliveira L
, Oliveira L ![]()
Received 22 September 2020
Accepted for publication 12 November 2020
Published 16 December 2020 Volume 2020:14 Pages 4415—4421
DOI https://doi.org/10.2147/OPTH.S283387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pedro Manuel Baptista,1,2 João Heitor Marques,1 Miguel Mesquita Neves,1 Miguel Gomes,1,2 Luís Oliveira1
1Ophthalmology Department, Centro Hospitalar Universitário Do Porto, Porto, Portugal; 2Instituto De Ciências Biomédicas Abel Salazar, Porto, Portugal
Correspondence: Pedro Manuel Baptista
Centro Hospitalar Universitário Do Porto, Largo Prof. Abel Salazar, Porto 4099-001, Portugal
Tel +0035-1917868372
Email [email protected]
Purpose: To describe the anatomical and functional results of the implantation of asymmetric thickness intracorneal ring segments (AS-ICRS) in eyes with keratoconus and asymmetric/irregular astigmatism (type 2 – Duck – and type 3 – Snowman – phenotypes, Fernandez-Vega/Alfonso morphologic Keratoconus classification).
Materials and Methods: Retrospective observational study including 19 consecutive patients (21 eyes) with keratoconus who underwent manual implantation of the Keraring® Asymmetric ICRS (AS). Analysis included demographic and clinical data and Pentacam (Oculus®) measurements: topographic astigmatism; topographic flat meridian (K1), steepest meridian (K2) and the maximum keratometric point (Kmax); total root mean square (RMS) and high order RMS (HOA) aberrations and comatic Zernike coefficients (Z31;Z3− 1) at 0º and 90º meridians.
Results: Overall mean age was 35.3± 11.7 years and median follow-up was 7.1 months (range 6– 12). At the end of follow-up, a significant improvement from baseline was achieved in both UDVA (0.24± 0.22; p=0.017) and CDVA (0.21± 0.17; p< 0.001). Regarding topographic measurements, the greatest decrease was observed in K2 (2.76± 1.9D; p< 0.001) and astigmatism (1.97± 1.5; p< 0.001). Aberrometry analysis showed a reduction of 1.27± 3.2μm in the total RMS (p=0.085), 0.24± 0.9μm in HOA (p=0.227) and 0.78± 0.5 (p< 0.001) in the 90º component of comatic aberration. The procedure effects in the CDVA, topographic and aberrometric parameters were higher in type 2 cones without statistical significance (p> 0.05 in all).
Conclusion: Implantation of the Keraring® Asymmetric ICRS in keratoconus with asymmetric/irregular astigmatism allowed an improvement of several clinical, topographic and aberrometric parameters, with clinical efficacy and safety, with a tendency to a greater effect in the type 2 cones.
Keywords: aberrometry, asymmetric, astigmatism, ICRS, keratoconus
Introduction
The implantation of intrastromal corneal ring segments (ICRS) in patients with keratoconus is a minimally invasive and reversible surgical procedure aimed to improve the uncorrected (UDVA) and best corrected (CDVA) distance visual acuities and reduce low and high order aberrations, with consequent improvement vision quality, acting by an “arc-shortening effect” on the corneal lamellae and flattening the central cornea.1 Additionally, the procedure may increase tolerance to contact lenses in some patients.2
Many keratoconus classifications have been made throughout the years.3–5 As the corneal morphologic study evolved, namely with the advent of tomography and aberrometry techniques, it was possible to make a better characterization of the corneal total shape and its refractive consequences. Regarding the implantation of ICRS, the SA-ANA classification6 is the most applied, dividing the implantation modalities using 2 basic criteria - symmetry and axiality - whose combination results in 4 major types.
There are several reports in literature showing good refractive and functional results after the implantation of ICRS.2,7,8 Nevertheless, a lack of parallelism between the objective tomographic and refractive results and visual complaints can be observed, and is more evident in cases with irregular and/or asymmetric of the topographic astigmatism and is usually due to a clinically significant comatic aberration component.9,10
The Fernandez-Vega/Alfonso morphologic Keratoconus classification11 divides the disease into six subtypes and takes into account the comatic issue. Types 2 and 3 are the most difficult to address with standard ICRS. Furthermore, besides all classifications, each keratoconus has a phenotypic identity, so the ring segments have evolved and recently a novel type of ICRS with asymmetric thickness became available, allowing to increase the customization in the treatment of eyes with asymmetric astigmatism, in which the flattest topographic axis diverges from the coma axis by more than 30º.
The aim of the present study was to evaluate the anatomical and functional results and the safety profile associated with the implantation of ICRS with asymmetric thickness in patients with keratoconus and compare the results between type 2 and type 3 phenotypes.
Materials and Methods
Design
This is a retrospective observational single-center clinical study set in the Ophthalmology Department, Centro Hospitalar e Universitário do Porto, Porto, Portugal, a tertiary center. The study adhered to the tenets of the Declaration of Helsinki. Approval was obtained from the “Departamento de Ensino, Formação e Investigação” (DEFI), nr: 130-DEFI-132-CE. Informed consent from the patients was waived by the DEFI due to total anonymization and confidentiality of the data and the absence of detailed individual data.
Population
Consecutive patients with keratoconus who underwent consecutive implantation of the Keraring® Asymmetric ICRS (AS) between January and August 2019. The indications for the procedure were: patient demand for improvement in visual acuity and/or rigid gas permeable contact lens intolerance; Grade 1–3 (Amsler-Krumeich, AK); stable disease; corneal thickness >400μm, Kmax <64D and asymmetric astigmatism in which the flattest topographic axis diverged from the coma axis by more than 30º (Duck and Snowman types). The exclusion criteria were: corneal opacity; history of herpes; glaucoma; cataract; uveitis; severe atopic disease or eye rubbing habit; auto-immune disorders.
Procedure
All ICRS were chosen according with the Mediphacos™ nomogram (http://keraring.online) and confirmed by the surgeon. As all corneas had mean front keratometry less than 52D, prismatic triangular section 160º arc length AS with 5.0mm optic zone were implanted in all eyes. The tunnel was made at 80% of total corneal thickness, manually in all cases. The minimum follow-up was 6 months.
The basic rules followed in the segment selection were different among the two subtypes (Figures 1 and 2). In cases of Type 2 paracentral keratoconus, in which both steep hemi-meridians were not aligned and presenting with a difference of 30º to 60º between the flat topographic and the coma axis, one AS was inserted with the thickest end oriented towards the steepest hemi-meridian and the middle of the ICRS centered on the flat topographic axis, with or without a second ring (symmetrical) at 180º. Eyes with Type 3 paracentral keratoconus, where both hemi-meridians were aligned but with the inferior hemi-meridian steeper than the superior one and the flat topographic and the coma axis were at 90º from each other, were implanted with one or two AS, inserted with the thickest end oriented toward the steepest hemi-meridian (one clockwise and one counter-clockwise). The midpoint of each ICRS was aligned on the flat topographical axis.
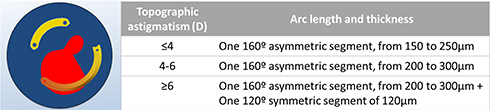 |
Figure 1 Segments selection according to MediphacosTM nomogram in Type 2 cones. |
 |
Figure 2 Segments selection according to MediphacosTM nomogram in Type 3 cones. |
Data Gathering
Demographic (age, gender), ocular and systemic history data were collected, along with information from intra and post-surgical complications during the entire follow-up. We collect the baseline and end of follow-up UDVA, CDVA (Snellen) and refractive status. Visual acuity data was converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis and presented in decimal notation for an intuitive analysis.
Data from Pentacam (Oculus®) were analyzed:
- Topographic keratometric values (central 8mm sphere) - flat meridian (K1); steepest meridian (K2), the maximum keratometric point (Kmax) and astigmatism;
- Total root mean square (RMS), high order RMS (HOA) aberrations and comatic aberration Zernike coefficients (Z31; Z3−1)– at 0º and 90º meridians (calculated for a pupil diameter of 6.0 mm).
Statistical Analysis
Statistical analysis was performed with the SPSS statistical software package, version 24.0 (SPSS, Chicago, IL®). Normality of the data was tested with the Shapiro–Wilk test. When parametric analysis could be applied, the Student’s t-test was used to compare the variables. When nonparametric tests were needed, the Wilcoxon rank-sum test was applied. Correlations were studied with Spearman rank correlation method. Values are show as mean ± standard deviation unless otherwise specified. All p-values (p) were 2-sided, and p- values < 0.05 were considered significant.
Results
Twenty-one eyes from 19 patients (11 men; 8 woman), with an overall mean age of 35.3±11.7 years and mean follow-up of 7.1 months (range 6–12) were analyzed. The most common keratoconus phenotype (Fernandez-Vega classification) was Type 3 with 14 eyes and the remaining 7 were classified into Type 2 category. Baseline measures are listed in Table 1.
 |
Table 1 Baseline, End of Follow-Up and Effect of the Procedure, All Sample |
Regarding systemic history, one patient had Hodgkin Lymphoma, with past chemotherapy treatment. In relation to ophthalmological history, one patient had exteriorization of a previous ICRS, one patient underwent corneal crosslinking procedure one and a half years before and one patient had history of diabetic macular edema (DME) treated with intravitreal anti-vascular endothelial growth factor. Regarding intraoperative complications, in one case, the ring segment broke during the implantation and was replaced in the same procedure. There were no other intra- or post-surgical complications to report until the end of follow-up.
At the end of follow-up, the UDVA and CDVA were 0.42±0.28 and 0.63±0.19, respectively. A significant improvement from baseline was achieved in both UDVA (0.24±0.22; p=0.017) and CDVA (0.21±0.17; p<0.001) (Table 1). Two eyes maintained the UDVA, another two eyes maintained the CDVA and a 1-line decrease in CDVA was observed in one eye. A significant decrease of 1.56±1.5D (p<0.001) in cylinder and 1.39±2.6D in SE were observed.
Regarding topographic measurements, the greater decrease observed in the K2 (2.76±1.9D; p<0.001), followed by the Kmax (2.46±2.6D; p<0.001) and the K1 (0.8±1.7D; p=0.047), with a significant decrease in the absolute topographic astigmatism value (1.97±1.5; p<0.001) (Table 1).
Additionally, stability of both flattest refractive (95.6±47º to 96.8±45º; p=0.804) and steepest topographic (83.1º to 86.6 º; p=0.565) axis was found after the procedure (Table 1).
Within the aberrometry analysis, reduction of 1.27±3.2µm in the total RMS (p=0.085) and 0.24±0.9µm in HOA (p= 0.227) were found. Additionally, significant absolute decrease (0.78±0.5; p<0.001) in the vertical (90º) component of comatic aberration was observed (Table 1).
Phenotypic Subgroup Analysis
The only baseline, significant difference between the two phenotypic groups was the higher topographic astigmatism in the type 2 (5.94±2.1D VS 3.81±1.3D p=0.012) (Table 1).
At the end of follow-up, UDVA was slightly higher in type 2 (0.53±0.3 VS 0.37±0.3; p=0.396) and CDVA was similar (0.62±0.2 VS 0.65±0.2; p=0.733). The procedure effect in the CDVA was slightly more pronounced in type 2 (0.27±0.2 VS 0.19±0.2; p=0.278) but there was a slightly higher SE decrease in type 3 group (1.52±3.0 VS1.16±1.3; p=0.804) (Table 2).
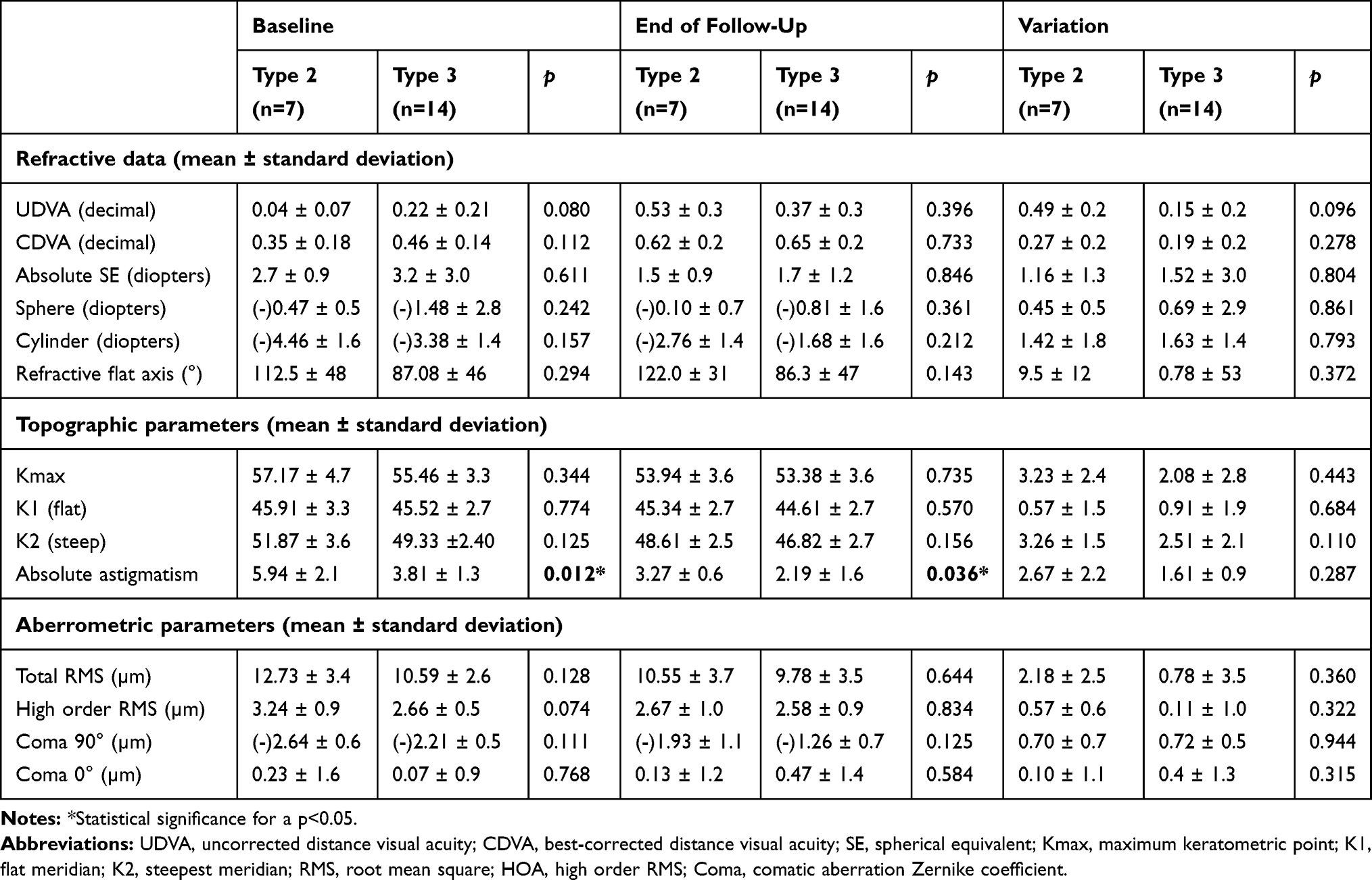 |
Table 2 Baseline, End of Follow-Up and Effect of Procedure, per Type of Cone |
Regarding the topographic parameters, the decrease found in both Kmax (3.23±2.4D VS 2.08±2.8D; p=0,443), K2 (3.26±1.5D VS 2.51±2.1D; p=0.110) and absolute astigmatism (2.67±2.2D VS 1.61±09D; p=0.287) was non-significantly higher in type 2 group (Table 2).
Within the aberrometry analysis, the variation in both total RMS (2.18±2.5µm VS 0.78±3.5 µm; p=0.360) and HOA (0.57±0.6µm VS 0.11±1.0µm; p=0.322) was non-significantly higher in type 2 group. The effect of the procedure in the vertical coma component was similar in the two groups (0.70±0.7µm VS 0.72±0.5µm; p=0.944) (Table 2).
Correlations
A higher postoperative CDVA was associated either with lower postoperative values of Kmax (r=−0.471; p=0.048), and total RMS (r=−0.509; p=0.031). A higher postoperative Kmax was associated with higher values of both baseline and postoperative of total RMS (r=0.673; p=0.001 and r=0.797; p<0.001, respectively) and HOA (r=0.544; p=0.011 and r=0.553; p=0.009, respectively). A higher postoperative K1 was associated with higher baseline values of either absolute coma 90º (r=0.502; p=0.020), total RMS (r=0.617; p=0.003) and HOA (r=0.571; p=0.007). A higher postoperative K2 was associated with higher preoperative values of either absolute coma 90º (r=0.499; p=0.021), total RMS (r=0.646; p=0.002) and HOA (r=0.572; p=0.007). A higher postoperative absolute coma 90º was associated with higher postoperative values of both K1 (r=0.562; p=0.008) and K2 (r=0.615; p=0.003).
Discussion
The present study found an average increment of more than two lines both in UDVA and CDVA, yet with similar amount of improvement achieved by sphero-cylindric means before and after the procedure. Predictably the lower values on the main topographic and aberrometric measurements (Kmax and RMS) were the most associated with higher visual acuities. These results are in line with those obtained in the 104 eyes cohort implanted with the same 5mm optic zone AS and following the same nomogram (Figures 1 and 2) in Type 2 and Type 3 phenotypes12 at 3 months follow up, with very similar final CDVA, even though with slightly higher increments both in UDVA and CDVA in our study (roughly 2.3 VS 1.5 Snellen lines in both). When compared with the symmetrical Ferrara® ICRS (6.0mm inner diameter and variable thickness - 150, 200, 250, and 300 µm - and arc lengths – 90º, 120º, 150º, and 210º) implanted in a large13 series of 409 paracentral cones (AK Grade 1 and 2) in which flattest topographic axis diverged from the coma axis less than 30º, similar increment in UDVA (roughly 2.4 VS 2.3 Snellen lines) but higher increment in CDVA (roughly 2.1 VS 0.8 Snellen lines) were found. Despite starting from lower baseline CDVAs, the present study further highlights the role of this AS in the enhancement of the residual sphero-cylindric correction by glasses or contact lenses, even in more difficult astigmatisms. Additionally, when compared with the recent 353° asymmetric ICRS Visumring®14 (quadrangular cross-section, inner diameter of 5.5mm, base width of 800µm and 2 asymmetric sections that can vary from 90º to 160º of arc lengths and customized thickness from 150 to 350µm) implanted in 30 asymmetric bowtie keratoconic eyes with or without skewed axes, and with preoperative higher refractive (spherical equivalent of −12.4D) and topographic values (SimK1 48.9D and SimK2 54.7D), higher increments in both UDVA (roughly 2.4 VS 1.4 Snellen lines) and CDVA (roughly 2.2 VS 1.9 Snellen lines) were found in the present study.
Regarding subjective refraction, the significant reduction of both the sphere and cylinder achieved was consistent with a significant flattening found in the keratometry readings. Several studies had shown significant improvement of the refraction and flattening of the cornea after the implantation of symmetrical ICRS.2,15,16 In the present study, the greatest reduction occurred in the Kmax and K2, which led to more than 2 diopters decrease on topographic astigmatism. Only one eye did not decrease but maintained the topographic astigmatism and the K2 values. Only one eye showed an increase in Kmax, yet with an improvement of one line in CDVA. These results have the same pattern but with slightly smaller decreases than the reported by Prisant et al.12 The Visumring® implantation14 showed a higher decrease in sphere and both K1 and K2, yet with an increase in topographic astigmatism and this can be explained as those were probably implantations of a large arc length ICRS in more myopic and central cones. Comparing with the large series from Vega et al13 of symmetrical ICRS implants in paracentral cones, this study found similar spherical equivalent decrease but higher decrease in keratometry readings.
Improvement in the Zernike coefficients after ICRS implantation have been reported in literature.16 The present study showed a clinically relevant decrease both in RMS and in HOA, but without significant statistical differences. While another study12 with AS did not perform aberrometric analysis, the Visumring®14 showed a higher decrease in total RMS but probably due to the effect on myopic spherical aberration, as the decrease in HOA was similar to the present study for a 6mm pupil. Two eyes showed a substantial increase both in the total RMS and the HOA, but without decrease in visual acuity (one maintained and another increase 1 Snellen line in CDVA). It is of notice that one of these eyes had concurrent history of DME.
Moreover, some reports, either with symmetrical17 or asymmetrical14 ICRS showed an improvement in the asymmetric aberrations as primary coma and coma-like aberrations which are known to be among the aberrations that negatively affect the visual function of the patients. The present study found a significant improvement in coma 90º aberration, which is known as the main clinically relevant high-order aberration found in keratoconic corneas. Predictably, the horizontal coma aberration slightly increased, as one cannot be altered without alteration of the other. We must notice a slightincrease in absolute coma 90º value in one eye, but without increase in both total RMS or HOA, yet with substantial improvement in UDVA (5 Snellen lines).
Finally, it is important to point out that all higher postoperative topographic values (Kmax, K1 and K2) were associated to higher baseline aberrometric parameters. Additionally, higher postoperative K1, K2 and coma 90º were positively associated. These associations highlight a potential role for the introduction of the aberrometric values in future nomograms for these AS.
Regarding the subgroup analysis, there was a tendency to a greater increment in both UDVA and CDVA in the type 2 phenotype but starting from lower initial values. The effects in both total RMS and HOA were slightly higher in the type 2 cases too. All this is in line with the reported by Prisant et al,12 although they have implanted only 1 segment in all Type 2 cases, and can be explained by the desirable cone re-centering effect made possible by the ICRS in these more decentered and aberrated cones. The same study12 found a greater effect both in subjective refractive and tomographic measurements in the Type 3 cases and explained that with the supposed greatest flattening effect of the 2 segments implanted in all of these more centered and myopic cones. The present study, despite a greater effect on spherical equivalent in the Type 3 group, showed a higher topographic flattening effect in the Type 2 group. On the other hand, a very similar effect in the coma 90º was observed in both groups.
As in the present study the majority of eyes were implanted with 1 ICRS, stratified statistical analysis by number of ICRS was not possible. Further studies are needed with stratifies analysis in order to strengthen the conclusions both by phenotypic type and number of implanted segments and even dividing eyes by disease severity perceiving at which stage of keratoconus the procedure can be the most efficient.
In relation to the complications, no rings have been explanted until the end of follow-up, similar to the reported by Prisant et al,12 and different than the 5 explants due to corneal melting reported with the larger Visumring®14 The ICRS broken during implantation was immediately replaced without associated consequences. Regarding manual tunnelization, no differences in the difficulty of ring insertion due to the progressive thickness throughout the ring body, were found. The same postoperative medications as in the symmetrical ICRS procedures were prescribed and there were no differences on patient complaints or ophthalmoscopy signs during the entire follow-up.
Limitations of the present study are the retrospective non-randomized design, the limited number of cases and the manual implantation technique. As the final ICRS result in corneal regularization may only be achieved at six months in some cases, the authors consider follow-up time a relative strength when compared with other work12 that studied the same type of ICRS as it had only three months follow-up and without possibility of stretching it, because crosslinking and topo-guided photorefractive keratectomy were performed thereafter in all patients.
To our knowledge, this is the second study to describe the clinical outcomes of this new ICRS design in asymmetric keratoconus cases. In fact, most of the time, patients with these type of cones continue to claim vision symptoms despite improvement in topographic and refractive parameters due, probably, to the comatic component that is not fully addressed with standard ICRS. The present study proves that, besides the improvements in the above parameters, total and high order aberrations can be diminished by the neutralization of vertical coma. However, a key question that remains unanswered is whether in similar eyes asymmetric thickness ICRSs enhance vision more than symmetric ICRSs. Although the present study results are in line with those reported for this type of ICRS, showing that specific keratoconus phenotypes can be ideal candidates for these AS, other comparative studies are needed to fully assess the difference between various models of ICRSs and validate this hypothesis.
Conclusion
In the present study, the implantation of the Keraring® Asymmetric ICRS in specific keratoconus phenotypes characterized by irregularity and/or asymmetry of the topographic astigmatism, in which it is difficult to increment quality of vision with the standard ICRS, allowed an improvement of several clinical, topographic and aberrometric parameters, with clinical efficacy and safety and with a tendency to a greater effect in the Duck type cones. As the phenotypic characterization is evolving, more studies are needed to optimize the nomograms in order to make the best of the customization possibilities associated to this type of ICRS.
Acknowledgments
The authors want to acknowledge all the support granted by the head of the Ophthalmology Department of Centro Hospitalar e Universitário do Porto, Prof. Dr. Pedro Menéres.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burris TE, Holmes-Higgin DK, Silvestrini TA, Scholl JA, Proudfoot RA, Baker PC. Corneal asphericity in eye bank eyes implanted with the intrastromal corneal ring. J Refractive Surg. 1997;13(6):556–567.
2. Vega-Estrada A, Alio JL. The use of intracorneal ring segments in keratoconus. Eye Vision. 2016;3(1):8. doi:10.1186/s40662-016-0040-z
3. Amsler M. [The “forme fruste” of keratoconus]. Wien Klin Wochenschr. 1961;73:842–843.
4. Rabinowitz YS, Rasheed K. KISA% index: a quantitative videokeratography algorithm embodying minimal topographic criteria for diagnosing keratoconus. J Cataract Refract Surg. 1999;25(10):1327–1335. doi:10.1016/S0886-3350(99)00195-9
5. Belin MW, Duncan JK. Keratoconus: the ABCD Grading System. Klin Monbl Augenheilkd. 2016;233(6):701–707. doi:10.1055/s-0042-100626
6. Barraquer R, Alfonso J, Murta J. Keratoconus patterns and intrastromal segments. J surg. 2012;90:s249.
7. Park SE, Tseng M, Lee JK. Effectiveness of intracorneal ring segments for keratoconus. Curr Opin Ophthalmol. 2019;30(4):220–228. doi:10.1097/ICU.0000000000000582
8. Benoist d’Azy C, Pereira B, Chiambaretta F, Dutheil F. Efficacy of different procedures of intra-corneal ring segment implantation in keratoconus: a systematic review and meta-analysis. Transl Vis Sci Technol. 2019;8(3):38. doi:10.1167/tvst.8.3.38
9. Tan B, Baker K, Chen Y-L, et al. How keratoconus influences optical performance of the eye. J Vis. 2008;8(2):13. doi:10.1167/8.2.13
10. Choi D, Appukuttan B, Binek SJ, et al. Prediction of cis-regulatory elements controlling genes differentially expressed by retinal and choroidal vascular endothelial cells. J Ocul Biol Dis Infor. 2008;1(1):37–45. doi:10.1007/s12177-008-9007-1
11. Alfonso JF, Lisa C, Fernández-Vega Cueto L, Poo A, Madrid D. Clasificación del queratocono basada en fenotipos clínicos. In: Del Buey Sayas MA, Peris Martínez C, editors. Influencia del astigmatismo congénito en la morfología del queratocono. Biomecánica y arquitectura corneal. Elsevier: Vol Monografias SECOIR. España, Barcelona; 2014:165–184.
12. Prisant O, Pottier E, Guedj T, Hoang Xuan T. Clinical outcomes of an asymmetric model of intrastromal corneal ring segments for the correction of keratoconus. Cornea. 2020;39(2):155–160. doi:10.1097/ICO.0000000000002160
13. Fernández-Vega Cueto L, Lisa C, Poo-López A, Madrid-Costa D, Merayo-Lloves J, Alfonso JF. Intrastromal corneal ring segment implantation in 409 paracentral keratoconic eyes. Cornea. 2016;35(11):1421–1426. doi:10.1097/ICO.0000000000000978
14. Vega-Estrada A, Chorro E, Sewelam A, Alio JL. Clinical outcomes of a new asymmetric intracorneal ring segment for the treatment of keratoconus. Cornea. 2019;38(10):1228–1232. doi:10.1097/ICO.0000000000002062
15. Sakellaris D, Balidis M, Gorou O, et al. Intracorneal ring segment implantation in the management of keratoconus: an evidence-based approach. Ophthalmol Therapy. 2019;8(Suppl S1):5–14. doi:10.1007/s40123-019-00211-2
16. Piñero DP, Alio JL. Intracorneal ring segments in ectatic corneal disease - a review. Clin Experiment Ophthalmol. 2010;38(2):154–167. doi:10.1111/j.1442-9071.2010.02197.x
17. Shabayek MH, Alió JL. Intrastromal corneal ring segment implantation by femtosecond laser for keratoconus correction. Ophthalmology. 2007;114(9):1643–1652. doi:10.1016/j.ophtha.2006.11.033
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.