Back to Journals » Journal of Asthma and Allergy » Volume 19
Asthma with Preserved Ratio Impaired Spirometry: A Distinct Phenotype Associated with Increased Exacerbation Burden
Authors Arimoto Y, Honda N, Haruki K, To Y ![]() , To M
, To M
Received 27 April 2026
Accepted for publication 1 July 2026
Published 17 July 2026 Volume 2026:19 618426
DOI https://doi.org/10.2147/JAA.S618426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Yoshihito Arimoto,1 Natsue Honda,1 Kosuke Haruki,1 Yasuo To,2,3 Masako To1,2
1Department of Laboratory Medicine, Dokkyo Medical University, Saitama Medical Center, Koshigaya, Saitama, Japan; 2Department of Allergy and Respiratory Medicine, The Fraternity Memorial Hospital, Sumida, Tokyo, Japan; 3Department of Pulmonary Medicine, International University of Health and Welfare Narita Hospital, Narita, Chiba, Japan
Correspondence: Masako To, Department of Laboratory Medicine, Dokkyo Medical University, Saitama Medical Center, 2-1-50 Minami-Koshigaya, Koshigaya, Saitama, 343-8555, Japan, Email [email protected]
Purpose: Asthma is a heterogeneous disease, and identifying phenotypes associated with an increased exacerbation burden is clinically important. Preserved ratio impaired spirometry (PRISm) has been linked to adverse health outcomes; however, its clinical impact on asthma remains incompletely defined. The aim of this study was to determine whether asthma with PRISm represents a distinct clinical phenotype characterised by an increased exacerbation burden.
Patients and Methods: We retrospectively analysed data from 1,411 adult patients with asthma. The patients were categorised into three groups according to %FEV1 and FEV1/FVC: control (n=1102), PRISm (n=133), and airflow obstruction groups (n=176). Clinical characteristics and asthma exacerbation profiles were compared among the groups.
Results: Age, sex, smoking status, and body mas index (BMI) significantly differed among the groups. The PRISm group had a significantly higher frequency of severe acute exacerbations than the control group, whereas no significant difference was observed between the PRISm and airflow obstruction groups. Severe asthma was more frequent in the PRISm group than in the control group, but its frequency was comparable between the PRISm and airflow obstruction groups. In multinomial logistic regression analysis, relative to the control group, the PRISm group was characterised by higher BMI (1.08 (1.03– 1.13), adjusted odds ratio (95% confidence interval)), longer asthma duration (1.02 (1.00– 1.03)), and higher severe acute exacerbation (2.31 (1.46– 3.64)). Relative to the airflow obstruction group, the PRISm group was characterised by higher BMI (1.15 (1.07– 1.24)) and shorter asthma duration (0.97 (0.96– 0.99)), while the frequency of severe acute exacerbations (1.39 (0.78– 2.48)) did not differ significantly between them.
Conclusion: Asthma with PRISm may represent a distinct and clinically relevant phenotype associated with a substantial exacerbation burden. Its clinical importance lies not merely in its spirometric profile, but in the identification of a subgroup of patients who may require closer surveillance and earlier optimisation of management.
Keywords: asthma phenotype, acute exacerbation of asthma, obesity, preserved ratio impaired spirometry
Introduction
Asthma is a heterogeneous disease with diverse clinical presentations and treatment responses.1–4 This heterogeneity contributes to substantial variations in disease burden and prognosis across patients. Among its clinical consequences, variability in exacerbation risk deserves particular attention, because exacerbations impair quality of life, increase healthcare utilisation, and often necessitate systemic corticosteroid treatment. Therefore, reducing exacerbation risk is a major objective of contemporary asthma management. Recent population-based work using machine-learning feature-importance analysis has further highlighted the multifactorial nature of asthma attacks and the importance of identifying clinical features associated with attack risk.5 Accordingly, identifying clinically relevant phenotypes associated with a high exacerbation burden is essential for improving risk assessment and informing tailored management strategies.
Preserved ratio impaired spirometry (PRISm) has attracted increasing attention in recent years. It is defined by a reduced forced expiratory volume in 1 second (FEV1), despite a preserved FEV1/forced vital capacity (FVC) ratio.6 Although this spirometric pattern does not meet the diagnostic criteria for chronic obstructive pulmonary disease, previous studies in general populations have shown that PRISm is associated with adverse health outcomes, including more frequent respiratory symptoms,6–8 a higher burden of comorbidities,9–12 and increased mortality.13,14 These observations suggest that PRISm is not merely a spirometric variation, but a condition with potentially important clinical consequences.
Given its association with adverse health outcomes in general populations, the coexistence of PRISm may also be clinically important in asthma. The clinical features often associated with PRISm, such as obesity and a higher burden of comorbidities, are not always shared by patients with airflow obstruction and may modify the clinical expression and progression of asthma. Therefore, distinguishing PRISm from airflow obstruction may have implications for prognosis, monitoring strategies, and tailored asthma management. Recent studies have supported this possibility by demonstrating that patients with asthma and PRISm had more frequent exacerbations, poorer symptom control, and a higher prevalence of small-airway dysfunction.15,16 In particular, Cottini et al characterised the PRISm phenotype across asthma severities and reported its association with a greater annual exacerbation burden and small-airway dysfunction.15 The multivariable analyses in those studies primarily addressed comparisons between PRISm and normal spirometry, thereby establishing that PRISm is associated with worse outcomes than preserved lung function. In contrast, whether asthma with PRISm differs clinically from asthma with obstructive ventilatory defects has not been sufficiently examined in corresponding multivariable analyses. This distinction is clinically important because PRISm may otherwise be interpreted merely as an intermediate spirometric pattern between normal spirometry and obstruction, rather than as a distinct phenotype with its own exacerbation burden. Therefore, the present study aimed to clarify the clinical position of PRISm in asthma by comparing patients with PRISm not only with those with normal spirometry but also with those with obstructive ventilatory defects. Clarifying this issue may help identify patients who require closer surveillance and earlier optimisation of management.
On the basis of these observations, we hypothesised that asthma with coexisting PRISm represents a distinct and clinically relevant phenotype. Accordingly, this study aimed to examine the clinical characteristics and exacerbation profile of patients with asthma and PRISm in comparison with those with normal spirometry and obstructive ventilatory defects.
Materials and Methods
Study Population
In this study, we used data from the “FD asthma database”, which was established previously.17 The database includes clinical information on patients with asthma who regularly attended the outpatient clinic of the Department of Allergy and Respiratory Medicine at The Fraternity Memorial Hospital in 2015. The database includes demographic details, comorbidities, asthma characteristics, types of asthma controller medications, frequency of severe acute exacerbations (assessed during the 2 years preceding enrolment and expressed as the annual number of exacerbations), and spirometry and laboratory data obtained during the stable asthma phase within 2 years before enrolment in the database. The inclusion criteria for the database were as follows: 1) asthma diagnosed according to the diagnostic flow chart presented in Box 1–1 of the Global Initiative for Asthma (GINA) guidelines 2015;18 2) regular attendance at our hospital and consistent use of asthma controller medications for at least 2 years prior to enrolment; 3) available spirometry data obtained during the stable asthma phase; and 4) no evidence of other respiratory diseases that could influence spirometry data, such as previous tuberculosis, diffuse emphysema, bronchiolitis, interstitial lung disease, or other diffuse lung diseases. Clinical and laboratory data were obtained from electronic medical records to establish the database.
Study Design
Data from adult patients with asthma aged 18–80 years were extracted from the database. The enrolled patients with asthma were categorised into three groups according to %FEV1 and FEV1/FVC: control (%FEV1 ≥80% and FEV1/FVC ≥70%), PRISm (%FEV1 <80% and FEV1/FVC ≥70%), and airflow obstruction (%FEV1 <80% and FEV1/FVC <70%) groups. Clinical characteristics and exacerbation profiles were compared among the three groups to examine the clinical position of asthma with PRISm relative to the control and airflow obstruction groups. This study was approved by the Research Ethics Committee of the Fraternity Memorial Hospital (reference number: 185) and conducted in accordance with the principles of the Declaration of Helsinki. As this was a retrospective study, the need for informed consent was waived through an opt-out approach.
Data Collection
All data were obtained from the FD asthma database. For the database, spirometry data, eosinophil counts, and radioallergosorbent test (RAST) results for allergen-specific immunoglobulin E (IgE) were collected from medical records. All spirometry and laboratory measurements were obtained during stable asthma phases. Allergen-specific IgE was considered positive when the level was 0.35 UA/mL or higher. Spirometry was performed by trained technicians in accordance with American Thoracic Society (ATS)/European Respiratory Society (ERS) recommendations. Reference values for spirometric indices were calculated using the prediction equations for Japanese individuals established by the Japanese Respiratory Society.19 Pre-bronchodilator spirometric values were used for the analysis. Measurements were excluded if they showed evidence of suboptimal effort, coughing during the manoeuvre, premature termination, or clearly implausible values. Severe asthma was defined according to the ERS/ATS guidelines for severe asthma.20 High-dose inhaled corticosteroid (ICS) use was classified using the ICS dose thresholds specified in ERS/ATS guidelines.20 “Severe acute exacerbation of asthma” was defined as an event requiring an emergency room visit and hospitalisation for treatment with systemic corticosteroids or an increase in the systemic corticosteroid dose from the stable maintenance level for ≥ 3 days.21 Height and body weight were measured at the time of spirometry, and BMI was calculated as weight in kilograms divided by height in metres squared. Obesity was defined according to the criteria of the Japan Society for the Study of Obesity as a body mass index (BMI) ≥25 kg/m2, as this cut-off maximises the sensitivity and specificity for obesity-related disorders in the Japanese population.22 This threshold is generally regarded as equivalent to BMI ≥30 kg/m2 in Western populations.
Statistical Analysis
Data were compared using Kruskal‒Wallis tests followed by post hoc Dunn’s tests. Chi-square tests were employed to compare the proportions of categorical variables. When chi-square tests indicated significance, pairwise multiple comparisons of categorical variables were performed. Multinomial logistic regression analysis was performed with the study group as the dependent variable to identify clinical characteristics independently associated with the PRISm group. To characterise the clinical position of asthma with PRISm relative to the other spirometric patterns, we first constructed two multinomial logistic regression models in which spirometric-pattern classification was used as the dependent variable. In these models, the control group and the airflow obstruction group were used as the reference categories, respectively, allowing asthma with PRISm to be evaluated in relation to both comparison groups. We then performed a multivariable logistic regression analysis using the presence or absence of a history of severe exacerbation as the dependent variable and spirometric-pattern classification as the primary exposure to evaluate whether this classification was independently associated with severe exacerbation after adjustment for relevant clinical covariates. For variables with missing data, analyses were performed using complete case analysis; missing values were not imputed. Statistical significance was set at p<0.05. For pairwise multiple comparisons of categorical variables, a p-value <0.016 was considered significant following the Bonferroni correction. All statistical analyses were performed using SPSS software version 29 (IBM, Armonk, NY, USA).
Results
Demographic and Clinical Characteristics
A total of 1,411 patients with asthma were included in the analysis: 1,102, 133, and 176 in the control, PRISm, and airflow obstruction groups, respectively. Demographic and clinical characteristics are summarised in Table 1. Age, sex distribution, smoking history, and BMI differed significantly among the three groups. The airflow obstruction group was older, whereas the PRISm group had a higher BMI and a greater prevalence of obesity than the other two groups.
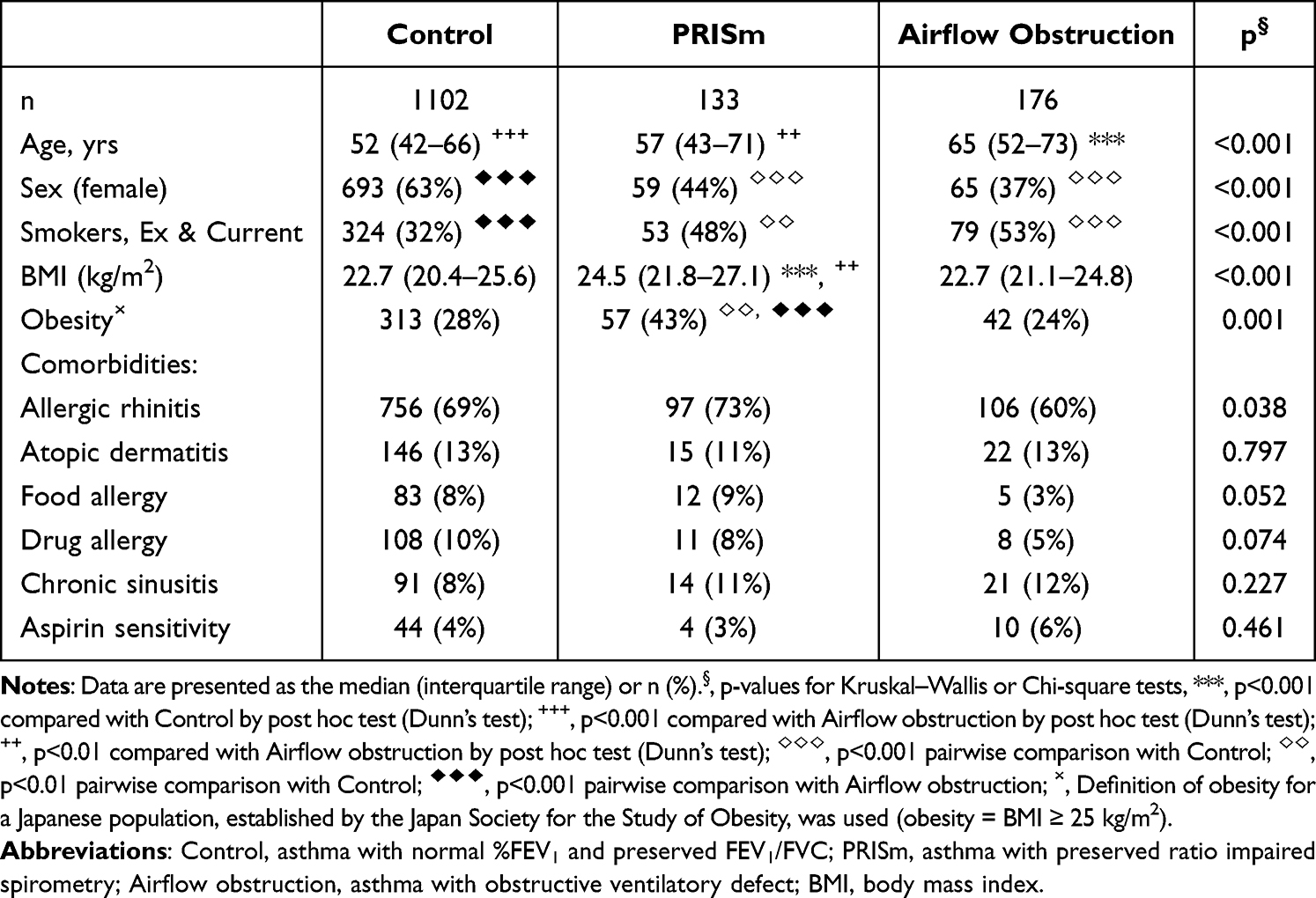 |
Table 1 Patient Demographic Data |
Exacerbation Burden, Asthma Severity, and Treatment
Asthma characteristics and treatment patterns are summarised in Table 2. Disease duration differed significantly among the three groups. Post hoc analysis showed that disease duration was significantly longer in the airflow obstruction group than in both the PRISm and control groups. The proportion of patients with severe asthma also differed significantly among the groups. Pairwise comparisons revealed that severe asthma was more frequent in the PRISm group than in the control group, whereas no significant difference was observed between the PRISm and airflow obstruction groups. Treatment patterns also differed significantly among the groups. The proportion of patients receiving high-dose inhaled corticosteroids and/or daily oral corticosteroids was significantly higher in the PRISm group than that in the control group, whereas no significant difference was observed between the PRISm and airflow obstruction groups. The proportion of patients with severe acute exacerbations also varied significantly among the groups (control: 24%, Prism: 40% and airflow obstruction: 30%, p<0.001). Post hoc analysis showed that severe acute exacerbations occurred more frequently in the PRISm group than in the control group (p<0.001), whereas the difference between the PRISm and airflow obstruction groups was not statistically significant.
 |
Table 2 Asthma Characteristics and Treatments |
Laboratory Data and Pulmonary Function Tests
The laboratory data and pulmonary function test results are summarised in Table 3. Significant differences in eosinophil counts and IgE levels were observed among the three groups. The eosinophil counts and IgE levels were higher in the PRISm group than those in the control group. According to the chi-square test, the proportion of patients with positive RAST results for house dust and/or mite allergens also differed significantly among the groups; however, pairwise comparisons did not identify significant differences between the PRISm group and either comparator group. Pulmonary function parameters differed significantly across the three groups.
 |
Table 3 Laboratory and Pulmonary Function Tests |
Factors Independently Associated with Asthma with PRISm
Multinomial logistic regression analyses were performed to examine the clinical variables distinguishing the PRISm group from the control and airflow obstruction groups. Candidate covariates for multivariable logistic regression were selected based on clinical relevance and prior evidence and included age, sex, BMI, smoking history, asthma duration, eosinophil count, IgE level, and the presence or absence of a history of severe exacerbation. Relative to the control group, the PRISm group was characterised by male predominance (0.54 (0.34–0.87), adjusted odds ratio (95% confidence interval), p=0.011)), higher BMI (1.08 (1.03–1.13), p=0.003), longer asthma duration (1.02 (1.00–1.03), p=0.030), and a higher proportion of patients with severe acute exacerbations (2.31 (1.46–3.64), p<0.001), whereas age and blood eosinophil count were not significantly associated. Relative to the airflow obstruction group, the PRISm group was characterised by younger age (0.97 (0.95–0.99), p=0.004), higher BMI (1.15 (1.07–1.24), p<0.001), and shorter asthma duration (0.97 (0.96–0.99), p=0.003). Notably, the proportion of patients with severe acute exacerbations (1.39 (0.78–2.48), p=0.267) did not significantly differ between the PRISm and airflow obstruction groups (Table 4).
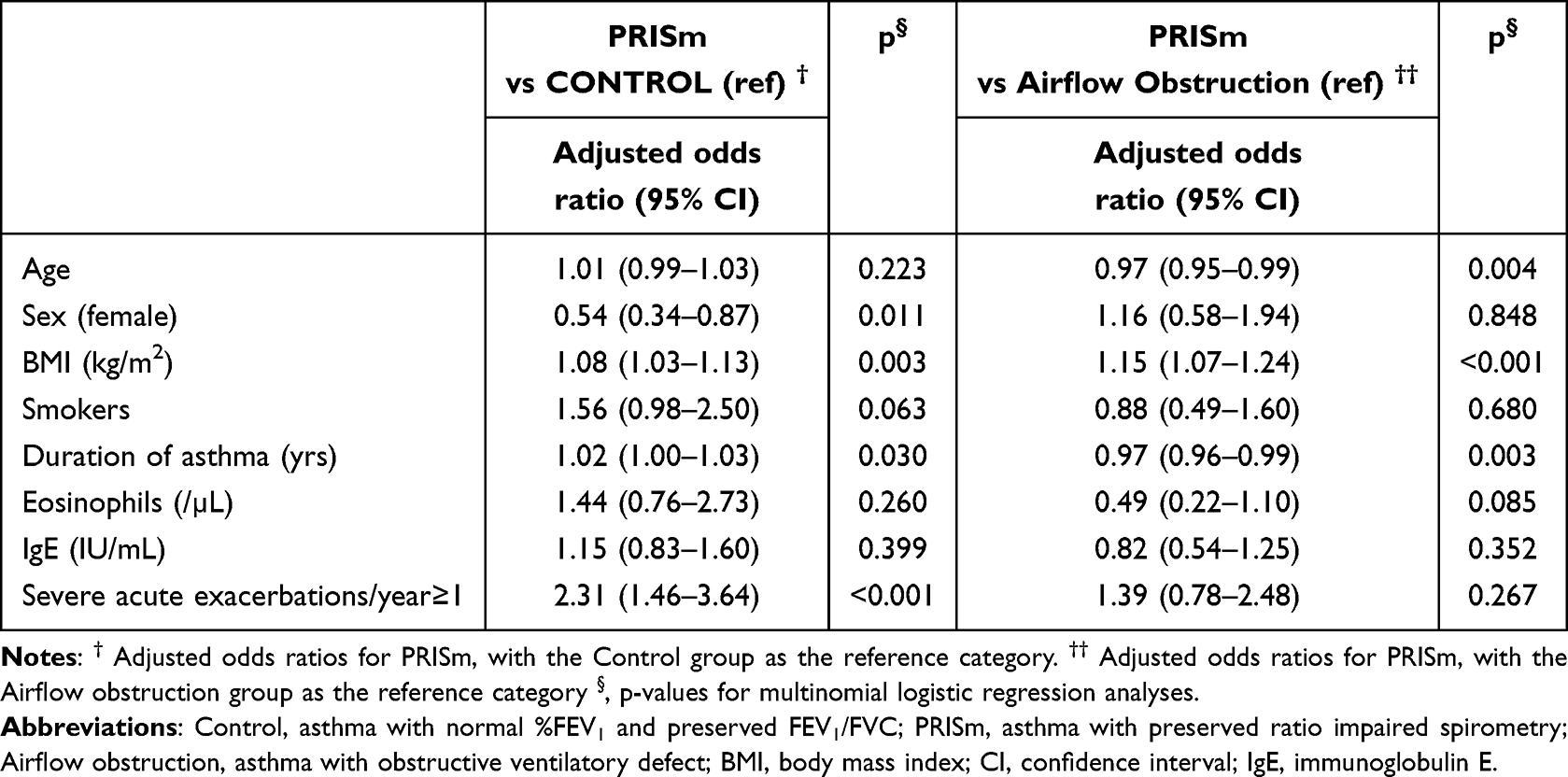 |
Table 4 Multinomial Logistic Regression Analysis Variables Related to Distinct Case Characteristics |
We then performed a multivariable logistic regression analysis using the presence or absence of a history of severe exacerbation as the dependent variable and spirometric-pattern classification as the primary exposure variable, adjusting for the same covariates used in the multinomial logistic regression models described above. With the control group as the reference category, the PRISm group had significantly higher odds of severe exacerbation (2.27 (1.44–3.58), p<0.001). When the airflow obstruction group was used as the reference category, the odds of severe exacerbation did not differ significantly between the PRISm group and those with airflow obstruction (1.37 (0.77–2.42), p=0.286).
Discussion
Our findings suggest that asthma with coexisting PRISm should be recognised not merely as a spirometric abnormality, but also as a clinically relevant phenotype characterised by an increased exacerbation burden. Compared with patients with normal %FEV1 and FEV1/FVC, those with PRISm had a higher proportion of patients with severe acute exacerbations, and this burden was comparable to that observed in patients with obstructive ventilatory defects (adjusted odds ratio: 1.37, 95% confidence interval: 0.77–2.42). In addition, patients with PRISm showed a distinct clinical profile, including higher BMI and an intermediate asthma duration between the control and airflow obstruction groups. Together, these findings suggest that PRISm in asthma may identify a clinically relevant subgroup associated with greater exacerbation burden and distinct clinical characteristics.
A key finding of this study is that patients with asthma accompanied by PRISm had a substantial exacerbation burden despite the absence of overt obstructive ventilatory impairment. This finding is consistent with recent multicentre data showing that, compared with normal spirometry, asthma with PRISm is associated with more frequent exacerbations.15 Given previous reports showing that a lower FEV1/FVC ratio is associated with a higher risk of exacerbation and that longer disease duration is linked to greater disease severity,23,24 the airflow obstruction group would ordinarily be expected to have a greater exacerbation burden than the PRISm group. However, exacerbation frequency was comparable between the 2 groups. This observation is clinically important because it suggests that asthma with PRISm may represent a vulnerable subgroup whose exacerbation risk is not adequately explained by conventional markers such as airflow obstruction or disease duration alone.
These findings raise the possibility that factors linked to PRISm may be associated with the exacerbation burden observed in this subgroup. Among the clinical features associated with asthma with PRISm, elevated BMI may be one factor to consider. In multinomial analyses, higher BMI remained independently associated with PRISm after adjustment for covariates. This observation is consistent with previous reports linking obesity to PRISm in non-asthmatic populations.9,10 Given that the asthma and PRISm subgroup was characterised by a greater exacerbation burden, elevated BMI may be better interpreted as a clinically meaningful feature of this phenotype rather than as a coincidental comorbidity. This interpretation is biologically plausible, because obesity can adversely affect asthma outcomes through multiple mechanisms, including mechanical constraint of the respiratory system, adipose tissue-driven inflammation, oxidative stress, and related metabolic abnormalities.25–30 Accordingly, elevated BMI may be one clinical factor associated with the poorer outcomes observed in patients with asthma and coexisting PRISm.
Several limitations should be acknowledged. First, owing to the cross-sectional design, a causal relationship between PRISm, obesity, and exacerbation risk cannot be established. Second, this was a single-centre retrospective study conducted exclusively in Japanese patients, which may limit the generalisability of the findings to other populations. Furthermore, the retrospective design carries an inherent risk of selection bias, as the study population was limited to patients who performed spirometry during routine clinical practice, potentially overrepresenting individuals with respiratory symptoms. Third, PRISm was defined on the basis of spirometric findings at a single time point during a stable phase of asthma; therefore, misclassification due to temporal variability in lung function or differences in spirometry timing remains possible. The longitudinal stability of PRISm could not be assessed and should be examined in future prospective studies. Fourth, treatment intensity could not be included as an objectively defined covariate in this retrospective database; therefore, residual confounding related to treatment intensity may remain.
Conclusion
Our study identifies asthma with coexisting PRISm as a clinically important phenotype characterised by increased exacerbation burden. The clinical significance of this subgroup lies not merely in its spirometric profile, but also in its association with exacerbation burden comparable to that observed in asthma with obstructive ventilatory defect. Recognition of asthma with coexisting PRISm may have potential clinical implications for identifying patients who may benefit from closer monitoring and more proactive optimisation of management. Further longitudinal and mechanistic studies are warranted to clarify the biological basis and clinical course of this phenotype.
Acknowledgments
Parts of this work were previously presented in abstract form at American Thoracic Society International Conference 2026 under the title ‘Asthma With Preserved Ratio Impaired Spirometry: A Distinct Phenotype Associated With Obesity and Exacerbation Risk.31
Funding
There is no funding to report.
Disclosure
YT received lecture fees from Novartis Pharma, GlaxoSmithKline, AstraZeneca, and Sanofi. However, they are unrelated to the current manuscript. All other authors declare that they have no significant conflicts of interest with any companies/organizations whose products or services are discussed in this article.
References
1. Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. 2012;18:716–9. doi:10.1038/nm.2678
2. Sharma S, Gerber AN, Kraft M, Wenzel SE. Asthma pathogenesis: phenotypes, therapies, and gaps: summary of the aspen lung conference 2023. Am J Respir Cell Mol Biol. 2024;71:154–168. doi:10.1165/rcmb.2024-0082WS
3. Gonzalez-Uribe V, Romero-Tapia SJ, Castro-Rodriguez JA. Asthma phenotypes in the era of personalized medicine. J Clin Med. 2023;12:1–21. doi:10.3390/jcm12196207
4. Moore WC, Meyers DA, Wenzel SE, et al. Identification of asthma phenotypes using cluster analysis in the severe asthma research program. Am J Respir Crit Care Med. 2010;181:315–323. doi:10.1164/rccm.200906-0896OC
5. Huang AA, Huang SY. Use of feature importance statistics to accurately predict asthma attacks using machine learning: a cross-sectional cohort study of the US population. PLoS One. 2023;18:e0288903. doi:10.1371/journal.pone.0288903
6. Wan ES, Castaldi PJ, Cho MH, et al. Epidemiology, genetics, and subtyping of preserved ratio impaired spirometry (PRISm) in COPDGene. Respir Res. 2014;15:89. doi:10.1186/s12931-014-0089-y
7. Kogo M, Sato S, Muro S, et al. Longitudinal changes and association of respiratory symptoms with preserved ratio impaired spirometry (PRISm): the nagahama study. Ann Am Thorac Soc. 2023;20:1578–1586. doi:10.1513/AnnalsATS.202301-050OC
8. Phillips DB, James MD, Vincent SG, et al. Physiological characterization of preserved ratio impaired spirometry in the CanCOLD study: implications for exertional dyspnea and exercise intolerance. Am J Respir Crit Care Med. 2024;209:1314–1327. doi:10.1164/rccm.202307-1184OC
9. Wan ES, Balte P, Schwartz JE, et al. Association between preserved ratio impaired spirometry and clinical outcomes in US adults. JAMA. 2021;326:2287–2298. doi:10.1001/jama.2021.20939
10. Higbee DH, Granell R, Davey Smith G, Dodd JW. Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir Med. 2022;10:149–157. doi:10.1016/S2213-2600(21)00369-6
11. Choi H, Oak CH, Jung MH, Jang TW, Nam SJ, Yoon T. Trend of prevalence and characteristics of preserved ratio impaired spirometry (PRISm): nationwide population-based survey between 2010 and 2019. PLoS One. 2024;19:e0307302. doi:10.1371/journal.pone.0307302
12. Kim J, Lee CH, Lee HY, Kim H. Association between comorbidities and preserved ratio impaired spirometry: using the korean national health and nutrition examination survey IV-VI. Respiration. 2022;101:25–33. doi:10.1159/000517599
13. Wijnant SRA, De Roos E, Kavousi M, et al. Trajectory and mortality of preserved ratio impaired spirometry: the Rotterdam study. Eur Respir J. 2020;55:1901217. doi:10.1183/13993003.01217-2019
14. Washio Y, Sakata S, Fukuyama S, et al. Risks of mortality and airflow limitation in japanese individuals with preserved ratio impaired spirometry. Am J Respir Crit Care Med. 2022;206:563–572. doi:10.1164/rccm.202110-2302OC
15. Cottini M, Poto R, Bhattacharjee A, et al. Characterizing the preserved ratio impaired spirometry phenotype in all severities of asthma. Respir Med. 2025;244:108180. doi:10.1016/j.rmed.2025.108180
16. Shi X, Li Q, Hu Z, Yang L, Wang Y, Nie H. Preserved ratio impaired spirometry and mortality in non-smoking asthma: a population-based cohort study. J Asthma. 2025;62:1893–1901. doi:10.1080/02770903.2025.2526388
17. To M, Arimoto Y, Honda N, Kurosawa Y, Haruki K, To Y. Clinical characteristics and cytokine profiles of adult obese asthma with type2 inflammation. Sci Rep. 2023;13:14799. doi:10.1038/s41598-023-41889-6
18. Global Initiative for Asthma. Global strategy for asthma management and prevention. 2015. Available from: https://ginasthma.org/wp-content/uploads/2016/01/GINA_Report_2015_Aug11-1.pdf.
19. Kubota M, Kobayashi H, Quanjer PH, Omori H, Tatsumi K, Kanazawa M. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig. 2014;52:242–250. doi:10.1016/j.resinv.2014.03.003
20. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43:343–373. doi:10.1183/09031936.00202013
21. Reddel HK, Taylor DR, Bateman ED, et al. An official American thoracic society/european respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180:59–99. doi:10.1164/rccm.200801-060ST
22. Examination Committee of Criteria for ‘Obesity Disease’ in Japan. Japan society for the study of obesity, new criteria for ‘obesity disease’ in Japan. Circ J. 2002;66:987–992. doi:10.1253/circj.66.987
23. Paterson F, On JY, Ahmed D, et al. Real-life evaluation of novel forced expiratory ratios with asthma exacerbations and symptoms. Ann Allergy Asthma Immunol. 2025;135:663–667.e1. doi:10.1016/j.anai.2025.08.015
24. To M, Tsuzuki R, Katsube O, et al. Persistent asthma from childhood to adulthood presents a distinct phenotype of adult asthma. J Allergy Clin Immunol Pract. 2020;8:1921–7.e2. doi:10.1016/j.jaip.2020.01.011
25. To M, Arimoto Y, Honda N, et al. Elevated oxidative stress and steroid insensitivity in patients with asthma and high body fat percentage. Ann Allergy Asthma Immunol. 2025;134:664–670. doi:10.1016/j.anai.2025.03.009
26. Tashiro H, Kurihara Y, Kuwahara Y, Takahashi K. Impact of obesity in asthma: possible future therapies. Allergol Int. 2024;73:48–57. doi:10.1016/j.alit.2023.08.007
27. To M, Hitani A, Kono Y, et al. Obesity-associated severe asthma in an adult Japanese population. Respir Investig. 2018;56:440–447. doi:10.1016/j.resinv.2018.07.003
28. Gibeon D, Batuwita K, Osmond M, et al. Obesity-associated severe asthma represents a distinct clinical phenotype: analysis of the British thoracic society difficult asthma registry patient cohort according to BMI. Chest. 2013;143:406–414. doi:10.1378/chest.12-0872
29. Dixon AE, Poynter ME. Mechanisms of asthma in obesity. pleiotropic aspects of obesity produce distinct asthma phenotypes. Am J Respir Cell Mol Biol. 2016;54:601–608. doi:10.1165/rcmb.2016-0017PS
30. To M, Kono Y, Ogura N, et al. Obesity-related systemic oxidative stress: an important factor of poor asthma control. Allergol Int. 2018;67:147–149. doi:10.1016/j.alit.2017.06.002
31. To M, Arimoto Y, Honda N, Haruki K, To Y. B22-06 asthma with preserved ratio impaired spirometry: a distinct phenotype associated with obesity and exacerbation risk. Am J Respir Crit Care Med. 2026;212:S286. doi:10.1093/ajrccm/aamag162.398
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.